Introduction
Metformin is a first-line oral hypoglycemic drug and
the most widely used drug for the treatment of type 2 diabetes
(1). Metformin is easily accessed in
clinical practice owing to its low-cost (2) and mild adverse drug reactions (3). The use of metformin has also been
reported to reduce the risk of certain types of cancer in patients
with type 2 diabetes mellitus (DM) (4–7).
Preclinical studies have indicated that metformin can inhibit the
proliferation of cancer cells in vitro and in vivo
(8), and simultaneously induce
apoptosis (9). Numerous clinical
studies have reported that metformin has an antineoplastic effect
on several types of malignancy, including colon cancer (4), gastric cancer (GC) (10), pancreatic cancer (11), breast cancer (12), and prostate cancer (5).
GC is one of the most common cancer types and the
second-leading cause of cancer-associated morbidity (13) owing to its high degree of malignancy,
and the recurrence and mortality rates are high, even following
radical resection and adjuvant radiation and chemotherapy. The
5-year overall survival (OS) rate is <25% (14).
To the best of our knowledge, no comprehensive
systematic review has reported the effect of metformin use on GC
patients with diabetes. Therefore, in the present study, a
systematic review was conducted to elucidate the potential effect
of metformin on GC among diabetic patients.
Materials and methods
Search strategy
Relevant articles were searched in major medical
databases, including PubMed (www.ncbi.nlm.nih.gov/pubmed; date of access, June 30
2016), EMBASE (www.embase.com; date of access, June
30 2016) and the Cochrane Library (www.cochranelibrary.com; date of access, June 30
2016). All English-language articles published prior to June 30th
2016 were searched using the keywords ‘metformin’,
‘dimethylbiguanide’, ‘metformin hydrochloride’, ‘metformin HCl’,
‘gastrointestinal neoplasms’, ‘digestive system neoplasms’,
‘stomach neoplasms’, ‘gastric cancer’, and ‘gastric neoplasms’. The
references of the relevant meta-analyses and systematic reviews
were then examined to identify other potentially relevant
studies.
Inclusion and exclusion criteria
The following studies met the inclusion criteria: i)
Studies that evaluated GC patients treated with metformin and
compared them with patients who used other antidiabetic drugs; ii)
studies that evaluated the association between metformin and GC
using the hazard ratio (HR) or adjusted HR and 95% confidence
intervals (CIs); and iii) retrospective or prospective cohort
studies, randomized clinical trials, and case-control studies. If
the data were from the same authors or institutes, only the most
recent article or the highest-quality article was included. The
following types of articles were excluded: i) Reviews, letters,
conference abstracts, and comments; ii) preclinical experiments on
metformin and GC in vitro and in vivo; and iii)
studies that evaluated the use of metformin for other metabolic or
endocrine diseases, such as endometriosis and polycystic ovary
syndrome.
Data extraction and quality
assessment
Two authors (Drs Peiwen Li and Cong Zhang)
independently reviewed the included articles and extracted data on
the study authors, year of publication, country, study design,
number of participants, patient age, follow-up, control groups
(treatment with insulin, sulfonylurea or thiazolidinedione, among
others), adjusting variables, adjusted hazard ratio (AHR) and 95%
CI, and conclusions (Table I). Any
disagreement between the two authors was resolved by consulting a
third author. The Newcastle-Ottawa Scale (NOS) (15) was used to assess the quality of the
studies. NOS scores ≥7 (NOS scores=7,8,9) were defined as high
quality studies. NOS scores ≥4 were defined as moderate quality
studies (NOS scores=4,5,6) and NOS scores=1,2,3 were defined as low
quality studies (Table II).
 | Table I.Summary of basic characteristics of
the articles included in this review. |
Table I.
Summary of basic characteristics of
the articles included in this review.
| Author, year | Country | Study design | Number of
patients | Patient age range,
years | Follow-up
duration | Control group
(non-metformin use) | Adjusting
variables | AHR (95% CI) | Conclusions | (Refs.) |
|---|
| Lee et al,
2016 | Korea | RC | 1,974 | 22–89(median,
59) | Median, 6.2 years;
range, 4.7–7.8 years | Sulfonylurea,
meglitinide, α-glucosidase inhibitors, thiazolidinediones, DPP-4
inhibitors, insulin | Sex, age, BMI,
insulin usage, postoperative chemotherapy, stage | Overall survival,
0.87 (0.801–0.945); cancer-specific survival, 0.865 (0.782–0.958);
recurrence-free survival, 0.864 (0.797–0.937) | Each additional
cumulative 6 months of metformin use after gastrectomy, the
recurrence, all-cause mortality and cancer-specific mortality rates
were decreased by 13.6%, 13.0% and 13.5%, respectively | (20) |
| Valent, 2015 | Italy | RC | 1,196,243 | 20–94 | NA | Sulfonylureas,
combinations of OGLDs, α-glucosidase inhibitors,
thiazolidinediones, DPP-4 inhibitors, others | Sex, age at start
of observation (years), time when prescription of each drug started
(time-dependent variable), total number of prescriptions of all the
other drugs | 0.990
(0.986–0.994) | Metformin was
associated with a reduced risk of most forms of digestive cancer;
sulfonylureas reduced stomach and pancreatic cancer risk | (18) |
| Kim et al,
2014 | Korea | RC | 39,989 | 30–97 | Insulin non-user
group: range, 0.5–7.0 years; median, 4.5 years; IQR, 2.4–6.0 years.
Regular insulin user group: range, 0.5–7.0 years; median, 4.6
years; IQR, 2.5–6.0 years. 3,943 patients were treated as censored
cases due to mortality | Regular insulin
users | Sex, age,
residential area, other antidiabetic drug use | In insulin
non-users, AHR of metformin was 0.73 (0.53–1.01); in insulin
non-users, in Model 1, AHR for duration of metformin use was 0.88
(0.81–0.96); in Model 2, duration of metformin use was >3 years,
AHR was 0.57 (0.37–0.87) | Duration of
metformin use >3 years is associated with a significantly
reduced GC risk in DM patients who do not use insulin | (10) |
| Ruiter et
al, 2012 | Netherlands | RC | 85,289 | ≥18 | (Mean ± SD)
1,031±853 days | Sulfonylurea
derivatives | Age at first OGLD,
sex, year in which the first OGLD prescription was dispensed,
number of unique drugs used in the year, number of hospitalizations
in the year before the start of the OGLD | AHR of metformin
compared with sulfonylurea derivatives, 0.83 (0.76–0.90) | Long-term metformin
use is associated with a lower risk of cancer compared with l
ong-term sulfonylurea derivatives use | (19) |
| Lee et al,
2011 | Taiwan | PC | 480,984 | ≥20 | DM with metformin
use: mean ± SD, 3.90±2.08 years; median ± IQR, 3.76±3.44 years | Non-metformin
users | Age, sex, other
oral antihyperglycemic medication, CCI score, duration of metformin
exposure (time-dependent variable) | AHR for metformin
use compared with any other oral antihyperglycemic medication, 1.41
(0.42–4.73) | Metformin can
decrease the incidence rates of several gastroenterological
cancers, but not GC | (21) |
| Table II.Assessment of the risk of bias in
each cohort study using the Newcastle-Ottawa scale. |
Table II.
Assessment of the risk of bias in
each cohort study using the Newcastle-Ottawa scale.
|
| Selection | Comparability | Outcome |
|
|
|
|---|
|
|
|
|
|
|
|
|
|---|
| Author, year | REC | SNEC | AE | DO | SC | AF | AO | FU | AFU | Total | Quality | (Refs.) |
|---|
| Lee et al,
2016 | − | + | + | + | − | − | + | + | − | 5 | Moderate | (20) |
| Valent, 2015 | + | + | + | + | − | − | + | + | − | 6 | Moderate | (18) |
| Kim et al,
2014 | + | + | + | + | − | − | + | + | − | 6 | Moderate | (10) |
| Ruiter et
al, 2012 | + | + | + | + | − | − | + | + | − | 6 | Moderate | (19) |
| Lee et al,
2011 | + | + | + | + | − | − | + | + | − | 6 | Moderate | (21) |
Statistical analysis
Statistical analysis was performed with Stata
software (version 12.0; StataCorp, College Station, TX, USA). The
AHR and 95% CI were used to estimate the association between
metformin and GC risk, and P<0.05 was considered to indicate
statistical significance. A P value <0.01 with an I2
value of >50% indicated substantial heterogeneity. The inverse
variance method with a fixed-effects model was applied if no
heterogeneity was detected, whereas a random-effects model was used
in the alternative cases.
Results
Search results
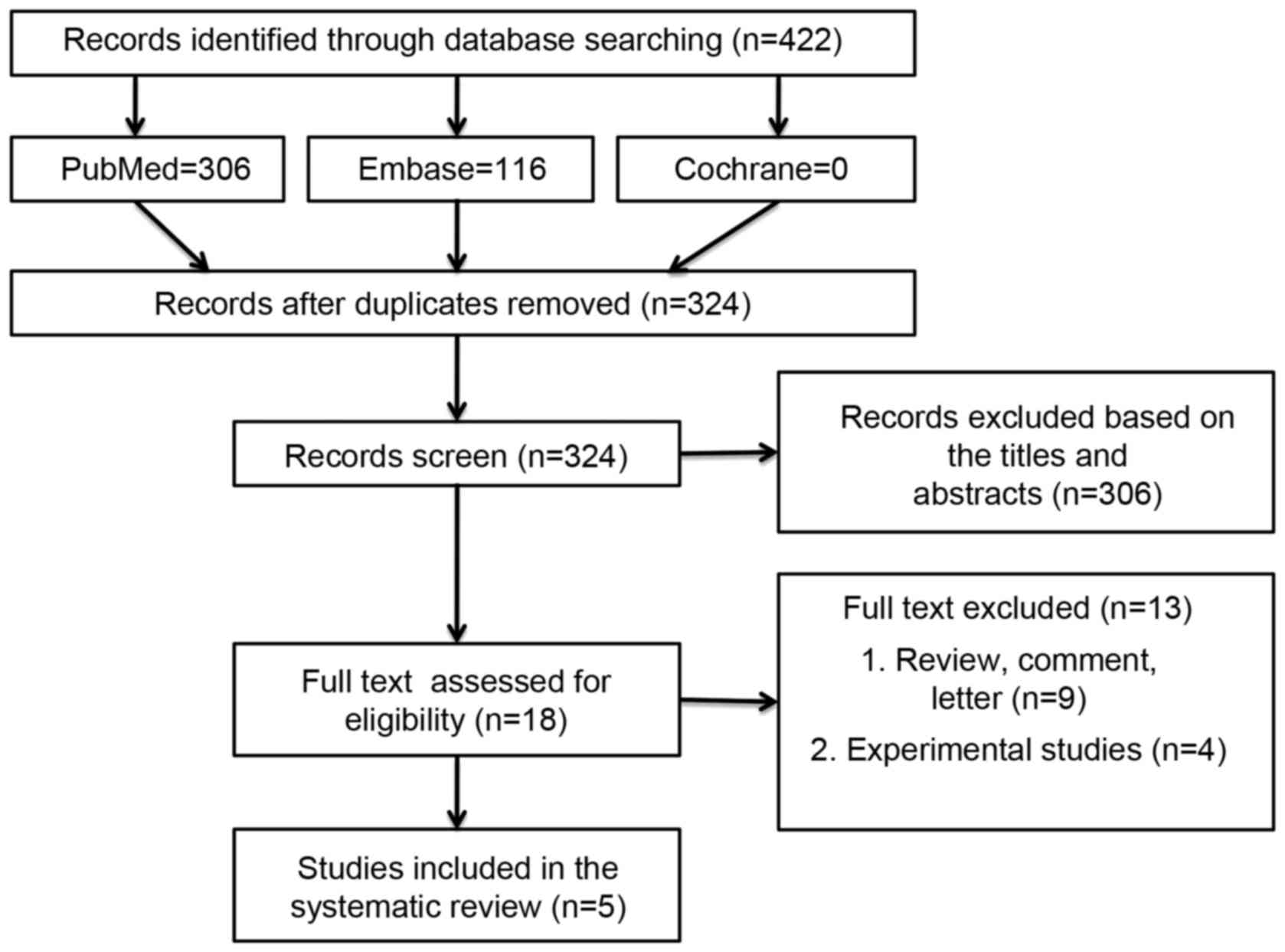
A total of 422 studies were initially identified,
and 98 were excluded owing to duplication. After reviewing titles
and abstracts, an additional 306 articles were excluded. The full
texts of 18 studies were then thoroughly reviewed. Of these, 13
articles were removed due to the publication type. Therefore, 5
studies were eventually included in the analysis. No additional
articles from the references were added to this review. Two
randomized controlled trials (RCTs) [A Diabetes Outcome Progression
Trial (ADOPT) (16) and Rosiglitazone
Evaluated for Cardiovascular Outcomes and Regulation of Glycemia in
Diabetes (RECORD) (17)] were
excluded from this review: In ADOPT, only one GC patient was
included, and no additional detailed information was available to
be extracted for comparison; and in RECORD, the gastric and
intestinal malignancies were counted together, which prevented the
determination of the number of cases of GC. The flow chart of the
selection criteria is shown in Fig.
1.
Study characteristics
All the selected articles were cohort studies,
including four retrospective cohort studies and one prospective
cohort study. The populations of the studies came from European
countries (18,19) and Asian countries (10,20,21). Two
included studies focused on GC, whereas the other three studies
evaluated other general cancer types in addition to GC. The
heterogeneity among the articles was extensive, and included
differences in the definition of the subgroups, follow-up period,
drug comparators, dosage, and duration of treatment.
Metformin and risk of GC
Four studies were based on data from national or
local health databases, or health insurance population-based
databases, and therefore the bias of selection was almost
negligible. However, these studies did not evaluate the same
confounding factors, including body mass index (BMI), obesity,
glucose level, glycated hemoglobin (HbA1c), smoking history,
lifestyle, dietary habits, and Helicobacter pylori
infection, as the databases containing all the information
necessary to estimate the effect of metformin were unavailable.
Valent (18) compared
the effect of the use of metformin together with other oral
hypoglycemic drugs (sulfonylureas, α-glucosidase inhibitors, and
thiazolidinediones, not including insulin) on the risk of various
digestive cancers. These authors found that type 1 or type 2
diabetes was associated with increased risk of digestive cancer.
Metformin use reduced the risk of the majority of digestive
cancers, including GC (AHR, 0.990; 95% CI, 0.986–0.994). Of note
was that the effect of sulfonylurea on GC was similar to that of
metformin (AHR, 0.989; 95% CI, 0.981–0.997).
Kim et al (10)
distinguished metformin users from regular users of insulin and
non-users of insulin. In the non-users of insulin cohort, patients
treated with metformin had a significantly lower rate of GC
compared with those not treated with metformin (P=0.047); whereas
no significant difference in the rate of GC was observed among the
regular users of insulin (P=0.379). In the group of non-users of
insulin, the authors divided the duration of metformin use into
four time intervals and detected a 43% decrease in the risk of GC
in DM patients who had used metformin for >3 years, after
adjusting for covariates (AHR, 0.57; 95% CI, 0.37–0.87;
P=0.009).
Ruiter et al (19) compared the risk of general cancer
between patients using metformin and those using sulfonylurea
derivatives, and found that the long-term use of metformin was
associated with a lower probability of cancer in general compared
with the use of sulfonylurea derivatives. Metformin presented a
lower risk of GC compared with sulfonylurea derivatives (AHR, 0.83;
95% CI, 0.76–0.90). The authors emphasized that the lower risk of
cancer in the metformin group and the actual decrease in the risk
of cancer by metformin were two different concepts. The comparison
of models on the basis of different covariables indicated that the
risk of cancer was lower in the metformin group compared with the
sulfonylurea group; however, this result did not prove that
metformin decreased the risk of cancer.
Lee et al (21)
performed a prospective cohort study in Taiwan and found that
metformin treatment reduced the incidence of total and specific
cancers (colorectal, liver, and pancreatic) compared with the
absence of treatment with metformin. For GC, their results
disagreed with those of previous studies, and metformin did not
significantly reduce the incidence of cancer (AHR, 1.41; 95% CI,
0.42–4.73).
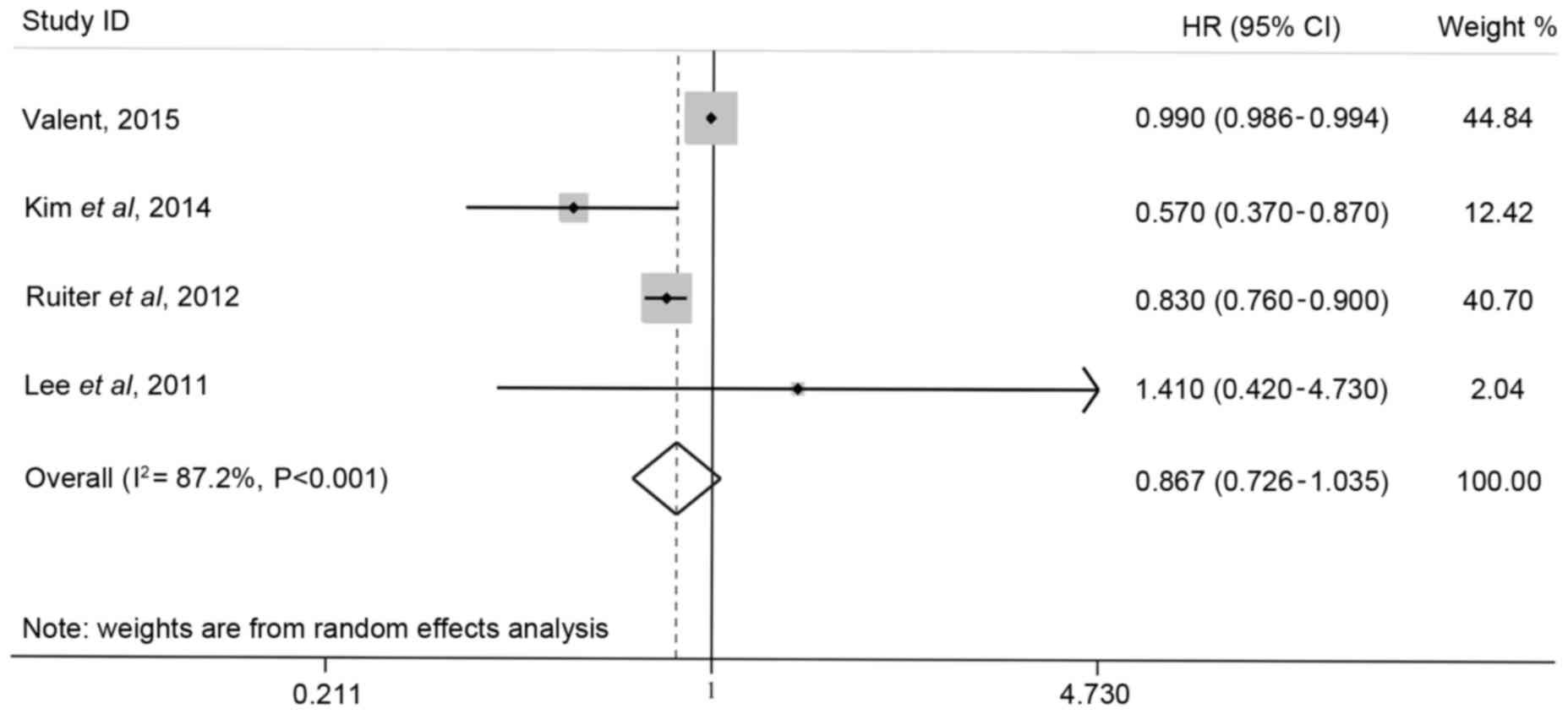
In the present study, the overall effect of
metformin on the risk of GC was determined by conducting a
meta-analysis using HRs combined with 95% CIs. The risk of GC in
the groups that used metformin cumulatively was lower than that in
other study groups, although there was no statistically significant
difference (overall HR, 0.867; 95% CI, 0.726–1.035;
I2=87.2%; Fig. 2).
Metformin and survival of GC
Lee et al (20)
evaluated 1,974 patients with GC who were subjected to curative
gastrectomy, and found that the non-diabetic patients had markedly
better OS, cancer-specific survival (CSS), and recurrence-free
survival (RFS) rates compared with the diabetic patients. By
contrast, the prognosis of patients with DM treated with metformin
was significantly more favorable than in those not treated with
metformin [OS HR, 0.584 (95% CI, 0.369–0.926); CSS HR, 0.57 (95%
CI, 0.334–0.975); RFS HR, 0.633 (95% CI, 0.410–0.977)]. The
improvement in the survival of DM patients treated with metformin
was similar to that of non-diabetic patients, particularly in stage
III patients. Furthermore, the results of the multivariable
analysis indicated that the decreased risks of recurrence,
cancer-specific mortality, and all-cause mortality were strongly
associated with each additional 6 months of metformin use [OS AHR,
0.870 (95% CI, 0.801–0.845); CSS AHR, 0.865 (95% CI, 0.782–0.958);
RFS AHR, 0.864 (95% CI, 0.797–0.937)]. As there was only one study
regarding the effect of metformin on the survival of GC, a
meta-analysis on this was not conducted.
Discussion
Several epidemiological studies have observed an
increased risk of cancer (22–26),
including stomach cancer (27–29),
colon, breast, endometrial, liver, pancreatic and bladder cancer
(30,31), and prostate cancer (32), in DM patients; however, the precise
underlying mechanisms have not been elucidated. Factors such as
insulin resistance, secondary hyperinsulinemia, sex hormones and
inflammatory cytokines may be associated with each other and may
promote tumor cell proliferation in vitro and in vivo
via insulin or insulin-like growth factor (IGF) pathways (26,33). A few
studies reported that diabetes or hyperglycemia was a
tumor-promoting factor for GC. Ikeda and Kiyohara (34) showed that elevated fasting blood
glucose greatly increased the incidence of GC and, although other
risk factors were adjusted for, including H. pylori
infection, a moderate increase in the HbA1c level remained a
promoter of GC. Zhou et al (35) determined that hyperglycemia promoted
the progression of GC via aquaporin 3 (AQP3); the in vitro
expression of AQP3 increased when the glucose levels increased, and
AQP3 was overexpressed in GC, leading to the increased migration of
cancer cells.
Metformin is the most widely prescribed oral
antidiabetic drug for patients with type 2 diabetes. Increasing
evidence has demonstrated the anticancer capacity of metformin. A
recent meta-analysis by Wu et al (36) in 2015 evaluated the use of metformin
in patients with type 2 diabetes and indicated that this use was
associated with 14 and 30% reductions in the rates of cancer
incidence and mortality, respectively. Furthermore, other
meta-analyses (37–40) obtained similar results, suggesting an
overall decrease in the risk of cancer by metformin.
Although several laboratory and epidemiological
studies have shown that metformin may serve a general antitumor
role in DM patients, it remains unclear whether metformin can
reduce the risk of specific types of cancer, such as GC. Therefore,
this systematic review was conducted to elucidate this issue. Three
studies (10,18,19) found
that metformin reduced the risk of GC, whereas one study (21) showed that metformin could reduce the
risk of other cancers, excluding GC. A recent clinical study
(20) reported that metformin
improved the survival of GC in diabetic patients subjected to
gastrectomy by decreasing the recurrence, all-cause mortality, and
cancer-specific mortality rates.
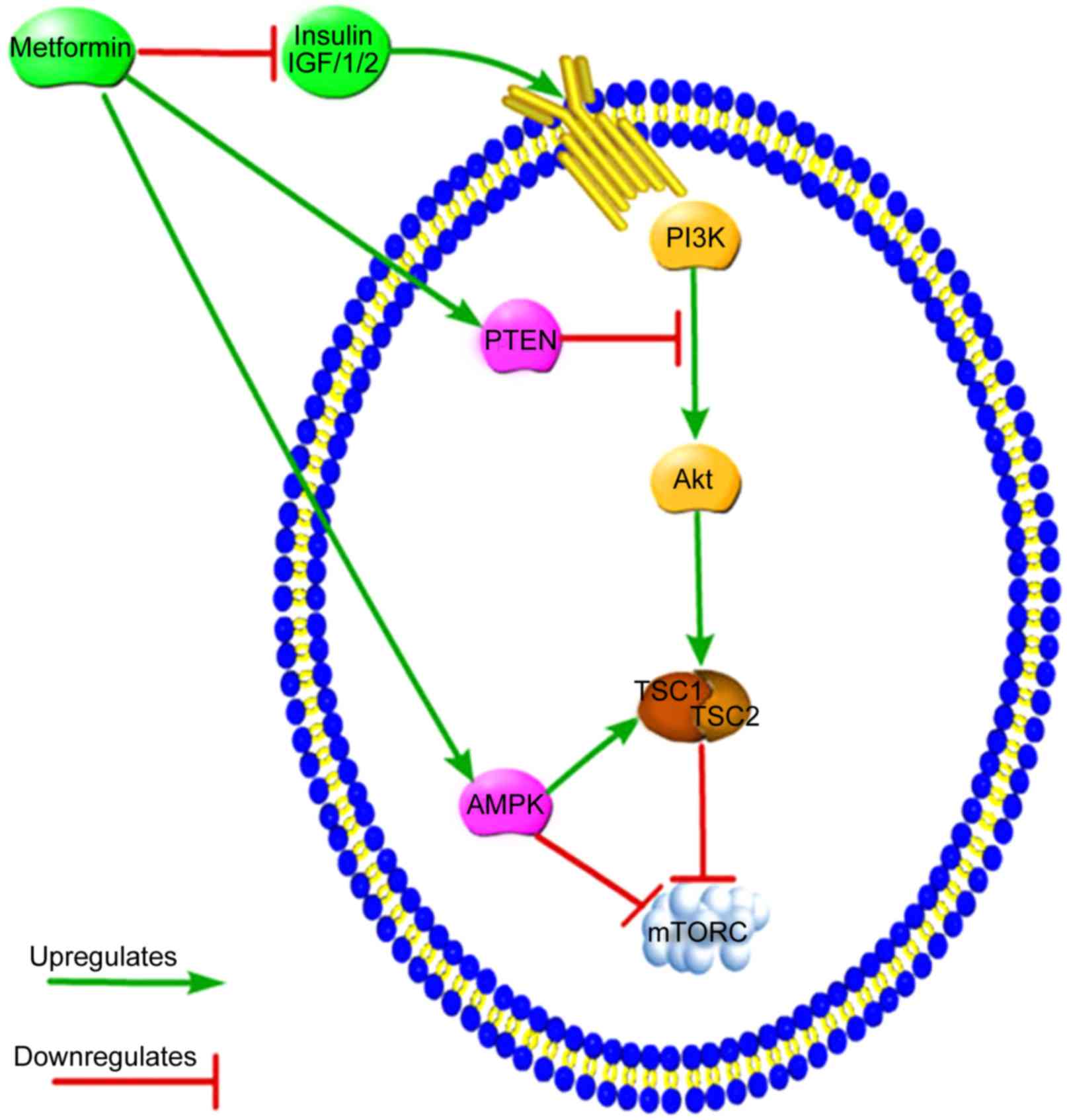
Mammalian target of rapamycin (mTOR) is a downstream
target and intersection of numerous signaling pathways and
functions as a modulator of protein synthesis, cellular growth,
cellular proliferation, autophagy and metabolism. mTOR is composed
of mTOR complex (mTORC)1 and mTORC2. Insulin or IGF1/2 can activate
the phosphatidylinositide 3-kinase (PI3K)-Akt-mTOR signaling
pathway primarily via mTORC1, thus promoting protein synthesis and
cellular growth and proliferation (41,42).
Metformin may indirectly reduce the circulating insulin levels by
increasing the sensitivity of peripheral tissues to insulin,
thereby impairing the insulin or IGF pathways (42). Phosphatase and tensin homolog deleted
on chromosome ten (PTEN) functions as a cancer suppressor by
negatively regulating Akt via interruption of the upstream signal
from PI3K, and metformin may exert its effect by increasing the
level of PTEN and inhibiting mTORC1 expression (43). Metformin directly activates adenosine
monophosphate-activated protein kinase (AMPK), which induces the
suppression of mTORC1 expression, ultimately decreasing cell growth
and proliferation (44). Tuberous
sclerosis complex (TSC)1 and TSC2 are proteins encoded by the
mutated tumor-suppressor gene in TSC disease (45); the TSC1/2 complex inhibits mTORC1
activity, while Akt suppresses the activity of TSC2 by
phosphorylation (46). AMPK promotes
the formation of the TSC1/2 complex, which inhibits mTORC1 activity
(47). Therefore, PTEN and AMPK can
suppress tumors by targeting upstream molecules of the mTOR pathway
(Fig. 3).
Zhou et al (48) conducted a review and found that
metformin could regulate miRNA directly and subsequently modulate
downstream genes to prevent oncogenesis and therapy. Kato et
al (8) found that metformin could
inhibit GC cell proliferation and tumor growth by depressing
cell-cycle factors via the modulation of miRNA expression in
vitro and in vivo. In addition, these authors reported
that different treatment periods and metformin concentrations may
lead to differential miRNA expression, which suggests that the
duration and dose of metformin should be considered on an
individual basis. Yu et al (43) showed that metformin inhibited cell
proliferation and tumor growth by targeting certain essential genes
that affect tumor growth, proliferation and metastasis. The authors
suggested that the dosage of metformin should be kept low, and that
treatment should be continuous. The results of the studies by Kato
et al (8) and Yu et al
(43) agreed with those of Lee et
al (20) and Kim et al
(10), who proposed that the
long-term use of metformin could improve survival and significantly
reduce the risk of GC.
Two of the studies (18,19)
included in this review evaluated another type of common
hypoglycemic drug, sulfonylureas or sulfonylurea derivatives.
Sulfonylureas are frequently prescribed with metformin for type 2
DM. As insulin secretagogues, sulfonylureas increase insulin and
IGF levels, which promote tumorigenesis (49); however, it is still debatable whether
sulfonylurea derivatives can increase the risk of cancer (50). Glibenclamide was the first
second-generation sulfonylurea drug, and it functions by targeting
sulfonylurea receptors (SURs). To date, a number of studies have
indicated that glibenclamide can inhibit the growth of various
types of cancer (51–54); however, the antitumor mechanisms have
not been fully elucidated. In recent years, certain studies have
focused on potassium (K+) channels, which are involved
in physiological cellular functions, including insulin release,
cell proliferation, and apoptosis. Therefore, the regulation of
K+ channels may form the basis of a therapeutic method
for cancer (55–57). Adenosine triphosphate-sensitive
potassium channels (KATP channels) in the plasma and mitochondrial
membrane are made of SURs, and glibenclamide may target SURs by
closing KATP channels, leading to cell damage and
apoptosis (58).
A cohort study by Yang et al (59) involving 6,103 Chinese patients in Hong
Kong showed that the use of gliclazide and glibenclamide may reduce
the risk of cancer in a dose-dependent manner. Additionally, a
meta-analysis by Thakkar et al (37) demonstrated that metformin use reduced
cancer risk (supported by cohort and case-control studies but not
by RCTs) and that sulfonylurea use was associated with an increase
in all-cancer risk (supported by cohort studies, although
case-control studies and RCTs did not prove this association).
Ruiter et al (19)
hypothesized that it is less likely that sulfonylureas are a
cancer-promoting factor. These authors found that the outcomes of
patients treated with a combination of metformin and sulfonylureas
were similar to those of patients treated with metformin alone.
Notably, Valent (18) found that
sulfonylureas had a unique protective association with the stomach
and pancreas, and that sulfonylureas did not increase the incidence
of any type of cancer.
In contrast to the results of other studies, Lee
et al (21) found that
metformin had no correlation with a reduced risk of GC. The
possible reasons for this are as follows: i) The duration of
metformin varied significantly among the studies, which prevented
the accurate evaluation of the cumulative effect [duration of
treatment with metformin, 931±765 days (mean ± standard deviation);
755±1,200 days (median ± interquartile range)]; and ii) certain
underlying complementary drugs, such as aspirin (60), vitamin D (61), and statins (62), which have been found to be associated
with cancer risk, may have confounded the effect of metformin.
There were a number of limitations to the current
study. No RCTs have reported the specific risk of GC in patients
treated with metformin; therefore, the analyses were based on
retrospective and prospective cohort studies, and strong
conclusions could not be made because of the intrinsic
heterogeneity of these analyses. Only five articles met the
inclusion criteria of this study. The data of the four studies
(10,18,19,21)
included herein were obtained from national or local health
databases or health insurance companies, from which critical data
were not available, causing heterogeneity in the results.
To the best of our knowledge, this is the first
systematic review to evaluate the effect of metformin on the risk
of GC. Although only a few studies have focused on this subject to
date, the current evidence indicates that metformin is associated
with reduced risk of GC and improved survival in patients with type
2 diabetes. However, more well-designed trials are required to
elucidate the anticancer effect of metformin. Metformin does not
decrease normal blood sugar level and, for this reason, it may be
used by non-diabetic individuals as a protective agent against
cancer. However, large, rigorously designed, and high-quality
clinical trials are necessary to validate this possible effect.
Acknowledgements
This study was funded by the Natural Science
Foundation of Liaoning Province (grant no. 2014029201), the Program
of Education Department of Liaoning Province (grant no. L2014307),
the Key Laboratory Programme of Education Department of Liaoning
Province (grant no. LZ2015076) and the Scientific Programme of
Science & Technology Department of Liaoning Province (grant no.
2015225002).
References
|
1
|
Nathan DM, Buse JB, Davidson MB,
Ferrannini E, Holman RR, Sherwin R and Zinman B; American Diabetes
Association, ; European Association for the Study of Diabetes, :
Medical management of hyperglycaemia in type 2 diabetes mellitus: A
consensus algorithm for the initiation and adjustment of therapy: A
consensus statement from the American Diabetes Association and the
European Association for the Study of Diabetes. Diabetologia.
52:17–30. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Decensi A, Puntoni M, Goodwin P, Cazzaniga
M, Gennari A, Bonanni B and Gandini S: Metformin and cancer risk in
diabetic patients: A systematic review and meta-analysis. Cancer
Prev Res (Phila). 3:1451–1461. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Goodwin PJ, Ligibel JA and Stambolic V:
Metformin in breast cancer: Time for action. J Clin Oncol.
27:3271–3273. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Sehdev A, Shih YC, Vekhter B, Bissonnette
MB, Olopade OI and Polite BN: Metformin for primary colorectal
cancer prevention in patients with diabetes: A case-control study
in a US population. Cancer. 121:1071–1078. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Tseng CH: Metformin significantly reduces
incident prostate cancer risk in Taiwanese men with type 2 diabetes
mellitus. Eur J Cancer. 50:2831–2837. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
El-Benhawy SA and El-Sheredy HG: Metformin
and survival in diabetic patients with breast cancer. J Egypt
Public Health Assoc. 89:148–153. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Tseng CH: Metformin may reduce oral cancer
risk in patients with type 2 diabetes. Oncotarget. 7:2000–2008.
2016. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Kato K, Gong J, Iwama H, Kitanaka A, Tani
J, Miyoshi H, Nomura K, Mimura S, Kobayashi M, Aritomo Y, et al:
The antidiabetic drug metformin inhibits gastric cancer cell
proliferation in vitro and in vivo. Mol Cancer Ther. 11:549–560.
2012. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Han G, Gong H, Wang Y, Guo S and Liu K:
AMPK/mTOR-mediated inhibition of survivin partly contributes to
metformin-induced apoptosis in human gastric cancer cell. Cancer
Biol Ther. 16:77–87. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Kim YI, Kim SY, Cho SJ, Park JH, Choi IJ,
Lee YJ, Lee EK, Kook MC, Kim CG, Ryu KW and Kim YW: Long-term
metformin use reduces gastric cancer risk in type 2 diabetics
without insulin treatment: A nationwide cohort study. Aliment
Pharmacol Ther. 39:854–863. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Sadeghi N, Abbruzzese JL, Yeung SC, Hassan
M and Li D: Metformin use is associated with better survival of
diabetic patients with pancreatic cancer. Clin Cancer Res.
18:2905–2912. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Xu H, Chen K, Jia X, Tian Y, Dai Y, Li D,
Xie J, Tao M and Mao Y: Metformin use is associated with better
survival of breast cancer patients with diabetes: A meta-analysis.
Oncol. 20:1236–1244. 2015. View Article : Google Scholar
|
|
13
|
Yamamoto H, Watanabe Y, Maehata T, Morita
R, Yoshida Y, Oikawa R, Ishigooka S, Ozawa S, Matsuo Y, Hosoya K,
et al: An updated review of gastric cancer in the next-generation
sequencing era: Insights from bench to bedside and vice versa.
World J Gastroenterol. 20:3927–3937. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Durães C, Almeida GM, Seruca R, Oliveira C
and Carneiro F: Biomarkers for gastric cancer: Prognostic,
predictive or targets of therapy? Virchows Arch. 464:367–378. 2014.
View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Stang A: Critical evaluation of the
Newcastle-Ottawa scale for the assessment of the quality of
nonrandomized studies in meta-analyses. Eur J Epidemiol.
25:603–605. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Kahn SE, Haffner SM, Viberti G, Herman WH,
Lachin JM, Kravitz BG, Yu D, Paul G, Holman RR and Zinman B;
Diabetes Outcome Progression Trial (ADOPT) Study Group, :
Rosiglitazone decreases C-reactive protein to a greater extent
relative to glyburide and metformin over 4 years despite greater
weight gain: Observations from a Diabetes Outcome Progression Trial
(ADOPT). Diabetes Care. 33:177–183. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Home PD, Kahn SE, Jones NP, Noronha D,
Beck-Nielsen H and Viberti G; ADOPT Study Group, ; RECORD Steering
Committee, : Experience of malignancies with oral glucose-lowering
drugs in the randomised controlled ADOPT (A Diabetes Outcome
Progression Trial) and RECORD (Rosiglitazone Evaluated for
Cardiovascular Outcomes and Regulation of Glycaemia in Diabetes)
clinical trials. Diabetologia. 53:1838–1845. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Valent F: Diabetes mellitus and cancer of
the digestive organs: An Italian population-based cohort study. J
Diabetes Complications. 29:1056–1061. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Ruiter R, Visser LE, van Herk-Sukel MP,
Coebergh JW, Haak HR, Geelhoed-Duijvestijn PH, Straus SM, Herings
RM and Stricker BH: Lower risk of cancer in patients on metformin
in comparison with those on sulfonylurea derivatives: Results from
a large population-based follow-up study. Diabetes Care.
35:119–124. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Lee CK, Jung M, Jung I, Heo SJ, Jeong YH,
An JY, Kim HI, Cheong JH, Hyung WJ, Noh SH, et al: Cumulative
metformin use and its impact on survival in gastric cancer patients
after gastrectomy. Ann Surg. 263:96–102. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Lee MS, Hsu CC, Wahlqvist ML, Tsai HN,
Chang YH and Huang YC: Type 2 diabetes increases and metformin
reduces total, colorectal, liver and pancreatic cancer incidences
in Taiwanese: A representative population prospective cohort study
of 800,000 individuals. BMC cancer. 11:202011. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Lo SF, Chang SN, Muo CH, Chen SY, Liao FY,
Dee SW, Chen PC and Sung FC: Modest increase in risk of specific
types of cancer types in type 2 diabetes mellitus patients. Int J
Cancer. 132:182–188. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Zhang PH, Chen ZW, Lv D, Xu YY, Gu WL,
Zhang XH, Le YL, Zhu HH and Zhu YM: Increased risk of cancer in
patients with type 2 diabetes mellitus: A retrospective cohort
study in China. BMC Public Health. 12:5672012. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Yeh HC, Platz EA, Wang NY, Visvanathan K,
Helzlsouer KJ and Brancati FL: A prospective study of the
associations between treated diabetes and cancer outcomes. Diabetes
Care. 35:113–118. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Lee MY, Lin KD, Hsiao PJ and Shin SJ: The
association of diabetes mellitus with liver, colon, lung, and
prostate cancer is independent of hypertension, hyperlipidemia, and
gout in Taiwanese patients. Metabolism. 61:242–249. 2012.
View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Shi Y and Hu FB: The global implications
of diabetes and cancer. Lancet. 383:1947–1948. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Yoon JM, Son KY, Eom CS, Durrance D and
Park SM: Pre-existing diabetes mellitus increases the risk of
gastric cancer: A meta-analysis. World J Gastroenterol. 19:936–945.
2013. View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Ikeda F, Doi Y, Yonemoto K, Ninomiya T,
Kubo M, Shikata K, Hata J, Tanizaki Y, Matsumoto T, Iida M and
Kiyohara Y: Hyperglycemia increases risk of gastric cancer posed by
Helicobacter pylori infection: A population-based cohort study.
Gastroenterology. 136:1234–1241. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Yamagata H, Kiyohara Y, Nakamura S, Kubo
M, Tanizaki Y, Matsumoto T, Tanaka K, Kato I, Shirota T and Iida M:
Impact of fasting plasma glucose levels on gastric cancer incidence
in a general Japanese population: The Hisayama study. Diabetes
Care. 28:789–794. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Giovannucci E, Harlan DM, Archer MC,
Bergenstal RM, Gapstur SM, Habel LA, Pollak M, Regensteiner JG and
Yee D: Diabetes and cancer: A consensus report. CA Cancer J Clin.
60:207–221. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Noto H, Goto A, Tsujimoto T, Osame K and
Noda M: Latest insights into the risk of cancer in diabetes. J
Diabetes Investig. 4:225–232. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
32
|
Stopsack KH, Ziehr DR, Rider JR and
Giovannucci EL: Metformin and prostate cancer mortality: A
meta-analysis. Cancer Causes Control. 27:105–113. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
33
|
Belfiore A, Frasca F, Pandini G, Sciacca L
and Vigneri R: Insulin receptor isoforms and insulin
receptor/insulin-like growth factor receptor hybrids in physiology
and disease. Endoc Rev. 30:586–623. 2009. View Article : Google Scholar
|
|
34
|
Ikeda F and Kiyohara Y: Helicobacter
pylori infection and Hyperglycemia/Diabetes are associated with an
increased risk of gastric cancer. Gan To Kagaku Ryoho. 42:529–533.
2015.(In Japanese). PubMed/NCBI
|
|
35
|
Zhou Y, Wang Y, Wang S and Shen L:
Hyperglycemia promotes human gastric carcinoma progression via
aquaporin 3. Dig Dis Sci. 60:2338–2345. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
36
|
Wu L, Zhu J, Prokop LJ and Murad MH:
Pharmacologic therapy of diabetes and overall cancer risk and
mortality: A meta-analysis of 265 studies. Sci Rep. 5:101472015.
View Article : Google Scholar : PubMed/NCBI
|
|
37
|
Thakkar B, Aronis KN, Vamvini MT, Shields
K and Mantzoros CS: Metformin and sulfonylureas in relation to
cancer risk in type II diabetes patients: A meta-analysis using
primary data of published studies. Metabolism. 62:922–934. 2013.
View Article : Google Scholar : PubMed/NCBI
|
|
38
|
Franciosi M, Lucisano G, Lapice E,
Strippoli GF, Pellegrini F and Nicolucci A: Metformin therapy and
risk of cancer in patients with type 2 diabetes: Systematic review.
PLoS One. 8:e715832013. View Article : Google Scholar : PubMed/NCBI
|
|
39
|
Soranna D, Scotti L, Zambon A, Bosetti C,
Grassi G, Catapano A, La Vecchia C, Mancia G and Corrao G: Cancer
risk associated with use of metformin and sulfonylurea in type 2
diabetes: A meta-analysis. Oncologist. 17:813–822. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
40
|
Noto H, Goto A, Tsujimoto T and Noda M:
Cancer risk in diabetic patients treated with metformin: A
systematic review and meta-analysis. PLoS One. 7:e334112012.
View Article : Google Scholar : PubMed/NCBI
|
|
41
|
Sciarretta S, Volpe M and Sadoshima J:
Mammalian target of rapamycin signaling in cardiac physiology and
disease. Circ Res. 114:549–564. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
42
|
Pasello G, Urso L, Conte P and Favaretto
A: Effects of sulfonylureas on tumor growth: A review of the
literature. Oncologist. 18:1118–1125. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
43
|
Yu G, Fang W, Xia T, Chen Y, Gao Y, Jiao
X, Huang S, Wang J, Li Z and Xie K: Metformin potentiates rapamycin
and cisplatin in gastric cancer in mice. Oncotarget. 6:12748–12762.
2015. View Article : Google Scholar : PubMed/NCBI
|
|
44
|
Dowling RJ, Niraula S, Chang MC, Done SJ,
Ennis M, McCready DR, Leong WL, Escallon JM, Reedijk M, Goodwin PJ
and Stambolic V: Changes in insulin receptor signaling underlie
neoadjuvant metformin administration in breast cancer: A
prospective window of opportunity neoadjuvant study. Breast Cancer
Res. 17:322015. View Article : Google Scholar : PubMed/NCBI
|
|
45
|
Crino PB, Nathanson KL and Henske EP: The
tuberous sclerosis complex. N Engl J Med. 355:1345–1356. 2006.
View Article : Google Scholar : PubMed/NCBI
|
|
46
|
Huang J and Manning BD: A complex
interplay between Akt, TSC2 and the two mTOR complexes. Biochem Soc
Trans. 37:217–222. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
47
|
Qin L, Wang Z, Tao L and Wang Y: ER stress
negatively regulates AKT/TSC/mTOR pathway to enhance autophagy.
Autophagy. 6:239–247. 2014. View Article : Google Scholar
|
|
48
|
Zhou JY, Xu B and Li L: A new role for an
old drug: Metformin targets MicroRNAs in treating diabetes and
cancer. Drug Dev Res. 76:263–269. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
49
|
Pollak M: Insulin and insulin-like growth
factor signalling in neoplasia. Nat Rev Cancer. 8:915–928. 2008.
View Article : Google Scholar : PubMed/NCBI
|
|
50
|
Monami M, Lamanna C, Balzi D, Marchionni N
and Mannucci E: Sulphonylureas and cancer: A case-control study.
Acta Diabetol. 46:279–284. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
51
|
Núñez M, Medina V, Cricco G, Croci M,
Cocca C, Rivera E, Bergoc R and Martín G: Glibenclamide inhibits
cell growth by inducing G0/G1 arrest in the human breast cancer
cell line MDA-MB-231. BMC Pharmacol Toxicol. 14:62013. View Article : Google Scholar : PubMed/NCBI
|
|
52
|
Zhanping W, Xiaoyu P, Na C, Shenglan W and
Bo W: Voltage-gated K+ channels are associated with cell
proliferation and cell cycle of ovarian cancer cell. Gynecol Oncol.
104:455–460. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
53
|
Abdul M and Hoosein N: Voltage-gated
potassium ion channels in colon cancer. Oncol Rep. 9:961–964.
2002.PubMed/NCBI
|
|
54
|
Malhi H, Irani AN, Rajvanshi P, Suadicani
SO, Spray DC, McDonald TV and Gupta S: KATP channels regulate
mitogenically induced proliferation in primary rat hepatocytes and
human liver cell lines. Implications for liver growth control and
potential therapeutic targeting. J Biol Chem. 275:26050–26057.
2000. View Article : Google Scholar : PubMed/NCBI
|
|
55
|
Bonnet S, Archer SL, Allalunis-Turner J,
Haromy A, Beaulieu C, Thompson R, Lee CT, Lopaschuk GD, Puttagunta
L, Bonnet S, et al: A mitochondria-K+ channel axis is suppressed in
cancer and its normalization promotes apoptosis and inhibits cancer
growth. Cancer Cell. 11:37–51. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
56
|
Felipe A, Vicente R, Villalonga N,
Roura-Ferrer M, Martínez-Mármol R, Solé L, Ferreres JC and Condom
E: Potassium channels: New targets in cancer therapy. Cancer Detect
Prev. 30:375–385. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
57
|
Conti M: Targeting K+ channels for cancer
therapy. J Exp Ther Oncol. 4:161–166. 2004.PubMed/NCBI
|
|
58
|
Ardehali H and O'Rourke B: Mitochondrial
K(ATP) channels in cell survival and death. J Mol Cell Cardiol.
39:7–16. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
59
|
Yang X, So WY, Ma RC, Yu LW, Ko GT, Kong
AP, Ng VW, Luk AO, Ozaki R, Tong PC, et al: Use of sulphonylurea
and cancer in type 2 diabetes-The Hong Kong Diabetes Registry.
Diabetes Res Clin Pract. 90:343–351. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
60
|
Elwood PC, Gallagher AM, Duthie GG, Mur LA
and Morgan G: Aspirin, salicylates, and cancer. Lancet.
373:1301–1309. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
61
|
Jamshidinaeini Y, Akbari ME, Abdollahi M,
Ajami M and Davoodi SH: Vitamin D status and risk of breast cancer
in Iranian women: A case-control study. J Am Coll Nutr. 35:639–646.
2016. View Article : Google Scholar : PubMed/NCBI
|
|
62
|
Osmak M: Statins and cancer: Current and
future prospects. Cancer Lett. 324:1–12. 2012. View Article : Google Scholar : PubMed/NCBI
|