Introduction
Although the incidence of gastric cancer has
decreased, it remains one of the most common types of cancer and
one of the leading causes of cancer-associated mortality worldwide,
including the region of North-East Italy (1–3). In this
region of Italy, the yearly gastric cancer incidence was estimated
to be 23.7/100,000 males and 11.7/100,000 females (3).
Peritoneal carcinomatosis (PC) in gastric cancer is
considered a distant metastasis and is detected in ~60% of patients
with gastric cancer subsequent to typical curative treatment
(4). PC is frequently a fatal disease
and has limited treatment options. In particular, the Evolution of
Peritoneal Carcinomatosis 1 study demonstrated a median overall
survival (OS) of 3.1 months in patients with PC (5). Cytoreductive surgery (CRS) associated
with hyperthermic intraperitoneal chemotherapy (HIPEC) has been
revealed to exhibit a beneficial effect against PC in gastric
cancer in a phase III trial (6).
As PC is difficult to diagnose in the early stages
of the disease through clinical and instrumental techniques
(7,8),
it is important to quantify the prevalence of microscopic PC at the
time of primary surgery, and to analyse the possible risk factors
for the presence of PC. Additionally, it may be useful to enable
the planning of extensive loco-regional treatments, and to
potentially perform CRS with HIPEC in selected patients who possess
a high probability of exhibiting microscopic PC at the time of
primary surgery.
The aim of the present study was to analyse the
prevalence of microscopic PC in patients receiving surgical
treatment for epithelial gastric tumours, examine the prognostic
value of microscopic PC through OS analysis and identify potential
predictive factors for the presence of microscopic PC.
Materials and methods
Patients
The present study was retrospective and included 399
patients whom received surgery for epithelial gastric tumours
between January 2001 and July 2013 and the pathological specimen
was assessed at the University Hospital of Udine (Udine, Italy).
Follow-up data was available until July 2014. The present study was
approved by the internal review board of the Department of medical
area (University of Udine, Udine, Italy) and was conducted in
accordance with the Helsinki Declaration and following the dictates
of the general authorisation to process personal data for
scientific research purposes by the Italian Data Protection
Authority.
Only patients that had undergone an adequate gastric
resection, with negative microscopic margins and adequate resection
of regional lymphatics, including greater and lesser omenta were
included in the present study. All patients that presented with
macroscopic PC at the time of surgery were excluded from the
analyses, even if they underwent radical surgery with complete
resection of peritoneal metastases.
A total of 403 patients with epithelial gastric
cancer that underwent complete surgical resection, including
greater and lesser omenta, were identified. Among these, 399
patients were eligible for the present study. A total of 4 patients
with macroscopic PC were excluded from the analyses. The
clinicopathological characteristics of the patients included in the
present study are presented in Table
I.
 | Table I.Clinicopathological characteristics of
the study population. |
Table I.
Clinicopathological characteristics of
the study population.
| Clinicopathological
characteristic | Percentage of
patients (no./total) |
|---|
| Sex |
|
|
Female | 37.8 (151/399) |
| Male | 62.2 (248/399) |
| Tobacco smoke | 4.2 (5/120) |
| Alcohol
consumption | 4.2 (5/120) |
| Tumour
characteristics |
|
| Histological
type |
|
|
Adenocarcinoma intestinal
type | 64.4 (257/399) |
|
Adenocarcinoma diffuse
type | 25.8 (103/399) |
|
Adenocarcinoma mixed type | 9.8 (39/399) |
| Location of
cancer |
|
|
Fundus | 14.8 (59/399) |
| Body | 44.9 (179/399) |
|
Antrum-pylorus | 37.8 (151/399) |
| Site of
previous gastric surgery | 2.5 (10/399) |
| Tumour extent |
|
| Tis | 1.3 (5/399) |
| T1 | 17.5 (70/399) |
| T2 | 28.6 (114/399) |
| T3 | 45.4 (181/399) |
| T4 | 7.3 (29/399) |
| Nodal status |
|
| N0 | 37.8 (151/399) |
| N1 | 30.3 (121/399) |
| N2 | 19.5 (78/399) |
| N3 | 12.3 (49/399) |
| TNM stage |
|
| Stage
0 | 1.3 (5/399) |
| Stage
I | 30.3 (121/399) |
| Stage
II | 39.6 (158/399) |
| Stage
III | 28.8 (115/399) |
| Tumour grading |
|
| G1 | 7.1 (28/392) |
| G2 | 33.4 (131/392) |
| G3 | 59.4 (233/392) |
| Lymphatic and
vascular invasion | 21.6 (86/399) |
Patient data
Data for the selection of patients were gathered
from University Hospital of Udine clinical and pathological files.
The primary outcomes evaluated in the present study were the
prevalence of microscopic PC and the OS rate. The analyses of
predictive factors for the presence of microscopic PC was
considered as a secondary outcome. The following data about patient
and tumour characteristics were collected: Patient age (at
diagnosis), sex, weight, tobacco usage and alcohol consumption, and
the tumour histotype, location, size, lymph node status, grading,
lymphatic and vascular invasion (LVI), and whether microscopic PC
was present (determined by pathological examination of tissue
samples obtained during gastric resection). In addition, the
therapeutic management used, including neoadjuvant and adjuvant
chemotherapy, and radiotherapy, was analysed. Furthermore,
information concerning post-operative follow-up and eventual
cancer-associated mortality was collected in all cases from the
clinical files of University Hospital of Udine.
Tumour classification and staging
Tumour stage was defined according to the seventh
edition of the Tumor-Node-Metastasis (TNM) staging classification
for carcinomas of the stomach of the American Joint Committee on
Cancer and Union for International Cancer Control. Tumour histology
was classified according to the Lauren classification of gastric
tumours (9) and tumour grading was
performed according to the fourth edition of the World Health
Organization classification of tumours of the digestive system
(10). LVI was considered as present
or absent, and the presence of LVI was defined as
microscopically-detected lymphovascular invasion in ≥1-2 lymphatics
or small veins in a mounted specimen containing the deepest portion
of the tumour on a glass slide, as previously described (11). Tumour location was divided as follows:
Fundus, body, antrum-pylorus or site of previous gastric surgery.
In the category ‘site of previous gastric surgery’, 3 patients who
had undergone previous gastric bypass surgery for severe obesity
and 2 patients who underwent previous Billroth II gastric resection
for peptic ulcer disease were included (in the remaining 5 cases
the reason of surgery for benign conditions was unknown).
Treatment
All patients included in the present study were
classified as type III according to the Siewert-Stein
classification of adenocarcinomas of the esophagogastric junction
(12) and were treated according to
national comprehensive cancer network guidelines for gastric cancer
(12). Routine post-operative
follow-up was performed every 3–6 months for the first 2 years,
every 6–12 months from 2.5–5 years and every 12 months thereafter.
Blood cell counts and chemistry profiling were performed, in
addition to diagnostic imaging or endoscopy when appropriate.
Outcomes and groupings
In the present study, OS was defined as the time
from the primary surgical procedure to mortality due to gastric
cancer or the last registered follow-up. The definition of
microscopic PC was as previously defined (13): The presence of peritoneal nodules
demonstrated to be of a gastric cancer origin without any
microscopic evidence of lymph node architecture or tissue, which
were not identified by macroscopic intraoperative examination. The
study population was divided into two groups according to the
presence or absence of microscopic PC.
Statistical analysis
Data were analysed using R software (version 3.1.0;
R Foundation for Statistical Computing, Vienna, Austria), and
P<0.05 was considered to indicate a statistically significant
difference. Univariate analysis was performed using Fisher's exact
test or χ2 test in the case of categorical variables,
and a Wilcoxon signed-rank test or unpaired t-test in the case of
continuous variables. In addition, Kaplan-Meier survival curves
were constructed, and a log-rank test was used to compare the OS
rates between the study groups. In addition, the Cox proportional
hazard regression model was used to assess OS and adjusted in the
multivariate analysis for possible confounding factors. Univariate
and multivariate logistic regression analyses were performed with
the presence of microscopic PC considered a dependent variable, and
with the possible predictors selected from the univariate analysis
considered as independent variables. The final multivariate model
was obtained through stepwise regression analyses and was
determined to be the most predictive model for the presence of
microscopic PC. Receiver operator characteristic (ROC) curves were
produced, and the area under the curve (AUC) was used to assess the
accuracy of the prediction of the model.
Results
Clinicopathological characteristics of
patients with epithelial gastric cancer
Table I summarises the
clinicopathological characteristics of the study population. The
mean age at diagnosis was 69.97±11.71 years and the median weight
was 67 kilograms [interquartile range (IQR), 55–75 (data not
shown)]. The majority of the patients were male (62.2%; 248/399).
The median follow-up time was 25 months (IQR, 11–72; data not
shown). Histological analysis revealed that 64.4% of patients
(257/399) exhibited the histotype of adenocarcinoma of the
intestinal type, 25.8% of patients (103/399) exhibited
adenocarcinoma of a diffuse type and 9.8% of patients (39/399)
exhibited adenocarcinoma of a mixed type. Microscopic PC exhibited
a prevalence of 5.5% (22/399; data not shown). Additionally, the
majority of patients were TNM stage II and tumour grading G3.
Lymphatic and vascular invasion was present in 21.6% of patients
(86/399).
Clinicopathological characteristics of
patients with epithelial gastric cancer in the absence or presence
of microscopic PC
Table II summarises
the differences between patients with or without microscopic PC. No
significant differences were identified in the patients with or
without microscopic PC for age at diagnosis [70.95 years (±13.88)
vs. 69.92 years (±11.59) P>0.05]. and weight [61.00 (±6.56) vs.
67.83 (±16.38) P>0.05]. (data not shown). Among the patients
with microscopic PC, a significantly higher prevalence of: Tobacco
smoking (unfortunately with 279 missing data), adenocarcinoma of a
diffuse type, T4 tumour extent, N2 nodal status, TNM stage III,
tumour grading G3 and lymphatic and vascular invasion. Typically, a
higher tumour extent and positive nodal status were associated with
the presence of microscopic PC. In addition, tumours arising from
previous non-oncological gastric surgery were more common in the
group of patients with microscopic PC compared with the patients
without microscopic PC, yet no significant difference was
observed.
| Table II.Clinicopathological characteristics of
the study population subdivided by the presence or absence of
microscopic PC. |
Table II.
Clinicopathological characteristics of
the study population subdivided by the presence or absence of
microscopic PC.
|
| Microscopic PC
status, percentage of patients (no./total) |
|
|---|
|
|
|
|
|---|
| Clinicopathological
characteristic | Absent (n=377) | Present (n=22) | P-value |
|---|
| Sex |
|
|
|
|
Female | 37.9 (143/377) | 36.4 (8/22) | 0.883 |
|
Male | 62.1%
(234/377) | 63.6 (14/22) | 0.883 |
| Tobacco smoke | 3.4 (4/117) | 33.3 (1/3) | <0.050 |
| Alcohol
consumption | 4.3 (5/117) | 0 (0/3) | 0.715 |
| Tumour
characteristics |
|
|
|
| Histological
type |
|
|
|
|
Adenocarcinoma intestinal
type | 66 (249/377) | 36.4 (8/22) | <0.050 |
|
Adenocarcinoma diffuse
type | 24.4 (92/377) | 50 (11/22) | <0.050 |
|
Adenocarcinoma mixed type | 9.5 (36/377) | 13.6 (3/22) | 0.530 |
| Location of
cancer |
|
|
|
|
Fundus | 15.4 (58/377) | 4.5 (1/22) | 0.164 |
|
Body | 44 (166/377) | 59.1 (13/22) | 0.167 |
|
Antrum-pylorus | 38.5 (145/377) | 27.3 (6/22) | 0.293 |
| Site of
previous gastric surgery | 2.1 (8/377) | 9.1 (2/22) | 0.100 |
| Tumour extent |
|
|
|
|
Tis | 1.3 (5/377) | 0 (0/22) | 0.587 |
| T1 | 18.6 (70/377) | 0 (0/22) | <0.050 |
| T2 | 29.2 (110/377) | 18.2 (4/22) | 0.267 |
| T3 | 44.8 (169/377) | 54.5 (12/22) | 0.373 |
| T4 | 6.1 (23/377) | 27.3 (6/22) | <0.050 |
| Nodal status |
|
|
|
| N0 | 39.3 (148/377) | 13.6 (3/22) | <0.050 |
| N1 | 30.2 (114/377) | 31.8 (7/22) | 0.876 |
| N2 | 18.6 (70/377) | 36.4 (8/22) | <0.050 |
| N3 | 11.9 (45/377) | 18.2 (4/22) | 0.386 |
| TNM stage |
|
|
|
| Stage
0 | 1.3 (5/377) | 0 (0/22) | 0.587 |
| Stage
I | 32.1 (121/377) | 0 (0/22) | <0.050 |
| Stage
II | 39 (147/377) | 50 (11/22) | 0.305 |
| Stage
III | 27.6 (104/377) | 50 (11/22) | <0.050 |
| Tumour grading |
|
|
|
| G1 | 7.6 (28/370) | 0 (0/22) | 0.181 |
| G2 | 34.9 (129/370) | 9.1 (2/22) | <0.050 |
| G3 | 57.6 (213/370) | 90.9 (20/22) | <0.050 |
| Lymphatic and
vascular invasion | 17.8 (67/377) | 86.4 (19/22) | <0.050 |
Predictive factors for microscopic
PC
Table III summarises
the univariate and the multivariate logistic regression analyses,
highlighting the most predictive factors considered in the final
multivariate model identified by step-wise regression analysis.
Tobacco smoke was excluded from this analysis due to missing data.
The final multivariate regression model considered the following
factors: Adenocarcinoma of a diffuse type, lymphatic and vascular
invasion, cancer location at the site of a previous gastric surgery
and tumour extent >T2. This model presented an AUC of the ROC
curve of 88.7% [95% confidence interval (CI), 80.9–96.5%]. The most
significant predictive factor was the presence of lymphatic and
vascular invasion.
| Table III.Univariate and multivariate logistic
regression analyses. |
Table III.
Univariate and multivariate logistic
regression analyses.
|
| Univariate
analysis | Multivariate
analysis |
|---|
|
|
|
|
|---|
| Independent
variable | OR (95% CI) | P-value | OR (95% CI) | P-value |
|---|
| Adenocarcinoma
diffuse type | 3.11
(1.3–7.42) | <0.050 | 2.92
(1.08–7.9) | <0.050 |
| Site of previous
gastric surgery | 4.52
(0.9–22.72) | 0.067 | 4.87
(0.69–34.57) | 0.113 |
| Tumour extent
>T2 | 4.17
(1.39–12.56) | <0.050 | 2.59
(0.79–8.46) | 0.116 |
| Nodal status
>N0 | 3.94
(1.15–13.57) | <0.050 | – | – |
| Tumour grading
G3 | 7.37
(1.7–32) | <0.050 | – | – |
| Lymphatic and
vascular invasion | 28.64
(8.24–99.58) | <0.050 | 22.65
(6.4–80.22) | <0.050 |
OS rate of patients with epithelial
gastric cancer in the absence or presence of microscopic PC
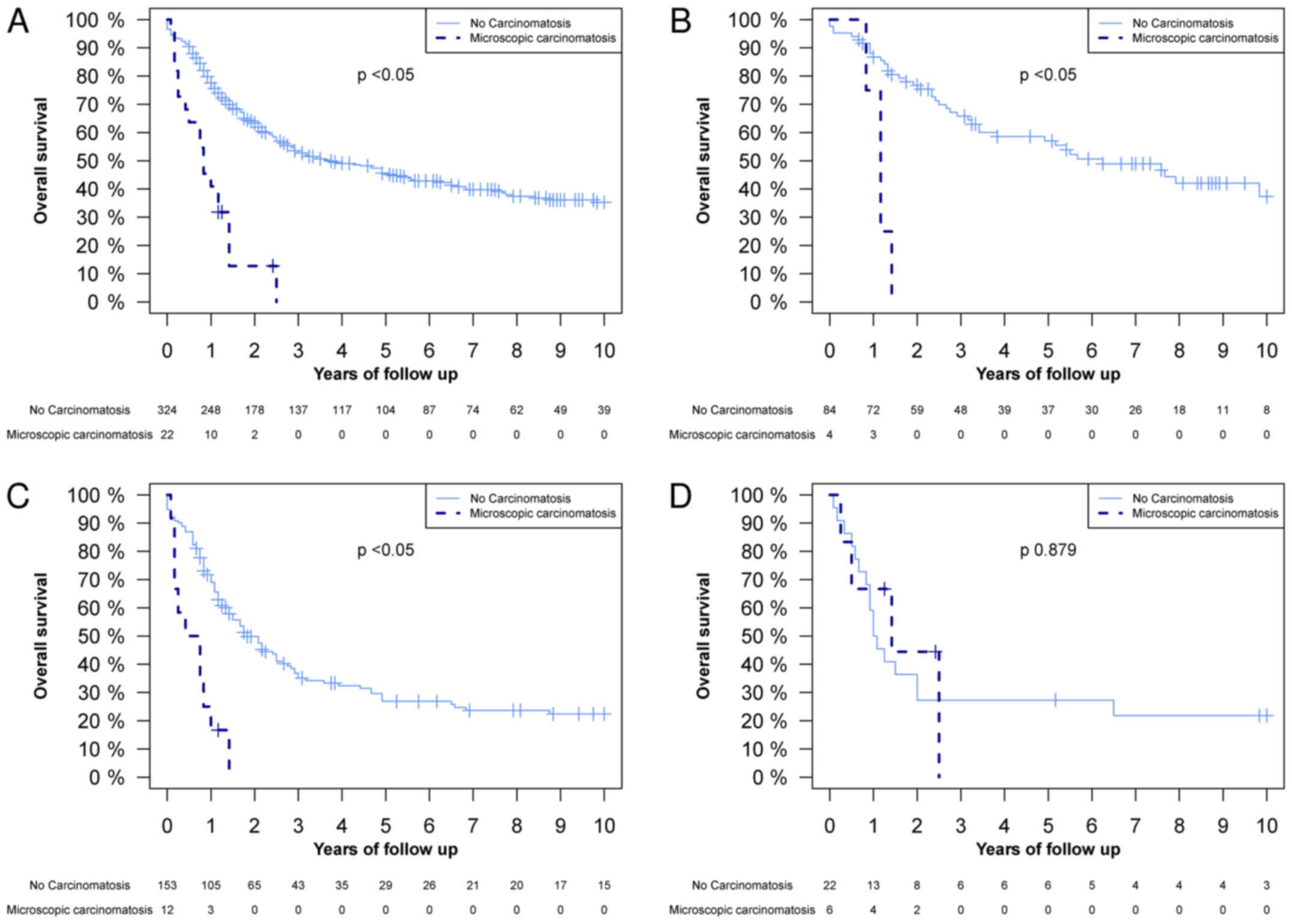
The differences in OS between patients with and
without microscopic PC were analysed. Fig. 1 demonstrates a significant difference
in the OS between the whole population, the T2 tumour extent group
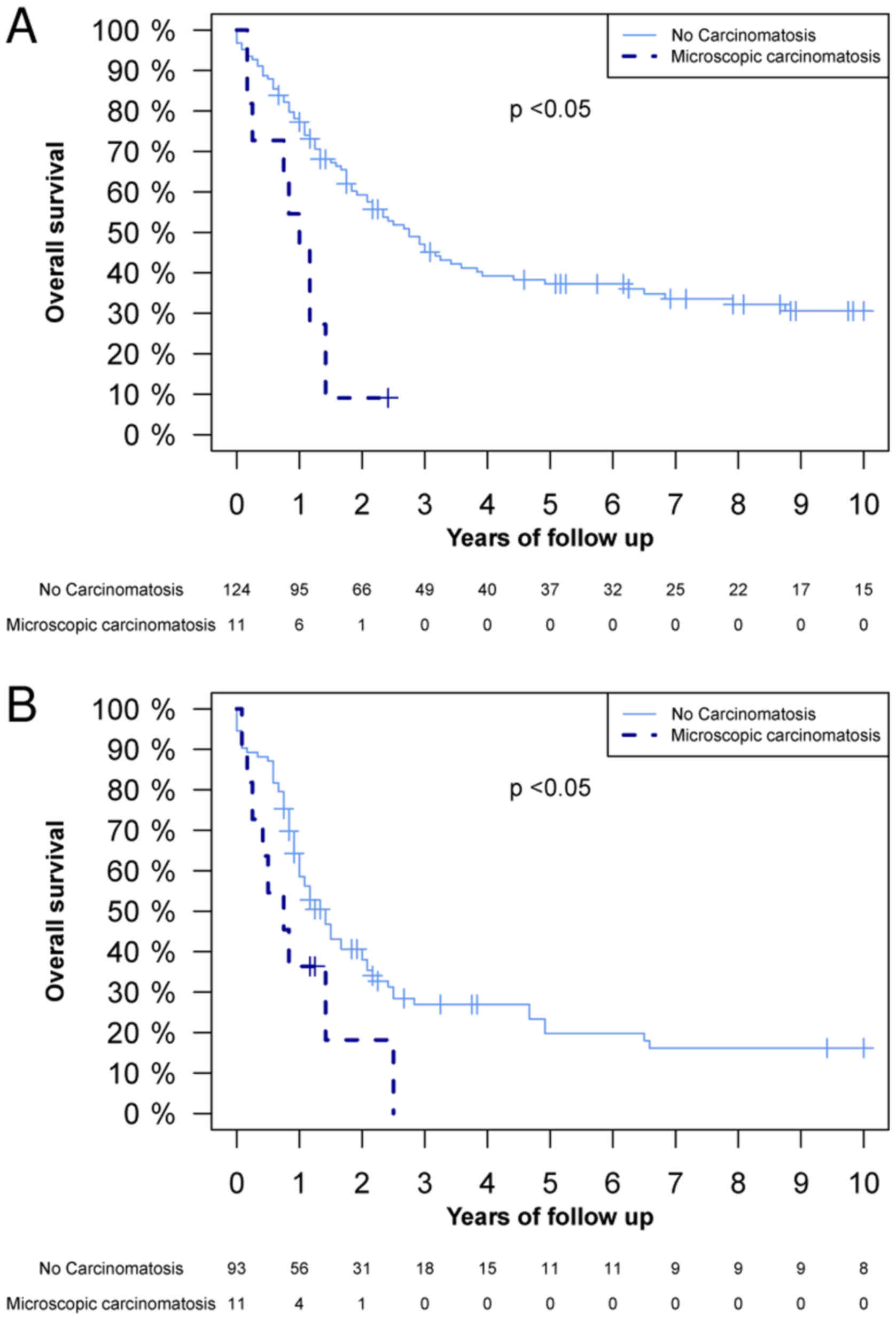
and the T3 tumour extent group. Fig.
2 illustrates that there was a significant difference in OS in
the TNM stage II and III groups between patients with and without
microscopic PC. The 1-year OS rate in patients without microscopic
PC was 77.5% (95% CI, 73.1–82.2), and in patients with microscopic
PC it was 40.1% (95% CI, 24.8–67.6%) (Fig. 1A). The 2-year OS rate was 63.3% (95%
CI, 58.1–68.9%) and 12.7% (95% CI, 3.7–43.8%) in patients without
and with microscopic PC, respectively (Fig. 1A). A Cox proportional hazard
regression model analysis was also performed, where microscopic PC
demonstrated a hazard ratio (HR) of 4.00 (95% CI, 2.45–6.53,
P<0.05; data not shown). Subsequent to adjustment for TNM stage,
cancer location, tumour grading, lymphatic and vascular invasion,
age, and neoadjuvant and adjuvant therapies in the multivariate
analyses, the HR was 2.02 (95% CI, 1.10–3.71, P<0.05; data not
shown).
Discussion
Among patients who received radical surgery for
gastric cancer, microscopic PC exhibited a prevalence of 5.5% in
the absence of any macroscopic PC. Additionally, microscopic PC
elicited a significant negative effect on OS, even in patients with
T2 gastric cancer. In the study population, the multivariate model
demonstrated that adenocarcinoma of a diffuse type, lymphatic and
vascular invasion, cancer location at the site of previous gastric
surgery and a tumour extent >T2 were the most predictive factors
for microscopic PC, with an AUC of the ROC curve of 88.7% (95% CI,
80.9–96.5). In particular, the presence of lymphatic and vascular
invasion was revealed to be the most significant and individual
predictive factor for microscopic PC.
The primary limitation of the present study was the
retrospective design and the limited number of patients affected by
microscopic PC. Other possible biases may be the limited
information concerning adjuvant and neoadjuvant treatment protocols
used for specific patients, and the incomplete information
concerning the timings of disease recurrence. Despite the limited
number of patients, significant differences in the OS rate between
patients who exhibited microscopic PC and those who did not were
observed, and this difference remained significant subsequent to
multivariate analyses and stratification for TNM stage and tumour
extent.
Other limitations may include the selection bias and
the limited amount of peritoneal tissue examined (greater and
lesser omenta and the transverse mesocolon). In particular, the
survival data may be affected by only taking into consideration
patients without macroscopic PC and those treated surgically with
curative intent. The analyses of the present study was intended to
assess whether or not there was a clinical basis for the
application of advanced loco-regional cancer treatments, including
HIPEC or early postoperative intraperitoneal chemotherapy, for
patients with an absence of macroscopic PC who were treated with
radical surgery with curative intent. Therefore, the aim of the
present study was to determine the role of microscopic PC not
identified by clinical examination at the time of surgery. The
present study included only patients who received standard surgical
treatment for gastric cancer, excluding cases affected by
macroscopic PC and those treated with peritonectomy and HIPEC, and
the location of excised peritoneum included only greater omenta,
lesser omenta and transverse mesocolon. In particular, the
prevalence of microscopic PC observed in the study population
(5.5%) was higher compared with that in a similar, previously
published study (2.7%) (13). Liu
et al (13) considered only
lesser omenta, greater omenta and transverse mesocolon locations,
however, they did not select their population and included patients
receiving palliative surgery in the prevalence denominator.
Therefore, it is expected that in the present study the prevalence
of microscopic PC would be higher compared with that presented by
Liu et al (13), as the
present study only included patients without evident PC at the time
of surgery. In this previous study (13) and the present study, there is a
potential underestimation of the real prevalence of microscopic PC
due to the limited peritoneal tissue examined. These prevalence
values of the previous study (13)
and the present study appear lower compared with those calculated
using positive peritoneal fluid cytology (14).
Among the patients treated with radical surgical
resection, the most frequent recurrence site of gastric cancer is
the peritoneum (15), which also
represents the most common site of metastasis in patients with
stage IV gastric cancer, and one of the leading causes of patient
mortality (16,17). In addition, the occasional
identification of isolated small peritoneal metastasis appears to
not be considered in the classification of PC in gastric cancer
(15). In a previously published
article about patients with microscopic PC, a shorter survival time
was demonstrated compared with patients without microscopic PC, but
a longer survival rate was identified compared with patients with
macroscopic PC (15). In accordance
with this study, the present study observed a significantly shorter
OS rate among patients affected by microscopic PC compared with
patients without microscopic PC.
A previous study described the use of peritoneal
fluid cytology as a prognostic factor for gastric cancer (18). The presence of intraperitoneal free
cancer cells appears to increase peritoneal recurrence risk, and to
predict poorer OS in patients affected by gastric cancer (18). However, the role that the presence or
the absence of intraperitoneal free cancer cells should have in the
management of gastric cancer remains unclear, as there is no
uniform way of interpreting the results of peritoneal fluid
cytology analyses (18). The presence
of intraperitoneal free cancer cells may be a sign of microscopic
PC that intra-operative examination and routine histology fail to
detect; however, this requires further investigation.
Knowing the high likelihood of the presence of
microscopic PC at the time of primary surgery for gastric cancer
through the identification of predictive factors or by novel rapid
diagnostic techniques will improve patient survival, through
enabling the selection of more aggressive treatments for these
patients, including HIPEC or emerging novel advanced loco-regional
treatment options like intraperitoneal immunotherapy (19). The present study revealed that
adenocarcinoma a diffuse type, lymphatic and vascular invasion,
cancer location at the site of a previous gastric surgery and a
tumour extent >T2 were significant predictive factors for the
presence of microscopic PC in a multivariate model.
In conclusion, the results of the present study
indicate that ≥5.5% of patients treated with surgery with a
curative intent may benefit from more aggressive loco-regional
treatment against microscopic PC at the time of primary surgery. In
particular, improvements to the efforts made in developing
techniques for identifying high-risk patients with microscopic PC
and to administer more aggressive and effective treatments for this
group are required.
Glossary
Abbreviations
Abbreviations:
|
AUC
|
area under the curve
|
|
CI
|
confidence interval
|
|
CRS
|
cytoreductive surgery
|
|
HIPEC
|
hyperthermic intraperitoneal
chemotherapy
|
|
HR
|
hazard ratio
|
|
IQR
|
inter-quartile range
|
|
LVI
|
lymphatic and vascular invasion
|
|
OS
|
overall survival
|
|
PC
|
peritoneal carcinomatosis
|
|
ROC
|
receiver operator characteristic
|
|
TNM
|
tumor-node-metastasis
|
References
|
1
|
Botterweck AA, Schouten LJ, Volovics A,
Dorant E and van Den Brandt PA: Trends in incidence of
adenocarcinoma of the oesophagus and gastric cardia in ten European
countries. Int J Epidemiol. 29:645–654. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Parkin DM, Bray F, Ferlay J and Pisani P:
Global cancer statistics, 2002. CA Cancer J Clin. 55:74–108. 2005.
View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Birri S, Bidoli E, Zucchetto A, Dal Maso
L, Zanier L and Serraino D: The tumors in friuli venezia giulia.
Data on incidence, survival and prevalence: Update to 2007.
Technical report, Regione Autonoma Friuli Venezia Giulia-Regional
Epidemiology Service. 2011
|
|
4
|
D'Angelica M, Gonen M, Brennan MF,
Turnbull AD, Bains M and Karpeh MS: Patterns of initial recurrence
in completely resected gastric adenocarcinoma. Ann Surg.
240:808–816. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Sadeghi B, Arvieux C, Glehen O, Beaujard
AC, Rivoire M, Baulieux J, Fontaumard E, Brachet A, Caillot JL,
Faure JL, et al: Peritoneal carcinomatosis from non-gynecologic
malignancies: Results of the EVOCAPE 1 multicentric prospective
study. Cancer. 88:358–363. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Yang XJ, Huang CQ, Suo T, Mei LJ, Yang GL,
Cheng FL, Zhou YF, Xiong B, Yonemura Y and Li Y: Cytoreductive
surgery and hyperthermic intraperitoneal chemotherapy improves
survival of patients with peritoneal carcinomatosis from gastric
cancer: Final results of a phase III randomized clinical trial. Ann
Surg Oncol. 18:1575–1581. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Pasqual EM, Bertozzi S, Bacchetti S,
Londero AP, Basso SM, Santeufemia DA, Lo Re G and Lumachi F:
Preoperative assessment of peritoneal carcinomatosis in patients
undergoing hyperthermic intraperitoneal chemotherapy following
cytoreductive surgery. Anticancer Res. 34:2363–2368.
2014.PubMed/NCBI
|
|
8
|
Pasqual E, Bertozzi S, Bacchetti S and
Londero A: Effective therapy in peritoneal neoplasia with low
peritoneal cancer index values: The difficulty of diagnosis. Int
Onkologie. 4:26–29. 2012.
|
|
9
|
Lauren P: The two histological main types
of gastric carcinoma: Diffuse and so-called intestinal-type
carcinoma. An attempt at a histo-clinical classification. Acta
Pathol Microbiol Scand. 64:31–49. 1965. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Bosman FT, Carneiro F, Hruban RH and
Theise ND: World Health Organization Classification of Tumours of
the Digestive System. 3. 4th. IARC Press; Lyon: 2010
|
|
11
|
Japanese Gastric Cancer Association, .
Japanese classification of gastric carcinoma- 2nd english edition.
Gastric Cancer. 1:10–24. 1998. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
National Comprehensive Cancer Network, .
Gastric Cancer (Version 1.2014). http://www.nccn.org/professionals/physician_gls/pdf/gastric.pdfAugust
29–2014
|
|
13
|
Liu X, Cai H, Sheng W and Wang Y:
Long-term results and prognostic factors of gastric cancer patients
with microscopic peritoneal carcinomatosis. PLoS One. 7:e372842012.
View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Oh CA, Bae JM, Oh SJ, Choi MG, Noh JH,
Sohn TS and Kim S: Long-term results and prognostic factors of
gastric cancer patients with only positive peritoneal lavage
cytology. J Surg Oncol. 105:393–399. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Li JH, Zhang SW, Liu J, Shao MZ and Chen
L: Review of clinical investigation on recurrence of gastric cancer
following curative resection. Chin Med J (Engl). 125:1479–1495.
2012.PubMed/NCBI
|
|
16
|
Saito H, Tsujitani S, Kondo A, Ikeguchi M,
Maeta M and Kaibara N: Expression of vascular endothelial growth
factor correlates with hematogenous recurrence in gastric
carcinoma. Surgery. 125:195–201. 1999. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Sarela AI, Miner TJ, Karpeh MS, Coit DG,
Jaques DP and Brennan MF: Clinical outcomes with laparoscopic stage
M1, unresected gastric adenocarcinoma. Ann Surg. 243:189–195. 2006.
View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Leake PA, Cardoso R, Seevaratnam R,
Lourenco L, Helyer L, Mahar A, Rowsell C and Coburn NG: A
systematic review of the accuracy and utility of peritoneal
cytology in patients with gastric cancer. Gastric Cancer. 1 Suppl
15:S27–S37. 2012. View Article : Google Scholar
|
|
19
|
Goéré D, Gras-Chaput N, Aupérin A, Flament
C, Mariette C, Glehen O, Zitvogel L and Elias D: Treatment of
gastric peritoneal carcinomatosis by combining complete surgical
resection of lesions and intraperitoneal immunotherapy using
catumaxomab. BMC Cancer. 14:1482014. View Article : Google Scholar : PubMed/NCBI
|