Introduction
Triple-negative breast cancer (TNBC) is
characterized by the absence of estrogen, progesterone and human
epidermal growth factor receptor 2 (HER2) receptors. TNBC makes up
between 15 and 20% of all types of breast cancer, are aggressive,
and are associated with poorer survival rates compared with
non-TNBC (1,2). Although patients with TNBC respond to
chemotherapy, they are more likely to suffer early relapse than
patients with other breast cancer subtypes (3). Therefore, there is a requirement to
identify prognostic and predictive markers in TNBC.
Cluster of differentiation 117 (CD117; encoded by
KIT) regulates cellular differentiation, proliferation,
adhesion and apoptosis (4). CD117 is
involved in the development of several malignant tumor types
including gastrointestinal stromal cell tumors, small-cell lung,
ovarian and breast cancer (4–7). Immunohistochemical staining has revealed
that CD117 protein is overexpressed in primary malignant tumors,
including operable esophageal squamous cell carcinoma and vulvar
melanoma, and may be a valuable prognostic marker in esophageal
squamous cell carcinoma (8). However,
the results of studies concerning the prognostic significance of
CD117 in patients with breast cancer or TNBC are conflicting:
Kashiwagi et al have suggested that CD117 protein is
associated with poor prognosis (9),
whereas others identified no significant association between CD117
and prognosis in breast cancer or TNBC (10,11).
The tumor protein P53 (TP53) gene encodes the
tumor suppressor protein p53, and is activated by various stresses
including genotoxic damage, hypoxia and heat shock (12,13).
TP53 mutations are most often located at exons 5–8,
inhibiting the tumor suppressor activity of p53 (14). The association between TP53
mutations, p53 expression and the prognosis of patients with breast
cancer or TNBC is inconsistent (15–17); a
group of patients with TP53 missense mutations experienced
the shortest survival and a reduction in relapse-free survival
rates (15,16); however, there was no association
between TP53 mutations and clinical outcome in another study
(17).
A previous study revealed that mutations to
TP53 upregulated CD117 expression in colon cancer cells and
promoted the invasion of tumor cells (18). TP53 mutations have been
demonstrated to inactivate the microRNA miR-34, and to promote
CD117 expression in human colorectal cancer cells (18); however, there are no reports regarding
the association between TP53 mutations and CD117 expression
in TNBC.
In the present study, it was hypothesized that CD117
expression was associated with TP53 mutations in patients
with TNBC. The expression levels of CD117 and p53 were measured and
TP53 mutations were assessed in 58 TNBC tumor specimens and
48 control specimens, and their association with the
clinicopathological characteristics of patients with TNBC was
analyzed.
Materials and methods
Patients
The Ethics Committee for Human Studies at Shanghai
Jiao Tong University (Shanghai, China) approved the present study,
which was conducted in accordance with The Declaration of Helsinki.
Participants were fully informed of the procedures, and written
informed consent was obtained from each.
Between January 2008 and August 2012 at Shanghai
Jiao Tong University Affiliated Sixth People's Hospital, 58 TNBC
tissues and 48 non-TNBC samples were collected during surgery. All
patients were women, with a mean age of 55.30±9.95 years (range,
32–80 years). Patients with non-TNBC had a mean age of 55.27±8.75
years (range, 43–77 years); patients with TNBC had a mean age of
55.33±10.92 (range, 32–80 years). Stages of breast cancer were
determined using Nottingham staging, recommended by the American
Joint Committee on Cancer (19). A
total of 39 specimens (20 TNBC and 19 non-TNBC cases) were
determined to be stage I, and 67 specimens (38 TNBC and 29 non-TNBC
cases) as stage II–III. All patients received modified radical
mastectomy without preoperative chemotherapy or radiotherapy.
Following surgery, routine neoadjuvant chemotherapy was
administered.
The end of follow-up was June 2014. The 5-year
survival rate for the entire cohort of 106 patients was 49%. The
recurrence rate was 35.8%. During the follow-up period, recurrence
occurred in 38 cases (30 patients succumbed to metastasis, and 8
patients succumbed whilst receiving chemotherapy). The median
follow-up period was 50.6 months. The overall survival time of
patients was calculated from the date of surgery to the date of
mortality or the date of last contact.
Immunohistochemistry
Immunohistochemistry was performed on 4-µm-thick
sections from 10% formalin-fixed paraffin-embedded (FFPE) tissue
specimens as previously described (20). Sections were deparaffinized with 100%
xylene (25°C) and rehydrated through a graded ethanol series (100,
95 and 70% ethanol) and were subjected to microwave antigen
retrieval by incubating sections at 98 to 100°C in 0.01 M citrate
buffer (pH 6.0) for 15 min. Antibodies targeting D2-40 (cat. no.
sc-59347; 1:100) were purchased from Santa Clara Biotechnology,
Inc. (Dallas, TX, USA). Other antibodies were purchased from Dako
(Agilent Technologies, Inc.), directed against the following:
Estrogen receptor (ER; cat. no. IS657; 1:80), progesterone receptor
(PR; cat. no. IS068; 1:50), human epidermal growth factor receptor
2 (HER2; cat. no. 20027850; 1:200), CD117 (cat. no. 10109679;
1:200), CD34 (cat. no. GA632; 1:50), marker of proliferation Ki-67
(MKI67; cat. no. IR626; 1:200), and p53 (cat. no. IS616; 1:100),
which reacts with an epitope between amino acids 19–26 and
recognizes wild-type and mutant p53 protein. The sections were
incubated with the primary antibodies for 1 h at 25°C, followed by
an incubation for 30 min at 37°C with a horseradish
peroxidase-conjugated secondary antibody [Dako EnVision+ System-HRP
(DAB); Dako, Agilent Technologies, Inc.]. The slides were assessed
in an auto immunostainer Link 48 (Agilent Technologies, Inc.; Dako)
according to the manufacturer's protocols. Slides were
counterstained with Mayer's hematoxylin. H&E staining of other
slides from the same samples was also performed in order to assess
the presence/absence of vascular invasion of tumors. Slides were
stained with hematoxylin (Harris Formula, Surgipath Medical
Industries, Inc., Richmond, IL, USA) at 25°C for 1 min, rinsed in
running distilled water (10 min), and then stained with an eosin
solution (Surgipath Medical Industries, Inc.) for 1 min and washed
with distilled water again, dehydrated with 100% ethanol (25°C) and
mounted.
All the results of immunohistohchemistry were
blindly accessed by 2 independent pathologists with long-standing
experience in the Department of Pathology, Shanghai Jiao Tong
University Affiliated Sixth People's Hospital. Nuclear staining
>10% in tumor cells was considered to indicate p53- or
MKI67-positivity. Nuclear staining in >1% of tumor cell nuclei
was considered a positive indication of the presence of ER and PR.
Immunostaining for HER2 and CD117 (11,21) was
graded according to the percentage of cells: 0, none; 1+, <10%
staining weak and incomplete; 2+, ≥10%, staining weak to moderate;
and 3+, ≥10% strong staining. HER2 immunostaining was considered
positive if graded 3+, or if gene amplification was confirmed by
fluorescence in situ hybridization (FISH) in patients
exhibiting 2+ immunostaining. Breast cancer samples with ≥10%
positive cells and with scores ≥2 were considered to indicate CD117
positivity. Vascular invasion was identified by staining for CD34
(endothelial cell marker) or D2-40 (podoplanin, a membrane protein
specific for lymphatic endothelium), in accordance with a previous
study (22).
FISH
HER2 status was detected using FISH. A
PathVysion dual-color fluorescence probes kit (HER2/CEP17)
was purchased from Vysis, Inc. (Abbott Pharmaceutical Co. Ltd.,
Lake Bluff, IL, USA). The assay was performed according to the
manufacturer's protocol. All samples were analyzed using an Olympus
BX51 fluorescence microscope (Olympus Corporation, Tokyo, Japan,
original magnification, ×1,000) equipped with a set of the
appropriate filters (Vysis Inc.; Abbott Pharmaceutical Co. Ltd.).
The hybridization results were evaluated by 2 independent
pathologists in the Department of Pathology, Shanghai Jiao Tong
University Affiliated Sixth People's Hospital, blinded to the
clinical outcomes. Categories of FISH were classified as previously
described (23).
TP53 mutation analysis
For each case, 10 5-µm-thick slices were collected
in a 1.5 ml tube, these FFPE specimen tissue sections were first
deparaffinized with 100% xylene at 25°C and 100% ethanol at 25°C.
Subsequently, DNA was extracted from FFPE tissue specimens using a
QIAamp DNA extraction kit (Qiagen GmbH, Hilden, Germany) according
to the manufacturer's protocol. The samples were incubated in 20 µl
proteinase K solution at 56°C for 1 h, and then incubated in FTB
buffer at 90°C for 1 h, then wash buffers (500 µl AW1 and 500 µl
AW2) washing for 1 min at 25°C. Finally, the DNA was eluted in DTE
buffer (all Qiagen GmbH).
Mutations in the TP53 gene were identified
via direct sequencing. Polymerase chain reaction (PCR)
amplification and direct sequencing of the TP53 gene (exon
4–8) were performed in 106 breast cancer samples. The primers were
designed to amplify exons 4–8 of TP53 (Table I). PCR was performed using a
Mastercycler gradient PCR machine (Eppendorf, Hamburg, Germany)
under the following amplification conditions: 94°C for 10 min; 40
cycles of 94°C for 45 sec, 61°C for 45 sec, and 72°C for 45 sec;
with a final extension at 72°C for 7 min. The PCR products were
purified using a QIAquick Gel Extraction kit (Qiagen GmbH) and were
prepared for sequencing via a 3500Dx genetic analyzer (Applied
Biosystems; Thermo Fisher Scientific, Inc., Waltham, MA, USA) with
a BigDye Terminator Cycle Sequencing Ready Reaction kit (Applied
Biosystems; Thermo Fisher Scientific, Inc.). The cycling conditions
were: 94°C for 1 min; 24 cycles of 94°C for 10 sec, 50°C for 5 sec,
and 60°C for 1 min; and final extension at 72°C for 5 min. The
sequences were analyzed using Chromas Lite software version 2.01
(Technelysium Pty Ltd., South Brisbane, Australia).
 | Table I.Polymerase chain reaction primers for
the tumor protein P53 gene. |
Table I.
Polymerase chain reaction primers for
the tumor protein P53 gene.
| Exon | Forward, 5′-3′ | Reverse, 5′-3′ |
|---|
| 4I |
GCTCTTTTCACCCATCTACAG |
GAAGGGACAGAAGATGACAG |
| 4II |
CTGCACCAGCAGCTCCTA |
GAAGTCTCATGGAAGCCAG |
| 5 |
TCACTTGTGCCCTGACTTTCA |
TCTCCAGCCCCAGCTGCT |
| 6 |
TTCCTCACTGATTGCTCTTAG |
GACCCCAGTTGCAAACCAG |
| 7 |
GCGCACTGGCCTCATCTTG |
CACAGCAGGCCAGTGTGCA |
| 8 |
AGGACCTGATTTCCTTACTGC |
GAATCTGAGGCATAACTGCAC |
Statistical analysis
The significance of association between TNBC and the
various clinical factors or potential prognostic markers was
determined using the χ2 test. Survival analysis was
performed using a Kaplan-Meier plot analysis and a log-rank test.
Hazard ratios with 95% confidence intervals were calculated using
the Cox proportional hazards model, which was used to compute
univariate and multivariate hazard ratios for the study parameters.
P<0.05 was considered to indicate a statistically significant
difference. Statistical analyses were performed using SPSS software
(version 13.0; SPSS, Inc., Chicago, IL, USA).
Results
Clinical characteristics of TNBC
patients
A total of 58 patients with TNBC and 48 patients
with non-TNBC were included in the study. Positive stains of ER,
PR, and MKI67 were primarily located in the nuclei (Fig. 1A-C). Immunohistochemistry revealed
that HER2 protein was located at the cell membrane, and gene
amplification of HER2 was detected using FISH analysis
(Fig. 1D and E). Vascular invasion
was assessed by hematoxylin and eosin staining (Fig. 1F) and by immunohistochemistry using
anti-CD34 (recognizing endothelial cells) and anti-D2-40
(recognizing lymphatic endothelial cells) antibodies (Fig. 1G and H). Compared with patients with
non-TNBC, those with TNBC had a higher rate of vascular invasion
(P=0.043), lymph node metastasis (P=0.017) and tumor recurrence
(P=0.012; Table II), and a higher
proliferation index (MKI67; P=0.025; Table III).
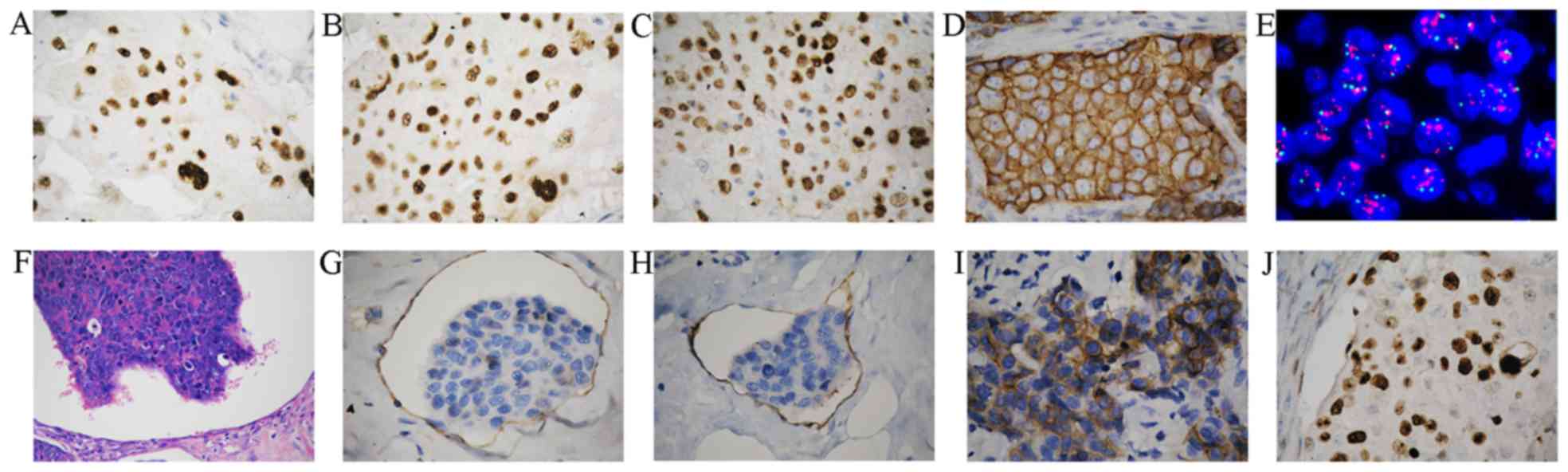 | Figure 1.Immunohistochemical analysis of
breast cancer tissues. Examples of positive immunohistochemical
staining for the (A) estrogen receptor, (B) progesterone receptor,
(C) MKI67, and (D) HER2 in tumor cells (original magnification,
×400). (E) Representative image of HER2 gene amplification
in tumor tissue was observed using FISH in non-TNBC tumor cells
(original magnification, ×1,000). (F) Tumor thrombus was observed
in vessels (original magnification, ×200). (G) Blood vessel
invasion was indicated by CD34 staining (original magnification,
×400). (H) Lymphatic invasion indicated by D2-40 staining (original
magnification, ×400). Representative examples of (I) positive CD117
protein staining (J) nuclear localization of p53 and were observed
in breast cancer (original magnification, ×400). HER2, human
epidermal growth factor receptor 2; CD, cluster of differentiation;
FISH, fluorescence in situ hybridization; TNBC, triple
negative breast cancer; MKI67, marker of proliferation Ki-67. |
| Table II.Summary of clinical and pathological
features of 106 patients with breast cancer. |
Table II.
Summary of clinical and pathological
features of 106 patients with breast cancer.
| Variable | Non-TNBC, n
(%) | TNBC, n (%) | Total, n (%) | P-value |
|---|
| Subjects | 48 | 58 | 106 |
|
| Age at operation,
years |
|
|
| 0.245 |
|
≤50 | 21 (43.8) | 19 (32.8) | 40 (37.7) |
|
|
>50 | 27 (56.3) | 39 (67.2) | 66 (62.3) |
|
| Tumor grade |
|
|
| 0.588 |
| I | 19 (39.6) | 20 (34.5) | 39 (36.8) |
|
|
II/III | 29 (60.4) | 38 (65.5) | 67 (63.2) |
|
| Tumor, cm |
|
|
| 0.302 |
| ≤2 | 28 (58.3) | 28 (48.3) | 56 (52.8) |
|
|
>2 | 20 (41.7) | 30 (51.7) | 50 (47.2) |
|
| Lymph node
status |
|
|
| 0.017 |
|
Negative | 31 (64.6) | 24 (41.4) | 55 (51.9) |
|
|
Positive | 17 (35.4) | 34 (58.6) | 51 (48.1) |
|
| Vascular
invasion |
|
|
| 0.043 |
| No | 43 (89.6) | 43 (74.1) | 85 (80.2) |
|
|
Yes | 5 (10.4) | 15 (25.9) | 21 (19.8) |
|
| Nerve invasion |
|
|
| 0.726 |
| No | 37 (77.1) | 43 (74.1) | 80 (75.5) |
|
|
Yes | 11 (22.9) | 15 (25.9) | 26 (24.5) |
|
| Recurrence |
|
|
| 0.012 |
| No | 37 (77.1) | 31 (53.4) | 68 (64.2) |
|
|
Yes | 11 (22.9) | 27 (46.6) | 38 (35.8) |
|
| Table III.TP53 and CD117 expression in
patients with breast cancer. |
Table III.
TP53 and CD117 expression in
patients with breast cancer.
| Variable | Non-TNBC, n
(%) | TNBC, n (%) | P-value |
|---|
| CD117 |
|
| 0.045a |
|
Negative | 34 (70.8) | 30 (51.7) |
|
|
Positive | 14 (29.2) | 28 (48.3) |
|
|
CD117/TP53MIS |
|
| 0.009a |
|
Negative | 42 (87.5) | 38 (65.5) |
|
|
Positive | 6 (12.5) | 20 (34.5) |
|
| TP53
MIS |
|
| 0.027a |
|
Negative | 31 (64.6) | 25 (43.1) |
|
|
Positive | 17 (35.4) | 33 (56.9) |
|
| MKI67 |
|
| 0.025a |
|
Negative | 27 (56.3) | 20 (34.5) |
|
|
Positive | 21 (43.8) | 38 (65.5) |
|
| p53 |
|
| 0.530 |
|
Negative | 31 (64.6) | 34 (58.6) |
|
|
Positive | 17 (35.4) | 24 (41.4) |
|
| TP53
mutation |
|
| 0.055 |
|
Negative | 16 (33.3) | 10 (17.2) |
|
|
Positive | 32 (66.7) | 48 (82.8) |
|
| Codon 72 |
|
| 0.530 |
|
Negative | 31 (64.6) | 34 (58.6) |
|
|
Positive | 17 (35.4) | 24 (41.4) |
|
Expression of CD117 is increased in
TNBC patients
CD117 expression was identified in 28/58 of TNBC
samples (48.3%), and in 14/48 of non-TNBC samples (29.2%). Positive
staining for CD117 was observed in the cytoplasm or at the cell
membrane (Fig. 1I). The TNBC tissues
exhibited a higher rate of positive staining for CD117 compared
with non-TNBC tissues (P=0.045; Table
III). The presence of p53 protein, localized in the nuclei
(Fig. 1J), was similar in TNBC and
non-TNBC patients (P=0.530; Table
III). Furthermore, in TNBC, positive expression of CD117 was
associated with vascular invasion (P=0.024), proliferation index
(P=0.01) and tumor recurrence (P=0.001; Table IV). No association was identified
between CD117 expression and tumor size, tumor grade, nerve
invasion, lymph node metastasis, p53 protein or TP53
mutation in TNBC (Table IV).
| Table IV.Association of CD117 with
clinicopathological features of 58 patients with TNBC. |
Table IV.
Association of CD117 with
clinicopathological features of 58 patients with TNBC.
|
| CD117 |
|
|---|
|
|
|
|
|---|
| Variable | Negative, n
(%) | Positive, n
(%) | P-value |
|---|
| p53 |
|
| 0.825 |
|
Negative | 18 (60.0) | 16 (57.1) |
|
|
Positive | 12 (40.0) | 12 (42.9) |
|
| TP53
MIS |
|
| 0.031 |
|
Negative | 17 (56.7) | 8 (28.6) |
|
|
Positive | 13 (43.3) | 20 (48.3) |
|
| TP53
mutation |
|
| 0.380 |
|
Negative | 7 (23.3) | 4 (14.3) |
|
|
Positive | 23 (76.7) | 24 (85.7) |
|
| Codon 72 |
|
| 0.754 |
|
Negative | 17 (56.7) | 17 (60.7) |
|
|
Positive | 13 (43.3) | 11 (39.3) |
|
| MKI67 |
|
| 0.010 |
|
Negative | 15 (50.0) | 5 (17.9) |
|
|
Positive | 15 (50.0) | 23 (82.1) |
|
| Age, years |
|
| 0.512 |
|
≤50 | 11 (36.7) | 8 (28.6) |
|
|
>50 | 19 (63.3) | 20 (71.4) |
|
| Tumor grade |
|
| 0.849 |
| I | 10 (33.3) | 10 (35.7) |
|
| II and
III | 20 (66.7) | 18 (64.3) |
|
| Tumor, cm |
|
| 0.786 |
| ≤2 | 15 (50.0) | 13 (46.4) |
|
|
>2 | 15 (50.0) | 15 (53.6) |
|
| Lymph node
status |
|
| 0.451 |
|
Negative | 11 (36.7) | 13 (46.4) |
|
|
Positive | 19 (63.3) | 15 (53.6) |
|
| Vascular
invasion |
|
| 0.024 |
| No | 26 (86.7) | 17 (60.7) |
|
|
Yes | 4 (13.3) | 11 (39.9) |
|
| Recurrence |
|
| 0.001 |
| No | 23 (76.7) | 9 (32.1) |
|
|
Yes | 7 (23.3) | 19 (67.9) |
|
| Nerve invasion |
|
| 0.649 |
| No | 23 (76.7) | 20 (71.4) |
|
|
Yes | 7 (23.3) | 8 (28.6) |
|
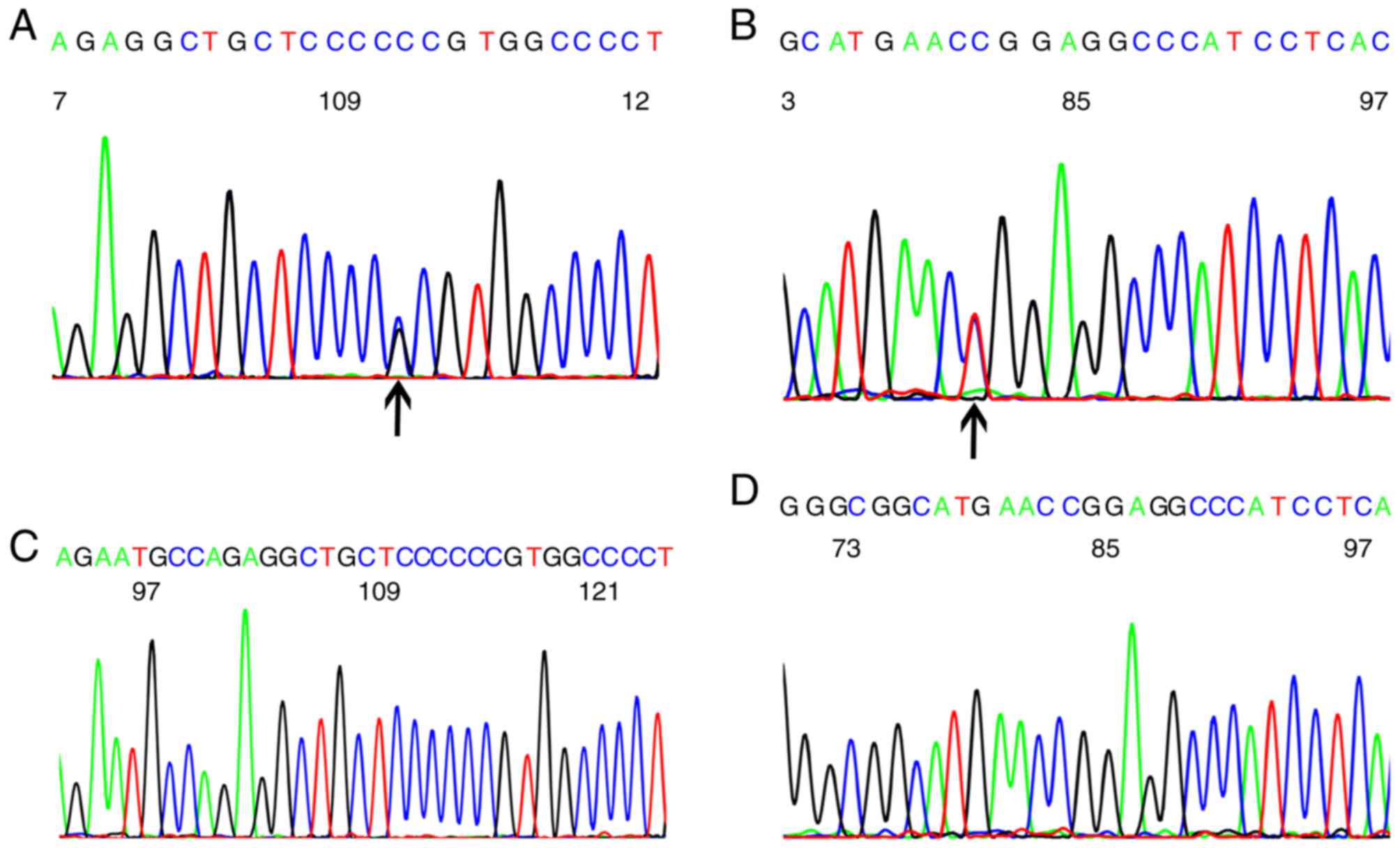
TP53 missense mutations occur at a
high frequency in TNBC
Missense mutations were the most common type of
TP53 mutations (40/106, 37.7%) in breast cancer. Frame-shift
mutations were identified in 7 patients (6.6%), nonsense mutations
were observed in 6 patients (5.67%) and silent mutations in 3
(1.89%). A polymorphism of codon 72 in exon 4 was present in 38.68%
(41/106) of patients. A codon 72 polymorphism (CCG to CCC) in exon
4 (Fig. 2A), and codon 248 mutations
(CGG to TGG) in exon 7 (Fig. 2B) were
the most common mutations. Wild-type codons 72, 61.3% (65/106) of
breast cancer patients, and codon 248, 82.1% (87/106) of breast
cancer patients were observed (Fig. 2C
and D).
TP53 missense mutations in exons 4–8 were all
functional mutations, with the exception of codon 72 mutations. The
rate of missense mutations in TNBC tissues (33/58, 56.9%) was
significantly higher than in non-TNBC tissues (17/48, 35.4%;
P=0.027); however, rates of total TP53 mutations (82.8 vs.
66.7%, respectively) and polymorphisms at codon 72 (41.4 vs. 35.4%,
respectively) were similar in TNBC vs. non-TNBC groups (Table III). The presence of p53 protein was
similar in the TNBC and non-TNBC patients (P=0.530; Table III). No association was identified
between TP53 mutations and the positive expression of p53
protein (Table V). TP53
mutations (P=0.001) were associated with tumor recurrence, whereas
expression of p53 protein was not associated with tumor recurrence
(Table V). TP53 missense
mutations were associated with tumor recurrence (P=0.006), but not
tumor grade, size, vascular invasion or lymph node metastasis
(Table V).
| Table V.Association between
clinicopathological features and TP53 missense
mutations. |
Table V.
Association between
clinicopathological features and TP53 missense
mutations.
|
| TP53
missense mutations |
|
|---|
|
|
|
|
|---|
| Variable | Negative | Positive | P-value |
|---|
| MKI67 |
|
| 0.442 |
|
Negative | 10 (40.0) | 10 (30.3) |
|
|
Positive | 15 (60.0) | 23 (69.7) |
|
| p53 |
|
| 0.853 |
|
Negative | 15 (60.0) | 19 (57.6) |
|
|
Positive | 10 (40.0) | 14 (42.4) |
|
| Age, years |
|
| 0.502 |
|
≤50 | 7 (28.0) | 12 (36.4) |
|
|
>50 | 18 (72.0) | 21 (63.6) |
|
| Tumor grade |
|
| 0.059 |
| I | 12 (48.0) | 8 (24.2) |
|
| II and
III | 13 (52.0) | 25 (75.8) |
|
| Tumor, cm |
|
| 0.971 |
| ≤2 | 12 (48.0) | 16 (48.5) |
|
|
>2 | 13 (52.0) | 17 (51.5) |
|
| Lymph node
status |
|
| 0. 853 |
|
Negative | 10 (40.0) | 14 (42.4) |
|
|
Positive | 15 (60.0) | 19 (57.6) |
|
| Vascular
invasion |
|
| 0.135 |
| No | 21 (84.0) | 22 (66.7) |
|
|
Yes | 4 (16.0) | 11 (33.3) |
|
| Recurrence |
|
| 0.006 |
| No | 19 (76.0) | 13 (39.4) |
|
|
Yes | 6 (24.0) | 20 (60.6) |
|
| Nerve invasion |
|
| 0.746 |
| No | 18 (72.0) | 25 (75.8) |
|
|
Yes | 7 (28.0) | 8 (24.2) |
|
Expression of CD117 is associated with
TP53 missense mutations in TNBC
The TNBC tissues exhibit a higher rate of CD117
positive/TP53 missense mutations (20/58, 34.5%) than
non-TNBC tissues (6/48, 12.5%; P=0.009; Table III). The presence of CD117 was
associated with TP53 missense mutations (P=0.031) in TNBC
(Table IV). The CD117
positive/TP53 missense mutations were associated with
vascular invasion (P=0.016), proliferation index (P=0.004) and
particularly tumor recurrence (P<0.001). There was no
association identified between CD117 positive/TP53 missense
mutations and age, grade, tumor size, node status and nerve
invasion (Table VI).
| Table VI.Association of
CD117+/TP53 missense mutation+ with
clinicopathological features of 58 patients with TNBC. |
Table VI.
Association of
CD117+/TP53 missense mutation+ with
clinicopathological features of 58 patients with TNBC.
|
| CD117/TP53
missense |
|
|---|
|
|
|
|
|---|
| Variable | Negative | Positive | P-value |
|---|
| MKI67 |
|
| 0.004 |
|
Negative | 18 (47.4) | 2 (10.0) |
|
|
Positive | 20 (52.6) | 18 (90.0) |
|
| Age, years |
|
| 0.792 |
|
≤50 | 12 (31.6) | 7 (35.0) |
|
|
>50 | 26 (68.4) | 13 (65.0) |
|
| Tumor grade |
|
| 0.270 |
| I | 15 (39.5) | 5 (25.0) |
|
| II and
III | 23 (60.5) | 15 (75.0) |
|
| Size, cm |
|
| 0.360 |
| ≤2 | 20 (52.6) | 8 (40.0) |
|
|
>2 | 18 (47.4) | 12 (60.0) |
|
| Lymph node
status |
|
| 0.877 |
|
Negative | 16 (42.1) | 8 (40.0) |
|
|
Positive | 22 (57.9) | 12 (60.0) |
|
| Vascular
invasion |
|
| 0.016 |
| No | 32 (84.2) | 11 (55.0) |
|
|
Yes | 6 (15.8) | 9 (45.0) |
|
| Recurrence |
|
| <0.001 |
| No | 28 (73.7) | 4 (20.0) |
|
|
Yes | 10 (26.3) | 16 (80.0) |
|
| Nerve invasion |
|
| 0.913 |
| No | 28 (73.7) | 15 (75.0) |
|
|
Yes | 10 (26.3) | 5 (25.0) |
|
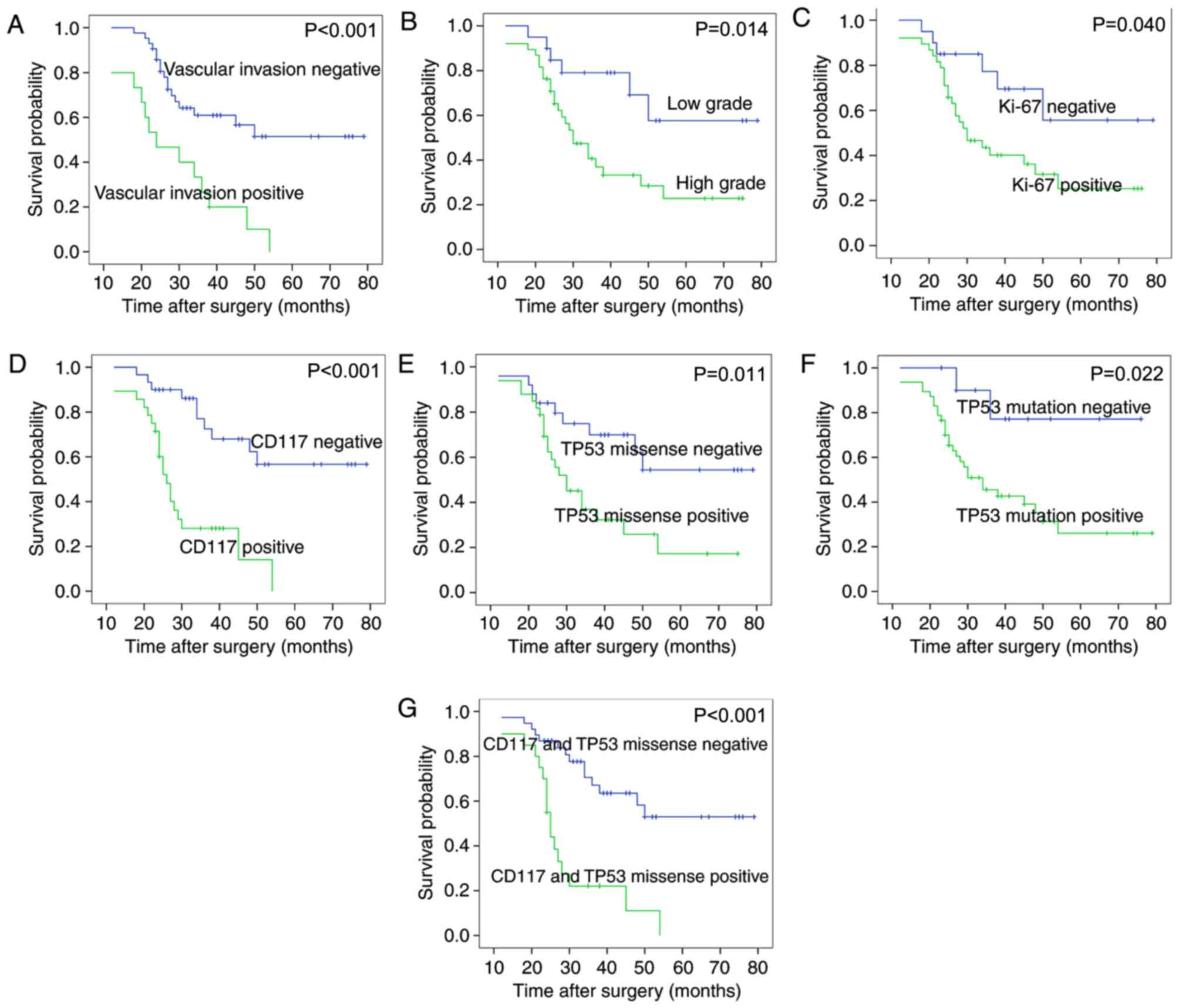
CD117+/TP53 missense
mutation+ and vascular invasion are independent
prognostic factors in TNBC
Survival analysis of the 58 patients with TNBC
revealed that tumor grade, vascular invasion, expression of CD117
and MKI67 protein, TP53 missense mutations, TP53
mutations or the CD117+/TP53 missense
mutation+ (CD117 and TP53 missense mutations together),
were associated with overall survival (Fig. 3 and Table
VII). The following features were not associated with the
overall survival rate of patients with TNBC: Age, tumor size, lymph
node status, nerve invasion, codon 72 mutations or expression of
p53 protein. The Cox proportional hazards model revealed that
CD117+/TP53 missense mutation+
[positive vs. negative group, P=0.004, RR=3.153; 95% confidence
interval (CI), 1.430–6.952] and vascular invasion (present vs. not
present, P=0.043, RR=2.234; 95% CI, 1.026–4.863) were independent
prognostic factors in patients with TNBC (Fig. 3; Table
VII).
| Table VII.Univariate and multivariate survival
analysis of 58 patients with TNBC. |
Table VII.
Univariate and multivariate survival
analysis of 58 patients with TNBC.
|
| P-value |
|
|
|---|
|
|
|
|
|
|---|
| Variable | Univariate | Multivariate | RR | 95% CI |
|---|
| Age, years (≤50 vs.
>50) | 0.738 |
|
|
|
| Tumor size, cm (≤2
vs. >2) | 0.389 |
|
|
|
| Lymph node status
(+ vs. −) | 0.601 |
|
|
|
| Histological grade
(high vs. low) | 0.014 |
|
|
|
| Vascular invasion
(yes vs. no) |
<0.001a | 0.043a | 2.234 | 1.026–4.863 |
| Nerve invasion (yes
vs. no) | 0.898 |
|
|
|
| CD117 (+ vs.
−) | <0.001 |
|
|
|
| MKI67 (+ vs.
−) | 0.040 |
|
|
|
| P53 (+ vs. −) | 0.651 |
|
|
|
| TP53 MIS (+
vs. −) | 0.011 |
|
|
|
| TP53
mutation (+ vs. −) | 0.022 |
|
|
|
| Codon 72 (+ vs.
−) | 0.837 |
|
|
|
| CD117/TP53MIS (+
vs. −) |
<0.001a | 0.004a | 3.153 | 1.430–6.952 |
Discussion
In the present study, patients with TNBC had a
higher rate of CD117 expression, TP53 missense mutations and
CD117+/TP53 missense mutation+ than
patients with non-TNBC. CD117, TP53 missense mutations and
CD117+/TP53 missense mutation+ were
associated with poor prognosis and tumor recurrence in patients
with TNBC. It was confirmed that CD117+/TP53
missense mutation+ was an independent prognostic factor
in patients with TNBC. CD117+/TP53 missense
mutation+ was associated with positive expression of
MKI67 and vascular invasion. It was identified that tumor grade and
the proliferation index (as indicated by MKI67 levels) were poor
prognostic factors, associated with a high risk of relapse in
patients with TNBC, consistent with previous reports (24–26).
Vascular invasion, an independent prognostic factor, was associated
with tumor recurrence in patients with TNBC in the present study.
The data generated in the present study were consistent with that
of a previous study (27), which
reported that the 5-year metastasis-free survival rate in patients
with TNBC and vascular invasion was lower than in TNBC patients
without vascular invasion (P=0.003) (27).
Simon et al (28) demonstrated that none of these tumors
contained mutated KIT; however, in the present study a
higher rate of CD117 expression was identified in patients with
TNBC than in patients with non-TNBC, consistent with previous
studies (11,29). It was also confirmed that the presence
of CD117 was associated with the expression of MKI67 and vascular
invasion in patients with TNBC, consistent with previous
observations (6,29).
There are conflicting reports regarding the
prognostic value of CD117 in TNBC; Several reports have
demonstrated that CD117 may not influence the survival of patients
with TNBC (11,30), whereas Kashiwagi et al have
confirmed a poorer outcome for CD117-positive TNBC (9). Overexpression of CD117 protein was
associated with poor prognosis and recurrence in TNBC, but was not
identified as an independent prognostic factor in the present
study. A possible explanation for these opposing results is
differences in threshold for categorizing samples as
KIT-positive; Thike et al (6) used ≥1% of tumor cells as positive
criteria, whereas Kashiwagi et al (9) set their threshold as ≥10%. In the
present study, the threshold was set at 10% of stained cells.
Another explanation for these opposing results is differences in
criteria of HER2 positive expression for the determination of TNBC.
Nielsen et al (30) classified
the HER2 expression according to a three-point scoring system, in
which patients were divided into three groups (negative,
weakly-positive and positive groups); overexpression of CD117
protein was considered not to be associated the poor prognosis of
TNBC patients. However, in the present study, HER2 immunostaining
was considered positive (graded 3+, or gene amplification confirmed
by FISH), since it is a standard threshold for TNBC assessment.
A number of previous studies have investigated
TP53 gene mutations in TNBC (31). In the present study, the frequency of
TP53 missense mutations was increased in TNBC compared with
non-TNBC tissues, consistent with previous observations (32). A positive association was not observed
between the expression of p53 protein and TP53 missense
mutations in TNBC in the present study using direct sequencing,
consistent with previous reports (33). However, Kim et al (34) reported that expression levels of p53
were also influenced by TP53 mutation status and mRNA level
of TP53. The authors detected TP53 mutations using
next-generation sequencing (34),
while direct sequencing in our study. Taylor et al (35) found that results of p53 by IHC could
identifying TP53 missense mutations in exons 4–8 in breast cancer,
because moderate/average nuclear staining intensity for TP53
as a positive criterion, rather than the >10% positive tumor
cells that was used in the present study. Furthermore, a previous
study reported the Arg72Pro polymorphism in the TNBC NIPBC-2 cell
line (36). In the present study, the
Arg72Pro polymorphism was identified in 41.4% of patients with TNBC
and in 35.4% of the non-TNBC patients; the positive rate in
patients of TNBC compared with in the non-TNBC patients was similar
(P=0.530).
It has been reported that p53 expression is
associated with the prognosis of patients with TNBC (15). The present study revealed that
TP53 missense mutations were associated with poor patient
prognosis and a high risk of relapse in patients with TNBC, which
was consistent with a previous report (37). Silwal-Pandit et al identified
that TP53 mutations in TNBC are not associated with an
unfavorable prognosis (38).
TP53 mutations were also detected in exon2-8 (38), whereas the present study analyzed
TP53 missense mutations in exon4-8.
To the best of our knowledge, the present study
reported an association between CD117 expression and TP53
missense mutations for the first time, but not the association
between CD117 expression and codon 72 polymorphisms, or synonymous
mutations in patients with TNBC. CD117+/TP53
missense mutation+ was associated with positive MKI67
expression, vascular invasion and tumor recurrence. On the basis of
these results, it may be hypothesized that
CD117+/TP53 missense mutation+ is
associated with the malignant biological behavior of patients with
TNBC. p53 has been reported to regulate numerous genes, including
MYC proto-oncogene and KIT, affecting the aggressive
biological behavior of cancer (39–41). p53
may also directly regulate microRNA-34 (miR-34), with inactivation
of p53 reducing miR-34 expression, promoting the invasion of colon
cancer cells (18). Furthermore, the
present study demonstrated that the expression of CD117 protein in
TNBC tissues was an independent prognostic factor in patients with
TNBC with TP53 missense mutations.
It was not possible to perform sub-categorization of
patients with TNBC according to biological characteristics such as
EGFR amplification, which may be one limitation of the present
study. CD117+/TP53 missense mutation+
was not analyzed in patients with TNBC of different genotypes. The
present study also did not detect the level of miR-34 or analyze
the association between miR-34 and CD117+/TP53
missense mutation+. Therefore, further study into the
effect of CD117+/TP53 missense
mutation+ in patients with TNBC with different genotypes
and the association between miR-34 and
CD117+/TP53 missense mutation+ is
required.
In conclusion, the present study confirmed that
CD117+/TP53 missense mutation+ was
associated with MKI67 expression, vascular invasion and tumor
recurrence in patients with TNBC. CD117 expression was indicative
of poor prognosis in patients with TNBC with TP53 missense
mutations.
Acknowledgements
The authors would like to thank thank Keyang Sun,
Liang Liu and Jie Chen for preparing the paraffin-embedded slides,
and Miss Liang Liu and Mr Jie Chen as technicians (Department of
Pathology, Shanghai No. 6 People's Hospital, Shanghai, China) for
their help with immunohistochemical staining was.
Funding
This project was supported by grants from the
National Natural Science Foundation (grant no. 81100223) and from
Shanghai Municipal Health Bureau Program (grant no. 20134052).
Availability of data and materials
The analyzed data sets generated during the study
are available from the corresponding author, on reasonable
request.
Authors' contributions
Preparation of the DNA, sequencing, IHC and analysis
of data were performed by YLL. Statistical analysis was also
performed by YLL. The slides were analyzed by HZZ and WTH. GL
participated in analysis of experimental data and conducted the PCR
experiment. The manuscript was written by YLL and reviewed by HZZ
and GL.
Ethics approval and consent to
participate
The Ethics Committee for Human Studies at Shanghai
Jiao Tong University (Shanghai, China) approved the present study,
which was conducted in accordance with The Declaration of Helsinki.
Participants were fully informed of the procedures, and written
informed consent was obtained from all patients.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Foulkes WD, Smith IE and Reis-Filho JS:
Triple-negative breast cancer. N Engl J Med. 363:1938–1948. 2010.
View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Changavi AA, Shashikala A and Ramji AS:
Epidermal growth factor receptor expression in triple negative and
nontriple negative breast carcinomas. J Lab Physicians. 7:79–83.
2015. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Metzger-Filho O, Tutt A, de Azambuja E,
Saini KS, Viale G, Loi S, Bradbury I, Bliss JM, Azim HA Jr, Ellis
P, et al: Dissecting the heterogeneity of triple-negative breast
cancer. J Clin Oncol. 30:1879–1887. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Lasota J and Miettinen M: Clinical
significance of oncogenic KIT and PDGFRA mutations in
gastrointestinal stromal tumours. Histopathology. 53:245–266. 2008.
View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Yoshida C, Tsuji AB, Sudo H, Sugyo A,
Kikuchi T, Koizumi M, Arano Y and Saga T: Therapeutic efficacy of
c-kit-targeted radioimmunotherapy using 90Y-labeled anti-c-kit
antibodies in a mouse model of small cell lung cancer. PLoS One.
8:e592482013. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Thike AA, Iqbal J, Cheok PY, Chong AP, Tse
GM, Tan B, Tan P, Wong NS and Tan PH: Triple negative breast
cancer: Outcome correlation with immunohistochemical detection of
basal markers. Am J Surg Pathol. 34:956–964. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Blassl C, Kuhlmann JD, Webers A, Wimberger
P, Fehm T and Neubauer H: Gene expression profiling of single
circulating tumor cells in ovarian cancer-Establishment of a
multi-marker gene panel. Mol Oncol. 10:1030–1042. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Fan H, Yuan Y, Wang J, Zhou F, Zhang M,
Giercksky KE, Nesland JM and Suo Z: CD117 expression in operable
oesophageal squamous cell carcinomas predicts worse clinical
outcome. Histopathology. 62:1028–1037. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Kashiwagi S, Yashiro M, Takashima T,
Aomatsu N, Kawajiri H, Ogawa Y, Onoda N, Ishikawa T, Wakasa K and
Hirakawa K: c-Kit expression as a prognostic molecular marker in
patients with basal-like breast cancer. Br J Surg. 100:490–496.
2013. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Medinger M, Kleinschmidt M, Mross K,
Wehmeyer B, Unger C, Schaefer HE, Weber R and Azemar M: c-kit
(CD117) expression in human tumors and its prognostic value: An
immunohistochemical analysis. Pathol Oncol Res. 16:295–301. 2010.
View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Jansson S, Bendah PO, Grabau DA, Falck AK,
Fernö M, Aaltonen K and Rydén L: The three receptor tyrosine
kinases c-KIT, VEGFR2 and PDGFRα, closely spaced at 4q12, show
increased protein expression in triple-negative breast cancer. PLoS
One. 9:e1021762014. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Kim HW, Lee HM, Hwang SH, Ahn SG, Lee KA
and Jeong J: Patterns and biologic features of p53 mutation types
in Korean breast cancer patients. J Breast Cancer. 17:1–7. 2014.
View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Kruiswijk F, Labuschagne CF and Vousden
KH: p53 in survival, death and metabolic health: A lifeguard with a
licence to kill. Nat Rev Mol Cell Biol. 16:393–405. 2015.
View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Fernández-Cuesta L, Oakman C,
Falagan-Lotsch P, Smoth KS, Quinaux E, Buyse M, Dolci MS, Azambuja
ED, Hainaut P, Dell'orto P, et al: Prognostic and predictive value
of TP53 mutations in node-positive breast cancer patients treated
with anthracycline- or anthracycline/taxane-based adjuvant therapy:
Results from the BIG 02–98 phase III trial. Breast Cancer Res.
14:R702012. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Chae BJ, Bae JS, Lee A, Park WC, Seo YJ,
Song BJ, Kim JS and Jung SS: p53 as a specific prognostic factor in
triple-negative breast cancer. Jpn J Clin Oncol. 39:217–224. 2009.
View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Olivier M, Langerød A, Carrieri P, Bergh
J, Klaar S, Eyfjord J, Theillet C, Rodriguez C, Lidereau R, Bièche
I, et al: The clinical value of somatic TP53 gene mutations in
1,794 patients with breast cancer. Clin Cancer Res. 12:1157–1167.
2006. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Foedermayr M, Sebesta M, Rudas M, Berghoff
AS, Promberger R, Preusser M, Dubsky P, Fitzal F, Gnant M, Steger
GG, et al: BRCA-1 methylation and TP53 mutation in triple-negative
breast cancer patients without pathological complete response to
taxane-based neoadjuvant chemotherapy. Cancer Chemother Pharmacol.
73:771–778. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Siemens H, Jackstadt R, Kaller M and
Hermeking H: Repression of c-Kit by p53 is mediated by miR-34 and
is associated with reduced chemoresistance, migration and stemness.
Oncotarget. 4:1399–1415. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Mittendorf EA, Ballman KV, McCall LM, Yi
M, Sahin AA, Bedrosian I, Hansen N, Gabram S, Hurd T, Giuliano AE
and Hunt KK: Evaluation of the stage IB designation of the American
Joint Committee on Cancer staging system in breast cancer. J Clin
Oncol. 33:1119–1127. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Penault-Llorca F, André F, Sagan C,
Lacroix-Triki M, Denoux Y, Verriele V, Jacquemier J, Baranzelli MC,
Bibeau F, Antoine M, et al: Ki67 expression and docetaxel efficacy
in patients with estrogen receptor-positive breast cancer. J Clin
Oncol. 27:2809–2815. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Huang Q, Li F, Liu X, Li W, Shi W, Liu FF,
O'Sullivan B, He Z, Peng Y, Tan AC, et al: Caspase 3-mediated
stimulation of tumor cell repopulation during cancer radiotherapy.
Nat Med. 17:860–866. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Yaman S, Gumuskaya B, Ozkan C, Aksoy S,
Guler G and Altundag K: Lymphatic and capillary invasion patterns
in triple negative breast cancer. Am Surg. 78:1238–1242.
2012.PubMed/NCBI
|
|
23
|
Varga Z, Noske A, Ramach C, Padberg B and
Moch H: Assessment of HER2 status in breast cancer: Overall
positivity rate and accuracy by fluorescence in situ hybridization
and immunohistochemistry in a single institution over 12 years: A
quality control study. BMC Cancer. 13:6152013. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Yue YI, Astvatsaturyan K, Cui X, Zhang X,
Fraass B and Bose S: Stratification of prognosis of triple-negative
breast cancer patients using combinatorial biomarkers. PLoS One.
11:e01496612016. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Ricciardi GR, Adamo B, Ieni A, Licata L,
Cardia R, Ferraro G, Franchina T, Tuccari G and Adamo V: Androgen
Receptor (AR), E-cadherin, and Ki-67 as emerging targets and novel
prognostic markers in Triple-Negative Breast Cancer (TNBC)
patients. PLoS One. 10:e01283682015. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Keam B, Im SA, Lee KH, Han SW, Oh DY, Kim
JH, Lee SH, Han W, Kim DW, Kim TY, et al: Ki-67 can be used for
further classification of triple negative breast cancer into two
subtypes with different response and prognosis. Breast Cancer Res.
13:R222011. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Sabatier R, Jacquemier J, Bertucci F,
Esterni B, Finetti P, Azario F, Birnbaum D, Viens P, Gonçalves A
and Extra JM: Peritumoural vascular invasion: A major determinant
of triple-negative breast cancer outcome. Eur J Cancer.
47:1537–1545. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Simon R, Panussis S, Maurer R, Spichtin H,
Glatz K, Tapia C, Mirlacher M, Rufle A, Torhorst J and Sauter G:
KIT (CD117)-positive breast cancers are infrequent and lack KIT
gene mutations. Clin Cancer Res. 10:178–183. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Kanapathy Pillai SK, Tay A, Nair S and
Leong CO: Triple-negative breast cancer is associated with EGFR,
CK5/6 and c-KIT expression in Malaysian women. BMC Clin Pathol.
12:182012. View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Nielsen TO, Hsu FD, Jensen K, Cheang M,
Karaca G, Hu Z, Hernandez-Boussard T, Livasy C, Cowan D, Dressler
L, et al: Immuno-histochemical and clinical characterization of the
basal-like subtype of invasive breast carcinoma. Clin Cancer Res.
10:5367–5374. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Fountzilas G, Giannoulatou E, Alexopoulou
Z, Zagouri F, Timotheadou E, Papadopoulou K, Lakis S, Bobos M,
Poulios C, Sotiropoulou M, et al: TP53 mutations and protein
immunopositivity may predict for poor outcome but also for
trastuzumab benefit in patients with early breast cancer treated in
the adjuvant setting. Oncotarget. 7:32731–32753. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
32
|
Kim Y, Kim J, Lee HD, Jeong J, Lee W and
Lee KA: Spectrum of EGFR gene copy number changes and KRAS gene
mutation status in korean triple negative breast cancer patients.
PLoS One. 8:e790142013. View Article : Google Scholar : PubMed/NCBI
|
|
33
|
Végran F, Rebucci M, Chevrier S, Cadouot
M, Boidot R and Lizard-Nacol S: Only missense mutations affecting
the DNA binding domain of p53 influence outcomes in patients with
breast carcinoma. PLoS One. 8:e551032013. View Article : Google Scholar : PubMed/NCBI
|
|
34
|
Kim JY, Park K, Jung HH, Lee E, Cho EY,
Lee KH, Bae SY, Lee SK, Kim SW, Lee JE, et al: Association between
mutation and expression of TP53 as a potential prognostic marker of
triple-negative breast cancer. Cancer Res Treat. 48:1338–1350.
2016. View Article : Google Scholar : PubMed/NCBI
|
|
35
|
Taylor NJ, Nikolaishvili-Feinberg N,
Midkiff BR, Conway K, Millikan RC and Geradts J: Rational manual
and automated scoring thresholds for the immunohistochemical
detection of TP53 missense mutations in human breast carcinomas.
Appl Immunohistochem Mol Morphol. 24:398–404. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
36
|
Pandrangi SL, Raju Bagadi SA, Sinha NK,
Kumar M, Dada R, Lakhanpal M, Soni A, Malvia S, Simon S, Chintamani
C, et al: Establishment and characterization of two primary breast
cancer cell lines from young Indian breast cancer patients:
Mutation analysis. Cancer Cell Int. 14:142014. View Article : Google Scholar : PubMed/NCBI
|
|
37
|
Dobes P, Podhorec J, Coufal O, Jureckova
A, Petrakova K, Vojtesek B and Hrstka R: Influence of mutation type
on prognostic and predictive values of TP53 status in primary
breast cancer patients. Oncol Rep. 32:1695–1702. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
38
|
Silwal-Pandit L, Vollan HK, Chin SF, Rueda
OM, McKinney S, Osako T, Quigley DA, Kristensen VN, Aparicio S,
Børresen-Dale AL, et al: TP53 mutation spectrum in breast cancer is
subtype specific and has distinct prognostic relevance. Clin Cancer
Res. 20:3569–3580. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
39
|
Abraham SA, Hopcroft LE, Carrick E, Drotar
ME, Dunn K, Williamson AJ, Korfi K, Baquero P, Park LE, Scott MT,
et al: Dual targeting of p53 and c-MYC selectively eliminates
leukaemic stem cells. Nature. 534:341–346. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
40
|
Yogev O, Barker K, Sikka A, Almeida GS,
Hallsworth A, Smith LM, Jamin Y, Ruddle R, Koers A, Webber HT, et
al: p53 loss in MYC-driven neuroblastoma leads to metabolic
adaptations supporting radioresistance. Cancer Res. 76:3025–3035.
2016. View Article : Google Scholar : PubMed/NCBI
|
|
41
|
Lai JH, Fleming KE, Ly TY, Pasternak S,
Godlewski M, Doucette S and Walsh NM: Pure versus combined Merkel
cell carcinomas: Immunohistochemical evaluation of cellular
proteins (p53, Bcl-2 and c-kit) reveals significant overexpression
of p53 in combined tumors. Hum Pathol. 46:1290–1296. 2015.
View Article : Google Scholar : PubMed/NCBI
|