Introduction
Colorectal cancer (CRC) is one of the most common
types of cancer worldwide and, according to cancer statistics in
China, CRC incidence and mortality rates were fifth of all cancer
in 2015 (1). In Eastern China,
age-standardized (Segi standard population) incidence and mortality
rates (2) for CRC remain high. The
occurrence and development of colorectal cancer is a process that
involves multiple factors, steps and genes, which results from a
complex combination of internal and external factors. CRC may be
divided into two groups: Inherited colorectal cancer and sporadic
colorectal cancer (SCRC), the latter of which accounts for ~85% of
all colorectal cancer cases (3). In
addition, it was reported that ~2/3 of all CRC tumors with
deficient DNA mismatch repair (dMMR) were SCRC (4), and dMMR was associated to a favorable
prognosis for CRC (5).
The process of CRC can involve three types of
genetic alterations: Activation or upregulation of oncogenes,
inactivation or loss of function of tumor suppressor genes, and
abnormalities or functional decline in DNA repair gene structure
(6). MMR aids the maintenance of
genome stability by correcting base-base mismatches and
insertion/deletion mis-pairing generated during DNA replication and
recombination (7). Deficiencies in
MMR are recognized through the presence of microsatellite
instability (MSI), which can be identified using polymerase chain
reaction amplification of specific tumor microsatellite foci, or by
a deficiency in expression of any of the MMR proteins, including
MutL homolog 1 (MLH1), MutS homolog 2 (MSH2), MSH6, and PMS1
homolog 2, mismatch repair system component (PMS2), detected by
immunohistochemistry (IHC) (8). IHC
analysis of expression of MMR proteins is frequently used as it
does not require a laboratory and the ability to identify the
affected gene by detecting loss of its protein product.
Furthermore, the IHC-detected loss of MMR protein expression was
highly concordant with DNA-based MSI testing (9). Notably, to the best of our knowledge,
only the loss of MLH1 protein expression, observed by IHC, has been
described in SCRCs (10).
Alterations in both the epigenome and genome occur
commonly in colorectal cancer and likely drive the tumorigenesis
process through activation of oncogenes and inactivation of tumor
suppressor genes (11). The present
study aimed to investigate the association between dMMR expression
and prognosis in SCRC with long-term individual survey. To the best
of our knowledge, the present study is the first to demonstrate an
association between MMR-deficiency and the prognosis of an Eastern
Chinese population of patients with sporadic CRC.
Materials and methods
Samples
A total of 221 patients with colorectal cancer
underwent radical surgery treatments with open surgery or
laparoscopic surgery in the Department of Gastrointestinal Surgery
of Weihai Municipal Hospital (Shandong, China) between January 2011
and January 2012. All patients had been pathologically confirmed to
have colorectal adenocarcinoma. Pathological stage was determined
according to tumor-node-metastasis staging system of American Joint
Committee on Cancer (AJCC) (12). The
tumor tissues were collected from 192 patients and additional
non-tumoral normal epithelial tissue samples (~5 cm from the border
of the main tumor lesion) were collected from 138 of these
patients. A total of 16 cases were excluded with strict exclusion
criteria; including, familial adenomatous polyposis (FAP),
hereditary non-polyposis colorectal cancer (HNPCC) based on
Bethesda guidelines (13), mortality
within 1 month of surgery, preoperative adjuvant therapy, and
non-colorectal adenocarcinoma (including neuroendocrine neoplasm
and lymphoma) (14,15). In order to exclude genetic effects,
patients with a known family history or those suspected to have
hereditary or familial CRC, FAP or HNPCC were excluded. In order to
exclude the effects of treatment, patients who succumbed within one
month following operation and those who underwent preoperative
adjuvant therapy were also excluded. One sample was diagnosed as
neuroendocrine neoplasm.
A total of 16 cases were excluded, which included
FAP (n=1), HNPCC (n=4), death from cardiopulmonary complication
(n=1), neuroendocrine neoplasm (n=1), recurrence of colorectal
carcinoma (n=1) and neo-adjuvant chemotherapy (n=8). A further 13
of 205 cases refused to participate in the present study; therefore
192 cases were enrolled. The age range of the patients was 33–89
years (mean, 63.2±10.8 years). A total of 112 of the patients were
male (mean age, 63.5±10.8 years) and 80 of the patients were female
(mean age, 62.9±11.0 years). The median follow-up time was 43.5
months. At the last follow-up (January 2016), 107 patients were
alive and 85 patients had succumbed to disease. An estimated 4-year
survival time for the entire population was 55.73%. The present
study was approved by the Ethics and Scientific Committees of
Weihai Municipal Hospital. Written informed consent was obtained
from all participants in the study.
Immunohistochemistry staining
Primary antibodies, including rabbit polyclonal
antibodies against human MSH2 (cat. no. AP08394PU-N), MSH6 (cat.
no. TA326879) and PMS2 (cat. no. AP00189PU-N) were purchased from
OriGene Technologies, Inc., Beijing, China. Primary mouse antibody
against human MLH1 (cat. no. sc-56161) was purchased from Santa
Cruz Biotechnology, Inc., Dallas, TX, USA. All specimens were fixed
with 10% formalin and embedded in paraffin at room temperature for
24 h, and each block was sectioned at 4 µm. All sections were
deparaffinized and rehydrated in a descending alcohol series.
Slides were heated (96–98°C) in 1 mmol/l EDTA buffer for 20 min for
antigen retrieval. Slides were incubated with 0.3% hydrogen
peroxide to quench endogenous peroxidase activity at room
temperature for 30 min, and non-specific binding was blocked in 10%
goat serum (DAB Detection kit (Streptavidin-Biotin) cat. no.
SP-9000; OriGene Technologies, Inc., Beijing, China) at room
temperature for 1 h. Slides were incubated at 4°C, overnight with
primary antibodies against MLH1, MSH2, MSH6 and PMS2 (dilution
1:500). The subsequent steps were performed according to
streptavidin-peroxidase method protocols (16). Then each slide was incubated with 30
µl of goat anti-rabbit or anti-mouse biotin-conjugated secondary
antibody for 30 min at 37°C (cat. no. SP-9000; ZSGB-BIO; Beijing,
China). A volume of 100 µl HRP conjugates were applied to the
sections, and incubated in a humidified chamber at room temperature
for 30 min. The primary antibody was replaced with normal goat
serum (OriGene Technologies, Inc.) or PBS for negative controls,
and nuclear staining of MMR proteins in normal colonic epithelium
cells and lymphocytes served as positive controls.
Staining evaluation
The samples with >10% of tumor cells stained for
any MMR protein were considered to be MMR-positive. The criteria
used for semi-quantification of immunohistochemical staining
included the staining intensity and the percentage of positively
stained cells. A range of 0–3 was defined for classifying the
intensity of staining: 0, Absence of staining; 1, weak staining; 2,
moderate staining; and 3, intense staining. Furthermore, extent of
staining was scored as 0 (<10%), 1 (11–25%), 2 (26–50%), 3
(51–75%), and 4 (76–100%) for evaluation. The final scores were
calculated by multiplying the staining intensity by the extension
(17). In the present study, all the
final scores were stratified as negative MMR expression (0 score)
or positive MMR expression (>0). The MMR-positive group included
low expression (1–4 score), moderate expression (5–8 score) and
high expression (9–12 score). All pathological sections were
reviewed by at least two experienced pathologists affiliated to the
Department of Pathology of Weihai Municipal Hospital.
Statistical analysis
All data are presented as the mean ± standard
deviation (SD) or the median SD. For example, data for OS or PFS
were median ± SD, and data for age were presented as mean ± SD.
SPSS 18.0 software (SPSS Inc., Chicago, IL, USA) was used for
statistical analysis. Fisher's exact test and χ2 test
were used to evaluate clinicopathological significance of enrolled
patients' characteristics in SCRC. The Kaplan-Meier method and log
rank test were used to calculate survival data. The Cox regression
tests were used for independent prognosis factor analysis.
Two-sided P-values were calculated, and P<0.05 was considered to
indicate a statistically significant difference.
Results
Patient characteristics
Samples from 192 patients with sporadic colorectal
cancer who had undergone complete surgical resection were obtained
in the present study (Table I). The
age distribution of cases was between 33 and 89 years old and the
mean age was 63.2±10.8 years. A total of 112 of 192 cases were
males and the mean age was 63.5±10.8 years; 80 of 192 patients were
female and the mean age was 62.9±11.0 years.
 | Table I.Clinical characteristics of 192
patients with sporadic colorectal cancer. |
Table I.
Clinical characteristics of 192
patients with sporadic colorectal cancer.
| Variables | Patients, n (%) |
|---|
| Sex |
|
| Male | 112 (58.3) |
|
Female | 80 (41.7) |
| Age, years |
|
| ≥60 | 124 (64.6) |
|
<60 | 68 (35.4) |
| Location |
|
| Right
colon | 40 (20.8) |
| Left
colon | 44 (22.9) |
|
Rectum | 108 (56.3) |
| Differentiation |
|
|
Well/moderate | 139 (72.4) |
| Poor | 53 (27.6) |
| Tumor stage |
|
|
T1+T2 | 42 (21.9) |
|
T3+T4 | 150 (78.1) |
| Lymph node
status |
|
| pN0 | 121 (63.0) |
| pN1 | 45 (23.4) |
| pN2 | 26 (13.6) |
| Metastasis
status |
|
|
Negative | 187 (97.4) |
|
Positive | 5 (2.6) |
| Invasion |
|
|
Negative | 129 (67.2) |
|
Positive | 63 (32.8) |
| MMR status |
|
|
dMMR | 28 (14.6) |
|
pMMR | 164 (85.4) |
Expression of MMR in sporadic
colorectal cancer
To investigate the status of the MMR proteins MLH1,
MSH2, MSH6, PMS2 in SCRC, an IHC assay was performed to evaluate
the expression of MMR. Fig. 1
demonstrates representative typical IHC staining images of positive
and negative nuclear expression of MLH1, MSH2, MSH6 and PMS2 in
different patients with SCRC. Fig. 1A
depicts tumor cells with retained MLH1, MSH2, MSH6 and PMS2
expression, which were regarded as MMR proficient, while Fig. 1B depicts cells lacking MLH1, MSH2,
MSH6 and PMS2, which were regarded as deficient MMR. Stromal cells
and lymphocytes served as internal positive controls and
non-tumoral normal epithelial tissue as normal controls (data not
shown). In the present study, the total rate of deficient MMR
(dMMR) was 14.58% (28/192): MSH6, 0.52% (1/192); PMS2, 4.17%
(8/192); MSH2/MSH6, 3.65% (7/192); and MLH1/PMS2, 6.25% (12/192).
These differences in expression may be due to race, sample size,
test methods and result evaluation. Distant metastasis was not
observed in the dMMR group on count of sample number probably,
while there were 5 cases of distant metastasis in the pMMR
group.
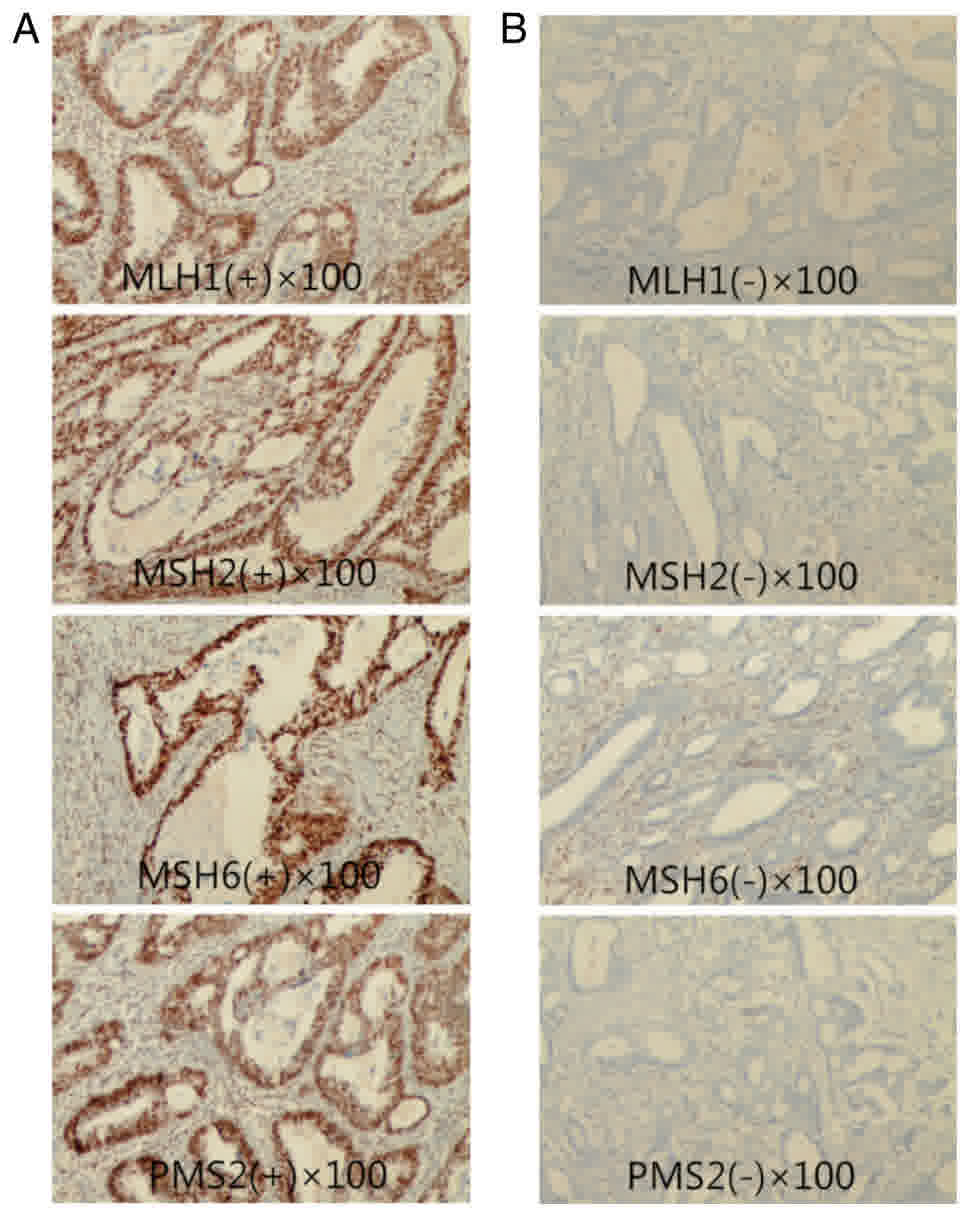 | Figure 1.Representative typical
immunohistochemical staining images of positive and negative
nuclear expression of MLH1, MSH2, MSH6 and PMS2 in different
patients with sporadic colorectal cancer. Tumor cells with (A)
retained MLH1, MSH2, MSH6 and PMS2 expression, which were regarded
as MMR proficient, and with (B) absent MLH1, MSH2, MSH6 and PMS2
expression, which were regarded as MMR deficient. MLH1, MutL
homolog 1; MSH2, MutS homolog 2; PMS2, PMS1 homolog 2, mismatch
repair system component; MMR, mismatch repair gene. |
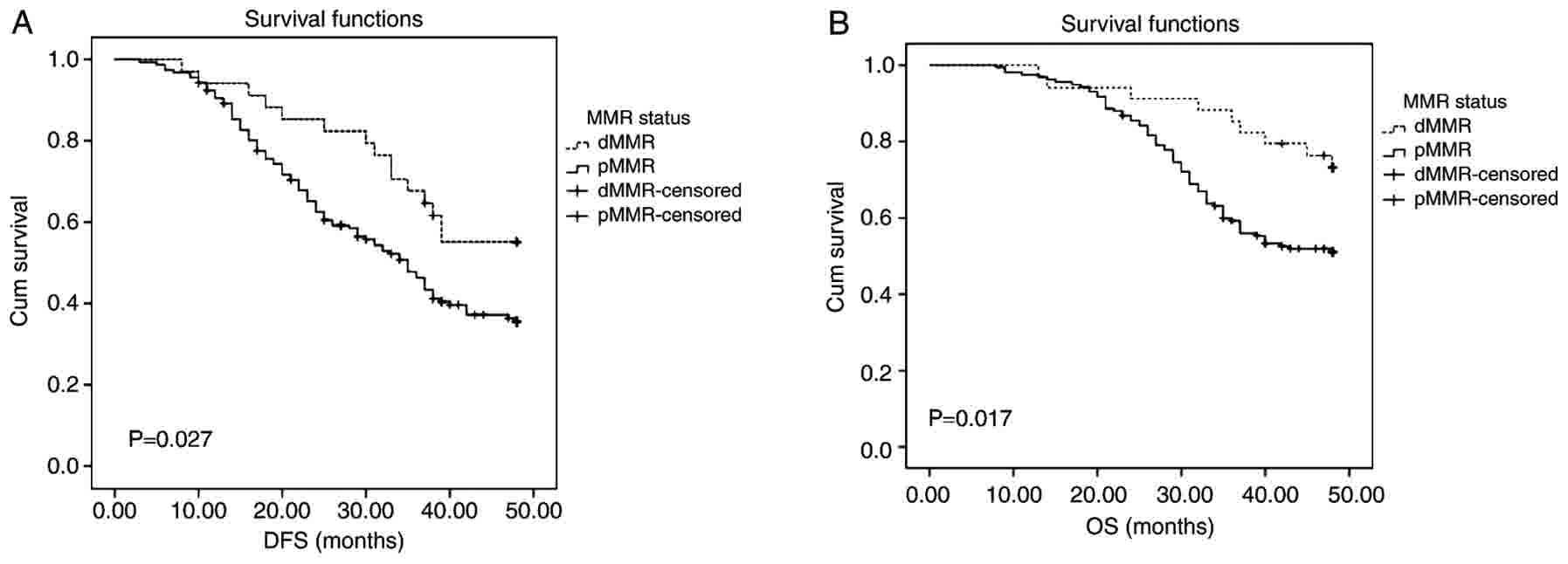
Association between MMR expression and
overall survival (OS) or disease-free survival (DFS) in sporadic
colorectal cancer
Patients were divided into pMMR and dMMR expression
groups. Kaplan-Meier curves and log-rank test results for DFS and
OS were demonstrated in Fig. 2.
Patients with dMMR presented with longer DFS and OS times (median
survival ± SD, 40±10.83 and 49±8.52, respectively) compared with
those with pMMR (median survival ± SD, 28±12.11 and 39±10.02,
respectively) (Fig. 2; P=0.027 and
P=0.017, respectively).
Univariate and multivariate analysis
of prognostic factors in sporadic colorectal cancer
To determine the association between MMR status and
prognostic factors in SCRC, Cox proportional hazard model was used,
and univariate analysis revealed that patient sex, age, tumor
location, tumor differentiation, tumor stage, lymph node status,
metastasis status, invasion and MMR status were significantly
associated with DFS and OS. Differentiation, tumor stage, lymph
node status, metastasis status, invasion and MMR status were
identified to be significant prognostic factors for DFS by
univariate analysis. For multivariate analysis, differentiation,
tumor stage, lymph node status and MMR status were independent
significant prognostic factors for DFS (P=0.006, P<0.001,
P<0.001, P=0.003, respectively; Table
II). Age, differentiation, tumor stage, lymph node status,
metastasis status, invasion and MMR status were identified to be
significant prognostic factors for OS by univariate analysis. For
multivariate analysis, age, differentiation, tumor stage, lymph
node status, metastasis status, invasion and MMR status were
identified to be independent prognostic factors for OS (Table III; P=0.003, P=0.047, P<0.001,
P<0.001, P=0.027, P=0.004, P<0.001, respectively).
| Table II.Univariate and multivariate analysis
of prognostic factors for disease-free survival in sporadic
colorectal cancer. |
Table II.
Univariate and multivariate analysis
of prognostic factors for disease-free survival in sporadic
colorectal cancer.
|
|
|
|
|
|
| 95% CI for HR |
|---|
|
|
|
|
|
|
|
|
|---|
| Factors | B | SE | Wald | P-value | HR | Lower | Upper |
|---|
| Univariate
analysis |
|
|
|
|
|
|
|
| Age
(years) | −0.358 | 0.194 | 3.398 | 0.065 | 0.699 | 0.478 | 1.023 |
|
Sex | 0.164 | 0.192 | 0.732 | 0.392 | 1.179 | 0.809 | 1.717 |
|
Location | −0.044 | 0.059 | 0.555 | 0.456 | 0.957 | 0.852 | 1.075 |
|
Differentiation | −0.862 | 0.188 | 21.044 | 0.001a | 0.422 | 0.292 | 0.610 |
| Tumor
stage | 1.151 | 0.226 | 25.987 | 0.001a | 3.162 | 2.031 | 4.923 |
| Lymph
node status | 1.239 | 0.123 | 101.937 | 0.001a | 3.453 | 2.714 | 4.391 |
|
Metastasis status | 2.471 | 0.471 | 27.541 | 0.001a | 11.834 | 4.703 | 29.779 |
|
Invasion | −1.033 | 0.194 | 28.264 | 0.001a | 0.356 | 0.243 | 0.521 |
| MMR
status | 0.599 | 0.278 | 4.623 | 0.032a | 1.819 | 1.054 | 3.140 |
| Multivariate
analysis |
|
|
|
|
|
|
|
|
Differentiation | −0.574 | 0.208 | 7.623 | 0.006a | 0.563 | 0.375 | 0.847 |
| Tumor
stage | 1.283 | 0.232 | 30.586 | 0.001a | 3.606 | 2.289 | 5.680 |
| Lymph
node status | 1.333 | 0.149 | 79.598 | 0.001a | 3.793 | 2.830 | 5.083 |
|
Metastasis status | 0.593 | 0.503 | 1.391 | 0.238 | 1.809 | 0.676 | 4.845 |
|
Invasion | 0.324 | 0.112 | 1.892 | 0.329 | 0.672 | 0.492 | 1.168 |
| MMR
status | 0.863 | 0.288 | 8.985 | 0.003a | 2.369 | 1.348 | 4.165 |
| Table III.Univariate and multivariate analysis
of prognostic factors for overall survival in sporadic colorectal
cancer. |
Table III.
Univariate and multivariate analysis
of prognostic factors for overall survival in sporadic colorectal
cancer.
|
|
|
|
|
|
| 95.0% CI for
HR |
|---|
|
|
|
|
|
|
|
|
|---|
| Factors | B | SE | Wald | P-value | HR | Lower | Upper |
|---|
| Univariate
analysis |
|
|
|
|
|
|
|
| Age
(years) | −0.580 | 0.227 | 6.515 | 0.011a | 0.560 | 0.359 | 0.874 |
|
Sex | 0.188 | 0.218 | 0.744 | 0.388 | 1.207 | 0.788 | 1.849 |
|
Location | −0.096 | 0.065 | 2.198 | 0.138 | 0.908 | 0.799 | 1.032 |
|
Differentiation | −0.790 | 0.212 | 13.849 | 0.001a | 0.454 | 0.299 | 0.688 |
| Tumor
stage | 1.036 | 0.248 | 17.420 | 0.001a | 2.819 | 1.733 | 4.585 |
| Lymph
node status | 1.297 | 0.134 | 94.256 | 0.001a | 3.658 | 2.815 | 4.752 |
|
Metastasis status | 2.832 | 0.482 | 34.472 | 0.001a | 16.978 | 6.597 | 43.696 |
|
Invasion | −1.015 | 0.218 | 21.655 | 0.001a | 0.362 | 0.236 | 0.556 |
| MMR
status | 0.813 | 0.353 | 5.307 | 0.021a | 2.255 | 1.129 | 4.504 |
| Multivariate
analysis |
|
|
|
|
|
|
|
|
Age | −0.789 | 0.237 | 11.232 | 0.003a | 0.238 | 0.278 | 0.696 |
|
Differentiation | −0.459 | 0.231 | 3.957 | 0.047a | 0.632 | 0.402 | 0.993 |
| Tumor
stage | 1.070 | 0.251 | 18.115 | 0.001a | 2.917 | 1.782 | 4.775 |
| Lymph
node status | 1.270 | 0.154 | 67.866 | 0.001a | 3.559 | 2.631 | 4.814 |
|
Metastasis status | 1.126 | 0.509 | 4.892 | 0.027a | 3.084 | 1.137 | 8.367 |
|
Invasion | 1.072 | 0.368 | 8.482 | 0.004a | 2.920 | 1.420 | 6.005 |
| MMR
status | 1.175 | 0.332 | 12.496 | 0.001a | 3.237 | 1.688 | 6.207 |
Discussion
Colorectal cancer is divided into two types, of
which one is an inherited disease, including FAP and HNPCC, and the
other is a sporadic disease (18).
The genetic foundation of HNPCC is intimately associated with MMR,
which has been well studied and proven (19). Approximately 15% of sporadic
colorectal cancer cases have been confirmed to be attributable to
the same processes and mechanisms involved in HNPCC (20); among which dMMR was a major type of
genomic instability caused by a failure to correct errors during
DNA replication. Mutation or modification of MMR genes (including
by methylation) usually causes the absence of MMR protein
expression and MSI (3). There are two
ways that tumorigenesis arises as a consequence of MMR function.
MSI can induce the activation of oncogenes or inhibition of tumor
suppressor genes. Alternatively, deficient MMR directly brings
about activation of oncogenes or the inhibition of tumor suppressor
genes (21).
The MMR system involves nine proteins: MLH1, MSH2,
MSH3, MSH6, MLH3, PMS1, PMS2, MSH4 and MSH5. Between 87 and 90% of
all mutated genes associated with colorectal cancer are MLH1 and
MSH2 (22). A study undertaken by
Herman et al (23)
demonstrated that 5′-CpG hypermethylation of MLH1 of SCRC often led
to the absence of MLH1 expression (23). In another study, Herman et al
(10) proposed that inhibition of
hypermethylation in the promoter of MLH1 of tumor cells with
demethylating agents would produce the reappearance of MLH1
expression. Another study demonstrated that the loss of MSH2
expression was linked to missense mutations (24). Other previous studies have
demonstrated that the mutation rate of MMR gene in SCRC was 10–20%
(25,26). Lindor et al (9) revealed that the absence of MLH1 protein
expression was present in 20.4% cases and that of MSH2 was absent
in in 8.8% cases in a sample of 1,114 patients with SCRC. Other
previous reports revealed that tumors in several patients with SCRC
with a deficient MMR system were frequently accompanied by poor
differentiation, mucinous subtype and occurred in the ascending
colon, as in patients with HNPCC (27,28). In
the present study, there were no significant differences in age,
sex, tumor staging, lymph node metastasis or vascular invasion
between the two groups.
Benatti et al (25) reported that mutations in the MMR gene
may only affect early-phase tumors, and were not associated with
invasion and metastasis. Other studies have demonstrated that the
outcome of patients with negative MMR expression with SCRC,
concerning overall survival and disease-free survival, were more
favorable those for the positive expression group (29). In addition, there was a reduced
relapse rate in the negative expression group (28,30). The
results from the present study are in accordance with the
conclusion above. In the present study, MMR expression status was
associated with OS and DFS rates of patients with SCRC, and with
one of the independent prognostic factors. The dMMR group had a
significantly higher OS rate than the pMMR group (P=0.017). The DFS
rate of dMMR group was also higher than those of the pMMR group
(P=0.027).
In addition, MMR system detection may have vital
predictive and guidance value for colorectal cancer response to
chemotherapy. Several studies (31,32) have
revealed that a deficiency in MMR protein expression status may be
a predictive marker of decreased benefit, and possibly even a
detrimental effect, from adjuvant therapy with fluoropyrimidine
alone in patients with stage II disease (29). Compared with patients that underwent
surgical resection alone, treatment with fluoropyrimidine following
surgery, exhibited a lower 5-year survival rate. However, it has
been reported that MMR status cannot be recommended to inform
adjuvant treatment decisions in patients with stage III CRC
(33). National Comprehensive Cancer
Network (NCCN) guidelines (34) state
that MMR testing should be performed for all patients with
colorectal cancer diagnosed at ≤70 years, including patients
diagnosed at older ages that meet the Bethesda guidelines, to
assess for the possibility of Lynch syndrome. Poorly differentiated
histology is not considered to be a high-risk feature for patients
with stage II disease whose tumors are dMMR (35).
There were certain limitations in the present study.
Although MMR status is associated with MSI level, MSI testing was
not performed. Secondly, MMR associated gene mutations were not
addressed in the present study, including those to KRAS
proto-oncogene, GTPase (KRAS) and B-Raf proto-oncogene,
serine/threonine kinase (BRAF). Mutation analysis for KRAS and
BRAF, in addition to MMR/MSI testing may be beneficial for patients
with CRC, in accordance with the NCCN guidelines (36).
In conclusion, the results of the present study
demonstrated that MMR status, as an independent prognostic factor,
has critical prognostic value in an Eastern Chinese population. MMR
testing may therefore have potential benefits in clinical
practice.
References
|
1
|
Chen W, Zheng R, Baade PD, Zhang S, Zeng
H, Bray F, Jemal A, Yu XQ and He J: Cancer statistics in China,
2015. CA Cancer J Clin. 66:115–132. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Zheng R, Zeng H, Zhang S and Chen W:
Estimates of cancer incidence and mortality in China, 2013. Chin J
Cancer. 36:662017. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Markowitz SD and Bertagnolli MM: Molecular
origins of cancer: Molecular basis of colorectal cancer. N Engl J
Med. 361:2449–2460. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Kawakami H, Zaanan A and Sinicrope FA:
Implications of mismatch repair-deficient status on management of
early stage colorectal cancer. J Gastrointest Oncol. 6:676–684.
2015.PubMed/NCBI
|
|
5
|
Popat S, Hubner R and Houlston RS:
Systematic review of microsatellite instability and colorectal
cancer prognosis. J Clin Oncol. 23:609–618. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Worthley DL, Whitehall VL, Spring KJ and
Leggett BA: Colorectal carcinogenesis: Road maps to cancer. World J
Gastroenterol. 13:3784–3791. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Sameer AS, Nissar S and Fatima K: Mismatch
repair pathway: Molecules, functions and role in colorectal
carcinogenesis. Eur J Cancer Prev. 23:246–257. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Korphaisarn K, Pongpaibul A, Limwongse C,
Roothumnong E, Klaisuban W, Nimmannit A, Jinawath A and Akewanlop
C: Deficient DNA mismatch repair is associated with favorable
prognosis in Thai patients with sporadic colorectal cancer. World J
Gastroenterol. 21:926–934. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Lindor NM, Burgart LJ, Leontovich O,
Goldberg RM, Cunningham JM, Sargent DJ, Walsh-Vockley C, Petersen
GM, Walsh MD, Leggett BA, et al: Immunohistochemistry versus
microsatellite instability testing in phenotyping colorectal
tumors. J Clin Oncol. 20:1043–1048. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Herman JG, Umar A, Polyak K, Graff JR,
Ahuja N, Issa JP, Markowitz S, Willson JK, Hamilton SR, Kinzler KW,
et al: Incidence and functional consequences of hMLH1 promoter
hypermethylation in colorectal carcinoma. Proc Natl Acad Sci USA.
95:6870–6875. 1998. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Grady WM and Carethers JM: Genomic and
epigenetic instability in colorectal cancer pathogenesis.
Gastroenterology. 135:1079–1099. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Edge SB and Compton CC: The American joint
committee on cancer: The 7th edition of the AJCC cancer staging
manual and the future of TNM. Ann Surg Oncol. 17:1471–1474. 2010.
View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Umar A, Boland CR, Terdiman JP, Syngal S,
de la Chapelle A, Rüschoff J, Fishel R, Lindor NM, Burgart LJ,
Hamelin R, et al: Revised bethesda guidelines for hereditary
nonpolyposis colorectal cancer (Lynch syndrome) and microsatellite
instability. J Natl Cancer Inst. 96:261–268. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Compton CC and Greene FL: The staging of
colorectal cancer: 2004 and beyond. CA Cancer J Clin. 54:295–308.
2004. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Compton CC, Fielding LP, Burgart LJ,
Conley B, Cooper HS, Hamilton SR, Hammond ME, Henson DE, Hutter RV,
Nagle RB, et al: Prognostic factors in colorectal cancer. College
of American Pathologists Consensus Statement 1999. Arch Pathol Lab
Med. 124:979–994. 2000.PubMed/NCBI
|
|
16
|
Wang LG, Ni Y, Su BH, Mu XR, Shen HC and
Du JJ: MicroRNA-34b functions as a tumor suppressor and acts as a
nodal point in the feedback loop with Met. Int J Oncol. 42:957–962.
2013. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Ma H, Wang L, Zhang T, Shen H and Du J:
Loss of β-arrestin1 expression predicts unfavorable prognosis for
non-small cell lung cancer patients. Tumour Biol. 37:1341–1347.
2016. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Bhattacharya P and McHugh TW: Lynch
SyndromeStatPearls. StatPearls Publishing StatPearls Publishing LLC
Treasure Island (FL); 2017
|
|
19
|
Kawakami H, Zaanan A and Sinicrope FA:
Microsatellite instability testing and its role in the management
of colorectal cancer. Curr Treat Options Oncol. 16:302015.
View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Win AK, Young JP, Lindor NM, Tucker KM,
Ahnen DJ, Young GP, Buchanan DD, Clendenning M, Giles GG, Winship
I, et al: Colorectal and other cancer risks for carriers and
noncarriers from families with a DNA mismatch repair gene mutation:
A prospective cohort study. J Clin Oncol. 30:958–964. 2012.
View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Sheng JQ, Chan TL, Chan YW, Huang JS, Chen
JG, Zhang MZ, Guo XL, Mu H, Chan AS, Li SR, et al: Microsatellite
instability and novel mismatch repair gene mutations in northern
Chinese population with hereditary non-polyposis colorectal cancer.
Chin J Dig Dis. 7:197–205. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Ericson K, Halvarsson B, Nagel J, Rambech
E, Planck M, Piotrowska Z, Olsson H and Nilbert M: Defective
mismatch-repair in patients with multiple primary tumours including
colorectal cancer. Eur J Cancer. 39:240–248. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Herman JG, Merlo A, Mao L, Lapidus RG,
Issa JP, Davidson NE, Sidransky D and Baylin SB: Inactivation of
the CDKN2/p16/MTS1 gene is frequently associated with aberrant DNA
methylation in all common human cancers. Cancer Res. 55:4525–4530.
1995.PubMed/NCBI
|
|
24
|
Belvederesi L, Bianchi F, Galizia E,
Loretelli C, Bracci R, Catalani R, Amati M and Cellerino R: MSH2
missense mutations and HNPCC syndrome: Pathogenicity assessment in
a human expression system. Hum Mutat. 29:E296–E309. 2008.
View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Benatti P, Gafa R, Barana D, Marino M,
Scarselli A, Pedroni M, Maestri I, Guerzoni L, Roncucci L,
Menigatti M, et al: Microsatellite instability and colorectal
cancer prognosis. Clin Cancer Res. 11:8332–8340. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Ohrling K, Edler D, Hallström M and
Ragnhammar P: Mismatch repair protein expression is an independent
prognostic factor in sporadic colorectal cancer. Acta Oncol.
49:797–804. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Greenson JK, Huang SC, Herron C, Moreno V,
Bonner JD, Tomsho LP, Ben-Izhak O, Cohen HI, Trougouboff P, Bejhar
J, et al: Pathologic predictors of microsatellite instability in
colorectal cancer. Am J Surg Pathol. 33:126–133. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Hutchins G, Southward K, Handley K, Magill
L, Beaumont C, Stahlschmidt J, Richman S, Chambers P, Seymour M,
Kerr D, et al: Value of mismatch repair, KRAS and BRAF mutations in
predicting recurrence and benefits from chemotherapy in colorectal
cancer. J Clin Oncol. 29:1261–1270. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Sargent DJ, Marsoni S, Monges G, Thibodeau
SN, Labianca R, Hamilton SR, French AJ, Kabat B, Foster NR, Torri
V, et al: Defective mismatch repair as a predictive marker for lack
of efficacy of fluorouracil-based adjuvant therapy in colon cancer.
J Clin Oncol. 28:3219–3226. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Sinicrope FA, Foster NR, Thibodeau SN,
Marsoni S, Monges G, Labianca R, Kim GP, Yothers G, Allegra C,
Moore MJ, et al: DNA mismatch repair status and colon cancer
recurrence and survival in clinical trials of 5-fluorouracil-based
adjuvant therapy. J Natl Cancer Inst. 103:863–875. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Hemminki A, Mecklin JP, Järvinen H,
Aaltonen LA and Joensuu H: Microsatellite instability is a
favorable prognostic indicator in patients with colorectal cancer
receiving chemotherapy. Gastroenterology. 119:921–928. 2000.
View Article : Google Scholar : PubMed/NCBI
|
|
32
|
Elsaleh H, Joseph D, Grieu F, Zeps N, Spry
N and Iacopetta B: Association of tumour site and sex with survival
benefit from adjuvant chemotherapy in colorectal cancer. Lancet.
355:1745–1750. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
33
|
Sinicrope FA and Yang ZJ: Prognostic and
predictive impact of DNA mismatch repair in the management of
colorectal cancer. Future Oncol. 7:467–474. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
34
|
Carroll PR, Parsons JK, Andriole G,
Bahnson RR, Castle EP, Catalona WJ, Dahl DM, Davis JW, Epstein JI,
Etzioni RB, et al: NCCN Guidelines Insights: Prostate cancer early
detection, version 2.2016. J Natl Compr Canc Netw. 14:509–519.
2016. View Article : Google Scholar : PubMed/NCBI
|
|
35
|
Engstrom PF, Arnoletti JP, Benson AB III,
Chen YJ, Choti MA, Cooper HS, Covey A, Dilawari RA, Early DS,
Enzinger PC, et al: NCCN clinical practice guidelines in oncology:
Colon cancer. J Natl Compr Canc Netw. 7:778–831. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
36
|
Benson AB III, Venook AP, Bekaii-Saab T,
Chan E, Chen YJ, Cooper HS, Engstrom PF, Enzinger PC, Fenton MJ,
Fuchs CS, et al: Colon cancer, version 3.2014. J Natl Compr Canc
Netw. 12:1028–1059. 2014. View Article : Google Scholar : PubMed/NCBI
|