Introduction
As a member of the malignancies globally with most
prevalence, hepatocellular carcinoma (HCC) has an escalated
associated mortality and morbidity recently (1). In spite of improvements in clinical
therapy and surveillance strategies, HCC's prognosis keeps
unsatisfied for great incidence of metastasis and recurrence in
patients with HCC after surgical resection (2). It is still challenging to predict
recurrence for patients who have undergone surgical resection.
Though HCC has several clinicopathological features like vascular
invasion and tumor multifocality which do good to assess HCC
patients' prognosis, they are not able to meet requirements in
clinic for predicting HCC course precisely (3). Thus, various biomarkers were explored to
make prediction of HCC outcomes, however, no one was accepted or
used widely in clinical practices.
In foregoing researches, Epstein-Barr virus-induced
gene 3 (EBI3) that was initiatively cloned to be a gene produced
within Epstein-Barr virus-transformed B cells via the oncogene
underlying membrane protein 1 presented a limited expression
pattern within B-cell lymphoma (4).
Recently researches showed that as one of the interleukin-12 IL-12)
family structural subunits, EBI3 can form a heterodimer with
IL-12p35 and IL-27p28 subunit to build IL-35 and IL-27,
respectively (5). Nevertheless, IL-35
inhibits whereas IL-27 stimulates anti-tumor responses of T
lymphocytes in the tumor local microenvironment (6–8). So, as a
dominant subunit of IL-27 or IL-35, EBI3 may participate in the
development or progression of cancers (9). Up to now, the information about the
expression pattern of EBI3 and its potential predicting prognosis
function on cancers are still limited and controversial.
Accumulating evidences suggested that upregulated expression of
EBI3 was associated with tumor progression and metastasis in a
variety of cancers, including lung cancer (10), gastric cancer (11), cervical cancer (12), nasopharyngeal carcinoma (13) and pancreatic cancer (14). Knockdown of EBI3 inhibited lung cancer
cell proliferation, while upregulation of EBI3 promoted lung cancer
cell growth (10). And tumor-derived
IL-35/EBI3 could promote tumor development by enhancing of tumor
angiogenesis, myeloid cell accumulation, and suppressing tumor
immunity (15). In addition, some
studies demonstrated that high expression levels of EBI3 were
associated with unfavorable prognosis in many types of cancer
patients (10,12,16).
Nevertheless, the current research about the significance of IL-35
in HCC seems to be contradictory (17,18).
Therefore, in order to explore the clinical
importance of EBI3 and its potential as a prognostic biomarker as
well as a therapeutic target, we used immunohistochemistry to
detect the expression of EBI3 in HCC TMAs with enlargement sample
size and appraised its predictive significance in the prognosis of
HCC patients receiving radical surgery resection.
Patients and methods
Patients and specimens
Twenty HCC tissues samples used in Western blot
assay, which were stored at −80°C in a refrigerator, were randomly
collected from patients suffering from liver resection at the
Affiliated Hospital of Nantong University (Nantong, China) from
2015 to 2016. Tumor specimens applied to tissue microarrays (TMAs)
analysis were consecutively chosen among 312 HCC patients
undergoing liver resection in our hospital between 2011 and 2014.
For these samples, 5-µm-thick formalin-fixed paraffin-embedded
slides were formulated in accordance with the protocol of the
Department of Pathology of our hospital. The patients'
clinicopathologic features were outlined in Table I. The enrollment criteria for all
patients in the study were i) HCC' distinctive pathologic
diagnosis; ii) with no anticancer treatment and distant metastases
before surgery; iii) underwent curative and primary resection for
HCC; and iv) availability of whole clinicopathologic and follow-up
data. Liver function was assessed by Child-Pugh classification. The
determination of tumor stage was based on the classification system
of American Joint Committee on Cancer/International Union Against
Cancer tumor-node-metastasis (TNM) in 2002. Tumor differentiation
was based by the Edmondson grading system. According to a uniform
guideline, postoperative treatments and surveillance were described
in our previous study (19). Data
were censored at last follow-up for patients without relapse or
death. The definition of time to recurrence (TTR) was time from
surgery to first detection of tumor recurrence. The definition of
overall survival (OS) was time from surgery to death for any
inducement. The study protocol was approved by the Human Research
Ethics Committee of Nantong University Affiliated Hospital and
conformed to the provisions of the Declaration of Helsinki in 1995.
Written informed consent was obtained from all study
participants.
 | Table I.Clinicopathological characteristics of
patients with hepatocellular carcinoma. |
Table I.
Clinicopathological characteristics of
patients with hepatocellular carcinoma.
| Indexes | N (total=312) | % |
|---|
| Age (years) |
|
|
| ≤52 | 155 | 49.68 |
|
>52 | 157 | 50.32 |
| Sex |
|
|
| Male | 47 | 15.06 |
|
Female | 265 | 84.94 |
| Liver cirrhosis |
|
|
| No | 33 | 10.58 |
| Yes | 279 | 89.42 |
| HBsAg |
|
|
|
Negative | 52 | 16.67 |
|
Positive | 260 | 83.33 |
| Tumor thrombus |
|
|
| No | 227 | 72.76 |
| Yes | 85 | 27.24 |
| γ-GT (U/l) |
|
|
| ≤54 | 148 | 47.44 |
|
>54 | 164 | 52.56 |
| AFP (ng/ml) |
|
|
| ≤20 | 121 | 38.78 |
|
>20 | 191 | 61.22 |
| Child-Pugh score |
|
|
| A | 309 | 99.04 |
| B | 3 | 0.96 |
| Tumor
differentiation |
|
|
| I–II | 232 | 74.36 |
|
III–IV | 80 | 25.64 |
| Tumor size (cm) |
|
|
| ≤5 | 207 | 66.35 |
|
>5 | 105 | 33.65 |
| Tumor number |
|
|
|
Single | 270 | 86.54 |
|
Multiple | 42 | 13.46 |
| Tumor
encapsulation |
|
|
|
Complete | 172 | 55.13 |
| None | 140 | 44.87 |
| TNM stage |
|
|
| I | 138 | 44.23 |
|
II–III | 174 | 55.77 |
| BCLC stage |
|
|
| A | 212 | 67.95 |
|
B-C | 100 | 32.05 |
Postoperative cumulative recurrence and survival
rates (in brackets) at 1, 3, and 5 years were 22.8% (89.7%), 42.9%
(71.9%), and 56.8% (59.9%) for the whole study population. At last
follow-up, either the recurrence of the disease (n=74) or
complications related to surgery without recurrence (n=44) caused
118 (37.8%) patients to die. The mean duration of follow-up of the
remaining 194 patients was 37.8 months (range: 17.4–58.9 months,
standard deviation: ±8.4).
TMAs construction and
immunohistochemistry
The construction of TMAs were done as previously
described (19). The TMAs were
derived from two typical histological cores out of blocks of HCC
tumor tissue embedded in paraffin using UT06 Quick-Ray Manual
Tissue Microarrayer (Unitma Co., Ltd., Seoul, South Korea).
Pathological analysis was reviewed by two independent skillful
pathologists for all specimens.
Immunohistochemistry (IHC) analysis got performed
according to the standard protocols of Envision+™
peroxidase kit (Dako, Carpinteria, CA, USA). Being deparaffinizated
and rehydrated, the tissue sections were subsequently heated with
1X sodium citrate solution at 100°C for 30 min, and then washed 3
times. Following immerged in 3% H2O2 for 15
min, the tissue sections were incubated with the rabbit polyclonal
anti-human EBI3 antibody (dilution 1:200; sc-32,868; Santa Cruz
Biotechnology, Inc., Dallas, TX, USA) overnight at 4°C. A two-step
incubation with a secondary antibody was performed using an
immunohistochemistry universal kit (ZSGB-BIO; Beijing, China).
Incubation of samples were with 3,3′-diaminobenzidine plus (Dako),
then counterstained by hematoxylin, dehydrated by graded alcohol,
cleared in xylene, and finally placed into permanent mounting media
with a cover slip.
All cases were calculated and scored by researchers
who blinded to the clinical characteristics of the patients. Taking
into account not only the staining intensity but also the
percentage of cells that stained at this intensity, scoring on EBI3
expression was calculated by the semi-quantitative H-score method.
The score of staining intensity was 0, no stain; 1+, weak stain;
2+, moderate stain; or 3+, intense stain. The intensity score
determined and multiplied the percentage of cells staining at each
intensity to create a score of intensity percentage. The scores
representing the percentage of positive cells were as follows: 0,
0–20%; 1, 21–50%, 2, 51–75%; 3, 76–100%. The calculation of final
staining scores was adding the four scores of intensity percentage.
It had a minimum value of 0 as no stain, as well as a maximum value
of 300 as 100% of cells with a 3+ staining intensity.
Cell culture
HCC cell lines Hep3B and SMMC-7721 were obtained
from the General Surgery Institute of our hospital. HCC cell lines
MHCC97-L, and MHCC97-H with low and high metastatic potential, as
well as normal human hepatic L-02 cells were purchased from Liver
Cancer Institute, Fudan University (Shanghai, China). These cells
were cultured in Dulbecco's modified Eagle's medium (DMEM; Gibco,
NY, USA) with the supplement of 10% fetal bovine serum (Hyclone,
Logan, UT, USA) and penicillin-streptomycin (Invitrogen; Carlsbad,
CA, USA) at 37°C in 5% CO2.
Western blot analysis
Tissue or cell lysates were produced and total
proteins were isolated employing standard sodium dodecyl sulfate
polyacrylamide gel electrophoresis (SDS-PAGE) and then were
transfered to polyvinylidene difluoride (PVDF) membranes
(Millipore, Billerica, MA, USA) which were washed and blocked
before incubation with anti-EBI3 (1:400, polyclonal, rabbit
anti-human; Santa Cruz Biotechnology Inc.), subsequently incubated
with horseradish peroxidase (HRP), as conjugated secondary
antibodies. An improved chemiluminescence assay was used to detect
the reactions. Glyceraldehyde-3-phosphate dehydrogenase (GAPDH) was
applied as a loading control. Western blot quantifications were
performed using Image J software (NIH, Bethesda, MD, USA).
Statistical analysis
The statistical analyses were performed using SPSS
22.0 (IBM Corporation, Armonk, NY, USA). X-tile software (Rimm Lab
at Yale University, http://medicine.yale.edu/lab/rimm/research/software.aspx)
was used to determine the cutoff values for high or low EBI3
expression (20). The relationship
between EBI3 expression and clinicopathologic features was assayed
using the χ2 test. Survival curves were speculated by
the Kaplan-Meier method and compared by log-rank test. Univariate
and multivariate analyses were made by Cox-regression model, where
all the clinicopathologic characteristics were functioned as
covariates. P<0.05 (two-tailed) was considered to indicate a
statistically significant difference.
Results
EBI3 expression pattern in HCC cell
lines and tissue samples
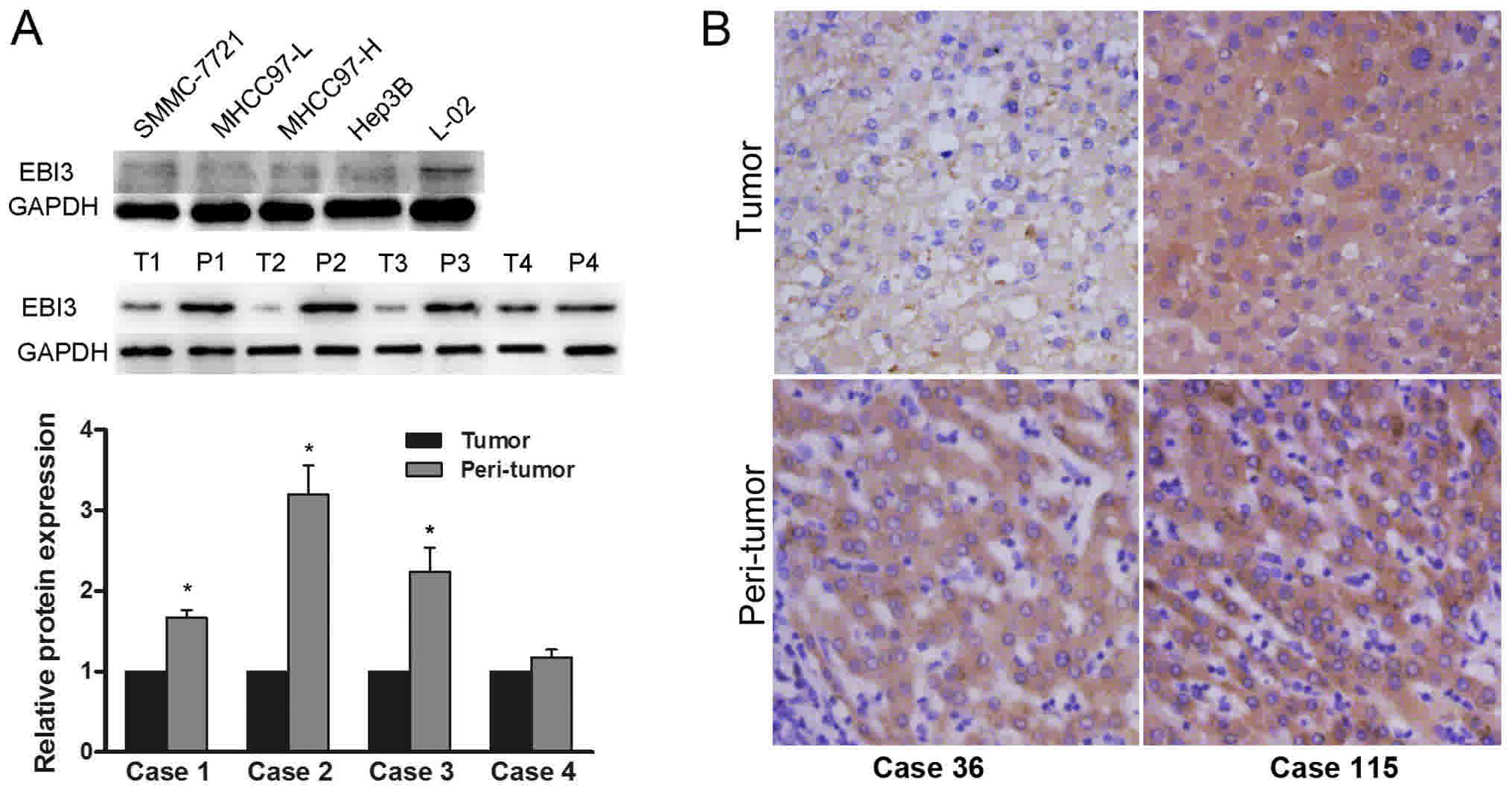
Western blot assay revealed constitutive EBI3
expression in 6 human hepatoma cell lines examined. The expression
of EBI3 was significantly upregulated in L-02 compared with that in
HCC cells MHCC97-H, MHCC97-L, and SMMC-7721 with different
metastatic potential. We found that protein expression of EBI3 was
significantly downregulated in tumors in comparison with the one in
relevant peritumoral liver tissues (Fig.
1A). Immunohistochemical analysis showed that the staining
pattern of EBI3 was mainly cytoplasmic with week or moderate
staining in tumor tissues (Fig.
1B).
Relationship of EBI3 with
clinicopathologic features
We speculated the correlationship between the
expression of EBI3 and the clinicopathologic characteristics in HCC
patients of study set. As the Table
II showed, the downregulated EBI3 was significantly correlated
with high AFP level (>20 ng/ml, P=0.001), poor differentiation
(III–IV, P<0.001), large tumor size (>5 cm, P=0.011), tumor
thrombus (P=0.027), and advanced stage tumor (BCLC stages B-C,
P=0.037; TNM stage II–III, P=0.013).
| Table II.Correlation of clinicopathologic
characteristics with EBI3 expression |
Table II.
Correlation of clinicopathologic
characteristics with EBI3 expression
|
| EBI3 expression
(n=312) |
|---|
|
|
|
|---|
| Characteristic | Total | Low | High | P-value | χ2 |
|---|
| Age (years) |
|
|
|
|
|
|
≤52 | 155 | 97 | 58 | 0.472 | 0.5178 |
|
>52 | 157 | 92 | 65 |
|
|
| Sex |
|
|
|
|
|
|
Female | 47 | 27 | 20 | 0.634 | 0.2270 |
|
Male | 265 | 162 | 103 |
|
|
| HBsAg |
|
|
|
|
|
| No | 52 | 35 | 17 | 0.277 | 1.1837 |
|
Yes | 260 | 154 | 106 |
|
|
| AFP (ng/ml) |
|
|
|
|
|
|
≤20 | 121 | 59 | 62 | 0.001 | 11.5567 |
|
>20 | 191 | 130 | 61 |
|
|
| Liver
cirrhosis |
|
|
|
|
|
| No | 33 | 19 | 14 | 0.709 | 0.1392 |
|
Yes | 279 | 170 | 109 |
|
|
| γ-GT (U/L) |
|
|
|
|
|
|
≤54 | 148 | 85 | 63 | 0.280 | 1.1658 |
|
>54 | 164 | 104 | 60 |
|
|
| Child-Pugh
score |
|
|
|
|
|
| A | 309 | 186 | 123 | 0.160 | 1.9713 |
| B | 3 | 3 | 0 |
|
|
| Tumor
differentiation |
|
|
|
|
|
|
I–II | 232 | 126 | 106 | <0.001 | 14.8784 |
|
III–IV | 80 | 63 | 17 |
|
|
| Tumor size
(cm) |
|
|
|
|
|
| ≤5 | 207 | 115 | 92 | 0.011 | 6.4941 |
|
>5 | 105 | 74 | 31 |
|
|
| Tumor number |
|
|
|
|
|
|
Single | 270 | 162 | 108 | 0.597 | 0.2795 |
|
Multiple | 42 | 27 | 15 |
|
|
| Encapsulation |
|
|
|
|
|
|
None | 172 | 101 | 71 | 0.457 | 0.5529 |
|
Complete | 140 | 88 | 52 |
|
|
| Tumor thrombus |
|
|
|
|
|
| No | 227 | 129 | 98 | 0.027 | 4.9037 |
|
Yes | 85 | 60 | 25 |
|
|
| TNM stage |
|
|
|
|
|
| I | 138 | 73 | 65 | 0.013 | 6.1089 |
|
II–III | 174 | 116 | 58 |
|
|
| BCLC stage |
|
|
|
|
|
| A | 212 | 120 | 92 | 0.037 | 4.3722 |
|
B/C | 100 | 69 | 31 |
|
|
EBI3 expression and patient
prognosis
According to data analysis of X-tile, the study set
(n=312) was divided into EBI3 low expression group (a score of from
0 to 140, n=189, 60.6%) and EBI3 high expression group (a score of
141–300, n=123, 39.4%) using a cutoff point of 140.
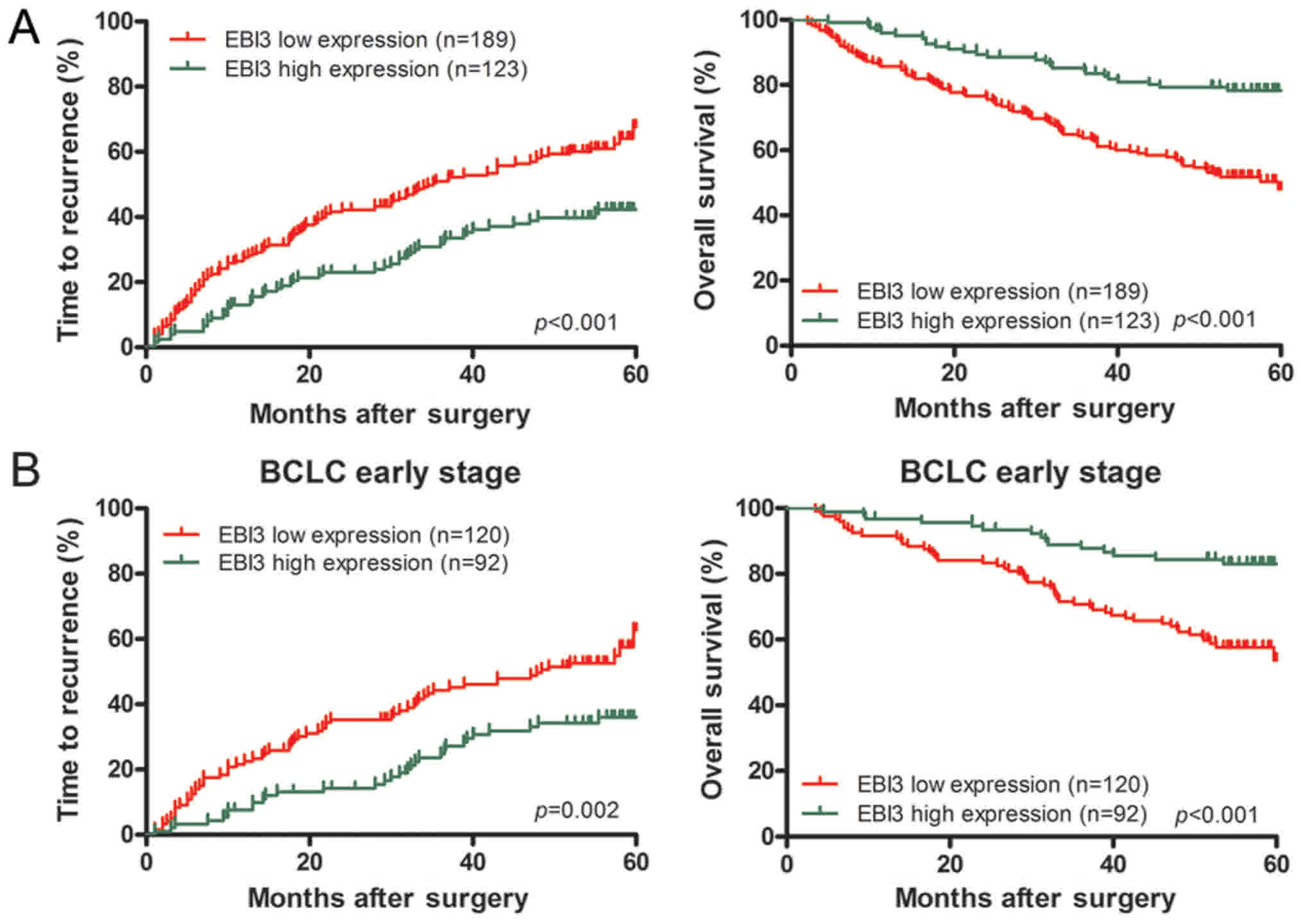
Analysis of survival showed that lower EBI3 level
was related with worse patient outcome. The median TTR was
significantly reduced among EBI3 protein-low patients (35.17±4.33
months, vs. 45.33±1.95 months for high levels, P<0.001). The
median OS was substantially reduced among patients with low EBI3
protein (43.26±1.56 months vs. 53.68±1.43 months for high levels,
P<0.001). Postoperative recurrence rates of HCC patients with
low and high expression (in brackets) of EBI3 at 1, 3, and 5 years
were 26.0% (4.8%), 50.5% (15.9%), and 68.5% (42.3%). Postoperative
OS rates of HCC patients with low and high expression (in brackets)
of EBI3 at 1, 3, and 5 years were 85.7% (95.9%), 63.8% (84.4%), and
48.1% (78.3%). Univairate analysis illustrated that downregulated
of EBI3 was significantly associated with TTR (P<0.001) and OS
(P<0.001) (Fig. 2A; Table III). Multivariate analysis
demonstrated that EBI3 was an independent predictor for TTR [hazard
ratio (HR)=0.634, 95% confidential interval (CI)=0.446–0.901,
P=0.013) and OS (HR=0.452, 95% CI=0.290–0.704, P=0.001] (Table III). In addition, apart from EBI3,
tumor size was associated with OS, and Child Pugh score and tumor
size were correlated with TTR in the multivariate analysis
(Table III).
| Table III.Univariate and multivariate analyses
of factors associated with survival and recurrence and early
stage. |
Table III.
Univariate and multivariate analyses
of factors associated with survival and recurrence and early
stage.
|
| TTR | OS |
|---|
|
|
|
|
|---|
|
| Univariate | Multivariate | Univariate | Multivariate |
|---|
|
|
|
|
|
|
|---|
| Variables | P-value | P-value | HR | 95% CI | P-value | P-value | HR | 95% CI |
|---|
| Early stage |
|
|
|
|
|
|
|
|
| AFP
level, ng/ml (≤20 vs. >20) | NS | NA |
|
| 0.035 | NS |
|
|
| Tumor
differentiation (I–II vs. III–IV) | NS | NA |
|
| NS | NA |
|
|
| Tumor
size, cm (≤5 vs. >5) | <0.001 | <0.001 | 2.089 | 1.381–3.159 | <0.001 | <0.001 | 3.345 | 2.053–5.452 |
| Tumor
number (single vs. multiple) | NS | NA |
|
| NS | NA |
|
|
|
Encapsulation (complete vs.
none) | NS | NA |
|
| NS | NA |
|
|
| EBI3
(low vs. high) | 0.003 | 0.007 | 0.553 | 0.359–0.851 | <0.001 | 0.001* | 0.388 | 0.17–0.694 |
| TMAs assay |
|
|
|
|
|
|
|
|
|
Child-Pugh score (A vs.
B) | 0.008 | 0.013 | 4.909 | 1.402–17.192 | NS | NA |
|
|
| AFP
level, ng/ml (≤20 vs. >20) | 0.021 | NS |
|
| 0.007 | NS |
|
|
| Liver
cirrhosis (no vs. yes) | NS | NA |
|
| NS | NA |
|
|
| Tumor
differentiation (I–II vs. III–IV) | NS | NA |
|
| NS | NA |
|
|
| Tumor
size, cm (≤5 vs. >5) | <0.001 | 0.046 | 1.607 | 1.008–2.563 | <0.001 | <0.001 | 3.020 | 1.796–5.078 |
| Tumor
thrombus (no vs. yes) | <0.001 | NS |
|
| <0.001 | NS |
|
|
|
Encapsulation (complete vs.
none) | NS | NA |
|
| NS | NA |
|
|
| Tumor
number (single vs. multiple) | 0.032 | NS |
|
| NS | NA |
|
|
| TNM
stage (I vs. II–III) | <0.001 | NS |
|
| <0.001 | NS |
|
|
| BCLC
stage (A vs. B-C) | <0.001 | NS |
|
| <0.001 | NS |
|
|
| EBI3
(low vs. high) | <0.001 | 0.013 | 0.634 | 0.446–0.901 | <0.001 | 0.001 | 0.452 | 0.290–0.704 |
In addition, because BCLC stage represented the
different stages of HCC progression, subgroup analysis was done for
a comprehensive knowledge about EBI3 function within different
stages. In early HCC (BCLC A stage), univairate analysis showed
that downregulated EBI3 was significantly associated with TTR
(P=0.003) and OS (P<0.001) (Fig.
2B). Multivariate analysis demonstrated that EBI3 was at high
risk of poor TTR (HR=0.553, P=0.007) and OS (HR=0.388, P=0.001)
(Table III).
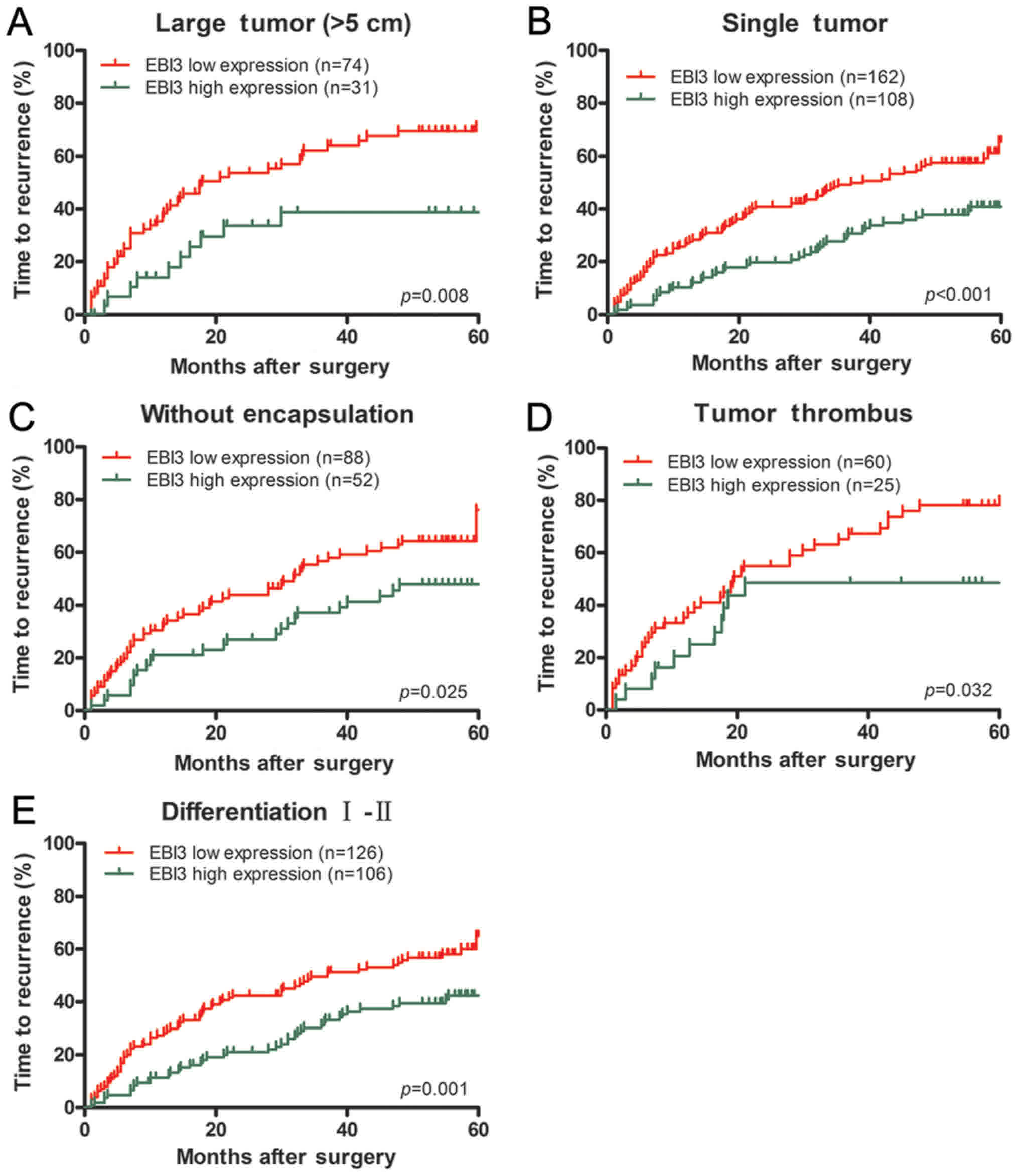
Furthermore, EBI3 downregulated expression had
prognostic values of TTR in the subgroup of HCC patients with large
tumor (>5 cm, P=0.008), single tumor (P<0.001), tumor
thrombus (P=0.032), tumor differentiation (I–II, P=0.001) or
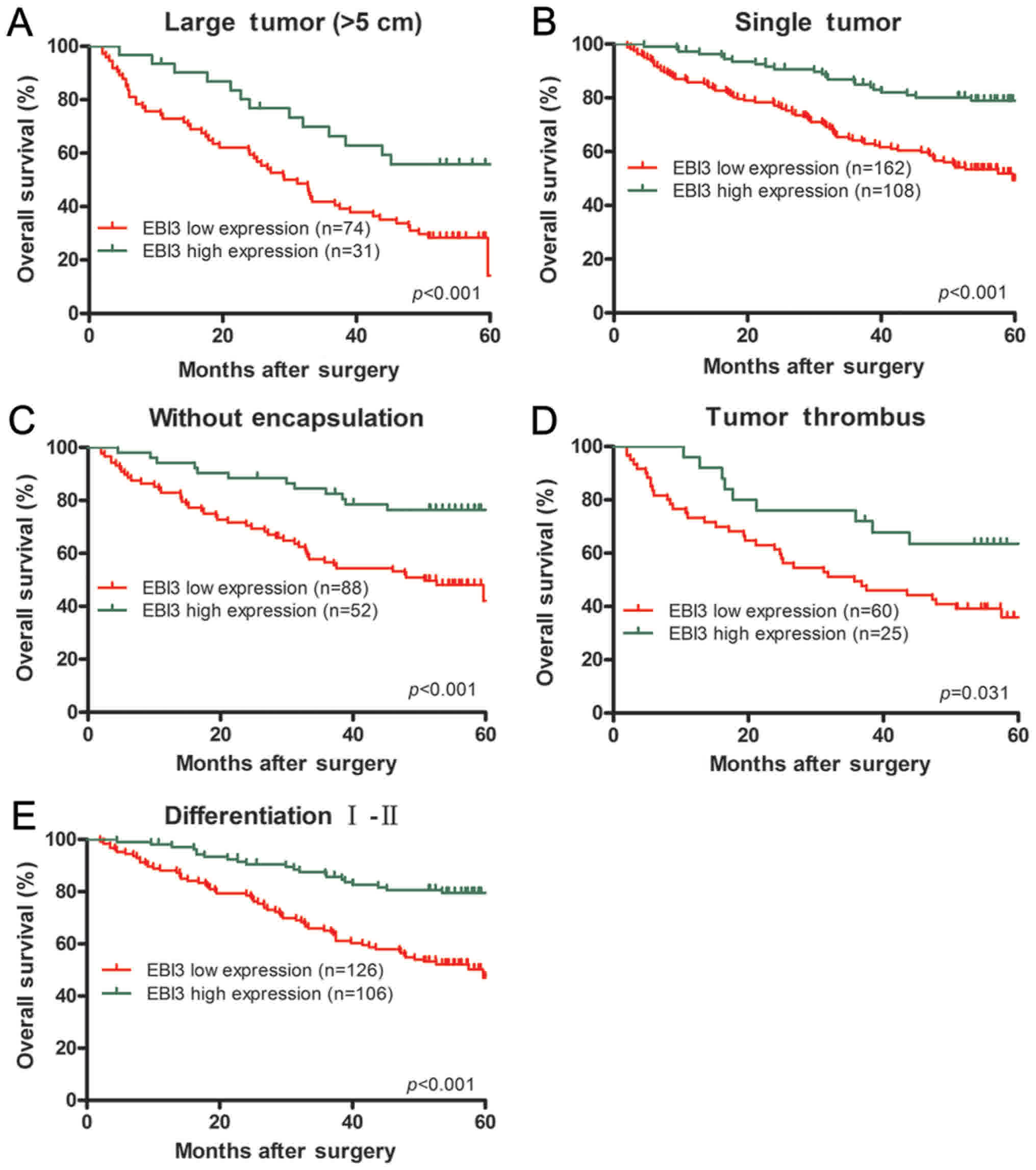
incomplete tumor encapsulation (P=0.025) (Fig. 3). Similarly, EBI3 could predict OS in
the subsets of HCC patients with large tumor (>5 cm;
P<0.001), single tumor (P<0.001), tumor thrombus (P=0.031),
tumor differentiation (I–II, P<0.001) or incomplete tumor
encapsulation (P<0.001) (Fig.
4).
Discussion
The results presented here demonstrated that EBI3
was a promising, independent predictor for survival and recurrence
in HCC patients. In the present study, we investigated the
expression of EBI3 in human HCC cell lines with low and high
metastatic potential as well as resected cancer specimens. And we
found that the patients with lower EBI3 expression had shorter
survival times and higher recurrence rates after curative
resection. In addition, tumor expression of EBI3 was an independent
prognostic parameter for survival and recurrence after
operation.
In the present study EBI3 downregulated expression
had close relationship with malignant tumor characteristics, like
tumor thrombus, poor differentiation and larger size. More
importantly, our results demonstrated that downregulation of EBI3
may represent an early event in HCC development. It is an obvious
advantage to predict the recurrence early for HCC patients after
resection for response to any treatment and therefore for clinical
outcome, particularly for HCC patients in early stage (21). For those in advanced stage, the
present vascular invasion and multinodularity has yet been adverse
predictors for prognosis established well after resection (22). Nevertheless, prognosis for HCC in
early stage is not homogenous at all, and is short of
clinicopathological indicators. For those early stage HCC (BCLC A
stage) patients, EBI3 revealed the ability in predicting the risk
of recurrence and patient survival. The independent prognostic
value of EBI3 in HCC patients with early stage is of clinical
importance. EBI3 low expression is related with pathogenesis of
HCC, and it may be an independent poor prognostic factor for HCC.
In this regard, EBI3 may be a cancer suppressor gene of HCC and a
potential molecular therapeutic target.
The reports of expression pattern and prognostic
information on EBI3 in cancers are few and inconsistent. Up to now,
it has been reported that immunoreactivity for EBI3 was
predominantly expressed in the cytoplasm of cervical cancer
(12), breast cancer (23) and lung cancer cells (10), and not in the nuclei of cancer and
stromal cells. Zhang et al (13) reported that EBI3 was also
over-expressed in the cytoplasm of the nasopharyngeal carcinoma
cells. Our findings are in consistent with these observations
previously reported. However, Wang et al (15) demonstrated that IL-35 was mainly
detected in the stromal cells with various shapes rather than in
nasopharyngeal carcinoma and skin melanoma cells. Thus, EBI3 may be
detected in various human cancer tissues and are likely of multiple
cellular sources. Moreover, high expression of EBI3 in many types
of human cancers has been shown to be associated with poor
prognosis. It was recently reported that the expression level of
IL-35 in HCC tissues is similar to paratumour tissues (17). And HCC patients with high intratumoral
IL-35 expression are related with significantly poorer
recurrence-free survival and OS than low IL-35 expression patients.
Furthermore, in multivariate analysis, IL-35 was found to be an
independent prognostic factor for recurrence-free survival but not
for OS. Interestingly, Long et al (18) found that the low expression of IL-35
in tumoral tissues seems contribute to the progression of HCC. And
they showed that expression levels of IL-35 are significantly
higher in the peri-tumoral tissue than the tumoral tissue.
Similarly, significantly lower level expression of IL-35 was
observed in HCC patients with larger tumor size, higher
histological grades, positively microvascular invasion and lymph
node. In the present study, we found that EBI3 expression was
predominantly downregulated in HCC tumor tissues in comparison to
peritumoral liver tissues, and low expression of EBI3 was related
with unfavorable TTR and OS in HCC patients. We also found that the
expression of IL-12p35, one of subunits of IL-35, is not been
detected in the HCC tissues. Although IL-12p35 positive expression
was associated with a worse survival in nasopharyngeal carcinoma,
multivariate analyses suggested EBI3 rather than IL-12p35 was an
independent prognostic marker (13).
We assumed that EBI3 may be as a main functional subunit and plays
a major role in IL-35, and has different impacts on prognosis based
on tumor type.
In spite of our findings, limitations of our
research need to be addressed. We lacked in vitro data to
verify our results and although we did examine the function of EBI3
in the HCC cell lines, further studies are necessary to investigate
the underlying mechanisms by which EBI3 influences the invasion and
metastasis of cancer cells.
Acknowledgements
The present study was funded by National Natural
Science Foundation of China (grant nos. 81572390 and 31300942),
Project of Nantong Science and Technology Bureau, Jiangsu Province,
China (grant no. MS22015116). The present study was supported by
the Clinical Biobank at Nantong University Affiliated Hospital in
Jiangsu, China.
References
|
1
|
Sun YF, Xu Y, Yang XR, Guo W, Zhang X, Qiu
SJ, Shi RY, Hu B, Zhou J and Fan J: Circulating stem cell-like
epithelial cell adhesion molecule-positive tumor cells indicate
poor prognosis of hepatocellular carcinoma after curative
resection. Hepatology. 57:1458–1468. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Chen R, Cui J, Xu C, Xue T, Guo K, Gao D,
Liu Y, Ye S and Ren Z: The significance of MMP-9 over MMP-2 in HCC
invasiveness and recurrence of hepatocellular carcinoma after
curative resection. Ann Surg Oncol. 19 Suppl 3:S375–S384. 2012.
View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Hanahan D and Weinberg RA: Hallmarks of
cancer: The next generation. Cell. 144:646–674. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Horlad H, Ma C, Yano H, Pan C, Ohnishi K,
Fujiwara Y, Endo S, Kikukawa Y, Okuno Y, Matsuoka M, et al: An
IL-27/Stat3 axis induces expression of programmed cell death 1
ligands (PD-L1/2) on infiltrating macrophages in lymphoma. Cancer
Sci. 107:1696–1704. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Collison LW, Delgoffe GM, Guy CS, Vignali
KM, Chaturvedi V, Fairweather D, Satoskar AR, Garcia KC, Hunter CA,
Drake CG, et al: The composition and signaling of the IL-35
receptor are unconventional. Nat Immunol. 13:290–299. 2012.
View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Vignali DA and Kuchroo VK: IL-12 family
cytokines: Immunological playmakers. Nat Immunol. 13:722–728. 2012.
View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Ma Y, Chen L, Xie G, Zhou Y, Yue C, Yuan
X, Zheng Y, Wang W, Deng L and Shen L: Elevated level of
interleukin-35 in colorectal cancer induces conversion of T cells
into iTr35 by activating STAT1/STAT3. Oncotarget. 7:73003–73015.
2016. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Olson BM, Jankowska-Gan E, Becker JT,
Vignali DA, Burlingham WJ and McNeel DG: Human prostate tumor
antigen-specific CD8+ regulatory T cells are inhibited by CTLA-4 or
IL-35 blockade. J Immunol. 189:5590–5601. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Liang Y, Chen Q, Du W, Chen C, Li F, Yang
J, Peng J, Kang D, Lin B, Chai X, et al: Epstein-Barr virus-induced
gene 3 (EBI3) blocking leads to induce antitumor cytotoxic T
lymphocyte response and suppress tumor growth in colorectal cancer
by bidirectional reciprocal-regulation STAT3 signaling pathway.
Mediators Inflamm. 2016:32141052016. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Nishino R, Takano A, Oshita H, Ishikawa N,
Akiyama H, Ito H, Nakayama H, Miyagi Y, Tsuchiya E, Kohno N, et al:
Identification of Epstein-Barr virus-induced gene 3 as a novel
serum and tissue biomarker and a therapeutic target for lung
cancer. Clin Cancer Res. 17:6272–6286. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Fan YG, Zhai JM, Wang W, Feng B, Yao GL,
An YH and Zeng C: IL-35 over-expression is associated with genesis
of gastric cancer. Asian Pac J Cancer Prev. 16:2845–2849. 2015.
View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Hou YM, Dong J, Liu MY and Yu S:
Expression of Epstein-Barr virus-induced gene 3 in cervical cancer:
Association with clinicopathological parameters and prognosis.
Oncol Lett. 11:330–334. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Zhang Y, Sun H, Wu H, Tan Q and Xiang K:
Interleukin 35 is an independent prognostic factor and a
therapeutic target for nasopharyngeal carcinoma. Contemp Oncol
(Pozn). 19:120–124. 2015.PubMed/NCBI
|
|
14
|
Jin P, Ren H, Sun W, Xin W, Zhang H and
Hao J: Circulating IL-35 in pancreatic ductal adenocarcinoma
patients. Hum Immunol. 75:29–33. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Wang Z, Liu JQ, Liu Z, Shen R, Zhang G, Xu
J, Basu S, Feng Y and Bai XF: Tumor-derived IL-35 promotes tumor
growth by enhancing myeloid cell accumulation and angiogenesis. J
Immunol. 190:2415–2423. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Zeng JC, Zhang Z, Li TY, Liang YF, Wang
HM, Bao JJ, Zhang JA, Wang WD, Xiang WY, Kong B, et al: Assessing
the role of IL-35 in colorectal cancer progression and prognosis.
Int J Clin Exp Pathol. 6:1806–1816. 2013.PubMed/NCBI
|
|
17
|
Fu YP, Yi Y, Cai XY, Sun J, Ni XC, He HW,
Wang JX, Lu ZF, Huang JL, Cao Y, et al: Overexpression of
interleukin-35 associates with hepatocellular carcinoma
aggressiveness and recurrence after curative resection. Br J
Cancer. 114:767–776. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Long J, Guo H, Cui S, Zhang H, Liu X, Li
D, Han Z, Xi L, Kou W, Xu J, et al: IL-35 expression in
hepatocellular carcinoma cells is associated with tumor
progression. Oncotarget. 7:45678–45686. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Wu H, Shi XL, Zhang HJ, Song QJ, Yang XB,
Hu WD, Mei GL, Chen X, Mao QS and Chen Z: Overexpression of
ST3Gal-I promotes migration and invasion of HCCLM3 in vitro and
poor prognosis in human hepatocellular carcinoma. Onco Targets
Ther. 9:2227–2236. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Huang J, Fan X, Wang X, Lu Y, Zhu H, Wang
W, Zhang S and Wang Z: High ROR2 expression in tumor cells and
stroma is correlated with poor prognosis in pancreatic ductal
adenocarcinoma. Sci Rep. 5:129912015. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Qi X, Jia J, Fan D and Han G: Brivanib for
hepatocellular carcinoma trials: Selection bias from barcelona
clinic liver cancer stage. J Clin Oncol. 32:9682014. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Lim KC, Wang VW, Siddiqui FJ, Shi L, Chan
ES, Oh HC, Tan SB and Chow PK: Cost-effectiveness analysis of liver
resection versus transplantation for early hepatocellular carcinoma
within the Milan criteria. Hepatology. 61:227–237. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Chen G, Liang Y, Guan X, Chen H, Liu Q,
Lin B, Chen C, Huang M, Chen J, Wu W, et al: Circulating low IL-23:
IL-35 cytokine ratio promotes progression associated with poor
prognosisin breast cancer. Am J Transl Res. 8:2255–2264.
2016.PubMed/NCBI
|