Introduction
Meningiomas, originating from arachnoid cells, are a
type of common intracranial tumor. They may be found at different
locations in brain, especially between the brain and the skull,
within ventricles, and along the spinal cord (1). These lesions can occur in people of any
age but commonly present among middle-aged individuals (2). Single and multiple occurrencesmay be
observed (3). The global incidence
rate is preceded only by glioma, occupying ~20% of intracranial
primary tumor types (4). It has been
demonstrated that ~7.61/100,000 population develop this type of
tumor, accounting for 36.1% of all intracranial tumor types; the
prevalence rate for meningiomas is 50.4/100,000, with a notable
increase in incidence rates in people aged >65 globally
(5). The primary clinical symptoms of
meningiomas are as follows: Headache; vomiting; epileptic seizure;
visual diminution; walking instability; and psychiatric symptoms
(6–9).
Furthermore, patients with psychiatric symptoms in meningiomas are
rare in clinical settings; most of them show hallucination,
delusion, analepsia, agitation, impulsive behavior and insomnia
(10). Some patients began with
psychiatric symptoms and underwent treatment in local psychiatric
hospitals; the head CT scan diagnosed the meningiomas in the end
due to poor therapeutic efficacy (11). A previous study hypothesized that the
psychiatric symptoms would disappear naturally once the occupying
lesions were removed (12); however,
others argued that alack of postoperative systemic antipsychotic
(SP) therapy would result in recurrent psychiatric symptoms
(13). In the present study, 42 cases
of patients with meningiomas and psychiatric symptoms were
collected, with 3 years of follow-up data. The effect of
postoperative SP therapy for 6 months on psychiatric recurrence was
observed.
Materials and methods
General information
The present study was a retrospective analysis
approved by the ethics committee and was conducted in accordance to
the relevant agreements with the Hunan Brain Hospital (Changsha,
China). A total of 42 cases of patients with meningiomas in Hunan
Brain Hospital from June 2005 to June 2013 were collected. The
patients' written informed consent permitted the publication of the
study results. All of the patients underwent computed tomography
(CT) scans in the patients' local hospital. At Hunan Brain
Hospital, the patients underwent 1.5 T enhanced magnetic resonance
imaging (MRI) scans and biopsy. The CT scan, enhanced MRI and
pathology data were used to confirm the diagnosis of meningioma.
All the cases, having complete clinical follow-up data, were in
accordance with the diagnostic criteria of International
Classification of Diseases-10 for ‘brain damage, dysfunction and
other mental disorders caused by somatic diseases’ (14). The patients were divided into two
groups. The first group was the SP group (n=20), undergoing 6
months of postoperative SP therapy. The other group was the none-SP
(NSP) group (n=22), who did not undergo postoperative antipsychotic
treatment. Tumors were classified according to the World Health
Organization (WHO) criteria for histological subtypes and tumor
grading (grade I–III) (15).
Hematoxylin and eosin (H&E)
staining and immunohistochemistry
Tumor specimens were fixed in 4% formalin for 12 h
at room temperature, followed by paraffin-embedded and cut into
slices. The thickness of the slices used for H&E staining and
immunohistochemistry was 2.5 µm. H&E staining was performed
using standard histological techniques at room temperature.
Sections were stained hematoxylin for 30 sec then rinsed in
H2O for 1 min. They were stained with 1% eosin Y
solution for 30 sec, and then dehydrated with a graded series of
alcohol (95, 95, 100 and 100%) for 30 sec each. The alcohol was
removed via washing with 95% xylene twice. A total of 1 or 2 drops
of neutral gum were added and the sections were covered with a
coverslip. The steps of immunohistochemistry were as follows:
Sections were immersed in hydrogen peroxide (0.3% in PBS) for 5 min
at room temperature, followed by incubation at room temperature for
2 h in solution with one of the following monoclonal rabbit
anti-rat antibodies (Quan Hui Co. Ltd, Guangzhou, China.): S-100
(dilution, 1:100; cat. no. 604660202); and CD34 (dilution, 1:100;
cat. no. 6052344101). Then samples were incubated for 30 min at
room temperature with the Poly-HRP Anti-Mouse/Rabbit IgG detection
kit (cat. no. WP140316; Zhongshan Golden Bridge Company, Beijing,
China.), according to the manufacturer's protocols, followed by
detection with a DAB Kit (cat. no. K145619C; Zhongshan Golden
Bridge Company, Beijing, China). Finally, sections were soaked in
95% xylene at room temperature for 2 min and sealed with neutral
gum. Sections were observed with a biological optical microscope
(Olympus Corporation, Tokyo, Japan) at ×100 magnification.
Treatment methods
All patients were treated with SP therapy prior to
surgery and craniotomy to remove the tumors in Hunan Brain
Hospital. Following surgical resection, 7 cases in the SP group and
9 cases in the NSP group received radiotherapy. Radiation doses
were 50–60 Gy, with 2 Gy per fraction, 5 fractions per week.
In the SP group, 10 cases were treated with
olanzapine 5–20 mg/day orally, 8 cases were administered quetiapine
fumarate 0.2–0.6 g/day orally and 2 cases were treated with
risperidone 3–5 mg/day orally. The SP therapy lasted for 6 months
following surgical resection. In the NSP group, 13 cases were
administered olanzapine 5–20 mg/day orally, 7 cases were treated
with quetiapine fumarate 0.2–0.6 g/day orally and 2 cases were
treated with risperidone 3–5 mg/day orally; however, all of them
reduced the dose or withdrew the antipsychotic drugs voluntarily.
Treatments varied according to the prescriptions of physicians.
Follow-up and effective rate
evaluation
All patients had complete follow-up records. They
were followed up at 6 months, 12 months and 3 years following
surgical resection. Psychiatric symptoms were evaluated via the
Positive and Negative Syndrome Scale (PANSS) (16) and Brief Psychiatric Rating Scale
(BPRS) (17) at 5 different time
points (prior to surgery, immediately following surgery, and 6
months, 12 months and 3 years following surgery). The evaluation
was assessed by two experienced physicians from Hunan Brain
Hospital who were blind to the treatment protocols. The effective
rate was assessed with BPRS. A reduction rate ≥75% represented
recovery, 50–74% represented significant progress, 25–49%
represented progress and <25% represented no progress. The
clinical criteria of recovery were as follows: Symptoms disappeared
completely; insight recovered; and social adaptability improved
notably, and that all of these lasted for ≥6 months.
Statistical analysis
Statistical analysis was performed with SPSS
(version 23.0; IBM Corp., Armonk, NY, USA). The quantitative data
are presented as mean ± standard deviation (SD), and the Student's
t-test was used for intergroup comparisons. The χ2 test
or Fisher's exact test were used for intergroup comparisons of
enumeration data, including: The recurrence rate at 6 months; and
the rehospitalization rate at 12 months. Kaplan-Meier survival
analysis with a log-rank test was used for recurrence and
rehospitalization. P<0.05 was considered to indicate a
statistically significant difference.
Results
General disease presentation
The SP group included 8 males and 12 females aged
16–52 years, and the mean ± SD patient age was 39.50±8.72 years.
The duration of disease ranged from 1–40 months, and the mean ± SD
duration was 18.35±12.87 months. The mean ± SD radiation doses were
54.13±3.76 Gy. The patients presented with different primary
symptoms, including: 7 cases of hallucination; 8 cases of delusion;
and 5 cases of impulsive and aggressive behavior. The NSP group
included 9 males and 13 females; aged 19–55 years, and the mean ±
SD patient age was 39.14±8.71 years. The duration of disease ranged
from 0.5–36 months, and the mean ± SD duration was 21.98±11.00
months. The mean ± SD radiation doses were 54.56±2.96 Gy. They
manifested different primary symptoms, including: 8 cases of
hallucination; 8 cases of delusion; and 6 cases of impulsive and
aggressive behavior. The aforementioned data had no statistical
significance (P>0.05). The radiation rate between the SP and NSP
groups had no statistical significance (P>0.05).
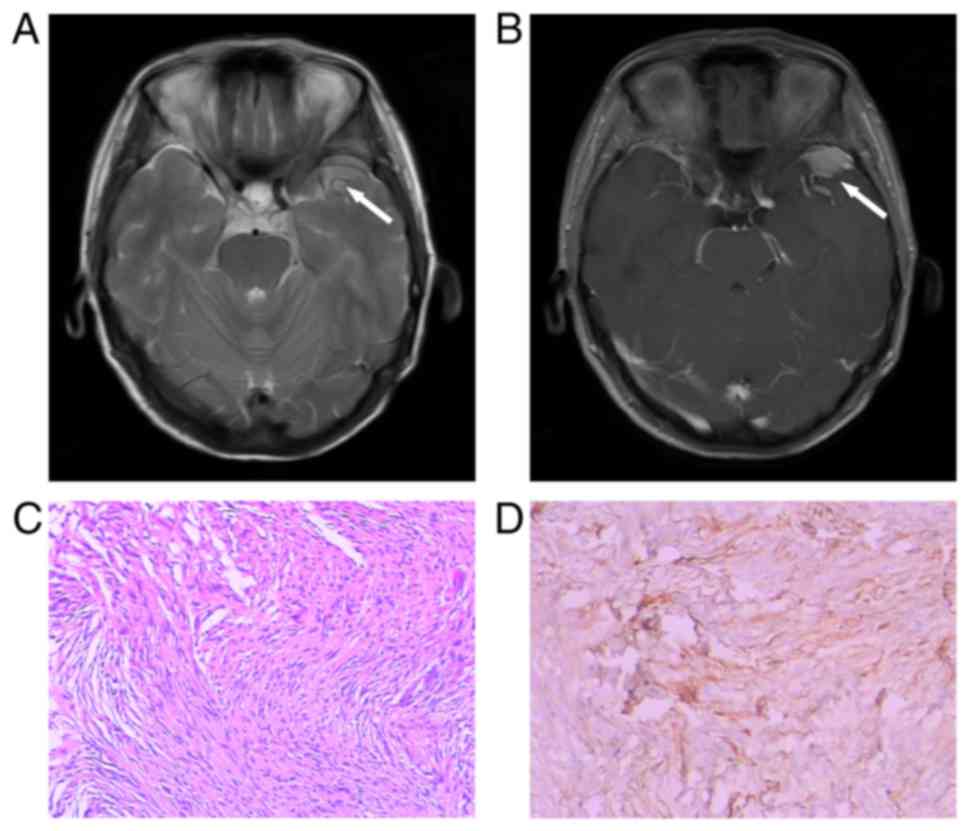
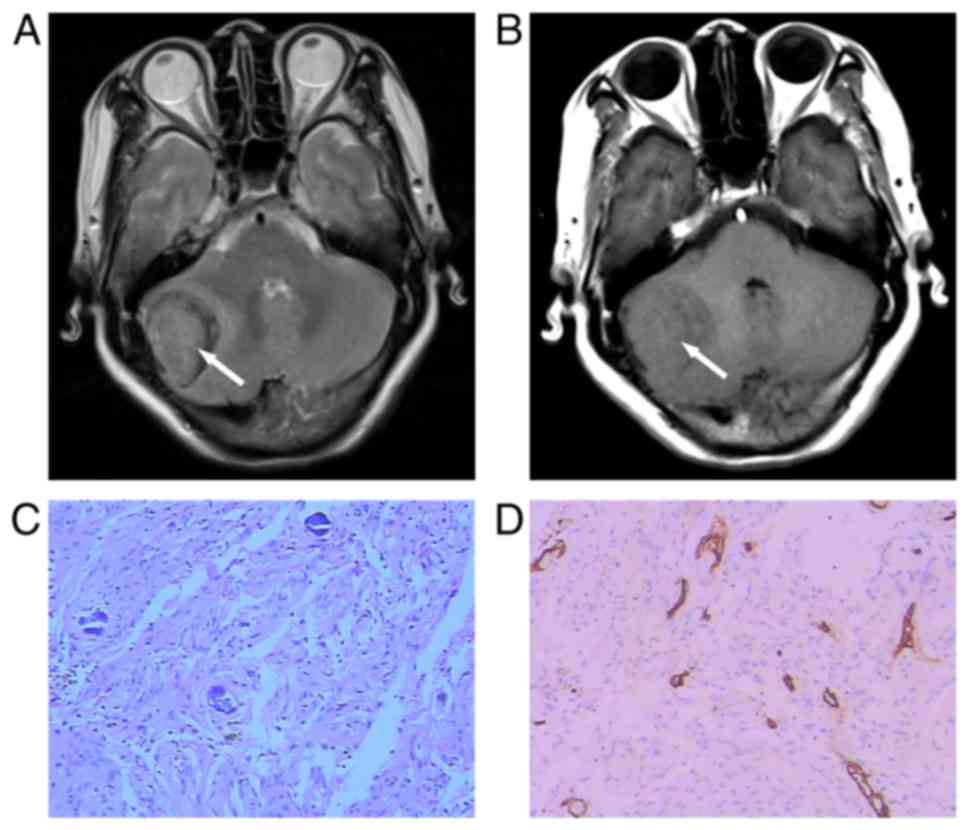
Lesions were located in different areas in the SP
group, including: 8 cases in the frontal lobe; 9 cases in the
temporal lobe; 1 case in the temporo-occipital area; 1 case near
the sagittal sinus in the parietal lobe; and 1 case in the
pontocerebellar peduncle. The mean ± SD diameter of the tumors was
3.85±0.55 cm. The NSP group included: 9 cases located in the
frontal lobe; 9 cases in the temporal lobe; 1 case in the
parieto-occipital area; 2 cases in the sphenoidal crest; and 1 case
in the posterior cranial fossa. The mean ± SD diameter of the
tumors was 4.13±0.54 cm. The postoperative pathology results
demonstrated that the SP group included 17 cases of WHO grade I (5
meningothelial type, 4 mixed type, 5 fibrous type and 3
psammomatous type) and 3 cases of WHO grade II (all atypical type).
The NSP group was composed of 18 cases of WHO grade I (4
meningothelial type, 5 mixed type, 5 fibrous type and 4
psammomatous type) and 4 cases of WHO grade II (atypical type). The
aforementioned data had no statistical significance (P>0.05;
Figs. 1 and 2).
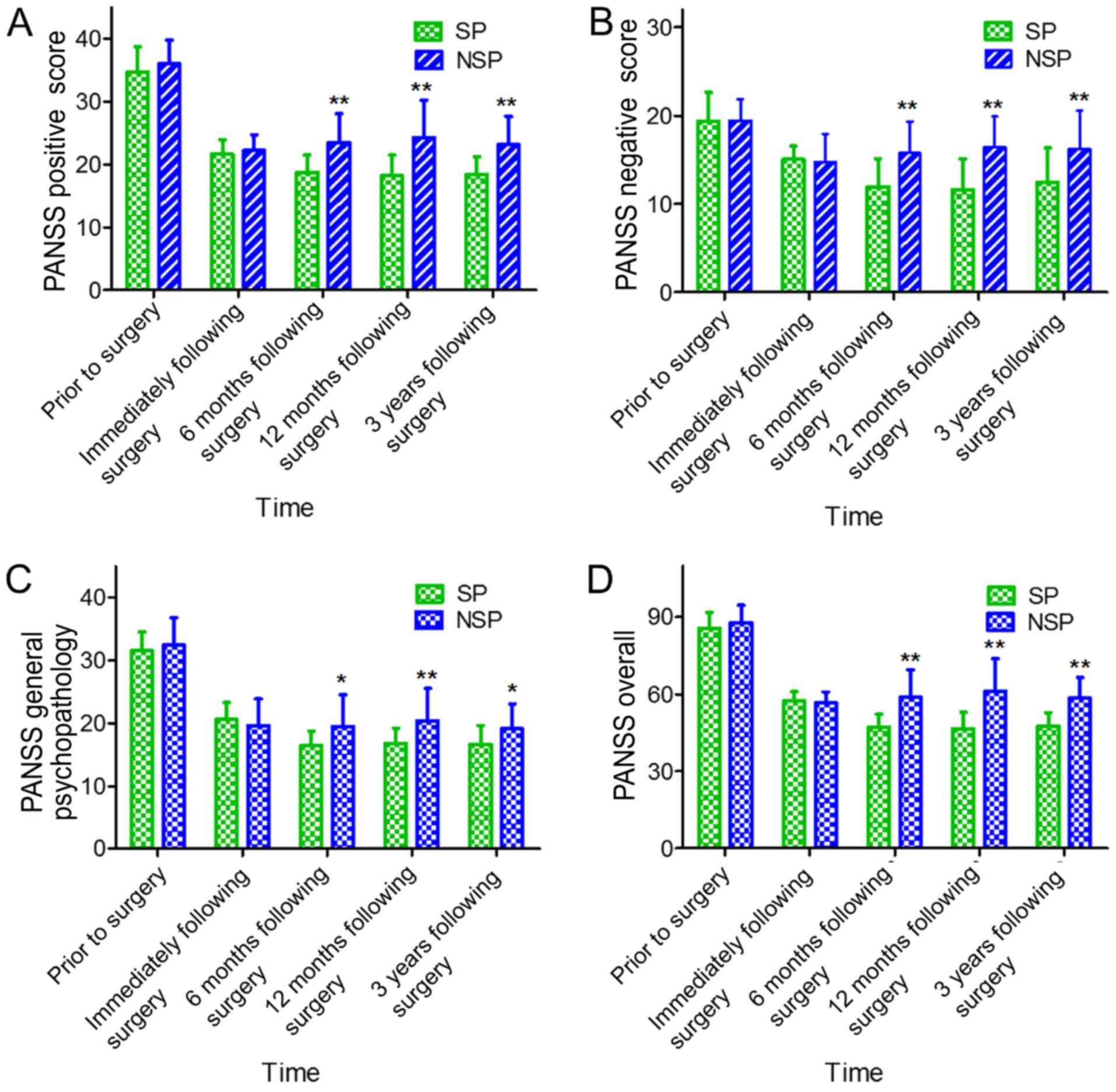
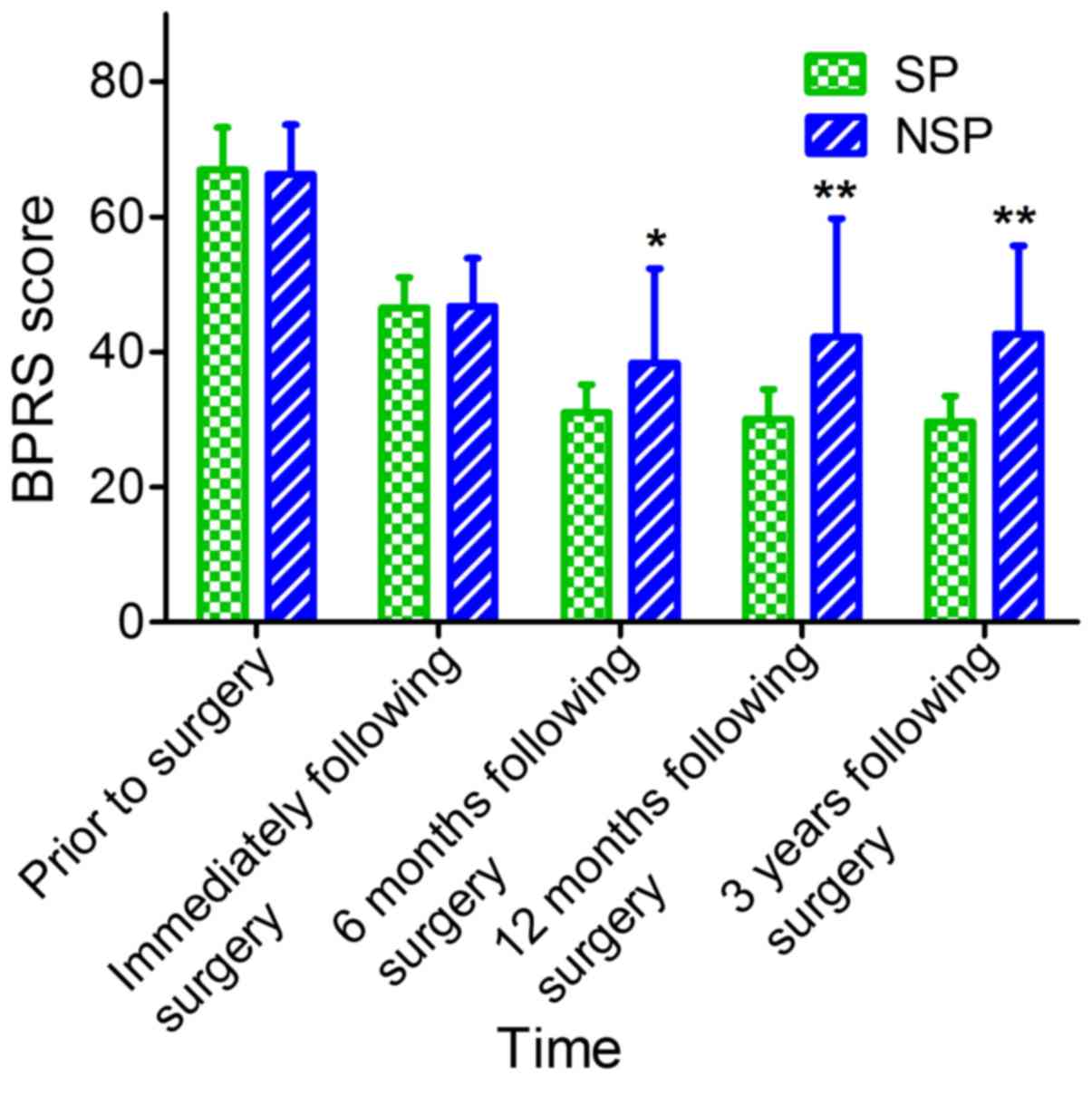
Comparison of PANSS and BPRS
There was no significant difference in PANSS and
BPRS between the two groups prior to and immediately following
surgical resection. The BPRS and PANSS scores (including PANSS
positive, PANSS negative, PANSS general psychopathology and PANSS
overall) in the SP group at 6 months, 12 months and 3 years were
significantly decreased compared with the NSP group (P<0.05;
Figs. 3 and 4).
Follow-up results
All patients were followed up at 6 months, 12 months
and 3 years. The effective rate was 95, 90 and 90% at 6 months, 12
months and 3 years, respectively, in the SP group, whilst it was
68.2, 63.6 and 59%, respectively, in the NSP group, which was
significantly different (χ2=4.89, χ2=4.01 and
χ2=5.12; P<0.05). The recurrence rate in the SP group
was 0, 5 and 10% at 6 months, 12 months and 3 years, respectively,
whilst in the NSP group it was 22.7, 31.8 and 54.5%, respectively,
which was statistically significant (χ2=5.16,
χ2=4.89 and χ2=9.34; P<0.05). The
rehospitalization rate of the SP group was 0, 0 and 5% at 6 months,
12 months and 3 years, respectively, whilst in the NSP group it was
13.6, 22.7 and 36.4%, respectively, and the data at 12 months and 3
years was statistically significant (χ2=5.16 and
χ2=6.12; P<0.05; Table
I).
 | Table I.Comparison of follow-up results. |
Table I.
Comparison of follow-up results.
| Group | Time following
surgery | n | Effective rate
(%) | Recurrence rate
(%) | Rehospitalization
rate (%) |
|---|
| SP | 6 months | 20 | 95.0 | 0.0 | 0.0 |
|
| 12 months | 20 | 90.0 | 5.0 | 0.0 |
|
| 3 years | 20 | 90.0 | 10.0 | 5.0 |
| NSP | 6 months | 22 | 68.2a | 22.7a | 13.6 |
|
| 12 months | 22 | 63.6a | 31.8a | 22.7a |
|
| 3 years | 22 | 59.0a | 54.5b | 36.4b |
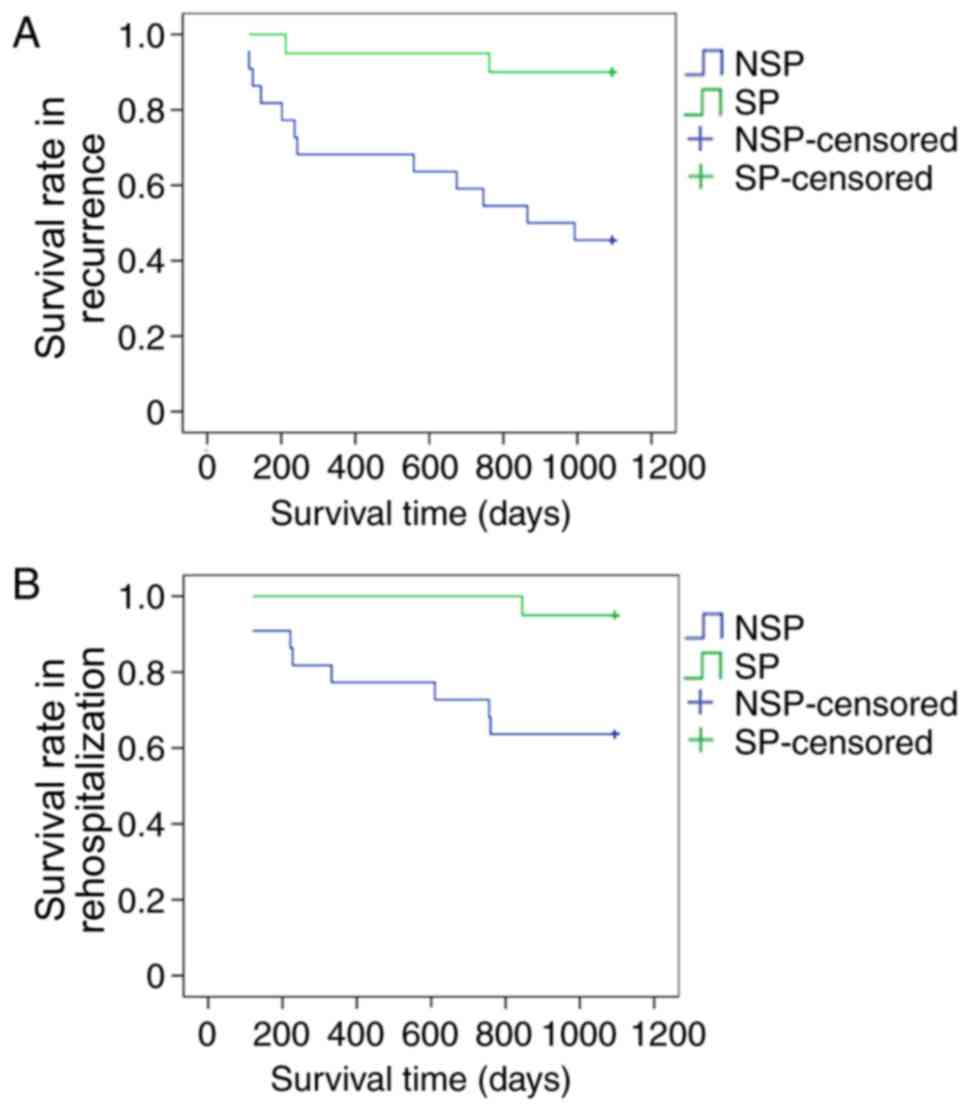
Kaplan-Meier survival analysis in
recurrence and rehospitalization
The accumulative survival rates of recurrence and
rehospitalization in the SP group were significantly improved
compared with the NSP group. The log-rank of recurrence was
χ2=9.369 (P=0.002) and the log-rank of rehospitalization
was χ2=6.330 (P=0.012; Fig.
5).
Discussion
The majority of meningiomas are benign tumors
(18). They grow slowly and the
disease course usually lasts for 2–4 years (19,20).
Detection is difficult at the early stages due to patients being
asymptomatic (21). It is only when
the activity of the nervous system becomes disrupted that the
serious clinical symptoms appear, thereby alerting clinicians
(22). The primary symptoms include:
Chronic headaches; hallucination; delusion; epilepsy; visual
diminution or loss; and impaired coordination (23–25).
Different locations of the meningiomas indicate various clinical
manifestations (26), and it has been
demonstrated that the incidence of patients with meningiomas and
psychiatric symptoms is rare (27,28). In
the present study, 30 of all 42 patients had a history of treatment
in other hospitals. Among them, 9 patients were diagnosed with
mental disorders at local hospitals for initial psychiatric
symptoms, and were treated with antipsychotics only. The diagnosis
of the meningiomas and treatment were delayed until serious
clinical symptoms emerged, which then resulted in additional
examination and eventual disease confirmation.
In the present study, there were 35 patients, in
which the meningiomas located in the frontal and temporal lobes
were present in 83.3% of all 42 patients. It has been determined
that the primary symptoms of frontotemporal tumors include:
Hallucination; delusion; impulsive aggressive behaviors; and
cognitive handicap (29–31), and it was considered that these mental
symptoms were closely associated with the location of the occupying
lesions (32). The treatment of
patients with meningiomas and psychiatric symptoms in neurosurgery
is difficult, for example, there were 10 patients in the present
study who could not undergo the surgical resection because of the
repeated symptoms of agitation and aggressive behavior; therefore,
doctors had to control their symptoms with the administration of
psychiatric treatment followed by the operation. Accompanied by the
improved mental symptoms, a debate exists between neurosurgeons and
psychiatrists concerning the application of antipsychotic drugs in
patients with meningiomas. The majority of the neurosurgeons
believe patients can withdraw the antipsychotic drugs immediately
following surgery. While in clinic, this could result in severe
mental symptoms and/or recurrent attacks which reduce the quality
of life (13).
At present, there are no studies focusing on the
duration of postoperative SP therapy for patients with meningiomas
and psychiatric symptoms. A number of previous studies have
suggested that antipsychotic drugs maybe gradually reduced until
withdrawal, following the slow improvement of psychiatric symptoms
(33,34). However, in a clinical setting, it was
determined that the withdrawal of antipsychotic drugs following
surgical resection may result in the recurrence of psychiatric
symptoms; subsequently, the patients would have to receive the
antipsychotic treatment again, which may be associated with local
metabolic imbalances caused by the pace-occupying lesions (35).
Therefore, the present study retrospectively
analyzed the patients with meningiomas and psychiatric symptoms
treated at Hunan Brain Hospital. All the patients were divided into
SP and NSP groups according to their treatment, and follow-up was
conducted for 3 years. The psychiatric symptoms were compared using
the PANSS, BPRS, effective rate, recurrence rate and
rehospitalization rate between these two groups.
All of the patients received tumorectomy, and 16 of
42 patients were treated with radiotherapy. The expression of S-100
or CD34 in the tumors was detected with immunohistochemistry. In
the present study, as the focus was not on the diagnosis of
meningioma but on the postoperative SP therapy, the
immunohistochemistry results were used to confirm the diagnosis of
meningioma and not for statistical analysis. Furthermore, the
patients failed to be analyzed for relevant biochemical indices,
including NSE, S-100 and CEA, due to funding limitations. This was
a limitation of the present study. Despite this, the results of the
CT and enhanced MRI scans and pathology data confirmed the
diagnosis of meningioma. It was determined that the BPRS score and
PANSS scores (including PANSS positive, PANSS negative, PANSS
general psychopathology and PANSS overall) in the SP group at 6
months, 12 months and 3 years were significantly decreased compared
with the NSP group, all of which were statistically significant.
The follow-up results demonstrated that the effective rate was
significantly increased, whilst the recurrence and
rehospitalization rates were significantly decreased in the SP
group, compared with the NSP group at 6 months, 12 months and 3
years. The Kaplan-Meier survival analysis demonstrated that the
accumulative survival rates of recurrence and rehospitalization in
the SP group were improved compared with the NSP group.
Postoperative SP therapy is of great importance to the
consolidation of mental symptoms in patients with meningiomas and
psychiatric symptoms, and it may significantly reduce the
recurrence and rehospitalization rates.
The results of the present study demonstrated that
postoperative SP therapy for 6 months is necessary for the
prevention of recurrence and reducing the rehospitalization rate in
patients with meningiomas and psychiatric symptoms. Additional
studies with Magnetic Resonance Spectrum Imaging of space-occupying
lesions are required, which would subsequently clarify whether the
psychiatric symptoms are associated with nervous metabolic
abnormalities following surgical resection.
Acknowledgements
Not applicable.
Funding
This work was supported by grants from the National
Natural Science Foundation of China (grant nos. 81603512 and
81373551) and the Science & Research Project of Hunan
Provincial Education Department (grant no. 15C1051).
Availability of data and materials
The datasets used and/or analyzed during the current
study are available from the corresponding author on reasonable
request.
Authors' contributions
LL and HYH designed the study. PY and MSL performed
the experiments. BZ participated in study design and data
collection. WPK was in charge of statistical analysis. PY wrote the
manuscript and LL revised the manuscript.
Ethics approval and consent to
participate
This present study was approved by the ethics
committee and was conducted in accordance with the relevant
agreements of the Hunan Brain Hospital (Changsha, China, No
2012–8). Written informed consent was obtained from all
participants prior to their inclusion within the study.
Consent for publication
The patients' written informed consent permitted the
publication of the study results. Identifying information about the
patients has been removed.
Competing interests
The authors declare that they have no competing
interests.
Glossary
Abbreviations
Abbreviations:
|
SP
|
systemic antipsychotic
|
|
NSP
|
none-systemic antipsychotics
|
|
PANSS
|
positive and negative syndrome
scale
|
|
BPRS
|
brief psychiatric rating scale
|
|
WHO
|
world health organization
|
References
|
1
|
Shintaku M, Hashimoto K and Okamoto S:
Intraventricular meningioma with anaplastic transformation and
metastasis via the cerebrospinal fluid. Neuropathology. 27:448–452.
2007. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Saha R, Jakhar K and Kumar R: Sphenoid
wing meningioma presenting as cognitive impairment. Shanghai Arch
Psychiatry. 28:173–176. 2016.PubMed/NCBI
|
|
3
|
Terrier LM and François P: Multiple
meningiomas. Neurochirurgie. 62:128–135. 2016.(In French).
View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Hwang WL, Marciscano AE, Niemierko A, Kim
DW, Stemmer-Rachamimov AO, Curry WT, Barker FG II, Martuza RL,
Loeffler JS, Oh KS, et al: Imaging and extent of surgical resection
predict risk of meningioma recurrence better than WHO
histopathological grade. Neuro Oncol. 18:863–872. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Silva CB, Ongaratti BR, Trott G, Haag T,
Ferreira NP, Leaes CG, Pereira-Lima JF and Oliveira Mda C:
Expression of somatostatin receptors (SSTR1-SSTR5) in meningiomas
and its clinicopathological significance. Int J Clin Exp Pathol.
8:13185–13192. 2015.PubMed/NCBI
|
|
6
|
Aizer AA, Bi WL, Kandola MS, Lee EQ, Nayak
L, Rinne ML, Norden AD, Beroukhim R, Reardon DA, Wen PY, et al:
Extent of resection and overall survival for patients with atypical
and malignant meningioma. Cancer. 121:4376–4381. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Deng WS, Zhou XY, Li ZJ, Xie HW, Fan MC
and Sun P: Microsurgical treatment for central gyrus region
meningioma with epilepsy as primary symptom. J Craniofac Surg.
25:1773–1775. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Wang DJ, Xie Q, Gong Y, Wang Y, Cheng HX,
Mao Y, Zhong P, Huang FP, Zheng K, Wang YF, et al: Secretory
meningiomas: Clinical, radiological and pathological findings in 70
consecutive cases at one institution. Int J Clin Exp Pathol.
6:358–374. 2013.PubMed/NCBI
|
|
9
|
Xu P, Luo H, Huang GL, Yin XH, Luo SY and
Song JK: Exposure to ionizing radiation during dental X-rays is not
associated with risk of developing meningioma: A meta-analysis
based on seven case-control studies. PLoS One. 10:e01132102015.
View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Tringale KR, Wilson BR, Hirshman B, Zhou
T, Folsom D, Norman MA, Grant I, Chen CC and Carter BS: Psychiatric
disease preceding intracranial tumor diagnosis: Investigating the
association. Prim Care Companion CNS Disord. 18:2016. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Wang RT: Meningiomas begin with
psychiatric symptoms: A case report. Chin Med Herald. 7:1042010.(In
Chinese).
|
|
12
|
Yakhmi S, Sidhu BS, Kaur J and Kaur A:
Diagnosis of frontal meningioma presenting with psychiatric
symptoms. Indian J Psychiatry. 57:91–93. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Zhou B, Kuang WP, Huang HX, Li B, Zhu Y,
Chen XF, Yan L and Yang P: Clinical research to the Meningioma
patients with psychiatric symptoms in 16 cases. Chin J Clin
Neurosci. 24:553–556. 2016.(In Chinese).
|
|
14
|
World Health Organization: The ICD-10
classification of mental and behavioural disorders: Clinical
descriptions and diagnostic guidelines. Geneva; 1992
|
|
15
|
Louis DN, Ohgaki H, Wiestler OD and
Cavenee WK: WHO classification of tumours of the central nervous
system. IARC Press; Lyon; 2007
|
|
16
|
Horga G, Cassidy CM, Xu X, Moore H,
Slifstein M, van Snellenberg JX and Abi-Dargham A: Dopamine-related
disruption of functional topography of striatal connections in
unmedicated patients with schizophrenia. JAMA Psychiatry.
73:862–870. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Lee SH, Niznikiewicz M, Asami T, Otsuka T,
Salisbury DF, Shenton ME and McCarley RW: Initial and progressive
gray matter abnormalities in insular gyrus and temporal pole in
First-episode schizophrenia contrasted with First-episode affective
psychosis. Schizophr Bull. 42:790–801. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Murnyák B, Csonka T and Hortobágyi T:
Molecular pathology of meningiomas. Ideggyogy Sz. 68:292–300.
2015.(In Hungarian). View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Du Z, Abedalthagafi M, Aizer AA, McHenry
AR, Sun HH, Bray MA, Viramontes O, Machaidze R, Brastianos PK,
Reardon DA, et al: Increased expression of the immune modulatory
molecule PD-L1 (CD274) in anaplastic meningioma. Oncotarget.
6:4704–4716. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Tang H, Gong Y, Mao Y, Xie Q, Zheng M,
Wang D, Zhu H, Wang X, Chen H, Chen X and Zhou L: CD133-positive
cells might be responsible for efficient proliferation of human
meningioma cells. Int J Mol Sci. 13:6424–6439. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Jurinovic P, Bulicic AR, Marcic M, Mise
NI, Titlic M and Suljic E: Foramen magnum meningioma: A case report
and review of literature. Acta Inform Med. 24:74–77. 2016.
View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Guo XB and Wang ZM: Mental disorder due to
meningiomas: A case report. J Clin Psychiatry. 17:273. 2007.(In
Chinese).
|
|
23
|
Serna E, Morales JM, Mata M,
Gonzalez-Darder J, San Miguel T, Gil-Benso R, Lopez-Gines C,
Cerda-Nicolas M and Monleon D: Gene expression profiles of
metabolic aggressiveness and tumor recurrence in benign meningioma.
PLoS One. 8:e672912013. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Oyama H, Kito A, Maki H, Hattori K, Noda T
and Wada K: Postoperative recovery from unilateral blindness caused
by tuberculum sellae meningioma. Nagoya J Med Sci. 74:181–187.
2012.PubMed/NCBI
|
|
25
|
Jung HW, Lee HC, Kim JH, Jang HM, Moon JH,
Sur JH, Ha J and Jung DI: Imatinib mesylate plus hydroxyurea
chemotherapy for cerebellar meningioma in a Belgian Malinois dog. J
Vet Med Sci. 76:1545–1548. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Wiemels J, Wrensch M and Claus EB:
Epidemiology and etiology of meningioma. J Neurooncol. 99:307–314.
2010. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Madhusoodanan S, Ting MB, Farah T and Ugur
U: Psychiatric aspects of brain tumors: A review. World J
Psychiatry. 5:273–285. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Madhusoodanan S, Patel S, Reinharth J,
Hines A and Serper M: Meningioma and psychiatric symptoms: A case
report and brief review. Ann Clin Psychiatry. 27:126–133.
2015.PubMed/NCBI
|
|
29
|
Cipolotti L, Healy C, Chan E, Bolsover F,
Lecce F, White M, Spano B, Shallice T and Bozzali M: The impact of
different aetiologies on the cognitive performance of frontal
patients. Neuropsychologia. 68:21–30. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
30
|
James AI, Bohnke JR, Young AW and Lewis
GJ: Modelling verbal aggression, physical aggression and
inappropriate sexual behaviour after acquired brain injury. Proc
Biol Sci:. 282:201507112015. View Article : Google Scholar
|
|
31
|
Yu G, Bao WM, Mao Y, Guo QH, Xie R, Shen
C, Gao C and Ji YD: Study of executive functions of patients with
tumor in both right and left frontal lobe. Chin J Clin Neurosci.
18:54–57. 2010.(In Chinese).
|
|
32
|
Lehmann G, Bremond J, Rabaud C and Paillas
JE: Space-occupying lesions of the occupital lobe of the cerebral
cortex. Neurochirurgie. 21:55–79. 1975.(In French). PubMed/NCBI
|
|
33
|
Wei YH and Pan RD: Clinical analysis to
viral encephalitis with initial psychiatric symptoms in 95 cases.
Chin J Nerv Ment Dis. 33:45–47. 2007.(In Chinese).
|
|
34
|
Więdłocha M, Marcinowicz P and
Stanczykiewicz B: Psychiatric aspects of herpes simplex
encephalitis, tick-borne encephalitis and herpes zoster
encephalitis among immunocompetent patients. Adv Clin Exp Med.
24:361–371. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
35
|
Zhao HH, You NX, Yan YX, Di LB and Guan
YR: Effect of olanzapine to mental disorders caused by organic and
somatic diseases. Chin J Psychiatry. 34:2252001.(In Chinese).
|