Introduction
Clinical and epidemiological studies have
established that infections by certain human papillomavirus (HPV)
types are associated with the development of cervical cancer and
its precursor lesions (1–4). The marked geographic differences in the
incidence of cervical cancer are not only the result of differences
in screening patterns to detect and treat precursor lesions, but
also due to differences in exposure to various risk factors.
Different HPV genotypes, including variant presence, genetic
alterations, host factors and environmental factors are involved in
the pathways underlying cervical carcinogenesis (5–8). A
persistent infection with carcinogenic types of HPV is a pivotal
event in the incidence of cervical cancer. However, few long-term
studies following persistent HPV infections and quantifying risk
have been performed (9).
In Colombia, the incidence of cervical cancer is
relatively high at 26.1/100,000, and it is the principal cause of
cancer-associated mortality among women (10). In this country, a prospective cohort
study was initiated in the early 1990s by the Colombian National
Institute of Cancer (Bogotá, Colombia) and the International Agency
for Research on Cancer (IARC; Lyon, France). The aim of the study
was to investigate the natural history of HPV infections and
cervical intraepithelial neoplasia (CIN) lesions among low-income
Colombian women (the Bogotá cohort); however, viral factors
including variant presence were not studied (11–13).
HPV type 58 (HPV58) is the second most prevalent
viral type (6.2%) and has the second highest rate of incident
infection (11.2%) in women with normal cytology from the Colombian
population (11,12). The relative contribution of HPV58 to
invasive cervical cancer and CIN 3 lesions worldwide is 2.3 and
9.0%, respectively (14), and certain
variants of HPV58 have been reported to have an increased risk of
development of high grade squamous intraepithelial lesions (HGSIL)
and cervical cancer in certain populations (15–17). In
South America there are few studies investigating HPV58 molecular
variants, and worldwide there are no follow-up studies analyzing
their involvement in the persistence and clearance of HPV58
incident infections in women with normal cytology. The present
study focuses on this analysis, and also provides information
concerning the function of other risk factors in the clearance of
HPV58 infections and whether the HPV58 infection-associated risk of
developing CIN 2,3 differs by variant. The aim of the present study
was to evaluate the presence and persistence of incident HPV58
E6/E7 variants during a long follow-up period in Colombian women
with normal baseline cytology, and then analyze variant status and
other risk factors associated with clearance of HPV58
infections.
Materials and methods
Study population
Between November 1993 and November 1995 a total of
2,200 sexually active women, 13–85 years old, who presented to
cervical cancer screening centres and family-planning clinics in
low socioeconomic settings in Bogotá, Colombia, were invited to
participate in a prospective study of cervical HPV infection
(11). Methods of recruitment and
data collection have been described previously (11,12). The
ethical committees of the National Cancer Institute and the IARC
approved the study protocol. A total of 1,610 women who were
HPV-negative and had normal cytology at base line were included in
the analysis of HPV incidence.
The analysis described in the present study was
performed in a subset of the study cohort of 71 women with incident
HPV58 infections, together with their respective longitudinal
follow-up every 6–9 months. A total of 639 samples were available
for analysis over 7 years.
Biological specimens
The cell pellets used in the present study were
obtained from women who were HPV58 positive, and were suspended in
1 ml Tris-HCl buffer (10 mM; pH 8.3) and stored at−70°C. For
analysis, 100 µl aliquots were boiled for 10 min at 100°C, cooled
on ice and centrifuged for 1 min at 3,000 × g at 4°C. A total of 10
µl of these pre-treated crude cell suspensions were used for
polymerase chain reaction (PCR) analysis. To assess the quality of
the target DNA, a 209 base pair amplifying β-globin PCR was
performed using the primer combination BGPCO3 and BGPCO5, as
described previously (18).
E6 and E7 HPV58 PCR amplification
The E6 and E7 regions of HPV58 positive samples were
amplified using E6 forward, (5′-CAGACATTTTTTGGTAGGCTA-3′); E7
reverse 1, (5′-TCTTAGCGTTGGGTTGTT-3′); E7 forward 1,
(5′-CTGTAACAACGCCATGAGAG-3′); and E7 reverse 2,
(5′-TCAGGGTCATCCATTGCAGA-3′) primers, which amplify fragments of
521 and 335 bp, respectively. The PCR amplifications were performed
in a final volume of 50 µl containing 10 mM Tris HCl, 2.5 mM
MgCl2, 0.2 mM of each dNTP, 25 pmol of each primer
(Integrated DNA Technologies, Inc., Coralville, IA, USA) 1.25 U Taq
polymerase (Amplitaq; Cetus; PerkinElmer, Inc., Waltham, MA, USA)
and 10 µl isolated nucleic acid. The optimal amplification
conditions for the PCR were as follows: Denaturation for 4 min at
94°C followed by 40 cycles of amplification. Each cycle consisted
of 1 min at 94°C, 1 min at 50°C and 1.5 min at 72°C. The final
elongation step was extended for a further 10 min. The amplified
DNA was analysed by 1.5% agarose gel electrophoresis and ethidium
bromide staining (0.5 µg/ml) and viewed with the Gel Doc XR Gel
Documentation System (Image Lab™ software; Bio-Rad Laboratories,
Inc., Hercules, CA, USA).
Negative controls, with PCR mix and water, and
positive controls with 100 fg and 1 pg cloned HPV58 DNA in a
background of 100 ng human placental DNA were included in each
experiment. These controls were obtained from the World Health
Organisation HPV DNA proficiency panel [HPV LabNet Global Reference
Laboratory (GRL), Sweden].
E6 and E7 HPV58 sequence analysis
The E6 and E7 HPV58 amplicons were purified using
the commercial GFX PCR kit (GE Healthcare, Chicago, IL, USA)
according the manufacturer's protocol. Cycle sequencing was
performed using the 7-Deaza-dGTP-Cy5.5 Dye Primer Cycle Sequencing
kit (Visible Genetics, Inc., Toronto, Canada) according to the
manufacturer's protocol, and was run on an automated DNA sequencer
(SEQ 4×4; GE Healthcare). For the sequencing reaction, the same
primers were used as for the PCR. Sequences of sense, antisense and
combined strands of the PCR products were generated. The sequences
were analyzed using the Basic Local Alignment Search Tool function
(BLAST + 2.2.28; National Center for Biotechnology Information;
U.S. National Library of Medicine, Bethesda, MD, USA), and variants
were interpreted visually in comparison with the HPV58R prototype
sequence (GenBank no. D90400.1) (19).
Statistical methods
Frequencies and percentages were used to analyse
HPV58 E6/E7 variants presence and viral load. An incident HPV58
infection was defined as the first positive type-specific result
following a negative result for the same type of HPV.
Correspondingly, type-specific HPV58 clearance was defined as the
first negative PCR result following an incident HPV58 infection.
Duration of an HPV58 incident infection was defined as the elapsed
time from the date of infection to the date of clearance. The
survival function, which describes the probability that an HPV
infection has cleared as a function of time, was estimated using
Kaplan-Meier analysis of interval-censored data, followed by the
log rank test. Cox regression analysis was performed to estimate
the age-adjusted hazard ratios (HRs) and 95% confidence intervals
(CIs) on clearance of HPV58 infection according to different risk
factors. All analyses were performed using SPSS software (version
17; SPSS Inc., Chicago, IL, USA). P<0.05 was considered to
indicate a statistically significant difference..
Results
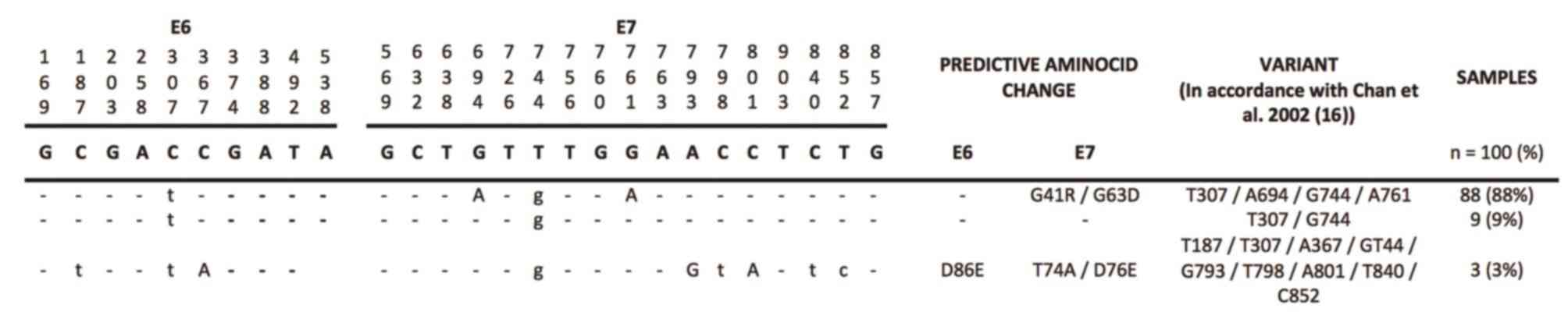
Frequency of HPV58 E6/E7 variants in
women with incident HPV58 infections
A total of 71 women had incident HPV58 infections
during the follow-up period. The median age of the women was 33.6
years (range, 16–67.72). The follow-up period lasted between 1 and
7 years, with a total of 2–12 visits (average, 8.72 visits). Of a
total of 639 cervical scrapes obtained during follow-up, 117
samples were HPV58-positive. However, variants were identified in
100 samples (85.5%). Three different variants were identified: 88%
of the samples were positive for the T307/A694/G744/A761 variant,
9% were positive for the T307/G744 variant and 3% were positive for
the T187/T307/A367/G744/G793/T798/A801/T840/C852 variant. None of
the samples were infected with multiple variants or the reference
sequence of HPV58. The E6 and E7/HPV58 sequence variants detected
during follow-up in women with incident HPV58 infections are
presented in Fig. 1.
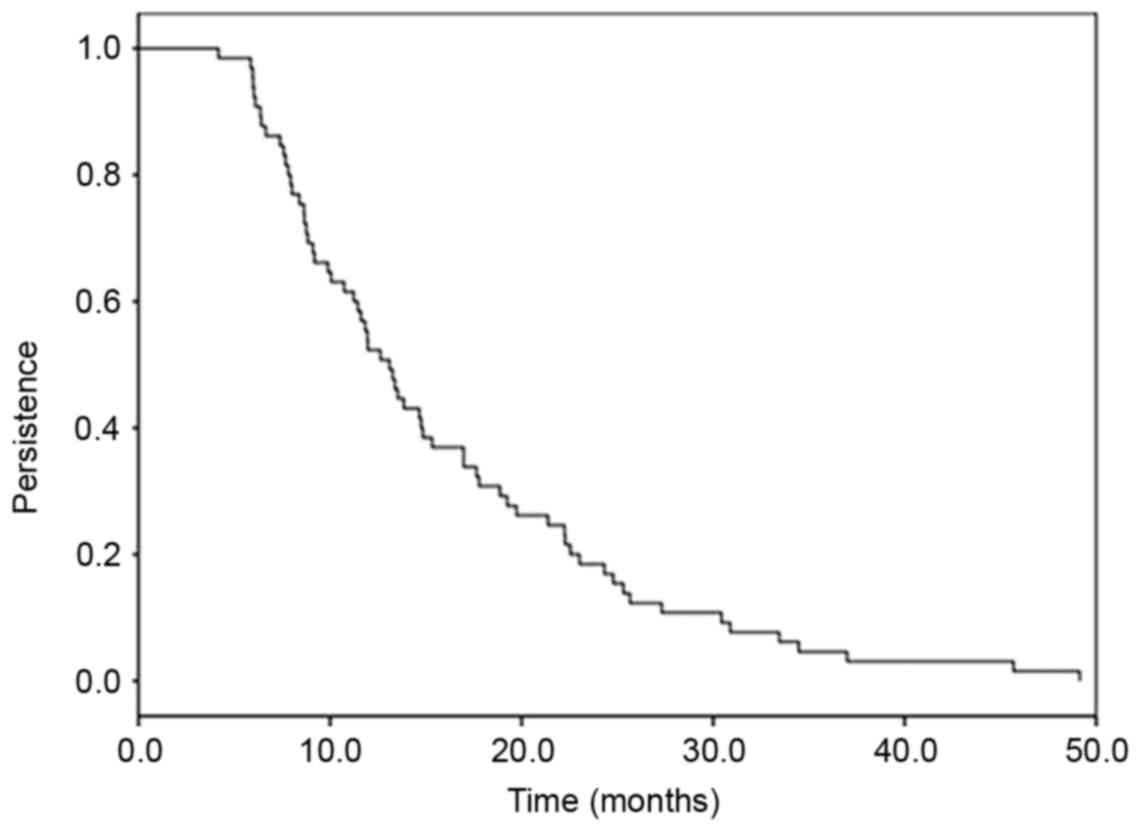
Clearance of incident HPV58
infections
From the 71 women who had incident HPV58 infections,
50 (70.4%) were transient, whilst 21 (29.6%) were persistent at
more than one visit. The persistence of HPV58 infections as a
function of time is presented in Fig.
2. Overall, 50% of HPV58 infections were still present at 1
year of follow-up, 15% at 2 years, 3% at 4 years and 0% at 7 years
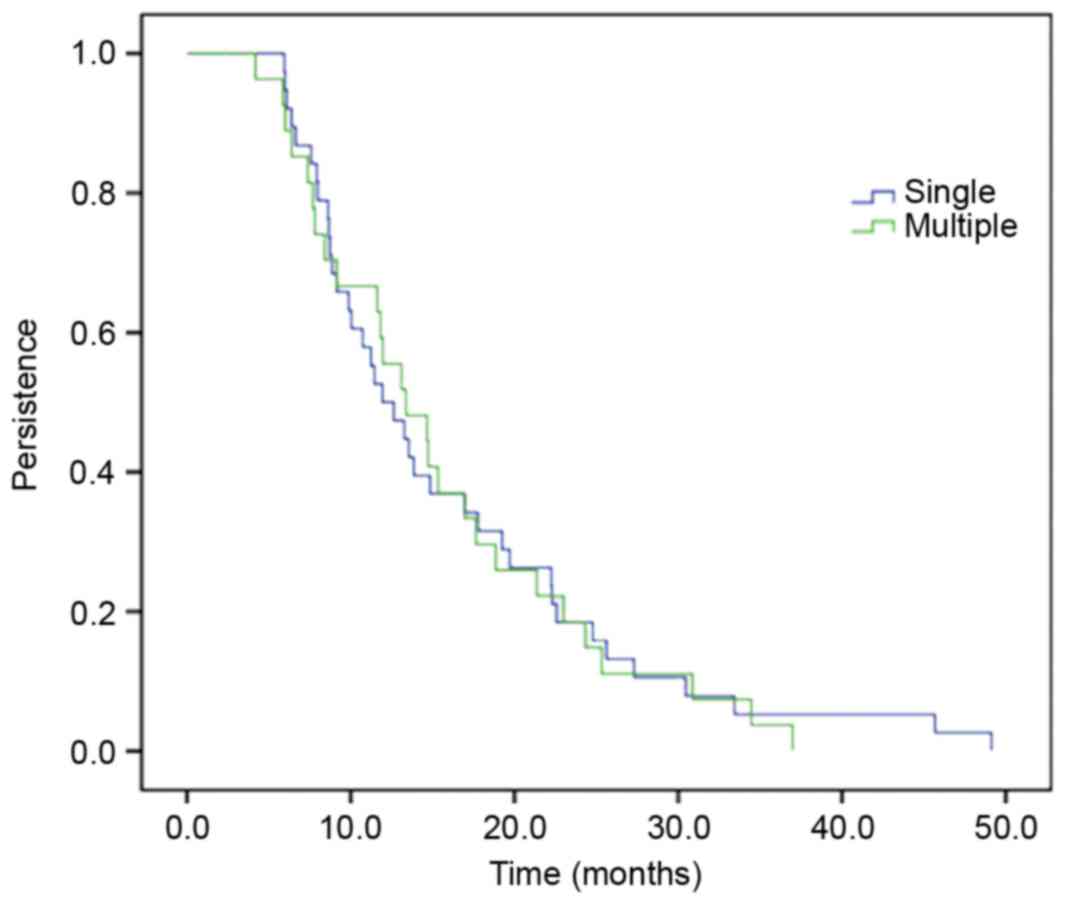
of follow-up. There was no difference in HPV58 persistence when the
HPV58 infection was identified in single or in multiple infections
(co-infection; Fig. 3). The mean
duration of HPV58 infection as a single infection was 16.03 months
and in multiple infections was 15.53 months (P=0.84; log rank
test).
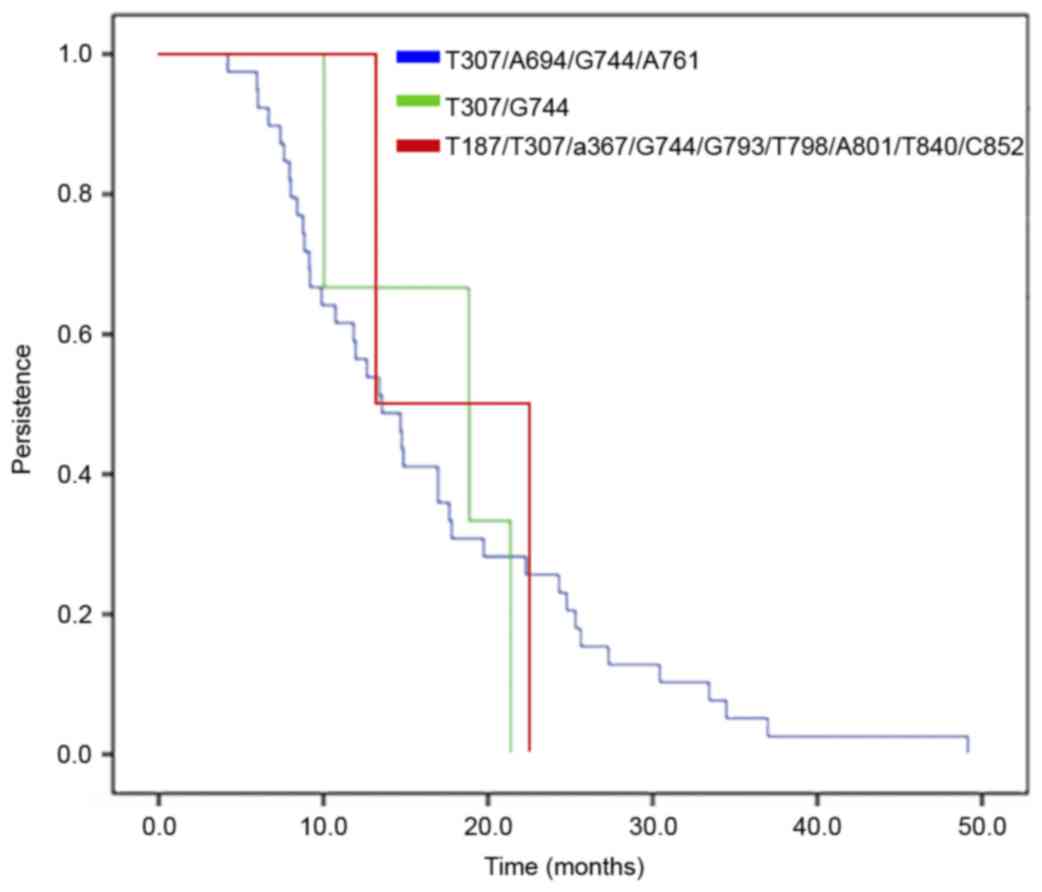
Clearance of HPV58 E6/E7 variants
The probability of persistence of HPV58 E6/E7
variants in women with incident HPV58 infections is presented in
Fig. 4. The same variant was
identified in persistent cases at all visits for all women. The
T307/A694/G744/A761 variant had a mean duration of infection of
16.65 months, while the mean duration for the T307/G744 variant was
16.76 months and for the
T187/T307/A367/G744/G793/T798/A801/T840/C852 variant 17.91 months
(P=0.98; log rank test).
Risk factors associated with clearance
of HPV58 incident infections
Table I presents the
age-adjusted and multivariate rate ratios of HPV58 clearance by
several viral and host characteristics. During follow-up, women
that first engaged sexual intercourse at >15 years of age had a
lower clearance rate than those who first engaged in sexual
intercourse at ≤15 years of age [hazard ratio (HR)=0.29; 95%
confidence interval (CI)=0.09–0.92]. In contrast, parous women were
associated with a higher clearance rate than nulliparous women
(HR=3.43, 95% CI=1.23–9.60). There was no difference in clearance
rates between the HPV58 variants.
 | Table I.HR and 95% CI for clearance of HPV58
incident infections. |
Table I.
HR and 95% CI for clearance of HPV58
incident infections.
| Clinicopathological
characteristic | No. | % | HR | 95% CI |
|---|
| Age, years |
|
<30 | 23 | 35.4 | 1.00 |
|
| ≥30 | 42 | 64.6 | 0.78 | 0.35–1.73 |
| Age at point of
first sexual intercourse, years |
|
≤15 | 15 | 23.1 | 1.00 |
|
|
>15 | 50 | 76.9 | 0.29 | 0.09–0.92 |
| Parity |
|
None | 11 | 16.9 | 1.00 |
|
| ≥1 | 54 | 83.1 | 3.43 | 1.23–9.60 |
| Use of oral
contraceptives |
| No | 48 | 75.0 | 1.00 |
|
|
Yes | 16 | 25.0 | 0.63 | 0.27–1.47 |
| Type of
infection |
|
Single | 41 | 63.1 | 1.00 |
|
|
Multiple | 24 | 36.9 | 0.72 | 0.32–1.00 |
| Viral load,
RLU |
| Low,
<0.5 | 16 | 24.6 | 1.00 |
|
| Medium,
≥0.5-<1.5 | 14 | 21.5 | 2.58 | 0.78–8.52 |
| High,
≥1.5 | 35 | 53.9 | 1.67 | 0.71–3.93 |
| HPV58 variant |
|
1a | 54 | 87.1 | 1.00 |
|
|
2b | 5 | 8.1 | 0.54 | 0.12–3.29 |
|
3c | 3 | 4.8 | 0.77 | 0.15–3.94 |
Characteristics of the women with
incident HPV58 infections that developed HGSIL during
follow-up
Table II lists the
characteristics of 2 women with incident HPV58 infections that
developed HGSIL during the follow-up. In the two women the HGSIL
was diagnosed at the second visit. The women were aged >35 years
and had multiple HPV infections.
| Table II.Characteristics of the patients with
incident HPV58 infections that developed high grade squamous
intraepithelial lesions during follow-up. |
Table II.
Characteristics of the patients with
incident HPV58 infections that developed high grade squamous
intraepithelial lesions during follow-up.
| Case | Visit | Age (years) | Type of
infection | HPV58 variant |
|---|
| 1 | 2 | 36 | Multiple
(HPV31-33-58) | No
amplification |
| 2 | 2 | 44 | Multiple
(HPV58-81) |
T307/A694/G744/A761 |
Discussion
A number of studies have demonstrated that certain
HPV58 E6/E7 variants are associated with a higher risk of cervical
cancer (15,16,20–27). In
the present study, the presence and persistence of incident HPV58
E6/E7 variants was assessed during a long follow-up period in women
with normal baseline cytology, as well as other risk factors
associated with clearance of HPV58 infections.
At present, information concerning sequence
variability of HPV58 is limited. The majority of studies have been
performed in Asian populations where higher rates of HPV58
prevalence have been reported compared with the rest of the world
(15,16,20–22). Only
a few studies in Latin-American countries have evaluated the
presence of HPV58 variants (23–29).
Two previous publications by an Asian group analyzed
samples from 15 different countries (30,31). These
studies reported sequence variability of the E6, E7, E2, E5, L1 and
LCR regions of the HPV58 genome, and proposed a novel
classification of HPV58 variants into 4 lineages. They also
identified specific variants that are associated with an increased
risk of cervical intraepithelial neoplasia grade III and invasive
cervical cancer (30,31). However, there is only one follow-up
study that analyzes the function of HPV58 variants in predicting
persistence of HPV58 infections in women with low grade squamous
intraepithelial lesions and atypical squamous cells of undetermined
significance (32). The present study
included women with normal baseline cytology who developed incident
HPV58 infections during follow-up.
Three different variants were identified in the
E6/E7 regions, with the T307/A694/G744/A761 variant demonstrating
the highest frequency (88% of the samples); which is in agreement
with a previous study examining the same cohort of women with
prevalent HPV58 variants (27) as
well as the study published by Chan et al (16) in 2002, where this variant was the most
frequent in women with normal cytology.
To the best of our knowledge there are no follow-up
studies analyzing the involvement of incident HPV58 variants in the
clearance of HPV58 infections and other risk factors in women with
normal cytology. The variant analysis demonstrated that for those
women with persistent HPV58 infections, the same variant was
detected over time. This confirmed the real persistence of HPV58
infections in the study population (27). In total, 50% of the HPV58 incident
infections were still present after 1 year of follow-up and 3%
after 4 years; a similar result to those reported by others
(33). The present study also
revealed no difference in HPV58 clearance rates when the infection
was a single event or comprised of multiple infections. In a
follow-up study of 2,462 women enrolled in the Ludwig-Mc Gill
cohort, Trottier et al (34)
revealed differences in HPV58 infection duration when the infection
was analyzed as mono-infection or co-infection with other HPV
genotypes. Differences between studies may be explained by study
design, the study population, and differences in data analysis and
methods of sampling and genotyping.
One of the aims of the present study was to analyze
whether there were differences in clearance rates between HPV58
variants in women with normal baseline cytology. The present study
revealed that there was no significant difference in clearance
rates and the variants detected had similar time of median
duration, suggesting that these variants did not serve a direct
function in the clearance of the HPV58 infection in this cohort of
women.
Clinicopathological characteristics, including age
at the point of first sexual intercourse and parity, were
associated with HPV58 incident infection clearance time. These
factors may therefore be added to the list of other previously
reported host factors that affect the clearance of HPV infections
(12).
In the present study only 2 women infected by HPV58
incident infections developed HGSIL. It was not possible to amplify
the E6 and E7 region in 1 patient, and the other presented with the
variant T307/A694/G744/A761, which has been previously reported in
other studies in women with normal histology and HGSIL (31). Other molecular HPV58 variants isolated
from HGSIL have been demonstrated to exhibit different
transcriptional activity that may be important in the expression of
E6 and E7 viral oncogenes (35).
The E6 and E7 regions of HPV58 positive samples were
amplified, but in a small number of samples it was not possible to
amplify these regions and therefore E6/E7 variants failed to be
identified. A potential reason for this may be low efficiency in
the amplification process due to the fragment size amplified
(36). Other reasons may involve DNA
degradation or DNA fragmentation in the samples analyzed, low viral
loads, viral integration or disruption in the HPV58 genome
(20).
The sample size in the present study was small,
which was a limitation to the analysis of the function of HPV58
variants in the development of HGSIL. Further studies are required
to examine the persistence of HPV58 E6/E7 variants in women with
abnormal cytology to analyze their pathological implications.
Acknowledgements
The authors would like to thank the National Cancer
Institute HPV study group: Dr Mauricio González, Dr Natasha Ortiz,
Dr Gustavo Hernández, Dr Oscar Gamboa, Dr Raul H Murillo, Dr
Joaquín Luna, Dr Hector Posso, Dr Margarita Ronderos, Dr Gilberto
Martínez, Dr Edmundo Mora, Dr Gonzalo Pérez, Dr José María Fuentes,
Dr Constanza Gómez, Dr Eva Klaus, Mrs Constanza Camargo, Mrs
Cecilia Tobón, Mrs Teodolinda Palacio, Dr Carolina Suarez, Mrs
Claudia Molina and Mr Alex Torres. The present study was supported
by the National Cancer Institute, Bogotá, Colombia (DNP grant no.
41030310-30).
References
|
1
|
Walboomers JM, Jacobs MV, Manos MM, Bosch
FX, Kummer JA, Shah KV, Snijders PJ, Peto J, Meijer CJ and Muñoz N:
Human papillomavirus is a necessary cause of invasive cervical
cancer worldwide. J Pathol. 189:12–19. 1999. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Muñoz N, Bosch FX, de Sanjosé S, Herrero
R, Castellsagué X, Shah KV, Snijders PJ and Meijer CJ:
International Agency for Research on Cancer Multicenter Cervical
Cancer Study Group: Epidemiologic classification of human
papillomavirus types associated with cervical cancer. New Eng J
Med. 348:518–527. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
de Sanjose S, Quint WG, Alemany L, Geraets
DT, Klaustermeier JE, Lloveras B, Tous S, Felix A, Bravo LE, Shin
HR, et al: Human papillomavirus genotype attribution in invasive
cervical cancer: A retrospective cross-sectional worldwide study.
Lancet Onco. 11:1048–1056. 2010. View Article : Google Scholar
|
|
4
|
Guan P, Howell-Jones R, Li N, Bruni L, de
Sanjosé S, Franceschi S and Clifford GM: Human papillomavirus (HPV)
types in 115,789 HPV-positive women: A meta-analysis from cervical
infection to cancer. Int J Cancer. 131:2349–2359. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Bosch FX, Manos MM, Muñoz N, Sherman M,
Jansen AM, Peto J, Schiffman MH, Moreno V, Kurman R and Shah KV:
Prevalence of human papillomavirus in cervical cancer: A worldwide
perspective. International biological study on cervical cancer
(IBSCC) Study Group. J Natl Cancer Inst. 87:796–802. 1995.
View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Palefsky JM, Minkoff H, Kalish LA, Levine
A, Sacks HS, Garcia P, Young M, Melnick S, Miotti P and Burk R:
Cervicovaginal human papillomavirus infection in human
immunodeficiency virus-1 (HIV)-positive and high-risk HIV-negative
women. J Natl Cancer Inst. 91:226–236. 1999. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Pett M and Coleman N: Integration of
high-risk human papillomavirus: A key event in cervical
carcinogenesis? J Pathol. 212:356–367. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Doeberitz MV and Vinokurova S: Host
factors in HPV-related carcinogenesis: Cellular mechanisms
controlling HPV infections. Arch Med Res. 40:435–442. 2009.
View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Chen HC, Schiffman M, Lin CY, Pan MH, You
SL, Chuang LC, Hsieh CY, Liaw KL, Hsing AW and Chen CJ: CBCSP-HPV
Study Group: Persistence of type-specific human papillomavirus
infection and increased long-term risk of cervical cancer. J Natl
Cancer Inst. 103:1387–1396. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Pardo C and Cendales R: Incidencia,
Mortalidad y Prevalencia de Cáncer en Colombia, 2007–2011. First
edtion. 1. Instituto Nacional de Cancerología; Bogotá, DC: pp.
1482015, (In Spanish).
|
|
11
|
Molano M, Posso H, Weiderpass E, van den
Brule AJ, Ronderos M, Franceschi S, Meijer CJ, Arslan A and Munoz
N: HPV Study Group HPV Study: Prevalence and determinants of HPV
infection among Colombian women with normal cytology. Br J Cancer.
87:324–333. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Muñoz N, Méndez F, Posso H, Molano M, van
den Brule AJ, Ronderos M, Meijer C and Muñoz A: Instituto Nacional
de Cancerologia HPV Study Group: Incidence, duration and
determinants of cervical human papillomavirus infection in a cohort
of Colombian women with normal cytological results. J Infect Dis.
190:2077–2087. 2004. View
Article : Google Scholar : PubMed/NCBI
|
|
13
|
Mendez F, Munoz N, Posso H, Molano M,
Moreno V, van den Brule AJ, Ronderos M, Meijer C and Munoz A:
Instituto Nacional de Cancerologia Human Papillomavirus Study
Group: Cervical coinfection with human papillomavirus (HPV) types
and possible implications for the prevention of cervical cancer by
HPV vaccines. J Infect Dis. 192:1158–1165. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Serrano B, Alemany L, Tous S, Bruni L,
Clifford GM, Weiss T, Bosch FX and de Sanjosé S: Potential impact
of a nine-valent vaccine in human papillomavirus related cervical
disease. Infect Agent Cancer. 7:382012. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Xin CY, Matsumoto K, Yoshikawa H, Yasugi
T, Onda T, Nakagawa S, Yamada M, Nozawa S, Sekiya S, Hirai Y, et
al: Analysis of E6 variants of human papillomavirus type 33, 52 and
58 in Japanese women with cervical intraepithelial
neoplasia/cervical cancer in relation to their oncogenic potential.
Cancer Lett. 170:19–24. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Chan PK, Lam CW, Cheung TH, Li WW, Lo KW,
Chan MY, Cheung JL and Cheng AF: Association of human
papillomavirus type 58 variant with the risk of cervical cancer. J
Natl Cancer Inst. 94:1249–1253. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Calleja-Macias IE, Villa LL, Prado JC,
Kalantari M, Allan B, Williamson AL, Chung LP, Collins RJ, Zuna RE,
Dunn ST, et al: Worldwide genomic diversity of the high-risk human
papillomavirus types 31, 35, 52 and 58, four close relatives of
human papillomavirus type 16. J Virol. 79:13630–13640. 2005.
View Article : Google Scholar : PubMed/NCBI
|
|
18
|
de Roda Husman AM, Walboomers JM, van den
Brule AJ, Meijer CJ and Snijders PJ: The use general primers GP5
and GP6 elongated at their 3′ ends with adjacent highly conserved
sequences improves human papillomavirus detection by PCR. J Gen
Virol. 76:1057–1062. 1995. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Benson DA, Karsch-Mizrachi I, Lipman DJ,
Ostell J and Wheeler DL: GenBank. Nucleic Acids Res. 33:D34–D38.
2005. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Wu EQ, Zha X, Yu XH, Zhang GN, Wu YG, Fan
Y, Ren Y, Kong LQ and Kong W: Profile of physical status and gene
variation of human papillomavirus 58 genome in cervical cancer. J
Gen Virol. 90:1229–1237. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Chang YJ, Chen HC, Lee BH, You SL, Lin CY,
Pan MH, Chou YC, Hsieh CY, Chen YM, Cheng YJ, et al: Unique
variants of human papillomavirus genotypes 52 and 58 and risk of
cervical neoplasia. Int J Cancer. 129:965–973. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Chan PK: Human papillomavirus type 58: The
unique role in cervical cancers in East Asia. Cell Biosci.
2:172012. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Veras VS, Cerqueira DM and Martins CR: L1
sequence of a new human papillomavirus type-58 variant associated
with cervical intraepithelial neoplasia. Braz J Med Biol Res.
38:1–4. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Raiol T, Wyant PS, de Amorim RM, Cerqueira
DM, Milanezi Nv, Brígido Mde M, Sichero L and Martins CR: Genetic
variability and phylogeny of the high-risk HPV-31, −33, −35, −52
and −58 in central Brazil. J Med Virol. 81:65–92. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Canche JC, López IR, Suárez NG, Acosta GC,
Conde-Ferráez L, Cetina TC and Losa MR: High prevalence and low E6
genetic variability of human papillomavirus 58 in women with
cervical cancer and precursor lesions in Southeast Mexico. Mem Inst
Oswaldo Cruz. 105:144–148. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Godínez JM, Heideman DA, Gheit T, Alemany
L, Snijders PJ, Tommasino M, Meijer CJ, de Sanjosé S, Bosch FX and
Bravo IG: Differential presence of Papillomavirus variants in
cervical cancer: An analysis for HPV33, HPV45 and HPV58. Infect
Genet Evol. 13:96–104. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Buitrago O, Morales N, Martín C, Huertas
A, Moreno P, Martínez T and Molano M: Presencia y persistencia de
variantes moleculares del ORF E6 y ORF E7 del VPH58 en mujeres con
citología normal que pertenecen a la cohorte de Bogotá, Colombia.
Rev Colomb Cancerol. 16:40–48. 2012.(In Spanish).
|
|
28
|
Mejía L, Muñoz D, Trueba G, Tinoco L and
Zapata S: Prevalence of human papillomavirus types in cervical
cancerous and precancerous lesions of Ecuadorian women. J Med
Virol. 88:144–152. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Gurgel AP, Chagas BS, do Amaral CM,
Nascimento KC, Leal LR, Silva Neto Jda C, Muniz Cartaxo MT and de
Freitas AC: Prevalence of human papillomavirus variants and genetic
diversity in the L1 gene and long control region of HPV16, HPV31
and HPV58 found in North-East Brazil. Biomed Res Int.
2015:1308282015. View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Chan PK, Luk AC, Park JS, Smith-McCune KK,
Palefsky JM, Konno R, Giovannelli L, Coutlée F, Hibbitts S, Chu TY,
et al: Identification of human papillomavirus type 58 lineages and
the distribution worldwide. Infect Dis. 203:1565–1573. 2011.
View Article : Google Scholar
|
|
31
|
Chan PK, Zhang C, Park JS, Smith-McCune
KK, Palefsky JM, Giovannelli L, Coutlée F, Hibbitts S, Konno R,
Settheetham-Ishida W, et al: Geographical distribution and
oncogenic risk association of human papillomavirus type 58 E6 and
E7 sequence variations. Int J Cancer. 132:2528–2536. 2013.
View Article : Google Scholar : PubMed/NCBI
|
|
32
|
Xi LF, Schiffman M, Koutsky LA, Hughes JP,
Hulbert A, Shen Z, Galloway DA and Kiviat NB: Variant-specific
persistence of infections with human papillomavirus Types 31, 33,
45, 56 and 58 and risk of cervical intraepithelial neoplasia. Int J
Cancer. 139:1098–1105. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
33
|
Insinga RP, Perez G, Wheeler CM, Koutsky
LA, Garland SM, Leodolter S, Joura EA, Ferris DG, Steben M,
Hernandez-Avila M, et al: Incident cervical HPV infections in young
women: Transition probabilities for CIN and infection clearance.
Cancer Epidemiol Biomarkers Prev. 20:287–296. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
34
|
Trottier H, Mahmud S, Prado JC, Sobrinho
JS, Costa MC, Rohan TE, Villa LL and Franco EL: Type-specific
duration of human papillomavirus infection: Implications for human
papillomavirus screening and vaccination. J Infect Dis.
197:1436–1447. 2008. View
Article : Google Scholar : PubMed/NCBI
|
|
35
|
Raiol T, de Amorim RM, Galante P, Martins
CR, Villa LL and Sichero L: HPV-58 molecular variants exhibit
different transcriptional activity. Intervirology. 54:146–150.
2011. View Article : Google Scholar : PubMed/NCBI
|
|
36
|
van den Brule AJ, Meijer CJ, Bakels V,
Kenemans P and Walboomers JM: Rapid detection of human
papillomavirus in cervical scrapes by combined general
primer-mediated and type-specific polymerase chain reaction. J Clin
Microbiol. 28:2739–2743. 1990.PubMed/NCBI
|