Introduction
Intestinal mucositis is an important safety concern
in patients undergoing chemotherapy. It can lead to considerable
diarrhea and dehydration, which could lead to poor overall health
(1–3).
However, there are few effective treatments or preventive methods.
Chemotherapy-induced mucositis can limit the dose of chemotherapy
and increase the risk of infection or hospitalization.
Consequently, mucositis during chemotherapy could increase clinical
and economic burdens (4).
5-Fluorouracil (5-FU) is a frequently prescribed
anticancer agent; however, it commonly causes chemotherapy-related
mucositis. Approximately 80% of patients subjected to chemotherapy
with 5-FU develop chemotherapy-induced mucositis (5). Inflammation, ulceration, and bleeding
can occur throughout the digestive tract, particularly in the small
intestine (6).
The present therapy for chemotherapy-associated
mucositis mainly consists of topical analgesics, mucosal coating
agents, antimicrobials, and cryotherapy (7). Recent studies have reported that
chemotherapy-induced mucositis improves with keratinocyte growth
factor and rhubarb extract in murine models (6–10). Current
treatment methods for chemotherapy-induced mucositis usually aim to
decrease the symptoms, rather than providing a complete cure. Thus,
it is necessary to discover novel therapies for preventing or
reducing this complication associated with chemotherapy.
Ursodeoxycholic acid (UDCA) is a physiological
component present in trace amounts in human bile and has been
prescribed in patients with various liver diseases (11–13). It
stabilizes cell membranes, inhibits apoptosis, and acts as an
antioxidant, thereby exerting cytoprotective effects (14–20). A
previous study reported that UDCA protects against experimental
ileitis by attenuating oxidative stress and intestinal barrier
dysfunction (21).
We hypothesized that the direct cytoprotective
effect of UDCA could protect against mucosal injury during
chemotherapy. The aim of present study was to examine the ability
of UDCA in protecting against chemotherapy-associated mucositis by
using an animal model.
Materials and methods
Animal trial
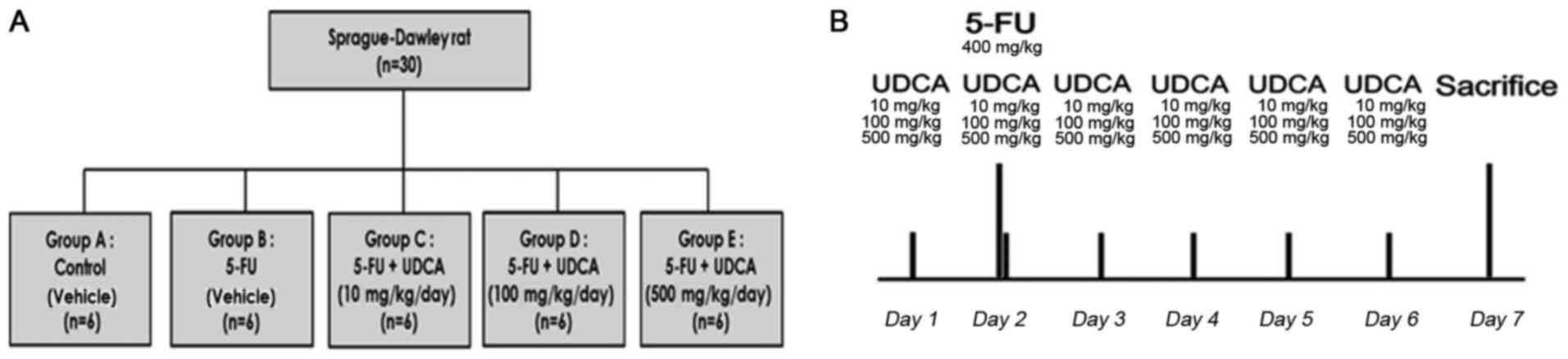
We randomized 30 male Sprague-Dawley rats (120–130
g) to the following five groups with six rats in each group:
Control (group A; n=6), 5-FU (group B; n=6), 5-FU + UDCA (10
mg/kg/day) (group C; n=6), 5-FU + UDCA (100 mg/kg/day) (group D;
n=6), and 5-FU + UDCA (500 mg/kg/day) (group E; n=6). The rats were
housed in a room maintained at a temperature of 24±2°C, photoperiod
of 12 h, and humidity of 60±5%. Water and food were provided ad
libitum. On day 7 of the experiment (i.e., 24 h after the last dose
of UDCA or its vehicle), the rats were sacrificed through
CO2 asphyxiation with a flow rate of ~10-30% of the
chamber volume per minute, and histological and hematological
analyses were performed (Fig. 1B).
The Committee on the Ethics of Animal Experiments of Korea
University Anam Hospital approved this protocol (permit no.
KUIACUC-2015-122).
Treatment with 5-FU
Gastrointestinal mucositis was induced via the
intraperitoneal administration of 5-FU. We injected a single dose
of 5-FU on day 2 (400 mg/kg; JW Pharm, Seoul, Korea). Physiological
saline was administered to the control group, and 5-FU solution in
saline was injected intraperitoneally to rats in the four other
experimental groups (Fig. 1A).
UDCA preparation
Suspensions of UDCA (Daewoong Pharmaceuticals Co.,
Ltd., Seoul, Korea) were prepared by adding UDCA to 10 ml of
vehicle [0.5% carboxymethyl cellulose (JW Pharm) +1% Tween-80 in
distilled water]. The vehicle of the same volume was also prepared
and administered to rats in the control group. UDCA suspensions
were administered daily by gavage for six days; the first dose was
administered one day before 5-FU injection.
Diarrhea and body weight
assessment
Diarrhea scores and body weights were assessed in
all rats from the day of UDCA administration. The occurrence and
grade of diarrhea were defined according to the diarrhea assessment
(22). Diarrhea score for each rat
was evaluated daily as follows: 0, normal stool (normal); 1,
considerably moist stool (mild); 2, unformed and wet stool
(moderate); and 3, watery stool (severe). The estimated mean scores
were used.
Histological analysis
On day 7, we sacrificed the rats and a 2-cm specimen
from the proximal lesion of all harvested small intestine was
processed and placed in formalin overnight. Then, the resected
intestinal specimens were dehydrated, cleared in xylol, embedded in
paraffin, and microtomed into sections of constant thickness for
staining. Crypt depth and villus height were evaluated using light
microscopy (magnification, 100 and ×400, respectively).
Inflammatory cytokine analysis
On day 7, the obtained intestinal tissues were
cleansed and stored in RNA later at 4°C before use. cDNA was
synthesized using the Superscript™ II real-time
polymerase chain reaction System (Invitrogen, Karlsruhe, Germany)
according to the manufacturer's recommendations. cDNA synthesis was
performed using 500 ng of RNA at 42°C and diluted 1:2 prior to use.
Quantitative PCR was carried out using ABI 7900 (Applied
Biosystems, Foster City, CA, USA). Primer/TaqMan probe combinations
of tumor necrosis factor (TNF)-α (reporter sequence
ACCCTCACACTCAGATCATCTTCTC) and interleukin (IL)-6 (reporter
sequence GGATATAACCAGGAAATTTGCCTAT) were designed for each target
sequence. mRNA expression levels were analyzed with the comparative
Cq method (23).
Myeloperoxidase (MPO) activity
analysis
MPO activity was calculated by immunohistochemistry
according to a method described previously (24). The results are represented as MPO
units per high-power field.
Statistical analysis
Data are shown as mean ± standard deviation and
percentages. Statistical analyses were performed using the
Kruskal-Wallis and Mann-Whitney U tests with the Bonferroni
correction, as appropriate. Statistical significance was
established at P<0.05. All statistical analyses were performed
using SPSS version 20.0 (IBM Corp., Armonk, NY, USA).
Results
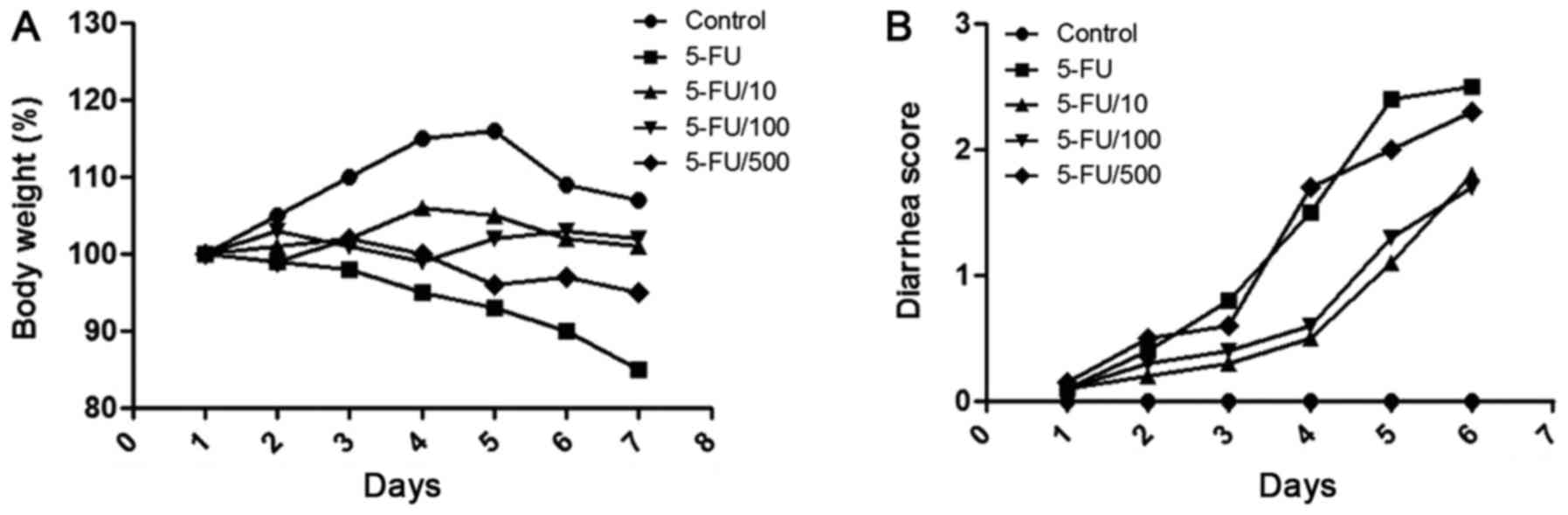
Alteration in body weight and diarrhea
score
5-FU administration caused diarrhea and body weight
loss (Fig. 2). On day 6, mean body
weight reduced to 89.6±1.7% of the original weight, and mean
diarrhea score was 1.7±0.51. Compared with the 5-FU administration
group, the daily administration of UDCA attenuated body weight loss
during the experiment in the 5-FU + UDCA (10 mg/kg/day) (P=0.139)
and the 5-FU + UDCA (100 mg/kg/day) groups (P=0.001). Diarrhea
score also decreased in the UDCA groups.
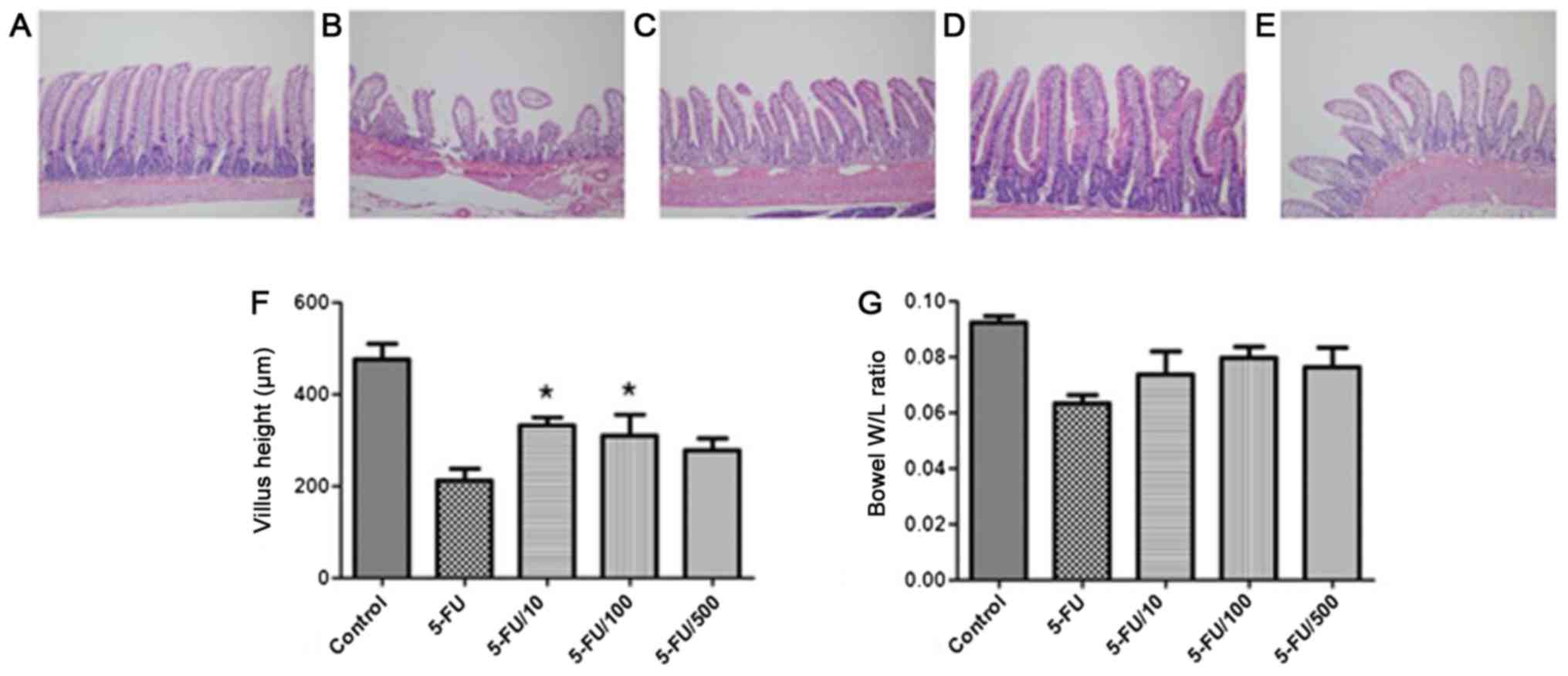
Histological analysis: Crypt depth and
villus height measurements
The evaluation of crypt depth and villus height can
indicate the overall severity of mucosal injury. Histological
alterations were assessed based on heights of jejunal villi. 5-FU
induced considerable alterations in the mucosa (Fig. 3). Compared with the 5-FU group, the
UDCA co-administration group showed a higher and an intact
epithelial layer. Compared to the jejunal villi lengths in the
vehicle + 5-FU group (212.8±58.0 µm), those in the 5-FU + UDCA (100
mg/kg/day) and 5-FU + UDCA (10 mg/kg/day) groups were significantly
greater [310.0±112.6 (P=0.046) and 331.3±18.0 µm (P=0.001),
respectively]. The weight-to-length ratio of the resected
intestinal tissue section was also increased in UDCA
co-administration groups compared with that in the 5-FU only
group.
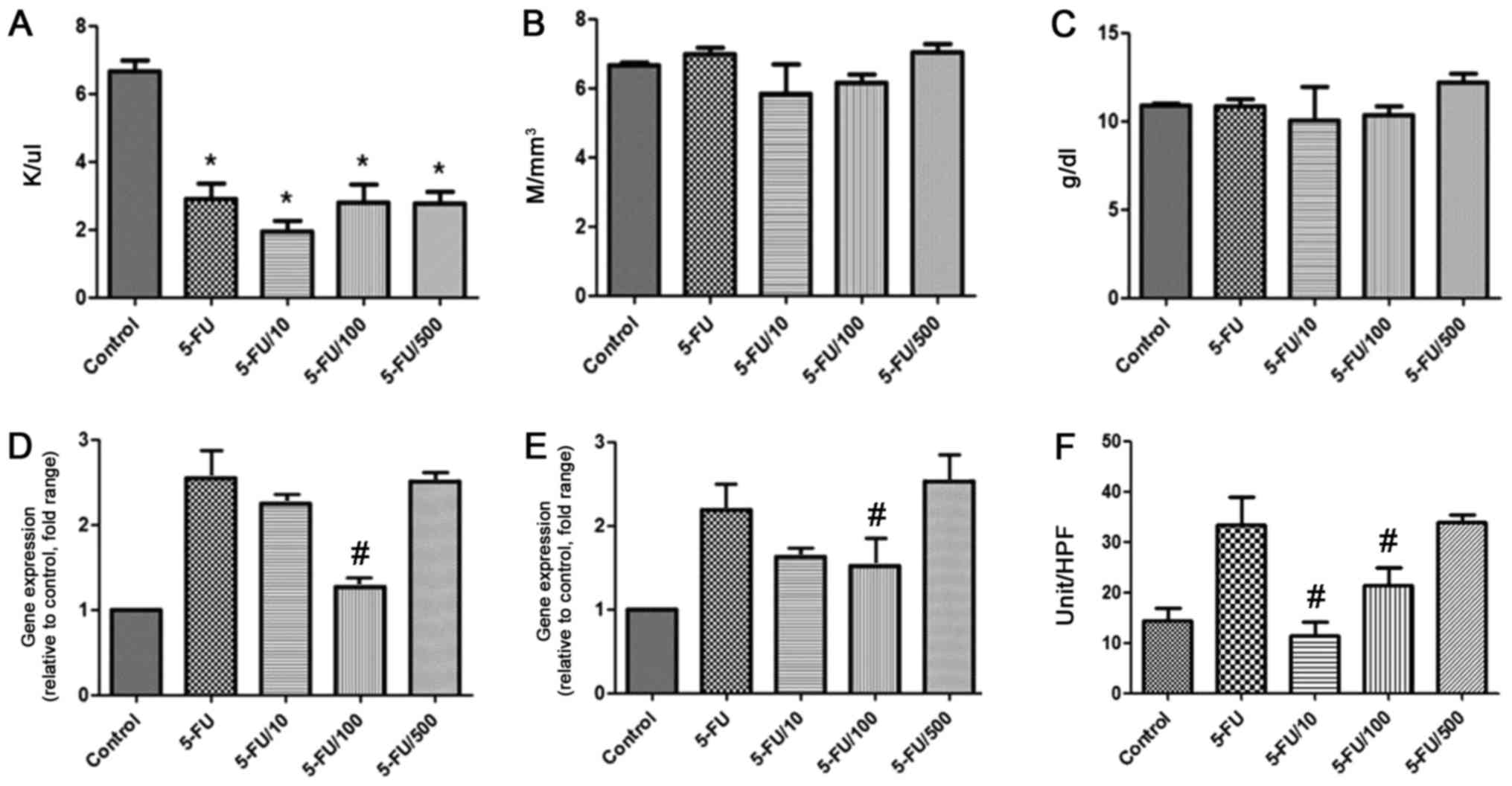
Hematological analysis
Hematological analysis revealed that white blood
cell (WBC) count significantly reduced in the 5-FU group compared
with the control group (P<0.05) (Fig.
4A). However, WBC count was also reduced in the UDCA groups.
red blood cell (RBC) count and hemoglobin level were not different
among the groups (Fig. 4B, C).
Inflammatory cytokine analysis
The mRNA expression of IL-6 and TNF-α was increased
by approximately two-fold because of 5-FU (Fig. 4D and E). UDCA administration (100
mg/kg/day) significantly reduced the 5-FU-mediated mRNA expression
of both TNF-α and IL-6 (P<0.05).
MPO activity
The activity of MPO (number of MPO-positive cells
per high-power field) was compared among the groups (Fig. 4F). MPO activity significantly
decreased in the 100 and 10 mg/kg/day UDCA groups compared with
corresponding levels in the 5-FU group (P<0.05).
Discussion
The aim of this study was to evaluate the protective
effect of UDCA against chemotherapy-associated intestinal
mucositis. Our results showed that UDCA attenuates
chemotherapy-induced reduction in villus height and decreases
levels of inflammatory cytokines and MPO activity.
5-FU is frequently used for treating
gastrointestinal malignancy. However, approximately 80% of patients
subjected to chemotherapy with 5-FU develop chemotherapy-induced
mucositis (5). This adverse effect
can worsen the quality of life in patients undergoing chemotherapy
and can cause an early cessation of chemotherapy. Therefore,
effective preventive and therapeutic agents against
chemotherapy-induced intestinal mucositis are needed.
UDCA has demonstrated efficacy in numerous types of
hepatic disorders, without considerable adverse effects upon
long-term administration (25–27). The
exact mechanism of UDCA in improving hepatic dysfunction remains to
be established; however, some assumptions have been made. In these
hypotheses, UDCA has been suggested to protect the liver from the
toxic effect of hydrophobic bile acids by altering the organization
of the bile acid pool (28–30). Further, UDCA exerts a direct
cytoprotective action by acting as an antioxidant, inhibiting
apoptosis, and stabilizing membranes (14–17). UDCA
decreased oxidative stress and intestinal permeability in an
indomethacin-induced ileitis model, relieved ibuprofen-induced
enteropathy, and improved trinitrobenzene sulfonic acid sodium
salt-induced colitis (21,31,32). These
effects coupled with its long-term safety have valuable
implications and highlight the potential of UDCA as a therapeutic
agent in non-hepatic disorders (26,27,33).
Consistent with previous findings, 5-FU
administration in this study led to considerable small bowel
mucositis. The induced mucositis was characterized by villus height
reduction and damage to crypts in the small intestine. The
co-administration of UDCA attenuated the degree of 5-FU-induced
mucosal injury and associated clinical symptoms, such as body
weight reduction and diarrhea. Therefore, UDCA co-administration
may be effective in treating 5-FU-associated intestinal mucositis
and its associated manifestations.
Regarding the pathogenesis of
chemotherapy-associated intestinal mucositis, several pathogenic
components have been suggested to present direct cytotoxicity, and
stimulate abnormal inflammation and hypoproliferation (2,34,35). 5-FU-induced apoptosis could be
provoked by the initiation of the extrinsic apoptotic pathway,
which is mediated by inflammatory cytokines (36). Previous studies have shown that
apoptosis caused by 5-FU administration is substantially
ameliorated through the inhibition of cytokines (37–39). In
the current study, UDCA co-administration (100 mg/kg/day) reduced
levels of TNF-α and IL-6 in the small intestine. This indicated
that UDCA may protect against chemotherapy-associated mucositis by
decreasing the levels of inflammatory cytokines.
The dose of UDCA was decided based on a previous
report that UDCA at a dose of 10 mg/kg/day relieves intestinal
inflammation (40); however, the
opposite effect occurs at a dose of approximately 400 mg/kg/day
(41). An investigation with colitis
models indicated that UDCA at doses of 10–50 mg/kg/day ameliorates
enteropathy, whereas UDCA at a dose of 400 mg/kg/day induces cell
membrane damage and solubilization due to an increase in
hydrophobic bile acid, resulting from an increase in secondary bile
acid levels. In the current study, UDCA at doses of 100 and 10
mg/kg/day exerted a protective effect against chemotherapy-induced
mucositis, as indicated by an improvement in reduced villus height.
The optimal dose should be established for chemotherapy-associated
mucositis.
The present study has limitations, including the
lack of assessment of other roles of UDCA in the prevention of
chemotherapy-associated mucositis. Furthermore, effects on the
intestine of UDCA alone at different doses were not evaluated.
However, to accurately evaluate the action of UDCA
in chemotherapy-induced mucositis, pro-inflammatory cytokine
production and damage to mucosal components were assessed. The
current findings demonstrated the protective effect of UDCA against
chemotherapy-associated mucositis. Further studies are necessary to
investigate other roles of UDCA against chemotherapy-associated
mucositis and to confirm the ideal dose.
UDCA is currently prescribed for the treatment of
various hepatic diseases without significant adverse events. Owing
to its cytoprotective effect, it can be assumed that UDCA can be
easily applied to treat chemotherapy-induced mucositis. However,
its possible adverse effects, such as skin rash, nephritis, and
vasculitis, also should be considered (42).
In conclusion, UDCA considerably decreased
inflammatory cytokine levels, intestinal villus damage, and MPO
activity. These results highlight the possibility of UDCA, at a
suitable dose, as a protective agent against
chemotherapy-associated intestinal mucositis.
Acknowledgements
Not applicable.
Funding
The present study was supported by the Ministry of
Trade, Industry & Energy (Korea) under the Industrial
Technology Innovation ‘Development of diagnostic device for
functional dyspepsia based on Korean-Western medicine fusion
abdominal diagnosis’ (grant no. 10060251), and by Daewoong
Pharmaceuticals Co. Ltd. (Seoul, Korea).
Availability of data and materials
All data generated or analyzed during this study are
included in this published article.
Authors' contributions
SHK, BK and HJC designed the research, and SHK and
BK performed the experiments. ESK, YTJ, HSL and CDK assisted in
data acquisition, and creating the tables and figures. HSC, YSS and
SHU analyzed the data. SHK wrote the manuscript.
Ethics approval and consent to
participate
The study was approved by the Ethics Committee of
Animal Experiments at Korea University Anam Hospital (approval no.
KUIACUC-2015-122).
Consent for publication
Not applicable.
Competing interests
Daewoong Pharmaceuticals Co., Ltd. (Seoul, Korea)
provided the UDCA used in the experiments and also financially
supported the present study.
Glossary
Abbreviations
Abbreviations:
|
UDCA
|
ursodeoxycholic acid
|
|
5-FU
|
5-fluorouracil
|
|
WBC
|
white blood cell
|
|
RBC
|
red blood cell
|
|
MPO
|
myeloperoxidase
|
|
IL
|
interleukin
|
|
TNF
|
tumor necrosis factor
|
References
|
1
|
Benson AB III, Ajani JA, Catalano RB,
Engelking C, Kornblau SM, Martenson JA Jr, McCallum R, Mitchell EP,
O'Dorisio TM, Vokes EE and Wadler S: Recommended guidelines for the
treatment of cancer treatment-induced diarrhea. J Clin Oncol.
22:2918–2926. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Bowen JM, Gibson RJ, Cummins AG and Keefe
DM: Intestinal mucositis: The role of the Bcl-2 family, p53 and
caspases in chemotherapy-induced damage. Support Care Cancer.
14:713–731. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Keefe DMK, Brealey J, Goland GJ and
Cummins AG: Chemotherapy for cancer causes apoptosis that precedes
hypoplasia in crypts of the small intestine in humans. Gut.
47:632–637. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Maioli TU, de Melo Silva B, Dias MN, Paiva
NC, Cardoso VN, Fernandes SO, Carneiro CM, Dos Santos Martins F and
de Vasconcelos Generoso S: Pretreatment with Saccharomyces
boulardii does not prevent the experimental mucositis in Swiss
mice. J Negat Results Biomed. 13:62014. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Smith CL, Geier MS, Yazbeck R, Torres DM,
Butler RN and Howarth GS: Lactobacillus fermentum BR11 and
fructo-oligosaccharide partially reduce jejunal inflammation in a
model of intestinal mucositis in rats. Nutr Cancer. 60:757–767.
2008. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Sonis ST, Elting LS, Keefe D, Peterson DE,
Schubert M, Hauer-Jensen M, Bekele BN, Raber-Durlacher J, Donnelly
JP, Rubenstein EB, et al: Perspectives on cancer therapy-induced
mucosal injury: Pathogenesis, measurement, epidemiology, and
consequences for patients. Cancer. 100(9 Suppl): S1995–S2025. 2004.
View Article : Google Scholar
|
|
7
|
Gibson RJ, Keefe DM, Lalla RV, Bateman E,
Blijlevens N, Fijlstra M, King EE, Stringer AM, van der Velden WJ,
Yazbeck R, et al: Systematic review of agents for the management of
gastrointestinal mucositis in cancer patients. Support Care Cancer.
21:313–326. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Rubenstein EB, Peterson DE, Schubert M,
Keefe D, McGuire D, Epstein J, Elting LS, Fox PC, Cooksley C, Sonis
ST, et al: Clinical practice guidelines for the prevention and
treatment of cancer therapy-induced oral and gastrointestinal
mucositis. Cancer. 100(9 Suppl): S2026–S2046. 2004. View Article : Google Scholar
|
|
9
|
Bhatt V, Vendrell N, Nau K, Crumb D and
Roy V: Implementation of a standardized protocol for prevention and
management of oral mucositis in patients undergoing hematopoietic
cell transplantation. J Oncol Pharm Pract. 16:195–204. 2010.
View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Bajic JE, Eden GL, Lampton LS, Cheah KY,
Lymn KA, Pei JV, Yool AJ and Howarth GS: Rhubarb extract partially
improves mucosal integrity in chemotherapy-induced intestinal
mucositis. World J Gastroenterol. 22:8322–8333. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Hwang MJ and Kim TN: Diffuse-type Caroli
disease with characteristic central dot sign complicated by
multiple intrahepatic and common bile duct stones. Clin Endosc.
50:400–403. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Kwon CI and Lehman GA: Mechanisms of
biliary plastic stent occlusion and efforts at prevention. Clin
Endosc. 49:139–146. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Yoo KH, Kwon CI, Yoon SW, Kim WH, Lee JM,
Ko KH, Hong SP and Park PW: An impacted pancreatic stone in the
papilla induced acute obstructive cholangitis in a patient with
chronic pancreatitis. Clin Endosc. 45:99–102. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Güldütuna S, Zimmer G, Imhof M, Bhatti S,
You T and Leuschner U: Molecular aspects of membrane stabilization
by ursodeoxycholate [see comment]. Gastroenterology. 104:1736–1744.
1993. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Rodrigues CM, Fan G, Ma X, Kren BT and
Steer CJ: A novel role for ursodeoxycholic acid in inhibiting
apoptosis by modulating mitochondrial membrane perturbation. J Clin
Invest. 101:2790–2799. 1998. View
Article : Google Scholar : PubMed/NCBI
|
|
16
|
Rodrigues CM, Fan G, Wong PY, Kren BT and
Steer CJ: Ursodeoxycholic acid may inhibit deoxycholic acid-induced
apoptosis by modulating mitochondrial transmembrane potential and
reactive oxygen species production. Mol Med. 4:165–178.
1998.PubMed/NCBI
|
|
17
|
Lapenna D, Ciofani G, Festi D, Neri M,
Pierdomenico SD, Giamberardino MA and Cuccurullo F: Antioxidant
properties of ursodeoxycholic acid. Biochem Pharmacol.
64:1661–1667. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Cao A, Wang L, Chen X, Guo H, Chu S, Zhang
X and Peng W: Ursodeoxycholic acid ameliorated diabetic nephropathy
by attenuating hyperglycemia-mediated oxidative stress. Biol Pharm
Bull. 39:1300–1308. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Mroz MS, Lajczak NK, Goggins BJ, Keely S
and Keely SJ: The bile acids, deoxycholic acid and ursodeoxycholic
acid, regulate colonic epithelial wound healing. Am J Physiol
Gastrointest Liver Physiol. 314:G378–G387. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Lajczak NK, Saint-Criq V, O'Dwyer AM,
Perino A, Adorini L, Schoonjans K and Keely SJ: Bile acids
deoxycholic acid and ursodeoxycholic acid differentially regulate
human β-defensin-1 and −2 secretion by colonic epithelial cells.
FASEB J. 31:3848–3857. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Bernardes-Silva CF, Damião AO, Sipahi AM,
Laurindo FR, Iriya K, Lopasso FP, Buchpiguel CA, Lordello ML,
Agostinho CL and Laudanna AA: Ursodeoxycholic acid ameliorates
experimental ileitis counteracting intestinal barrier dysfunction
and oxidative stress. Dig Dis Sci. 49:1569–1574. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Kurita A, Kado S, Kaneda N, Onoue M,
Hashimoto S and Yokokura T: Modified irinotecan hydrochloride
(CPT-11) administration schedule improves induction of
delayed-onset diarrhea in rats. Cancer Chemother Pharmacol.
46:211–220. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Livak KJ and Schmittgen TD: Analysis of
relative gene expression data using real-time quantitative PCR and
the 2(-Delta Delta C(T)) method. Methods. 25:402–408. 2001.
View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Krawisz JE, Sharon P and Stenson WF:
Quantitative assay for acute intestinal inflammation based on
myeloperoxidase activity. Assessment of inflammation in rat and
hamster models. Gastroenterology. 87:1344–1350. 1984.PubMed/NCBI
|
|
25
|
Lindor KD, Kowdley KV, Luketic VA,
Harrison ME, McCashland T, Befeler AS, Harnois D, Jorgensen R, Petz
J, Keach J, et al: High-dose ursodeoxycholic acid for the treatment
of primary sclerosing cholangitis. Hepatology. 50:808–814. 2009.
View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Cullen SN, Rust C, Fleming K, Edwards C,
Beuers U and Chapman RW: High dose ursodeoxycholic acid for the
treatment of primary sclerosing cholangitis is safe and effective.
J Hepatol. 48:792–800. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Oh B, Choi WS, Park SB, Cho B, Yang YJ,
Lee ES and Lee JH: Efficacy and safety of ursodeoxycholic acid
composite on fatigued patients with elevated liver function and/or
fatty liver: A multi-centre, randomised, double-blinded,
placebo-controlled trial. Int J Clin Pract. 70:302–311. 2016.
View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Renner EL, Lake JR, Cragoe EJ Jr, van Dyke
RW and Scharschmidt BF: Ursodeoxycholic acid choleresis:
Relationship to biliary HCO-3 and effects of Na+-H+ exchange
inhibitors. Am J Physiol. 254:G232–G241. 1988.PubMed/NCBI
|
|
29
|
Sagawa H, Tazuma S and Kajiyama G:
Protection against hydrophobic bile salt-induced cell membrane
damage by liposomes and hydrophilic bile salts. Am J Physiol.
264:G835–G839. 1993.PubMed/NCBI
|
|
30
|
Hofmann AF: Pharmacology of
ursodeoxycholic acid, an enterohepatic drug. Scand J Gastroenterol
Suppl. 204:1–15. 1994. View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Kullmann F, Arndt H, Gross V, Rüschoff J
and Schölmerich J: Beneficial effect of ursodeoxycholic acid on
mucosal damage in trinitrobenzene sulphonic acid-induced colitis.
Eur J Gastroenterol Hepatol. 9:1205–1211. 1997.PubMed/NCBI
|
|
32
|
Lloyd-Still JD, Beno DW, Uhing MR,
Jiyamapa-Serna VA and Kimura RE: Ursodeoxycholic acid ameliorates
ibuprofen-induced enteropathy in the rat. J Pediatr Gastroenterol
Nutr. 32:270–273. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
33
|
Braga MF, Grace MG, Lenis J, Kennedy FP,
Teplinsky AL, Roederer G, Palumbo PJ, Colin P and Leiter LA:
Efficacy and safety of ursodeoxycholic acid in primary, type IIa or
IIb hypercholesterolemia: A multicenter, randomized, double-blind
clinical trial. Atherosclerosis. 203:479–482. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
34
|
Duncan M and Grant G: Oral and intestinal
mucositis - causes and possible treatments. Aliment Pharmacol Ther.
18:853–874. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
35
|
Daniele B, Secondulfo M, de Vivo R,
Pignata S, de Magistris L, Delrio P, Palaia R, Barletta E, Tambaro
R and Carratù R: Effect of chemotherapy with 5-fluorouracil on
intestinal permeability and absorption in patients with advanced
colorectal cancer. J Clin Gastroenterol. 32:228–230. 2001.
View Article : Google Scholar : PubMed/NCBI
|
|
36
|
Kato S, Hayashi S, Kitahara Y, Nagasawa K,
Aono H, Shibata J, Utsumi D, Amagase K and Kadowaki M: Saireito
(TJ-114), a Japanese traditional herbal medicine, reduces
5-fluorouracil-induced intestinal mucositis in mice by inhibiting
cytokine-mediated apoptosis in intestinal crypt cells. PLoS One.
10:e01162132015. View Article : Google Scholar : PubMed/NCBI
|
|
37
|
Wu ZQ, Han XD, Wang Y, Yuan KL, Jin ZM, Di
JZ, Yan J, Pan Y, Zhang P, Huang XY, et al: Interleukin-1 receptor
antagonist reduced apoptosis and attenuated intestinal mucositis in
a 5-fluorouracil chemotherapy model in mice. Cancer Chemother
Pharmacol. 68:87–96. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
38
|
Yasuda M, Kato S, Yamanaka N, Iimori M,
Matsumoto K, Utsumi D, Kitahara Y, Amagase K, Horie S and Takeuchi
K: 5-HT(3) receptor antagonists ameliorate 5-fluorouracil-induced
intestinal mucositis by suppression of apoptosis in murine
intestinal crypt cells. Br J Pharmacol. 168:1388–1400. 2013.
View Article : Google Scholar : PubMed/NCBI
|
|
39
|
Huang TY, Chu HC, Lin YL, Ho WH, Hou HS,
Chao YC and Liao CL: Minocycline attenuates 5-fluorouracil-induced
small intestinal mucositis in mouse model. Biochem Biophys Res
Commun. 389:634–639. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
40
|
Kullmann F, Gross V, Rüschoff J, Arndt H,
Benda W, Winkler von Mohrenfels A and Schölmerich J: Effect of
ursodeoxycholic acid on the inflammatory activity of
indomethacin-induced intestinal inflammation in rats. Z
Gastroenterol. 35:171–178. 1997.PubMed/NCBI
|
|
41
|
Uchida A, Yamada T, Hayakawa T and Hoshino
M: Taurochenodeoxycholic acid ameliorates and ursodeoxycholic acid
exacerbates small intestinal inflammation. Am J Physiol.
272:G1249–G1257. 1997.PubMed/NCBI
|
|
42
|
Kotb MA: Molecular mechanisms of
ursodeoxycholic acid toxicity & side effects: Ursodeoxycholic
acid freezes regeneration & induces hibernation mode. Int J Mol
Sci. 13:8882–8914. 2012. View Article : Google Scholar : PubMed/NCBI
|