Introduction
Carcinoid tumors are neuroendocrine neoplasms
derived from enterochromaffin cells, which are widely distributed
in the body (1–4). Carcinoid tumors usually occur in the
gastrointestinal tract (58–75%) and lung (20–31%), although they
may occur anywhere in the body (2–4).
Carcinoid tumors are rare, occurring in only 1–2 cases per 100,000,
and vary with age, gender and ethnicity. Clinical presentation of a
carcinoid tumor is dominated by symptoms caused by amines secreted
by the tumor. The classical carcinoid syndrome includes diarrhea,
flushing, bronchial obstruction and carcinoid heart disease and
correlates with the serotonin-secreting activity of the tumor
(2,5). Carcinoid tumors usually metastasize to
the liver, lymph nodes and lungs (3). In approximately 10% of cases, the
primary tumor site remains unknown (4). The mainstay of treatment for carcinoid
tumors is surgical resection. Octreotide has become the main
therapeutic regimen for carcinoid syndrome-related complaints.
Octreotide has often been suggested to prolong survival, but this
hypothesis has never been confirmed (6). Chemotherapy is not considered to be a
first-line treatment for carcinoid tumors. The overall 5-year
survival rate for all carcinoid tumors ranges from 70 to 80%
(6,7). As expected, the stage of disease
significantly affects the prognosis, with the best 5-year survival
rate in patients with localized disease (93%) and a poor 5-year
survival rate in patients with distant metastatic disease (20–30%)
(4,5).
In the past, skeletal metastases from carcinoid
tumors were considered to be extremely rare (1,8).
However, skeletal metastases are becoming more prevalent due to
longer survival and advances in earlier detection (9). Recent studies have revealed that the
incidence of skeletal metastases in carcinoid tumors is
approximately 10% (3,5). Some patients with skeletal metastases
from carcinoid tumors complain of pain at the site of metastases,
and occasionally develop pathological fractures and spinal cord
injuries due to metastasis to the spine. Despite the increasing
need for precise evaluation and treatment, skeletal metastasis may
frequently remain undetected, as some patients with skeletal
metastases do not complain of any symptoms. Moreover, the nature of
the skeletal metastasis from carcinoid tumors has not been fully
elucidated.
In this study, we present two cases of carcinoid
tumors that metastasized to the bone. Furthermore, we reviewed 50
published case reports and described the occurrence, site and
clinical course of skeletal metastasis in patients with carcinoid
tumors.
The study was approved by the Ethics Committee of
the hospital, and consent was obtained from the patients
involved.
Case report
Case 1
A 59-year-old man had a history of multiple previous
metastases, with a carcinoid tumor that was originally found in the
lung in 2000. The patient underwent a surgical resection of the
primary lesion, but developed liver and skeletal metastases in
2004. Although the patient had received chemotherapy after the
metastases were detected, he complained of back pain and numbness
in the lower limbs, and was admitted to our hospital in August
2009. Magnetic resonance imaging (MRI) revealed extensive
metastases at almost all levels of the thoracic spine, with
epidural extension of the tumor at the Th9 level (Fig. 1A and B). Computed tomography (CT)
revealed a mixture of osteosclerotic and osteolytic changes in the
Th9 vertebra (Fig. 1C). Bone
scintigraphy using 99mTc-methylene diphosphonate
(99mTc-MDP) demonstrated abnormal uptake into the Th9
vertebra. A spinal decompression was performed at Th8–9 with Th7–10
posterior fusion using spinal instrumentation. The pain and
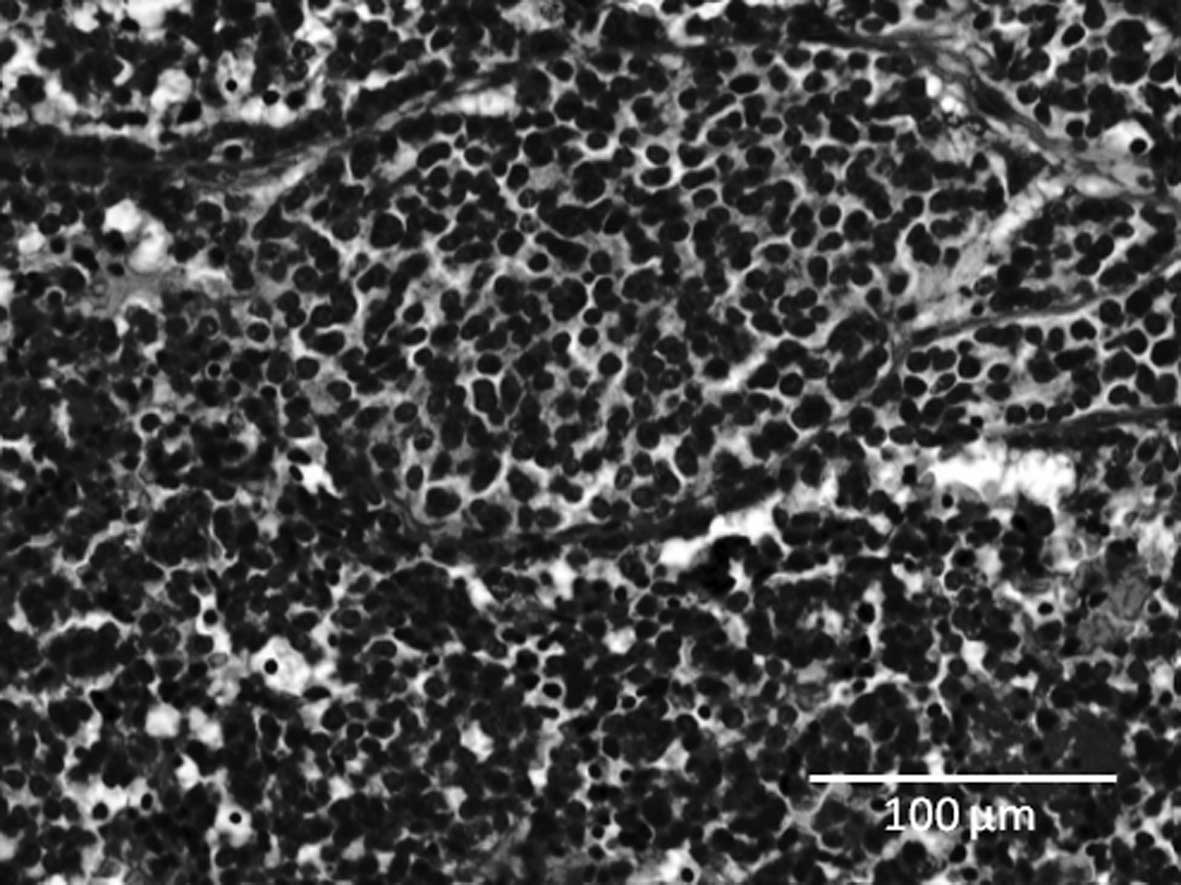
numbness were resolved following surgery. A histological
examination of the surgical specimen demonstrated that the tumor
consisted of cellular nests of small round cells (Fig. 2). The majority of tumor cells were
positive for chromogranin A, synaptophysin and CD56 (data not
shown). The histological diagnosis was metastases to the spine from
a carcinoid tumor. The patient underwent chemotherapy following
surgery and remained alive with slight numbness in his leg in
August 2010.
Case 2
A 74-year-old man was referred to our hospital with
complaints of left thigh pain and impaired gait. The patient had
been diagnosed with a lung carcinoid tumor 15 years previously, and
had developed liver metastases 1 year before admission to our
hospital. A radiograph showed osteolytic lesions in the shaft of
the left femur (Fig. 3A). CT
revealed destruction of the cancellous bone and thinning of the
cortex in the shaft of the left femur (Fig. 3B). Bone scintigraphy using
99mTc-MDP demonstrated increased uptake into multiple
bones including the cervical, thoracic and lumbar vertebrae, ribs,
humerus, femurs and pelvis (Fig.
3C). According to these images, we diagnosed a pathological
fracture of the left femur due to skeletal metastasis from a
carcinoid tumor and surgery was performed to remove the lesion. We
repaired the femur using intramedullary nails following curettage
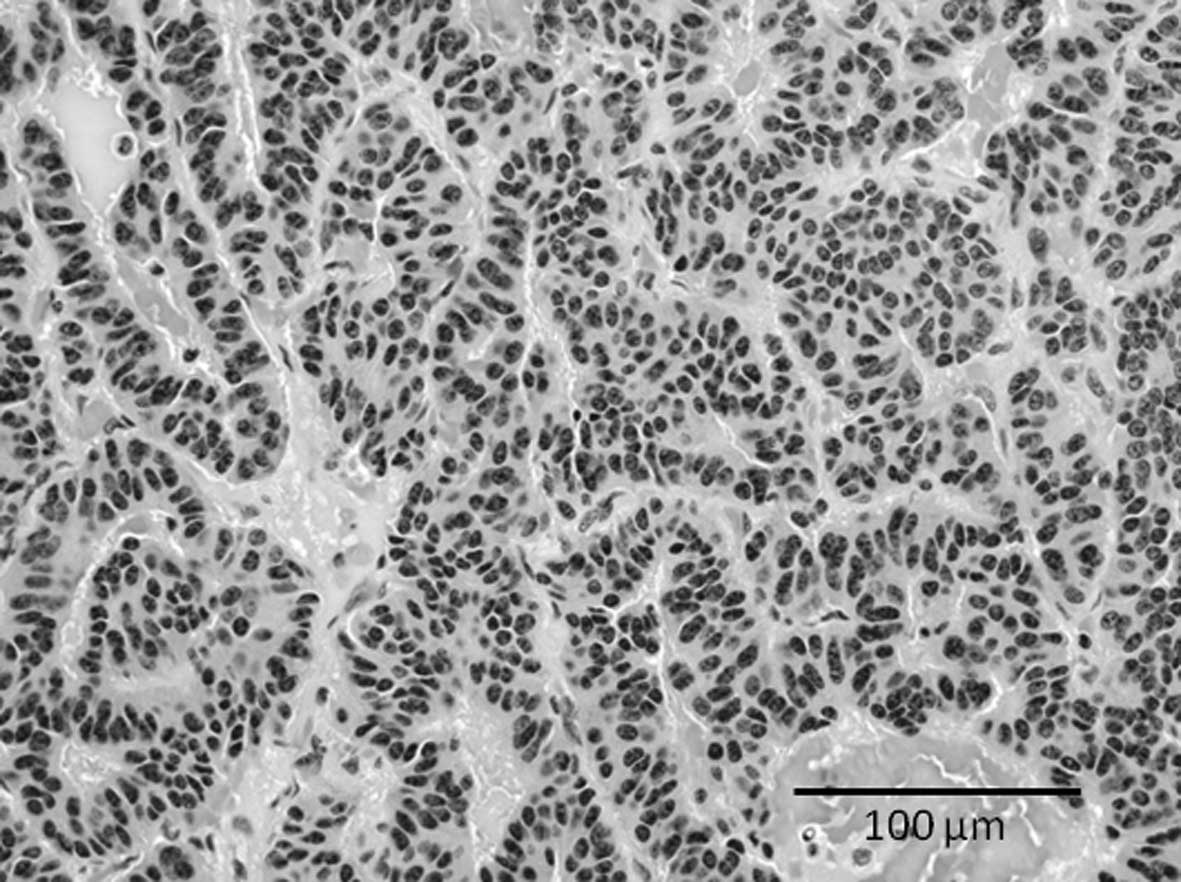
of the tumor. A histological examination of the surgical specimen
demonstrated that the tumor consisted of cellular nests of small
round cells (Fig. 4). The majority
of tumor cells were positive for chromogranin A, synaptophysin and
CD56 (data not shown). The histological diagnosis was metastases to
the femur from a carcinoid tumor. A radiograph of the femur showed
a callus on the pathological fracture. The patient was able to walk
using a crutch 3 months after surgery.
Discussion
Skeletal metastases from carcinoid tumors have been
considered extremely rare in the past (8). In most cases, examination for the
presence of skeletal metastases was initiated in patients with
clinical symptoms suggestive of skeletal metastases. However,
patients with carcinoid tumors with skeletal metastasis do not
always complain of pain at the site of skeletal metastasis, as
demonstrated by case 2 and previous reports (5,9).
Previous studies evaluating the use of octreotide scintigraphy in
carcinoid tumors describe a rate of skeletal metastases of between
7 and 20% (5,9–11).
Ross and Roberts reported that autopsy revealed a higher rate (42%)
of skeletal metastases in 36 patients with carcinoid tumors
(12). Thus, we considered that
skeletal metastasis from carcinoid tumors is not as rare as
previously thought. Meijer et al reported that bone
scintigraphy and octreotide scintigraphy have acceptable
sensitivity and that MRI has high sensitivity for detecting bone
metastases (5).
Fluoro-2-deoxy-D-glucose positron emission computerized tomography
is also useful for detecting multiple bone metastases from
carcinoid tumors (13). Even if
patients do not complain of any symptoms, patients with carcinoid
tumors should be followed up carefully using effective inspection
methods.
We reviewed 50 cases that described skeletal
metastasis from carcinoid tumors (3,13–28).
The characteristics of the reported patients are shown in Table I. The average age of the patients
was 54.9 years (range, 19–82) and 33 patients (66%) were male. The
primary lesion site was the gastrointestinal tract in 17 cases, the
pulmonary region in 13 cases and other regions in 20 cases. The
rate of skeletal metastasis from pulmonary carcinoid tumors appears
higher than that from gastrointestinal carcinoid tumors, as
carcinoid tumors usually occur in the gastrointestinal tract
(58–75%) (2–4). The most common site of skeletal
metastasis is the spine, and 40% of cases revealed metastases to
thoracic vertebrae, 34% to the lumbar vertebrae and 32% to the
cervical vertebrae. Other common sites were the ribs (28%) and the
pelvis (26%). The average period between the initial diagnosis of
carcinoid tumor and skeletal metastasis was 22 months (range,
0–144; n=46). Regarding treatment, surgery was performed in 15 out
of 50 cases (30%). Spinal decompression was indicated in 11 cases
and extirpation was performed in 4 cases. We also used the
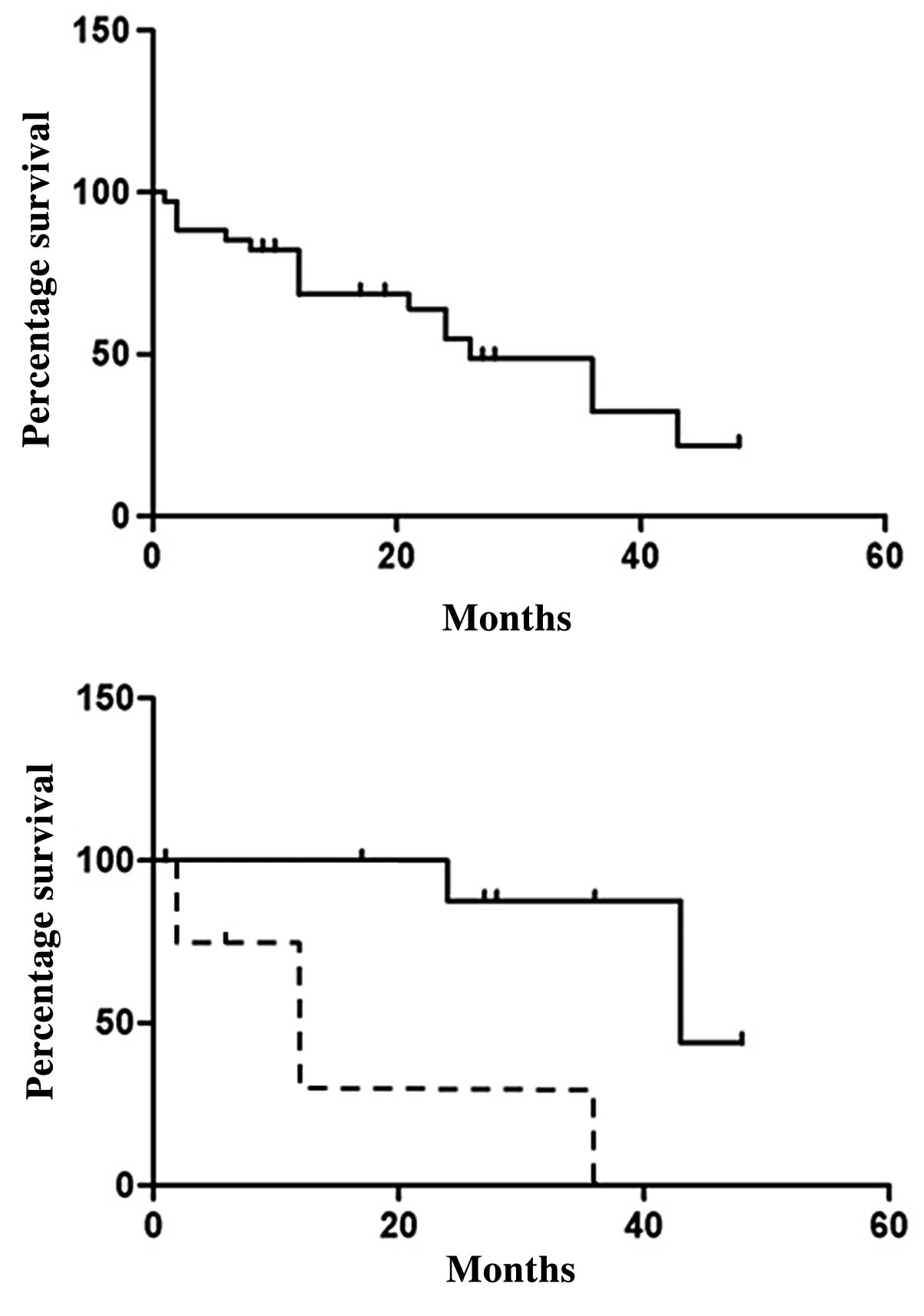
Kaplan-Meier method to investigate the survival rate of patients
who developed skeletal metastasis from carcinoid tumors (n=35).
Fig. 5A shows the survival rate of
the 35 cases following skeletal metastasis. The survival rate
gradually decreased, and 50% of patients died 24 months following
skeletal metastasis. We noted that 5 of 9 patients with osteolytic
skeletal metastasis died within 1 year of skeletal metastasis,
whereas none of the 9 patients with osteosclerotic metastasis died.
We compared the survival of patients with osteolytic metastasis to
the survival of those with osteosclerotic metastasis. Fig. 5B shows that the survival of patients
who developed osteolytic skeletal metastasis is worse than that of
patients who developed osteosclerotic skeletal metastasis. We
investigated gender, age, site of primary lesion of the carcinoid
tumor, secretion and pathology in osteosclerotic and osteolytic
cases to identify differences between osteosclerotic and osteolytic
metastases, but we did not determine a significant factor leading
to osteolytic changes at metastatic sites. The average period
between diagnosis of carcinoid tumor and skeletal metastasis in
osteolytic patients (n=13) was 2.0 months (0–24), whereas in
osteosclerotic patients (n=15) this period was 27.9 months (0–144).
Eleven of 13 cases had already developed skeletal metastasis when
the initial diagnosis of carcinoid tumors showed osteolytic
changes. These results demonstrate that the majority of patients
who developed osteolytic skeletal metastasis presented skeletal
metastasis at the initial visit, and osteolytic bone metastasis may
be an adverse prognostic factor in patients with carcinoid
tumors.
 | Table ICharacteristics of the reported
patients. |
Table I
Characteristics of the reported
patients.
| Characteristics | No. of patients |
|---|
| Male/female | 33/17 |
| Mean age (range) | 54.9 (19–82) |
| Primary site |
| Rectum | 12 |
| Duodenum | 2 |
| Lung | 13 |
| Thymus | 6 |
| Others | 14 |
| Metastasis site |
| Spine |
| Cervical | 6 (32.0%) |
| Thoracic | 20 (40.0%) |
| Lumbar | 17 (34.0%) |
| Sacrum | 9 (22.5%) |
| Extremity |
| Humerus | 3 (6.0%) |
| Femur | 10 (20.0%) |
| Others |
| Rib | 14 (28.0%) |
| Pelvis | 13 (26.0%) |
In this study, we reported two cases of skeletal
metastasis from carcinoid tumors. The patients had osteolytic
skeletal metastatic lesions, and surgery was effective for treating
the lesion. However, these patients should be followed up carefully
as osteolytic skeletal metastasis is an adverse prognostic factor
in patients with carcinoid tumors.
Acknowledgements
We thank Takashi Kondo, Department of Radiological
Science, University of Toyama, for statistical analysis.
References
|
1
|
Powell JM: Metastatic carcinoid of bone.
Report of two cases and review of the literature. Clin Orthop Relat
Res. 230:266–272. 1988.PubMed/NCBI
|
|
2
|
Janmohamed S and Bloom SR: Carcinoid
tumours. Postgrad Med J. 73:194–200. 1997. View Article : Google Scholar
|
|
3
|
Arnold PM, Floyd HE, Anderson KK and
Newell KL: Surgical management of carcinoid tumors metastatic to
the spine: report of three cases. Clin Neurol Neurosurg.
112:443–445. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Zuetenhorst JM and Taal BG: Metastatic
carcinoid tumors: a clinical review. Oncologist. 10:123–131. 2005.
View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Meijer WG, van der Veer E, Jager PL, van
der Jagt EJ, Piers BA, Kema IP, de Vries EG and Willemse PH: Bone
metastases in carcinoid tumors: clinical features, imaging
characteristics, and markers of bone metabolism. J Nucl Med.
44:184–191. 2003.PubMed/NCBI
|
|
6
|
Quaedvlieg PF, Visser O, Lamers CB,
Janssen-Heijen ML and Taal BG: Epidemiology and survival in
patients with carcinoid disease in The Netherlands. An
epidemiological study with 2391 patients. Ann Oncol. 12:1295–1300.
2001. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Modlin IM, Lye KD and Kidd M: A 5-decade
analysis of 13,715 carcinoid tumors. Cancer. 97:934–959. 2003.
View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Kirkpatrick DB, Dawson E, Haskell CM and
Batzdorf U: Metastatic carcinoid presenting as a spinal tumor. Surg
Neurol. 4:283–287. 1975.PubMed/NCBI
|
|
9
|
Zuetenhorst JM, Hoefnageli CA, Boot H,
Valdés Olmos RA and Taal BG: Evaluation of (111)In-pentetreotide,
(131)I-MIBG and bone scintigraphy in the detection and clinical
management of bone metastases in carcinoid disease. Nucl Med
Commun. 23:735–741. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Westlin JE, Janson ET, Arnberg H, Ahlström
H, Oberg K and Nilsson S: Somatostatin receptor scintigraphy of
carcinoid tumours using the [111In-DTPA-D-Phe1]-octreotide. Acta
Oncol. 32:783–786. 1993.
|
|
11
|
Kwekkeboom DJ, Krenning EP, Bakker WH, Oei
HY and Kooij PP: Somatostatin analogue scintigraphy in carcinoid
tumours. Eur J Nucl Med. 20:283–292. 1993. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Ross EM and Roberts WC: The carcinoid
syndrome: comparison of 21 necropsy subjects with carcinoid heart
disease to 15 necropsy subjects without carcinoid heart disease. Am
J Med. 79:339–354. 1985. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Kobashi Y, Shimizu H, Mouri K, Irei T and
Oka M: Clinical usefulness of fluoro-2-deoxy-D-glucose PET in a
case with multiple bone metastases of carcinoid tumor after ten
years. Intern Med. 48:1919–1923. 2009.PubMed/NCBI
|
|
14
|
Katai M, Sakurai A, Inaba H, Ikeo Y,
Yamauchi K and Hashizume K: Octreotide as a rapid and effective
painkiller for metastatic carcinoid tumor. Endocr J. 52:277–280.
2005. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Gray JA, Nishikawa H, Jamous MA and
Grahame-Smith DG: Spinal cord compression due to carcinoid
metastasis. Postgrad Med J. 64:703–705. 1988. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Ozkan M, Er O, Karahan IO, Deniz K, Coşkun
R, Küçük C, Yurci A and Altinbaş M: Rectal carcinoid tumor with
bone marrow and osteoblastic bone metastasis: a case report. Turk J
Gastroenterol. 18:111–114. 2007.PubMed/NCBI
|
|
17
|
Nguyen BD and Ram PC: Bronchopulmonary
carcinoid tumor and related cervical vertebral metastasis with
PET-positive and octreotide-negative scintigraphy. Clin Nucl Med.
31:101–103. 2006. View Article : Google Scholar
|
|
18
|
Goddard MJ and Atkinson C: Cardiac
metastasis from a bronchial carcinoid: report of a case presenting
with diffuse thickening of the left ventricular wall. J Clin
Pathol. 57:778–779. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Ashraf MH: Bronchial carcinoid with
osteoblastic metastases. Thorax. 32:509–511. 1977. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Isaka T, Maruno M, Suzuki T, Sato M and
Yoshimine T: Skull metastases from atypical pulmonary carcinoid
tumor in a 19-year-old man. Neurol Med Chir (Tokyo). 46:609–613.
2006.PubMed/NCBI
|
|
21
|
Pellini R, Ruggieri M, Pichi B, Covello R,
Danesi G and Spriano G: A case of cervical metastases from temporal
bone carcinoid. Head Neck. 27:644–647. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Blondet E, Dulou R, Camparo P and Pernot
P: Lumbar intradural metastasis of a primary carcinoid tumor of the
lung. Case illustration. J Neurosurg Spine. 2:2312005. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Lim KH, Huang MJ, Yang S, Hsieh RK and Lin
J: Primary carcinoid tumor of prostate presenting with bone marrow
metastases. Urology. 65:1742005. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Tanabe M, Akatsuka K, Umeda S, Shomori K,
Taniura S, Okamoto H, Kamitani H and Watanabe T: Metastasis of
carcinoid to the arch of the axis in a multiple endocrine neoplasia
patient: a case report. Spine J. 8:841–844. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Brown LR, Aughenbaugh GL, Wick MR, Baker
BA and Salassa RM: Roentgenologic diagnosis of primary
corticotropin-producing carcinoid tumors of the mediastinum.
Radiology. 142:143–148. 1982. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Gowitt GT and Mirra SS: Malignant
carcinoid causing spinal cord compression. Neurosurgery.
17:801–806. 1985. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Noshiro H, Satoh K, Gondoh T, Iwata T,
Fujii T, Mezuki M, Masuda H and Inoue T: A case of rectal carcinoid
with extensive sacral breakage. Jpn J Surg. 20:443–447. 1990.
View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Sato K, Higaki Y, Sakaguchi S, Hirano M,
Tanimura A and Sasaguri Y: Carcinoid tumor of the larynx. Auris
Nasus Larynx. 18:39–53. 1991. View Article : Google Scholar
|