Introduction
Glomus tumors are benign lesions that originate from
modified smooth muscle cells of the glomus body that help regulate
arteriolar blood flow. These tumors are commonly observed in the
dermis or subcutis, but are rarely located in the stomach, occuring
in ~2% of all benign gastric tumors (1). Gastric glomus tumors are most commonly
described as solitary, well-defined, submucosal lesions in the
antrum, presenting with a variety of symptoms. Gastrointestinal
bleeding with hematemesis/melena and epigastric discomfort are the
most common initial symptoms and, in rare cases, may be
life-threatening or lead to severe chronic anemia. Nausea and
vomiting can also occur (2,3). Surgery is often performed promptly
since malignancy cannot be excluded due to the rarity of this tumor
(4). Gastric glomus tumors have a
good prognosis due to low recurrence and rarity of malignant
transformation. However, a long follow-up is required for further
study. Patient provided written informed consent.
Case report
A 47-year-old female was admitted to The Second
Affiliated Hospital of Zhejiang University (Hangzhou, China) on
March 20, 2013 due to intermittent epigastralgia for four months,
which could be temporarily relieved by eating. The patient denied
any associated weight loss, fevers, chills, nausea, vomiting or
melena. Acid suppression therapy had been administered with only
minimal relief. A physical examination revealed only mild
tenderness in the epigastric area, and serum levels of tumor makers
were all within normal limits. The patient’s father had died of
gastric carcinoma.
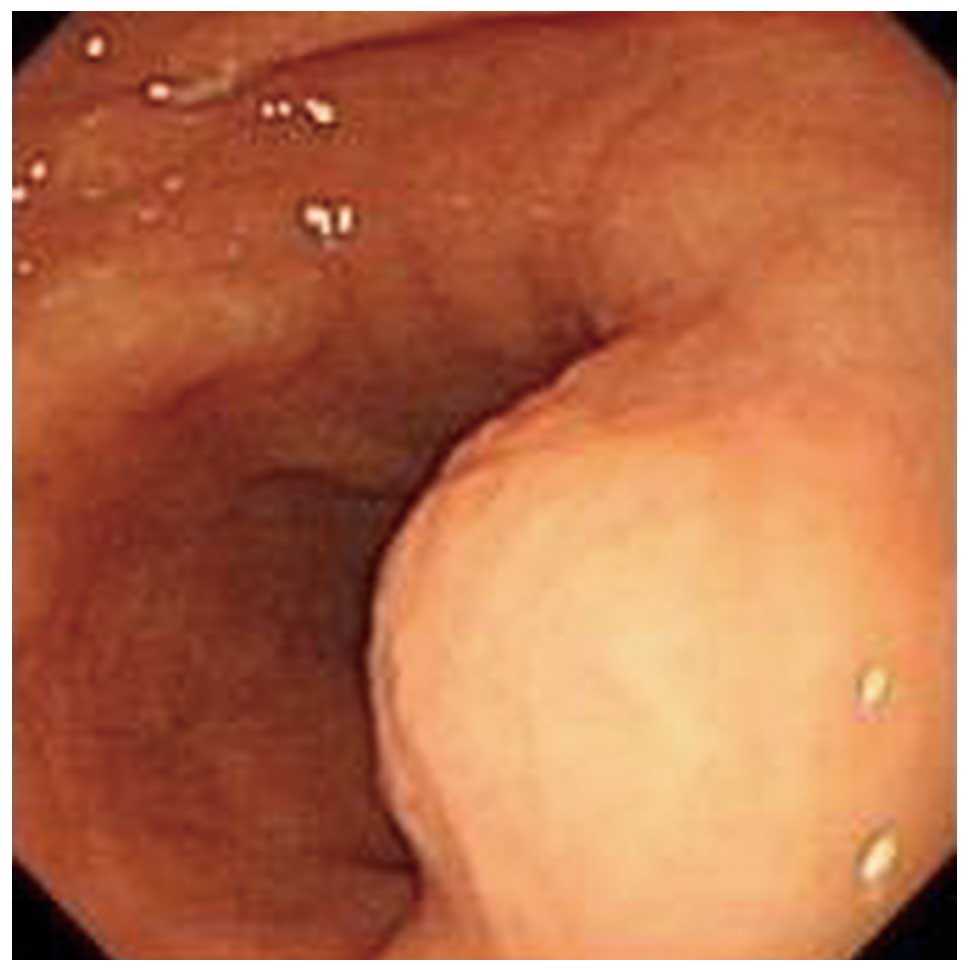
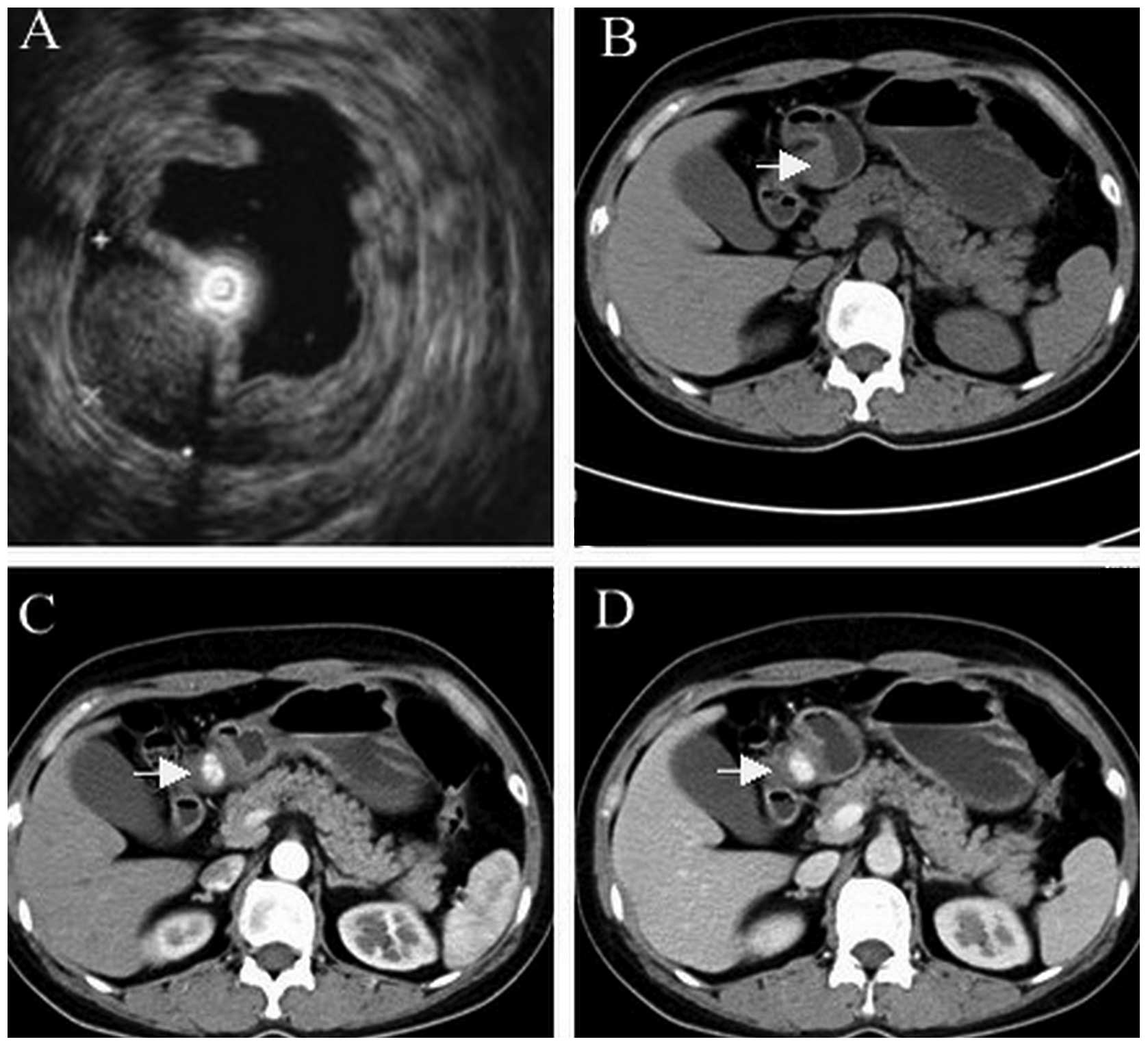
Endoscopic ultrasound (EUS) revealed a protrusion on
the posterior wall of the gastric antrum (Figs. 1 and 2A). Computed tomography (CT) scan
identified a mass on the antrum ~10 mm in diameter (Fig. 2B–D).
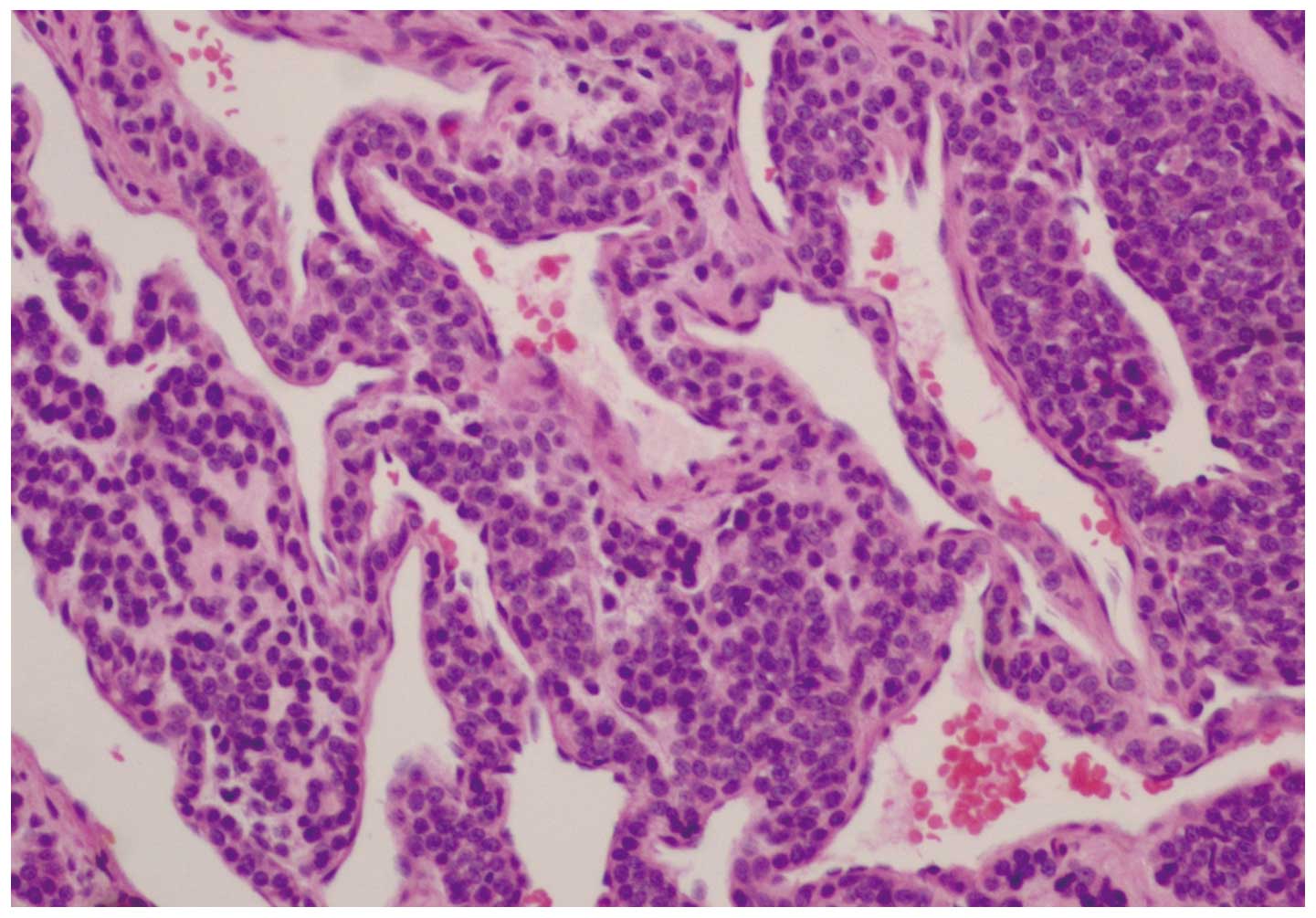
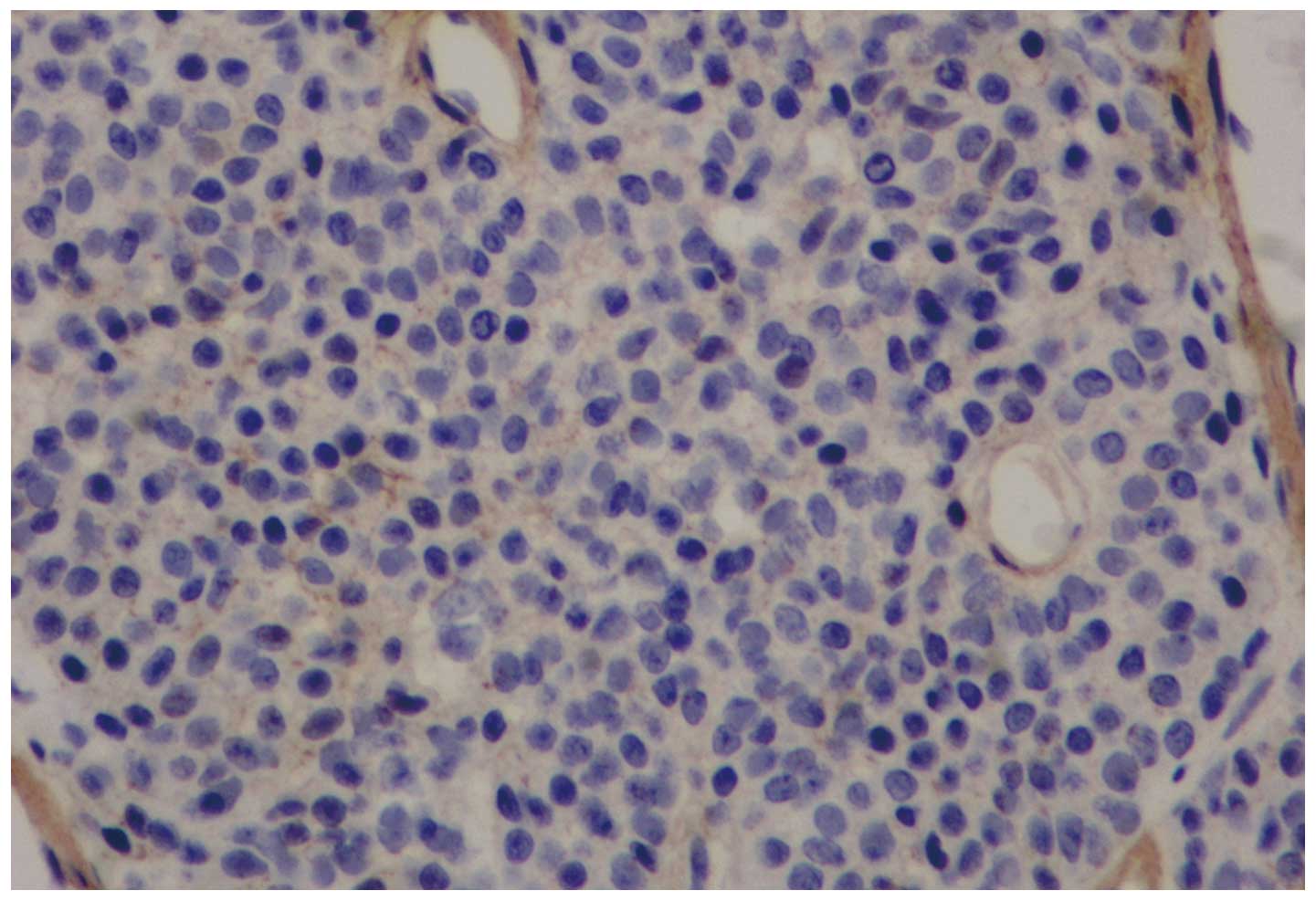
Immunoperoxidase stains revealed positive staining
for smooth muscle actin (SMA) and collagen type IV, while being
negative for synaptophysin, chromogranin A, laminin, S-100, cluster
of differentiation (CD)34, CD31, CD99, cytokeratin (AE1/AE3),
desmin and epithelial membrane antigen. The proliferation marker
Ki-67 was positive in <5% of tumor cell nuclei (Figs. 3–5).
A complete resection of the lesion was performed at
The Second Affiliated Hospital of Zhejiang University. The patient
was followed up for five months and recovered uneventfully without
signs of relapse or gastrointestinal bleeding.
Discussion
Glomus tumors are rare in the stomach, and were
first reported by De Busscher in 1948 as benign lesions (5). Gastric glomus tumors are now defined
as mesenchymal tumors with potential malignant behavior. Malignant
glomus tumors of the stomach with various organ metastases have
been reported (6,7). Criteria for identifying malignant
potential in gastric glomus tumors remain to be established
(8).
Pre-operative diagnosis of gastric glomus tumors is
challenging and requires a multi-faculty medical approach. On
unenhanced CT, they manifest as well-circumscribed submucosal
masses with homogeneous density and may contain tiny flecks of
calcification. Following the administration of contrast medium,
these tumors demonstrate strong enhancement on arterial-phase scans
and persistent enhancement on portal venous-phase scans (2). By contrast, the density of
gastrointestinal stromal tumors is lower and these do not exhibit
prolonged enhancement in the delayed phase (9). EUS features of gastric glomus tumors
are heterogeneous, hypoechoic or hyperechoic, and hypervascular
masses with internal hyperechoic spots and few tubular structures,
mostly located on the fourth echolayer (10,11).
CT and EUS are useful in the early identification of gastric glomus
tumors, particularly in terms of assessing tumor blood supply
(12). On magnetic resonance
images, gastric glomus tumors are marginally hypointense on
T1-weighted images, slightly hyperintense on T2-weighted images,
and hypervascular. In addition, gastric glomus tumors exhibit
persistent enhancement following gadopentetate dimeglumine
administration (13).
Immunohistochemistry (IHC) is the preferred diagnostic tool, by
which distinctive small, uniform and round tumor cells surrounding
capillaries can be found, which are strongly positive for SMA,
vimentin, calponin, collagen type IV and laminin (14).
Fine needle aspiration (FNA) can distinguish glomus
tumors from more aggressive gastric tumors rapidly and
pre-operatively, avoiding extensive surgical resection,
particularly in larger tumors (8,15,16).
However, FNA can also incorrectly diagnose glomus tumors as
leiomyomas or well-differentiated neuroendocrine tumors (2). Recently, Mohanty et al reported
a case of gastric glomus tumor diagnosed by EUS-guided FNA and cell
block IHC prior to endoscopic submucosal resection (ESMR) (17).
Complete surgical excision is the optimal treatment
for a single lesion (18), although
subtotal gastrectomy has been proposed for tumors suspected of
malignancy (1). To minimize
surgical trauma and the inflammatory response, the benign nature
and small median size [varying between 2 and 3 cm (19)] of glomus tumors allows them to be
removed by laparoscopic wedge resection (9,20–22),
or endoscopic submucosal enucleation in select cases (22,23)
where the lesion is not close to the pylorus, porta hepatis and
along the lesser curvature (24).
In summary, gastric glomus tumors are rare solitary
submucosal tumors for which pre-operative diagnosis is challenging.
Imaging findings assist significantly in making differential
diagnoses. FNA with IHC may also be a promising method of
diagnosis, helping the surgeon to plan an ESMR rather than more
radical surgery. Exact diagnosis relies on histopathological
examinations. Local resection by open or laparoscopic surgery is
usually the most efficient therapy, although endoscopic submucosal
enucleation may be another effective treatment.
Acknowledgements
The authors are grateful to Jing-Hong Xu, Department
of Pathology, The Second Affiliated Hospital, College of Medicine,
Zhejiang University, Hangzhou, China, for advice on
histopathological examinations and helpful discussions.
References
|
1
|
Lee HW, Lee JJ, Yang DH and Lee BH: A
clinicopathologic study of glomus tumor of the stomach. J Clin
Gastroenterol. 40:717–720. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Vassiliou I, Tympa A, Theodosopoulos T, et
al: Gastric glomus tumor: a case report. World J Surg Oncol.
8:2010.
|
|
3
|
Nascimento EF, Fonte FP, Mendonça RL,
Nonose R, de Souza CA and Martinez CA: Glomus tumor of the stomach:
a rare cause of upper gastrointestinal bleeding. Case Rep Surg.
2011:3710822011.PubMed/NCBI
|
|
4
|
Chou HP, Tiu CM, Chen JD and Chou YH:
Glomus tumor in the stomach. Abdom Imaging. 35:390–392. 2010.
View Article : Google Scholar : PubMed/NCBI
|
|
5
|
De Busscher G: Les anatomoses
arterioveineuses de l’estomac: An ultrastructural study. Acta
Neurol Morphol. 6:87–105. 1948.
|
|
6
|
Song SE, Lee CH, Kim KA, Lee HJ and Park
CM: Malignant glomus tumor of the stomach with multiorgan
metastases: report of a case. Surg Today. 40:662–667. 2010.
View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Bray AP, Wong NA and Narayan S: Cutaneous
metastasis from gastric glomus tumour. Clin Exp Dermatol.
34:e719–e721. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Huang CC, Yu FJ, Jan CM, et al: Gastric
glomus tumor: a case report and review of the literature. Kaohsiung
J Med Sci. 26:321–326. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Baek YH, Choi SR, Lee BE and Kim GH:
Gastric glomus tumor: analysis of endosonographic characteristics
and computed tomographic findings. Dig Endosc. 25:80–83. 2013.
View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Chou KC, Yang CW and Yen HH: Rare gastric
glomus tumor causing upper gastrointestinal bleeding, with review
of the endoscopic ultrasound features. Endoscopy. 42:E58–E59. 2010.
View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Yan SL, Yeh YH, Chen CH, Yang CC, Kuo CL
and Wu HS: Gastric glomus tumor: a hypervascular submucosal tumor
on power Doppler endosonography. J Clin Ultrasound. 35:164–168.
2007. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Tang M, Hou J, Wu D, Han XY, Zeng MS and
Yao XZ: Glomus tumor in the stomach: computed tomography and
endoscopic ultrasound findings. World J Gastroenterol.
19:1327–1329. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Liu KL, Wang HP, Tseng WY, Shun CT, Chen
SJ and Tsang YM: Glomus tumor of the stomach: MRI findings. AJR Am
J Roentgenol. 185:1190–1192. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Fang HQ, Yang J, Zhang FF, Cui Y and Han
AJ: Clinicopathological features of gastric glomus tumor. World J
Gastroenterol. 16:4616–4620. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Vinette-Leduc D and Yazdi HM: Fine-needle
aspiration biopsy of a glomus tumor of the stomach. Diagn
Cytopathol. 24:340–342. 2001. View
Article : Google Scholar : PubMed/NCBI
|
|
16
|
Debol SM, Stanley MW, Mallery S, Sawinski
E and Bardales RH: Glomus tumor of the stomach: cytologic diagnosis
by endoscopic ultrasound-guided fine-needle aspiration. Diagn
Cytopathol. 28:316–321. 2003. View
Article : Google Scholar : PubMed/NCBI
|
|
17
|
Mohanty SK, Pradhan D, Stavropoulos S,
Donovan V and Gupta M: Diagnosis of gastric glomus tumour by
endoscopic ultrasound-guided fine needle aspiration cytology: a
case report. Cytopathology. May 1–2013.(Epub ahead of print).
View Article : Google Scholar
|
|
18
|
Kang G, Park HJ, Kim JY, et al: Glomus
tumor of the stomach: a clinicopathologic analysis of 10 cases and
review of the literature. Gut Liver. 6:52–57. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Miettinen M, Paal E, Lasota J and Sobin
LH: Gastrointestinal glomus tumors: a clinicopathologic,
immunohistochemical, and molecular genetic study of 32 cases. Am J
Surg Pathol. 26:301–311. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Vanwijnsberghe S, Rubay R, Descamps C,
Verdebout JM and Navez B: A glomic tumour of the stomach treated by
laparoscopy. Acta Chir Belg. 106:613–615. 2006.PubMed/NCBI
|
|
21
|
Campbell MJ, Irani S, Olgac S and Chang
LC: Laparoscopic resection of a gastric glomus tumor. Indian J
Surg. 73:230–232. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Zhang Y, Zhou P, Xu M, et al: Endoscopic
diagnosis and treatment of gastric glomus tumors. Gastrointest
Endosc. 73:371–375. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Xu M, Jiang XM, He YL, Zhang YL, Xu MD and
Yao LQ: Glomus tumor of the stomach: A case treated by endoscopic
submucosal dissection. Clin Res Hepatol Gastroenterol. 35:325–328.
2011. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Lorber J, Kalish J, Farraye FA, Cerda S
and Babineau TJ: Glomus tumor of the gastric antrum: case report.
Curr Surg. 62:436–438. 2005. View Article : Google Scholar : PubMed/NCBI
|