Introduction
Necrotizing fasciitis (NF) is a serious infectious
condition that may compromise the patient's life. It originates
from a soft tissue infection that spreads rapidly to the deep
fascia and produces secondary necrosis, with rapid evolution and
multisystem involvement. It mainly affects the lower limbs in up to
50% of cases but may also affect other areas such as the perineum
(Fournier's gangrene) and the submandibular region (Ludwig's
angina) (1,2).
NF is a rare condition, with an incidence of
0.3-5/100,000 patients and high mortality (70-80%) despite
technological advances in diagnosis and treatment. Up to 25% of
these patients have an initial misdiagnosis due to the ambiguity of
presentation and similarity with other soft tissue infections
(1,2). Early clinical diagnosis is the
determining factor to the patient's prognosis. It is necessary to
resort to diagnostic aids to identify unclear cases. However, the
limitation of physical examination and diagnostic aids in its
identification is known; thus, the method for differentiating
necrotizing from non-necrotizing infections is surgical exploration
(1,3).
On physical examination, the external findings of NF
are generally not consistent with the severity of manifestations
expressed by the patient. In addition, they are similar to other
less serious soft tissue infections. When relevant and
characteristic clinical findings are present, the infection is
usually already in advanced stages. The presence of fever,
hemorrhagic bullae and hypotension have a sensitivity of <50%,
but the latter two findings have a specificity of >90%, i.e.,
the absence of these signs on physical examination does not
necessarily rule out the disease (1).
Certain paraclinical tests are used as a diagnostic
aid. Among them, the Laboratory Risk Indicator for NECrotizing
fasciitis score (LRINEC) is a validated tool to differentiate NF
from other soft tissue infections, with a cut-off at ≥6 points for
a diagnostic probability of 50-75%, with a sensitivity of 68% and
specificity of 84%. However, a negative LRINEC does not necessarily
rule out the disease, because with a moderate pre-test probability,
there is still a ~25% chance of presenting with NF. Higher cut-off
points sacrifice sensitivity to improve specificity (1).
Axial computerized tomography (CT) is used in the
diagnostic process of this pathology, with findings suggestive of
fasciitis and the presence of air or gas around the fascia. It has
a sensitivity of 88% and a specificity of 93%, but looking for
other suggestive signs, such as soft tissue edema or fascial
thickening, increases the sensitivity but decreases the specificity
of the test. A limitation of this test is the delay in care times,
particularly in surgical management (1).
Ultrasound may indicate certain signs suggestive of
NF, such as the identification of gas in soft tissues with small
hyperechoic lines above the fascia, acoustic shadowing and the
presence of irregularity, and/or thickening of the fascia. Other
described findings are the hyperechogenicity of the fat overlying
the fascia, and the cobblestone-like appearance that indicates
subcutaneous edema; in addition, in tissues underlying the fascia
(beyond 4 mm), the presence of hypoechogenicity is indicative of
edema. A sensitivity of 88% and a specificity of 93% for the
diagnosis of NF have been reported for this test (2,4).
Ultrasound is a cost-effective, non-invasive tool,
useful for early diagnosis or diagnostic guidance, allowing early
decision-making, although CT and magnetic resonance imaging (MRI)
subsequently rule out the diagnosis (4,5).
Recently, point-of-care ultrasonography (PoCUS)
demonstrated its usefulness in the diagnosis of soft tissue
infections (6). Furthermore, its
portability allows rapid identification of necrotizing fasciitis,
reducing morbidity and mortality (3). PoCUS has also been reported to be
useful in emergency departments to evaluate patients with soft
tissue infections and has also been indicated to help differentiate
abscesses from cellulitis (7,8).
As only a small number of studies have described the
use of PoCUS in the diagnostic approach for patients with NF, the
present case study demonstrates its utility in this setting,
compared to more specific tools such as CT and MRI, to define
whether it may be implemented as a diagnostic aid in care
protocols.
Case report
A 42-year-old male patient with a history of peptic
acid disease and previous smoking, treated with omeprazole, with no
other relevant history, consulted the emergency department of a
high-complexity institution due to a one-day episode of increased
pain in the region of the neck and sensation of dyspnea, which was
exacerbated after lifting a heavy object, radiating to the
retrosternal region, with subsequent appearance of edema and
erythema in the same area of pain.
The patient reported the presence of subjective
fever, general malaise, myalgias, non-productive cough, dysphagia
and neck pain ~1 week prior to admission. Initially, the patient
did not consult any clinic and decided to self-medicate; however,
he did not remember the medications taken to control the
symptoms.
The patient presented at Hospital San Vicente
Fundación (Rionegro, Colombia) in May 2022. Vital signs-associated
parameters on admission indicated oxygen saturation below the
normal percentage, without any other alterations. Physical
examination revealed pain on palpation, edema and erythema in the
anterior region of the neck and upper third of the chest, without
any lesions or abscesses in the oropharyngeal cavity, crepitus in
lung bases predominantly right, without any signs of respiratory
distress and without any other abnormal findings on physical
examination.
Vascular dissection was considered an initial
diagnostic suspicion; thus, angiotomography of neck vessels was
performed, ruling out aortic and neck vessel dissection. The
radiology reading indicated a negative result for aortic syndrome
and cervical vascular disease, but with cervical-mediastinal edema
with lamellar fluid between muscular and fatty planes, posterior
pulmonary atelectasis, without pleural fluid, without
consolidations and tonsillar hypertrophy and without abscesses.
In addition, the paraclinical tests indicated an
increase in acute phase reactants [leukocytes, 19,200/ml (normal
range, 4,500-11,500/ml); neutrophils, 16,950/ml (normal range,
2,000-7,500/ml); and C-reactive protein (CRP), 34.6 mg/dl (normal
range, 0,4-1 mg/dl)]; cellulitis without abscess was then
considered. The patient was hospitalized and antibiotic management
was started (clindamycin 900 mg every 8 h). Blood culture was also
requested.
Due to the rapid evolution of the condition, the
presence of dyspnea with the need for supplemental oxygen, and the
disproportion between the intensity of the pain described by the
patient and the external findings observed, NF was considered.
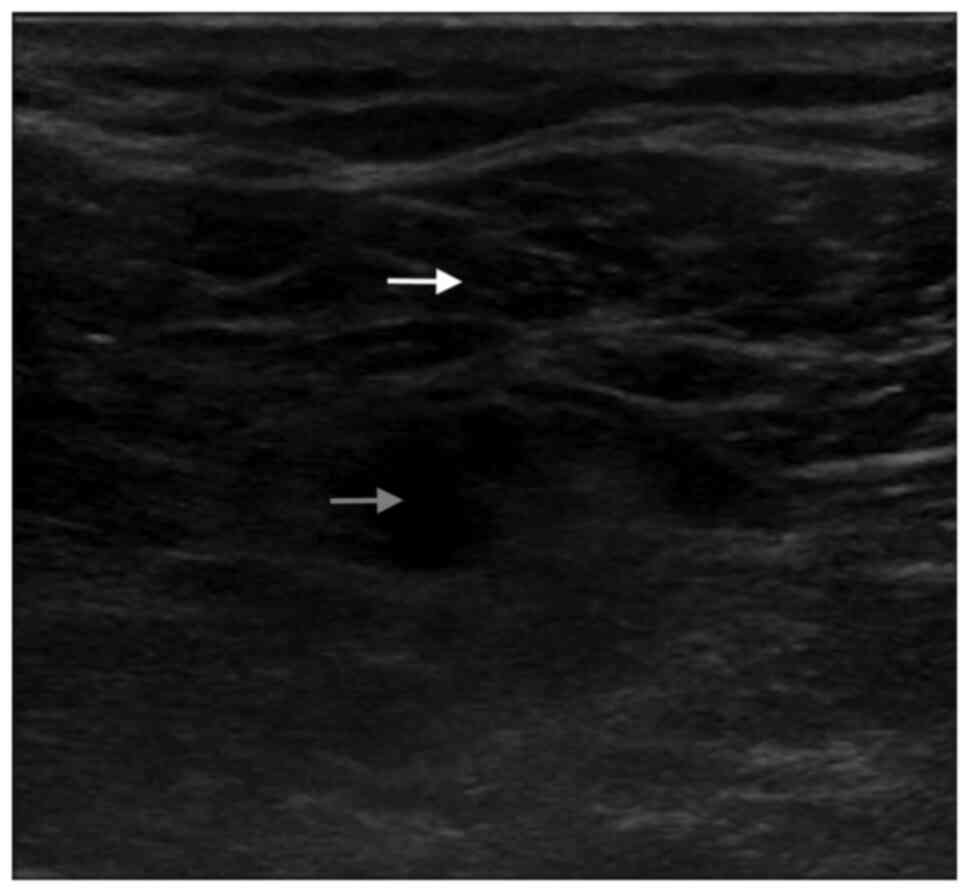
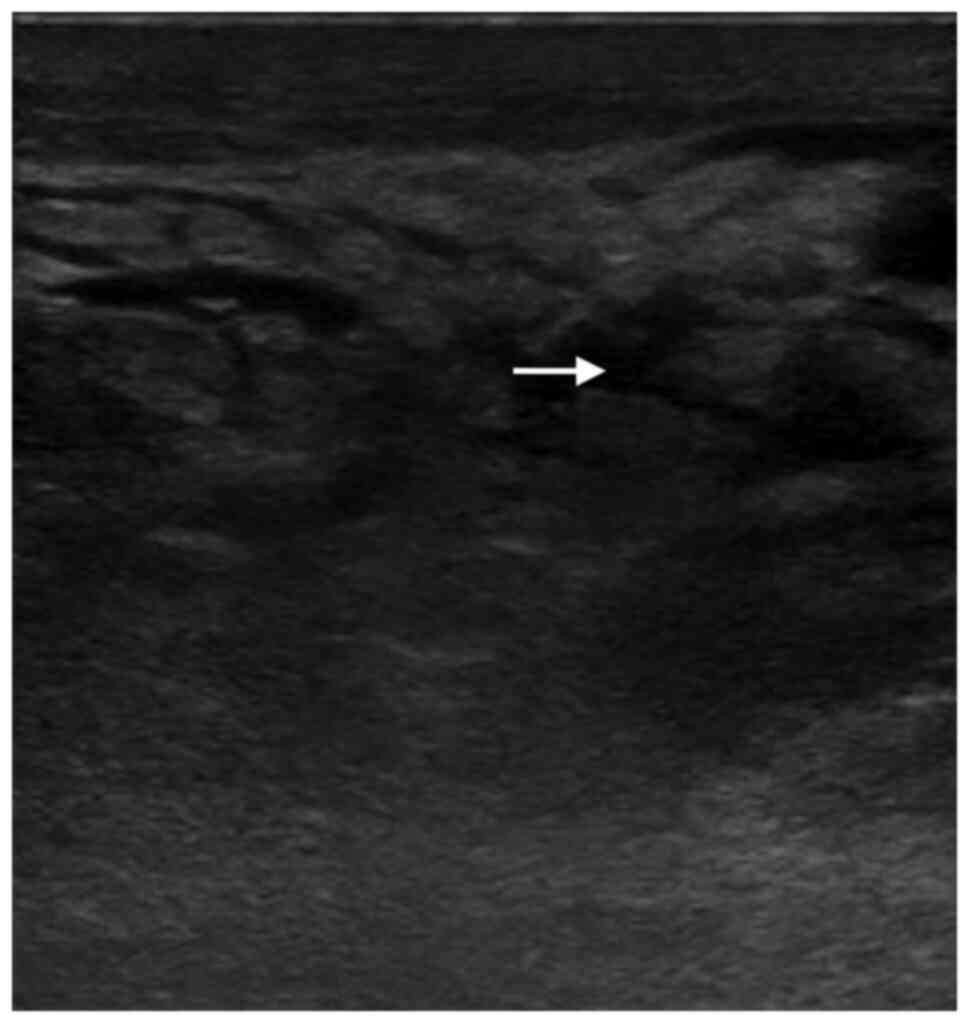
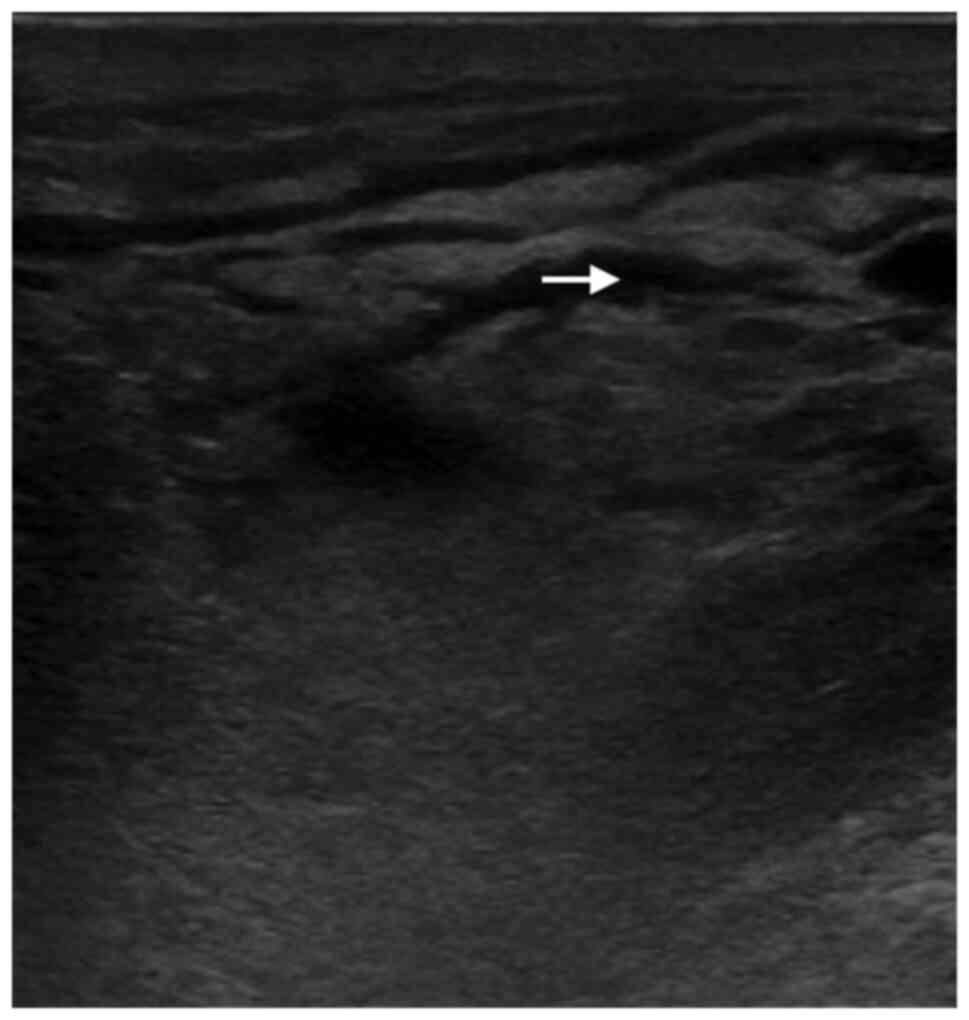
PoCUS was performed, evidencing a cobblestone-like pattern of the
subcutaneous cellular tissue, with diffuse thickening of the
anterior cervical fascia and increased echogenicity with soft
tissue edema posterior to the fascia (Fig. 1, Fig.
2 and Fig. 3).
According to the diagnostic suspicion, it was
decided to hospitalize the patient in a special care unit.
Antibiotic therapy (vancomycin 1.4 g every 12 h and
piperacillin-tazobactam 4.5 g every 6 h) was escalated until blood
culture results, and evaluation for general surgery and chest
surgery was requested.
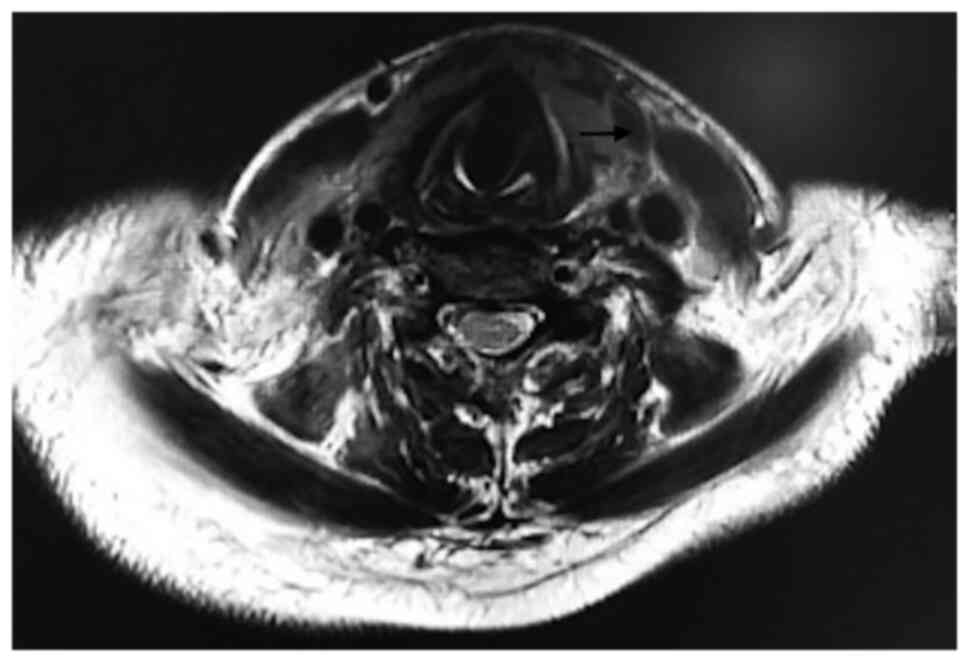
During the hospital stay, the patient presented a
torpid evolution, with little improvement in pain, a persistent
need for supplemental oxygen at low flow, and an increase in acute
phase reactants (leukocytes, 26,500/ml; neutrophils, 23,690/ml;
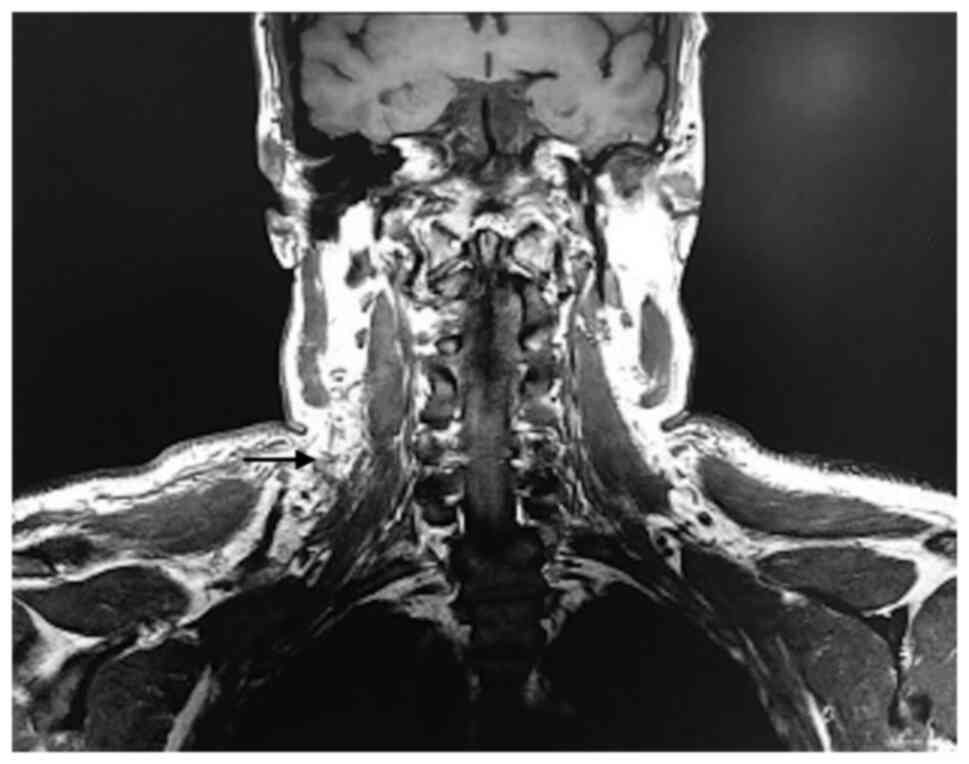
CRP, 22.51 mg/dl), and with negative blood cultures at 72 h. In
addition, the chest MRI revealed cellulitis, myositis and fasciitis
in the anterior wall of the chest inlet, and signs of infectious
mediastinitis, with multifocal abscesses distributed in the
anterior region of the visceral space (laminar), right paratracheal
region to the height of the sternoclavicular joint, anterior
paratracheal up to the carina (laminar) and cranial to the arch of
the azygos of probable bacterial origin (Figs. 4 and 5).
Due to the finding of mediastinitis and a history of
chest pain, it was decided to rule out an inadvertent injury to the
esophagus, and an upper gastrointestinal endoscopy was then
performed. During this procedure, a highly swollen airway was
observed. Furthermore, before the start of the procedure, dyspnea
and subcostal retractions were observed, but with adequate
saturation with low oxygen flow. Due to the above, the procedure
was completed without any evident injuries to the esophagus. The
patient was intubated due to the imminent risk of airway loss and
was transferred to the intensive care unit. After 20 days, the
patient was discharged from the intensive care unit and remained
hospitalized for another 10 days before being discharged.
Antibiotics were prescribed for two weeks and the patient was
scheduled for regular check-ups. In the last check-up after two
months of being discharged, the patient was in an adequate health
state.
Discussion
In the current case, the patient presented with
nonspecific manifestations with inflammatory changes in the soft
tissues of the neck, which were initially interpreted as
cellulitis, but given the progressive deterioration, the
discrepancy between the inflammatory changes observed and the
severity of the symptoms, the diagnosis of NF was considered. The
patient provided a diagnostic challenge due to the manifestations
described that diverted the focus to other pathologies that were
then to be ruled out. Furthermore, the patient did not have any
significant pathological or traumatic history that may have led to
soft tissue infection. In addition, the lesion was found in an
unusual area.
Cervical NF is a rare pathology that mainly affects
patients with immunosuppressive conditions (e.g. diabetes mellitus,
HIV, alcoholism, cirrhosis, malignancy and chronic steroid use) and
there is usually a known source of infection (e.g. odontogenic,
oropharyngeal, traumatic or cutaneous); however, in ~10% of cases,
there is no identified cause (5).
As previously described, to decrease morbidity and
mortality rates in patients with NF, early diagnosis is required.
However, the physical examination is not specific in the early
stages of the disease; furthermore, waiting for characteristic
findings to appear also increases the probability of death
(4). Waiting for paraclinical and
imaging results to make decisions also delays the start of measures
that have an impact on morbidity and survival, which is why
diagnostic aids are required that allow early and rapid
identification with acceptable diagnostic accuracy, which promotes
early therapeutic decision-making.
In this way, PoCUS has been a tool which, in recent
decades, has gained ground for the evaluation of multiple
conditions in emergency services, helping in early decision-making
in time-sensitive conditions (7,8).
Although there are descriptions of the characteristics identified
by ultrasound of soft tissue infections, only a small number of
studies are available on the usefulness of PoCUS in diagnosis and
its efficacy in improving outcomes compared to current
protocols.
A recent prospective study compared the findings of
PoCUS in patients with suspected NF at the emergency department,
with the results obtained by CT and/or surgical evaluation. A
sensitivity of 100%, specificity of 98%, positive predictive value
of 89% and negative predictive value of 100% were obtained, with an
area under the curve of 99%, with thickening of the fascia and
edema between planes being the more frequent findings, in addition
to the presence of hyperechoic foci suggestive of air, a late
finding in the presentation of fasciitis. The study indicated that
PoCUS may be used to identify NF with high sensitivity and
specificity (3).
The present case report corroborates the usefulness
of PoCUS as a tool of easy and rapid access in situations of
non-timely availability of other diagnostic tools, which in
suggestive clinical conditions and with early ultrasound findings
typical of soft tissue infection, allows ruling out or confirming
more serious conditions, allowing for the prompt initiation of
treatments or decisions that impact outcomes.
In conclusion, PoCUS, in the context of serious soft
tissue infections, is a good tool that allows for the
differentiation of superficial infections from those that are deep
and abscessed, an aspect that influences treatment decisions.
Furthermore, in the appropriate clinical context, it allows the
diagnosis of necrotizing infections, with specific ultrasound signs
that are indicative of a serious compromise. It also allows to
identify the condition in the early stages, facilitating
therapeutic decision-making that reduces morbidity and
mortality.
Acknowledgements
Not applicable.
Funding
Funding: No funding was received.
Availability of data and materials
The datasets used and/or analyzed during the present
study are available from the corresponding author on reasonable
request.
Authors' contributions
WCC, MZG, DGA and CMA contributed to the conception
and design of the study. CMA wrote the manuscript. WCC and CMA
searched the literature. WCC, MZG and DGA provided clinical
assistance to the patient and were responsible for the treatments.
DGA and CMA revised the manuscript. MZG and CMA confirm the
authenticity of all the raw data. All authors have read and
approved the final manuscript.
Ethics approval and consent to
participate
The Bioethics Committee of San Vicente Fundación
Hospital (Rionegro, Colombia) approved the publication of this
case.
Patient consent for publication
Written informed consent for the publication of
clinical details and images was obtained from the patient.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Fernando SM, Tran A, Cheng W, Rochwerg B,
Kyeremanteng K, Seely AJE, Inaba K and Perry JJ: Necrotizing soft
tissue infection: Diagnostic accuracy of physical examination,
imaging, and LRINEC score: A systematic review and meta-analysis.
Ann Surg. 269:58–65. 2019.PubMed/NCBI View Article : Google Scholar
|
|
2
|
Tso DK and Singh AK: Necrotizing fasciitis
of the lower extremity: Imaging pearls and pitfalls. Br J Radiol.
91(20180093)2018.PubMed/NCBI View Article : Google Scholar
|
|
3
|
Lahham S, Shniter I, Desai M, Andary R,
Saadat S, Fox JC and Pierce S: Point of care ultrasound in the
diagnosis of necrotizing fasciitis. Am J Emerg Med. 51:397–400.
2022.PubMed/NCBI View Article : Google Scholar
|
|
4
|
Lin CN, Hsiao CT, Chang CP, Huang TY,
Hsiao KY, Chen YC and Fann WC: The relationship between fluid
accumulation in ultrasonography and the diagnosis and prognosis of
patients with necrotizing fasciitis. Ultrasound Med Biol.
45:1545–1550. 2019.PubMed/NCBI View Article : Google Scholar
|
|
5
|
Sideris G, Nikolopoulos T and Delides A:
Cervical necrotizing fasciitis affects only immunocompromized
patients? Diagnostic challenges, treatment outcomes and clinical
management of eleven immunocompetent adult patients with a still
fatal disease. Am J Otolaryngol. 41(102613)2020.PubMed/NCBI View Article : Google Scholar
|
|
6
|
Subramaniam S, Bober J, Chao J and
Zehtabchi S: Point-of-care ultrasound for diagnosis of abscess in
skin and soft tissue infections. Acad Emerg Med. 23:1298–1306.
2016.PubMed/NCBI View Article : Google Scholar
|
|
7
|
Hakkarainen TW, Kopari NM, Pham TN and
Evans HL: Necrotizing soft tissue infections: Review and current
concepts in treatment, systems of care, and outcomes. Curr Probl
Surg. 51:344–362. 2014.PubMed/NCBI View Article : Google Scholar
|
|
8
|
Kaafarani HM and King DR: Necrotizing skin
and soft tissue infections. Surg Clin North Am. 94:155–163.
2014.PubMed/NCBI View Article : Google Scholar
|