Introduction
Coronavirus disease 2019 (COVID-19) is an infectious
disease that continues to have a major worldwide impact.
Governments have been imposing strong infection control measures to
minimise the negative impacts of COVID-19, such as maintaining
physical distancing and wearing masks (1). It is important to provide prompt and
high-quality medical care for patients with COVID-19 who require
medical interventions. Thus, pharmacists, as members of the
healthcare team, have an important responsibility to improve the
quality of drug therapy.
While numerous efforts have been made by healthcare
providers to improve the quality of care for patients with
COVID-19, the role of the pharmacist in this process has remained
to be clarified (2,3). The pharmacist's role has been proposed
to include medication counselling, management of long-term
prescriptions to reduce the frequency of hospital visits and drug
delivery (4,5). These activities are generally related
to supporting outpatient care for patients with comorbidities who
require long-term management, although there are several consistent
recommendations regarding the tasks expected of pharmacists for
patients hospitalised with COVID-19 (6,3).
Simply put, pharmacists should support pharmaceutical care services
by participating in making evidence-based decisions for medication,
monitoring and evaluating medication safety and efficacy, providing
enhanced care for special populations and patients with combined
underlying diseases, monitoring and management of convalescent
plasma therapy, providing emotional counselling and psychological
support, and providing scientific information about COVID-19
vaccines. However, there have been few studies on pharmacists'
actual approaches to inpatient pharmacotherapy in the context of
COVID-19(7).
At the same time, there is abundant evidence for the
role of pharmacists in managing hospitalised patients without
COVID-19. The Society of Critical Care Medicine has proposed 82
types of roles for pharmacists, including patient care and
improving the quality of medical care. Above all, ensuring the
safety and effectiveness of drug therapy is an essential task for
pharmacists (8). Patients with
severe COVID-19 require endotracheal intubation and must receive
multidisciplinary treatment. Among these, drug therapy occupies an
important place, with antiviral therapy centered on remdecivir,
immunomodulatory therapy with steroids and tocilizumab, and
anticoagulation therapy. Numerous other drugs are also in use,
including antimicrobial therapy for complicated infections and
analgesics and sedatives for pain during endotracheal intubation.
Therefore, pharmacists, as experts in pharmacology, need to
contribute to safe and effective drug therapy.
Against this background, the present study
retrospectively examined pharmacist interventions among
hospitalised patients with COVID-19, particularly severe cases. By
doing so, the present study aimed to clarify the pharmacist's role
in COVID-19 inpatient admissions and to identify standardised tasks
to be performed by pharmacists.
Patients and methods
Selection of cases
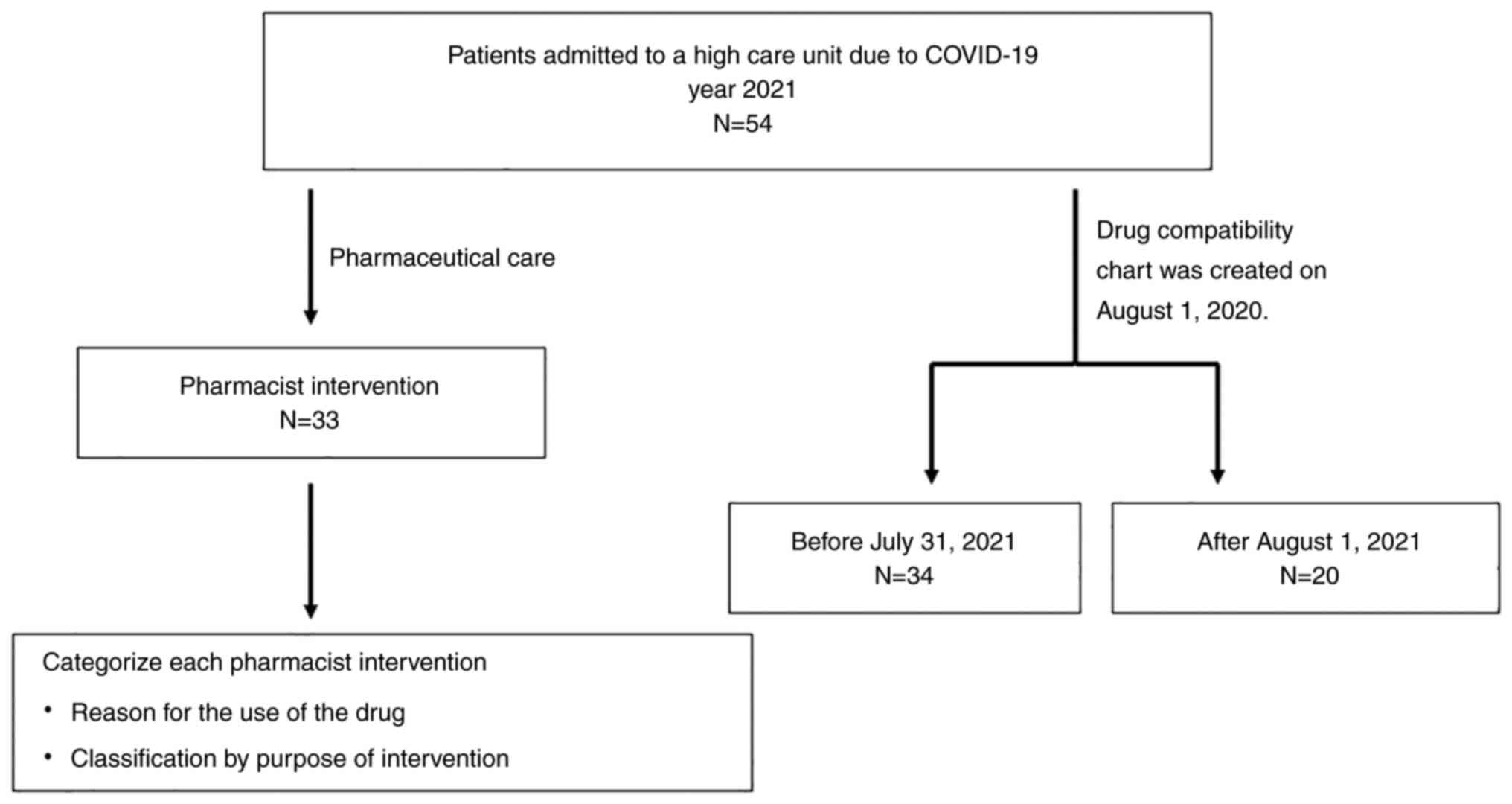
Patients with COVID-19 admitted to the emergency
center of Ogaki Municipal Hospital (Ogaki, Japan) between the 1st
of January and 31st of December 2021 were included in the present
study. Enrolment in this study was done retrospectively. This
hospital had been designated as a COVID-19 priority medical
institution in the Gifu Prefecture of Japan; nine beds in the
emergency center were reserved for patients with severe COVID-19 or
those at high risk of severe disease. This study included all
patients who used these beds. An overview of the present study is
provided in Fig. 1.
Intervention by pharmacists
During the study period, the clinical pharmacist in
charge of ward pharmacy services at the high-care units provided
pharmacological management for patients with COVID-19. The
high-care unit is a ward that is commonly used in Japan to care for
critically ill patients, similar to the intensive care unit. A
clinical pharmacist collected patient information from electronic
medical records to perform pharmacy management, and in addition,
information was collected from physicians, nurses and other
healthcare professionals as necessary. For severe cases of
COVID-19, the pharmacist participated in weekday conferences with
physicians, nurses, physical therapists and clinical engineering
technicians to share information. The pharmacist addressed
pharmacological management issues and interventions to improve the
quality of patient care.
In addition, to aid comprehension of drug
compatibility for injectable drugs, a drug compatibility chart was
created exclusively for patients with COVID-19, which had been put
into operation on the 1st of August 2021. The drug compatibility
chart was limited to those drugs that were frequently used by
physicians dealing with severe cases. The chart was also designed
concisely so that it could be easily referred to, even during busy
working hours while wearing personal protective equipment. In
addition, it depicted examples of intravenous injection route
combinations of the commonly used drugs. This table was prepared
with reference to those that have been reported to be useful in the
past (9,10). The chart is presented in Table I.
 | Table IDrug compatibility chart for severe
COVID-19 cases: Combination of continuous injections that should
not be mixed. |
Table I
Drug compatibility chart for severe
COVID-19 cases: Combination of continuous injections that should
not be mixed.
| Drugs | Amino acid | Dobutamine | Nicardipine | Nor-adrenaline | hANP | Insulin | Furosemide | Heparin |
|---|
| Amino acid | | | x | | x | | | |
| Dobutamine | | | | | x | | | x |
| Nicardipine | x | | | | | x | | |
| Nor-adrenaline | | | | | | x | | |
| hANP | x | x | | | | x | x | x |
| Insulin | | | x | x | x | | | |
| Furosemide | | | | | x | | | |
| Heparin | | x | | | x | | | |
Evaluation methods
Interventions by pharmacists were classified
according to their content. Two methods were used for
classification. First, the interventions were classified according
to the reason for the use of the drug that was the subject of the
intervention and its pathophysiology. For instance, a case in which
the pharmacist proposed steroid administration considering the
stage of COVID-19 or discontinuation of remdesivir was classified
as an ‘intervention for COVID-19 drugs’. Second, referring to
previous research (6,3), the interventions were categorised
according to their purpose: i) Evidence-based decisions for
medication; ii) medication safety; iii) medication efficacy; iv)
drug interaction and management; v) pharmaceutical care for special
populations; and vi) pharmaceutical care for patients with combined
underlying diseases. Each item was counted for interventions
relating to multiple items. For instance, designing antimicrobial
dosing for haemodialysis patients fulfilled items ii), iii) and v).
Pharmacist interventions that were continuous over a long period,
such as drug blood level monitoring, were counted as a single
intervention.
In the present study, patients were classified by
respiratory physicians upon admission according to the severity
classification widely used in Japan (11): Mild disease (no pneumonia), moderate
disease I (no respiratory failure), moderate disease II (pneumonia
but no ventilatory management) or severe disease (mechanical
ventilation required).
Statistical analysis
The usefulness of the injectable drug compatibility
chart was evaluated using Fisher's exact test for the proportion of
intervention cases prior to and after the start of its operation.
EZRver2.3 (The R Foundation for Statistical Computing) was used for
all statistical analyses. P<0.05 was considered to indicate
statistical significance.
Results
Patient characteristics
A total of 54 patients were included in the present
study, with 33 cases of severe disease and 16 cases of moderate
disease II. There were also 2 mild and 3 moderate I cases who were
considered to be at high risk for severe disease. Details on the
patients' backgrounds are presented in Table II. Of these patients, 28 (52%) were
subjected to pharmacist interventions, 25 of which were severe
cases. There were 68 pharmacist interventions in total.
| Table IIPatient characteristics (n=54). |
Table II
Patient characteristics (n=54).
| Parameter | Value |
|---|
| Age, years | 64 (50-73) |
| Male sex | 37 (68.5) |
| Body mass index,
kg/m2 | 25.9 (22.3-31.5) |
| Body weight, kg | 69.5 (57.3-86) |
| Hemodialysis
treatment | 2 (3.7) |
| Underlying
diseases | |
|
Diabetes | 17 (31.4) |
|
Hypertension | 11 (20.3) |
|
Stroke | 8 (14.8) |
|
Pulmonary
diseasesa | 7 (13.0) |
|
Tumor | 3 (5.6) |
| Severityb | |
|
Mild | 2 (3.7) |
|
Moderate
I | 3 (5.6) |
|
Moderate
II | 16 (29.6) |
|
Severe | 33 (61.1) |
| Medical
intervention | |
|
Mechanical
ventilation | 32 (59.3) |
|
Extracorporeal
membrane oxygenation | 2 (3.7) |
|
Remdesivir | 47 (87.0) |
|
Steroid | 50 (92.6) |
|
Antithrombotic
drugs | 18 (33.3) |
|
Antibiotics | 36 (66.7) |
| Intubation or until
tracheostomy, days | 14 (11-20) |
| Length of stay,
days | 24 (15-38) |
| Length of stay in
high care unit, days | 13 (5-19) |
| Clinical outcome | |
|
Home
discharge | 35 (64.8) |
|
Transfer or
institutional discharge | 7 (13.0) |
|
Death | 13 (24.1) |
Classification of pharmacist
interventions for patients with COVID-19
The classification of pharmacist interventions is
indicated in Table III. In terms
of target drugs or conditions, antimicrobial interventions were the
most common, accounting for 28 cases (41.2%). This was followed by
interventions related to nutrition and infusion (10.3%), as well as
COVID-19 drugs (8.8%). In addition, according to the abovementioned
classification, based on previous studies (6,3),
interventions related to the safe use of medicines were the most
common, followed by interventions focused on achieving high
efficacy.
| Table IIIClassification of pharmacological
interventions. |
Table III
Classification of pharmacological
interventions.
| A, Classification by
target drug or condition of intervention (n=68) |
|---|
| Pharmacological
intervention | N |
|---|
| Antimicrobial
agent | 28 |
| Nutritional
supplements and infusions | 7 |
| Anti-COVID-19
drugs | 6 |
| Antithrombotic
drugs | 5 |
| Medication for
underlying diseases | 4 |
| Sedation and delirium
medications | 2 |
| Diuretics | 2 |
| Others | 1 |
| Compatibility
management | 13 |
| B, Classification
based on previous studies (n=68 cases) (3,7) |
| Pharmacological
intervention | N |
| Evidence-based
decision-making for medication | 6 |
| Monitoring and
evaluation of medication safety | 37 |
| Monitoring and
evaluation of medication efficacy | 28 |
| Drug interaction
management | 14 |
| Pharmaceutical care
for special populations | 17 |
| Pharmaceutical care
for patients with combined underlying diseases | 5 |
| Others | 2 |
Table IV provides
examples of pharmacist interventions for the patient population of
the present study. The most common intervention was the
recommendation to change to an appropriate antimicrobial agent due
to the detection of drug-resistant bacteria. The most common
intervention was to suggest appropriate antimicrobials for
drug-resistant organisms. Another common intervention was
therapeutic drug monitoring to maximize efficacy and contribute to
safety.
| Table IVExamples of pharmaceutical
interventions. |
Table IV
Examples of pharmaceutical
interventions.
| Summary of
pharmaceutical intervention | Intervention target
drugs | Expected
benefits | Number of cases
with similar interventions within the present study |
|---|
| Therapeutic drug
monitoring of vancomycin in patients with severe obesity or renal
failure | Antibiotics | Maximisation of
effectiveness and minimisation of side effects | 7 |
| Recommendation to
change to an appropriate antimicrobial due to the detection of
drug-resistant bacteria | Antibiotics | Maximisation of
effectiveness | 8 |
| Recommendations for
antimicrobial dosing according to renal function and other
factors | Antibiotics | Maximisation of
effectiveness and minimisation of side effects | 4 |
| Recommendation to
end unnecessary zinc supplementation | Nutritional
supplements | Minimisation of
side effects; cost reduction | 2 |
| Recommendation to
change from oligomeric formula enteral nutrition to polymeric
formula enteral nutrition for patients without gastrointestinal
tract function problems | Nutritional
supplements | Increase of
physiological nutrient supply | 2 |
| Recommendation to
discontinue remdesivir in palliative treatment patients | Anti-COVID-19
drugs | Minimisation of
side effects; cost reduction | 1 |
| Recommendation to
discontinue remdesivir dosing beyond 10 days | Anti-COVID-19
drugs | Evidence-based
treatment practices; cost reduction | 1 |
| Recommendations for
anticoagulant use or activated partial thromboplastin time
monitoring in patients experiencing atrial fibrillation | Antithrombotic
drugs | Evidence-based
treatment practices | 4 |
| Recommendations not
to interrupt antiplatelet medications in patients with a history of
myocardial infarction | Medication for
underlying diseases | Evidence-based
treatment practices | 2 |
| Recommendation to
discontinue diuretics in anuric patients dependent on
hemodialysis | Diuretics | Minimisation of
side effects; cost reduction | 1 |
Outcomes from the use of the specific
COVID-19 treatment drug compatibility chart
Before to the use of the drug compatibility chart,
pharmacist interventions for drug compatibility were provided to 9
of 34 patients (26.5%). After its use, 3 of 20 patients (15.0%)
received interventions. There was no statistically significant
difference between the two groups (P=0.5). With regard to severe
cases, interventions were performed in 9 of 21 (42.9%) cases before
the chart's use and 3 of 12 (25%) cases after its use. There was no
significant difference between the two groups (P=0.5). Obstruction
of the intravenous administration route occurred once before and
once after the use of the drug compatibility chart.
Discussion
The present study provides information on the role
of pharmacists in team care for patients with COVID-19 admitted to
an intensive care unit. The study demonstrates that several
pharmacist interventions are used, particularly for severely ill
patients with COVID-19. In other words, pharmacists may improve the
quality of drug treatments for patients with COVID-19 through a
variety of interventions. The study also suggests that providing
information about antimicrobials and combination changes to
patients with COVID-19 is an important task for pharmacists.
Klopotowska et al (12) reported that antimicrobial-related
interventions accounted for 23.4% of all prescribing interventions
by resident pharmacists in intensive care units. In the present
study, antimicrobial-related interventions accounted for the
largest proportion of pharmacist interventions, i.e. ~40%. The
reason for the higher rate of antimicrobial interventions than in
previous studies may be that secondary bacterial infections
frequently occur in patients with COVID-19. Infections caused by
drug-resistant organisms such as methicillin-resistant
Staphylococcus aureus are particularly problematic in severe
cases (13). In general, the
treatment of drug-resistant organisms frequently involves a
difficult choice of antimicrobial agents; drugs that require
therapeutic drug monitoring, such as vancomycin, are often
necessary. In addition, severe COVID-19 cases frequently occur
among elderly patients with impaired organ function and obese
patients, for whom drug doses must be carefully adjusted (14,15).
Furthermore, while intravenous antimicrobials are used in >80%
of patients with severe COVID-19(16), complications from bacterial
infection are thought to occur in ~8% of cases (17). Thus, the inappropriate use of
antimicrobial agents may be an issue; therefore, such treatments
must be optimised. Accordingly, pharmacists with expertise in
antimicrobial chemotherapy are expected to have a significant role
in the care of critically ill patients with COVID-19.
Providing information on drug compatibility
accounted for 19% of the pharmacist interventions. In the present
study, pharmacists were unable to perform bedside intravenous drip
route checks from an infection control perspective. Therefore,
interventions were required to be based on prescription details and
information about the intravenous route from care team members,
considering the risk of drug compatibility. Consequently, the route
of administration was required to be discussed for most cases over
time, which required significant effort among care team members.
Pharmacists attempted to simplify this process by creating a drug
compatibility chart.
In the present study, the usefulness of the chart
could not be statistically confirmed. However, after the creation
of the drug compatibility chart, the number of situations in which
pharmacist interventions were necessary decreased by ~43%, which
may have reduced the burden on the medical team and on the
patients. There have been several studies on drug compatibility
charts and their usefulness (9,10).
However, no studies have focused on the creation of a chart
tailored to the characteristics of COVID-19. In caring for patients
with COVID-19, the creation of individualised tools that focus only
on drugs suitable for these patients and are easily visible even
when personal protective equipment is required. Creating effective
tools to minimise drug-related problems is an important
responsibility for pharmacists.
The present study has several limitations. First,
the study reported from a single center and thus did not consider
the impact of facility conditions and care team skills. Another
limitation is the small sample size. The sample size and
intervention rate of the present study yielded a statistical power
of 0.09; this value is low and the results should thus be
interpreted with caution. However, the 43% reduction in the
requirement of pharmacist intervention for drug compatibility is
clinically important. Furthermore, the present study analysed the
content of pharmacist interventions; however, there is limited
information on whether these interventions led to improved clinical
outcomes. In addition, as pharmacy management was conducted without
any direct patient observation in terms of infection control,
information related to efficacy and side effects was only obtained
at the case review by the care team, which may have led to a
decrease in the quality and number of interventions. It is esteemed
that future studies will address these issues.
COVID-19 is a new infectious disease with a short
history and its pharmacological treatment is still evolving. In the
present study, interventions were applied that led to the
appropriate use of remdesivir. In other words, pharmacists are
required to organise information about COVID-19 drugs and provide
interventions that promote their proper use. In addition, diabetes
mellitus and cerebral infarction have been reported as risk factors
regarding the severity of COVID-19 and a large proportion of
patients with underlying diseases are at risk (18). In other words, numerous patients
with COVID-19 are taking certain medications prior to admission and
supporting seamless pharmacy management for patients with severe
disease is a key task for pharmacists.
In summary, the present study indicated that
pharmacists have a responsibility to improve the quality of
pharmacotherapy for patients with COVID-19, with a focus on
creating specific medication-related tools and supporting the
appropriate use of antimicrobials for secondary bacterial
infections.
Acknowledgements
Not applicable.
Funding
Funding: No funding was received.
Availability of data and materials
The datasets generated and analyzed in this study
are available from the corresponding author upon reasonable
request.
Authors' contributions
YS conceived and designed the study, acquired and
interpreted the data and wrote the manuscript. KO, TM and TY
contributed to the interpretation of the data. All authors have
read and approved the final manuscript. YS, KO, TM and TY reviewed
manuscript and confirm the authenticity of all the raw data.
Ethics approval and consent to
participate
In accordance with the ethical code of our hospital,
opt-out consent was obtained for all patients. This study was
conducted in accordance with the Ethical Guidelines in Japan with
approval from the Clinical Research Review Committee at Ogaki
Municipal Hospital (Ogaki, Japan) and with considerations for the
protection of personal information (approval no. 20220428-14).
Patient consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Chu DK, Akl EA, Duda S, Solo K, Yaacoub S
and Schünemann HJ: COVID-19 Systematic Urgent Review Group Effort
(SURGE) study authors. Physical distancing, face masks, and eye
protection to prevent person-to-person transmission of SARS-CoV-2
and COVID-19: A systematic review and meta-analysis. Lancet.
395:1973–1987. 2020.PubMed/NCBI View Article : Google Scholar
|
|
2
|
Mistretta FA, Luzzago S, Molendini LO,
Ferro M, Dossena E, Mastrilli F, Musi G and de Cobelli O: A guide
for oncologic patient management during COVID-19 pandemic: The
initial experience of an Italian oncologic hub with exemplificative
focus on Uro-oncologic patients. Cancers (Basel).
12(1513)2020.PubMed/NCBI View Article : Google Scholar
|
|
3
|
Song Z, Hu Y, Ren Z, Wang G, Liu S, Zheng
S, Yang L and Zhao R: Optimal management of the public and patients
by pharmacists in the era of COVID-19: An evidence-based review and
practical recommendations. Front Public Health.
9(758325)2022.PubMed/NCBI View Article : Google Scholar
|
|
4
|
Li M, Razaki H, Mui V, Rao P and Brocavich
S: The pivotal role of pharmacists during the 2019 coronavirus
pandemic. J Am Pharm Assoc (2003). 60:e73–e75. 2020.PubMed/NCBI View Article : Google Scholar
|
|
5
|
Nguy J, Hitchen SA, Hort AL, Huynh C and
Rawlins MDM: The role of a Coronavirus disease 2019 pharmacist: An
Australian perspective. Int J Clin Pharm. 42:1379–1384.
2020.PubMed/NCBI View Article : Google Scholar
|
|
6
|
Song Z, Hu Y, Zheng S, Yang L and Zhao R:
Hospital pharmacists' pharmaceutical care for hospitalized patients
with COVID-19: Recommendations and guidance from clinical
experience. Res Social Adm Pharm. 17:2027–2031. 2021.PubMed/NCBI View Article : Google Scholar
|
|
7
|
Gillespie L, Khan RZ, Stillson JE, Bunch
CM, Shariff FS, Speybroeck J, Grisoli A, Schmidt MW, Phyu H,
Jablonski J, et al: Impact of a clinical pharmacist on
ultrasound-guided venous thromboembolism screening in hospitalized
COVID-19 patients: A pilot prospective study. J Pharm Health Care
Sci. 7(19)2021.PubMed/NCBI View Article : Google Scholar
|
|
8
|
Lat I, Paciullo C, Daley MJ, MacLaren R,
Bolesta S, McCann J, Stollings JL, Gross K, Foos SA, Roberts RJ, et
al: Position paper on critical care pharmacy services: 2020 Update.
Crit Care Med. 48:e813–e834. 2020.PubMed/NCBI View Article : Google Scholar
|
|
9
|
Kondo M, Tanaka C, Tagami T, Nagano M,
Sugaya K, Tagui N, Kaneko J, Kudo S, Kuno M, Unemoto K and Takase
H: Utility of a compatibility chart for continuous infusions in the
intensive care unit. J Nippon Med Sch. 89:227–232. 2022.PubMed/NCBI View Article : Google Scholar
|
|
10
|
Maison O, Tardy C, Cabelguenne D, Parat S,
Ducastelle S, Piriou V, Lepape A and Lalande L: Drug
incompatibilities in intravenous therapy: Evaluation and
proposition of preventive tools in intensive care and hematology
units. Eur J Clin Pharmacol. 75:179–187. 2019.PubMed/NCBI View Article : Google Scholar
|
|
11
|
Oda Y, Shimada M, Shiraishi S and Kurai O:
Treatment and outcome of COVID-19 patients in a specialized
hospital during the third wave: Advance of age and increased
mortality compared with the first/second waves. JA Clin Rep.
7(85)2021.PubMed/NCBI View Article : Google Scholar
|
|
12
|
Klopotowska JE, Kuiper R, van Kan HJ, de
Pont AC, Dijkgraaf MG, Lie-A-Huen L, Vroom MB and Smorenburg SM:
On-ward participation of a hospital pharmacist in a Dutch intensive
care unit reduces prescribing errors and related patient harm: An
intervention study. Crit Care. 14(R174)2010.PubMed/NCBI View
Article : Google Scholar
|
|
13
|
Ahmed N, Khan M, Saleem W, Karobari MI,
Mohamed RN, Heboyan A, Rabaan AA, Mutair AA, Alhumaid S, Alsadiq
SA, et al: Evaluation of Bi-Lateral Co-Infections and antibiotic
resistance rates among COVID-19 patients. Antibiotics (Basel).
11(276)2022.PubMed/NCBI View Article : Google Scholar
|
|
14
|
Cai Z, Yang Y and Zhang J: Obesity is
associated with severe disease and mortality in patients with
coronavirus disease 2019 (COVID-19): A meta-analysis. BMC Public
Health. 21(1505)2021.PubMed/NCBI View Article : Google Scholar
|
|
15
|
Dadras O, SeyedAlinaghi S, Karimi A,
Shamsabadi A, Qaderi K, Ramezani M, Mirghaderi SP, Mahdiabadi S,
Vahedi F, Saeidi S, et al: COVID-19 mortality and its predictors in
the elderly: A systematic review. Health Sci Rep.
5(e657)2022.PubMed/NCBI View
Article : Google Scholar
|
|
16
|
Guan WJ, Ni ZY, Hu Y, Liang WH, Ou CQ, He
JX, Liu L, Shan H, Lei CL, Hui DSC, et al: Clinical characteristics
of coronavirus disease 2019 in China. N Engl J Med. 382:1708–1720.
2020.PubMed/NCBI View Article : Google Scholar
|
|
17
|
Langford BJ, So M, Raybardhan S, Leung V,
Westwood D, MacFadden DR, Soucy JR and Daneman N: Bacterial
co-infection and secondary infection in patients with COVID-19: A
living rapid review and meta-analysis. Clin Microbiol Infect.
26:1622–1629. 2020.PubMed/NCBI View Article : Google Scholar
|
|
18
|
Terada M, Ohtsu H, Saito S, Hayakawa K,
Tsuzuki S, Asai Y, Matsunaga N, Kutsuna S, Sugiura W and Ohmagari
N: Risk factors for severity on admission and the disease
progression during hospitalisation in a large cohort of patients
with COVID-19 in Japan. BMJ Open. 11(e047007)2021.PubMed/NCBI View Article : Google Scholar
|