1. Introduction
The ongoing coronavirus disease 2019 (COVID-19)
pandemic has had significant repercussions on health systems
globally, as well as a profound impact on individuals' mental
health (1-5).
Furthermore, there is evidence to suggest that severe acute
respiratory syndrome coronavirus 2 (SARS-CoV-2) infection may be
associated with the presence of neuropsychiatric manifestations
during the acute phase of COVID-19, and a number of individuals may
experience a range of new, recurring or ongoing symptoms, including
neuropsychiatric manifestations, that persist beyond the acute
illness and comprise a condition that is colloquially referred to
as ‘long-COVID’ syndrome (6-10).
In particular, neuropsychiatric symptoms associated with
‘long-COVID’ may include depression, anxiety, post-traumatic stress
symptoms, sleep disturbances, fatigue, cognitive
impairment/deficits and psychotic features, which can potentially
become debilitating and have a disconcerting impact on the
well-being of COVID-19 survivors (10,11).
Previous studies have reviewed neuropsychiatric
symptoms associated with ‘long-COVID’ syndrome and their
correlates, highlighting the long-term effects of COVID-19 on the
mental health of individuals, especially among vulnerable groups
(i.e. patients with mental health history) (10-15).
Nevertheless, as researchers strive to identify the
mechanisms implicated in the neuropsychiatric manifestations of
‘long-COVID’, it is of crucial importance to better understand the
potential new-onset mental health symptoms that may follow initial
recovery from an acute COVID-19 infection or persist beyond the
acute illness. The aim of the present review was to provide a
comprehensive overview of the published literature on new-onset
neuropsychiatric sequelae of COVID-19 and to provide insight into
the putative underlying pathophysiological mechanisms.
2. New-onset neuropsychiatric sequelae in
COVID-19 survivors
Studies attempting to investigate the association of
long COVID with new-onset neuropsychiatric manifestations have
mainly used retrospective cohort study designs and data from
national health registries (16-25).
In most of these studies, which have attempted to investigate the
incidence of neuropsychiatric symptoms among COVID-19 survivors,
individuals with pre-existing psychiatric problems were excluded
(specific criteria vary within each study design). Moreover, in
order to explore whether COVID-19 survivors experience a higher
risk of presenting neuropsychiatric manifestations, most studies
have included as control group individuals without COVID-19 or
survivors of other disorders, usually influenza, while sub-analyses
of hospitalized or non-hospitalized patients have also been applied
(Table I).
 | Table IStudies reporting neuropsychiatric
sequelae following SARS-CoV-2 infection. |
Table I
Studies reporting neuropsychiatric
sequelae following SARS-CoV-2 infection.
| First author,
year | Study design | Country | Participants | Age | Time since acute
COVID-19/Follow-up period | Inclusion
criteria | Exclusion
criteria | Main findings | (Refs.) |
|---|
| Lund, 2021 | Population- based
cohort study | Denmark | • 8,983 individuals
positive for SARS-CoV-2 who were not admitted to hospital 2 weeks
after their positive test along with 80,894 eligible
SARS-CoV-2-negative individuals • 1,310 patients who tested
positive for SARS-CoV-2 and were admitted to hospital within 2
weeks of their test | Median (IQR) • 43
(30-56) years in SARS-CoV-2-positive non-hospitalized individuals •
43 (29-56) years in SARS-CoV-2-negative individuals • 64 (52-76)
years in SARS-CoV-2-positive hospitalized individuals | 2 weeks
post-positive test to 6 months | • Individuals with
a positive or negative SARS-CoV-2 test in Denmark between February
27 and May 31, 2020 • Patients who were alive 2 weeks after their
positive test | • Less than 1 year
of residency in Denmark • Inconclusive test results • Patient death
in the 2 weeks after their test • Prescription drug use and medical
history (any time to day 13) | • Lower risk of
first ever anxiety diagnosis in non-hospitalized patients with
SARS-CoV-2- positive compared with negative controls. No
differences in first ever depression or first ever fatigue-related
disorder diagnosis • No differences in first ever psychiatric
diagnosis among patients positive for SARS-CoV-2, with respect to
hospital admission status | (18) |
| Abel, 2021 | Retrospective
cohort study | United Kingdom | • 86,922
SARS-CoV-2- positive patients • 345,764 matched controls with
negative SARS-CoV-2 test result | Median (IQR) • 44
(30-61) years in the eligible cohort of 11,923,105 individuals | Follow-up for up to
10 months, from February 1 to December 9, 2020 | • Individuals aged
16 years or older during 2020 • Individuals registered at the
Clinical Practice Research Datalink Aurum participating clinical
practice from February 1 to December 8, 2020 | • Individuals with
less than 2 years of historical data or less than 1 week follow-up
were excluded • In the incident cohort, individuals with recorded
histories of psychiatric morbidity, fatigue, sleep problems, or
psychotropic medications in the 5 years prior to their index
date | • Individuals with
a SARS-CoV-2- positive test had increased risk of any psychiatric
morbidity (i.e., new-onset anxiety, depression, self-harm, fatigue
and sleep disorders), as well as of being prescribed psychotropic
medication compared with negative individuals • Higher risk of
psychiatric manifestations for individuals with influenza compared
with negative individuals | (21) |
| Park, 2021 | Nationwide
retrospective cohort study | Korea | • 6,148 COVID-19
survivors • 254,735 individuals without a COVID-19 diagnosis | • In total sample,
most individuals (24.5%) were between 20-29 and between 30-39
(17.5%) years of age • Statistically significant differences
between the groups | Data were extracted
from January 1 to June 4, 2020 and development of mental illness
was determined from January 1 to December 1, 2020 | Individuals
included in the National Health Insurance Service COVID-19 data
base in South Korea (from January 1 to June 4, 2020) | • Individuals under
the age of 20 • Individuals who had a previous history of mental
illness up until December 31, 2019 • For COVID-19 patients:
Patients who died from the infection during their hospital
admission | • Anxiety and
stress-related disorder, as well as mood disorders without
psychotic features, were significantly more frequent in the
COVID-19 cohort as compared with the control group • No differences
emerged regarding alcohol or drug misuse, eating disorders,
personality disorders, non- affective psychotic disorders or
affective psychotic disorders | (26) |
| Taquet, 2021 | Retrospective
cohort study | USA | • 236,379 patients
who had a COVID-19 diagnosis • 105,579 matched controls diagnosed
with influenza • 236,038 matched controls diagnosed with any RTI,
including influenza | Mean (SD) • 46
(19.7) years in patients with COVID-19 • 38.6 (19.7) years in
propensity score- matched patients with influenza • 46.0 (20.4)
years in propensity score- matched patients with any RTI | Follow-up, 1-180
days after the index event | All cohorts
included patients older than 10 years who had an index event on or
after January 20, 2020 (the date of the first recorded COVID-19
case in the USA), and who were still alive at the time of the main
analysis (December 13, 2020), from the TriNetX electronic health
records network | Individuals with a
psychiatric diagnosis before the index event (excluded when
estimating first diagnoses incidence) | • Psychiatric
disorders' first diagnosis (mood disorder, anxiety disorder,
psychotic disorder, insomnia) was more common in COVID-19 survivors
in comparison with patients with influenza or RTI • Patients with
COVID-19 experienced a higher risk of new-onset substance use
disorder compared with patients with influenza, but lower compared
with patients with RTI • Higher incidences in patients with more
severe COVID-19 | (20) |
| Taquet, 2021 | Retrospective
cohort study | USA | 44,779 COVID-19
survivors without pre-existing psychiatric illness, compared with
propensity score- matched control cohorts presenting other health
events (i.e., including influenza, other RTI, skin infection,
cholelithiasis, urolithiasis and fracture of a large bone) | Mean (SD) • 49.3
(19.7) years in patients with COVID-19 • 41.8 (19.8) years in
patients with influenza, 47.2 (19.9) years in patients with other
RTI, 46.7 (20.9) years in patients with skin infection, 53.2 (19.3)
years in patients with cholelithiasis, 50.2(18) years in patients
with urolithiasis and 48 (23.6) years in patients with fracture of
a large bone | Follow-up, 14-90
days after COVID-19 diagnosis | • Patients
diagnosed with COVID-19 between January 20 and August 1, 2020, from
the TriNetX electronic health records network • All seven cohorts
(COVID-19 and six control health events) included all patients
older than 10 years who had the corresponding health event on or
after January 20, 2020 | • Patients who had
died by the time of the analyses (August 1, 2020) • In the primary
analysis, patients who had a psychiatric diagnosis recorded before
the health event (COVID-19 or control health event) | • In patients with
no psychiatric history, a diagnosis of COVID-19 was associated with
increased incidence of a first psychiatric diagnosis in the
following 14 to 90 days compared with the six other health event
cohorts • Greatest incidences noted for anxiety disorders • When
diagnoses were considered separately (i.e. for anxiety disorder,
mood disorder, psychotic disorder, insomnia) incidences were
greater in patients with COVID-19 compared with patients with
influenza, as well as patients with other RTI (except psychotic
disorder); differences also emerged when comparing with the other
health events. | (16) |
| Patel, 2022 | Retrospective
cohort study | USA | 778,738 veterans,
who were tested for COVID-19. Among them, 123,757 (15.9%) were
diagnosed with COVID-19 | Mean (SD) age of
the total cohort was 61 (15.4) years | Follow-up 7 days to
3 months after the index date (i.e., date of the earliest positive
test or negative test. If the patient had been admitted to a VA
hospital during the preceding 15 days, the date of admission served
as the index date) | Veterans, who were
tested for COVID-19 at VA facilities between February 20, 2020 and
March 27, 2021, for any indication, and who had at least one
primary care follow-up in the previous 18 months | • Patients defined
as employees and others, keeping only veterans with proven
established care at the VA healthcare system • Patients who died
within 3 months of the index date or who did not have a minimum of
3 months of follow-up after the index date • Patients who had the
respective physical and mental health conditions as prevalent
conditions before the index date • Patients with an index date
later than December 27, 2020 | • COVID-19
survivors and particularly those who required hospitalization,
developed new-onset depressive episode, adjustment disorder,
insomnia and dementia at a significantly higher rate than those
without • Hospitalization was associated with a significantly
higher incidence and odds of developing mental health
conditions | (22) |
| Chen, 2022 | Retrospective
cohort study | USA | 3,158 veteran
patient who were hospitalized for COVID-19, between March and
August 2020 | Mean (SD) age of
total sample was 64.33 (14.78) years | Follow-up, up to
6-months following COVID-19 hospitalization | All veterans
hospitalized at Veterans Health Administration hospitals for COVID-
19 from March through August of 2020 | • Patients who died
during hospitalization or within 6 months of discharge, or were
missing covariate information • Patients who had been diagnosed
with the respective psychiatric condition within 2 years prior to
hospitalization | • 277 (7.9%)
patients developed a new mental health diagnosis following
hospitalization with the most common being depressive, anxiety, and
adjustment disorders • Patients with mental health history were not
excluded and thus among patients with a new mental health
diagnosis, 64% had an existing comorbid diagnosis | (23) |
| Xie, 2022 | Retrospective
cohort study | USA | 153,848 individuals
who survived the first 30 days of SARS-CoV-2 infection, and two
control groups: A contemporary group (n=5,637,840) with no evidence
of SARS-CoV-2, and a historic control group (n=5,859,251) that
predated the COVID-19 pandemic | Mean (SD) after
weighting • 63.06 (16.18) years in the COVID-19- positive cohort •
63.40 (16.22) years in the contemporary control group • 63.32
(16.30) years in the historic control group | • For the COVID-19-
positive cohort: Follow-up from the date of the positive test
result up to November 30, 2021 (median follow-up days, IQR: 377,
347-469). • Contemporary control group had a similar distribution
of follow-up time (median, IQR: 378, 348-471), while similar
methods were applied with respect to the historic group (median,
IQR: 378, 347-470) | • For the COVID-19-
positive cohort: individuals who had used the Veterans Health
Administration in 2019 and had at least one positive COVID-19 test
result between March 1, 2020 and January 15, 2021, and also were
alive 30 days after the positive test result • For the contemporary
control group: Individuals who used the Veterans Health
Administration in 2019 and that were alive by 1 March 2020 and not
in the COVID-19 group • For the historic control group: Individuals
who used the Veterans Health Administration in 2017, were alive on
March 1, 2018 and were not in the COVID-19 group | Individuals with
mental health history (from 2 years before the positive SARS-CoV-2
test up to 30 days after the test) | • Compared to their
contemporary SARS-CoV-2 negative counterparts, COVID-19 survivors
presented an increased risk of incidence of any mental health
diagnosis, any mental health-related drug prescription and any
mental health diagnosis or prescription, even among
non-hospitalized individuals • Findings were also consistent in
comparisons using the historic control group • Risk of new-onset
mental health disorders was higher in patients with COVID-19
compared with both patients with seasonal influenza and individuals
admitted to hospital for any other cause | (25) |
| Iosifescu,
2022 | Retrospective
cohort study | USA | • 388 patients with
COVID-19 with new- onset neurological/ neuropsychiatric symptoms •
18,423 patients with COVID-19 without neurological/
neuropsychiatric symptoms • 149 patients with influenza with new-
onset neurological/ neuropsychiatric symptoms | Mean (SD) • 57.2
(19.3) years in patients with COVID-19 with new- onset
neurological/ neuropsychiatric symptoms • 55.2 (20.8) years in
patients with COVID-19 without neurological/ neuropsychiatric
symptoms • 40.0 (24.0) years in patients with influenza with new-
onset neurological/ neuropsychiatric symptoms | Individuals were
retrospectively screened between January 1, 2020 and June 9,
2021 | • Patients of the
Montefiore Health System, one of the largest healthcare systems in
New York City (data between January 1, 2020 and June 9, 2021) • For
the COVID-19 cohort, all individuals who tested positive for
SARS-CoV-2 infection • For the influenza cohort individuals:
Diagnosed with influenza in the same hospital system and within the
same timeframe, but without a COVID-19 diagnosis | • Individuals not
screened • Having neurological/ neuropsychiatric symptoms prior to
diagnosis • Developed symptoms <2 weeks after the diagnosis | • New-onset
neuropsychiatric symptoms were recorded in 2.06% of COVID-19
survivors and in 2.58% of patients with influenza • Patients with
influenza presented similar neuropsychiatric manifestations to
COVID-19 survivors, apart from a lower incidence in altered mental
status | (17) |
| Clift, 2022 | Retrospective
cohort study | UK | • 32,525 COVID-19
hospital admission survivors • 16,679 SARI admission survivors •
8,330,986 adults in the reference population | Mean (SD) • 65.40
(18.42) years in COVID-19 admission survivors • 69.34 (18.70) years
in SARI admission survivors • 49.07 (18.40) years in adults of the
reference population | • Follow-up time
was calculated from the discharge date for those surviving a
COVID-19 or SARI-related hospital admission and for the remaining
population from January 24, 2020 • Patient follow-up was until the
earliest date of outcome of interest or censoring (left practice,
died for any reason, or reached the end of follow-up alive) •
Follow-up was truncated to 1 year for analysis | • Adults alive and
registered with a contributing general practice from January 24,
2020 (date of first COVID-19 case in England), until the data
extract date (July 7, 2021) • In historic cohort: Adults aged 18
years and older entering the cohort from January 24, 2015 to
January 23, 2020 | For each outcome,
the authors excluded individuals with previously recorded records
of the outcome of interest | • Both SARI
survivors and COVID-19 survivors displayed higher risk for
new-onset neuropsychiatric diagnosis post discharge for all studied
outcomes compared with the general population • No significant
differences between COVID-19 survivors and SARI survivors | (24) |
| Coleman, 2022 | Retrospective
cohort study | USA | • 46,610 COVID-19-
positive individuals • 46,610 propensity score-matched controls
with RTI diagnosis | Not included in the
paper | • Follow-up 21 to
365 days after initial presentation (cutoff date, October 20,
2021) | • Individuals
included in National COVID Cohort Collaborative electronic health
record repository (January 2020-October 2021) • For COVID-19
cohort: SARS-CoV-2 positive test after January 1, 2020 • For
control cohort: Patients with a diagnosis of a RTI other than
COVID-19 | • Patients with a
history of any mental illness prior to 21 days after COVID-19
diagnosis • Patients without a medical record extending back to a
year prior to COVID-19 | • New-onset anxiety
disorder diagnosis was higher in patients with COVID-19 compared to
in patients with RTI in the early post-acute phase (from 21 to 120
days), but not during the late post-acute phase (from 121 to 365
days) • No differences in new-onset mood disorders, neither in the
early post-acute phase nor in the late post-acute phase | (19) |
| Rivera- Izquierdo,
2022 | Prospective,
multicenter, cohort study | Spain | • 453 patients
hospitalized due to COVID-19 • 453 patients hospitalized due to
other causes | Mean (SD) • 61.2
(14.3) years in patients hospitalized due to COVID-19 • 55.9 (17.8)
years in patients hospitalized due to other causes | Patients were
consulted by telephone 12 months after discharge | • Adults
hospitalized and discharged alive from March 1 to April 15, 2020,
in four hospitals in Andalusia, Spain • For COVID-19 cohort:
SARS-CoV-2 positive test | • Patients lost to
follow-up • Symptoms that were present prior to hospital
admission | • Higher incidences
in anxiety symptoms and confusion/ memory loss in COVID-19
survivors compared with individuals hospitalized due to other
causes • No significant differences in depressive symptoms, sleep
disturbances, fatigue, or headache | (27) |
| Jacob, 2022 | Retrospective
cohort study | Germany | • 56,350 patients
with COVID-19 • 56,350 propensity score-matched controls with
AURI | Mean (SD) • 43.6
(19.2) years in patients with COVID-19 • 43.6 (19.2) years in AURI
controls | Up to 14 months
follow-up; patients were diagnosed between March 2020 and May
2021 | • Adults with at
least one visit to one of 1,198 general practices in Germany
between March 2020 and May 2021 • Patients diagnosed with COVID-19
or AURI | • COVID-19
diagnosis within the preceding year • Depression or anxiety
disorder history within the preceding year | No significant
difference in incidence of depression or anxiety disorder between
patients with COVID-19 and AURI | (28) |
A population-based cohort study by Lund et al
(18) using Danish registry data
comprised 8,983 patients who tested positive for SARS-CoV-2
infection (follow-up was from 2 weeks after a positive test to 6
months) during the first wave of the COVID-19 pandemic
(February-May 2020), who were alive and not admitted to hospital 2
weeks after their positive test. This previous study also included
1,310 patients who tested positive for SARS-CoV-2 and were admitted
to hospital within 2 weeks of their test, along with a matched
SARS-CoV-2-negative reference population of 80,894 individuals.
Notably, non-hospitalized patients positive for SARS-CoV-2 [27 out
of 8,586 (0.3%)] presented a statistically significantly lower risk
[adjusted risk ratio (aRR), 0.62; 95% confidence interval (CI),
0.42-0.91] for first-ever psychiatric diagnosis compared with their
SARS-CoV-2-negative counterparts [429 out of 74,641 (0.6%)]. Among
patients positive for SARS-CoV-2, regarding first-ever diagnosis of
psychiatric illnesses, no differences emerged with respect to
hospital admission status (no vs. yes; RR, 0.63; 95% CI,
0.26-1.52). Notably, in comparison with SARS-CoV-2-negative
individuals, patients positive for SARS-CoV-2 were not at an
increased risk of initiating psychiatric drugs, including
antidepressants (aRR, 0.84; 95% CI, 0.62-1.13), benzodiazepines and
Z-drugs (aRR, 1.03; 95% CI, 0.75-1.41) or antipsychotics (aRR,
0.93; 95% CI, 0.61-1.42).
In another cohort study by Abel et al
(21), the risk of incident mental
health symptoms occurring following SARS-CoV-2 infection (follow-up
was from 1 week to 10 months) was investigated using data from a UK
primary care registry (February-December 2020), including 86,922
patients positive for SARS-CoV-2 and 345,764 matched controls with
a negative SARS-CoV-2 test result (without mental distress, sleep
problems or fatigue in the preceding 5 years). In this previous
study, having a positive result on a SARS-CoV-2 test was associated
with an increased risk of any psychiatric morbidity [adjusted
hazard ratio (aHR), 1.83; 95% CI, 1.66-2.02] and of being
prescribed psychotropic medication (aHR, 2.24; 95% CI, 2.09-2.40).
The association between SARS-CoV-2 infection and psychiatric
morbidity was greater for older adults, while women with a positive
SARS-CoV-2 test had a higher incidence for all outcomes compared
with men, albeit the relative increase associated with a positive
test result was larger for men than for women based on tests for
equivalence of aHRs. Notably, a higher risk of psychiatric
manifestations was also found for individuals with influenza
compared with control individuals (aHR, 2.98; 95% CI, 1.55-5.75).
Crucially, the results of a further analysis of that study to
explore confounding bias (using a negative exposure control) were,
according to the authors, suggestive of unobserved confounding.
In a nationwide cohort study in South Korea (data
extracted, January-June 2020; follow-up until December 2020), Park
et al (26) used data from
the National Health Insurance Service COVID-19 database, and
compared 6,148 COVID-19 survivors with 254,735 individuals without
a COVID-19 diagnosis, after excluding individuals with mental
health history prior to 2020. Newly diagnosed mental disorders were
significantly more frequent in the COVID-19 cohort [738 out of
6,148 (12.0%)] compared with the control group [19,524 out of
254,357 (7.7%); P<0.001].
In accordance with the results of the previous
study, Taquet et al (20)
performed a retrospective cohort study (January-December 2020)
using electronic health records in the USA. This previous study
investigated the incidence of first neurological/psychiatric
diagnoses (i.e. excluding those diagnosed before the index event)
among 236,379 COVID-19 survivors in the 6 months post-infection
(i.e. 1-180 days post-index event) and compared associated risks
with two propensity score-matched control cohorts of 105,579
patients diagnosed with influenza and of 236,038 patients with any
respiratory tract infection (RTI), including influenza, during the
same period. According to the findings of this study, 8.63% (95%
CI, 8.28-8.98) of the survivors received a first diagnosis of any
psychiatric disorder (either anxiety disorder, mood disorder or
psychotic disorder) in the 6 months after COVID-19 diagnosis,
whereas the estimated incidence was higher for patients with
intensive care unit (ICU) admission (12.96; 95% CI, 12.28-14.24).
Notably, a first diagnosis of a psychiatric disorder was more
common in COVID-19 survivors in comparison to both patients with
influenza (HR, 1.81; 95% CI, 1.69-1.94) and those presenting other
RTIs (HR, 1.48; 95% CI, 1.42-1.55).
It should be noted that a previous retrospective
cohort study (16), which was
performed by the same research group using USA electronic health
records (January-August 2020), assessed the incidence of first
psychiatric diagnoses in 44,779 COVID-19 survivors, without
pre-existing psychiatric illness, at 14-90 days post-COVID-19
diagnosis and also compared associated risks with matched control
cohorts presenting with other health events (including influenza,
other RTIs, skin infection, cholelithiasis, urolithiasis and
fracture of a large bone). Among the COVID-19 survivors, 5.8% (95%
CI, 5.2-6.4) had their first recorded diagnosis of psychiatric
illness in comparison to 2.5-3.4% of patients in the aforementioned
control cohorts.
In accordance with the findings of previous studies
suggesting an increased risk for new-onset psychiatric disease in
the post-COVID-19 period, a propensity score-matched retrospective
cohort study was conducted to compare US veterans who were tested
for COVID-19 between February 2020 and March 2021 vs. patients with
negative SARS-CoV-2 test results (22). Incident conditions were defined as
conditions that developed during a follow-up period of 7 days to 3
months post-index date in patients without such pre-existing
conditions. COVID-19 survivors (15.9% out of 778,738 veterans),
particularly those who required hospitalization, developed
new-onset neuropsychiatric symptoms at a significantly higher rate
than those without COVID-19. In the outpatient setting, the results
were more perplexing. Although the incidence of mental health
conditions was overall rather low (0.2-1.5%), patients with
COVID-19 presented a significantly lower incidence of mental health
conditions than patients negative for COVID-19. When comparing the
incidence of mental health conditions between COVID-19-positive
matched patients who were hospitalized to those treated as
outpatients, it emerged that hospitalization was associated with a
significantly higher incidence and odds of developing mental health
conditions.
Another study in veteran patients (n=3,518), who
were all hospitalized for COVID-19, between March and August 2020,
revealed that 277 (7.9%) patients developed a new mental health
diagnosis following hospitalization (i.e. having not been diagnosed
with the specific condition within 2 years prior to
hospitalization) (23). Younger
patients and those residing in rural areas were more likely to
develop new mental health diagnoses, whereas women and patients
with more comorbidities were less likely to develop new
diagnoses.
Furthermore, a recent cohort study of US veterans
(March 2020-November 2021) estimated the risks of incident mental
health disorders in COVID-19 survivors (i.e. without a history of
the mental health outcome in the 2 years prior to the beginning of
follow-up) (25). This previous
study included 153,848 individuals who survived the first 30 days
of SARS-CoV-2 infection, 5,637,840 individuals as a contemporary
control group with no evidence of SARS-CoV-2 and 5,859,251
individuals as a historic pre-pandemic control group (totalling
13,052,788 person-years of follow-up). The results of this study
showed that compared with their contemporary SARS-CoV-2-negative
counterparts, COVID-19 survivors presented an increased risk of any
incident mental health diagnosis (HR,1.46; 95% CI, 1.40-1.52), any
incident mental health-related drug prescription (HR, 1.86; 95% CI,
1.78-1.95), and any incident mental health diagnosis or
prescription (HR, 1.60; 95% CI, 1.55-1.66). The risks of examined
outcomes were found to be increased even among non-hospitalized
individuals but were the highest among patients hospitalized during
the acute phase of COVID-19. Findings were also consistent in
comparisons performed using the historic control group.
Furthermore, the risk of incident mental health disorders was
higher in patients with COVID-19 compared with both patients with
seasonal influenza and individuals admitted to hospital for any
other cause.
Iosifescu et al (17), in a retrospective cohort study
performed in a large healthcare network in New York City, USA,
screened patients with COVID-19 and influenza (January 2020-June
2021) for the presence of new-onset neurological/neuropsychiatric
symptoms persisting ≥2 weeks past COVID-19 or influenza diagnosis,
respectively. Notably, those with pre-existing
neurological/neuropsychiatric symptoms were excluded. New-onset
neuropsychiatric symptoms were recorded in 2.05% (388 out of
18,881) of COVID-19 survivors and in 2.58% (149 out of 5,772) of
patients with influenza. It should be noted that patients with
influenza presented neuropsychiatric manifestations similar to
COVID-19 survivors, apart from a lower incidence of altered mental
status and a non-significantly lower incidence of fatigue. The mean
onset of neurological/neuropsychiatric symptoms among COVID-19
survivors was 138 days post-diagnosis, with inpatients experiencing
symptoms significantly earlier than outpatients (120 vs. 146 days,
respectively). Conversely, patients with influenza displayed a
significant delay in symptom onset (mean onset, 238 days) compared
with COVID-19 survivors. These findings could indicate that
COVID-19, in comparison to other respiratory viruses, may induce
early neurological/neuropsychiatric manifestations, whereas severe
and mild COVID-19 infection may be potentially associated with
earlier symptom onset or more gradual development of
neurological/neuropsychiatric manifestations, respectively.
Furthermore, compared with patients with COVID-19 without
neurological/neuropsychiatric symptoms, patients with COVID-19 with
such symptoms were older, more likely female and had lower levels
of laboratory parameters, such as lactate dehydrogenase, C-reactive
protein (CRP) and D-dimer. Conversely, race, ethnicity,
hospitalization status, body mass index (BMI), blood urea nitrogen
(BUN), lymphocytes, leukocytes and comorbidities were not
significantly associated with neurological/neuropsychiatric
symptoms among COVID-19 survivors. Among patients with new-onset
neurological/neuropsychiatric symptoms, COVID-19 survivors compared
with patients with influenza, were significantly older, prevalently
male and presented higher hospitalization rate, BMI, as well as
laboratory values (i.e. CRP, D-dimer and BUN).
One of the largest published studies on the
incidence of neuropsychiatric disorders post-COVID thus far is an
English cohort study (24). This
previous study comprised data from 8.38 million adults (January
2020-July 2021), including 16,679 (0.20%) individuals surviving
hospitalization for severe acute respiratory infections (SARI)
other than COVID-19 and 32,525 (0.39%) individuals surviving
hospitalization for COVID-19. These patient groups were compared
with the remaining general population regarding new-onset diagnoses
of neuropsychiatric conditions (individuals with previous records
of the outcome of interest were excluded) or first psychiatric
medication prescription during 12 months of follow-up from hospital
discharge. Both SARI survivors and COVID-19 survivors displayed a
higher risk for new-onset neuropsychiatric diagnosis post-discharge
for all studied outcomes compared with the general population.
Nevertheless, no significant differences were observed when
COVID-19 survivors were compared with SARI survivors regarding
new-onset neuropsychiatric symptoms. Regarding the first recorded
neuropsychiatric prescription after hospital discharge, the risks
were significantly higher in survivors of SARI and hospitalized
patients with COVID-19 compared with the remaining population for
all medications analysed (i.e. antidepressants,
hypnotics/anxiolytics and antipsychotics). Conversely, no
significant differences emerged between the COVID-19 and the SARI
cohort, except for a lower risk of antipsychotic prescriptions in
COVID-19 survivors (aHR, 0.80; 95% CI, 0.69-0.92).
Similar results suggesting an excess risk for
new-onset neuropsychiatric diagnoses during the post-COVID period
were found in a retrospective electronic health record cohort study
(January 2020-October 2021) by Coleman et al (19), including 46,610 propensity
score-matched patient pairs of individuals positive for COVID-19
and comparable controls with RTI diagnosis. This previous study
investigated the incidence of new-onset mental illness from day 21
to 1 year following initial presentation (patients with any
psychiatric diagnosis during COVID-19 infection, i.e. first 21 days
after diagnosis or prior to COVID-19 infection, were excluded). A
statistically significant difference was identified in the hazard
rate of new-onset psychiatric sequelae between COVID-19 and control
groups in the early post-acute phase (from 21 to 120 days), but not
in the late post-acute phase (from 121 to 365 days). In particular,
the estimated incidence proportion of a new-onset psychiatric
diagnosis in the early post-acute phase for the COVID-19 group was
3.8% (95% CI, 3.6-4.0), which was significantly higher than the
3.0% (95% CI, 2.8-3.2) for the RTI group (HR, 1.3; 95% CI,
1.2-1.4).
From the previous evidence, new-onset
neuropsychiatric morbidity seems strongly associated with
respiratory infections, particularly SARS-CoV-2. Nevertheless, the
findings regarding increased neuropsychiatric incidence in
survivors of COVID-19 in comparison with other respiratory
infections vary among studies. Since most studies suffer from
methodological limitations and biases, future well-designed
cohorts, basic research studies and focused meta-analyses are
required to evaluate the true extent of the association between
‘long-COVID’ and new-onset neuropsychiatric disorders.
New-onset affective and anxiety
symptoms and ‘long-COVID’
In studies investigating new-onset neuropsychiatric
manifestations in COVID-19 survivors without pre-existing mental
health problems, depression and anxiety emerge among the most
commonly reported symptoms.
In particular, Taquet et al (20) found in a retrospective cohort study
of 236,379 COVID-19 survivors that 1-180 days post-COVID-19
diagnosis, 7.11% (95% CI, 6.82-7.41; ICU admission, 9.79; 95% CI,
8.65-11.06) received a first diagnosis of an anxiety disorder,
whereas 4.22% (95% CI, 3.99-4.47; ICU admission, 5.82; 95% CI,
4.86-6.97) received a first diagnosis of a mood disorder. When
compared with patients with influenza and patients with other RTIs,
COVID-19 survivors had higher probabilities of new-onset anxiety
(HR 1.78 and 1.48, respectively) and mood disorder (HR 1.79 and
1.41, respectively). In a previous retrospective cohort study
(16) from the same research
group, including 44,779 COVID-19 survivors, it emerged that 14-90
days post-COVID-19 diagnosis, 2.0% (95% CI, 1.7-2.4) received their
first recorded diagnosis of a mood disorder (depressive episode,
1.7; 95% CI, 1.4-2.1; mania/bipolar, 0.1; 95% CI, 0.04-0.25),
whereas 4.7% (95% CI, 4.2-5.3) received their first diagnosis of a
anxiety disorder; both were found to present more commonly in the
COVID-19 cohort compared with the influenza and other RTI matched
cohorts. When anxiety disorders were analysed individually,
adjustment disorder (0.94; 95% CI, 0.74-1.2) and generalized
anxiety disorder (0.85; 95% CI, 0.66-1.1) were the most frequent,
followed by post-traumatic stress disorder (PTSD; 0.25; 95% CI,
0.16-0.4) and panic disorder (0.26; 95% CI, 0.17-0.4), whereas
obsessive-compulsive disorder (OCD) presented rarely (0.04; 95% CI,
0.008-0.17).
Furthermore, Park et al (26) in a South Korean nationwide cohort
study, compared 6,148 COVID-19 survivors with 254,735 individuals
without a COVID-19 diagnosis and found that significantly more
COVID-19 survivors presented anxiety and stress-related disorder
(8.0 vs. 5.2%, P<0.001), as well as mood disorders without
psychotic features (5.6 vs. 3%, P<0.001).
A prospective cohort study by Rivera-Izquierdo et
al (27) in Spain investigated
the incidence (symptoms that were present prior to hospital
admission were excluded) of sequelae or persistent symptoms 12
months after discharge in 453 individuals hospitalized due to
COVID-19 compared with an equal number of individuals hospitalized
due to other causes (March-April 2020) and discharged alive.
According to the findings of this study, a higher incidence of
anxiety symptoms was noted in COVID-19 survivors compared with in
individuals hospitalized due to other causes (7.3 vs. 3.1%; RR,
2.36; 95% CI, 1.28-4.34), while no differences emerged in
depressive symptoms (4.0 vs. 3.5%; RR, 1.13; 95% CI,
0.58-2.18).
Consistent with the aforementioned findings, Coleman
et al (19), in a
retrospective cohort study of 46,610 propensity score-matched
patient pairs of individuals positive for COVID-19 and comparable
controls with a RTI diagnosis indicated that new-onset anxiety
disorder diagnosis was significantly increased for patients with
COVID-19 compared with patients with RTI in the early post-acute
phase (HR, 1.3; 95% CI, 1.1-1.4), but not during the interval of
121-365 days following initial presentation (HR, 1.0, 95% CI,
0.91-1.1). However, regarding new-onset mood disorders, no
differences emerged in the early post-acute phase (21-120 days) or
in the late post-acute phase (121-365 days).
Conversely, Patel et al (22), in a retrospective cohort study of
US veterans, found that COVID-19 survivors that required
hospitalization, compared with propensity-matched hospitalized
patients negative for COVID-19, displayed significantly higher
incidences of a depressive episode (6.6 vs. 4.3%; P<0.001) and
adjustment disorder (2.5 vs. 1.7%, P<0.001), whereas no
statistically significant differences emerged regarding the
incidence of panic disorder, generalized anxiety and PTSD. With
respect to admission to hospital, hospitalized patients with
COVID-19 compared with those treated as outpatients demonstrated
higher incidences of depressive episodes (6.6 vs. 1.2%;
P<0.001), panic disorder (0.3 vs. 0.1%; P<0.001), generalized
anxiety (0.7 vs. 0.3%; P<0.001), PTSD (1.4 vs. 0.5%; P<0.001)
and adjustment disorder (2.4 vs. 0.9%; P<0.001). Accordingly,
Chen et al (23) found that
among the 277 (7.9% of 3,518) veteran hospitalized COVID-19
survivors with new-onset mental health manifestations, the most
common new diagnoses included depression (28%), anxiety (28%),
adjustment disorders (24%) and PTSD (17%), whereas in another US
veteran cohort study, Xie et al (25) found that COVID-19 survivors
compared with individuals without COVID-19 presented increased
risks of anxiety, depression, stress and adjustment disorders.
In a cohort study by Clift et al (24), SARI and COVID-19 survivors compared
with the general population displayed higher levels of new-onset
anxiety (SARI aHR, 1.86; 95% CI, 1.56-2.21; COVID-19 aHR, 2.36; 95%
CI, 2.03-2.74), depression (SARI aHR, 3.46; 95% CI, 2.21-5.40;
COVID-19 aHR, 1.95; 95% CI, 1.05-3.65) and bipolar disorder (SARI
aHR, 2.26; 95% CI, 1.25-4.08; COVID-19 aHR, 2.26; 95% CI,
1.25-4.07). No differences were found between the COVID-19 and the
SARI cohort (reference group) regarding new-onset anxiety disorder
(aHR, 1.00; 95% CI, 0.79-1.27), depression (aHR, 0.63; 95% CI,
0.25-1.58) or bipolar affective disorder (aHR, 0.74; 95% CI,
0.32-1.69).
Similar were the findings in a retrospective cohort
study by Jacob et al (28)
(March 2020-May 2021) including patients without a history of
depression or anxiety disorder within the preceding year, which
were followed in general practices in Germany. In this study,
56,350 patients with COVID-19 were compared with an equal sample of
patients with acute upper respiratory infection matched using
propensity scores based on sex, age, index month and Charlson
comorbidity index. According to the findings, COVID-19 diagnosis
was not significantly associated with an increase in the incidence
of depression [incidence rate ratio (IRR), 1.02; 95% CI, 0.95-1.10]
or anxiety disorder (IRR, 0.94; 95% CI, 0.83-1.07) in comparison to
a diagnosis of acute upper respiratory infection. No significant
association emerged between COVID-19 diagnosis and the incidence of
either depression or anxiety in all sex and age subgroups.
In accordance with the previous studies, in a
retrospective cohort study by Iosifescu et al (17), among 388 patients with COVID-19
with neurological/neuropsychiatric sequalae (out of 18,811 patients
with COVID-19), 30% reported anxiety disorders and 27% depression,
albeit no differences were found with respect to the flu
cohort.
Lund et al (18) in a population-based cohort study,
found that non-hospitalized individuals positive for SARS-CoV-2 [9
out of 8,884 (0.1%)], compared with negative individuals [107 out
of 79,616 (0.1%)], did not present a significantly different risk
of first ever depression diagnosis (aRR, 0.91; 95% CI, 0.46-1.80).
However, patients with COVID-19 had a significantly lower risk [15
out of 8,786 (0.2%)] of first anxiety diagnosis compared with
SARS-CoV-2-negative individuals [293 out of 77,654 (0.4%); aRR,
0.54; 95% CI, 0.32-0.90].
In a cohort study by Abel et al (21), patients with SARS-CoV-2 infection
compared with individuals with SARS-CoV-2 negative test results,
presented increases in new-onset anxiety (aHR, 1.93; 95% CI,
1.71-2.18), depression (aHR, 1.74; 95% CI, 1.52-2.00) and self-harm
risks (aHR, 2.21; 95% CI, 1.11-4.39). Regarding psychiatric
medications, the largest increases included receipt of
nonbenzodiazepine hypnotics (aHR, 4.90; 95% CI, 4.00-5.99), mood
stabilizers (aHR, 3.55; 95% CI, 2.74-4.61), benzodiazepines (aHR,
3.50; 95% CI, 2.95-4.15) and antidepressants (aHR, 1.72; 95% CI,
1.57-1.88). However, these findings should be interpreted with
caution considering that the results of a further analysis
performed in the same study using a negative exposure control to
explore confounding bias were suggestive of unobserved
confounding.
Despite evidence of an association between COVID-19
and new-onset anxiety and depression symptoms, especially among
patients with increased disease severity, further research is
required using methodological approaches less susceptible to
confounding bias given the inconsistent findings regarding the
comparison of COVID-19 survivors with other respiratory
infections.
New-onset psychotic symptoms,
insomnia, other neuropsychiatric symptoms and ‘long-COVID’
Individual cases of putative COVID-19-associated
neuropsychiatric disorders (e.g. psychosis, OCD, etc.) (29,30)
have been reported since the COVID-19 pandemic outbreak; more
recently, studies using large sets of health record data have
attempted to investigate if this association is significant
considering possible confounding factors (16,29).
Research regarding the possible association of ‘long-COVID’
syndrome with new-onset neuropsychiatric symptoms has aimed to
estimate incidences and risks regarding psychotic disorders, sleep
disturbances, fatigue, substance use disorders and other mental
health manifestations among COVID-19 survivors, in comparison,
usually, either with individuals without SARS-CoV-2 infection or
with patients who had other illnesses, such as influenza and other
RTIs (20-22).
Taquet et al (20), in a retrospective cohort study,
found that in the 6 months succeeding COVID-19 diagnosis, the first
psychotic disorder diagnosis was recorded in 0.42% (95% CI,
0.36-0.49; ICU admission, 0.70; 95% CI, 0.46-1.06), first substance
use disorder diagnosis in 1.92% (95% CI, 1.77-2.07; ICU admission,
3.15; 95% CI, 2.60-3.82) and first insomnia diagnosis in 2.53% (95%
CI, 2.37-2.71; ICU admission, 4.24; 95% CI, 3.55-5.07) of COVID-19
survivors, with higher incidences observed among those admitted to
the ICU. When compared with patients with influenza, COVID-19
survivors had higher probabilities of a new-onset psychotic
disorder (HR, 2.16), newly diagnosed substance use disorder (HR,
1.22) and new-onset insomnia (HR, 1.92). Similar were the results
when compared with patients with RTI, with the exception that
new-onset substance use disorder was less common in patients with
COVID-19 (HR, 0.92). In a previous retrospective cohort study by
Taquet et al (16), 14-90
days after COVID-19 diagnosis, 0.1% of COVID-19 survivors (95% CI,
0.08-0.2) had their first recorded diagnosis of psychotic disorder
and 1.9% (95% CI, 1.6-2.2) had their first diagnosis of insomnia,
while both diagnoses were more frequently recorded in the COVID-19
cohort as compared with a matched cohort of individuals who had
influenza.
Park et al (26), in a nationwide cohort study in
South Korea, compared 6,148 COVID-19 survivors with 254,735
individuals without a COVID-19 diagnosis regarding the development
of neuropsychiatric manifestations following recovery. Although
they found differences related to COVID-19 diagnosis, these were
potentially explained by increases in anxiety and mood disorders
since when individual diagnoses were explored no differences
emerged regarding alcohol or drug misuse (0.2 vs. 0.3; P=0.612),
eating disorders (0.0 vs. 0.1; P=0.315), personality (0.0 vs. 0.0%;
P=0.601) non-affective (0.2 vs. 0.3%; P=0.224) and affective
psychotic (1.1 vs. 1.1%, P=0.968) disorders.
Abel et al (21), in a cohort study comparing patients
with SARS-CoV-2 infection with individuals with SARS-CoV-2 negative
test results, found that COVID-19 was related to increases in
fatigue (aHR, 5.98; 95% CI, 5.33-6.71) and sleep disorders (aHR,
3.16; 95% CI, 2.64-3.78), while an initially recorded increase in
psychosis lost statistical significance after adjusting for
confounders (HR, 2.34; 95% CI, 1.48-3.70; aHR, 1.84; 95% CI,
0.93-3.64). Regarding psychiatric medications, the largest
increases were for receipt of antipsychotics (aHR, 7.61; 95% CI,
5.00-11.60).
Patel et al (22) found that, among hospitalized US
veteran patients, COVID-19 was associated with significantly higher
incidences of insomnia (4.9 vs. 3.2%; P<0.001) and dementia (3.0
vs. 1.9%; P<0.001) compared with propensity-matched hospitalized
patients negative for COVID-19, while in outpatient settings
patients with COVID-19 presented a significantly higher incidence
of dementia (0.3 vs. 0.2%; P=0.03). Additionally, when comparing
hospitalized and non-hospitalized patients with COVID-19, it
emerged that hospitalized patients presented significantly
increased rates of insomnia (4.9 vs. 1.1%; P<0.001) and dementia
(3.0 vs. 0.6%; P<0.001). In another US veteran cohort study, Xie
et al (25) found that
COVID-19 survivors compared with individuals without COVID-19
presented increased risks of incident opioid and other (non-opioid)
substance use disorders, as well as neurocognitive decline and
sleep disorders.
According to the findings of a Spanish prospective
cohort study by Rivera-Izquierdo et al (27), incidence was higher for
hospitalized COVID-19 survivors compared with individuals
hospitalized due to other causes regarding confusion or memory loss
(3.1 vs. 0.9%; RR, 3.50; 95% CI, 1.16-10.55), while no differences
emerged for sleep disturbances (2.2 vs. 1.5%; RR, 1.43; 95% CI,
0.55-3.81), fatigue (7.7 vs. 8.8%; RR, 0.88; 95% CI, 0.57-1.35) or
headache (2.0 vs. 2.0%; RR, 1.00; 95% CI, 0.40-2.50). In line with
the aforementioned non-significant results concerning fatigue, in a
Danish population-based cohort study (18), individuals positive for COVID-19
but not hospitalized (18 of 8,809 individuals, 0.2%) did not
present a statistically significantly different risk of first-ever
fatigue-related disorder diagnosis compared with negative
individuals (175 of 78,543 individuals, 0.2%; aRR, 0.97; 95% CI,
0.60-1.59).
In an English cohort study (24), SARI and COVID-19 survivors (both
requiring hospitalization), when compared with the general
population, displayed higher first recorded new-onset diagnosis of
dementia (SARI aHR, 2.55; 95% CI, 2.17-3.00; COVID-19 aHR, 2.63;
95% CI, 2.21-3.14) and psychotic disorder (SARI aHR, 3.63; 95% CI,
1.88-7.00; COVID-19 aHR, 3.05; 95% CI, 1.58-5.90). No differences
in new-onset psychiatric morbidity emerged between the two patient
groups, whereas regarding the first recorded neuropsychiatric
prescription only significantly lower risk of antipsychotic
prescriptions was noted among COVID-19 survivors (aHR, 0.80; 95%
CI, 0.69-0.92).
Findings of a systematic review of 40 case reports
regarding the incidence of COVID-19-associated psychosis suggested
that clinical presentations often lacked clinically relevant
information, such as whether a delirium diagnosis was excluded
(29). Thus, an appropriate
differential diagnosis between non-delirious psychosis and delirium
is crucial in order to prevent the risk of overreporting psychotic
disorders by misdiagnosing cases of delirium, especially among
patients hospitalized for COVID-19 and older patients. In addition,
distinguishing psychotic features as part of a broader syndrome,
such as delirium, from a distinct clinical psychotic disorder
related to COVID-19 infection is also of paramount importance
(29,31,32).
3. Pathophysiological mechanisms and
‘long-COVID’ neuropsychiatric symptoms
Putative pathophysiological mechanisms involved in
newly diagnosed neuropsychiatric manifestations in patients without
a history of mental illness following the acute phase of COVID-19
are multifactorial, resulting either from long-term damage to the
brain as a consequence of direct viral effects, persistent systemic
inflammation or the psychosocial negative impact of the pandemic,
including social isolation, financial instability, fear of
infection, lockdowns and lack of family support (Fig. 1) (33-36).
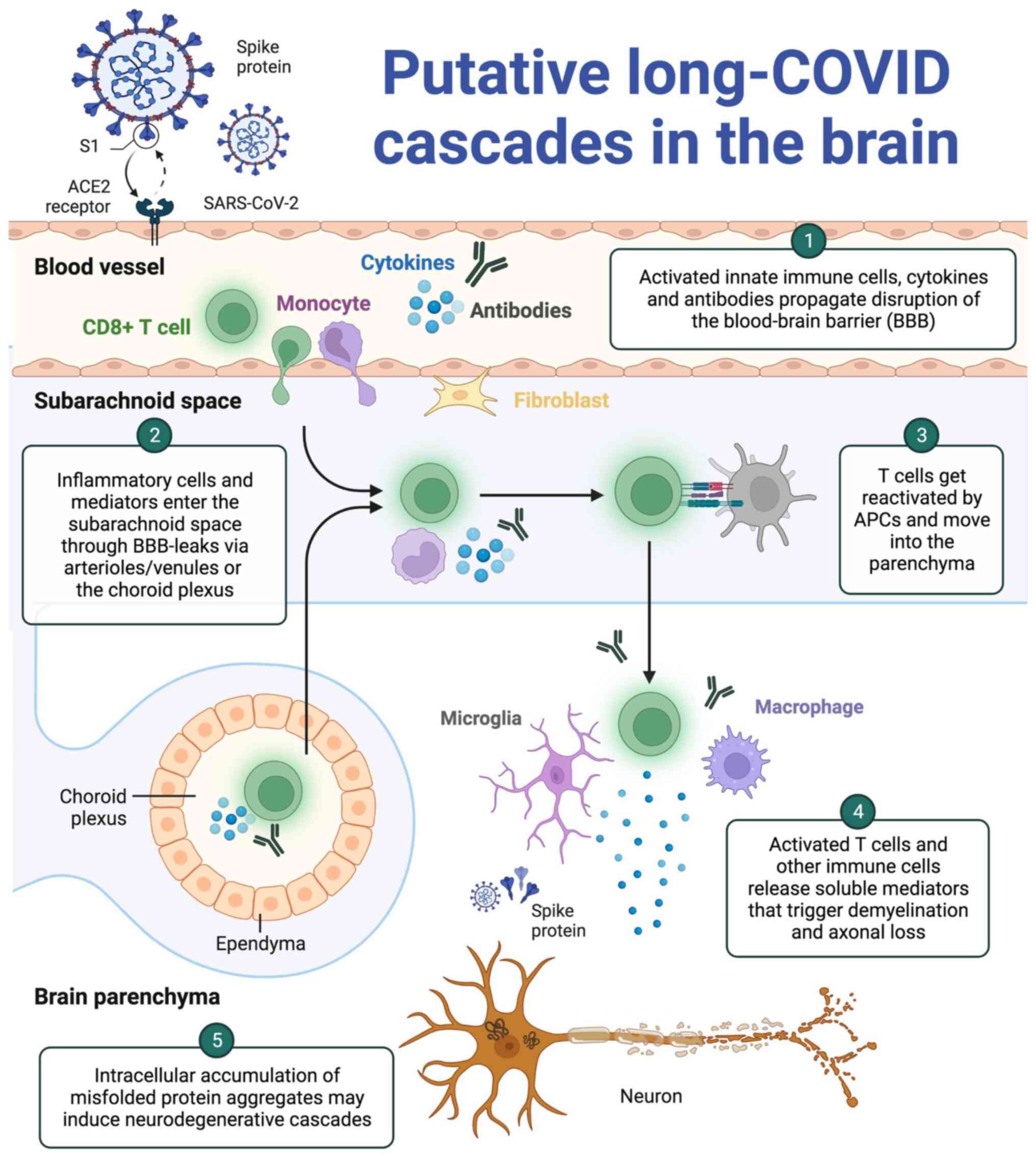 | Figure 1Putative ‘long-COVID’ cascades in the
brain. Following the acute phase of SARS-CoV-2 infection,
circulating (auto)antibodies, cytokines and activated innate immune
cells (including CD8+ T cells and monocytes) may persist
for several months during the post-COVID period, potentially
propagating LCS symptoms via a disruption of the BBB (77). Activated fibroblasts and
endothelial cells at the BBB lining are also implicated in BBB
disruption, causing increased BBB permeability and permitting the
transmigration of (auto)antibodies, cytokines and activated immune
cells in the subarachnoid space. Within the subarachnoid space, T
cells can be reactivated by antigen-presenting cells (78). Within the brain tissue, a limited
presence of SARS-CoV-2 spike protein or viral particles is
hypothesized in LCS; thus, neurovirulence is probably not strongly
associated with LCS pathophysiology (79). Conversely, autoantibodies,
cytokines and immune cells are considered the main orchestrators of
LCS, precipitating microglial activation and overt immune
reactions, which lead to demyelination and neuronal loss. At the
neuronal level, it is hypothesized that in LCS, the ongoing
neuroinflammatory processes may lead to accumulation of misfolded
protein aggregates, which could further induce metabolic stress and
neurodegenerative cascades (80).
This image was created with BioRender (https://biorender.com). SARS-CoV-2, severe acute
respiratory syndrome coronavirus 2; ACE2, angiotensin-converting
enzyme 2; BBB, blood-brain barrier; APCs, antigen-presenting cells;
LCS, long-COVID syndrome. |
OCD was described in case reports as occurring in
the weeks following the resolution of COVID-19 infection. In these
cases, OCD was associated with inflammatory factors, in particular
autoantibodies produced in response to the virus and targeting the
basal ganglia, causing neuronal injury that was seen as
abnormalities in cortico-basal ganglia-thalamocortical loops using
functional neuroimaging analyses (37-39).
These patients had no previous personal or family history of mental
illness, indicating that autoimmunity triggered by the virus
against convergent surface epitopes in the central nervous system
(CNS) was partly responsible for their symptoms. Moreover,
dysregulated microglial activation by SARS-CoV-2 outlasts the
initial immune host response, ensuing pathological synaptic
pruning, and leading to altered behaviour and cognition (40,41).
Psychological factors are also involved in the disease process, as
high-stress levels during the COVID-19 pandemic are linked with
high cortisol levels in the serum, which correlate with obsessive
symptoms, but are not related to compulsive behaviours (42).
Newly reported cognitive symptoms and attention
complaints by patients were found to be independent of disease
severity, suggesting conspicuous vulnerability of the CNS to
SARS-CoV-2 infection, as a consequence of high inflammatory
response and prolonged hospitalization (43). The dysregulated inflammatory
process in SARS-CoV-2 infection is due to high levels of
proinflammatory cytokines (IL-6 and TNF-α) secreted by activated
macrophages (44,45). Sleep disorders are also accompanied
by high IL-6 levels in the serum, indicating this as a possible
underlying mechanism in poor sleep quality in patients during the
‘long-COVID’ phase (46,47). This so called ‘cytokine storm’ is
shown to be caused by the S1 subunit of the SARS-CoV-2 spike
protein and contributes to disruption of the blood-brain barrier
(BBB), therefore facilitating the entry of the virus in the CNS
(48,49) and organ damage and/or failure
(50-52).
Another factor initiating the cytokine release is activation of the
NLR family pyrin domain-containing 3 inflammasome leading to
dissemination of inflammatory precursors and pyroptosis, a form of
cell death (53,54).
The hypometabolic state of different important brain
areas in the frontal and temporal lobes, due to cytokine and
neurotropism-related encephalopathy (55), contributes to the brain pathology
and is evident as diffuse slowing in electroencephalography and
bilateral frontotemporal hypoperfusion in arterial spin labelling
MRI (56,57). Neuroinvasion of the virus is
suspected to occur either through cranial nerves that innervate the
respiratory tract (particularly the olfactory nerve), or through
hematogenous spread by crossing the BBB or the blood-cerebrospinal
fluid barrier (58-60).
Once inside the CNS, the virus enters the cells expressing
angiotensin-converting enzyme 2, such as neurons, astrocytes,
oligodendrocytes and choroid plexus cells, with the choroidal
epithelial cells being distinctly susceptive to SARS-CoV-2
infection as suggested by a number of studies (61-66).
SARS-CoV-2 also induces infection-associated
thrombosis by platelet activation and endothelial damage, leading
to cerebrovascular events and subsequent ischemia (56,67).
The procoagulant effect of the virus is exerted by endothelial
damage of the infected organs, activation of the complement system
and NETs release through neutrophil recruitment (48,68,69).
This hypoxia-induced injury results in neuronal apoptosis and
disrupted brain function, impeding distal brain connectivity
(70).
Neuronal autoantibodies in the CSF have been
detected in a number of patients presenting with psychosis in the
post-COVID-19 context. A patient in May 2020 with SARS-CoV-2
infection and consequent anti-N-methyl-D-aspartate receptor
(NMDA-R) encephalitis was admitted with a number of psychiatric
symptoms, including psychomotor agitation, auditory hallucinations,
dyskinesias and anxiety, and had a background of substance abuse
but no past psychiatric history (71). NMDA-R antibodies were seen in a CSF
sample of this patient, while increased levels of CSF
autoantibodies have also been reported to be present in 11 patients
with SARS-CoV-2 infection and concomitant neurological symptoms
(72). This case, along with the
case of a previously healthy man with COVID-19-associated catatonia
and IgG autoantibodies against several murine proteins detected in
immunohistochemistry (with marked staining in neuronal cells in the
hippocampus, somatosensory cortex, and thalamus, the ependymal
cells of the ventricles and choroid plexus, along with the neuropil
of the caudate putamen), suggests a form of psychopathology arising
from autoimmune encephalitis attributed to COVID-19 infection
(73-75).
Further research in these areas is needed, as well
as close monitoring of neuropsychological function in patients with
COVID-19 months after disease recovery. New COVID-19 variants are
rapidly emerging across the world and it remains unclear how
individuals infected with these strains will be impacted in the
long term (76).
4. Conclusions
The present review provided a comprehensive overview
of the currently published epidemiological data on new-onset
neuropsychiatric manifestations associated with ‘long COVID’
syndrome, as well as insights into the underlying putative
pathophysiological mechanisms implicated in the development of
new-onset neuropsychiatric symptoms in COVID-19 survivors. While
there is evidence of an association between SARS-CoV-2 infection
and subsequent occurrence of neuropsychiatric symptoms, considering
possible unobserved confounding0, further research using approaches
less susceptible to bias is required with a view to establishing
causal relationships. Furthermore, follow-up of patients recovering
from COVID-19 by interdisciplinary health care teams and the
application of well-documented diagnostic criteria of
neuropsychiatric disorders are essential to ensure the correct
differential diagnosis of ‘long-COVID’ syndrome in clinical
practice.
Acknowledgements
Not applicable.
Funding
Funding: No funding was received.
Availability of data and materials
Not applicable.
Authors' contributions
VE, MIS, MD, NSi, EK and MM wrote the original
draft, edited and critically revised the manuscript. GT, VZ, SPK,
JNT, DAS, PF, NSm and ER critically revised and edited the
manuscript. All authors substantially contributed to the
conception, writing and revision of the work. All authors have read
and approved the final version of the manuscript. Data
authentication is not applicable.
Ethics approval and consent to
participate
Not applicable.
Patient consent for publication
Not applicable.
Competing interests
DAS is the Editor-in-Chief for the journal, but had
no personal involvement in the reviewing process, or any influence
in terms of adjudicating the final decision, for this article. The
other authors declare that they have no competing interests.
References
|
1
|
Zoumpourlis V, Goulielmaki M, Rizos E,
Baliou S and Spandidos DA: [Comment] The COVID-19 pandemic as a
scientific and social challenge in the 21st century. Mol Med Rep.
22:3035–3048. 2020.PubMed/NCBI View Article : Google Scholar
|
|
2
|
Tsamakis K, Tsiptsios D, Ouranidis A,
Mueller C, Schizas D, Terniotis C, Nikolakakis N, Tyros G,
Kympouropoulos S, Lazaris A, et al: COVID-19 and its consequences
on mental health (Review). Exp Ther Med. 21(244)2021.PubMed/NCBI View Article : Google Scholar
|
|
3
|
Tsamakis K, Triantafyllis AS, Tsiptsios D,
Spartalis E, Mueller C, Tsamakis C, Chaidou S, Spandidos DA, Fotis
L, Economou M and Rizos E: COVID-19 related stress exacerbates
common physical and mental pathologies and affects treatment
(Review). Exp Ther Med. 20:159–162. 2020.PubMed/NCBI View Article : Google Scholar
|
|
4
|
Efstathiou V, Stefanou MI, Siafakas N,
Makris M, Tsivgoulis G, Zoumpourlis V, Spandidos DA, Smyrnis N and
Rizos E: Suicidality and COVID-19: Suicidal ideation, suicidal
behaviors and completed suicides amidst the COVID-19 pandemic
(Review). Exp Ther Med. 23(107)2022.PubMed/NCBI View Article : Google Scholar
|
|
5
|
Giannopoulou I, Galinaki S, Kollintza E,
Adamaki M, Kympouropoulos S, Alevyzakis E, Tsamakis K, Tsangaris I,
Spandidos DA, Siafakas N, et al: COVID-19 and post-traumatic stress
disorder: The perfect ‘storm’ for mental health (Review). Exp Ther
Med. 22(1162)2021.PubMed/NCBI View Article : Google Scholar
|
|
6
|
Centers for Disease Control and Prevention
(CDC): Post-COVID conditions: Information for healthcare providers,
2021. Available at: https://www.cdc.gov/coronavirus/2019-ncov/hcp/clinical-care/post-covid-conditions.html.
|
|
7
|
Deer RR, Rock MA, Vasilevsky N, Carmody L,
Rando H, Anzalone AJ, Basson MD, Bennett TD, Bergquist T, Boudreau
EA, et al: Characterizing long COVID: Deep phenotype of a complex
condition. EBioMedicine. 74(103722)2021.PubMed/NCBI View Article : Google Scholar
|
|
8
|
Brodin P: Immune determinants of COVID-19
disease presentation and severity. Nat Med. 27:28–33.
2021.PubMed/NCBI View Article : Google Scholar
|
|
9
|
Stefanou MI, Palaiodimou L, Bakola E,
Smyrnis N, Papadopoulou M, Paraskevas GP, Rizos E, Boutati E,
Grigoriadis N, Krogias C, et al: Neurological manifestations of
long-COVID syndrome: A narrative review. Ther Adv Chronic Dis.
13(20406223221076890)2022.PubMed/NCBI View Article : Google Scholar
|
|
10
|
Efstathiou V, Stefanou MI, Demetriou M,
Siafakas N, Makris M, Tsivgoulis G, Zoumpourlis V, Kympouropoulos
SP, Tsoporis JN, Spandidos DA, et al: Long COVID and
neuropsychiatric manifestations (Review). Exp Ther Med.
23(363)2022.PubMed/NCBI View Article : Google Scholar
|
|
11
|
Schou TM, Joca S, Wegener G and
Bay-Richter C: Psychiatric and neuropsychiatric sequelae of
COVID-19-A systematic review. Brain Behav Immun. 97:328–348.
2021.PubMed/NCBI View Article : Google Scholar
|
|
12
|
Bourmistrova NW, Solomon T, Braude P,
Strawbridge R and Carter B: Long-term effects of COVID-19 on mental
health: A systematic review. J Affect Disord. 299:118–125.
2022.PubMed/NCBI View Article : Google Scholar
|
|
13
|
Ceban F, Ling S, Lui LMW, Lee Y, Gill H,
Teopiz KM, Rodrigues NB, Subramaniapillai M, Di Vincenzo JD, Cao B,
et al: Fatigue and cognitive impairment in post-COVID-19 syndrome:
A systematic review and meta-analysis. Brain Behav Immun.
101:93–135. 2021.PubMed/NCBI View Article : Google Scholar
|
|
14
|
Renaud-Charest O, Lui LMW, Eskander S,
Ceban F, Ho R, Di Vincenzo JD, Rosenblat JD, Lee Y,
Subramaniapillai M and McIntyre RS: Onset and frequency of
depression in post-COVID-19 syndrome: A systematic review. J
Psychiatr Res. 144:129–137. 2021.PubMed/NCBI View Article : Google Scholar
|
|
15
|
Shanbehzadeh S, Tavahomi M, Zanjari N,
Ebrahimi-Takamjani I and Amiri-arimi S: Physical and mental health
complications post-COVID-19: Scoping review. J Psychosom Res.
147(110525)2021.PubMed/NCBI View Article : Google Scholar
|
|
16
|
Taquet M, Luciano S, Geddes JR and
Harrison PJ: Bidirectional associations between COVID-19 and
psychiatric disorder: Retrospective cohort studies of 62 354
COVID-19 cases in the USA. Lancet Psychiatry. 8:130–140.
2021.PubMed/NCBI View Article : Google Scholar
|
|
17
|
Iosifescu AL, Hoogenboom WS, Buczek AJ,
Fleysher R and Duong TQ: New-onset and persistent neurological and
psychiatric sequelae of COVID-19 compared to influenza: A
retrospective cohort study in a large New York City healthcare
network. Int J Methods Psychiatr Res. 31(e1914)2022.PubMed/NCBI View
Article : Google Scholar
|
|
18
|
Lund LC, Hallas J, Nielsen H, Koch A,
Mogensen SH, Brun NC, Christiansen CF, Thomsen RW and Pottegård A:
Post-acute effects of SARS-CoV-2 infection in individuals not
requiring hospital admission: A Danish population-based cohort
study. Lancet Infect Dis. 21:1373–1382. 2021.PubMed/NCBI View Article : Google Scholar
|
|
19
|
Coleman B, Casiraghi E, Blau H, Chan L,
Haendel MA, Laraway B, Callahan TJ, Deer RR, Wilkins KJ, Reese J
and Robinson PN: Risk of new-onset psychiatric sequelae of COVID-19
in the early and late post-acute phase. World Psychiatry.
21:319–320. 2022.PubMed/NCBI View Article : Google Scholar
|
|
20
|
Taquet M, Geddes JR, Husain M, Luciano S
and Harrison PJ: 6-month neurological and psychiatric outcomes in
236 379 survivors of COVID-19: A retrospective cohort study using
electronic health records. Lancet Psychiatry. 8:416–427.
2021.PubMed/NCBI View Article : Google Scholar
|
|
21
|
Abel KM, Carr MJ, Ashcroft DM, Chalder T,
Chew-Graham CA, Hope H, Kapur N, McManus S, Steeg S, Webb RT and
Pierce M: Association of SARS-CoV-2 infection with psychological
distress, psychotropic prescribing, fatigue, and sleep problems
among UK primary care patients. JAMA Netw Open.
4(e2134803)2021.PubMed/NCBI View Article : Google Scholar
|
|
22
|
Patel N, Dahman B and Bajaj JS:
Development of new mental and physical health sequelae among US
veterans after COVID-19. J Clin Med. 11(3390)2022.PubMed/NCBI View Article : Google Scholar
|
|
23
|
Chen JI, Hickok A, O'Neill AC,
Niederhausen M, Laliberte AZ, Govier DJ, Edwards ST, Gordon HS,
Slatore CG, Weaver FM, et al: Psychiatric disorders newly diagnosed
among veterans subsequent to hospitalization for COVID-19.
Psychiatry Res. 312(114570)2022.PubMed/NCBI View Article : Google Scholar
|
|
24
|
Clift AK, Ranger TA, Patone M, Coupland
CAC, Hatch R, Thomas K, Hippisley-Cox J and Watkinson P:
Neuropsychiatric ramifications of severe COVID-19 and other severe
acute respiratory infections. JAMA Psychiatry. 79:690–698.
2022.PubMed/NCBI View Article : Google Scholar
|
|
25
|
Xie Y, Xu E and Al-Aly Z: Risks of mental
health outcomes in people with covid-19: Cohort study. BMJ.
376(e068993)2022.PubMed/NCBI View Article : Google Scholar
|
|
26
|
Park HY, Song IA, Lee SH, Sim MY, Oh HS,
Song KH, Yu ES, Park HY and Oh TK: Prevalence of mental illness
among COVID-19 survivors in South Korea: Nationwide cohort. BJPsych
Open. 7(e183)2021.PubMed/NCBI View Article : Google Scholar
|
|
27
|
Rivera-Izquierdo M, Láinez-Ramos-Bossini
AJ, de Alba IG, Ortiz-González-Serna R, Serrano-Ortiz Á,
Fernández-Martínez NF, Ruiz-Montero R and Cervilla JA: Long COVID
12 months after discharge: Persistent symptoms in patients
hospitalised due to COVID-19 and patients hospitalised due to other
causes-a multicentre cohort study. BMC Med. 20(92)2022.PubMed/NCBI View Article : Google Scholar
|
|
28
|
Jacob L, Koyanagi A, Smith L, Bohlken J,
Haro JM and Kostev K: No significant association between COVID-19
diagnosis and the incidence of depression and anxiety disorder? A
retrospective cohort study conducted in Germany. J Psychiatr Res.
147:79–84. 2022.PubMed/NCBI View Article : Google Scholar
|
|
29
|
Smith CM, Gilbert EB, Riordan PA, Helmke
N, von Isenburg M, Kincaid BR and Shirey KG: COVID-19-associated
psychosis: A systematic review of case reports. Gen Hosp
Psychiatry. 73:84–100. 2021.PubMed/NCBI View Article : Google Scholar
|
|
30
|
Alkhamees AA: Obsessive-compulsive
disorder post-COVID-19: A case presentation. Egypt J Neurol
Psychiatr Neurosurg. 57(150)2021.PubMed/NCBI View Article : Google Scholar
|
|
31
|
Webster R and Holroyd S: Prevalence of
psychotic symptoms in delirium. Psychosomatics. 41:519–522.
2000.PubMed/NCBI View Article : Google Scholar
|
|
32
|
Rogers JP and David AS: A longer look at
COVID-19 and neuropsychiatric outcomes. Lancet Psychiatry.
8:351–352. 2021.PubMed/NCBI View Article : Google Scholar
|
|
33
|
Yang CP, Chang CM, Yang CC, Pariante CM
and Su KP: Long COVID and long chain fatty acids (LCFAs):
Psychoneuroimmunity implication of omega-3 LCFAs in delayed
consequences of COVID-19. Brain Behav Immun. 103:19–27.
2022.PubMed/NCBI View Article : Google Scholar
|
|
34
|
Druss BG: Addressing the COVID-19 pandemic
in populations with serious mental illness. JAMA Psychiatry.
77:891–892. 2020.PubMed/NCBI View Article : Google Scholar
|
|
35
|
Moreno C, Wykes T, Galderisi S, Nordentoft
M, Crossley N, Jones N, Cannon M, Correll CU, Byrne L, Carr S, et
al: How mental health care should change as a consequence of the
COVID-19 pandemic. Lancet Psychiatry. 7:813–824. 2020.PubMed/NCBI View Article : Google Scholar
|
|
36
|
Kola L: Global mental health and COVID-19.
Lancet Psychiatry. 7:655–657. 2020.PubMed/NCBI View Article : Google Scholar
|
|
37
|
Gerentes M, Pelissolo A, Rajagopal K,
Tamouza R and Hamdani N: Obsessive-compulsive disorder:
Autoimmunity and neuroinflammation. Curr Psychiatry Rep.
21(78)2019.PubMed/NCBI View Article : Google Scholar
|
|
38
|
Maia TV, Cooney RE and Peterson BS: The
neural bases of obsessive-compulsive disorder in children and
adults. Dev Psychopathol. 20:1251–1283. 2008.PubMed/NCBI View Article : Google Scholar
|
|
39
|
Uvais NA: Obsessive-compulsive disorder
following COVID-19 infection. Prim Care Companion CNS Disord.
23(21cr03063)2021.PubMed/NCBI View Article : Google Scholar
|
|
40
|
Frick L and Pittenger C: Microglial
dysregulation in OCD, tourette syndrome and PANDAS. J Immunol Res.
2016(8606057)2016.PubMed/NCBI View Article : Google Scholar
|
|
41
|
Awogbindin IO, Ben-Azu B, Olusola BA,
Akinluyi ET, Adeniyi PA, Di Paolo T and Tremblay MÈ: Microglial
implications in SARS-CoV-2 infection and COVID-19: Lessons from
viral RNA neurotropism and possible relevance to Parkinson's
disease. Front Cell Neurosci. 15(670298)2021.PubMed/NCBI View Article : Google Scholar
|
|
42
|
Morgado P, Freitas D, Bessa JM, Sousa N
and Cerqueira JJ: Perceived stress in obsessive-compulsive disorder
is related with obsessive but not compulsive symptoms. Front
Psychiatry. 4(21)2013.PubMed/NCBI View Article : Google Scholar
|
|
43
|
Pilotto A, Cristillo V, Cotti Piccinelli
S, Zoppi N, Bonzi G, Sattin D, Schiavolin S, Raggi A, Canale A,
Gipponi S, et al: Long-term neurological manifestations of
COVID-19: Prevalence and predictive factors. Neurol Sci.
42:4903–4907. 2021.PubMed/NCBI View Article : Google Scholar
|
|
44
|
Park MD: Macrophages: A Trojan horse in
COVID-19? Nat Rev Immunol. 20(351)2020.PubMed/NCBI View Article : Google Scholar
|
|
45
|
Tizenberg BN, Brenner LA, Lowry CA,
Okusaga OO, Benavides DR, Hoisington AJ, Benros ME, Stiller JW,
Kessler RC and Postolache TT: Biological and psychological factors
determining neuropsychiatric outcomes in COVID-19. Curr Psychiatry
Rep. 23(68)2021.PubMed/NCBI View Article : Google Scholar
|
|
46
|
Titze-de-Almeida R, da Cunha TR, dos
Santos Silva LD, Ferreira CS, Silva CP, Ribeiro AP, de Castro
Moreira Santos Júnior A, de Paula Brandão PR, Silva APB, da Rocha
MCO, et al: Persistent, new-onset symptoms and mental health
complaints in long COVID in a Brazilian cohort of non-hospitalized
patients. BMC Infect Dis. 22(133)2022.PubMed/NCBI View Article : Google Scholar
|
|
47
|
Hong S, Mills PJ, Loredo JS, Adler KA and
Dimsdale JE: The association between interleukin-6, sleep and
demographic characteristics. Brain Behav Immun. 19:165–172.
2005.PubMed/NCBI View Article : Google Scholar
|
|
48
|
Iadecola C, Anrather J and Kamel H:
Effects of COVID-19 on the nervous system. Cell. 183:16–27.e1.
2020.PubMed/NCBI View Article : Google Scholar
|
|
49
|
Erickson MA and Banks WA: Neuroimmune axes
of the blood-brain barriers and blood-brain interfaces: Bases for
physiological regulation, disease states and pharmacological
interventions. Pharmacol Rev. 70:278–314. 2018.PubMed/NCBI View Article : Google Scholar
|
|
50
|
Giamarellos-Bourboulis EJ, Netea MG,
Rovina N, Akinosoglou K, Antoniadou A, Antonakos N, Damoraki G,
Gkavogianni T, Adami ME, Katsaounou P, et al: Complex immune
dysregulation in COVID-19 patients with severe respiratory failure.
Cell Host Microbe. 27:992–1000.e3. 2020.PubMed/NCBI View Article : Google Scholar
|
|
51
|
Cheon SY and Koo BN: Inflammatory response
in COVID-19 patients resulting from the interaction of the
inflammasome and SARS-CoV-2. Int J Mol Sci. 22(7914)2021.PubMed/NCBI View Article : Google Scholar
|
|
52
|
Leisman DE, Ronner L, Pinotti R, Taylor
MD, Sinha P, Calfee CS, Hirayama AV, Mastroiani F, Turtle CJ,
Harhay MO, et al: Cytokine elevation in severe and critical
COVID-19: A rapid systematic review, meta-analysis, and comparison
with other inflammatory syndromes. Lancet Respir Med. 8:1233–1244.
2020.PubMed/NCBI View Article : Google Scholar
|
|
53
|
Liu X, Zhang Z, Ruan J, Pan Y, Magupalli
VG, Wu H and Lieberman J: Inflammasome-activated gasdermin D causes
pyroptosis by forming membrane pores. Nature. 535:153–158.
2016.PubMed/NCBI View Article : Google Scholar
|
|
54
|
Zhao N, Di B and Xu LL: The NLRP3
inflammasome and COVID-19: Activation, pathogenesis and therapeutic
strategies. Cytokine Growth Factor Rev. 61:2–15. 2021.PubMed/NCBI View Article : Google Scholar
|
|
55
|
Shah P, Patel J, Soror NN and Kartan R:
Encephalopathy in COVID-19 patients. Cureus.
13(e16620)2021.PubMed/NCBI View Article : Google Scholar
|
|
56
|
Moore P, Esmail F, Qin S, Nand S and Berg
S: Hypercoagulability of COVID-19 and neurological complications: A
review. J Stroke Cerebrovasc Dis. 31(106163)2022.PubMed/NCBI View Article : Google Scholar
|
|
57
|
Helms J, Kremer S, Merdji H, Clere-Jehl R,
Schenck M, Kummerlen C, Collange O, Boulay C, Fafi-Kremer S, Ohana
M, et al: Neurologic features in severe SARS-CoV-2 infection. N
Engl J Med. 382:2268–2270. 2020.PubMed/NCBI View Article : Google Scholar
|
|
58
|
Bauer L, Laksono BM, de Vrij FMS, Kushner
SA, Harschnitz O and van Riel D: The neuroinvasiveness,
neurotropism, and neurovirulence of SARS-CoV-2. Trends Neurosci.
45:358–368. 2022.PubMed/NCBI View Article : Google Scholar
|
|
59
|
Ludlow M, Kortekaas J, Herden C, Hoffmann
B, Tappe D, Trebst C, Griffin DE, Brindle HE, Solomon T, Brown AS,
et al: Neurotropic virus infections as the cause of immediate and
delayed neuropathology. Acta Neuropathol. 131:159–184.
2016.PubMed/NCBI View Article : Google Scholar
|
|
60
|
Koyuncu OO, Hogue IB and Enquist LW: Virus
infections in the nervous system. Cell Host Microbe. 13:379–393.
2013.PubMed/NCBI View Article : Google Scholar
|
|
61
|
Fodoulian L, Tuberosa J, Rossier D,
Boillat M, Kan C, Pauli V, Egervari K, Lobrinus JA, Landis BN,
Carleton A and Rodriguez I: SARS-CoV-2 receptors and entry genes
are expressed in the human olfactory neuroepithelium and brain.
iScience. 23(101839)2020.PubMed/NCBI View Article : Google Scholar
|
|
62
|
Lukiw WJ, Pogue A and Hill JM: SARS-CoV-2
infectivity and neurological targets in the brain. Cell Mol
Neurobiol. 42:217–224. 2022.PubMed/NCBI View Article : Google Scholar
|
|
63
|
Jacob F, Pather SR, Huang WK, Zhang F,
Wong SZH, Zhou H, Cubitt B, Fan W, Chen CZ, Xu M, et al: Human
pluripotent stem cell-derived neural cells and brain organoids
reveal SARS-CoV-2 neurotropism predominates in choroid plexus
epithelium. Cell Stem Cell. 27:937–950.e9. 2020.PubMed/NCBI View Article : Google Scholar
|
|
64
|
Pellegrini L, Albecka A, Mallery DL,
Kellner MJ, Paul D, Carter AP, James LC and Lancaster MA:
SARS-CoV-2 infects the brain choroid plexus and disrupts the
blood-CSF barrier in human brain organoids. Cell Stem Cell.
27:951–961.e5. 2020.PubMed/NCBI View Article : Google Scholar
|
|
65
|
McMahon CL, Staples H, Gazi M, Carrion R
and Hsieh J: SARS-CoV-2 targets glial cells in human cortical
organoids. Stem Cell Reports. 16:1156–1164. 2021.PubMed/NCBI View Article : Google Scholar
|
|
66
|
Zhang BZ, Chu H, Han S, Shuai H, Deng J,
Hu YF, Gong HR, Lee AC, Zou Z, Yau T, et al: SARS-CoV-2 infects
human neural progenitor cells and brain organoids. Cell Res.
30:928–931. 2020.PubMed/NCBI View Article : Google Scholar
|
|
67
|
Beristain-Covarrubias N, Perez-Toledo M,
Thomas MR, Henderson IR, Watson SP and Cunningham AF: Understanding
infection-induced thrombosis: Lessons learned from animal models.
Front Immunol. 10(2569)2019.PubMed/NCBI View Article : Google Scholar
|
|
68
|
Goshua G, Pine AB, Meizlish ML, Chang CH,
Zhang H, Bahel P, Baluha A, Bar N, Bona RD, Burns AJ, et al:
Endotheliopathy in COVID-19-associated coagulopathy: Evidence from
a single-centre, cross-sectional study. Lancet Haematol.
7:e575–e582. 2020.PubMed/NCBI View Article : Google Scholar
|
|
69
|
Ramlall V, Thangaraj PM, Meydan C, Foox J,
Butler D, Kim J, May B, De Freitas JK, Glicksberg BS, Mason CE, et
al: Immune complement and coagulation dysfunction in adverse
outcomes of SARS-CoV-2 infection. Nat Med. 26:1609–1615.
2020.PubMed/NCBI View Article : Google Scholar
|
|
70
|
Groff D, Sun A, Ssentongo AE, Ba DM,
Parsons N, Poudel GR, Lekoubou A, Oh JS, Ericson JE, Ssentongo P
and Chinchilli VM: Short-term and long-term rates of postacute
sequelae of SARS-CoV-2 infection: A systematic review. JAMA Netw
Open. 4(e2128568)2021.PubMed/NCBI View Article : Google Scholar
|
|
71
|
Panariello A, Bassetti R, Radice A,
Rossotti R, Puoti M, Corradin M, Moreno M and Percudani M:
Anti-NMDA receptor encephalitis in a psychiatric Covid-19 patient:
A case report. Brain Behav Immun. 87:179–181. 2020.PubMed/NCBI View Article : Google Scholar
|
|
72
|
Franke C, Ferse C, Kreye J, Reincke SM,
Sanchez-Sendin E, Rocco A, Steinbrenner M, Angermair S, Treskatsch
S, Zickler D, et al: High frequency of cerebrospinal fluid
autoantibodies in COVID-19 patients with neurological symptoms.
Brain Behav Immun. 93:415–419. 2021.PubMed/NCBI View Article : Google Scholar
|
|
73
|
Mulder J, Feresiadou A, Fällmar D,
Frithiof R, Virhammar J, Rasmusson A, Rostami E, Kumlien E and
Cunningham JL: Autoimmune encephalitis presenting with malignant
catatonia in a 40-year-old male patient with COVID-19. Am J
Psychiatry. 178:485–489. 2021.PubMed/NCBI View Article : Google Scholar
|
|
74
|
Endres D, Maier V, Leypoldt F, Wandinger
KP, Lennox B, Pollak TA, Nickel K, Maier S, Feige B, Domschke K, et
al: Autoantibody-associated psychiatric syndromes: A systematic
literature review resulting in 145 cases. Psychol Med. 52:1–12.
2020.PubMed/NCBI View Article : Google Scholar : (Epub ahead of
print).
|
|
75
|
Watson CJ, Thomas RH, Solomon T, Michael
BD, Nicholson TR and Pollak TA: COVID-19 and psychosis risk: Real
or delusional concern? Neurosci Lett. 741(135491)2021.PubMed/NCBI View Article : Google Scholar
|
|
76
|
Desai AD, Lavelle M, Boursiquot BC and Wan
EY: Long-term complications of COVID-19. Am J Physiol Cell Physiol.
322:C1–C11. 2022.PubMed/NCBI View Article : Google Scholar
|
|
77
|
Phetsouphanh C, Darley DR, Wilson DB, Howe
A, Munier CML, Patel SK, Juno JA, Burrell LM, Kent SJ, Dore GJ, et
al: Immunological dysfunction persists for 8 months following
initial mild-to-moderate SARS-CoV-2 infection. Nat Immunol.
23:210–216. 2022.PubMed/NCBI View Article : Google Scholar
|
|
78
|
Farzi R, Aghbash PS, Eslami N, Azadi A,
Shamekh A, Hemmat N, Entezari-Maleki T and Baghi HB: The role of
antigen-presenting cells in the pathogenesis of COVID-19. Pathol
Res Pract. 233(153848)2022.PubMed/NCBI View Article : Google Scholar
|
|
79
|
Spudich S and Nath A: Nervous system
consequences of COVID-19. Science. 375:267–269. 2022.PubMed/NCBI View Article : Google Scholar
|
|
80
|
Sulzer D, Antonini A, Leta V, Nordvig A,
Smeyne RJ, Goldman JE, Al-Dalahmah O, Zecca L, Sette A, Bubacco L,
et al: COVID-19 and possible links with Parkinson's disease and
parkinsonism: From bench to bedside. NPJ Parkinsons Dis.
6(18)2020.PubMed/NCBI View Article : Google Scholar
|














