Introduction
Sepsis, also called septicemia, is a serious
complication of patients undergoing pathogen infection, trauma,
burn, hypoxia, reperfusion injury and surgery, which could affect
myocardial contractility, decreased organ oxygen uptake capacity,
and can lead to septic shock and multiple organ dysfunction
syndrome. This state is called systemic inflammatory response
syndrome (1,2). The incidence of sepsis is extremely high
in the intensive care unit (ICU), with a mortality of ≤40–80%. As
reported, the kidney is one of the most susceptible target organs
of sepsis (3). Approximately 50% of
patients suffer from acute kidney injury (AKI) caused by sepsis.
Notably, mortality of these patients is as high as 70% (4,5). However,
the mechanisms of sepsis-induced AKI remain unclear and effective
therapy strategies are also lacking.
Inflammatory factors, such as interleukin 6 (IL-6),
IL-18 and tumor necrosis factor α (TNF-α), play an important role
in the pathological and physiological process, particularly IL-18.
As recently reported, IL-18 was a sensitive and specific biomarker
of the AKI diagnosis and predicted mortality of patients (6). From other aspects, IL-18 induced
expression of TNF-α and IL-6 and made the inflammatory reaction
more serious, which contributed to organ injuries (7). Thus, modulation of the inflammatory
reaction in sepsis is extremely important to protect against organ
injuries, including kidneys.
As a commonly used anesthetic, dexmedetomidine (DEX)
is widely used in the ICU and the surgical room. DEX is a highly
selective α-2 adrenoceptor agonist and inhibits sympathetic
activity effectively (8,9). In recent years, increasing basic and
clinical studies have proved that DEX protected against different
types of organs. Duan et al (10) reported that DEX was not neurotoxic and
attenuated neuroapoptosis; other studies indicated that DEX
application following cardiac surgery was associated with a lower
incidence of atrial arrhythmias (11);
more noteworthy, it was recently reported that DEX reduced
intestinal and hepatic injury following hepatectomy and protected
against ischemia/reperfusion injury in rat kidney through
inhibiting apoptosis (12,13). However, mechanisms of the DEX
protective effects are unclear, particularly for renal protection.
Thus, the purpose of the present study was to explore the
protective effects of DEX on the renal tissue of rats in
lipopolysaccharide (LPS)-induced AKI models and its relative
mechanisms mediated by α-2 adrenoceptor activities.
Materials and methods
Animals and treatment
All the experiments followed the National Institutes
of Health criteria for the care and use of laboratory animals. The
study was also approved by the Laboratory Animal Care Committee of
Sun Yat-sen University (Guangzhou, China). Male Sprague Dawley rats
(180–220 g) were purchased from the Laboratory Animal Center of Sun
Yat-sen University and randomly divided into four groups: Sham,
LPS, DEX + LPS and yohimbine (YOH) + DEX + LPS. Every group
contained 8 samples. Rats were fasted for 12 hours, but not
forbidden to drink. The rat sepsis models were generated through
LPS injection (5 mg/kg; Sigma-Aldrich, St. Louis, MO, USA) in the
tail vein (14). Rats were pretreated
with DEX (10 µg/kg; Jiangsu Hengrui Medicine Co., Ltd.,
Lianyungang, Jiangsu, China) 10 min before LPS injection (15). A unique α-2-adrenergic receptor
antagonist, YOH (1 mg/kg; Sigma Aldrich), was injected
intraperitoneally 30 min before DEX exposure (16). All the rats were sacrificed 4 h later.
Blood samples were obtained from the abdominal artery to measure
creatinine (Cr) and blood urea nitrogen (BUN); IL-6, IL-18 and
TNF-α. The left kidney was removed, fixed in 10% formalin for
tissue pathological analysis, and the right was used to detect the
expression of kidney injury molecule-1 (KIM-1) and high mobility
group protein 1 (HMGB-1).
Assessment of kidney damage
Cr and BUN were measured in blood samples with an
automatic biochemistry analyzer (Hitachi 7600-020/7170A; Hitachi
High-Technologies Corp., Tokyo, Japan). Kidney specimens were fixed
in 10% buffered formalin, embedded in paraffin and processed for
hematoxylin and eosin staining (Nanjing Keygen Biotech Co., Ltd.,
Nanjing, Jiangsu, China) for morphological examination. Each
microsection was counted in five randomly selected areas/slide at
magnification, x400. The renal injury quantification method was
performed using a 0–3 grading system, as described by Hamar et
al (17).
Measurement of plasma IL-6, IL-18 and
TNF-α
Blood samples were collected in heparinized tubes
and centrifuged at 2,500 × g for 15 min. Plasma was stored at
−80˚C. Serum IL-6, IL-18 and TNF-α were measured by ELISA kits
according to the manufacturer's instructions (IL-6, IL-18 and TNF-α
assay kits; all purchased from Nanjing Keygen Biotech. Co.,
Ltd).
Western blot analysis of KIM-1 and
HMGB-1
Western blot analysis was used to calculate the
protein expression following the renal tissue protein extraction.
The sample was solubilized in sodium dodecyl sulfate (SDS) loading
buffer (Bio-Rad, Hercules, CA, USA) by boiling. The samples were
loaded onto a 10% polyacrylamide gel (Invitrogen Life Technologies,
Carlsbad, CA, USA) and SDS-PAGE (Bio-Rad) was conducted. The
samples were subsequently transferred to a polyvinylidene
difluoride (Bio-Rad) membrane. Membranes were further incubated
overnight at 4˚C with specific antibodies against KIM-1 (cat. no.
sc-47495, 1:2,000 dilution; Santa Cruz Biotechnology, Inc., Dallas,
TX, USA) and HMGB-1 (cat. no. sc-26351, 1:2,000 dilution; Santa
Cruz Biotechnology, Inc.). All the blots were subsequently washed
and incubated with respective horseradish peroxidase-coupled
secondary antibodies (cat. no. sc-2020, 1:1,500 dilution; Santa
Cruz Biotechnology, Inc.) at room temperature for one hour. The
protein bands were detected by an enhanced chemiluminescent
detective system (Amersham Biosciences UK Ltd., Little Chalfont,
UK) and were quantified using the Quantity One software package
(Bio-Rad). GAPDH (1:2,000 dilution; Thermo Fisher Scientific Inc.,
Fremont, CA, USA) was presented as the internal control to
calculate the ratio of optical density, and values were compared
with those of the Sham groups.
Statistical analysis
All the data were analyzed using SPSS software,
version 12.0 (SPSS, Inc., Chicago, IL, USA). The differences
between groups were analyzed using one-way analysis of variance,
followed by Tukey post hoc comparisons. A two-tailed P<0.05 was
considered to indicate a statistically significant difference.
Results
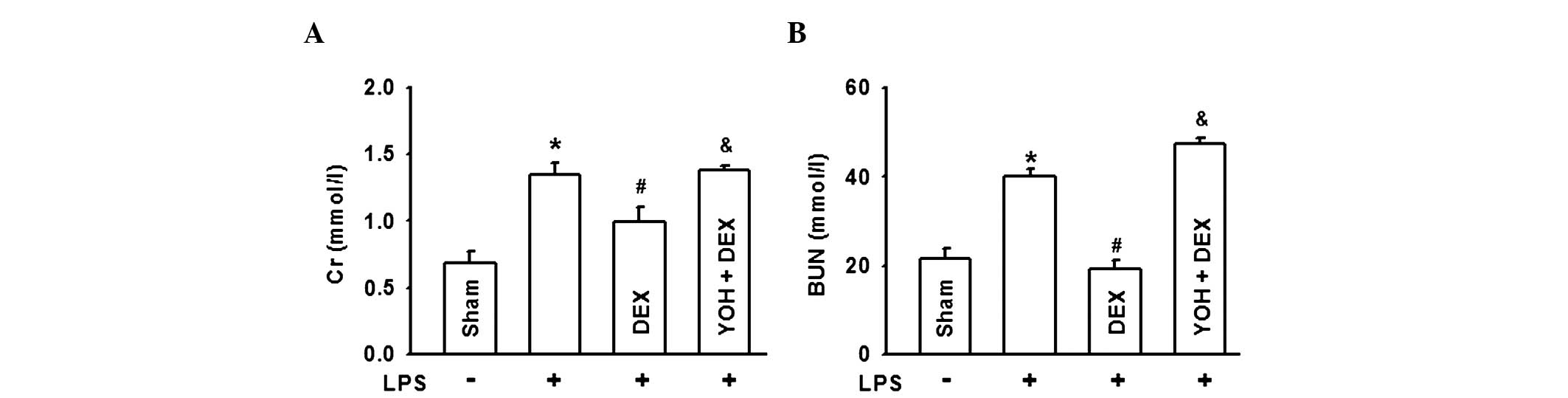
DEX decreases BUN and Cr levels in
LPS-induced AKI and YOH reverses the protective effect of DEX
In order to explore the protective effect of DEX on
AKI in sepsis, rat sepsis models were established with LPS
injection in the tail vein. The results in Fig. 1 showed that serum Cr and BUN levels
evidently increased, nearly two-fold compared to the Sham group,
which illustrated that the kidney was damaged severely. When rats
were pretreated with DEX, levels of serum Cr and BUN were reduced;
however, this protective effect of DEX was reversed by the
α-2-adrenergic receptor antagonist, YOH. When α-2 adrenoceptor was
antagonized by YOH, the protective effect of DEX was
diminished.
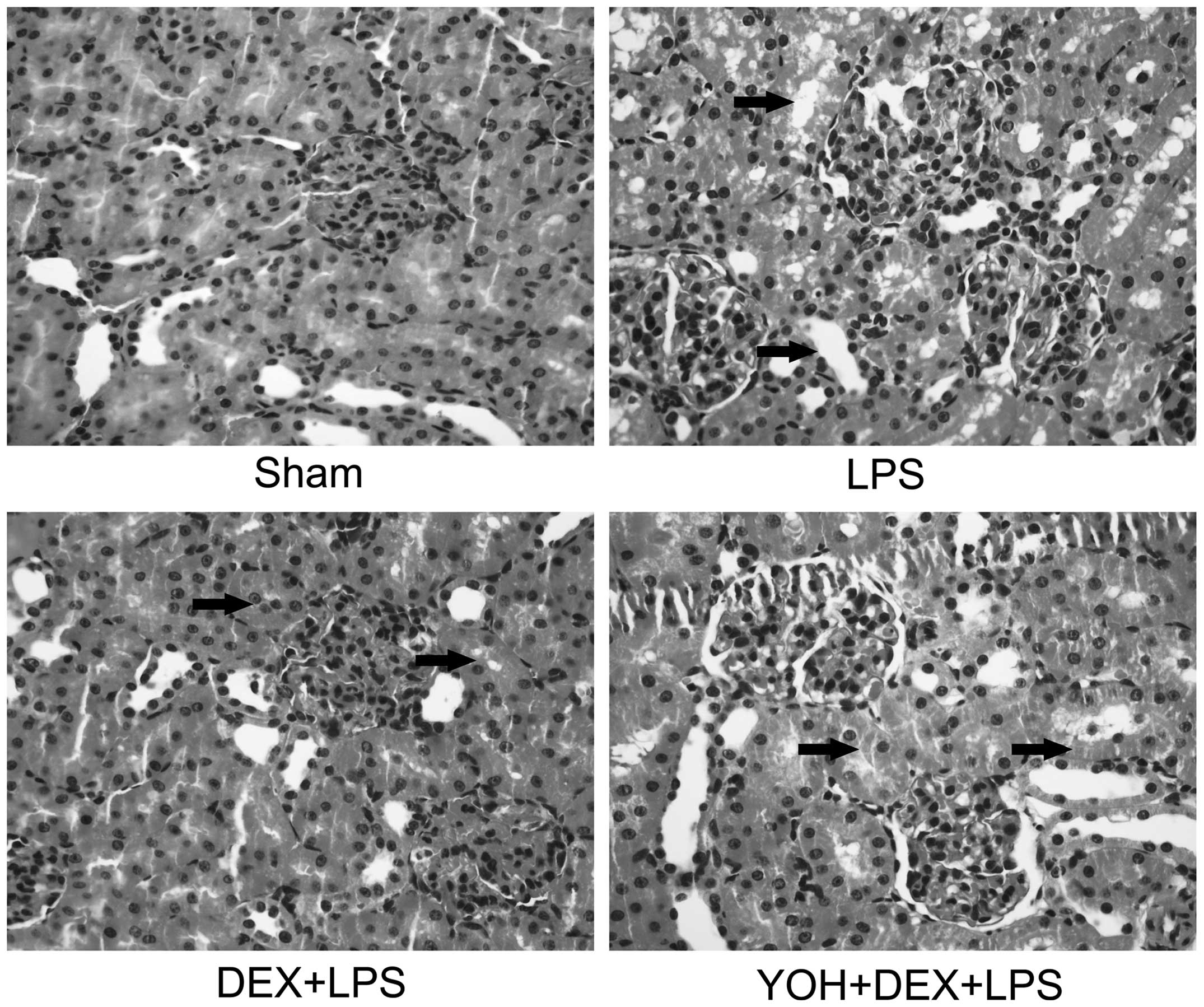
DEX ameliorates the pathological
damage of kidneys in LPS-induced AKI and YOH reverses the
protective effect of DEX
In order to further confirm the protective effect of
DEX, the change of renal pathological morphology was analyzed in
the rat sepsis models according to the Hamar score method (17). The results in Fig. 2 indicated that in the Sham group,
normal kidney tissues were without lumen expansion and epithelial
cell flattening in the glomerular and renal tubule; however, when
rats were exposed to LPS, kidney pathological damage was clear:
Renal tubular epithelial cell degeneration, renal tubular cavity
expansion and tube formation and renal interstitial inflammatory
cell infiltration are all serious. DEX application protected
against LPS-induced renal damage, which was reversed by YOH. Rat
pathological injury was coincidental with the levels of serum Cr
and BUN in Fig. 1. The results in
Figs. 1 and 2 indicated that the protective effect of DEX
was relative with its function of activating α-2 adrenoceptor and
inhibiting sympathetic activity.
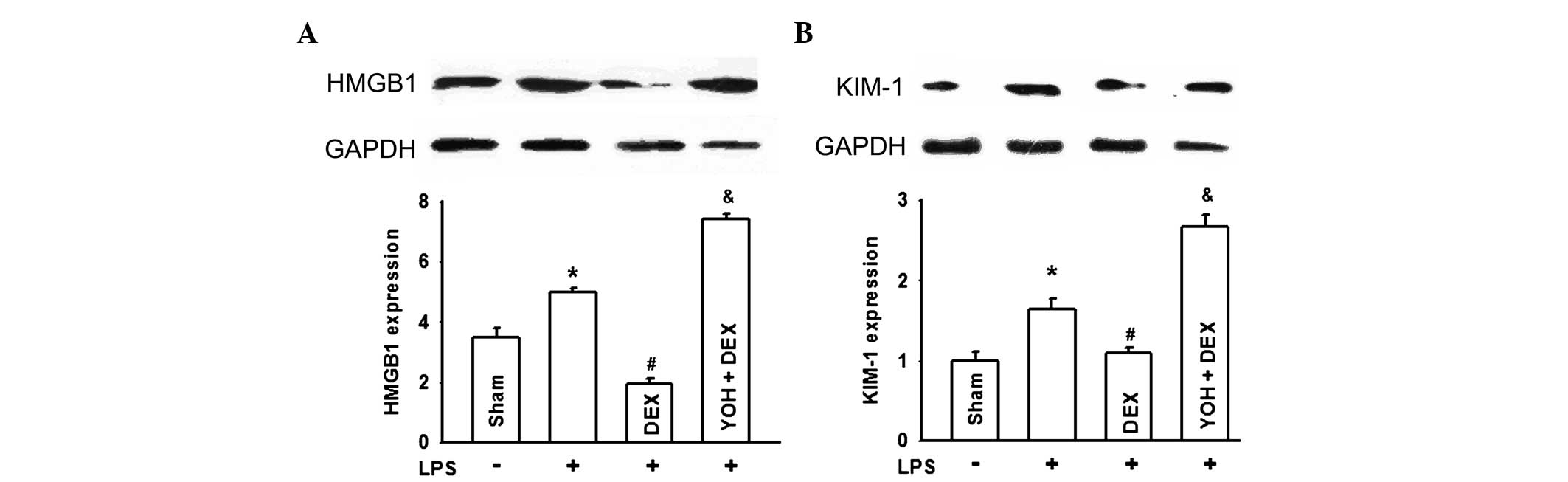
DEX downregulates KIM-1 and HMGB-1
expression of kidneys in LPS-induced AKI and YOH reverses this type
of effect of DEX
To more specifically establish the protective role
of DEX in LPS-induced AKI, KIM-1 and HMGB-1 expression, as two
types of more specific and sensitive biomarker for the diagnosis of
early damage of kidneys, were determined in Fig. 3. When rats were pretreated with LPS,
KIM-1 and HMGB-1 expression evidently increased indicating that
kidney damage was significant. DEX application ameliorated KIM-1
and HMGB-1 expression increasing in kidneys of LPS-exposure rats.
Similarly, YOH counteracted the protective effects of DEX.
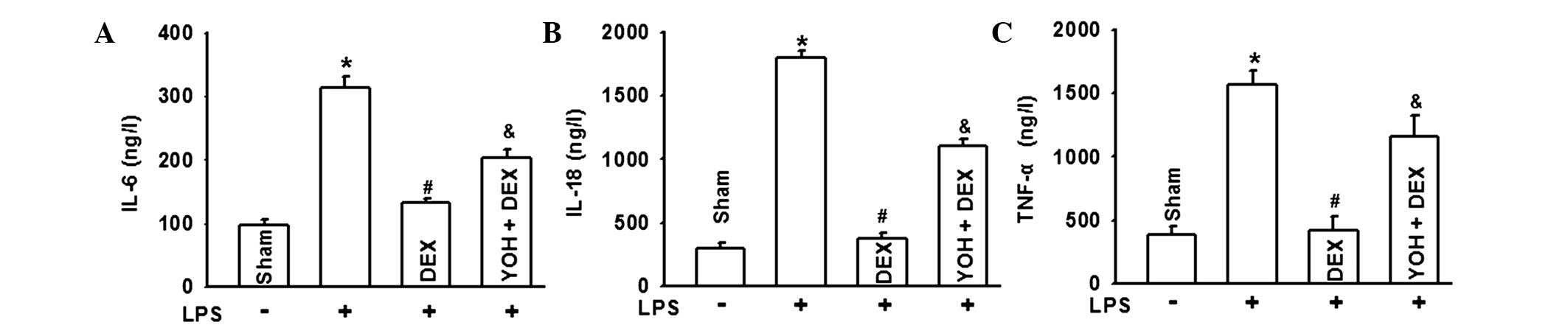
DEX ameliorates the inflammatory
reaction of kidneys in LPS-induced AKI and YOH reverses the
protection effects of DEX
To the best of our knowledge, AKI caused by sepsis
was always associated with inflammatory reactions (18,19). Thus,
in order to explore the protective mechanisms of DEX for AKI,
representative inflammatory factors, such as IL-6, IL-18 and TNF-α
were detected. Fig. 4 demonstrates
that IL-6, IL-18 and TNF-α were all significantly increased in the
LPS group and DEX pretreatment downregulated the increase of these
three types of inflammatory factors. Similarly, YOH application
reversed this type of DEX effect. These results suggested that the
protective function of DEX was associated with its
anti-inflammatory effects through activating the α-2
adrenoceptor.
Discussion
Patients with sepsis undergoing AKI is extremely
common in clinical practice, particularly in ICU, which influences
patient survival. Approximately 80% of acute renal failure is
caused by renal tubular injury (20,21). The
pathophysiological process of AKI induced by sepsis is extremely
complex and severely affects patient survival. To the best of our
knowledge, numerous different types of mechanisms were associated
with this complication. Renal ischemia-reperfusion injury,
inflammatory reaction, oxidative stress injury, nitric oxide
release, cell apoptosis, endothelial dysfunction and the direct
injury of endotoxin all participated in this process (19,22–26). However, mechanisms of sepsis-induced
AKI remain unclear and effective therapies are lacking.
Rat sepsis models with LPS injection from tail vein
were used to explore the protective effects of DEX against AKI. The
analysis of the experimental results found that pretreatment with
DEX ameliorated AKI, including renal function, pathological damage
and two types of specific and sensitive biomarkers for the
diagnosis of early kidney damage: KIM-1 and HMGB-1 expression.
However, all the protective effects could be reversed by the
α-2-adrenergic receptor antagonist, YOH. It is suggested that the
protective effect of DEX was associated with its function of
activating α-2 adrenoceptor. Of note, the inflammatory factor
increase in the LPS group could be diminished by YOH application.
All the results indicated that DEX ameliorated AKI through
decreasing α-2-adrenergic receptor-mediated inflammatory reaction.
Thus, DEX application in clinical practice may be a totally new
therapy for this type of serious complication.
In the present study, KIM-1 and HMGB-1 expression,
two types of specific and sensitive biomarkers for the diagnosis of
early kidney damage, were determined. HMGB1 contributed to the
pathogenesis of several chronic inflammatory and autoimmune
diseases, including kidney disease. HMGB1 mediated the inflammatory
response upon binding to mediators of inflammation, such as
Toll-like receptor-2 (TLR-2) or TLR-4 and activated additional
proinflammatory cytokines release, such as TNF-α or IL-6. Another
type of protein is KIM-1, a type 1 transmembrane tubular protein
with an immunoglobulin and mucin domain, which is undetectable in
normal kidneys, but is markedly induced in experimental renal
injury. KIM-1 is associated with T-cell activation and immune
response (27) and is also considered
as a unique marker for diagnosis of early kidney damage with high
sensitivity and specificity (28–31). In the
present study, HMGB1 and KIM-1 expression were coincidental with
renal function and pathological damage. When AKI was significant,
KIM-1 and HMGB-1 expression was also increased; as DEX application
ameliorated AKI, they were also decreased. These two proteins are
good markers for AKI diagnosis, but more noteworthy, changes of
KIM-1 and HMGB-1 expression provided an indication that LPS-induced
AKI was associated with an inflammatory reaction, as these two
types of protein not only mediated the inflammatory response, but
also promoted proinflammatory cytokines release. Thus, the function
of the inflammatory reaction in AKI and whether the protective
effect of DEX was associated with inflammatory reaction depression
were explored. Fig. 4 showed that the
representative inflammatory factors, IL-6, IL-18 and TNF-α,
increased in the LPS-induced AKI group, which could be reversed by
DEX application.
As reported, the inflammatory reaction has always
played an important role in the pathogenesis of AKI (32). Lu et al (33) reported that nine polymorphism genes are
closely associated with AKI, including TNF-α and IL-6 in
particular. A large number of studies illustrated these
inflammatory factors not only lead to AKI, but also promoted it to
become worse. As reported previously, IL-18 is mainly produced from
macrophages, which can effectively predict the mortality of
patients. Urinary IL-18 was significantly increased with 90%
sensitivity and specificity in the diagnosis of AKI; thus, it can
be used as a sensitive index of patients undergoing AKI (34); and more notably, IL-18 induced the
expression of TNF-α and IL-6. This made the inflammatory reaction
more serious and contributed to organ injuries (7). In the present experiment, DEX application
decreased these inflammatory factors and protected against
LPS-induced AKI, which may be a useful therapy for AKI; however,
the protective mechanism of DEX remains unclear.
DEX is a highly selective α-2-adrenergic receptor
antagonist and effectively inhibited sympathetic activity widely.
In recent years, investigators have found that DEX also played an
important role in organ protection from numerous different aspects,
such as anti-inflammation, oxidative stress inhibition or apoptosis
regulation. Villela et al (35)
reported that DEX protected against kidney damage through its
diuretic effect. Other studies clarified that DEX decreased renal
cell apoptosis through activating α-2 adrenoceptor and
downregulating TLR4 expression (36).
DEX also had preventive effects on acute lung injury through
mediating oxidative stress (37). In
the present study, DEX ameliorated LPS-induced AKI through reducing
the levels of inflammatory factors, such as IL-6, IL-18 and TNF-α.
Thus, DEX application was beneficial for kidney protection,
particularly in sepsis.
When the unique α-2-adrenergic receptor antagonist,
YOH, was used, the protective effect of DEX was counteracted and
the inflammatory factors, IL-6, IL-18 and TNF-α, were reversed,
suggesting that DEX protected against AKI through α-2-adrenergic
receptor activation. α-2-adrenergic receptors are widely
distributed in various tissues and organs, including the renal
proximal tubule, collecting duct and microvascular system (38). As reported previously, α-2-adrenergic
receptor activation regulated the function of the sympathetic nerve
and led to the cholinergic anti-inflammatory pathway, which
downregulated different types of inflammatory factors (39,40). Other
studies reported that α-2-adrenergic receptor activation inhibited
Janus kinase/signal transducers and activators of transcription and
TLR-4/nuclear factor-κB/mitogen-activated protein kinases signal
pathways to exert anti-inflammatory effects (41). These conclusions mean that DEX played
an important role in anti-inflammation. Thus, DEX protected against
LPS-induced AKI through α-2-adrenergic receptor activation, which
decreased the inflammatory factors, IL-6, IL-18 and TNF-α.
Acknowledgements
The present study was supported by the Medical
Research Foundation of Guangdong Province (grant nos. A2012565 and
B2014141); and the National Natural Science Foundation of China
(grant no. 81401628).
References
|
1
|
Puri VK: Of mice and MODS, TNF-alpha, and
sepsis. Crit Care Med. 26:11601998. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Oda S, Hirasawa H, Sugai T, Shiga H,
Nakanishi K, Kitamura N, Sadahiro T and Hirano T: Comparison of
Sepsis-related Organ Failure Assessment (SOFA) score and CIS
(cellular injury score) for scoring of severity for patients with
multiple organ dysfunction syndrome (MODS). Intensive Care Med.
26:1786–1793. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Bagshaw SM, George C and Bellomo R: ANZICS
Database Management Committee: Early acute kidney injury and
sepsis: A multicentre evaluation. Crit Care. 12:R472008. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Schrier RW and Wang W: Acute renal failure
and sepsis. N Engl J Med. 351:159–169. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Rajapakse S, Rodrigo C, Rajapakse A,
Kirthinanda D and Wijeratne S: Renal replacement therapy in
sepsis-induced acute renal failure. Saudi J kidney Dis Transpl.
20:553–559. 2009.PubMed/NCBI
|
|
6
|
Nisula S, Yang R, Poukkanen M, et al: The
FINNAKI Study Group: Predictive value of urine interleukin-18 in
the evolution and outcome of acute kidney injury in critically ill
adult patients. Br J Anaesth. Dec 3–2014.(Epub ahead of print).
PubMed/NCBI
|
|
7
|
Yang Y, Zhang ZX, Lian D, Haig A,
Bhattacharjee RN and Jevnikar AM: IL-37 inhibits IL-18 induced
tubular epithelial cell expression of pro-inflammatory cytokines
and renal ischemia reperfusion injury. Kidney Int. 87:396–408.
2015. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Miranda ML, Balarini MM and Bouskela E:
Dexmedetomidine Attenuates the Microcirculatory Derangements Evoked
by Experimental Sepsis. Anesthesiology. Oct 13–2014.(Epub ahead of
print).
|
|
9
|
Geloen A, Chapelier K, Cividjian A,
Dantony E, Rabilloud M, May CN and Quintin L: Clonidine and
dexmedetomidine increase the pressor response to norepinephrine in
experimental sepsis: A pilot study. Crit Care Med. 41:e431–e438.
2013. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Duan X, Li Y, Zhou C, Huang L and Dong Z:
Dexmedetomidine provides neuroprotection: Impact on
ketamine-induced neuroapoptosis in the developing rat brain. Acta
Anaesthesiol Scand. 58:1121–1126. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Turan A, Bashour CA, You J, Kirkova Y,
Kurz A, Sessler DI and Saager L: Dexmedetomidine sedation after
cardiac surgery decreases atrial arrhythmias. J Clin Anesth.
26:634–642. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Wang ZX, Huang CY, Hua YP, Huang WQ, Deng
LH and Liu KX: Dexmedetomidine reduces intestinal and hepatic
injury after hepatectomy with inflow occlusion under general
anaesthesia: A randomized controlled trial. Br J Anaesth.
112:1055–1064. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Si YN, Bao HG, Xu L, Wang XL, Shen Y, Wang
JS and Yang XB: Dexmedetomidine protects against
ischemia/reperfusion injury in rat kidney. Eur Rev Med Pharmacol
Sci. 18:1843–1851. 2014.PubMed/NCBI
|
|
14
|
Bayraktar O, Tekin N, Aydın O, Akyuz F,
Musmul A and Burukoglu D: Effects of S-allyl cysteine on lung and
liver tissue in a rat model of lipopolysaccharide-induced sepsis.
Naunyn Schmiedebergs Arch Pharmacol. Dec 6–2014.(Epub ahead of
print). PubMed/NCBI
|
|
15
|
Restitutti F, Laitinen MR, Raekallio MR,
Vainionpää M, O'Brien RT, Kuusela E and Vainio OM: Effect of MK-467
on organ blood flow parameters detected by contrast-enhanced
ultrasound in dogs treated with dexmedetomidine. Vet Anaesth Analg.
40:e48–e56. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Wang Y, Yu X, Wang F, Wang Y, Wang Y, Li
H, Lv X, Lu D and Wang H: Yohimbine promotes cardiac NE release and
prevents LPS-induced cardiac dysfunction via blockade of
presynaptic α2A-adrenergic receptor. PLoS ONE. 8:e636222013.
View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Hamar P, Song E, Kökény G, Chen A, Ouyang
N and Lieberman J: Small interfering RNA targeting Fas protects
mice against renal ischemia-reperfusion injury. Proc Natl Acad Sci
USA. 101:14883–14888. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Ratliff BB, Rabadi MM, Vasko R, Yasuda K
and Goligorsky MS: Messengers without borders: Mediators of
systemic inflammatory response in AKI. J Am Soc Nephrol.
24:529–536. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Westenfelder C: Programmed
anti-inflammatory macrophages protect against AKI and promote
repair through trophic actions. Kidney Int. 81:939–941. 2012.
View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Singbartl K and Kellum JA: AKI in the ICU:
Definition, epidemiology, risk stratification, and outcomes. Kidney
Int. 81:819–825. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Honore PM, Jacobs R, Joannes Boyau O, et
al: Septic AKI in ICU patients. Diagnosis, pathophysiology and
treatment type, dosing, and timing: A comprehensive review of
recent and future developments. Ann Intensive Care. 1:322011.
View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Venkatachalam MA and Weinberg JM: The
conundrum of protection from AKI by adenosine in rodent clamp
ischemia models. Kidney Int. 84:16–19. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Myrvang H: Acute kidney injury: Obesity is
associated with AKI after surgery via oxidative stress. Nat Rev
Nephrol. 8:4332012. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Choe JY, Park KY and Kim SK: Oxidative
stress by monosodium urate crystals promotes renal cell apoptosis
through mitochondrial caspase dependent pathway in human embryonic
kidney 293 cells: Mechanism for urate-induced nephropathy.
Apoptosis. 20:38–49. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Anjaneyulu M and Chopra K: Effect of
irbesartan on the antioxidant defence system and nitric oxide
release in diabetic rat kidney. Am J Nephrol. 24:488–496. 2004.
View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Yatim KM and Oberbarnscheidt MH: Endotoxin
and AKI: Macrophages Protect after Preconditioning. J Am Soc
Nephrol. Nov 14–2014.(Epub ahead of print). View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Rodríguez-Iturbe B, Johnson RJ and
Herrera-Acosta J: Tubulointerstitial damage and progression of
renal failure. Kidney Int Suppl. 99:S82–S86. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Han WK, Bailly V, Abichandani R, Thadhani
R and Bonventre JV: Kidney Injury Molecule-1 (KIM-1): A novel
biomarker for human renal proximal tubule injury. Kidney Int.
62:237–244. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Vaidya VS, Ramirez V, Ichimura T,
Bobadilla NA and Bonventre JV: Urinary kidney injury molecule-1: A
sensitive quantitative biomarker for early detection of kidney
tubular injury. Am J Physiol Renal Physiol. 290:F517–F529. 2006.
View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Liangos O, Perianayagam MC, Vaidya VS, et
al: Urinary N-acetyl-beta-(D)-glucosaminidase activity and kidney
injury molecule-1 level are associated with adverse outcomes in
acute renal failure. J Am Soc Nephrol. 18:904–912. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Lameire N, Van Biesen W and Vanholder R:
Acute renal failure. Lancet. 365:417–430. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
32
|
Cunningham PN, Wang Y, Guo R, He G and
Quigg RJ: Role of Toll-like receptor 4 in endotoxin-induced acute
renal failure. J Immunol. 172:2629–2635. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
33
|
Lu JCT, Coca SG, Patel UD, Cantley L and
Parikh CR: Translational Research Investigating Biomarkers and
Endpoints for Acute Kidney Injury (TRIBE-AKI) Consortium: Searching
for genes that matter in acute kidney injury: A systematic review.
Clin J Am Soc Nephrol. 4:1020–1031. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
34
|
Hall IE, Yarlagadda SG, Coca SG, Wang Z,
Doshi M, Devarajan P, Han WK, Marcus RJ and Parikh CR: IL-18 and
urinary NGAL predict dialysis and graft recovery after kidney
transplantation. J Am Soc Nephrol. 21:189–197. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
35
|
Villela NR, do Nascimento Júnior P, de
Carvalho LR and Teixeira A: Effects of dexmedetomidine on renal
system and on vasopressin plasma levels. Experimental study in
dogs. Rev Bras Anestesiol. 55:429–440. 2005.PubMed/NCBI
|
|
36
|
Hanci V, Yurdakan G, Yurtlu S, Turan IO
and Sipahi EY: Protective effect of dexmedetomidine in a rat model
of α-naphthylthiourea-induced acute lung injury. J Surg Res.
178:424–430. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
37
|
Cekic B, Geze S, Ozkan G, et al: The
effect of dexmedetomidine on oxidative stress during
pneumoperitoneum. BioMed research international. 2014:7603232014.
View Article : Google Scholar : PubMed/NCBI
|
|
38
|
Gu J, Sun P, Zhao H, Watts HR, Sanders RD,
Terrando N, Xia P, Maze M and Ma D: Dexmedetomidine provides
renoprotection against ischemia-reperfusion injury in mice. Crit
Care. 15:R1532011. View
Article : Google Scholar : PubMed/NCBI
|
|
39
|
Tracey KJ: Physiology and immunology of
the cholinergic antiinflammatory pathway. J Clin Invest.
117:289–296. 2007. View
Article : Google Scholar : PubMed/NCBI
|
|
40
|
Nance DM and Sanders VM: Autonomic
innervation and regulation of the immune system (1987–2007). Brain
Behav Immun. 21:736–745. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
41
|
Si Y, Bao H, Han L, et al: Dexmedetomidine
protects against renal ischemia and reperfusion injury by
inhibiting the JAK/STAT signaling activation. J Transl Med.
11:1412013. View Article : Google Scholar : PubMed/NCBI
|