Introduction
Systemic lupus erythematosus (SLE) is a human
chronic inflammatory disorder encompassing multisystem organs with
a broad spectrum. Overproduction of auto-antibodies in the
formation of immune complexes may lead to hyperactivation of the
immune system. These immune complexes, accumulated in several
tissues and organs, have key roles in certain clinical
manifestations of SLE. The prevalence of SLE in the general
population is 20–150 cases/100,000 people worldwide and it is more
common in women; almost 10-fold higher than men (1). Although genetic and environmental factors
appear to have a significant role in the pathogenesis of SLE, the
etiology of this disease remains to be elucidated. Familial studies
have revealed that 10–12% of SLE patients that have an affected
first-degree relative show a 20 to 50-fold occurrence increment
when compared to the general population. Evidence in monozygotic
and dizygotic twins has indicated that the disease occurs in 24–69%
of the cases in monozygotic twins, but only 2–9% of the cases in
dizygotic twins (2,3).
Osteopontin (OPN) is a chemokine-like glycoprotein,
rich in aspartate and sialic acid residues, which has a key
function in bone biology, and was recently found as prominent in
regulating inflammation and immunity. As OPN is produced upon
activation of cell, this glycoprotein was termed early T-lymphocyte
activation protein-1 (Eta-1), which increases the Th1 response as
well as inhibits the Th2 response (4).
There are at least two OPN isoforms, including secreted OPN (sOPN)
and intracellular OPN (iOPN), which are produced by translation
from alternative initiation sites. The OPN protein is exposed to
various post-translational modifications including glycosylation,
phosphorylation and tyrosine sulfation, which are specific for cell
type. These modifications could depend on physiological and
pathophysiological factors and affect the OPN structure and
function (5).
OPN activates immune cells, such as T cells, natural
killer (NK) cells, macrophages and Kupffer cells (6). There are multiple receptors for OPN, and
amongst them, cluster of differentiation 44 (CD44) is the most
known receptor and mediates the cell chemotaxis and attachment
(7). A number of studies have reported
that serum OPN levels are increased in several autoimmune diseases,
such as multiple sclerosis and SLE (8–10),
therefore, OPN could contribute to the SLE pathogenesis or its
manifestation. The association between OPN polymorphisms and SLE
susceptibility has been studied in different populations; however,
their results have been controversial (11–13).
As there are few studies regarding the effect of the
OPN rs1126616 polymorphism on SLE and its association with
serum OPN levels, the present study was performed to investigate
the association between the OPN rs1126616 polymorphism and
serum level of OPN with SLE susceptibility and its manifestations
in southeast Iran.
Materials and methods
Patients and sample collection
The present study was approved by the Zahedan
University of Medical Sciences Ethics Committee (Zahedan, Iran).
This case-control investigation was conducted on all SLE patients
(163 patients: 13 men and 150 women) who were referred to the
Rheumatology Clinics of Ali-Ebne-Abitaleb Hospital in Zahedan
between 2011 and 2013.
Individuals with malignant tumors, infectious
disease and other rheumatic diseases were excluded from the study.
All SLE patients fulfilled at least four items of SLE according to
the ACR 1997 criteria (American College of Rheumatology) (14).
The control group consisted of 180 gender-, age- and
ethnically matched volunteers (14 men and 166 women) with a
negative antinuclear antibodies test that was randomly selected
from healthy individuals who were referred to the Internal Medicine
Clinic for check-up examinations.
The control group had no systemic disease and family
association with lupus patients. Written informed consent according
to the declaration of Helsinki was provided from all
participants.
Genotyping of the OPN gene rs1126616
polymorphism
Genomic DNA was isolated from whole blood leukocytes
by the salting-out procedure. OPN polymorphisms were
identified by the polymerase chain reaction (PCR)-restriction
fragment length polymorphism technique. Two oligonucleotide
primers: Forward, 5′-TACCCTGATGCTACAGACGAGG-3′ and reverse,
5′-CTGACTATCAATCACATCGGAATG-3′; based on the flanking sequences of
the OPN rs1126616 polymorphism were used to amplify the
corresponding DNA. PCR was carried out in a 25 µl total final
volume containing 25 pmol of each primer, 0.1 mM dNTP, 0.5–1 µg
genomic DNA, 1.5 mM MgCl2, 2.5 µl of 10X PCR buffer and
1.5 unit TaqDNA polymerase (both from Fermentas, Vilnius,
Lithuania). Thermal cycling conditions were as follows: Initial
denaturation at 94°C for 5 min; 35 cycles of denaturation at 94°C
for 40 sec, annealing for 30 sec at 60°C, and extension at 72°C for
45 sec; and final extension at 72°C for 6 min. The 252-base pair
(bp) PCR fragment was digested with the AluI restriction
enzyme. The C allele had one AluI cleavage site and was
digested to 147 and 105 bp fragments, whereas for the T allele, the
105 bp fragment was cleaved to 61 and 44 bp fragments.
Digested products were separated by electrophoresis
on a 3% agarose gel and visualized by ethidium bromide
staining.
OPN measurement
Blood samples were collected after 12 h of fasting.
Following this, samples were centrifuged at 3,000 × g for 10 min
after clotting for 30 min at room temperature and were stored at
−70°C until analysis. Serum OPN levels were measured using human
OPN kit (R&D Systems, Minneapolis, MN, USA) according to the
manufacturer's protocol.
Statistical analysis
Data were analyzed using the statistical software
SPSS version 18 (SPSS, Inc., Chicago, IL, USA). The differences
between the groups were analyzed by independent sample t-test,
χ2 test or Fisher's exact test, as appropriate. For
determining the frequency of the allele, the direct gene counting
method was used. The genotype and allele frequencies were compared
between SLE patients and controls by χ2 test and
Fisher's exact test. The odds ratio (OR) and 95% confidence
intervals (CI) were also estimated. Logistic regression analysis
was used to assess the independent effect of each risk polymorphism
on SLE. P<0.05 was considered to indicate a statistically
significant difference.
Results
Demographic and clinical
characteristics
Demographic and clinical data of the SLE patients
and control group are shown in Table
I. There were no significant differences in age, gender and
ethnicity between SLE and control groups (Table I). Dermomucus manifestations were
identified in 83% of SLE patients (54% with malar rash). Joint
symptoms were improved in 87% of patients and neuropsychiatric
manifestations were observed in 24% of patients. Lupus nephritis
(LN) was developed with raised serum creatinine in 22% of
patients.
 | Table I.Demographic and clinical
characteristics of SLE patients and controls. |
Table I.
Demographic and clinical
characteristics of SLE patients and controls.
| Parameter | SLE patients,
n=163 | Controls, n=180 | P-value |
|---|
| Age, year | 32.6±8.6 | 32.1±11.7 | 0.68 |
| Gender (male/female),
n | 13/150 | 14/166 | 0.55 |
| Ethnicity, n (%) |
|
|
|
|
Persian | 82
(50) | 86 (48) | 0.36 |
|
Balouch | 81
(50) | 94 (52) |
|
| Joint symptoms, n
(%) | 141 (87) | − |
|
| Renal diseases, n
(%) | 36
(22) | − |
|
| Dermomucus disorder,
n (%) | 135 (83) | − |
|
| Neurological
disorder, n (%) | 23
(14) | − |
|
| Hematological
disorder, n (%) | 98
(60) | − |
|
| Oral ulcer, n
(%) | 45
(28) |
|
|
| Antinuclear
antibodies, n (%) | 147 (90) | − |
|
| Anti-dsDNA
antibodies, n (%) | 122 (75) | − |
|
Polymorphism frequency
The frequency of the OPN rs1126616
polymorphism genotypes and alleles between the two groups is
summarized in Table II. The frequency
of the OPN rs1126616 polymorphism genotypes was in
Hardy-Weinberg equilibrium for cases and controls. Although the
frequency of the OPN rs1126616 T allele was higher in SLE
patients compared to the controls (17.2 vs. 12.2%), the difference
was not statistically significant. There were no significant
differences in the CT and TT genotypes between the SLE patients and
control group. However, a higher frequency of the CT genotype was
observed in patients with LN compared to patients without LN and
healthy controls (Table III),
therefore this genotype may increase the LN risk (OR, 3.1; 95% CI,
1.4–6.9; P=0.004 and OR, 3.5; 95% CI, 1.6–7.4; P=0.001,
respectively). The frequency of the TT genotype was significantly
higher in patients with LN compared to the controls (OR, 8.1; 95%
CI, 1.1–62.5). There was no association between the OPN
rs1126616 polymorphism and other SLE manifestations.
| Table II.Genotypes and alleles frequency of
OPN rs1126616 polymorphism in SLE patients and controls. |
Table II.
Genotypes and alleles frequency of
OPN rs1126616 polymorphism in SLE patients and controls.
| OPN
rs1126616 | SLE patients,
n=163 | Controls,
n=180 | P-value | OR (95% CI) |
|---|
| Genotypes, n
(%) |
|
|
|
|
| CC | 112 (69) | 138 (77) |
| 1.0 |
| CT | 46 (28) | 40 (22) | 0.17 | 1.4 (0.9–2.3) |
| TT | 5 (3) | 2 (1) | 0.18 | 1.8 (0.8–4.0) |
| CT +
TT | 51(31) | 42 (23) | 0.10 | 1.5 (0.9–2.4) |
| Alleles, n (%) |
|
|
|
|
| C | 270 (82.8) | 316 (87.8) |
| 1.0 |
| T | 56 (17.2) | 44 (12.2) | 0.07 | 1.5 (1–2.3) |
| Table III.Genotypes frequency of OPN
rs1126616 polymorphism in SLE patients with and without LN. |
Table III.
Genotypes frequency of OPN
rs1126616 polymorphism in SLE patients with and without LN.
| OPN
rs1126616 | SLE patients with
LN n=36 | SLE patients
without LN n=127 | Controls n=180 |
P-valuea | OR (95%
CI)a |
P-valueb | OR (95%
CI)b |
|---|
| Genotypes, n
(%) |
|
|
|
|
|
|
| CC | 17 (47) | 94 (74) | 138 (77) |
| 1 |
| 1 |
| CT | 17 (47) | 30 (24) | 40 (22) | 0.004 | 3.1 (1.4–6.9) | 0.001 | 3.5 (1.6–7.4) |
| TT | 2 (6) | 3 (2) | 2 (1) | 0.170 | 3.7 (0.6–23.7) | 0.043 | 8.1 (1.1–62.5) |
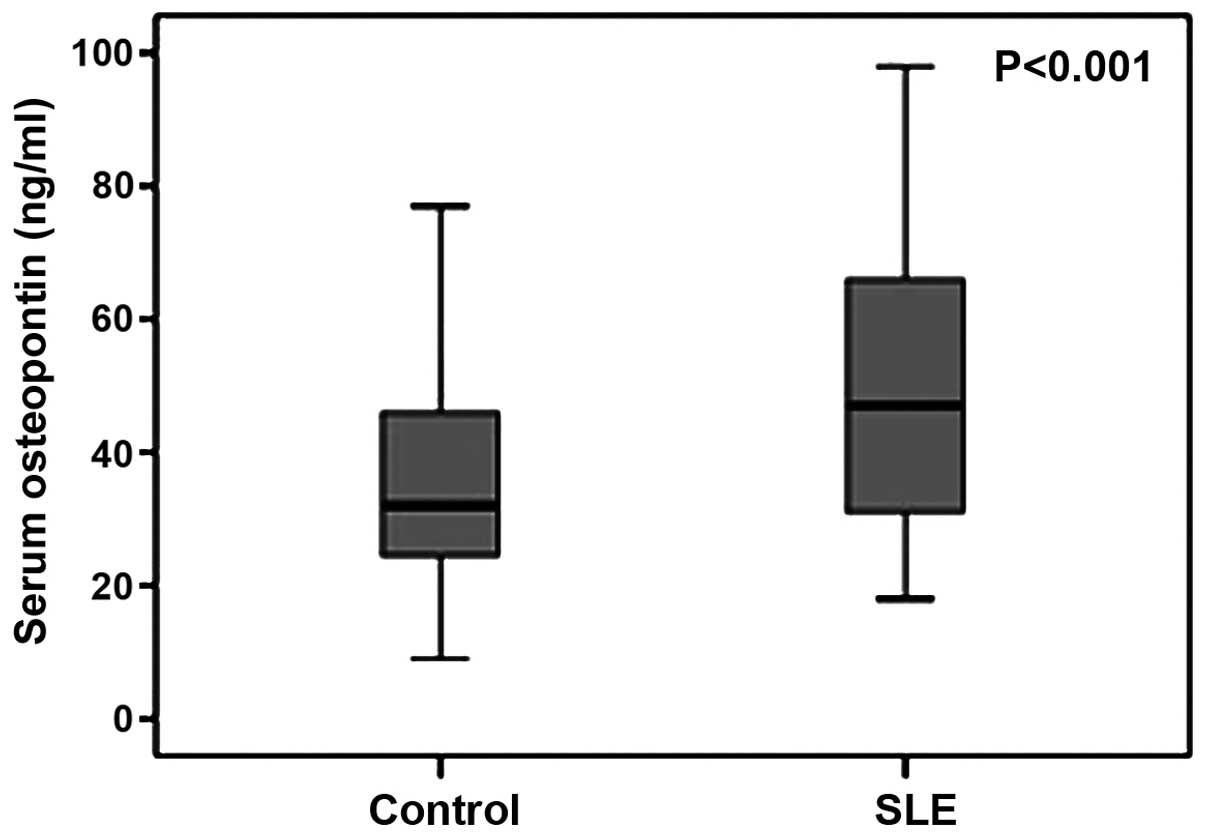
Serum OPN levels
The serum OPN levels were 50.6±22 ng/ml in SLE
patients (n=46) and 35.6±15.8 ng/ml in the control group (n=43),
which indicated a significant elevation in SLE patients
(P<0.001) (Fig. 1).
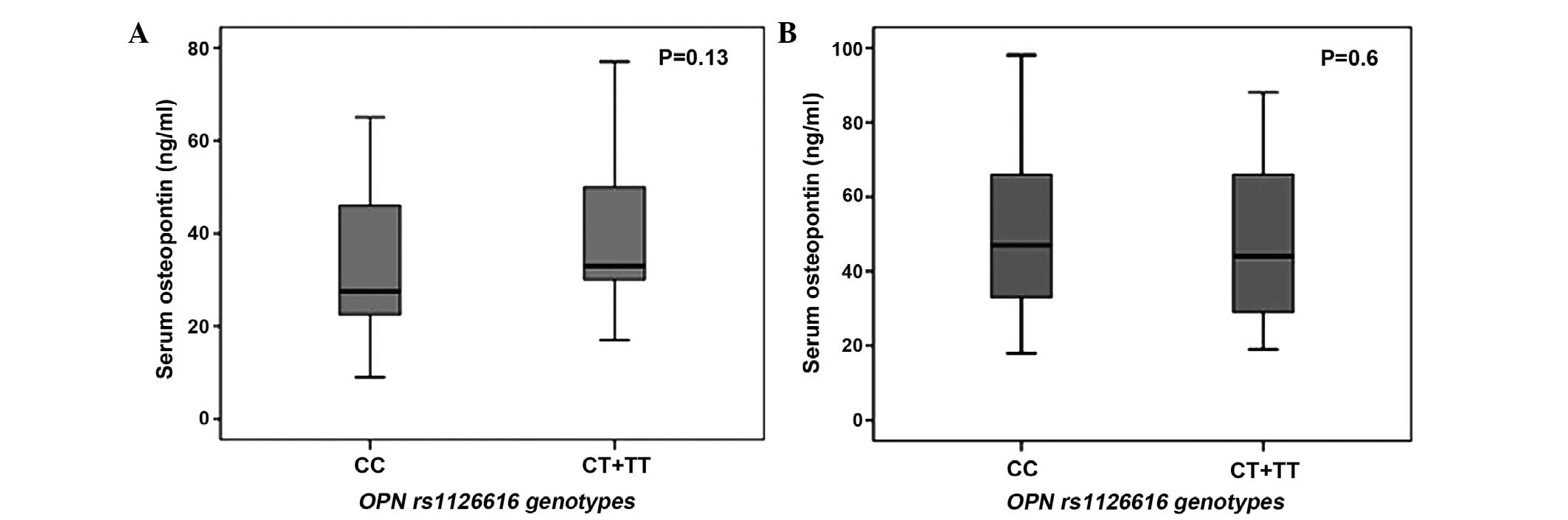
The serum OPN levels were 48.7±21.5 ng/ml in
individuals with the T allele (CT+TT genotypes) and 52.2±22.7 ng/ml
in those without the T allele (CC genotype) in SLE patients, which
were not statistically different (P=0.13) (Fig. 2A). In addition, the serum OPN levels
were not different between individuals with the T allele (39.7±16.1
ng/ml) and individuals without the T allele (32.4±15 ng/ml) in the
control group (P=0.6) (Fig. 2B).
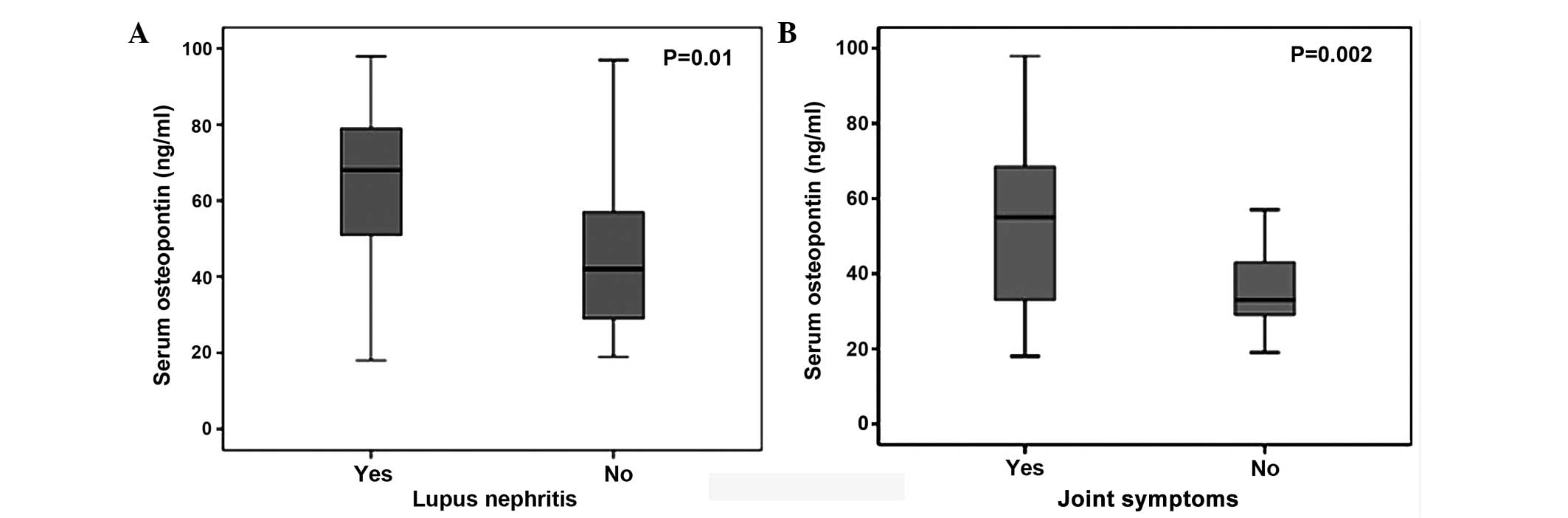
Higher serum OPN levels were observed in SLE
patients with LN compared to SLE patients without this
manifestation (63.9±19.7 vs. 45.3±20.9 mg/ml, respectively, P=0.01)
(Fig. 3A). The serum OPN levels were
significantly higher in SLE patients with joint symptoms compared
to those without joint symptoms (54.4±22 vs. 36.6±12 mg/ml,
respectively, P=0.002) (Fig. 3B).
Discussion
In the present study no association between the
allelic frequency of the OPN rs1126616 polymorphism and SLE
susceptibility was observed. Although the frequency of CT and TT
genotypes was higher in SLE patients, the differences were not
significant. However the frequency of the OPN rs1126616CT
genotype was significantly higher in patients with LN compared to
patients without LN and controls. Furthermore, the frequency of
OPN rs1126616TT was higher in the LN group compared to the
control. There was no correlation between the rs1126616
polymorphism and other SLE manifestations. Additionally, an
elevated serum OPN level was identified only in SLE patients. A
higher serum OPN concentration was observed in SLE patients with LN
and joint symptoms compared to SLE patients without these
manifestations.
OPN as a secretory ECM protein, is involved in
different physiological as well as pathophysiological processes,
such as cell attachment, migration, proliferation, bone formation,
cytokine expression, acute and chronic inflammation, leukocyte
recruitment and immunological activity regulation (15–18). OPN can
exert pro-inflammatory and anti-inflammatory functions, and its
mere effect depends on the nature of scenario (4). OPN has a role in the production of type I
interferon (IFN) and can be involved in autoimmune disease
pathogenesis (19). Several studies
have shown the association between OPN and SLE pathogenesis, as
well as other autoimmune diseases (8,9).
A higher OPN expression has been observed in
macrophages and CD4−/CD8− T cells in MRL/lpr
lupus murine, which stimulates polyclonal antibodies expression
(20). In addition, Li et al
(21) reported that OPN and OPN
mRNA expression was elevated in peripheral blood mononuclear cells
of SLE patients.
In an experimental study performed by Iizuka
(22), it was shown that OPN may have
an important role in proliferation and differentiation of B1 cells
and autoantibody production.
Wong et al (10)
revealed that the plasma OPN level was significantly higher in SLE
patients and the increased OPN level correlated with the SLE
disease activity index score in all SLE patients. Additionally,
elevated plasma OPN concentrations were identified in SLE patients
with renal impairment compared to controls and they suggested that
OPN production was correlated with the inflammatory process.
A recent study by Briggs (9) confirmed the correlation between raised
baseline plasma OPN and IFN levels. Furthermore, the study reported
the elevated level of OPN prior to the onset of increased
cumulative disease and end-organ damage. These associations were
particularly observed in pediatric SLE, which signified that OPN
may be a useful biomarker of disease activity in childhood
lupus.
Although the OPN gene has not been introduced
as a SLE susceptibility gene, various polymorphisms of the
OPN gene have been associated with elevated IFN-α induction
in young patients with SLE and specific clinical phenotypes
(23,24).
Therefore, several studies have been performed to
assess the correlation between the OPN gene polymorphisms
and predisposition to SLE and its manifestations. In 2002, Forton
et al (12) showed the
association between the C707T polymorphism of the OPN gene
with SLE susceptibility. In addition, the study suggested the
association between this polymorphism with renal disease and
opportunistic infections. D'Alfonso et al (11) scanned the coding 5′ and 3′ flanking
regions of the OPN gene in SLE patients and revealed the
correlation between the −156G allele in the promoter and +1239C
allele in the 3′-untranslated region of the OPN gene and SLE
susceptibility. In addition, an association between lymphadenopathy
and −156 genotypes was observed.
Although Xu et al (13) observed a lower frequency of the TT
genotype and higher frequency of the TC genotype of the OPN
polymorphism in SLE patients compared to controls, no association
between this polymorphism and SLE was observed in the present
study. Similar to the results of the present study, the correlation
between the OPN polymorphism and LN has been reported in the
southern Chinese Han population (25).
Han et al (26)
performed a large cohort study regarding the effect of A7385G,
A1239C and C750T polymorphisms of the OPN gene in SLE
susceptibility in European-American and African-American
populations. The study concluded that the frequency of the 750T and
1239C minor alleles were associated with a higher risk of SLE in
males only. Additionally, a significant association between the
750T-7385A-1239C haplotype with SLE was observed, particularly in
males.
Similarly, Kariuki et al (23) reported the association between the
OPN 1239C allele with higher serum OPN and IFN-α levels in
men. This association in women was restricted to younger subjects.
Trivedi et al (24) showed a
significant association between the 1239C allele and
photosensitivity in SLE patients. Additionally, an association
between the C allele with thrombocytopenia and hemolytic anemia in
patients was identified.
Although the majority of the available SLE patients
in southeast Iran were included in the present study, the study is
limited by the small sample size. In addition, as the number of
males (13 men) that were included in the SLE group was low, the
effect of gene-gender interaction could not be analyzed. Therefore,
further studies using higher sample size is suggested for assessing
the effect of the gene-gender interaction.
In conclusion, there was no association between the
OPN rs1126616 polymorphism and predisposition to SLE. The
OPN rs1126616 polymorphism was correlated with LN.
Additionally, higher serum OPN levels were observed in SLE patients
and SLE patients with LN and joint symptoms.
Acknowledgements
The authors would like to thank the Deputy of
Research at Zahedan University of Medical Sciences for the
financial support of this research.
References
|
1
|
Crispín JC, Liossis SN, Kis-Toth K,
Lieberman LA, Kyttaris VC, Juang YT and Tsokos GC: Pathogenesis of
human systemic lupus erythematosus: Recent advances. Trends Mol
Med. 16:47–57. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Harley JB, Kelly JA and Kaufman KM:
Unraveling the genetics of systemic lupus erythematosus. Springer
Semin Immunopathol. 28:119–130. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Deapen D, Escalante A, Weinrib L, Horwitz
D, Bachman B, Roy-Burman P, Walker A and Mack TM: A revised
estimate of twin concordance in systemic lupus erythematosus.
Arthritis Rheum. 35:311–318. 1992. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Mazzali M, Kipari T, Ophascharoensuk V,
Wesson JA, Johnson R and Hughes J: Osteopontin - a molecule for all
seasons. QJM. 95:3–13. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Christensen B, Kazanecki CC, Petersen TE,
Rittling SR, Denhardt DT and Sorensen ES: Cell type-specific
post-translational modifications of mouse osteopontin are
associated with different adhesive properties. J Biol Chem.
282:19463–19472. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Scatena M, Liaw L and Giachelli CM:
Osteopontin: a multifunctional molecule regulating chronic
inflammation and vascular disease. Arterioscler Thromb Vasc Biol.
27:2302–2309. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Weber GF, Ashkar S, Glimcher MJ and Cantor
H: Receptor-ligand interaction between CD44 and osteopontin
(Eta-1). Science. 271:509–512. 1996. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Murugaiyan G, Mittal A and Weiner HL:
Increased osteopontin expression in dendritic cells amplifies IL-17
production by CD4+ T cells in experimental autoimmune
encephalomyelitis and in multiple sclerosis. J Immunol.
181:7480–7488. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Briggs TA: Osteopontin - a biomarker for
organ damage in paediatric lupus? Arthritis Res Ther. 15:1102013.
View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Wong CK, Lit LC, Tam LS, Li EK and Lam CW:
Elevation of plasma osteopontin concentration is correlated with
disease activity in patients with systemic lupus erythematosus.
Rheumatology (Oxford). 44:602–606. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
D'Alfonso S, Barizzone N, Giordano M,
Chiocchetti A, Magnani C, Castelli L, Indelicato M, Giacopelli F,
Marchini M, Scorza R, et al: Two single-nucleotide polymorphisms in
the 5′ and 3 ends of the osteopontin gene contribute to
susceptibility to systemic lupus erythematosus. Arthritis Rheum.
52:539–547. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Forton AC, Petri MA, Goldman D and
Sullivan KE: An osteopontin (SPP1) polymorphism is associated with
systemic lupus erythematosus. Hum Mutat. 19:4592002. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Xu AP, Bai J, Lü J, Liang YY, Li JG, Lai
DY, Wan X and Huang HH: Osteopontin gene polymorphism in
association with systemic lupus erythematosus in Chinese patients.
Chin Med J (Engl). 120:2124–2128. 2007.PubMed/NCBI
|
|
14
|
Hochberg MC: Updating the American College
of Rheumatology revised criteria for the classification of systemic
lupus erythematosus. Arthritis Rheum. 40:17251997. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Ashkar S, Weber GF, Panoutsakopoulou V,
Sanchirico ME, Jansson M, Zawaideh S, Rittling SR, Denhardt DT,
Glimcher MJ and Cantor H: Eta-1 (osteopontin): An early component
of type-1 (cell-mediated) immunity. Science. 287:860–864. 2000.
View Article : Google Scholar : PubMed/NCBI
|
|
16
|
El-Tanani MK: Role of osteopontin in
cellular signaling and metastatic phenotype. Front Biosci.
13:4276–4284. 2008. View
Article : Google Scholar : PubMed/NCBI
|
|
17
|
Weber GF and Cantor H: The immunology of
Eta-1/osteopontin. Cytokine Growth Factor Rev. 7:241–248. 1996.
View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Weber GF, Zawaideh S, Hikita S, Kumar VA,
Cantor H and Ashkar S: Phosphorylation-dependent interaction of
osteopontin with its receptors regulates macrophage migration and
activation. J Leukoc Biol. 72:752–761. 2002.PubMed/NCBI
|
|
19
|
Shinohara ML, Kim JH, Garcia VA and Cantor
H: Engagement of the type I interferon receptor on dendritic cells
inhibits T helper 17 cell development: Role of intracellular
osteopontin. Immunity. 29:68–78. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Lampe MA, Patarca R, Iregui MV and Cantor
H: Polyclonal B cell activation by the Eta-1 cytokine and the
development of systemic autoimmune disease. J Immunol.
147:2902–2906. 1991.PubMed/NCBI
|
|
21
|
Li L, Yu XQ, Yin PD, Chen YX, Liu YG and
Xu HS: OPN expression of peripheral blood mononuclear cells in
systemic lupus erythematosus (SLE) and its clinical significance.
Chin J Rheumatol Chin. 3:84–86. 1999.(In Chinese).
|
|
22
|
Iizuka J: Relationship between osteopontin
expression and autoimmune disease - analysis of osteopontin
expressed in transgenic mice. Hokkaido Igaku Zasshi. 73:487–495.
1998.(In Japanese). PubMed/NCBI
|
|
23
|
Kariuki SN, Moore JG, Kirou KA, Crow MK,
Utset TO and Niewold TB: Age- and gender-specific modulation of
serum osteopontin and interferon-alpha by osteopontin genotype in
systemic lupus erythematosus. Genes Immun. 10:487–494. 2009.
View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Trivedi T, Franek BS, Green SL, Kariuki
SN, Kumabe M, Mikolaitis RA, Jolly M, Utset TO and Niewold TB:
Osteopontin alleles are associated with clinical characteristics in
systemic lupus erythematosus. J Biomed Biotechnol. 2011:8025812011.
View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Xu AP, Liang YY, Lü J, Li JG and Wang Z:
Association of osteopontin gene polymorphism with lupus nephritis
in Chinese Han population. Nan Fang Yi Ke Da Xue Xue Bao.
27:1348–1351. 2007.(In Chinese). PubMed/NCBI
|
|
26
|
Han S, Guthridge JM, Harley IT, Sestak AL,
Kim-Howard X, Kaufman KM, Namjou B, Deshmukh H, Bruner G, Espinoza
LR, et al: Osteopontin and systemic lupus erythematosus
association: A probable gene-gender interaction. PLoS One.
3:e00017572008. View Article : Google Scholar : PubMed/NCBI
|