Introduction
Protease-activated receptor-1 (PAR-1), the
prototypic member of the PAR family, is activated by thrombin
following cleavage of its extracellular amino terminus domain
(1–7).
PAR-1 and its activating factors, which are expressed on tumor
cells and their stroma, induce coagulation and have a significant
role in promoting tumor progression in several carcinomas such as
breast, pancreas, laryngeal and gastric cancer (1,7).
Gastric cancer constitutes multifactorial etiology
and its genetic and immunological background remains to be
elucidated. Cultured gastric cancer cell lines produce extreme
concentrations of cytokines and growth factors with pleiotropic
biological activities in in vitro trials. Among them, PAR-1
functions as an autocrine and paracrine factor that induces a
number of cellular functions, including tumor growth, angiogenesis,
invasion and metastasis (1–4).
Expression and secretion of the PAR-1 isoform in
gastric cancer cells has been determined by previous studies
(1–4).
Increased PAR-1 expression levels were associated with increased
gastric cancer cell proliferation and metastatic potential
(1–4).
Currently however, the molecular function of PAR-1 and the possible
clinical significance of PAR-1 in gastric cancer patients remain to
be elucidated.
Although all the available data have been provided
from preclinical trials, thus far there is no clinical study to
investigate the clinical value of the PAR-1 isoform in serum or
plasma in patients with gastric cancer. Therefore, the significance
of the circulating PAR-1 levels in gastric cancer patients remains
to be elucidated. Thus, the serum levels of PAR-1 in gastric cancer
patients was investigated, and its association with the prognosis,
various clinical variables and response to chemotherapy was
assessed, so as to confirm whether this biomarker may be useful for
the diagnosis and in the assessment of the prognosis, and for use
in the treatment of gastric cancer.
Materials and methods
Patients and therapy
The present study included 63 consecutive patients
with histologically confirmed gastric cancer who were admitted to
the Institute of Oncology (Istanbul University, Istanbul, Turkey).
All the patients had not received any type of therapy, chemotherapy
or chemoradiation, during the last 6 months. The staging was
according to the American Joint Committee on Cancer and Union for
International Cancer Control staging systems (8). Detailed patient history, physical
examination and blood tests including complete blood count and
biochemistry analyses were performed for each patient. Patients
with Eastern Cooperative Oncology Group performance status ≤2, and
suitable blood test results received chemotherapy included
different combinations of various chemotherapeutic agents, such as
fluorouracil, folinic acid, epirubicine, cisplatin, capecitabine
and docetaxel. Chemotherapy responsiveness was determined by the
revised Response Evaluation Criteria in Solid Tumors criteria
version 1.1 (9).
A total of 30 healthy control subjects were included
in the analysis. Informed consent was provided from all the
patients. The ethics committee of the Institute of Oncology
reviewed and approved the study.
Measurement of serum PAR-1 levels
Blood serum samples of patients were provided on
first admission by venipuncture prior to chemotherapy or follow-up,
and were clotted at room temperature. The sera were collected
following centrifugation and were frozen at −20°C until
analysis.
The human PAR-1 enzyme-linked immunosorbent assay
(ELISA) (Wuhan EIAab Science Co., Ltd., Wuhan, China) used a
double-antibody sandwich ELISA to determine the level of human
PAR-1 in the samples.
Measurement of lactate dehydrogenase
(LDH), carcinoembryonic antigen (CAE) and carbohydrate antigen 19-9
(CA 19-9)
The serum CEA and CA 19-9 levels were determined by
the microparticle enzyme immunoassay (Abbott Diagnostics, Chicago,
IL, USA). Serum LDH activity was determined immediately following
collection by the kinetic method on a Targa-3000 autoanalyzer
(Pointe Scientific Inc., Lincoln Park, MI, USA).
Statistical analysis
Parameters were classified as median values and as
cut-off points. Comparisons between clinical or laboratory
parameters and serum PAR-1 assay levels were performed using
Mann-Whitney U test. Survival estimations of patients were
determined by Kaplan-Meier method and differences of survivals were
performed by the log-rank statistics. P≤0.05 was considered to
indicate a statistically significant difference. The SPSS 16.0
software (SPSS, Inc., Chicago, IL, USA) was used for statistical
analyses.
Results
Patient characteristics
In total, 63 patients with gastric cancer were
enrolled in the study. The demographic and histopathological
features of the patients are shown in Table I. The median age of patients was 62
years (range, 28–82 years).
 | Table I.Characteristics of patients and
disease status. |
Table I.
Characteristics of patients and
disease status.
| Parameter | Patients, n (%) |
|---|
| Total patients | 63 (100) |
| Age, years |
|
| ≥60 | 35 (56) |
|
<60 | 28 (44) |
| Gender |
|
| Male | 25 (40) |
|
Female | 38 (60) |
| Localization of
tumor |
|
|
Cardia | 21 (33) |
|
Antrum | 27 (43) |
|
Undetermined | 15 (24) |
| Histology |
|
|
Adenocarcinoma | 42 (67) |
|
Signet-ring cell | 21 (33) |
| Grade |
|
| I–II | 10 (16) |
| III | 44 (70) |
|
Undetermined | 9 (14) |
| Tumor (T) stage |
|
| 1–3 | 14 (22) |
| 4 | 22 (35) |
|
Unknown | 27 (43) |
| No. of involved lymph
node |
| 0–2 | 12 (19) |
| ≥3 | 13 (21) |
|
Unknown | 38 (60) |
| Disease stage |
|
|
Non-metastatic | 32 (51) |
|
Metastatic | 31 (49) |
| Liver
metastasisa |
|
| Yes | 14 (45) |
| No | 17 (55) |
| Curative
surgeryb |
|
| Yes | 17 (53) |
| No | 9 (28) |
|
Unknown | 6 (19) |
| Hemoglobin level,
g/dl |
|
| Low,
<12 | 35 (56) |
| Normal,
≥12 | 28 (44) |
| WBC count |
|
| Normal,
<10,000 | 52 (83) |
| High,
≥10,000 | 11 (17) |
| Platelet count |
|
| Normal,
<350,000 | 54 (86) |
| High,
>350,000 | 9 (14) |
| LDH level, U/l |
|
| Normal,
<450 | 43 (68) |
| High,
≥450 | 10 (16) |
|
Unknown | 10 (16) |
| ESR, /h |
|
| High,
≥50 | 16 (25) |
| Normal,
<50 | 10 (16) |
|
Unknown | 37 (59) |
| CEA level, ng/ml |
|
| Normal,
<10 | 44 (70) |
| High,
≥10 | 13 (21) |
|
Unknown | 6 (9) |
| CA 19–9 level,
IU/ml |
|
| Normal,
<40 | 32 (51) |
| High,
≥40 | 25 (40) |
|
Unknown | 6 (9) |
| Chemotherapy
responsiveness |
|
|
Responsive | 13 (43) |
|
Non-responsive | 17 (57) |
| Last status |
|
|
Alive | 28 (44) |
|
Succumbed | 35 (56) |
Serum PAR-1 levels
No significant difference was observed in the serum
PAR-1 levels between the gastric cancer patients and healthy
subjects (P=0.5) (Table II). The
demographic, pathological, clinical and biochemistry variables,
including patient age, gender, localization of lesion, histology,
pathological grade, stage of disease, and serum tumor markers
including LDH, CAE and CA 19-9 were not correlated with serum PAR-1
levels (P>0.05) (Table III).
Similarly, no association was identified between the serum PAR-1
level and chemotherapy responsiveness (P=0.43) (Table III).
| Table II.Serum PAR-1 levels in the gastric
cancer patients and controls. |
Table II.
Serum PAR-1 levels in the gastric
cancer patients and controls.
|
| Median PAR-1 (range),
ng/ml |
|
|---|
|
|
|
|
|---|
| Assay | Patients, n=63 | Controls, n=30 | P-value |
|---|
| PAR-1 | 0.06 (0.01–4.05) | 0.08 (0.03–8.67) | 0.5 |
| Table III.Distribution and survival associations
of serum PAR-1 levels on the clinical parameters in gastric cancer
patients. |
Table III.
Distribution and survival associations
of serum PAR-1 levels on the clinical parameters in gastric cancer
patients.
|
| Serum PAR-1 level,
P-value |
|---|
|
|
|
|---|
| Parameters | Distribution | Survival |
|---|
| Age, years | 0.06 | 0.61 |
|
<60/≥60 |
|
| Gender | 0.59 | 0.56 |
|
Male/female |
|
| Localization of
tumor | 0.10 | 0.04 |
|
Cardia/antrum |
|
|
| Histology | 0.27 | 0.22 |
|
Adenocarcinoma/signet
ring |
|
|
| Grade | 0.41 | 0.10 |
|
I–II/III |
|
| Tumor (T) stage | 0.12 | 0.06 |
|
1–3/4 |
|
| No. of involved lymph
node | 0.57 | 0.21 |
|
0–2/≥3 |
|
| Curative surgery | 0.46 | 0.36 |
|
Yes/no |
|
| Metastasis | 0.99 | 0.03 |
|
Yes/no |
|
| Liver metastasis | 0.38 | 0.11 |
|
Yes/no |
|
| Hemoglobin level | 0.23 | 0.34 |
|
Low/normal |
|
| WBC count | 0.06 | 0.30 |
|
High/normal |
|
| Platelet count | 0.68 | 0.51 |
|
High/normal |
|
| ESR | 0.97 | 0.02 |
|
High/normal |
|
| LDH level | 0.70 | 0.11 |
|
High/normal |
|
| CEA level | 0.66 | 0.01 |
|
High/normal |
|
| CA 19–9 level | 0.92 | 0.04 |
|
High/normal |
|
| Chemotherapy
responsiveness | 0.43 | 0.05 |
|
Yes/no |
|
|
| Serum PAR-1
level | – | 0.27 |
| Median,
< or ≥ |
|
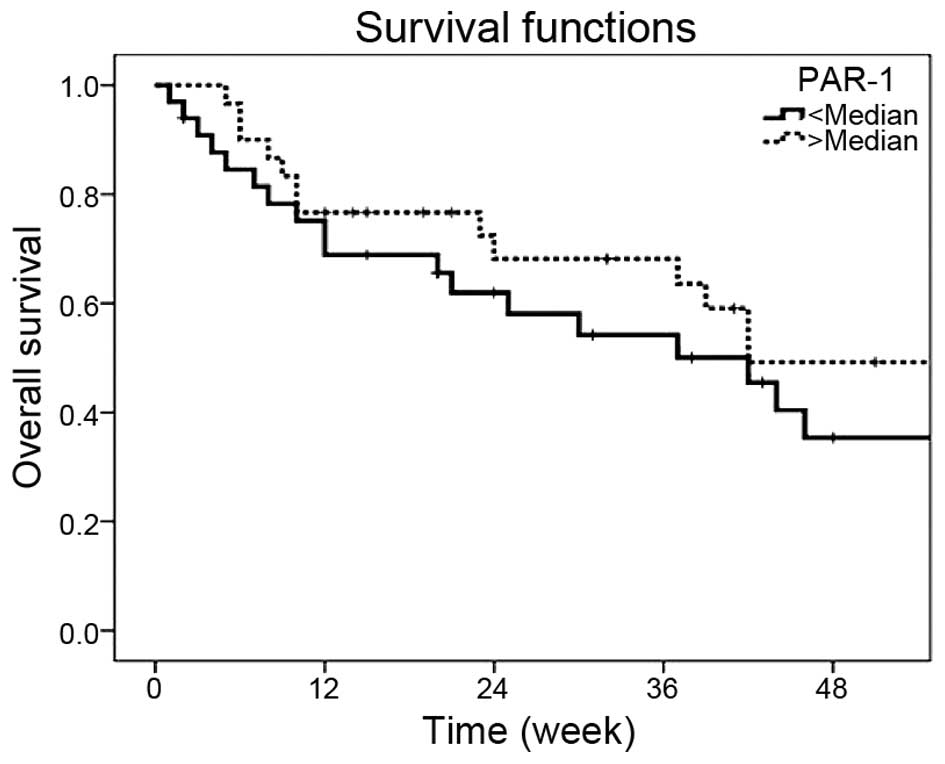
The median survival time for patients was 42.0
weeks. The 1-year survival rate was 42.2%. The presence of distant
metastasis (P=0.03), antrum site (P=0.04), high erythrocyte
sedimentation rate (P=0.02), elevated serum CEA levels (P=0.01),
high serum CA 19-9 levels (P=0.04) and chemotherapy responsiveness
(P=0.05) were significantly poor outcome parameters (Table III). However, serum PAR-1 levels were
not associated with survival (P=0.27) (Table III and Fig.
1).
Discussion
Although overexpression of PAR-1 has been determined
in gastric cancer, its clinical significance has remained ambiguous
in patients with gastric cancer. The possible cause of this
situation is limited data; only a few trials have been performed
thus far (1–4).
Although PAR-1 expression has been correlated with
tumor invasion and metastasis in several types of cancer, the
pioneering study presented the associations between
immunohistochemical (IHC) status of PAR-1 and clinicopathological
factors and outcome in gastric cancer in 2008 (1). An IHC study was performed in 129 samples
of gastric cancer by the anti-PAR monoclonal antibody. Of the 129
gastric cancer specimens, tumor tissues of 58 (45%) observed
positive immunoreactivity for PAR-1. The PAR-1 expression was
highly intensive on the cell membranes. Significant associations
between PAR-1 staining and wall invasion depth (P=0.0028) and
peritoneal dissemination (P=0.041) were found. However, no
correlation was identified between PAR-1 staining and
histopathological stage, histological differentiation, macroscopic
type, lymph node metastasis, liver metastasis or surgical
curability. The patient survival analysis for gastric cancer
overexpressing PAR-1 showed a higher risk of fatality compared with
no overexpression (P<0.0001). Therefore, univariate and
multivariate analysis identified that PAR-1 expression was an
independent prognostic factor. The investigators concluded that the
gastric cancer tissue produces matrix metalloproteinase-1 (MMP-1),
cleaving PAR-1 to generate a new receptor N-terminus in the
autocrine and paracrine manner, and activated PAR-1 causes cell
invasion and metastasis. Another study also showed that the PAR-1
protein level was only significantly correlated with tumor size
(2). In this study, ncRuPAR, a novel
long non-coding RNA molecule that can upregulate PAR-1, inhibited
the development of gastric cancer, and its possible underlying
mechanism involves the PAR-1 inhibition.
To investigate how PAR-1 has a significant role in
gastric cancer cells, a few studies were performed in addition to
the studies aforementioned (3,4). In gastric cancer cells, activation of
PAR-1 can trigger an array of responses, thus, it would support
tumor cell growth and tumor invasion (3). Overexpression of nuclear factor-κB,
epidermal growth factor receptor (EGFR) and tenascin-C are among
the effects of PAR-1 activation, and tenascin-C promotes EGFR
activation by the autocrine route. Furthermore, in another study,
galectin-3, MMP-3 and PAR-1 were highly expressed and co-localized
in cancerous tissues from patients with gastric cancer. Galectin-3
increased cell migration and invasion via PAR-1 upregulation
(4). The investigators of these two
studies concluded that PAR-1 was a potentially significant target
for the gastric cancer therapy.
All these findings regarding PAR-1 were provided by
preclinical trials. Thus far, PAR-1 was not studied in the sera of
gastric cancer patients. The aim of the present study was to
investigate the clinical significance of the serum PAR-1 levels in
gastric cancer patients. The serum levels of PAR-1 were
quantitatively analyzed by ELISA. The results showed that serum
PAR-1 was not able to discriminate between the gastric carcinoma
patients and controls, indicating that PAR-1 was not a good
serological diagnostic marker in gastric cancer. Furthermore, no
significant associations were identified between the levels of
serum PAR-1 and the tumor features such as stage, histology, grade
and serum tumor markers. Similarly, the serum level of PAR-1 was
not associated with outcome. Thus, serum PAR-1 levels could not be
used as a prognostic indicator to predict tumor prognosis. In
addition, no link between serum PAR-1 concentrations and
sensitivity to chemotherapy has raised the possibility of using
PAR-1 as predictors of chemotherapy responsiveness in patients
scheduled to undergo chemotherapy regimens. The serum PAR-1
concentrations may not be a potential predictor of clinical
responsiveness to chemotherapy. Thus, it means that these findings
are inconsistent with the aforementioned data provided from
preclinical trials.
In conclusion, the serum PAR-1 levels have no
diagnostic, predictive and prognostic values in gastric cancer
patients. Although the small sample size and the short follow-up
time are the limitations and may have influenced the results, the
present study contributes significant information to the literature
in that it was carried out with the serum instead of tissue, and it
contained all stages of the disease. Larger scale studies in larger
patient populations are required to determine the exact role of
serum PAR-1 in gastric cancer patients.
References
|
1
|
Fujimoto D, Hirono Y, Goi T, Katayama K
and Yamaguchi A: Prognostic value of protease-activated receptor-1
(PAR-1) and matrix metalloproteinase-1 (MMP-1) in gastric cancer.
Anticancer Res. 28(2A): 847–854. 2008.PubMed/NCBI
|
|
2
|
Liu L, Yan B, Yang Z, Zhang X, Gu Q and
Yue X: ncRuPAR inhibits gastric cancer progression by
down-regulating protease-activated receptor-1. Tumour Biol.
35:7821–7829. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Fujimoto D, Hirono Y, Goi T, Katayama K,
Matsukawa S and Yamaguchi A: The activation of proteinase-activated
receptor-1 (PAR1) mediates gastric cancer cell proliferation and
invasion. BMC Cancer. 10:4432010. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Kim SJ, Shin JY, Lee KD, Bae YK, Choi IJ,
Park SH and Chun KH: Galectin-3 facilitates cell motility in
gastric cancer by up-regulating protease-activated receptor-1
(PAR-1) and matrix metalloproteinase-1 (MMP-1). PLoS One.
6:e251032011. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Henrikson KP, Salazar SL, Fenton JW II and
Pentecost BT: Role of thrombin receptor in breast cancer
invasiveness. Br J Cancer. 79:401–406. 1999. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Rudroff C, Schafberg H, Nowak G, Weinel R,
Scheele J and Kaufmann R: Characterization of functional thrombin
receptors in human pancreatic tumor cells (MIA PACA-2). Pancreas.
16:189–194. 1998. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Kaufmann R, Schafberg H, Rudroff C and
Nowak G: Thrombin receptor activation results in calcium signaling
and protein kinase C-dependent stimulation of DNA synthesis in
HEp-2g laryngeal carcinoma cells. Cancer. 80:2068–2074. 1997.
View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Ahn HS, Lee HJ, Hahn S, Kim WH, Lee KU,
Sano T, Edge SB and Yang HK: Evaluation of the seventh American
Joint Committee on Cancer/International Union Against Cancer
Classification of gastric adenocarcinoma in comparison with the
sixth classification. Cancer. 116:5592–5598. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Eisenhauer EA, Therasse P, Bogaerts J,
Schwartz LH, Sargent D, Ford R, Dancey J, Arbuck S, Gwyther S,
Mooney M, et al: New response evaluation criteria in solid tumours:
Revised RECIST guideline (version 1.1). Eur J Cancer. 45:228–247.
2009. View Article : Google Scholar : PubMed/NCBI
|