Introduction
Moyamoya disease (MMD) is a type of chronic vascular
occlusive disease of unknown etiology that was first identified in
Japan in 1965 (1), though has since
been established to have a global distribution (2). MMD is characterized by ischemia and
hemorrhage. Cases in children are more often characterized by
ischemia, whereas more than half of adult MMD patients exhibit
various types of cerebral hemorrhages (3–5). China and
the surrounding Asian countries are areas of high prevalence of MMD
(6–8).
Although previous studies have investigated MMD in Japan and South
Korea, few clinical epidemiological studies on MMD have been
conducted in China, with even fewer studies on hemorrhagic MMD
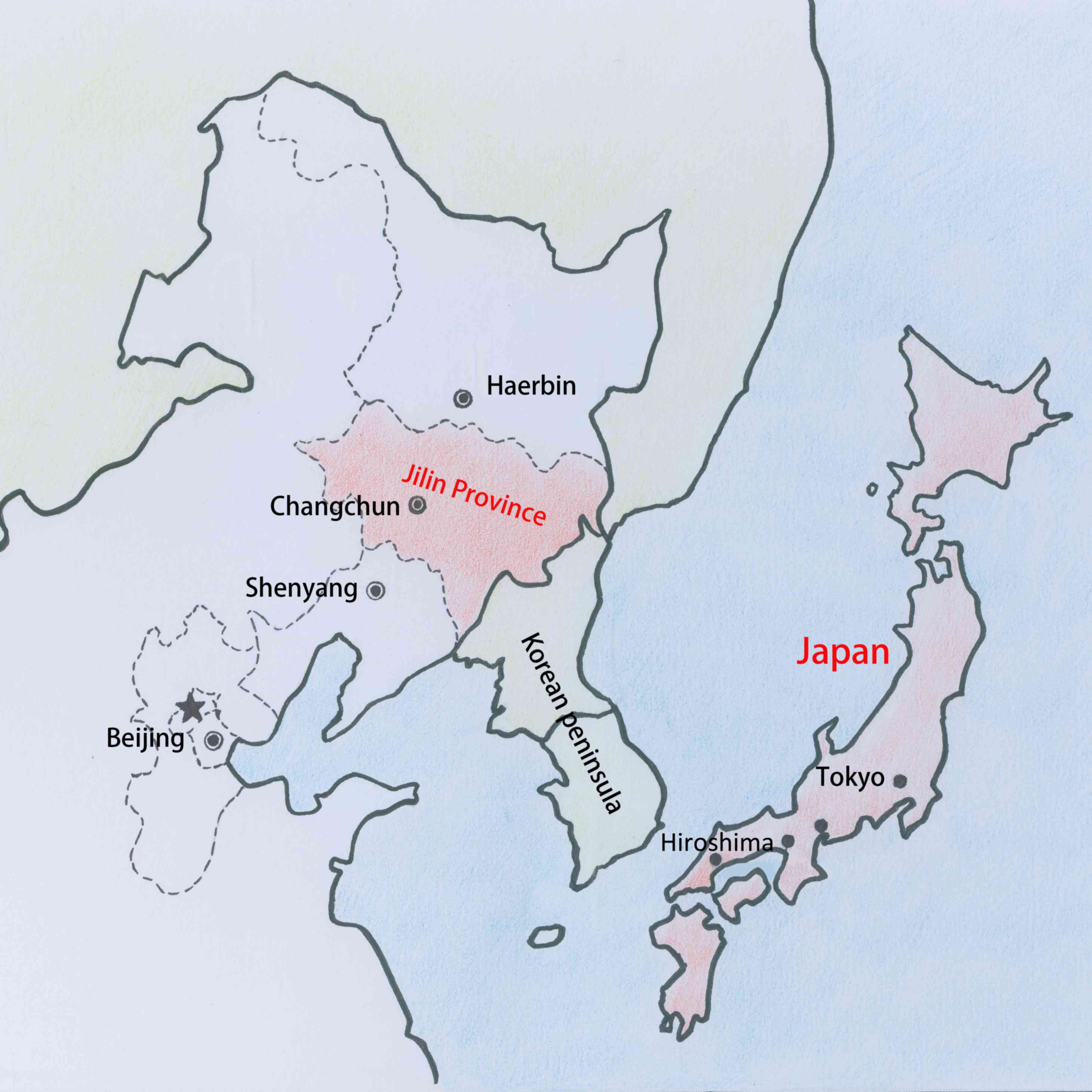
(9–11). Therefore, it is warranted to study
hemorrhagic MMD in Jilin, as a province in northeast China adjacent
to Japan (Fig. 1). The present study
consecutively enrolled hemorrhagic MMD cases from the Neurosurgery
Department at the First Hospital of Jilin University (Changchun,
China). The First Hospital of Jilin University is currently the
largest medical institution in Jilin province, and MMD cases
admitted to the Neurosurgery Department account for approximately
80% of the confirmed MMD cases in Jilin province (12,13);
therefore, the present study may be considered as representative.
Jilin province is located in the middle of northeast China, at
122–131° north and 41–46° east. It has a temperate monsoon climate,
with typical continental characteristics, namely megathermal wet
summers and dry cold winters (14,15).
Hemorrhagic MMD in this area may have certain clinical
characteristics that differ from those in neighboring Japan and
Korea. The present study systemically reviewed the clinical data of
patients with hemorrhagic MMD admitted to the Neurosurgery
Department of the First Hospital of Jilin University between
January 2009 and January 2014. This aimed to summarize the clinical
epidemiological characteristics of hemorrhagic MMD in Jilin
province, to ultimately provide information on key epidemiological
characteristics for future research.
Subjects and methods
Subjects
A total of 212 patients with hemorrhagic MMD were
consecutively enrolled from the Neurosurgery Department of the
First Hospital of Jilin University between January 2011 and January
2015. The inclusion criteria were patients definitively diagnosed
with cerebral hemorrhage using head computed tomography (CT) and
confirmed to have MMD using CT angiography (CTA) and/or digital
subtraction angiography (DSA). Patients with comorbidities and/or a
medical history of other conditions were included. Following
diagnosis, the patients were administered appropriate treatments.
Cases with incomplete information on any relevant data collected
for the study were excluded. The study protocol was approved by the
Ethics Committee of the First Hospital of Jilin University, and
written informed consent was obtained from all patients allowing
the use and publication of their data in the study.
Data collection methods
The MMD cases were screened on the medical records
management system of the First Hospital of Jilin University in
chronological order according to the inclusion criteria, and the
patients' gender, age, history of previous illnesses, onset time,
onset symptoms, hemorrhage type, Hunt-Hess Scale grading (with
minor revision in 2001) (16),
imaging results, treatments and prognostic Glasgow Outcome Scale
(GOS) (17,18) score were recorded.
Statistical methods
SPSS 19.0 (IBM Corp., Armonk, NY, USA) was used for
the statistical analyses. χ2 tests were used for the
enumeration data, with an inspection level of α=0.05, and P<0.05
was considered to indicate statistical significance.
Results
Age and gender characteristics of the
hemorrhagic MMD patients
In total, 212 patients ranging in age from 14 to 84
ears and with an average age of 47.7±11.5 years were included in
the study. There were 101 female patients and 111 male patients,
with a gender ratio of 1:1.1.
History of previous illnesses
Among the 212 patients, 13 (6.1%) had a history of
cerebral ischemia, 32 (15.1%) had a history of cerebral hemorrhage,
50 (23.6%) had a history of hypertension and 7 (3.3%) had a history
of diabetes.
Hemorrhage types and onset
symptoms
The hemorrhage types of the 212 patients were as
follows: Subarachnoid hemorrhage (SAH; 116 cases, 54.7%),
intraventricular hemorrhage (IVH; 25 cases, 11.8%) and
intracerebral hemorrhage (ICH; 71 cases, 33.5%).
The onset symptoms of the 212 patients were as
follows: Headache associated with nausea and vomiting (130 cases,
61.3%), unconsciousness (43 cases, 20.3%), limb paralysis and/or
aphasia (23 cases, 10.8%), transient unconsciousness and subsequent
headache, nausea and vomiting (9 cases, 4.3%), dizziness (6 cases,
2.8%) and oculomotor nerve paralysis (1 case, 0.5%).
Hunt-Hess classification at
admission
Among the 212 patients, Hunt-Huss grade I was
observed in 111 (52.4%), grade II in 23 (10.8%), grade III in 51
(24.1%), grade IV in 24 (11.3%) and grade V in 3 (1.4%).
Imaging characteristics
Among the 212 patients, 122 (57.5%) underwent CTA
only, 50 (23.6%) underwent DSA only, and 40 (18.9%) underwent CTA
and DSA.
Hemisphere involvement
MMD involving a unilateral artery was identified in
110 cases (51.9%) and MMD involving bilateral arteries was
identified in 102 cases (48.1%).
Association with aneurysms
Among the 212 cases, 74 (34.9%) were accompanied by
aneurysms. Among the 74 cases involving aneurysms, 57 (77.0%)
involved anterior circulation aneurysms, which included anterior
communicating aneurysms (27/74, 36.5%), distal anterior artery
aneurysms (2/74, 2.7%), posterior communicating aneurysms (9/74,
12.1%), middle cerebral artery aneurysms (8/74, 10.8%), ophthalmic
aneurysms (5/74, 6.8%), choroid aneurysms (1/74, 1.4%) and
perforator aneurysms of the middle cerebral artery distribution
area (5/74, 6.8%). The remaining 17 cases (17/74, 23.0%) involved
posterior circulation aneurysms, including posterior cerebral
aneurysms (9/74, 12.2%), basilar artery apex aneurysms (6/74,
8.1%), superior cerebellar artery aneurysms (1/74, 1.4%), and
anterior inferior cerebellar artery aneurysms (1/74, 1.4%).
Among the 212 cases, expansion of the anterior
choroid artery (AChA) and/or the posterior communicating artery
(PComA) was observed in 51 cases (24.1%).
Treatments and prognosis
Of the 212 patients, 144 (67.9%) underwent
conservative treatments, while 68 (32.1%) underwent surgical
treatments.
Among the 68 patients who underwent surgical
treatments, aneurysm embolization was performed in 21 cases
(30.9%), aneurysm clipping in 18 cases (26.5%), removal of the
hematoma plus a decompressive craniectomy in 10 cases (14.7%),
lateral ventricle drainage in 9 cases (13.2%), aneurysm clipping
plus roofing of the temporal muscle (encephalo-myo-synangiosis) in
8 cases (11.8%) and simple encephalo-myo-synangiosis in 2 cases
(2.9%).
Among the 212 cases, GOS scores of 5, 4, 3, 2 and 1
were observed in 139 (65.6%), 21 (9.9%), 28 (13.2%), 13 (6.1%) and
11 (5.2%) cases, respectively.
Effect of an association with aneurysm
on hemorrhage type and prognosis
The 212 cases were divided into aneurysm and
non-aneurysm groups according to the presence of an aneurysm. The
results of a χ2 test indicated that there was a statistically
significant difference (P<0.05) between the two groups regarding
the distributions of the hemorrhage types and prognostic GOS
scores.
According to the results of the cross table, in the
aneurysm group, the highest proportion of patients had SAH (86.5%),
followed by ICH (10.8%) and IVH (2.7%). In the non-aneurysm group,
the majority of the patients had ICH (45.6%), followed by SAH
(37.7%) and IVH (16.7%). The χ2 test
(χ2=46.394 and P<0.05) suggested these results were
statistically significant (Table
I).
 | Table I.Effect of combined aneurysm on
hemorrhage type in moyamoya disease. |
Table I.
Effect of combined aneurysm on
hemorrhage type in moyamoya disease.
|
| Hemorrhage
type |
|
|---|
|
|
|
|
|---|
| Variables | SAH | IVH | ICH | Total |
|---|
| Combined with an
aneurysm |
|
|
|
|
| N |
|
|
|
|
|
Count | 52 | 23 | 63 | 138 |
|
Percentage
(%) | 37.7 | 16.7 | 45.6 | 100.0 |
| Y |
|
|
|
|
|
Count | 64 | 2 | 8 | 74 |
|
Percentage
(%) | 86.5 | 2.7 | 10.8 | 100.0 |
| Total |
|
|
|
|
|
Count | 116 | 25 | 71 | 212 |
|
Percentage(%) | 54.7 | 11.8 | 33.5 | 100.0 |
A total of 86.5% of the patients in the aneurysm
group had GOS scores of 5 or 4, which was higher than that in the
non-aneurysm group (69.6%), indicating good prognosis in these
patients. A χ2 test (χ2=14.589 and P<0.05) suggested
that these results were statistically significant (Table II).
| Table II.Effect of the combination of moyamoya
disease and aneurysm on prognostic GOS score. |
Table II.
Effect of the combination of moyamoya
disease and aneurysm on prognostic GOS score.
|
| Prognostic GOS
score |
|
|---|
|
|
|
|
|---|
| Variables | 1 | 2 | 3 | 4 | 5 | Total |
|---|
| Combined with an
aneurysm |
|
|
|
|
|
|
| N |
|
|
|
|
|
|
|
Count | 9 | 10 | 23 | 18 | 78 | 138 |
|
Percentage
(%) | 6.5 | 7.2 | 16.7 | 13.1 | 56.5 | 100.0 |
| Y |
|
|
|
|
|
|
|
Count | 2 | 3 | 5 | 3 | 61 | 74 |
|
Percentage
(%) | 2.7 | 4.0 | 6.8 | 4.1 | 82.4 | 100.0 |
| Total |
|
|
|
|
|
|
|
Count | 11 | 13 | 28 | 21 | 139 | 212 |
|
Percentage (%) | 5.2 | 6.1 | 13.2 | 9.9 | 65.6 | 100.0 |
Effect of the involvement of
unilateral or bilateral arteries on aneurysm site
In total, 74 patients presented with aneurysms and
were further divided into a bilateral involvement or unilateral
involvement group according to the imaging data. A χ2
test comparing the unilateral and bilateral distribution between
the two groups indicated statistically significant differences
(P<0.05).
Among the MMD cases involving bilateral arteries,
63.3% involved anterior circulation aneurysms and 36.7% involved
posterior circulation aneurysms, whereas among the MMD cases
involving unilateral arteries, 86.4% involved anterior circulation
aneurysms and 13.6% involved posterior circulation aneurysms. The
χ2 test (χ2=5.347 and P<0.05) suggested
that these results were statistically significant (Table III). Thus, patients with MMD
involving bilateral arteries were more likely to develop posterior
circulation aneurysms than patients with MMD involving unilateral
arteries; however, the percentage of patients with anterior
circulation aneurysms was markedly high in both groups.
| Table III.Effect of unilateral and bilateral
moyamoya disease on aneurysm site. |
Table III.
Effect of unilateral and bilateral
moyamoya disease on aneurysm site.
|
| Aneurysm |
|
|---|
|
|
|
|
|---|
| Variables | Anterior
circulation | Posterior
circulation | Total |
|---|
| Side |
|
|
|
|
Unilateral |
|
|
|
|
Count | 38 | 6 | 44 |
|
Percentage
(%) | 86.4 | 13.6 | 100.0 |
|
Bilateral |
|
|
|
|
Count | 19 | 11 | 30 |
|
Percentage
(%) | 63.3 | 36.7 | 100.0 |
| Total |
|
|
|
|
Count | 57 | 17 | 74 |
|
Percentage (%) | 77.0 | 23.0 | 100.0 |
Effect of an expansion of the AChA
and/or PComA on hemorrhage type
The 212 cases were further divided into two groups
according to the presence or absence of AChA and/or PComA expansion
based on the imaging data. A χ2 test comparing the hemorrhagic-type
distribution between the groups indicated a statistically
significant difference (P<0.05).
The statistical results demonstrated that 51
patients in the expansion group presented with AChA and/or PComA
expansion, with the incidence rates of ICH, IVH and SAH being 41.2,
35.3 and 23.5%, respectively. In the 161 patients in the
non-expansion group who did not present with AChA and/or PComA
expansion, the incidence rates of SAH, ICH and IVH were 64.6, 31.1%
and 4.3%, respectively. The results of the χ2 test
(χ2=5.347 and P<0.05) suggested a statistically
significant difference in the distribution of hemorrhage types
between the two groups (Table
IV).
| Table IV.Effect of AChA and/or PComA expansion
on hemorrhage type. |
Table IV.
Effect of AChA and/or PComA expansion
on hemorrhage type.
|
| Hemorrhage
type |
|
|---|
|
|
|
|
|---|
| Variables | SAH | IVH | ICH | Total |
|---|
| AChA and/or PComA
expansion |
|
|
|
|
| N |
|
|
|
|
|
Count | 104 | 7 | 50 | 161 |
|
Percentage
(%) | 64.6 | 4.3 | 31.1 | 100.0 |
| Y |
|
|
|
|
|
Count | 12 | 18 | 21 | 51 |
| Percentage (%) | 23.5 | 35.3 | 41.2 | 100.0 |
| Total |
|
|
|
|
|
Count | 116 | 25 | 71 | 212 |
|
Percentage(%) | 54.7 | 11.8 | 33.5 | 100.0 |
Association of hemorrhage history with
prognostic scores
The 212 patients were further divided into two
groups according to hemorrhage history. A total of 32 patients had
a history of hemorrhage. A χ2 test comparing GOS score
distribution between the two groups indicated statistically
significant results (P<0.05).
Among the 212 patients, 32 patients had a history of
hemorrhage, with GOS scores of 5 or 4 accounting for 43.8% of the
patients. In the 180 patients with no history of hemorrhage, cases
with GOS scores of 5 or 4 accounted for 81.1% of the patients. The
χ2 test (χ2=32.195 and P<0.05) suggested
that the prognosis of patients with a history of hemorrhage was
poorer than that of patients without a history of hemorrhage
(Table V).
| Table V.Effect of a history of hemorrhage on
prognostic GOS score. |
Table V.
Effect of a history of hemorrhage on
prognostic GOS score.
|
| Prognostic GOS
score |
|
|---|
|
|
|
|
|---|
| Variables | 1 | 2 | 3 | 4 | 5 | Total |
|---|
| Hemorrhage
history |
|
|
|
|
|
|
| N |
|
|
|
|
|
|
|
Count | 7 | 8 | 19 | 14 | 132 | 180 |
|
Percentage
(%) | 3.9 | 4.4 | 10.6 | 7.8 | 73.3 | 100.0 |
| Y |
|
|
|
|
|
|
|
Count | 4 | 5 | 9 | 7 | 7 | 32 |
|
Percentage (%) | 12.5 | 15.6 | 28.1 | 21.9 | 21.9 | 100.0 |
| Total |
|
|
|
|
|
|
|
Count | 11 | 13 | 28 | 21 | 139 | 212 |
|
Percentage (%) | 5.2 | 6.1 | 13.2 | 9.9 | 65.6 | 100.0 |
Discussion
MMD is a rare cerebrovascular disease of unknown
etiology, characterized by progressive intracranial internal
carotid artery stenosis and occlusion (8). It was first identified in Japan in 1965,
after which Suzuki and Takaku termed the condition moyamoya
disease, as the terminology still used to date (19). Previous results have suggested that
the occurrence and development of MMD are associated with genetic
and immune factors (20). The 212
patients with hemorrhagic MMD enrolled in the current study did not
have an obvious history of familial heredity, which may be due to
the description of illness history and/or lack of knowledge on MMD
among the patients' families. Epidemiological studies have
demonstrated that MMD occurs more frequently in Asian countries
(21–23); the prevalence rate was 3.92/100,000 in
China in 2010 (24), 18.1/100,000 in
Korea in 2013 (25), and estimated to
be as high as 50.7/100,000 in Japan in 2016 (26,27).
Furthermore, the prevalence of MMD tends to be twice as high in
females as in males (28). The gender
ratio of hemorrhagic MMD cases included in the present study was
approximately 1:1, which did not indicate a gender difference. This
finding may be due to the small sample size and/or due to the
inclusion of only hemorrhagic MMD cases. Nevertheless, this result
suggests that male MMD patients may be more prone to hemorrhagic
lesions. Previous studies have reported that the age of onset of
MMD exhibits a bimodal distribution, with the first peak occurring
at 5–10 years of age and the second peak occurring at 40–50 years
of age (29,30). The average age of the patients in the
current study was 47.7±11.5 years, which is consistent with the
timing of the second peak. As few children were enrolled, the first
age peak was not observed; this may be attributed to the fact that
MMD in children is mainly characterized by ischemia, whereas in
adults, hemorrhagic MMD accounts for more than half of all MMD
cases (5).
Previous studies have demonstrated that patients
with MMD combined with aneurysms were more vulnerable to
hemorrhage, and 3–15% of MMD cases were accompanied by an aneurysm
(31,32). However, hemorrhage caused by MMD
includes not only the rupture hemorrhage of the merged aneurysm but
also the rupture hemorrhage of the pseudoaneurysm or small cystic
aneurysm formed by the expanded moyamoya-like vessels or terminal
arteries (33). Aneurysms of the main
trunk primarily cause SAH (34), and
hemorrhage caused by small aneurysms of moyamoya-like vessels or
terminal arteries are prioritized over ICH, mainly of the
periventricular type, and/or IVH (35,36). Among
the 212 patients with hemorrhagic MMD included in the current
study, SAH was the major hemorrhagic type in the MMD patients with
an aneurysm, whereas ICH was the major hemorrhagic type in the
patients without aneurysms, which is consistent with the results of
previous reports (37,38). Previous studies have also identified
that MMD combined with aneurysms may be associated with cerebral
hemodynamic changes, and that aneurysm is often observed in the
anterior communicating artery of unilateral MMD patients (39), but not in the posterior circulation
system of bilateral MMD patients (40). Common non-hemorrhage symptoms of MMD
patients include headaches, mild hemiparesis, sensory abnormalities
or dysarthria, whereas visual symptoms, cognitive symptoms and
epilepsy are rare (26). In the
present study, the patients with hemorrhagic MMD mainly experienced
headaches, altered consciousness, nausea and vomiting, which is
consistent with the symptoms of SAH and ICH (41). The clinical manifestations are
associated with the type, severity and position of the hemorrhage
(42).
The present study also evaluated the relationship
between MMD accompanied by aneurysms and the prognostic GOS scores.
The results suggested that a higher proportion of MMD patients with
aneurysms compared with those without aneurysms had mild disability
(namely GOS scores above 4). This finding indicated that if the
patient survived following rupture of an aneurysm of a major blood
vessel, then aneurysm treatment may improve prognosis. For patients
with hemorrhagic MMD, endovascular interventional treatment may be
used to treat patients with major artery aneurysms (13,43).
Aneurysms can also be clipped directly, though craniotomy clipping
may destroy the collateral circulation of the aneurysm, thus
causing cerebral ischemia (39).
However, for hemorrhage due to rupture of a pseudoaneurysm or small
cystic aneurysm formed by expanded moyamoya-like vessels or
terminal arteries, a craniotomy or interventional treatment has
difficulty in achieving satisfactory results; therefore,
cerebrovascular bypass surgery is often adopted with the parent
artery sacrificed (8,44). Furthermore, indirect bypass treatment
generally requires more than 3 months to develop collateral
circulation (45). In the current
study, vascular interventions or clipping achieved more ideal
clinical effects in MMD patients with aneurysms, whereas for
patients with ICH or IVH, craniotomies or vascular interventions
were not effective, probably due to the cerebral hematoma
destroying the functional areas, which may be a reason for the low
prognostic scores in these patients.
Previous reports also state that hemorrhagic MMD
combined with AChA and/or PComA expansion may be the major cause of
hemorrhage (32,46,47).
Morioka et al (48) examined
107 cases of MMD with AChA and/or PComA expansion (including 70
cases of the ischemic type and 37 cases of the hemorrhagic type) in
2003 and observed that AChA and/or PComA expansion was
significantly associated with hemorrhagic MMD. Although the present
study did not include ischemic MMD patients, among the 212
patients, 24.1% of the hemorrhagic MMD patients exhibited AChA
and/or PComA expansion. In addition, a previous study also reported
that AChA and/or PComA expansion was an independent risk factor for
IVH (49). Similarly, in the current
study, the proportion of ICH was higher in the patients with AChA
and/or PComA expansion compared with the patients without AChA
and/or PComA expansion.
Previous studies have also demonstrated that a
notable proportion of adult patients exhibited minor hemorrhage
with or without symptoms, which significantly predicted the
deterioration of MMD and increased the hemorrhage risk (3,50). In the
current study, the rate of mild disability, namely prognostic GOS
scores of 5 or 4, was markedly lower in the MMD patients with a
history of hemorrhage than in the MMD patients without a history of
hemorrhage, which may be due to the MMD patients with a history of
hemorrhage undergoing repeated progression, and thus demonstrating
rapid progression that resulted in irreversible damage. Therefore,
for patients with confirmed MMD, a positive follow-up should be
conducted even if the patient does not present with serious
clinical symptoms, and intracranial vascular changes should be
closely monitored.
In conclusion, the present analyses of the clinical
characteristics of MMD in Jilin province (northeast China)
indicated that the characteristics of MMD are distinct in this
area. The average age of onset was 47.7±11.5 years, and the gender
ratio was approximately to 1:1. Furthermore, approximately 1/3 of
the hemorrhagic MMD cases were accompanied by aneurysm, and the
most common hemorrhagic type was SAH. The prognosis of the patients
with an aneurysm was more favorable compared with that of the
hemorrhagic MMD patients without an aneurysm. The ratio of ICH and
IVH was also higher in the MMD patients with AChA and/or PComA
expansion, and the prognostic GOS scores were poorer in the
patients with a history of hemorrhage. The patients with bilateral
involvement were also more likely to develop posterior circulation
aneurysms than those with unilateral involvement. In China, the
epidemiological study of MMD is rare, and thus the present findings
may improve understanding of the epidemiology of MMD in this
region.
References
|
1
|
Hemangiomatous malformation of the
bilateral internal carotid arteries at the base of brain. No To
Shinkei. 17:750–756. 1965.(In Japanese).
|
|
2
|
Goto Y and Yonekawa Y: Worldwide
distribution of moyamoya disease. Neurol Med Chir (Tokyo).
32:883–886. 1992. View Article : Google Scholar
|
|
3
|
Jo KI, Kim MS, Yeon JY, Kim JS and Hong
SC: Recurrent Bleeding in Hemorrhagic Moyamoya Disease: Prognostic
Implications of the Perfusion Status. J Korean Neurosurg Soc.
59:117–121. 2016. View Article : Google Scholar
|
|
4
|
Kuroda S and Houkin K: Moyamoya disease:
Current concepts and future perspectives. Lancet Neurol.
7:1056–1066. 2008. View Article : Google Scholar
|
|
5
|
Piao J, Wu W, Yang Z and Yu J: Research
Progress of Moyamoya Disease in Children. Int J Med Sci.
12:566–575. 2015. View Article : Google Scholar
|
|
6
|
Kuriyama S, Kusaka Y, Fujimura M, Wakai K,
Tamakoshi A, Hashimoto S, Tsuji I, Inaba Y and Yoshimoto T:
Prevalence and clinicoepidemiological features of moyamoya disease
in Japan: Findings from a nationwide epidemiological survey.
Stroke. 39:42–47. 2008. View Article : Google Scholar
|
|
7
|
Hung CC, Tu YK, Su CF, Lin LS and Shih CJ:
Epidemiological study of moyamoya disease in Taiwan. Clin Neurol
Neurosurg. 99 Suppl 2:S23–S25. 1997. View Article : Google Scholar
|
|
8
|
Yu J, Shi L, Guo Y, Xu B and Xu K:
Progress on Complications of Direct Bypass for Moyamoya Disease.
Int J Med Sci. 13:578–587. 2016. View Article : Google Scholar
|
|
9
|
Ikezaki K, Han DH, Kawano T, Kinukawa N
and Fukui M: A clinical comparison of definite moyamoya disease
between South Korea and Japan. Stroke. 28:2513–2517. 1997.
View Article : Google Scholar
|
|
10
|
Hayashi K, Horie N, Izumo T and Nagata I:
A nationwide survey on unilateral moyamoya disease in Japan. Clin
Neurol Neurosurg. 124:1–5. 2014. View Article : Google Scholar
|
|
11
|
Ikezaki K, Han DH, Kawano T, Inamura T and
Fukui M: Epidemiological survey of moyamoya disease in Korea. Clin
Neurol Neurosurg. 99 Suppl 2:S6–S10. 1997. View Article : Google Scholar
|
|
12
|
Rao M, Zhang H, Liu Q, Zhang S, Hu L and
Deng F: Clinical and experimental pathology of Moyamoya disease.
Chin Med J (Engl). 116:1845–1849. 2003.
|
|
13
|
Yu JL, Wang HL, Xu K, Li Y and Luo Q:
Endovascular treatment of intracranial aneurysms associated with
moyamoya disease or moyamoya syndrome. Interv Neuroradiol.
16:240–248. 2010. View Article : Google Scholar
|
|
14
|
Li C, Yan Z, Zhang L and Li Y: Research
and implementation of good agricultural practice for traditional
Chinese medicinal materials in Jilin Province, China. J Ginseng
Res. 38:227–232. 2014. View Article : Google Scholar
|
|
15
|
Liu J, Yang J, Guan G, Liu A, Wang B, Luo
J and Yin H: Molecular detection and identification of piroplasms
in sika deer (Cervus nippon) from Jilin Province, China. Parasit
Vectors. 9:1562016. View Article : Google Scholar
|
|
16
|
Stranjalis G and Sakas DE: A minor
revision of Hunt and Hess scale. Stroke. 32:22082001.
|
|
17
|
McMillan T, Wilson L, Ponsford J, Levin H,
Teasdale G and Bond M: The Glasgow Outcome Scale-40 years of
application and refinement. Nat Rev Neurol. 12:477–485. 2016.
View Article : Google Scholar
|
|
18
|
Jennett B, Snoek J, Bond MR and Brooks N:
Disability after severe head injury: Observations on the use of the
Glasgow Outcome Scale. J Neurol Neurosurg Psychiatry. 44:285–293.
1981. View Article : Google Scholar
|
|
19
|
Suzuki J and Takaku A: Cerebrovascular
‘moyamoya’ disease. Disease showing abnormal net-like vessels in
base of brain. Arch Neurol. 20:288–299. 1969. View Article : Google Scholar
|
|
20
|
Achrol AS, Guzman R, Lee M and Steinberg
GK: Pathophysiology and genetic factors in moyamoya disease.
Neurosurg Focus. 26:E42009. View Article : Google Scholar
|
|
21
|
Chen JB, Liu Y, Zhou LX, Sun H, He M and
You C: Prevalence of autoimmune disease in moyamoya disease
patients in Western Chinese population. J Neurol Sci. 351:184–186.
2015. View Article : Google Scholar
|
|
22
|
Ahn IM, Park DH, Hann HJ, Kim KH, Kim HJ
and Ahn HS: Incidence, prevalence, and survival of moyamoya disease
in Korea: A nationwide, population-based study. Stroke.
45:1090–1095. 2014. View Article : Google Scholar
|
|
23
|
Takamatsu Y, Higashimoto K, Maeda T,
Kawashima M, Matsuo M, Abe T, Matsushima T and Soejima H:
Differences in the Genotype Frequency of the RNF213 Variant in
Patients with Familial Moyamoya Disease in Kyushu, Japan. Neurol
Med Chir (Tokyo). 57:607–611. 2017. View Article : Google Scholar
|
|
24
|
Huang S, Guo ZN, Shi M, Yang Y and Rao M:
Etiology and pathogenesis of Moyamoya Disease: An update on disease
prevalence. Int J Stroke. 12:246–253. 2017. View Article : Google Scholar
|
|
25
|
Kim T, Lee H, Bang JS, Kwon OK, Hwang G
and Oh CW: Epidemiology of Moyamoya Disease in Korea: Based on
National Health Insurance Service Data. J Korean Neurosurg Soc.
57:390–395. 2015. View Article : Google Scholar
|
|
26
|
Kim JS: Moyamoya Disease: Epidemiology,
Clinical Features, and Diagnosis. J Stroke. 18:2–11. 2016.
View Article : Google Scholar
|
|
27
|
Hishikawa T, Sugiu K and Date I: Moyamoya
Disease: A Review of Clinical Research. Acta Med Okayama.
70:229–236. 2016.
|
|
28
|
Kleinloog R, Regli L, Rinkel GJ and Klijn
CJ: Regional differences in incidence and patient characteristics
of moyamoya disease: A systematic review. J Neurol Neurosurg
Psychiatry. 83:531–536. 2012. View Article : Google Scholar
|
|
29
|
Hoshino H, Izawa Y and Suzuki N: Research
Committee on Moyamoya Disease: Epidemiological features of moyamoya
disease in Japan. Neurol Med Chir (Tokyo). 52:295–298. 2012.
View Article : Google Scholar
|
|
30
|
Ikezaki K, Fukui M, Inamura T, Kinukawa N,
Wakai K and Ono Y: The current status of the treatment for
hemorrhagic type moyamoya disease based on a 1995 nationwide survey
in Japan. Clin Neurol Neurosurg. 99 Suppl 2:S183–S186. 1997.
View Article : Google Scholar
|
|
31
|
Zhang L, Xu K, Zhang Y, Wang X and Yu J:
Treatment strategies for aneurysms associated with moyamoya
disease. Int J Med Sci. 12:234–242. 2015. View Article : Google Scholar
|
|
32
|
Jang DK, Lee KS, Rha HK, Huh PW, Yang JH,
Park IS, Ahn JG, Sung JH and Han YM: Clinical and angiographic
features and stroke types in adult moyamoya disease. AJNR Am J
Neuroradiol. 35:1124–1131. 2014. View Article : Google Scholar
|
|
33
|
Rhim JK, Cho YD, Jeon JP, Yoo DH, Cho WS,
Kang HS, Kim JE and Han MH: Ruptured Aneurysms of Collateral
Vessels in Adult Onset Moyamoya Disease with Hemorrhagic
Presentation. Clin Neuroradiol. Dec 13–2016.(Epub ahead of print).
View Article : Google Scholar
|
|
34
|
Aoki N and Mizutani H: Does moyamoya
disease cause subarachnoid hemorrhage? Review of 54 cases with
intracranial hemorrhage confirmed by computerized tomography. J
Neurosurg. 60:348–353. 1984. View Article : Google Scholar
|
|
35
|
Matsuoka G, Kubota Y and Okada Y: Delayed
cerebral ischemia associated with reversible cerebral
vasoconstriction in a patient with Moyamoya disease with
intraventricular hemorrhage: Case report. Neuroradiol J.
28:322–324. 2015. View Article : Google Scholar
|
|
36
|
Liu P, Liu AH, Han C, Chen C, Lv XL, Li
DS, Ge HJ, Jin HW, Li YX and Duan L: Difference in Angiographic
Characteristics Between Hemorrhagic And Nonhemorrhagic Hemispheres
Associated with Hemorrhage Risk of Moyamoya Disease in Adults: A
Self-Controlled Study. World Neurosurg. 95:348–356. 2016.
View Article : Google Scholar
|
|
37
|
Funaki T, Takahashi JC, Houkin K, Kuroda
S, Takeuchi S, Fujimura M, Tomata Y and Miyamoto S: on behalf of
the JAM Trial Investigators: Angiographic features of hemorrhagic
moyamoya disease with high recurrence risk: A supplementary
analysis of the Japan Adult Moyamoya Trial. J Neurosurg. 14:1–8.
2017. View Article : Google Scholar
|
|
38
|
Wan M and Duan L: Recent progress in
hemorrhagic moyamoya disease. Br J Neurosurg. 29:189–191. 2015.
View Article : Google Scholar
|
|
39
|
Yu J, Yuan Y, Zhang D and Xu K: Moyamoya
disease associated with arteriovenous malformation and anterior
communicating artery aneurysm: A case report and literature review.
Exp Ther Med. 12:267–271. 2016. View Article : Google Scholar
|
|
40
|
Chen Y, Dai D, Fang Y, Yang P, Huang Q,
Zhao W, Xu Y and Liu J: Endovascular Treatment of Ruptured Large or
Wide-Neck Basilar Tip Aneurysms Associated with Moyamoya Disease
Using the Stent-Assisted Coil Technique. J Stroke Cerebrovasc Dis.
24:2229–2235. 2015. View Article : Google Scholar
|
|
41
|
Wan M, Han C, Xian P, Yang WZ, Li DS and
Duan L: Moyamoya disease presenting with subarachnoid hemorrhage:
Clinical features and neuroimaging of a case series. Br J
Neurosurg. 29:804–810. 2015. View Article : Google Scholar
|
|
42
|
Fujimura M, Mugikura S, Shimizu H and
Tominaga T: Asymptomatic moyamoya disease subsequently manifesting
as transient ischemic attack, intracerebral hemorrhage, and
subarachnoid hemorrhage in a short period: Case report. Neurol Med
Chir (Tokyo). 50:316–319. 2010. View Article : Google Scholar
|
|
43
|
Wada K, Hattori K, Araki Y, Noda T, Maki
H, Oyama H, Kito A and Wakabayashi T: A case of moyamoya disease
with a subarachnoid hemorrhage treated with endovascular technique.
No Shinkei Geka. 42:1027–1033. 2014.(In Japanese).
|
|
44
|
Zhao WG, Luo Q, Jia JB and Yu JL: Cerebral
hyperperfusion syndrome after revascularization surgery in patients
with moyamoya disease. Br J Neurosurg. 27:321–325. 2013. View Article : Google Scholar
|
|
45
|
Wang L, Qian C, Yu X, Fu X, Chen T, Gu C,
Chen J and Chen G: Indirect Bypass Surgery May Be More Beneficial
for Symptomatic Patients with Moyamoya Disease at Early Suzuki
Stage. World Neurosurg. 95:304–308. 2016. View Article : Google Scholar
|
|
46
|
Qi L and Jinlu Y: Moyamoya disease with
posterior communicating artery aneurysm: A case report. Turk
Neurosurg. 23:546–550. 2013.
|
|
47
|
Yang S, Yu JL, Wang HL, Wang B and Luo Q:
Endovascular embolization of distal anterior choroidal artery
aneurysms associated with moyamoya disease. A report of two cases
and a literature review. Interv Neuroradiol. 16:433–441. 2010.
View Article : Google Scholar
|
|
48
|
Morioka M, Hamada J, Kawano T, Todaka T,
Yano S, Kai Y and Ushio Y: Angiographic dilatation and branch
extension of the anterior choroidal and posterior communicating
arteries are predictors of hemorrhage in adult moyamoya patients.
Stroke. 34:90–95. 2003. View Article : Google Scholar
|
|
49
|
Nah HW, Kwon SU, Kang DW, Ahn JS, Kwun BD
and Kim JS: Moyamoya disease-related versus primary intracerebral
hemorrhage: [corrected] location and outcomes are different.
Stroke. 43:1947–1950. 2012. View Article : Google Scholar
|
|
50
|
Yu J, Yuan Y, Li W and Xu K: Moyamoya
disease manifested as multiple simultaneous intracerebral
hemorrhages: A case report and literature review. Exp Ther Med.
12:1440–1444. 2016. View Article : Google Scholar
|