Introduction
Many cytotoxic drugs currently used in cancer
treatment are also myelosuppressive due to their toxicity against
rapidly dividing cells of the hematopoietic system. Thus, some of
the most common side effects/complications of chemotherapy include
injury to the hematopoietic system, mainly neutropenia or
agranulocytosis. The occurrence of neutropenia, especially
clinically significant neutropenia [absolute neutrophil count (ANC)
<1×103/µl], is highly unfavorable and dangerous for
the patient. Clinically significant neutropenia usually requires
delay in the administration of the next cycle of systemic treatment
and thereby reduces the dose density. This may have a negative
impact on its effectiveness and worsen patient prognosis. Moreover,
severe or prolonged neutropenia (ANC <0.5×103/µl,
>7 days) is associated with high risk of infectious
complications, which require hospitalization and aggressive
treatment and may cause high mortality (1,2). Clinically
significant neutropenia may also be accompanied by fever in the
form of febrile neutropenia (FN). According to the European Society
of Medical Oncology (ESMO), FN is defined as a decrease in ANC of
<0.5×103/µl or <1×103/µl, with an
expected decrease in ANC to <0.5×103/µl within 48 h,
accompanied by fever (>38.5°C) and/or clinical manifestations of
sepsis (3–5). Therefore, preventing the incidence of
neutropenia and FN during cytotoxic therapy within primary or
secondary prevention is highly desirable.
Recombinant hematopoietic growth factors, most
commonly granulocyte colony stimulating factor (G-CSF), were
developed and implemented into daily clinical practice for the
primary and secondary prophylaxis of neutropenia and FN. Filgrastim
is one of the most widely used G-CSF currently available. It is a
glycoprotein that stimulates the production and release of
neutrophils from the bone marrow, resulting in a significant
increase in this fraction of leukocytes in the peripheral blood
within 24 h from drug intake, as well as a slight increase in
monocytes (2–4). The use of filgrastim in patients
undergoing cancer chemotherapy has been shown to reduce the
incidence, severity and duration of neutropenia and FN (3,4).
Recommendations for clinical use of hematopoietic growth factors
such as filgrastim are regulated by appropriate guidelines,
including these of the ESMO and the European Organisation for
Research and Treatment of Cancer (1,3,5,6). In clinical
practice, different preparations of filgrastim are used, including
biosimilar drugs (also termed ‘biosimilars’ or ‘follow-on
biologicals’). As the name suggests, these products are
biologically similar to their original drug counterparts, with
similar physicochemical properties, and therefore, should possess
similar efficacy and safety (7–9).
The aim of the present study was to determine the
characteristics of use of the biosimilar (follow-on) drug
filgrastim in the primary and secondary prevention of FN, as well
as to evaluate its efficacy and safety.
Materials and methods
Study design
This was a multicenter, non-interventional,
real-life, epidemiological study sponsored by Accord Healthcare
Polska (Warsaw, Poland), which involved an electronic
questionnaire. The questionnaires were completed by participating
physicians (clinical oncologists) based on the analysis of
patients' medical history, including laboratory tests, a targeted
interview and physical examination during routine visits.
Patient characteristics
The present study ultimately included 170 cancer
patients, aged 23–82 (mean 59.5 years). Demographic characteristics
of included patients are presented in Table I.
 | Table I.Demographic characteristics. |
Table I.
Demographic characteristics.
| Sex (%) |
|
| Male | 32.9 |
|
Female | 67.1 |
| Age, years
(min-max) |
|
|
Median | 62 (23–82) |
| Body weight, kg
(min-max) |
|
|
Median | 68 (41–116) |
| Body surface area,
m2 (min-max) |
|
|
Median | 1.7 (1.4–2.4) |
| Clinical stage
(%) |
|
| II | 10.6 |
| III | 35.3 |
| IV | 54.1 |
| ECOG performance
score (%) |
|
| 0 | 14.1 |
| 1 | 63.5 |
| 2 | 20 |
| 3 | 0.6 |
| 4 | 1.8 |
| Cancer type, n
(%) |
|
| Breast
cancers in women | 46 (27.1) |
|
Gynecological cancers | 31 (18.2) |
| Malignant
colorectal cancers | 24 (14.1) |
| Malignant
pleural and lung cancers | 23 (13.5) |
| Blood and
lymphatic tissue | 16 (9.4) |
|
Pancreatic cancers | 9 (5.3) |
| Malignant
neoplasms of male genital organs | 8 (4.7) |
| Malignant
gastric cancers | 5 (2.9) |
| Other,
<5 units (%) | 8 (4.7) |
Scheme of monitoring
At the first visit (visit 1), basic data (age, sex,
weight and body surface area, the diagnosis of the underlying
disease, disease stage and the Eastern Cooperative Oncology Group
performance status) were recorded for each patient. A targeted
medical interview and physical examination were also undertaken.
Assessment of FN risk relating to the chosen (planned) systemic
treatment protocol and the possibility of additional FN risk
factors for the patient was performed. Additionally, the number of
cycles of planned chemotherapy, the type of FN prevention (primary
or secondary) and additional factors affecting the overall risk of
FN were recorded. Finally, the overall risk of FN was evaluated. At
subsequent visits (visits 2–5), the course of the G-CSF (Accofil®,
Accord Healthcare Ltd., North Harrow, UK) therapy was monitored,
including the assessment of chemotherapy dose density, the
occurrence or lack of FN following the last cycle of treatment, the
continuation of G-CSF in subsequent cycles, the total G-CSF dose
and whether it was self-injected, the presence of pain, and the
convenience of using the drug according to patients' opinion were
recorded. Hematological parameters of peripheral blood including
total number of leukocytes, ANC, hemoglobin concentration and
platelet count were also monitored.
Phase IV study
The study was a non-interventional post marketing
study (phase IV). Accofil® was administrated in line with approved,
labeled indications. Data were collected retrospectively and
analyzed by statistical methods (standard descriptive statistics
methods, including pie charts, bar charts and box plots). Ethical
committee approval was not obtained, as personal information on
study subjects was not used, processed, transferred and disclosed.
Eligible patients provided informed consent before treatment. The
protocol was compliant with the legal and regulatory requirements
in the country.
Results
Risk of FN
The overall risk of FN, as well as risk of FN
relating to the systemic treatment protocol or other factors, is
presented in Table II. In 60% of
cases, physicians estimated that the overall risk of FN was high
(>20%). The presence of additional factors that contribute to
the risk of FN was found in 74.7% of cases.
| Table II.Summary of patients' risk for FN. |
Table II.
Summary of patients' risk for FN.
| Type of tderapy | % |
| Radical
intention | 45.3 |
|
Palliative | 54.7 |
| FN risk associated
with chemotherapy regimen used |
|
|
<10 | 15.9 |
|
10–20 | 53.5 |
|
>20 | 30.6 |
| Additional risk
factors for FN |
|
| Sex | 42.6 |
| Cancer
stage | 41.1 |
| Age | 27.1 |
| Previous
neutropenia | 14.7 |
|
Comorbidities | 11.6 |
| Previous
FN | 9.3 |
| Earlier
radio- or chemotherapy | 7.8 |
|
Anemia | 7.0 |
|
Cardiovascular diseases | 6.2 |
|
Diabetes | 5.4 |
| Cancer
cachexia | 5.4 |
| Internal
diseases burden | 5.4 |
| Low
levels of Hb | 5.4 |
| Ischemic
myocardium | 3.1 |
| No
antibiotic prophylaxis | 3.1 |
| Cardiac
diseases burden | 3.1 |
| Other (3
or less units) | 17.8 |
| The overall risk of
FN |
|
|
<10 | 4.1 |
|
10–20 | 35.9 |
|
>20 | 60.0 |
Number of chemotherapy cycles
In majority of cases (40.6%), six cycles of
chemotherapy were planned; more than six cycles were planned in
28.2% of cases. Accofil® was used as primary prophylaxis in 60% of
cases and as secondary prophylaxis in the remaining 40% of
patients.
Continuation of therapy with
Accofil®
Actual continuation of therapy with Accofil® was
recorded at each visit (beginning from visit 2). At visit 2, 98.2%
of patients who initiated Accofil® therapy continued, while 96.4%
continued at visit 3, 91.3% continued at visit 4, and 86.3%
continued at visit 5. The most common reason for discontinuation of
therapy was disease progression.
The dose of filgrastim taken was calculated at each
of the five visits. The average (mean ± standard deviation) dose
was 220.9±84.4 million units at visit 1; 222.4±87.2 million units
at visit 2; 223.9±90.3 million units at visit 3; 231.6±95.7 million
units at visit 4; and 224.8±98.8 million units at visit 5. In half
of the patients, the dose was <240 million units for all visits.
Whether chemotherapy was continued at the previously recommended
dose was assessed from visit 2 through the visit 5. Most patients
continued chemotherapy with planned dosage (i.e., 95.3% of patients
continued chemotherapy at the same dose at visit 2, 94.7% at visit
3, 96.2% at visit 4, and 90.4% at visit 5). Whether FN had occurred
following the previous cycle of chemotherapy was also assessed from
visit 2 to visit 5 (92.9% of patients reported no FN at visit 2,
94.1% at visit 3, 91.2% at visit 4, and 92.6% at visit 5).
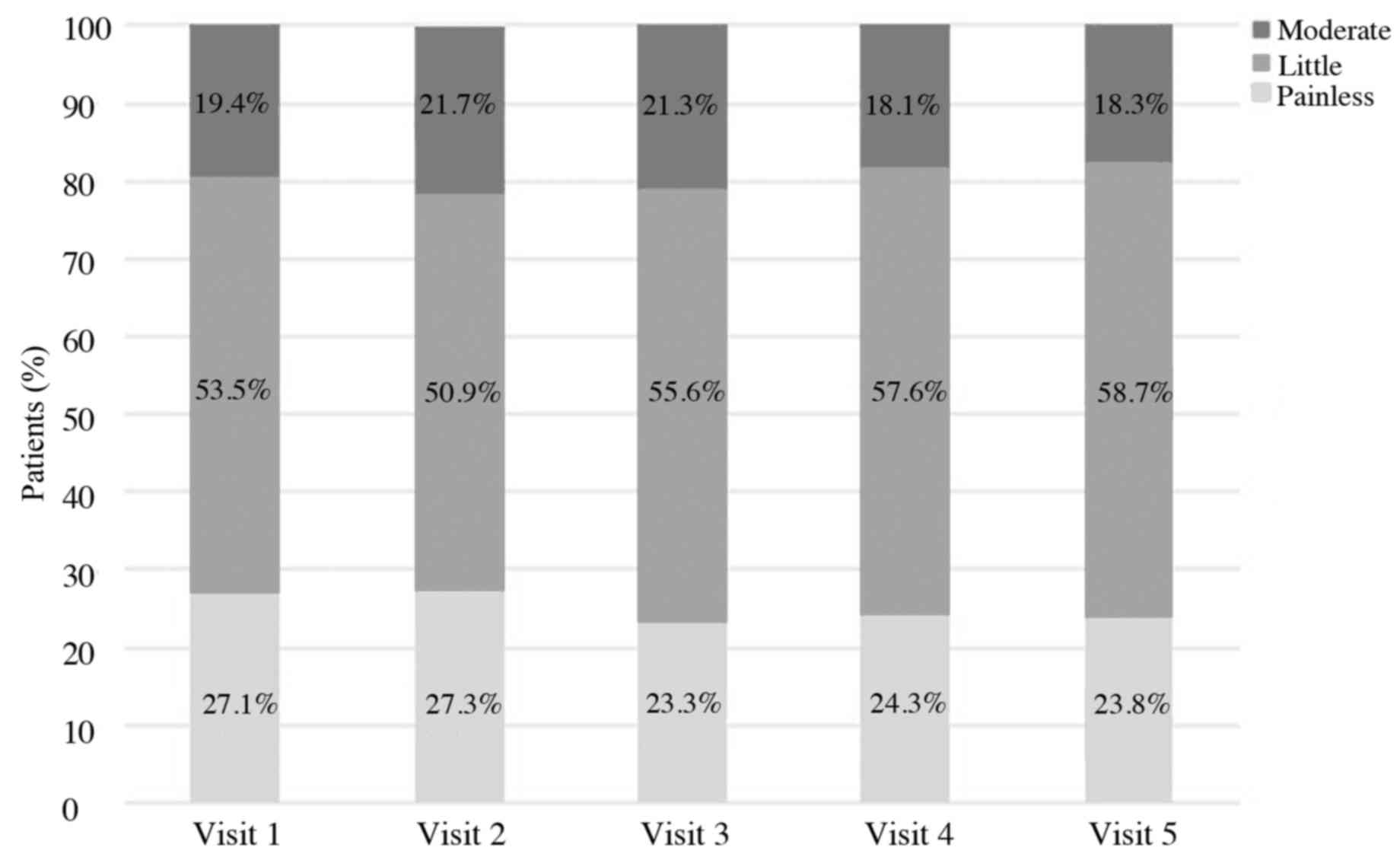
Convenience of injection
Patients' opinions about the convenience of the
therapy were also collected. Patients were asked to assess the
convenience of the use of Accofil® at each visit, using a scale of
1 to 10, where 1 denotes the least convenient use and 10 is the
most convenient. At every visit (1–5), half of the
patients rated the treatment as >8. The average rates were:
7.4±2.1, 7.7±1.8, 7.9±1.8, 7.9±1.7 and 7.8±2.0 (mean ± standard
deviation), at visits 1, 2, 3, 4 and 5, respectively. The injection
soreness was also evaluated. At every visit (1–5), more than
half of the patients responded that the pain of the procedure was
small (Fig. 1).
Hematological parameters
Hematological parameters were also assessed at each
visit, with data collected prior to continuing therapy with G-CSF.
At visit 1, median neutrophil count was 2.2×103/µl and did not fall
below that level at any of the five visits (i.e., median ANC were
2.7×103/µl, 2.5×103/µl, 2.4×103/µl and 2.2×103/µl, at visit 2, 3, 4
and 5, respectively. Other hematological parameters are presented
in Table III.
| Table III.Hematological data at each visit
(V1-V5). |
Table III.
Hematological data at each visit
(V1-V5).
|
| V1 | V2 | V3 | V4 | V5 |
|---|
| Hb level, median
(x103/µl) | 12 | 11.7 | 11.2 | 11 | 10.9 |
| WBC level, median
(x103/µl) | 5.3 | 5.6 | 5.5 | 5.3 | 5 |
| PLT level, median
(x103/µl) | 246 | 232 | 222 | 223 | 211 |
Discussion
Appropriate supportive treatment in systemic therapy
of neoplastic diseases is important for maintaining the density of
the chemotherapeutic dose, reducing the risk of side
effects/complications and related unplanned hospitalizations, and
improving patients' quality of life. Both primary and secondary FN
prevention are among the most important actions in the field of
supportive care during cancer chemotherapy. The ability to
administer the planned dose of cytotoxic drugs on time without
delaying the next cycle or a dose reduction is important for
effective systemic treatment; however, this is only possible when
peripheral blood parameters do not differ significantly from the
reference values.
In the present study, the authors identified that
the risk of neutropenia/FN associated with the applied chemotherapy
was in the range of 10–20% in more than half of the patients, and
that majority of patients (>70%) presented additional risk
factors for FN. Thus, a large proportion of patients were in the
‘risk group’ for chemotherapy-induced neutropenia and its
complications. Previous systematic review including 3,494 patients
demonstrated that compared to controls, the prophylactic use of
G-CSF significantly reduced the relative risk (RR) of FN in
patients receiving anticancer chemotherapy (RR reduction of 46%),
and reduced early mortality as well as mortality due to infectious
complications (RR reductions of 40% and 45%, respectively)
(10). Furthermore, prophylactic use
of G-CSF in these patients resulted in a significant improvement in
maintaining the desired density of the cytotoxic dose (10). At the same time, a significantly higher
incidence of bone and musculoskeletal pain was observed in patients
receiving G-CSF compared to those without (19.6% vs. 10.4%,
respectively) (10).
Clinical trials have indicated that biosimilar
preparations of filgrastim have similar benefits compared to the
original product, as well as similar safety and tolerability
profiles. For example, in the phase III randomized trial comparing
biosimilar filgrastim (EP2006) with the original product
(Neupogen®; Amgen Inc., Thousand Oaks, CA, USA) in the prevention
of severe neutropenia in 218 patients with breast cancer receiving
chemotherapy [according to the TAC (docetaxel, doxorubicin and
cyclophosphamide) protocol], no significant differences in efficacy
and safety were observed (11). There
was also no difference between the studied preparations in the
duration of severe neutropenia during the first cycle of treatment,
which was the primary endpoint of the study (1.2 days for the
biosimilar filgrastim and 1.2 days for the original preparation,
respectively) (11). No differences in
other clinically relevant features (including the incidence of FN,
the need for hospitalization due to FN, the incidence of infectious
complications, depth and time of the ANC nadir and the
normalization of ANC) during the first and all subsequent cycles of
treatment were observed (11).
In a previous non-interventional observational study
involving >1,300 patients undergoing chemotherapy (the HEXAFIL
study), the clinical usefulness, efficacy and safety of biosimilar
filgrastim was evaluated (12). A
large number of patients (44.9%) received biosimilar filgrastim for
primary prevention of FN, similar to the present study in which 60%
received biosimilar filgrastim for primary prophylaxis.
Approximately 90% of patients could continue chemotherapy without
need for treatment modification (i.e., cytostatic dose or time of
administration) (12). Complications
associated with neutropenia occurred in 7.9, 6.9 and 3.9% of
patients at the first, second and third treatment cycle,
respectively (12). During the first
cycle of chemotherapy, only 1.8% of patients experienced FN.
Tolerance and safety of biosimilar filgrastim was similar to that
previously known for this class of drugs; that is, bone and muscle
pain were the most common treatment-related adverse events
(12).
Characteristics of use and effectiveness of
biosimilar filgrastim (Zarzio®; Sandoz, Holzkirchen, Germany) in
the prevention of chemotherapy-induced neutropenia (and FN) were
also investigated in the international, multicenter,
non-interventional observational (MONITOR-GCSF) study (13). In the current study involving >1,400
patients, the majority (72.3%) of patients received G-CSF in
primary prophylaxis (similar to the 60% recorded in our study).
Based on their data, it was concluded that the clinical efficacy
and safety of biosimilar filgrastim (Zarzio®) is comparable to
historical data collected in studies on the original product
(Neupogen®) (13). Similar conclusions
were drawn based in the French prospective observational
multicenter study (n=184 patients), where the same biosimilar
filgrastim preparation (Zarzio®) was used (14). No cases of FN were noted in the current
study; however, neutropenia requiring hospitalization and/or
antibiotic use occurred in 10 patients (14). Biosimilar filgrastim (Zarzio®) was also
evaluated in a population of patients with soft tissue sarcomas
receiving chemotherapy according to EI protocol (epirubicin,
ifosfamide) in the NEUSAR study (15).
The frequency of neutropenia of all grades and grade 4 neutropenia
(ANC <0.5×103/µl) were comparable for biosimilar
filgrastim and original products (Granulokine® and Neupogen®; Amgen
Inc.) (15). Similarly, the incidence
of FN did not significantly differ with the biosimilar drug
compared to the originators; the incidence was 44% for biosimilar
filgrastim and 40% for the original filgrastim (12). On the basis of the present study, it
was concluded that biosimilar filgrastim is effective in the
prevention of FN and reduces the frequency of unplanned
hospitalization in patients with soft tissue sarcomas (15). Comparable clinical efficacy of
biosimilar filgrastim (Zarzio®/Filgrastim Hexal®; Sandoz) to the
original product (Neupogen®) was also found in a non-interventional
study (16), in which 77 patients with
cancer were treated with biosimilar filgrastim and 25 were treated
with the original product. In both the biosimilar filgrastim and
original product treatment arms, FN only occurred in one patient
(16). Only 6.5% of patients receiving
biosimilar filgrastim developed neutropenia requiring chemotherapy
dose reduction or its discontinuation compared with 8% of patients
treated with the original product (16).
Together, the accumulating findings indicated the
usefulness of biosimilar filgrastim in the primary and secondary
prevention of chemotherapy-induced neutropenia/FN, as well as its
clinical efficacy, safety, tolerance and acceptance by patients. In
the present study, the authors evaluated a new biosimilar
filgrastim, Accofil®. The results are consistent with published
reports, including those mentioned above. A high percentage
(>90%) of patients treated with biosimilar filgrastim (Accofil®)
could continue the chemotherapy according to plan for each of the
analyzed cycles. Furthermore, a high percentage (>90%) of
patients treated with Accofil® did not experience FN at all cycles
of chemotherapy. An added benefit of Accofil® is the ease of which
it can be applied; a high percentage of patients self-injected the
biosimilar filgrastim in the present study. Furthermore, Accofil®
reported good tolerance and safety in the patients. Finally, both
the present study and previous literature indicate that
biologically similar G-CSF preparations demonstrate clinical
efficacy in patients with different malignancies, including solid
tumors, neoplasms of the lymphatic system, tumors of epithelial
origin and soft tissues tumors.
In summary, biologically similar filgrastim
(Accofil®) used in the primary and secondary prevention of
chemotherapy-induced neutropenia/FN, shows high efficiency, safety
and tolerability while being readily-accepted by patients and
convenient to use. By combining the current results with the data
presented in the literature, it may be concluded that the efficacy
and safety of Accofil® is comparable to the original filgrastim
product (Neupogen®) and to other biosimilar filgrastim preparations
(Zarzio®, Sandoz). Thus, Accofil® should be recommended for use in
everyday clinical practice.
Acknowledgements
The present study and the preparation of the
manuscript have been supported by Accord Healthcare.
References
|
1
|
Crawford J, Caserta C and Roila F: ESMO
Guidelines Working Group: Hematopoietic growth factors: ESMO
Clinical Practice Guidelines for the applications. Ann Oncol. 21
Suppl 5:v248–v251. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Dale DC: Colony-stimulating factors for
the management of neutropenia in cancer patients. Drugs. 62 Suppl
1:1–15. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
de Naurois J, Novitzky-Basso I, Gill MJ,
Marti FM, Cullen MH and Roila F: ESMO Guidelines Working Group:
Management of febrile neutropenia: ESMO Clinical Practice
Guidelines. Ann Oncol. 21 Suppl 5:v252–v256. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
European Commission, . Community register
of medicinal products for human use: Accofil. http://ec.europa.eu/health/documents/community-register/html/h946.htmFeb
11–2017
|
|
5
|
Greil R, Psenak O and Roila F: ESMO
Guidelines Working Group: Hematopoietic growth factors: ESMO
recommendations for the applications. Ann Oncol. 19 Suppl
2:ii116–ii118. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Aapro MS, Bohlius J, Cameron DA, Dal Lago
L, Donnelly JP, Kearney N, Lyman GH, Pettengell R, Tjan-Heijnen VC,
Walewski J, et al: European Organisation for Research and Treatment
of Cancer: 2010 update of EORTC guidelines for the use of
granulocyte-colony stimulating factor to reduce the incidence of
chemotherapy-induced febrile neutropenia in adult patients with
lymphoproliferative disorders and solid tumours. Eur J Cancer.
47:8–32. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Weise M, Bielsky MC, de Smet K, Ehmann F,
Ekman N, Narayanan G, Heim HK, Heinonen E, Ho K, Thorpe R, et al:
Biosimilars-why terminology matters. Nat Biotechnol. 29:690–693.
2011. View
Article : Google Scholar : PubMed/NCBI
|
|
8
|
Dranitsaris G, Amir E and Dorward K:
Biosimilars of biological drug therapies: Regulatory, clinical and
commercial considerations. Drugs. 71:1527–1536. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Gottlieb S: Biosimilars: Policy, clinical,
and regulatory considerations. Am J Health Syst Pharm. 65 Suppl
6:S2–S8. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Kuderer NM, Dale DC, Crawford J and Lyman
GH: Impact of primary prophylaxis with granulocyte
colony-stimulating factor on febrile neutropenia and mortality in
adult cancer patients receiving chemotherapy: A systematic review.
J Clin Oncol. 25:3158–3167. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Blackwell K, Semiglazov V, Krasnozhon D,
Davidenko I, Nelyubina L, Nakov R, Stiegler G, Singh P, Schwebig A,
Kramer S, et al: Comparison of EP2006, a filgrastim biosimilar, to
the reference: A phase III, randomized, double-blind clinical study
in the prevention of severe neutropenia in patients with breast
cancer receiving myelosuppressive chemotherapy. Ann Oncol.
26:1948–1953. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Tesch H, Ulshöfer T, Vehling-Kaiser U,
Ottillinger B, Bulenda D and Turner M: Prevention and treatment of
chemotherapy-induced neutropenia with the biosimilar filgrastim: A
non-interventional observational study of clinical practice
patterns. Oncol Res Treat. 38:146–152. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Erratum G, ascón P, Aapro M, Ludwig H,
Bokemeyer C, Boccadoro M, Turner M, Denhaerynck K, MacDonald K and
Abraham I: Treatment patterns and outcomes in the prophylaxis of
chemotherapy-induced (febrile) neutropenia with biosimilar
filgrastim (the MONITOR-GCSF study). Support Care Cancer.
24:911–925. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Nahon S, Rastkhah M, Ben Abdelghani M,
Soumoudronga RF, Gasnereau I and Labourey JL: Zarzio®, biosimilar
of filgrastim, in prophylaxis of chemotherapy-induced neutropenia
in routine practice: A French prospective multicentric study.
Support Care Cancer. 24:1991–1998. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Bongiovanni A, Monti M, Foca F, Recine F,
Riva N, Di Iorio V, Liverani C, de Vita A, Miserocchi G, Mercatali
L, et al: Recombinant granulocyte colony-stimulating factor
(rG-CSF) in the management of neutropenia induced by anthracyclines
and ifosfamide in patients with soft tissue sarcomas (NEUSAR).
Support Care Cancer. 25:111–117. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Verpoort K and Möhler TM: A
non-interventional study of biosimilar granulocyte
colony-stimulating factor as prophylaxis for chemotherapy-induced
neutropenia in a community oncology centre. Ther Adv Med Oncol.
4:289–293. 2012. View Article : Google Scholar : PubMed/NCBI
|