Introduction
Endometriosis is a benign tumor, classically defined
as the presence of endometrial tissues at sites outside the uterine
cavity. Endometriosis affects 6-10% of women of reproductive age
(1). The most common symptoms of
endometriosis include dysmenorrhea, dyspareunia, chronic pelvic
pain, and infertility (2). Abdominal
wall endometriosis arises in the location above the peritoneum or
in scar tissues. Abdominal wall endometriosis is rare, with a
reported incidence of 0.03-3.5% (3).
Although Caesarean section surgical scars are the most common sites
of abdominal wall endometriosis, it has also been reported in
laparoscopic trocar tracts or at episiotomy incision sites
(4). It is often misdiagnosed as a
hernia, hematoma, abscess, or lipoma because of its rarity
(5-7).
The high rate of misdiagnosis causes unnecessary procedures with
increased emotional and physical distress among these patients
(8). It is not uncommon to refer
patients to an orthopedic department since physicians suspect that
a mass may be an abdominal wall tumor, but this is not familiar to
orthopedic surgeons. Herein, we describe three cases of abdominal
wall endometriosis. Written informed consent for the present report
was obtained from all patients. Institutional review board approval
was waived because of the nature of this study.
Case reports
Case 1
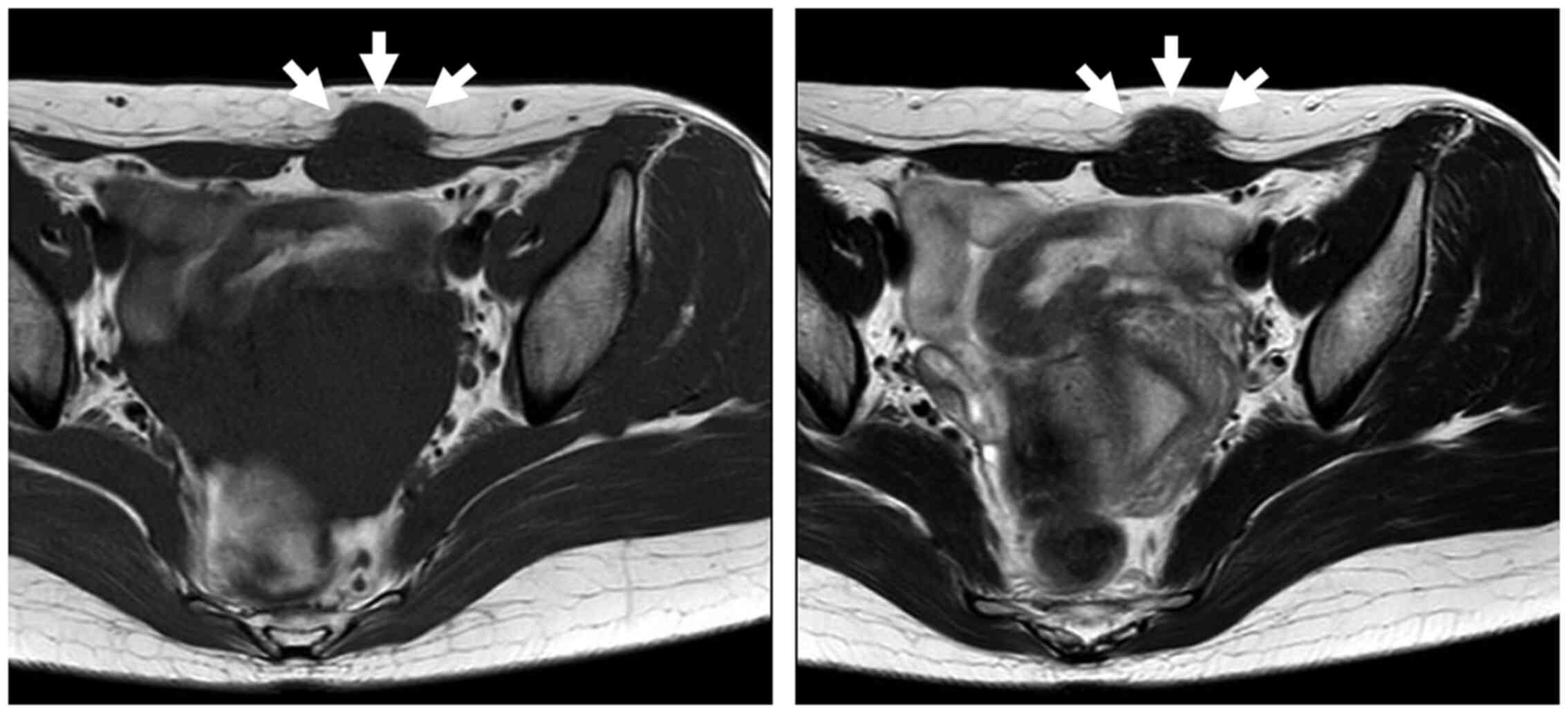
A 44-year-old healthy woman developed a lower
abdominal painful mass 3 years prior. She mentioned that the mass
was associated with her menstrual cycle. She had undergone
Caesarean section 6 years before the initial presentation. At the
clinical examination, a painful, elastic, hard, round mass
approximately 30 mm in diameter was observed above her Caesarean
section surgical scar. Pelvic magnetic resonance imaging (MRI)
revealed a 25-mm mass in the subcutaneous abdominal wall. The mass
showed isointensity compared to the muscle on both T1- and
T2-weighted images (Fig. 1). We
suspected abdominal wall endometriosis because of the patient's
medical history, clinical symptoms, and radiological examination
findings. We planned to resect the tumor to confirm the diagnosis.
The pathological findings confirmed endometrial gland and
endometrial stroma features; the final diagnosis was endometriosis.
Adequate surgical margins were acquired at a distance of 10 mm. At
the 3-year follow-up, there was no recurrence, and she did not
experience pain.
Case 2
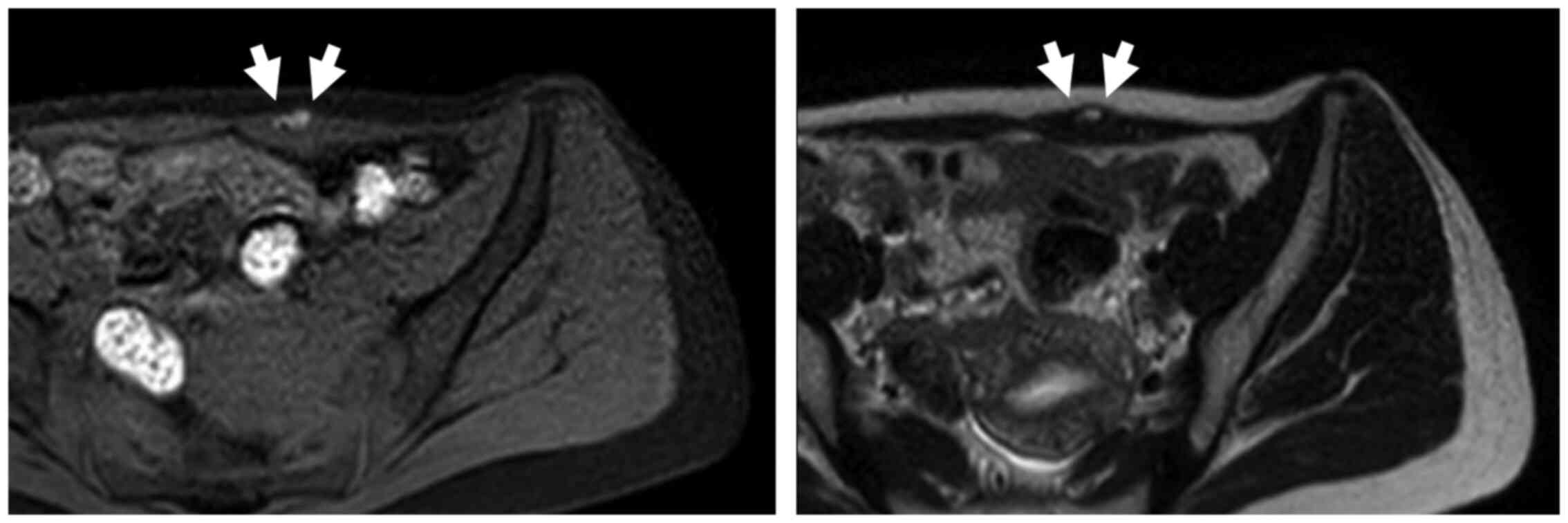
A 37-year-old woman developed a lower abdominal
painful mass 3 years prior. She mentioned that the mass was
associated with her menstrual cycle. She had undergone Caesarean
section twice: 5 and 7 years before the initial presentation. At
the clinical examination, a painful, elastic, hard, round mass
approximately 20 mm in diameter was detected 20 mm proximal to the
Caesarean section surgical scar. Pelvic MRI revealed a 15-mm mass
in the subcutaneous abdominal wall. The mass showed hyperintensity
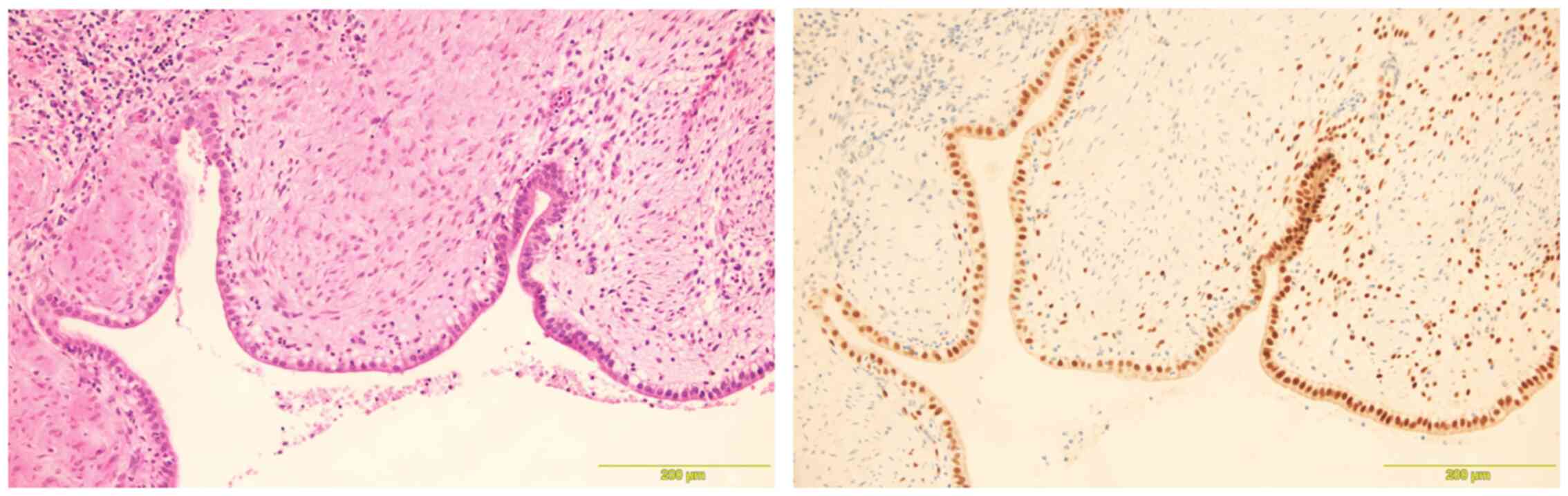
compared to the muscle on both T1- and T2-weighted images (Fig. 2). As we suspected abdominal wall
endometriosis, tumor resection was performed. Estrogen receptors
tested positive on immunohistochemical analysis (Fig. 3). At the 1-year follow-up, there was
no recurrence, and she did not experience pain.
Case 3
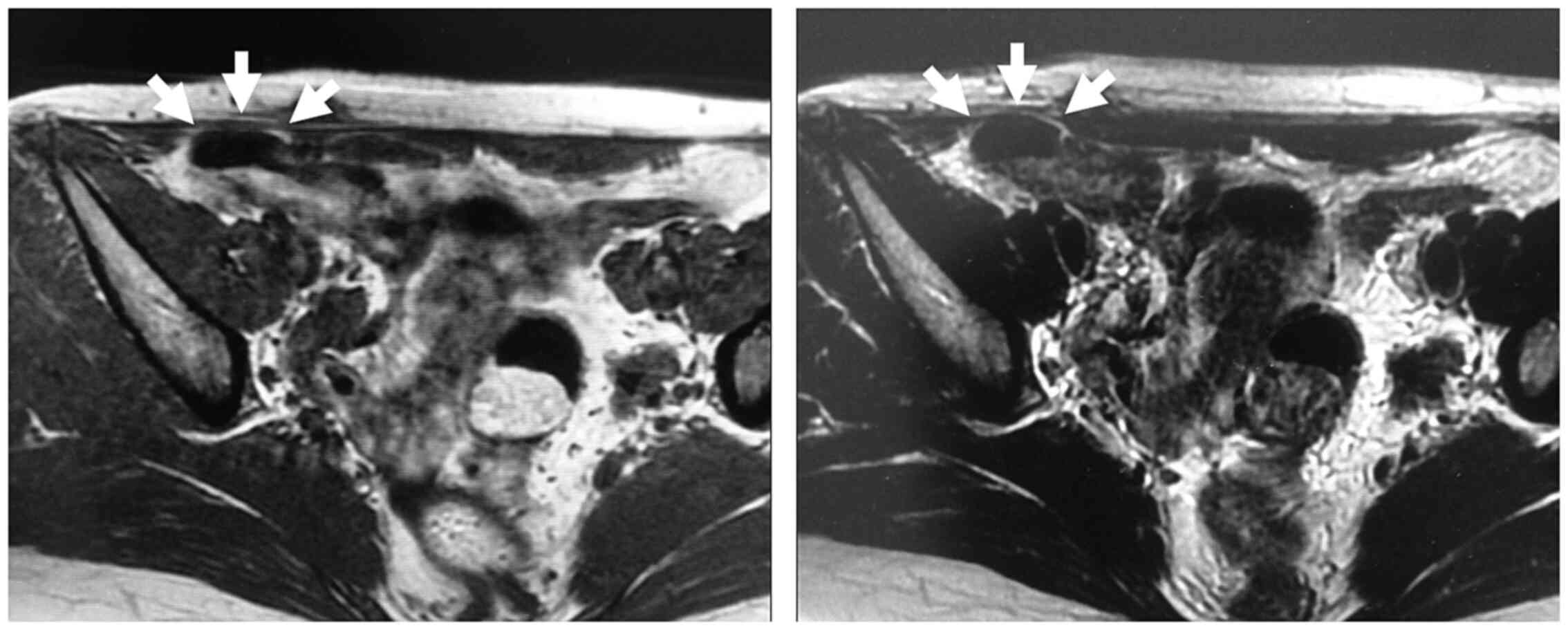
A 26-year-old woman developed a lower abdominal
painful mass 6 months prior. She had undergone Caesarean section
twice: 1 and 5 years before the initial presentation. At the
clinical examination, a painful, elastic, hard, round mass
approximately 30 mm in diameter was detected 5 mm to the right of
her Caesarean section surgical scar. Pelvic MRI revealed a 20-mm
mass in the subcutaneous abdominal wall. The mass showed
isointensity compared to the muscle on both T1- and T2-weighted
images (Fig. 4). As we suspected
abdominal wall endometriosis, tumor resection was performed. At the
1-year follow-up, there was no recurrence, and she did not
experience pain.
Discussion
The most evident clinical manifestation of
endometriosis is a painful subcutaneous mass with cyclic pain
associated with menses (9). The
cyclical nature of the complaint is present in 40-73% of cases
(7,8,10). The
symptoms are often associated with a history of development of a
palpable mass within or adjacent to a surgical scar. The incidence
of endometriosis after a Caesarean section has been estimated to be
0.26% in a 25-year interval (3).
Another paper published by Singh et al reported a similar
incidence, i.e., 0.2% in a 10-year interval (11). The average duration between Caesarean
section surgery and the onset of symptoms is 3.7-4.5 years
(12). The incidence of
endometriosis after a Caesarean section shows a significantly high
relative risk of 3.3 compared to that of endometriosis associated
with scars concerning other surgical procedures, such as
laparoscopic trocar or episiotomy (3). This high risk can be explained by the
higher exposure of endometrial cells to the subcutaneous tissue
during the procedure. Some studies have demonstrated the use of
oral contraceptives, gonadotropin-releasing hormone analogs,
danazol, and progesterone, which are approved for treating pelvic
endometriosis (13). However,
complete surgical excision of endometriotic lesions is required to
avoid recurrence. The recurrence rate with inadequate resection has
been reported as 4.5-9.1% (8). In
the present cases, adequate surgical margins were acquired and
there were no recurrences.
The pathogenesis of endometriosis is explained
mainly by the metaplasia theory, embryonic rest theory, or
transport theory. The metaplasia theory suggests that primitive
mesenchymal cells undergo specialized differentiation of metaplasia
to form endometrial implants (11).
The embryonic rest theory hypothesizes that Müllerian remnants can
differentiate into endometrial tissue, which may cause symptoms
(12). The transport theory,
specifically the implantation theory, suggests that endometrial
cells escape through an incision made in the uterus during the
surgical procedure and are implanted within the abdominal wall
(14). In our study, all patients
were young women of reproductive age, had a history of prior
Caesarean section, and harbored an abdominal mass in or adjacent to
their Caesarian surgical scars. These findings suggest a surgically
induced iatrogenic implantation etiology.
The use of MRI, computed tomography,
ultrasonography, and fine-needle aspiration in clinical practice
for the diagnosis of abdominal wall endometriosis is well reported
(15,16). Although these diagnostic techniques
can adequately depict abdominal wall lesions, these imaging
modalities cannot provide a definitive preoperative diagnosis.
Concerning MRI, typical ovarian endometriosis shows hyperintensity
on T1-weighted images and hypointensity on T2-weighted images. On
the other hand, in the abdominal wall, endometriosis may be
isointense or mildly hyperintense to muscle on both T1- and
T2-weighted images. In some cases, there may be cystic areas of
hemorrhage within abdominal wall endometriosis that appear
homogeneously hyperintense on T1-weighted images (13,17).
Among the present cases, two patients showed hyperintensity to the
muscle on both T1- and T2-weighted images, and one patient showed
isointensity on both T1- and T2-weighted images. Therefore,
hematoma, suture granuloma, or desmoid may be considered among the
differential diagnoses of abdominal wall endometriosis. The
reported accurate preoperative diagnosis rate varies between 20 and
50% (6,10). We decided to perform wide resection
in all cases since function could be preserved. A possible
explanation of diagnostic failure is that the diagnoses are almost
always confirmed by physicians who are not very familiar with this
entity. Therefore, we must obtain the needed patient medical
histories and perform physical examinations. Finally, we can be led
to suspect abdominal wall endometriosis based on several findings
including medical history, typical symptoms, and radiological
examinations.
Acknowledgements
Not applicable.
Funding
No funding was received.
Availability of data and materials
Additional information concerning the three case
reports is available from the corresponding author upon reasonable
request.
Authors' contributions
TN conceived the study, treated the patients,
collected the data and wrote the manuscript. THag collected,
analyzed and interpreted the clinical data. THas and KA performed
the surgery, analyzed and interpreted the clinical data. AS
analyzed and interpreted the clinical data and reviewed the
manuscript. All authors read and approved the manuscript and agree
to be accountable for all aspects of the research in ensuring that
the accuracy or integrity of any part of the work are appropriately
investigated and resolved.
Ethics approval and consent to
participate
Written informed consent for the present report was
obtained from all patients. Institutional review board approval was
waived because of the nature of this study.
Patient consent for publication
Written informed consent was obtained from the
patients for the publication of the case details and associated
images.
Competing interests
The authors declare that they have no competing
interests.
Authors' information
Tomohito Hagi: ORCID: 0000-0002-2937-3447.
References
|
1
|
Burney RO and Giudice LC: Pathogenesis and
pathophysiology of endometriosis. Fertil Steril. 98:511–519.
2012.PubMed/NCBI View Article : Google Scholar
|
|
2
|
Cozzolino M, Magnolfi S, Corioni S,
Moncini D and Mattei A: Abdominal wall endometriosis on the right
port site after laparoscopy: Case report and literature review.
Ochsner J. 15:262–264. 2015.PubMed/NCBI
|
|
3
|
Nominato NS, Prates LF, Lauar I, Morais J,
Maia L and Geber S: Caesarean section greatly increases risk of
scar endometriosis. Eur J Obstet Gynecol Reprod Biol. 152:83–85.
2010.PubMed/NCBI View Article : Google Scholar
|
|
4
|
Gidwaney R, Badler RL, Yam BL, Hines JJ,
Alexeeva V, Donovan V and Katz DS: Endometriosis of abdominal and
pelvic wall scars: Multimodality imaging findings, pathologic
correlation, and radiologic mimics. Radiographics. 32:2031–2043.
2012.PubMed/NCBI View Article : Google Scholar
|
|
5
|
Tazaki T, Oue N, Ichikawa T, Tsumura H,
Hino H, Yamaoka H, Kanehiro T and Yasui W: A case of endometriosis
of the appendix. Hiroshima J Med Sci. 59:39–42. 2010.PubMed/NCBI
|
|
6
|
Horton JD, Dezee KJ, Ahnfeldt EP and
Wagner M: Abdominal wall endometriosis: A surgeon's perspective and
review of 445 cases. Am J Surg. 196:207–212. 2008.PubMed/NCBI View Article : Google Scholar
|
|
7
|
Ozel L, Sagiroglu J, Unal A, Unal E, Gunes
P, Baskent E, Aka N, Titiz MI and Tufekci EC: Abdominal wall
endometriosis in the cesarean section surgical scar: A potential
diagnostic pitfall. J Obstet Gynaecol Res. 38:526–530.
2012.PubMed/NCBI View Article : Google Scholar
|
|
8
|
Khan Z, Zanfagnin V, El-Nashar SA,
Famuyide AO, Daftary GS and Hopkins MR: Risk factors, clinical
presentation, and outcomes for abdominal wall endometriosis. J
Minim Invasive Gynecol. 24:478–484. 2017.PubMed/NCBI View Article : Google Scholar
|
|
9
|
Woodward PJ, Sohaey R and Mezzetti TP Jr:
Endometriosis: Radiologic-pathologic correlation. Radiographics.
21:193–216. 2001.PubMed/NCBI View Article : Google Scholar
|
|
10
|
Bektaş H, Bilsel Y, Sari YS, Ersöz F, Koc
O, Deniz M, Boran B and Huq GE: Abdominal wall endometrioma; a
10-year experience and brief review of the literature. J Surg Res.
164:e77–e81. 2010.PubMed/NCBI View Article : Google Scholar
|
|
11
|
Singh KK, Lessells AM, Adeam DJ, Jordan C,
Miles WF, Macintyre IM and Greig JD: Presentation of endometriosis
to general surgeons: A 10-year experience. Br J Surg. 82:1349–1351.
1995.PubMed/NCBI View Article : Google Scholar
|
|
12
|
Agarwal N and Subramanian A:
Endometriosis-morphology, clinical presentations and molecular
pathology. J Lab Physicians. 2:1–9. 2010.PubMed/NCBI View Article : Google Scholar
|
|
13
|
Hensen JH, Van Breda Vriesman AC and
Puylaert JB: Abdominal wall endometriosis: Clinical presentation
and imaging features with emphasis on sonography. AJR Am J
Roentgenol. 186:616–620. 2006.PubMed/NCBI View Article : Google Scholar
|
|
14
|
Blanco RG, Parithivel VS, Shah AK, Gumbs
MA, Schein M and Gerst PH: Abdominal wall endometriomas. Am J Surg.
185:596–598. 2003.PubMed/NCBI View Article : Google Scholar
|
|
15
|
Francica G: Reliable clinical and
sonographic findings in the diagnosis of abdominal wall
endometriosis near cesarean section scar. World J Radiol.
4:135–140. 2012.PubMed/NCBI View Article : Google Scholar
|
|
16
|
Stein L, Elsayes KM and Wagner-Bartak N:
Subcutaneous abdominal wall masses: Radiological reasoning. AJR Am
J Roentgenol. 198:W146–W151. 2012.PubMed/NCBI View Article : Google Scholar
|
|
17
|
Busard MP, Mijatovie V, van Kuijk C,
Hompes PG and van Waesberghe JH: Appearance of abdominal wall
endometriosis on MR imaging. Eur Radiol. 20:1267–1276.
2010.PubMed/NCBI View Article : Google Scholar
|