Introduction
Constipation is one of the most common
gastrointestinal complaints, and its incidence appears to increase
with increasing age (1). It was
reported that in an internet survey, 28.4% of the respondents
considered themselves to be constipated in Japan (2). Since chronic constipation greatly
impairs a patient's quality of life (QOL), measures to treat
constipation are an important issue in elderly adults (3). In addition, Choung et al
reported that neurological and cardiovascular diseases are linked
to constipation, and it was suggested that constipation was
associated with systemic disease (4). Sarcopenia is an age-related geriatric
syndrome that is characterized by the gradual loss of muscle mass,
muscle strength, and muscle quality. It was reported that
sarcopenia is associated with cardiovascular mortality and
all-cause mortality (5). In
addition, the prevalence of sarcopenia is higher among subjects
with various diseases such as type 2 diabetes, osteoporosis, mild
cognitive impairment and Alzheimer disease (6-8).
The elderly population has increased rapidly in Japan, and the care
of elderly patients has become a serious issue, with sarcopenia
attracting much attention as a cause of the heavy burden to
families and society (9). Sarcopenia
and chronic constipation frequently occur in elderly adults;
however, the association between the two diseases has not been
clearly established. In the present study, we carried out a
single-center university hospital-based retrospective
cross-sectional analysis to clarify the association between the
severity of constipation and sarcopenia in elderly adults.
Materials and methods
Study design
We conducted a single-center university
hospital-based, retrospective cross-sectional study of consecutive
outpatients ≥65 years of age who were being treated at the
Department of Gastroenterology of Juntendo Tokyo Koto Geriatric
Medical Center between April 2017 and March 2020.
Inclusion criteria
Subjects were included if all of the following
information was available from their medical records: i) patient
profile [age, sex, body mass index (BMI)]; ii) use of
laxative/prokinetics; iii) evaluation of sarcopenia; iv)
nutritional status [albumin level, cholesterol level, lymphocyte
count, CONtrolling NUTritional status (CONUT) score]; v)
questionnaires concerning the severity of constipation
[Constipation Scoring System (CSS)] vi) questionnaire concerning
abdominal symptom-related QOL (Izumo scale) and vii) questionnaire
concerning stool shape [Bristol Stool Form Scale (BSFS)].
We included patients for whom we had performed
colonoscopy (or barium enema) and chest, abdominal, and pelvic
computed tomography within one year. The data on patient profile,
medications, questionnaires, and findings concerning sarcopenia
were collected at the same time.
Exclusion criteria
Patients who were unable to walk due to severe
osteoarthritis or neuromuscular disease, immobile patients,
patients presenting with delirium tremens, and patients with a
history of acute cerebrovascular, gastrointestinal, renal,
coronary, hepatic, or respiratory events were excluded from this
study. We excluded patients found to have the following conditions:
History of gastrectomy, inflammatory bowel disease (IBD), malignant
disease (gastric, esophageal, colon, lung, pancreatic, liver, bile
duct, gallbladder, breast, uterine, ovarian, prostate, and bladder
cancer, as well as malignant lymphoma, leukemia, and multiple
myeloma), type 1 diabetes mellitus, hypo/hyper-thyroidism,
hypo/hyper-parathyroid disorder, or mental illness.
Patients were also excluded if they met any of the
following criteria that affect sarcopenia: Severe cardiac,
pulmonary, or musculoskeletal disorders; severe neurologic
disorders, such as Parkinson's disease or stroke; and patients in
Japan's long-term care service.
Definition of sarcopenia
We defined sarcopenia using the diagnostic algorithm
recommended by the Asian Working Group for Sarcopenia: 2019
Consensus Update on Sarcopenia Diagnosis and Treatment, which
assesses the presence of both low muscle function (low physical
performance or low muscle strength) and low muscle mass (10).
In the present study, we considered subjects ≥65
years of age as having sarcopenia if they had a low appendicular
skeletal muscle mass with either a low handgrip strength or slow
gait speed. The handgrip strength, gait speed, and muscle mass were
measured as follows. The handgrip strength was measured using a
handgrip dynamometer (Toei Light Co., Ltd., Saitama, Japan). Both
hands were tested, and the larger value was noted as the maximum
muscle strength. A low grip strength was established according to
the sex-specific cut-off for the maximum muscle strength of the
subject according to the Asian Working Group for Sarcopenia (AWGS)
criteria (<28 kg for men; <18 kg for women). Gait speed was
manually assessed using a stopwatch. A slow gait speed was defined
as a gait speed of <1.0 m/sec according to the AWGS criteria.
Regional fat and lean mass were measured by whole-body dual X-ray
absorptiometry (DXA; Prodigy Advance, GE Healthcare). Subjects were
positioned for whole-body scans in accordance with the
manufacturer's protocol. The whole-body fat mass and lean mass were
divided into several regions, such as the arms, legs, and trunk.
The appendicular lean mass was estimated as the sum of the lean
mass of the two upper limbs and the lean mass of the two lower
limbs. The appendicular skeletal muscle mass index (SMI) was
calculated as the appendicular lean mass divided by the square of
the height (kg/m2). A low appendicular skeletal muscle
mass was defined as an SMI of <7.0 kg/m2 in men and
<5.4 kg/m2 in women.
Nutritional status
In this study, the CONUT score (between 0 and 12)
was used to evaluate the objective nutritional status. This score
is composed of the following three parameters: Serum albumin level,
total cholesterol level, and total lymphocyte count (11). The serum albumin level indicates the
protein reserves, the serum total cholesterol level indicates
caloric depletion, and the total lymphocyte count indicates
impairment of the immune system due to malnutrition. The CONUT
score is based on the following: Albumin (≥3.5 g/dl, 0 points;
3.00-3.49 g/dl, 2 points; 2.50-2.99 g/dl, 4 points; <2.50 g/dl,
6 points), total cholesterol (≥180 mg/dl, 0 points; 140-179 mg/dl,
1 point; 100-139 mg/dl, 2 points; <100 mg/dl, 3 points), and
total lymphocyte count (≥1,600/µl, 0 points; 1,200-1,599/µl, 1
point; 800-1,199/µl, 2 points; <800/µl, 3 points). Venous blood
samples for serum preparation were obtained in the early morning
after 12 h of fasting from all subjects, and the serum
concentration of albumin (g/dl), total lymphocyte count, and total
cholesterol level (mg/dl) were measured.
Questionnaire concerning the severity
of constipation
The CSS questionnaire, which is a self-administered
questionnaire concerning the severity of constipation, has been
validated for the assessment of constipation in clinical trial
settings (12). The CSS comprises 8
items describing the following symptoms of constipation: Frequency
of bowel movements, painful evacuation, incomplete evacuation,
abdominal pain, length of time per attempt, assistance for
evacuation, unsuccessful attempts at evacuation per 24 h, and
duration of constipation. The score for each item ranges from 0 to
4 with the exception of ‘assistance for evacuation’, whose score
ranges from 0 to 2. Consequently, the overall score for CSS ranges
from 0 to 30, with a higher score indicating worse constipation
symptoms.
Questionnaire concerning abdominal
symptom-related QOL
The Izumo scale was designed for the quantitative
measurement of abdominal symptom-related QOL (13). It is based on a self-reported
questionnaire including 15 items in 5 domains: Reflux, Upper
abdominal pain, Fullness, Constipation, and Diarrhea. Each item is
scored from 0 to 5 on a Likert scale according to the degree of
symptoms, as follows: 0=not bothered, 1=not so bothered, 2=slightly
bothered, 3=bothered, 4=strongly bothered and 5=intolerably
bothered. Each domain comprises three items and each domain has a
score from 0 to 15 points to evaluate the severity of symptoms,
with higher scores indicating more severe symptoms. Each question
is grouped into one of the five domains, in which questions 1, 2
and 3 are grouped into the Reflux domain, questions 4, 5 and 6 into
the Upper abdominal pain domain, questions 7, 8 and 9 into the
Fullness domain, questions 10, 11 and 12 into the Constipation
domain, and questions 13, 14 and 15 into the Diarrhea domain.
Domain-specific QOL impairment in the Izumo scale is ranked from 0
(no QOL impairment) to 15. It has good internal consistency and has
good correlation with the Gastrointestinal Symptom Rating Scale. In
each patient, the sum of the scores obtained for the three
questions in each domain (Reflux, Upper abdominal pain, Fullness,
Constipation, and Diarrhea) was calculated and defined as the
reflux-related QOL score, upper abdominal pain-related QOL score,
fullness-related QOL score, constipation-related QOL score, and
diarrhea-related QOL score, respectively.
Questionnaire concerning stool
shape
Stool consistency and shape were assessed by the
Bristol Stool Form Scale (BSFS) (14), which classifies stool into seven
categories: 1, nut-like; 2, lumpy sausage; 3, sausage with cracks;
4, smooth snake; 5, soft blobs; 6, fluffy pieces; and 7,
watery.
Ethics
This study was conducted in accordance with the
tenets of the Declaration of Helsinki. The Juntendo Tokyo Koto
Geriatric Medical Center Ethics Committee approved the study and
the study protocol (protocol no. 106-12). With regard to informed
consent of the participants, the Juntendo Tokyo Koto Geriatric
Medical Center Ethics Committee determined that this study was
exempt from the need to obtain patient consent. According to the
decision of the Juntendo Tokyo Koto Geriatric Medical Center Ethics
Committee, we notified the study subjects about our study contents
on the homepage of our hospital and guaranteed them the opportunity
to refuse participation.
Statistical analyses
Clinical characteristics were compared between the
sarcopenia and non-sarcopenia groups and univariate analyses of
clinical characteristics were performed using χ2 test
and t-test. Correlations between the constipation scoring system
(CSS) score and various clinical parameters (age, BMI, albumin
level, cholesterol level, lymphocyte count, CONUT score, BSFS
score, and reflux-related, upper abdominal pain-related,
fullness-related, constipation-related, and diarrhea-related QOL
scores) were determined based on Pearson's correlation
coefficients. The age, BMI, albumin level, cholesterol level,
lymphocyte count, CONUT score, CSS score, BSFS score, and
reflux-related, upper abdominal pain-related, fullness-related,
constipation-related, diarrhea-related QOL scores are presented as
the mean ± standard deviation. Comparison between the CSS score and
sarcopenia was analyzed using the box-and-whisker plot method.
Multiple regression analysis was performed with CSS score as the
dependent variable, and with age, sex, BMI, laxative/prokinetics
use, sarcopenia, albumin level, cholesterol level, lymphocyte
count, CONUT score, BSFS score, and reflux-related, upper abdominal
pain-related, fullness-related, constipation-related, and
diarrhea-related QOL scores as independent variables. Multiple
regression analysis of the risk factors for high CSS score was
performed using a forced entry method and we judged
multicollinearity by the variance inflation factor (VIF). All
statistical analyses were performed using the SPSS version 19
software program (IBM Corp.). P<0.05 was considered to indicate
a statistically significant difference.
Results
Clinical characteristics of the study
patients
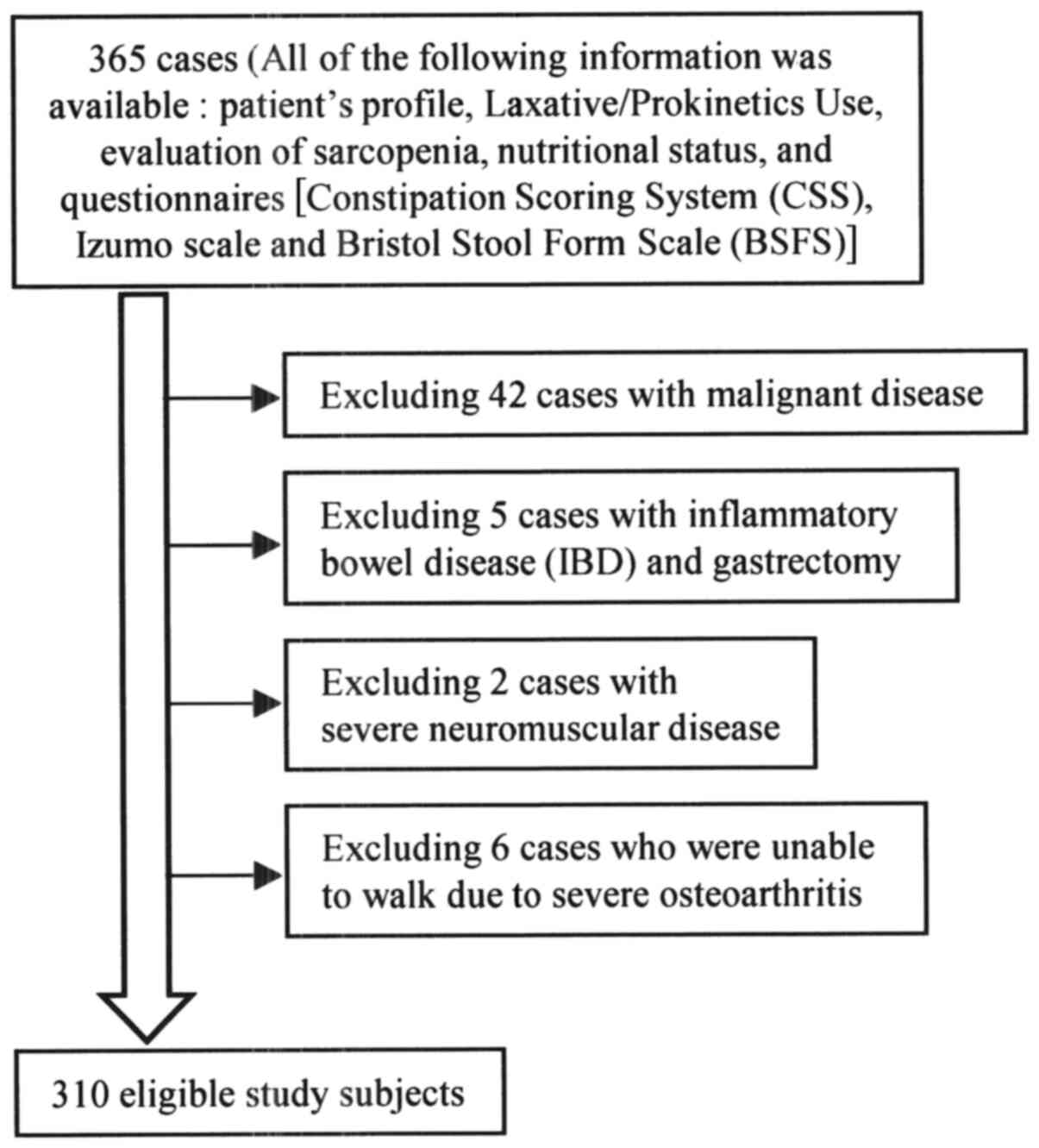
A flow chart of participants is shown in Fig. 1. The clinical characteristics of the
310 eligible study subjects [149 men (48.1%) and 161 women (51.9%);
mean age, 75.7±6.1 years; mean body mass index, 23.0±3.6
kg/m2] are summarized in Table I. The CSS score was significantly
higher in the sarcopenia group (n=83) than in the non-sarcopenia
group (n=227) (4.9±4.9 vs. 3.6±3.6, P=0.009). In addition, age
(P<0.001), male gender (P=0.004), prevalence of
laxative/prokinetic use (P=0.009) and CONUT score (P=0.001) were
significantly higher, while BMI (P<0.001), albumin level
(P=0.003) and cholesterol level (P=0.021) were significantly lower
in the sarcopenia group than in the non-sarcopenia group.
 | Table IClinical characteristics of the study
patients (n=310). |
Table I
Clinical characteristics of the study
patients (n=310).
| Patient profile | Total (n=310) | Sarcopenia
(n=83) | Non-sarcopenia
(n=227) | P-value |
|---|
| Age (years) | 75.7
(±6.1)b | 79.1
(±6.1)b | 74.4
(±5.7)b | <0.001 |
| Sex | | | | |
|
Male | 149
(48.1)a | 51
(61.4)a | 98
(43.2)a | |
|
Female | 161
(51.9)a | 32
(38.6)a | 129
(56.8)a | 0.004 |
| BMI
(kg/m2) | 23.0
(±3.6)b | 21.4
(±2.7)b | 23.6
(±3.7)b | <0.001 |
| Internal medicine
therapeutic agents | | | | |
|
Laxative/prokinetics | | | | |
|
Non-user | 241
(77.7)a | 56
(67.5)a | 185
(81.5)a | |
|
User | 69
(22.3)a | 27
(32.5)a | 42
(18.5)a | 0.009 |
| Nutritional
status | | | | |
|
Albumin
level (g/dl) | 4.2
(±0.4)b | 4.1
(±0.4)b | 4.2
(±0.3)b | 0.003 |
|
Cholesterol
level (mg/dl) | 204
(±36)b | 196
(±40)b | 206
(±34)b | 0.021 |
|
Lymphocyte
count (/µl) | 1,869
(±632)b | 1,768
(±690)b | 1,906
(±607)b | 0.088 |
|
CONUT
score | 0.9
(±1.2)b | 1.2
(±1.4)b | 0.7
(±1.1)b | 0.001 |
| Severity of
constipation | | | | |
|
CSS
score | 4.0
(±4.0)b | 4.9
(±4.9)b | 3.6
(±3.6)b | 0.009 |
| Abdominal
symptom-related QOL | | | | |
|
Reflux-related
QOL score | 1.5
(±2.0)b | 1.3
(±1.7)b | 1.5
(±2.1)b | 0.250 |
|
Upper
abdominal pain-related QOL score | 1.2
(±2.0)b | 0.9
(±2.0)b | 1.3
(±2.1)b | 0.150 |
|
Fullness-related
QOL score | 1.5
(±2.1)b | 1.3
(±2.0)b | 1.6
(±2.1)b | 0.178 |
|
Constipation-related
QOL score | 2.3
(±2.7)b | 2.4
(±2.7)b | 2.2
(±2.7)b | 0.520 |
|
Diarrhea-related
QOL score | 1.6
(±2.4)b | 1.7
(±2.6)b | 1.6
(±2.3)b | 0.814 |
| Stool shape | | | | |
|
BSFS
score | 4.0
(±1.0)b | 4.0
(±1.2)b | 4.0
(±1.0)b | 0.791 |
Correlations between the CSS score and
various clinical parameters
The results of Pearson's correlation coefficients
are shown in Table II. The CSS
score was significantly and positively correlated with the CONUT
score (r=0.130, P=0.011), reflux-related QOL score (r=0.155,
P=0.003), upper abdominal pain-related QOL score (r=0.171,
P=0.001), fullness-related QOL score (r=0.299, P<0.001),
constipation-related QOL score (r=0.615, P<0.001) and
diarrhea-related QOL score (r=0.235, P<0.001), while it was
significantly and negatively correlated with the albumin level
(r=-0.148, P=0.004), lymphocyte count (r=-0.118, P=0.019) and BSFS
score (r=-0.114, P=0.023).
| Table IICorrelations between the constipation
scoring system (CSS) score and various clinical parameters. |
Table II
Correlations between the constipation
scoring system (CSS) score and various clinical parameters.
| Clinical
parameters | r | P-value |
|---|
| Age (years) | 0.083 | 0.07 |
| BMI
(kg/m2) | -0.077 | 0.09 |
| Albumin level
(g/dl) | -0.148 | <0.01 |
| Cholesterol level
(mg/dl) | -0.086 | 0.07 |
| Lymphocyte count
(/µl) | -0.118 | <0.05 |
| CONUT score | 0.130 | <0.05 |
| Reflux-related QOL
score | 0.155 | <0.01 |
| Upper abdominal
pain-related QOL score | 0.171 | <0.01 |
| Fullness-related
QOL score | 0.299 | <0.001 |
|
Constipation-related QOL score | 0.615 | <0.001 |
| Diarrhea-related
QOL score | 0.235 | <0.001 |
| BSFS score | -0.114 | <0.05 |
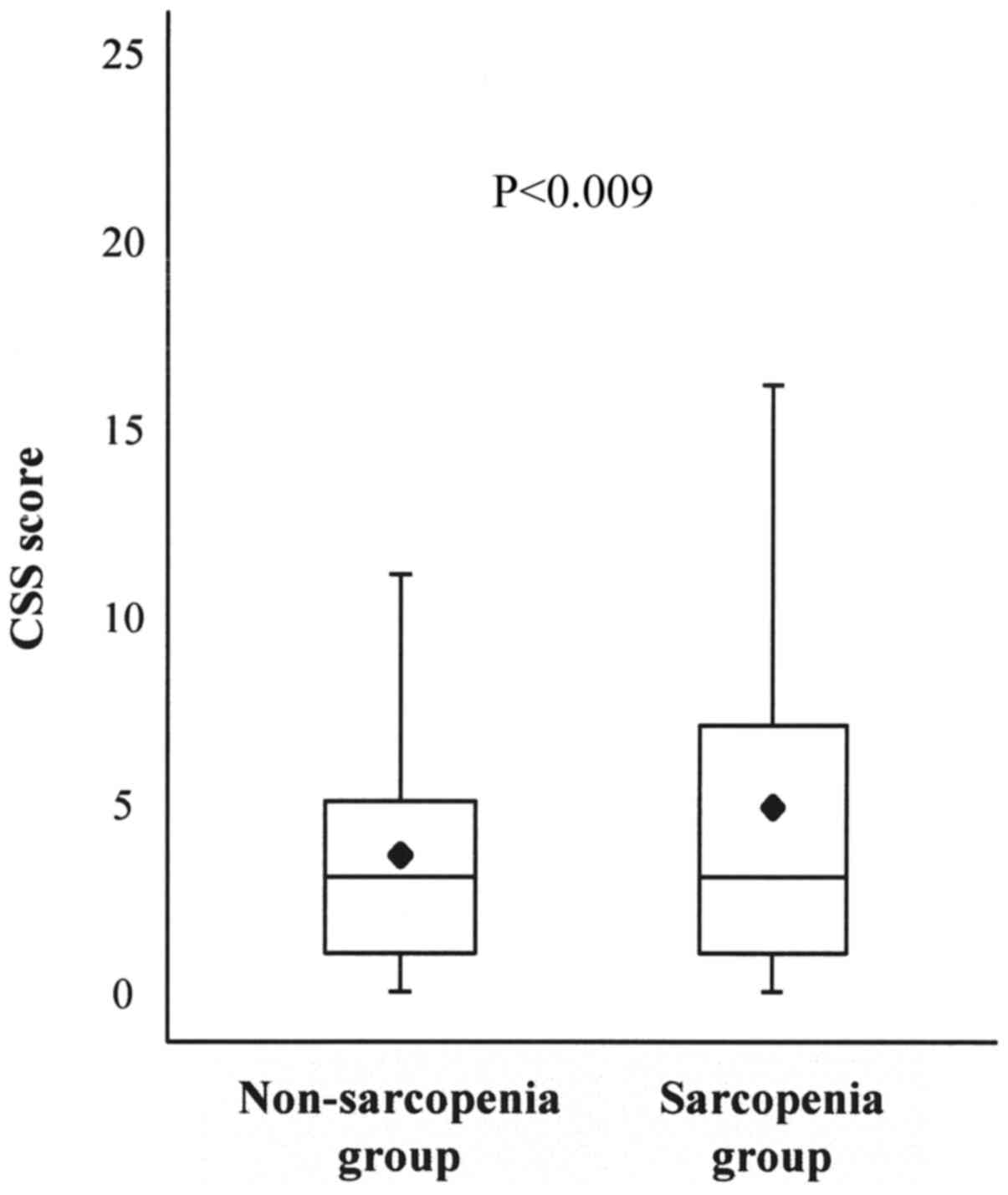
Association between the severity of
constipation and sarcopenia
The association between the CSS score and sarcopenia
was analyzed using the box-and-whisker plot method. The lower
hinge, median, and upper hinge of the box corresponded to the 25,
50, and 75th percentiles, respectively. The mean of the data set is
indicated by the rhombus. The CSS score was significantly higher in
subjects with sarcopenia than in subjects without sarcopenia
(4.9±4.9 vs. 3.6±3.6, P<0.001) (Table
I, Fig. 2).
Results of the multiple regression
analysis
The multiple regression analysis results are shown
in Table III. In the multiple
regression analysis, independent predictors for CSS score were
sarcopenia (standardized partial regression coefficient [β]=0.107,
P=0.032), constipation-related QOL score (β=0.537, P<0.001),
laxative/prokinetics use (β=0.211, P<0.001) and BSFS score
(β=-0.098, P=0.031) (R2=0.436).
| Table IIIAssociation between the constipation
scoring system (CSS) score and other variables in the multiple
regression analysis. |
Table III
Association between the constipation
scoring system (CSS) score and other variables in the multiple
regression analysis.
| Variables | B | SE | 95% CI of B | β | t | VIF | P-value |
|---|
| Age | -0.059 | 0.031 | 0.120, 0.002 | -0.091 | -1.905 | -0.081 | 0.058 |
| Sex | 0.477 | 0.372 | -0.256, 1.210 | 0.060 | 1.280 | 0.055 | 0.201 |
| BMI | -0.033 | 0.052 | -0.136, 0.070 | -0.029 | -0.625 | -0.027 | 0.533 |
|
Laxative/prokinetics use | 2.027 | 0.432 | 1.176, 2.878 | 0.211 | 4.688 | 0.200 | <0.001 |
| Sarcopenia | 0.966 | 0.447 | 0.086, 1.845 | 0.107 | 2.160 | 0.092 | 0.032 |
| Albumin level | -1.113 | 0.569 | -2.233, 0.008 | -0.098 | -1.954 | -0.083 | 0.052 |
| Cholesterol
level | -0.006 | 0.006 | -0.017, 0.006 | -0.051 | -0.971 | -0.041 | 0.332 |
| Lymphocyte
count | 0.000 | 0.000 | -0.001, 0.000 | -0.051 | -0.917 | -0.039 | 0.360 |
| CONUT score | -0.166 | 0.227 | -0.612, 0.279 | -0.049 | -0.735 | -0.031 | 0.463 |
| Reflux-related QOL
score | -0.078 | 0.101 | -0.278, 0.121 | -0.038 | -0.771 | -0.033 | 0.442 |
| Upper abdominal
pain-related QOL score | -0.048 | 0.104 | -0.253, 0.157 | -0.025 | -0.463 | -0.020 | 0.644 |
| Fullness-related
QOL score | 0.109 | 0.116 | -0.120, 0.337 | 0.056 | 0.937 | 0.040 | 0.350 |
|
Constipation-related QOL score | 0.803 | 0.078 | 0.650, 0.957 | 0.537 | 10.313 | 0.441 | <0.001 |
| Diarrhea-related
QOL score | 0.079 | 0.090 | -0.097, 0.256 | 0.047 | 0.884 | 0.038 | 0.378 |
| BSFS score | -0.382 | 0.176 | -0.728, -0.035 | -0.098 | -2.169 | -0.093 | 0.031 |
Discussion
To the best of our knowledge, no previous studies
have investigated the association between the severity of
constipation and sarcopenia in elderly adults. The present study
demonstrated that independent predictors for the Constipation
Scoring System (CSS) score were sarcopenia, constipation-related
quality of life (QOL) score, laxative/prokinetics use and Bristol
Stool Form Scale (BSFS) score in multiple regression analysis.
In this study, we demonstrated that there was a
positive association between the severity of constipation and
sarcopenia in elderly adults. Functional constipation can be
classified into normal transit constipation, slow transit
constipation, and functional defecation disorder (15). The process of defecation is carried
out in the following order. First, the anorectal angle assumes a
linear shape by the musculus puborectalis relaxing at the same time
to increase abdominal pressure. Furthermore, defecation is finally
performed by relaxation of the musculus sphincter ani externus
(16). Therefore, in the defecation
process, pelvic floor dysfunction and/or a decrease in abdominal
pressure may cause functional defecation disorder. Kepenekci et
al (17) demonstrated that age
was the major factor associated with the development of pelvic
floor dysfunction. Dimpfl et al (18) reported that aging and vaginal
childbirth lead to histomorphological changes in the pelvic floor
muscle that are consistent with changes of myogenic origin. Muscle
weakness by sarcopenia may cause pelvic floor dysfunction and/or a
decrease in abdominal pressure. As a result, painful evacuation
effort and feeling incomplete evacuation are caused, and the
severity of constipation might increase. In addition, due to
sarcopenia, the decrease of the muscular strength necessary for the
movement to the restroom might decrease stool frequency.
On the other hand, several studies reported a
neurologic change in the intestinal tract in patients with
constipation. Hanani et al (19) suggested that there is an increase in
the number of abnormally appearing myenteric ganglia in the human
colon with age, which may contribute to disturbed colonic motility
in the aging population. Bassotti et al (20) reported that patients with chronic
constipation have several abnormalities reconductable to
alterations in the enteric nervous system, abnormalities mainly
characterized by a constant decrease in enteric glial cells and
interstitial cells of Cajal. Kwon and Yoon (21) suggested that there are many
neurologic insults on sarcopenia at various levels from the brain
to the neuromuscular junctions (NMJs) to generate a volitional
task. Regarding the neurologic change in the intestinal tract, the
histopathological association between chronic constipation and
sarcopenia is unclear at present; however, a common neuropathy may
underlie both constipation and sarcopenia.
In addition, we found that the severity of
constipation was positively related to the constipation-related QOL
score and laxative/prokinetics use, and negatively related to stool
shape (BSFS score) in this study. Wald et al (3) suggested that chronic constipation
greatly impairs a patient's QOL. There were few reports of the
association between use of laxative/prokinetics and severity of
constipation in Japan. By the recent internet survey on the actual
situation of constipation in the Japanese population, 77.1% of
patients with functional constipation used laxatives (22). In our study, it was shown that
laxative/prokinetics users may have severe constipation. In a
previous study, Tanabe et al (23) reported that QOL was significantly
impaired in the constipated group, and that the BSFS score in the
constipation group was significantly lower than that in the control
group, indicating that the stool was harder in the constipation
group than in the control group.
There were several limitations to this study. First,
the single-center university hospital-based retrospective
cross-sectional design prevented us from establishing causal
associations between the severity of constipation and sarcopenia.
Second, the sample size was limited and we did not investigate the
life background of the subjects such as history of smoking/alcohol
use, exercise habits, meal contents, occupation/career, education
level, marital status, and medication use except
laxative/prokinetics. Thus, the findings in this study should be
considered preliminary owing to the relatively small sample size.
Therefore, it is possible that the present data are not
generalizable to all community-dwelling elderly individuals.
In conclusion, we found that there was a positive
association between the severity of constipation and sarcopenia in
elderly adults in a single-center university hospital-based,
retrospective cross-sectional study. It may be important in the
future to consider the therapy for constipation in elderly adults
with a comprehensive view that considers the prevention of
sarcopenia as well as meals, daily life guidance and medical
therapy. The findings in this study should be considered
preliminary owing to the relatively small sample size. Further
studies are required to understand these associations including
biological mechanisms.
Acknowledgements
The authors thank all of the participants for
cooperating with the study.
Funding
No funding was received.
Availability of data and materials
The datasets used during the present study are
available from the corresponding author upon reasonable
request.
Authors' contributions
DAs and AN conceived and designed the study. DAs
analyzed the data. DAs, TT, YI, DAb, YS, KeM, HU, KoM, HK, YA, TO,
MH and AN performed the data collection. All authors contributed to
the writing of the manuscript and reviewed and approved the final
manuscript.
Ethics approval and consent to
participate
The present study was conducted in accordance with
the tenets of the Declaration of Helsinki. The Juntendo Tokyo Koto
Geriatric Medical Center Ethics Committee approved the study and
the study protocol. According to the decision of the Juntendo Tokyo
Koto Geriatric Medical Center Ethics Committee, we notified the
study subjects concerning the contents of our study on the homepage
of our hospital and guaranteed them the opportunity to refuse
participation.
Patient consent for publication
Not applicable.
Competing interests
The authors declare that they have no conflicts of
interest.
References
|
1
|
Higgins PD and Johanson JF: Epidemiology
of constipation in North America: A systematic review. Am J
Gastroenterol. 99:750–759. 2004.PubMed/NCBI View Article : Google Scholar
|
|
2
|
Tamura A, Tomita T, Oshima T, Toyoshima F,
Yamasaki T, Okugawa T, Kondo T, Kono T, Tozawa K, Ikehara H, et al:
Prevalence and Self-recognition of chronic constipation: Results of
an internet survey. J Neurogastroenterol Motil. 22:677–685.
2016.PubMed/NCBI View
Article : Google Scholar
|
|
3
|
Wald A, Scarpignato C, Kamm MA,
Mueller-Lissner S, Helfrich I, Schuijt C, Bubeck J, Limoni C and
Petrini O: The burden of constipation on quality of life: Results
of a multinational survey. Aliment Pharmacol Ther. 26:227–236.
2007.PubMed/NCBI View Article : Google Scholar
|
|
4
|
Choung RS, Rey E, Richard Locke G III,
Schleck CD, Baum C, Zinsmeister AR and Talley NJ: Chronic
constipation and Co-morbidities: A prospective population-based
nested Case-control study. United European Gastroenterol J.
4:142–151. 2016.PubMed/NCBI View Article : Google Scholar
|
|
5
|
Atkins JL, Whincup PH, Morris RW, Lennon
LT, Papacosta O and Wannamethee SG: Sarcopenic obesity and risk of
cardiovascular disease and mortality: A population-based cohort
study of older men. J Am Geriatr Soc. 62:253–260. 2014.PubMed/NCBI View Article : Google Scholar
|
|
6
|
Anbalagan VP, Venkataraman V, Pradeepa R,
Deepa M, Anjana RM and Mohan V: The prevalence of presarcopenia in
Asian Indian individuals with and without type 2 diabetes. Diabetes
Technol Ther. 15:768–775. 2013.PubMed/NCBI View Article : Google Scholar
|
|
7
|
Yoshimura N, Muraki S, Oka H, Iidaka T,
Kodama R, Kawaguchi H, Nakamura K, Tanaka S and Akune T: Is
osteoporosis a predictor for future sarcopenia or vice versa?
Four-year observations between the second and third ROAD study
surveys. Osteoporos Int. 28:189–199. 2017.PubMed/NCBI View Article : Google Scholar
|
|
8
|
Sugimoto T, Ono R, Murata S, Saji N,
Matsui Y, Niida S, Toba K and Sakurai T: Prevalence and associated
factors of sarcopenia in elderly subjects with amnestic mild
cognitive impairment or Alzheimer disease. Curr Alzheimer Res.
13:718–726. 2016.PubMed/NCBI View Article : Google Scholar
|
|
9
|
Woo J, Leung J and Morley JE: Defining
sarcopenia in terms of incident adverse outcomes. J Am Med Dir
Assoc. 16:247–252. 2015.PubMed/NCBI View Article : Google Scholar
|
|
10
|
Chen LK, Woo J, Assantachai P, Auyeung TW,
Chou MY, Iijima K, Jang HC, Kang L, Kim M, Kim S, et al: Asian
working group for sarcopenia: 2019 consensus update on sarcopenia
diagnosis and treatment. J Am Med Dir Assoc. 21:300–307.
2020.PubMed/NCBI View Article : Google Scholar
|
|
11
|
Ignacio de Ulíbarri J, González-Madroño A,
de Villar NG, González P, González B, Mancha A, Rodríguez F and
Fernández G: CONUT: A tool for controlling nutritional status.
First validation in a hospital population. Nutr Hosp. 20:38–45.
2005.PubMed/NCBI
|
|
12
|
Agachan F, Chen T, Pfeifer J, Reissman P
and Wexner SD: A constipation scoring system to simplify evaluation
and management of constipated patients. Dis Colon Rectum.
39:681–685. 1996.PubMed/NCBI View Article : Google Scholar
|
|
13
|
Furuta K, Ishihara S, Sato S, Miyake T,
Ishimura N, Koshino K, Tobita H, Moriyama I, Amano Y, Adachi K, et
al: Development and verification of the Izumo Scale, new
questionnaire for quality of life assessment of patients with
gastrointestinal symptoms. Nihon Shokakibyo Gakkai Zasshi.
106:1478–1487. 2009.PubMed/NCBI(In Japanese).
|
|
14
|
Lewis SJ and Heaton KW: Stool form scale
as a useful guide to intestinal transit time. Scand J
Gastroenterol. 32:920–944. 1997.PubMed/NCBI View Article : Google Scholar
|
|
15
|
Locke GR III, Pemberton JH and Phillips
SF: AGA technical review on constipation. American
Gastroenterological Association. Gastroenterology. 119:1766–1778.
2000.PubMed/NCBI View Article : Google Scholar
|
|
16
|
Bouras EP and Tangalos EG: Chronic
constipation in the elderly. Gastroenterol Clin North Am.
38:463–480. 2009.PubMed/NCBI View Article : Google Scholar
|
|
17
|
Kepenekci I, Keskinkilic B, Akinsu F,
Cakir P, Elhan AH, Erkek AB and Kuzu MA: Prevalence of pelvic floor
disorders in the female population and the impact of age, mode of
delivery, and parity. Dis Colon Rectum. 54:85–94. 2011.PubMed/NCBI View Article : Google Scholar
|
|
18
|
Dimpfl T, Jaeger C, Mueller-Felber W,
Anthuber C, Hirsch A, Brandmaier R and Schuessler B: Myogenic
changes of the levator ani muscle in premenopausal women: The
impact of vaginal delivery and age. Neurourol Urodyn. 17:197–205.
1998.PubMed/NCBI View Article : Google Scholar
|
|
19
|
Hanani M, Fellig Y, Udassin R and Freund
HR: Age-related changes in the morphology of the myenteric plexus
of the human colon. Auton Neurosci. 113:71–78. 2004.PubMed/NCBI View Article : Google Scholar
|
|
20
|
Bassotti G, Villanacci V, Creţoiu D,
Creţoiu SM and Becheanu G: Cellular and molecular basis of chronic
constipation: Taking the functional/idiopathic label out. World J
Gastroenterol. 19:4099–4105. 2013.PubMed/NCBI View Article : Google Scholar
|
|
21
|
Kwon YN and Yoon SS: Sarcopenia:
Neurological point of view. J Bone Metab. 24:83–89. 2017.PubMed/NCBI View Article : Google Scholar
|
|
22
|
Kawamura Y, Yamamoto S, Funaki Y, Ohashi
W, Yamamoto K, Ozeki T, Yamaguchi Y, Tamura Y, Izawa S, Hijikata Y,
et al: Internet survey on the actual situation of constipation in
the Japanese population under 70 years old: Focus on functional
constipation and Constipation-predominant irritable bowel syndrome.
J Gastroenterol. 55:27–38. 2020.PubMed/NCBI View Article : Google Scholar
|
|
23
|
Tanabe A, Adachi K, Yamaguchi Y, Izawa S,
Yamamoto S, Hijikata Y, Ebi M, Funaki Y, Ogasawara N, Goto C, et
al: Gut Environment and dietary habits in healthy japanese adults
and their association with bowel movement. Digestion. 21:1–11.
2019.PubMed/NCBI View Article : Google Scholar
|