1. Introduction
Nosocomial or hospital-acquired pneumonia (HAP) is
an infection that appears during a hospital stay, usually 48 h or
more after being admitted or within 14 days of discharge and was
either absent or not incubating at the time of admission (1). HAP is the second most frequent
nosocomial infection following urinary tract infections, with an
incidence of 15-20%, according to a study from the United States
(2). It is one of the primary
causes of mortality in intensive care unit (ICU) patients
(accounting for 25-50% of deaths) (1) and one of the causes of fatal hospital
infections (mortality rate, 13%). Mechanical ventilation for >48
h (HAP incidence, 9-40%), length of hospital stay (HAP incidence,
3.3% until day 5; 1.3% at day 15), severity of underlying disease,
Acute Physiology and Chronic Health Evaluation (APACHE) score
(3), and the presence of
comorbidities are the most important risk factors (4).
Hospitalized patients with central nervous system
(CNS) injuries are particularly vulnerable to pneumonia, which can
be exacerbated by bed rest, dysphagia, mental instability, or
mechanical ventilation brought on by weak respiratory muscles
(5). Pneumonia is one of the most
common respiratory complications in stroke patients, affecting 5 to
9% of patients (6,7), and is much commoner in patients
admitted to neuro-ICUs, which are ICUs devoted to the care of
patients with immediately life-threatening neurological problems
(incidence, 13-33%) (8). Due to the
long time spent in the prone position and the risk of inhaling
stomach contents that comes with it, a large number of people (up
to 60%) with serious brain injuries develop pneumonia (9).
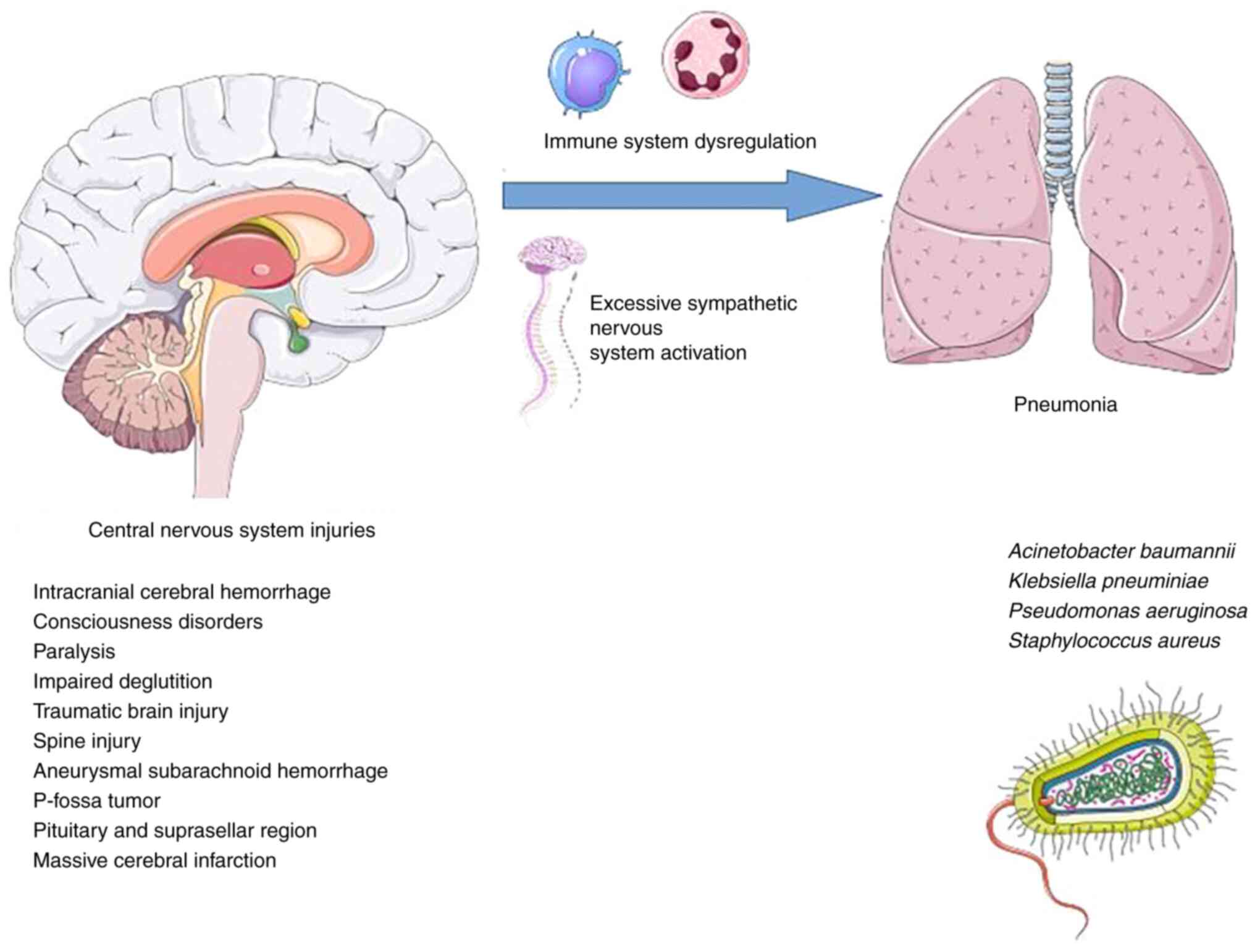
Immune system dysregulation due to persistent
inflammatory response and excessive sympathetic activation are
involved in the pathogenesis of pneumonia in individuals with CNS
injuries. More specifically, in CNS injuries, secondary brain
tissue damage is caused by the acute immune response, which is
followed by immunosuppression caused by sympathetic nervous system
activation. The latter raises the risk of infectious complications
such as pneumonia. The inflammatory state caused by pneumonia can
trigger a bystander autoimmune response against CNS antigens,
resulting in a vicious cycle (10).
Nosocomial pneumonia affects ~36% of patients
hospitalized for >48 h in neuro-ICUs (11). Other common infections in neuro-ICUs
are urinary tract infections, bacteremia, and intracranial
infections such as ventriculitis and meningitis (11). These infections can affect patient
outcomes and increase mortality rates in critically ill patients.
In addition, these infections increase the costs placed on
healthcare systems (12,13).
Among the most frequent types of infections in
patients admitted to neuro-ICUs is ventilator-associated pneumonia
(VAP), which appears in mechanically ventilated individuals at
least 48 h after endotracheal intubation without any signs of a
prior infection. It usually results from aspiration of
oropharyngeal secretions into the tracheobronchial tree around the
endotracheal cuff (14).
Subarachnoid hemorrhage (SAH), traumatic brain injury (TBI), and
stroke patients all require intensive care and may be admitted to
neuro-ICUs, where they may be vulnerable to nosocomial infections
such as pneumonia. Patients with subdural hematomas and
intracerebral/intraventricular hemorrhages (IVH) have the greatest
incidence rates of nosocomial infections, with rates of 21.3 and
21.1 cases per 1,000 days of hospitalization at the neuro-ICU,
respectively (15).
Multidrug-resistant (MDR) microorganisms are defined
as those that are resistant to at least one agent from three or
more antimicrobial classes, including β-lactam/β-lactamase
inhibitors; carbapenems; aminoglycosides; third- or
fourth-generation cephalosporins, fluoroquinolones, and carbapenems
for Gram-negative pathogens; non-susceptibility to oxacillin and/or
cefoxitin (anti-staphylococcal β-lactams) for Gram-positive
Staphylococcus aureus (S. aureus); and
non-susceptibility to vancomycin and/or teicoplanin for
Gram-positive Enterococcus spp. (16,17).
MDR microorganisms are a prevalent and serious
concern with increased mortality in HAP and VAP (18). There is a scarcity of information on
pneumonia due to MDR pathogens in patients with CNS injuries. The
aim of the present review was to report the current evidence
regarding pneumonia due to MDR pathogens in patients with CNS
injuries.
2. Data extraction and synthesis
In order to provide insight regarding MDR pneumonia
in patients with CNS injuries, an electronic search in PubMed and
Google Scholar was performed with the keywords ‘multi-drug
resistant pneumonia’ OR ‘MDR pneumonia’ OR ‘multi-drug resistant
respiratory infections’ OR ‘MDR respiratory infections’ AND
‘central nervous injuries’ OR ‘brain injuries’ OR ‘stroke’ OR
‘intracranial hemorrhage’ OR ‘subarachnoid hemorrhage’ OR
‘neurorehabilitation unit’ OR ‘neurointensive care unit’ OR
‘neurological disorders’ OR ‘neurological injuries’, without
language limitations in the selection of articles reporting data on
MDR pneumonia in CNS injuries. Two authors thoroughly reviewed all
articles. The reference list of each article that met the criteria
was also hand-searched for other potentially relevant studies.
Overall, 192 articles were found using the search criteria and the
reference lists of previously identified documents. After
eliminating duplicates, 119 were eliminated after title, abstract,
or full text screening. Finally, nine articles presenting original
studies providing data on MDR pneumonia in CNS injuries were
included in data synthesis.
3. Mechanisms responsible for pneumonia
development in CNS injuries
Critical illnesses of the CNS are more likely to
result in pneumonia than in other illnesses in ICUs due to factors
such as immunological dysregulation and immunosuppression resulting
from brain injury, increased incidence of dysphagia, and the
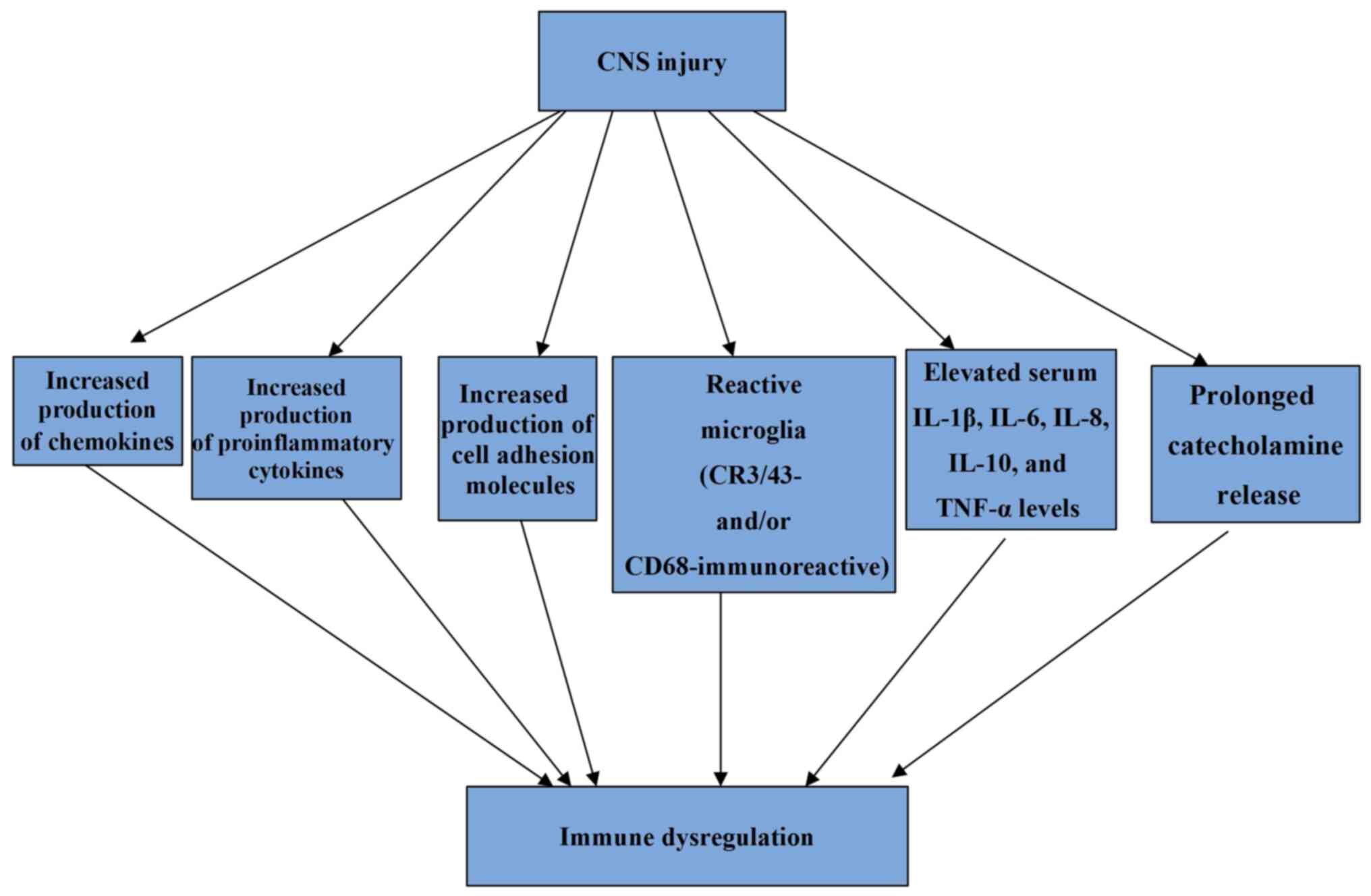
insertion of external ventricular drains (EVDs) (19). In patients with brain damage,
immunological dysregulation is predominantly caused by a heightened
inflammatory response that results in the production of chemokines,
proinflammatory cytokines, and cell adhesion molecules both
centrally and peripherally (20).
These cytokines are produced to eliminate cellular debris in the
CNS after injury, and an inflammatory response develops. However, a
persistent and protracted inflammatory response can result in
immune system dysregulation (21-23).
More specifically, it has been found that three months after TBI,
affected individuals frequently display extensive, densely packed,
reactive microglia (CR3/43- and/or CD68-immunoreactive) and in the
context of this inflammatory pathology, evidence of ongoing white
matter degradation has also been observed (21). There is also evidence that increased
microglial activation can be present up to 17 years after TBI
(23). Moreover, TBI could be
viewed as a condition with a persistent inflammatory state as
elevated serum interleukin (IL)-1β, IL-6, IL-8, IL-10, and TNF-α
levels over the first year post-injury have been detected (22).
The terms brain injury-induced immunodepression
syndrome (BIIDS) and stroke-induced immunodepression syndrome
(SIDS) refer to dysregulation occurring as a result of trauma,
brain surgery, spinal cord injury (SCI), or SAH (23-25).
SIDS is thought to have two phases. The early transitory activation
of the first phase begins as soon as 12 h after the first injury
and lasts for up to 24 h. The second phase is characterized by a
systemic immunodepression that can last for many weeks (26-28).
Immunosuppression also develops from prolonged
catecholamine release. Catecholamines are released after a brain
injury because the hypothalamic-pituitary axis and sympathetic
nervous system are engaged. Inflammatory response, as previously
stated (29-31),
can also be brought on by this. Additionally, the reaction is also
mediated by 2-adrenergic receptors (32). In patients with brain injuries,
infections are strongly correlated with increased sympathetic
system activity, elevated catecholamine levels, and
immunosuppression (33-35).
According to previous research (36), putamen and right frontal injuries
render patients more vulnerable to infections. Due to their link to
excessive sympathetic activation, which directly promotes cardiac
and vascular alterations and leads to increased vigilance, heart
rate, and blood flow to the skeletal muscles, insular brain strokes
are associated with the highest risk of pneumonia (37).
The mechanisms responsible for pneumonia development
in CNS injuries are illustrated in Fig.
1 and the mechanisms involved in immune system dysregulation
caused by CNS injuries are illustrated in Fig. 2.
4. Prevalence of pneumonia due to MDR
pathogens in CNS injuries
All the studies providing data regarding pneumonia
due to MDR pathogens in CNS injuries are summarized in Table I (38-45).
Regarding patients with TBI and pneumonia, the prevalence of MDR
pneumonia ranges between 5.4 and 29.6%, according to different
studies (39,40). In a study by Yang et al of
the 324 patients with intracranial cerebral hemorrhage, 122
developed pneumonia, of whom 42 (34.2%) had MDR pathogen isolation
(41). The reported incidence of
MDR pneumonia among patients with various CNS injuries and
pneumonia ranges between 8.5 and 42.2% (42,43).
In a previous study including 89 patients with subarachnoid
hemorrhage, intracerebral hemorrhage, and massive cerebral
infarction, Teng et al found that among 40 patients who
developed pneumonia, 15 (37.5%) had MDR pathogens (44).
 | Table IStudies describing patients with CNS
injuries and pneumonia due to MDR pathogens. |
Table I
Studies describing patients with CNS
injuries and pneumonia due to MDR pathogens.
| Study | CNS injury | Participants | Pneumonia | Pneumonia due to
MDR pathogens | MDR pathogens |
|---|
| Yang et al,
2022(41) | Intracranial
cerebral hemorrhage | 324 | 122 | 42/122 (34.2%) | A. baumannii
(40.5%) |
| | | | | | K.
pneumoniae (26.2%) |
| | | | | | P.
aeruginosa (23.8%) |
| Jiang et al,
2022(45) | • Consciousness
disorders | 575 | 427 | 79/427 (18.5%) | A. baumannii
(45.3%) |
| | • Paralysis | | | | P.
aeruginosa (36.8%) |
| | • Impaired
deglutition | | | | K.
pneumoniae (12.6%) |
| | | | | | E. cloacae
(1.1%) |
| | | | | | S. aureus
(4.2%) |
| Lee et al,
2019(42) | Various CNS
illnesses | 277 | 351 | 148/351
(42.2%) | A. baumannii
(23.6%) |
| | | | | | S.
pneumoniae (5.4%) |
| | | | | | P.
aeruginosa (4%) |
| | | | | | K.
pneumoniae (14.9%) |
| | | | | | K. aerogenes
(1.4%) |
| | | | | | S. aureus
(45.3%) |
| Shrestha et
al, 2019(43) | • Traumatic brain
injury | 106 | 35 | 3/35 (8.5%) | K.
pneumoniae (66.7%) |
| | • Spine injury | | | | Acinetobacter
spp. (33.3%) |
| | • Aneurysmal
SAH | | | | |
| | •
Miscellaneous | | | | |
| | • P-fossa
tumor | | | | |
| | • Pituitary and
suprasellar region | | | | |
| Beghi et al,
2018(4) | Traumatic brain
injury | 61 | 8 | 6/8 (75%) | P.
aeruginosa (33.3%) |
| | | | | | K.
pneumoniae (16.6%) |
| | | | | | P. mirabilis
(16.6%) |
| | | | | | S.
maltophilia (16.6%) |
| | | | | |
Methicillin-resistant
coagulase-negative |
| | | | | |
Staphylococci (16.6%) |
| Ye et al,
2022(40) | Traumatic brain
injury | 230 | 230 | 68/230 (29.6%) | A. baumannii
(45.2%) |
| | | | | | K.
pneumoniae (23.3%) |
| | | | | | P.
aeruginosa (16.4%) |
| | | | | | S. aureus
(15.1%) |
| Leone et al,
2002(39) | Traumatic brain
injury | 116 | 58 | 4/73 (5.4%) | S. aureus
(100%) |
| Teng et al,
2022(44) | • SAH | 89 | 40 | 15/40 (37.5%) | S. aureus
(20%) |
| | • Intracerebral
hemorrhage | | | | B. cepacia
(20%) |
| | • Massive cerebral
infarction | | | | K.
pneumoniae (20%) |
| | | | | | C. striatum
(20%) |
| | | | | | Acinetobacter
spp (20%) |
| Jovanovic et
al, 2015(38) | Traumatic brain
injury | 144 | 35 | 6/107 (5.6%) | S. aureus
(100%) |
In a study by Beghi et al which included 61
individuals with TBI, 8 patients developed pneumonia in a
rehabilitation unit, of whom 6 (75%) had an MDR pathogen isolation
(4). In addition, Jiang et
al in a recent study of 575 patients with consciousness
disorders, paralysis, and impaired deglutition who were admitted to
a rehabilitation unit, recorded 427 episodes of pneumonia, of which
79 (18.5%) were MDR pneumonia (45).
5. Risk factors for pneumonia due to MDR
pathogens in CNS injuries
Given the worsening patient outcomes and the
significant expenses affecting the healthcare system as a result of
greater lengths of stay and prolonged duration of treatment, it is
critical to be able to identify which patients are at higher risk
of developing pneumonia due to MDR pathogens.
Patients with TBI acquire nosocomial infections at a
rate of 41%, with pneumonia being the most frequent, with a
prevalence rate of ≥30% (45).
Surgical procedures, prolonged hospitalization, CNS injury, CSF
leak, administration of barbiturates, nasal carriage of S. aureus,
and the necessity for intubation and mechanical ventilation have
all been found to play a significant role in pneumonia development
in these patients (46).
Furthermore, patients with the following features had a higher risk
of developing pneumonia: Intubation on the scene or in the
emergency department; younger age; lower Glasgow Coma Scale (GCS)
score; males; prolonged mechanical ventilation; higher injury
severity score (ISS), and additional brain injuries (47). Table
II summarizes identified risk factors for pneumonia due to MDR
pathogens in CNS injuries as well as their prevalence in cases of
pneumonia due to MDR pathogens among various studies (40,42-45).
| Table IIIdentified risk factors for MDR
pneumonia in CNS injuries. |
Table II
Identified risk factors for MDR
pneumonia in CNS injuries.
| Study | Type of CNS
injury | Identified risk
factors |
|---|
| Ye et al,
2022(40) | Traumatic brain
injury | Age >60 years
(67.4%) |
| | | Diabetes mellitus
(45.7%) |
| | | Chronic obstructive
pulmonary disease (34.8%) |
| | | Mechanical
ventilation ≥7 days (69.6%) |
| | | Transfer from other
hospitals (17.4%) |
| Lee et al,
2019(42) | Various CNS
injuries | Risk factors for
MDR i.e., antimicrobial agent use in the previous 90 days,
hospitalization for 2 days in the previous 90 days, nursing home
residency (61.6%) |
| Shrestha et
al, 2019(43) | Various CNS
injuries | Head injury
(45.7%) |
| | | Spine injury
(20%) |
| Teng et al,
2022(44) | Subarachnoid
hemorrhage | Age >65 years
(57.5%) |
| | Intracerebral
hemorrhage | Therapeutic
hypothermia (32.5%) |
| | Massive cerebral
infarction | |
| Jiang et al,
2022(45) | Hospitalization in
neurorehabilitation units | Recent antibiotic
exposure (100%) |
| | | Low albumin level
(52.1%) |
| | | Performance of
tracheostomy (25%) |
6. Microbiological data
Common microorganisms involved in pneumonia due to
MDR pathogens in CNS injuries are presented in Table I.
Rare causes of pneumonia in immunocompromised
patients may include microorganisms which may rarely be encountered
in immunocompetent patients (48).
For example, cases of severe invasive infections such as pneumonia
due to C. striatum may occur especially among
immunocompromised patients who have a history of long hospital
admissions, numerous courses of antibiotics, and/or those who have
used invasive medical devices (49,50).
According to some studies, Corynebacterium spp. should also
be considered as potential pathogens, and suspicious isolates
should be identified to the species level since C. striatum
is frequently MDR (51,52).
Regarding Gram-positive MDR pathogens, of great
interest is a study that examined the proportion of MDR of common
bacteria isolated from hospitalized neurology patients with
pneumonia in ICU and non-ICU settings, between the early and late
years of the period 2007-2016. The prevalence of MDR among
infections caused by S. aureus and S. pneumoniae did
not differ significantly between the early and late study periods.
S. pneumoniae exhibited sensitivity to penicillin,
ceftriaxone and levofloxacin, especially during the late study
period and resistance to tetracycline, erythromycin and
trimethoprim-sulfamethoxazole. S. aureus exhibited
sensitivity to vancomycin, quinupristin/dalfopristin,
chloramphenicol, rifampicin and teicoplanin and resistance to
clindamycin, ciprofloxacin, moxifloxacin, tetracycline,
erythromycin and trimethoprim-sulfamethoxazole during the early and
the late study period (42). In a
study by Shrestha et al including patients with various CNS
injuries with MDR VAP, all Gram-positive pathogens were sensitive
to co-trimoxazole (43).
In a study by Lee et al (42), both the ICU and non-ICU settings
have experienced an increase in the proportion of cases with
Gram-negative bacteria that are resistant to various antibiotics
and in both settings, the percentage of non-susceptibility to
amikacin and colistin remained low between the early and late years
of the period 2007-2016(42). In
the study by Shrestha et al all Gram-negative bacterial
strains were sensitive to colistin (43). Gram-negative organisms have recently
been reported to be dominant in neurorehabilitation ward patients,
with Acinetobacter baumannii (A. baumannii) being
almost universally resistant to ciprofloxacin, imipenem,
piperacillin, piperacillin/tazobactam and meropenem and
Klebsiella pneumoniae (K. pneumoniae) being resistant
to numerous antibiotics, except tigecycline,
cefoperazone/sulbactam, sulfonamide, cefepime, and
piperacillin/tazobactam (44).
7. Imaging data
Imaging data on patients with pneumonia due to MDR
pathogens and CNS injuries is limited. A study investigating the
pathogen distribution and imaging characteristics in patients with
severe craniocerebral injuries with pneumonia due to MDR pathogens
reported that the imaging features included consolidation, pleural
effusion, and ground-glass opacities accounting for 63.24, 72.06
and 45.59%, respectively (40).
8. Prevention
In the neuro-ICU, proposed VAP prevention strategies
include daily sedation interruption and a readiness-to-extubate
evaluation; facilitation of early morbidity, elevating the head of
the bed to 30-45˚; utilization of endotracheal tubes with
subglottic secretion drainage ports and a closed/in-line
endotracheal suctioning system; substituting the ventilator circuit
if visibly soiled or malfunctioning; monitoring of residual gastric
volume; early parenteral nutrition; and deep venous thrombosis
prophylaxis (38). Other suggested
preventive measures for VAP include antiseptic mouth wash,
spontaneous breathing trial, and early extubation (15).
In addition, comprehensive rehabilitation
approaches, including secretion management, training of respiratory
muscles, airway clearance techniques, swallowing exercises, and
pharyngeal electrical stimulation have been suggested for
tracheotomized patients in neurorehabilitation units for the
prevention of infections (47).
Moreover, short-duration, high-dose antibiotic regimens appear to
be effective in reducing the risk of antibiotic resistance
(41).
An additional prevention approach is addressing
brain injury-induced immunosuppression, which is mainly induced by
sympathetic nervous system activation (53). With regard to microorganism
infection in humans, the human host immunity response must be taken
into account. Owing to the host immune defenses, most of the viral
and bacterial infections are self-limiting to an immunocompetent
host (54), and the microorganisms
become commensal microorganisms if they can co-exist with human
beings. In addition as indicated, MDR only becomes a significant
issue when there is immunological dysregulation and
immunosuppression in the host. Thus, eliminating immunological
dysregulation and immunosuppression in patients with CNS injuries
may provide a more feasible therapeutic solution than targeting MDR
microorganisms and eliminating these microorganisms.
The pivotal role of immunity in acquiring essential
nutrition from the human microbiota (55-57)
should also be considered. The human microbiome is essential to the
health and wellbeing of individuals, as they are the indispensable
source of metabolites for the body (57). In the case of acute infection, with
the help of a special pathway of the innate immune defense,
programmed cell death, such as apoptosis, necroptosis, and
pyroptosis (58,59), both the microorganisms and damaged
host cells will be destroyed and become a source of nutrition for
healing.
By using these preventive strategies, the reduction
of all pulmonary infections will result in the reduction of
pneumonia caused by MDR bacteria.
9. Conclusions
The incidence of pneumonia due to MDR pathogens in
CNS injuries varies among different settings, underlying injuries,
and countries in which the studies were performed. Certain risk
factors for the development of MDR pneumonia in ICUs and in
neurorehabilitation units have been identified. The most frequently
isolated microorganisms in pneumonia due to MDR pathogens in CNS
injuries are A. baumannii, K. pneumoniae,
Pseudomonas aeruginosa, and S. aureus with various
patterns of resistance. The application of preventive strategies
and the early detection and close monitoring of MDR strains may
reduce the burden of antimicrobial resistance, which is now a
global issue. Further multicenter prospective studies are needed to
provide data on the clinical characteristics and outcomes of these
patients as the data concerning these issues are limited.
Acknowledgements
Not applicable.
Funding
Funding: No funding was received.
Availability of data and materials
Not applicable.
Authors' contributions
AG and VEG conceptualized the study. VEG, AAF, IT,
GF, KF, KP and NT reviewed the data for inclusion in the review,
and wrote and prepared the draft of the manuscript. VEG and GF
provided critical revisions. Data authentication is not applicable.
All authors contributed to manuscript revision and have read and
approved the final version of the manuscript.
Ethics approval and consent to
participate
Not applicable.
Patient consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Kalil AC, Metersky ML, Klompas M,
Muscedere J, Sweeney DA, Palmer LB, Napolitano LM, O'Grady NP,
Bartlett JG, Carratalà J, et al: Management of adults with
hospital-acquired and ventilator-associated pneumonia: 2016
clinical practice guidelines by the infectious diseases society of
America and the American Thoracic Society. Clin Infect Dis.
63:e61–e111. 2016.PubMed/NCBI View Article : Google Scholar
|
|
2
|
Magill SS, O'Leary E, Janelle SJ, Thompson
DL, Dumyati G, Nadle J, Wilson LE, Kainer MA, Lynfield R, Greissman
S, et al: Changes in prevalence of health care-associated
infections in U.S. Hospitals. N Engl J Med. 379:1732–1744.
2018.PubMed/NCBI View Article : Google Scholar
|
|
3
|
Knaus WA, Draper EA, Wagner DP and
Zimmerman JE: APACHE II: A severity of disease classification
system. Crit Care Med. 13:818–829. 1985.PubMed/NCBI
|
|
4
|
Beghi G, De Tanti A, Serafini P, Bertolino
C, Celentano A and Taormina G: Monitoring of Hospital acquired
pneumonia in patients with severe brain injury on first access to
intensive neurological rehabilitation: First year of observation.
Monaldi Arch Chest Dis. 88(888)2018.PubMed/NCBI View Article : Google Scholar
|
|
5
|
Zhang X, Xiao L, Niu L, Tian Y and Chen K:
Comparison of six risk scores for stroke-associated pneumonia in
patients with acute ischemic stroke: A systematic review and
Bayesian network meta-analysis. Front Med (Lausanne).
9(964616)2022.PubMed/NCBI View Article : Google Scholar
|
|
6
|
Finlayson O, Kapral M, Hall R, Asllani E,
Selchen D and Saposnik G: Canadian Stroke Network; Stroke Outcome
Research Canada (SORCan) Working group. Risk factors, inpatient
care, and outcomes of pneumonia after ischemic stroke. Neurology.
77:1338–1345. 2011.PubMed/NCBI View Article : Google Scholar
|
|
7
|
Ingeman A, Andersen G, Hundborg HH,
Svendsen ML and Johnsen SP: In-hospital medical complications,
length of stay, and mortality among stroke unit patients. Stroke.
42:3214–3218. 2011.PubMed/NCBI View Article : Google Scholar
|
|
8
|
Juan W, Zhen H, Yan-Ying F, Hui-Xian Y,
Tao Z, Pei-Fen G and Jian-Tian H: A comparative study of two tube
feeding methods in patients with dysphagia after stroke: A
randomized controlled trial. J Stroke Cerebrovasc Dis.
29(104602)2020.PubMed/NCBI View Article : Google Scholar
|
|
9
|
Lee K and Rincon F: Pulmonary
complications in patients with severe brain injury. Crit Care Res
Pract. 2012(207247)2012.PubMed/NCBI View Article : Google Scholar
|
|
10
|
Winklewski PJ, Radkowski M and Demkow U:
Cross-talk between the inflammatory response, sympathetic
activation and pulmonary infection in the ischemic stroke. J
Neuroinflammation. 11(213)2014.PubMed/NCBI View Article : Google Scholar
|
|
11
|
Busl KM: Healthcare-associated infections
in the neurocritical care unit. Curr Neurol Neurosci Rep.
19(76)2019.PubMed/NCBI View Article : Google Scholar
|
|
12
|
Chacón-Aponte AA, Durán-Vargas ÉA,
Arévalo-Carrillo JA, Lozada-Martínez ID, Bolaño-Romero MP,
Moscote-Salazar LR, Grille P and Janjua T: Brain-lung interaction:
A vicious cycle in traumatic brain injury. Acute Crit Care.
37:35–44. 2022.PubMed/NCBI View Article : Google Scholar
|
|
13
|
Gonçalves B, Rynkowski C, Turon R, Charris
N, Miranda F, de Caro V, Prazeres M, Santos T, Greer DM, Sharshar
T, et al: Clinical characteristics and outcomes of patients with
aneurysmal subarachnoid hemorrhage: A prospective multicenter study
in a middle-income country. Neurocrit Care: Nov 2, 2022. doi:
10.1007/s12028-022-01629-6 (Epub ahead of print).
|
|
14
|
Rafa E, Kołpa M, Wałaszek MZ, Domański A,
Wałaszek MJ, Różańska A and Wójkowska-Mach J: Healthcare-Acquired
infection surveillance in neurosurgery patients, incidence and
microbiology, five years of experience in two polish units. Int J
Environ Res Public Health. 19(7544)2022.PubMed/NCBI View Article : Google Scholar
|
|
15
|
Abulhasan YB, Rachel SP, Châtillon-Angle
MO, Alabdulraheem N, Schiller I, Dendukuri N, Angle MR and Frenette
C: Healthcare-associated infections in the neurological intensive
care unit: Results of a 6-year surveillance study at a major
tertiary care center. Am J Infect Control. 46:656–662.
2018.PubMed/NCBI View Article : Google Scholar
|
|
16
|
Magiorakos AP, Srinivasan A, Carey RB,
Carmeli Y, Falagas ME, Giske CG, Harbarth S, Hindler JF, Kahlmeter
G, Olsson-Liljequist B, et al: Multidrug-resistant, extensively
drug-resistant and pandrug-resistant bacteria: An international
expert proposal for interim standard definitions for acquired
resistance. Clin Microbiol Infect. 18:268–281. 2012.PubMed/NCBI View Article : Google Scholar
|
|
17
|
Marston HD, Dixon DM, Knisely JM, Palmore
TN and Fauci AS: Antimicrobial resistance. JAMA. 316:1193–1204.
2016.PubMed/NCBI View Article : Google Scholar
|
|
18
|
Sfeir MM: Diagnosis of multidrug-resistant
pathogens of pneumonia. Diagnostics (Basel).
11(2287)2021.PubMed/NCBI View Article : Google Scholar
|
|
19
|
Lord AS, Nicholson J and Lewis A:
Infection prevention in the neurointensive care unit: A systematic
review. Neurocrit Care. 31:196–210. 2019.PubMed/NCBI View Article : Google Scholar
|
|
20
|
Le Thuc O, Blondeau N, Nahon JL and Rovère
C: The complex contribution of chemokines to neuroinflammation:
Switching from beneficial to detrimental effects. Ann N Y Acad Sci.
1351:127–140. 2015.PubMed/NCBI View Article : Google Scholar
|
|
21
|
Johnson VE, Stewart JE, Begbie FD,
Trojanowski JQ, Smith DH and Stewart W: Inflammation and white
matter degeneration persist for years after a single traumatic
brain injury. Brain. 136:28–42. 2013.PubMed/NCBI View Article : Google Scholar
|
|
22
|
Kumar RG, Boles JA and Wagner AK: Chronic
inflammation after severe traumatic brain injury: Characterization
and associations with outcome at 6 and 12 months postinjury. J Head
Trauma Rehabil. 30:369–381. 2015.PubMed/NCBI View Article : Google Scholar
|
|
23
|
Ramlackhansingh AF, Brooks DJ, Greenwood
RJ, Bose SK, Turkheimer FE, Kinnunen KM, Gentleman S, Heckemann RA,
Gunanayagam K, Gelosa G and Sharp DJ: Inflammation after trauma:
Microglial activation and traumatic brain injury. Ann Neurol.
70:374–383. 2011.PubMed/NCBI View Article : Google Scholar
|
|
24
|
Shim R and Wong CH: Ischemia,
immunosuppression and infection-tackling the predicaments of
post-stroke complications. Int J Mol Sci. 17(64)2016.PubMed/NCBI View Article : Google Scholar
|
|
25
|
Cui P, McCullough LD and Hao J: Brain to
periphery in acute ischemic stroke: Mechanisms and clinical
significance. Front Neuroendocrinol. 63(100932)2021.PubMed/NCBI View Article : Google Scholar
|
|
26
|
Chamorro A, Urra X and Planas AM:
Infection after acute ischemic stroke: A manifestation of
brain-induced immunodepression. Stroke. 38:1097–103.
2007.PubMed/NCBI View Article : Google Scholar
|
|
27
|
Chang L, Chen Y, Li J, Liu Z, Wang Z, Chen
J, Cao W and Xu Y: Cocaine-and amphetamine-regulated transcript
modulates peripheral immunity and protects against brain injury in
experimental stroke. Brain Behav Immun. 25:260–269. 2011.PubMed/NCBI View Article : Google Scholar
|
|
28
|
Offner H, Subramanian S, Parker SM,
Afentoulis ME, Vandenbark AA and Hurn PD: Experimental stroke
induces massive, rapid activation of the peripheral immune system.
J Cereb Blood Flow Metab. 26:654–665. 2006.PubMed/NCBI View Article : Google Scholar
|
|
29
|
Meisel C, Schwab JM, Prass K, Meisel A and
Dirnagl U: Central nervous system injury-induced immune deficiency
syndrome. Nat Rev Neurosci. 6:775–786. 2005.PubMed/NCBI View
Article : Google Scholar
|
|
30
|
Prass K, Braun JS, Dirnagl U, Meisel C and
Meisel A: Stroke propagates bacterial aspiration to pneumonia in a
model of cerebral ischemia. Stroke. 37:2607–2612. 2006.PubMed/NCBI View Article : Google Scholar
|
|
31
|
Wong CHY: Effects of stroke beyond the
brain. Nat Rev Immunol. 19(719)2019.PubMed/NCBI View Article : Google Scholar
|
|
32
|
Mracsko E, Liesz A, Karcher S, Zorn M,
Bari F and Veltkamp R: Differential effects of sympathetic nervous
system and hypothalamic-pituitary-adrenal axis on systemic immune
cells after severe experimental stroke. Brain Behav Immun.
41:200–209. 2014.PubMed/NCBI View Article : Google Scholar
|
|
33
|
Chamorro A, Amaro S, Vargas M, Obach V,
Cervera A, Gómez-Choco M, Torres F and Planas AM: Catecholamines,
infection, and death in acute ischemic stroke. J Neurol Sci.
252:29–35. 2007.PubMed/NCBI View Article : Google Scholar
|
|
34
|
Haeusler KG, Schmidt WU, Föhring F, Meisel
C, Helms T, Jungehulsing GJ, Nolte CH, Schmolke K, Wegner B, Meisel
A, et al: Cellular immunodepression preceding infectious
complications after acute ischemic stroke in humans. Cerebrovasc
Dis. 25:50–58. 2008.PubMed/NCBI View Article : Google Scholar
|
|
35
|
Klehmet J, Harms H, Richter M, Prass K,
Volk HD, Dirnagl U, Meisel A and Meisel C: Stroke-induced
immunodepression and post-stroke infections: Lessons from the
preventive antibacterial therapy in stroke trial. Neuroscience.
158:1184–1193. 2009.PubMed/NCBI View Article : Google Scholar
|
|
36
|
Pluta R, Januszewski S and Czuczwar SJ:
Neuroinflammation in Post-ischemic neurodegeneration of the brain:
Friend Foe or Both? Int J Mol Sci. 22(4405)2021.PubMed/NCBI View Article : Google Scholar
|
|
37
|
Walter U, Kolbaske S, Patejdl R,
Steinhagen V, Abu-Mugheisib M, Grossmann A, Zingler C and Benecke
R: Insular stroke is associated with acute sympathetic
hyperactivation and immunodepression. Eur J Neurol. 20:153–159.
2013.PubMed/NCBI View Article : Google Scholar
|
|
38
|
Jovanovic B, Milan Z, Markovic-Denic L,
Djuric O, Radinovic K, Doklestic K, Velickovic J, Ivancevic N,
Gregoric P, Pandurovic M, et al: Risk factors for
ventilator-associated pneumonia in patients with severe traumatic
brain injury in a Serbian trauma centre. Int J Infect Dis.
38:46–51. 2015.PubMed/NCBI View Article : Google Scholar
|
|
39
|
Leone M, Bourgoin A, Giuly E, Antonini F,
Dubuc M, Viviand X, Albanèse J and Martin C: Influence on outcome
of ventilator-associated pneumonia in multiple trauma patients with
head trauma treated with selected digestive decontamination. Crit
Care Med. 30:1741–1746. 2002.PubMed/NCBI View Article : Google Scholar
|
|
40
|
Ye YQ, He LL, Liu GL, Zhang J and Long LS:
Pathogen distribution, imaging characteristics, and establishment
and verification of risk prediction model of pulmonary infection
with multi-drug resistant organism in patients with severe
craniocerebral injury. Zhongguo Yi Xue Ke Xue Yuan Xue Bao.
44:636–642. 2022.PubMed/NCBI View Article : Google Scholar : (In Chinese).
|
|
41
|
Yang H, Fan Y, Li C, Zhang M and Liu W: A
retrospective study on risk factors and disease burden for
Hospital-acquired pneumonia caused by multi-drug-resistant bacteria
in patients with intracranial cerebral hemorrhage. Neurol Sci.
43:2461–2467. 2022.PubMed/NCBI View Article : Google Scholar
|
|
42
|
Lee HS, Moon J, Shin HR, Ahn SJ, Kim TJ,
Jun JS, Lee ST, Jung KH, Park KI, Jung KY, et al: Pneumonia in
Hospitalized neurologic patients: Trends in pathogen distribution
and antibiotic susceptibility. Antimicrob Resist Infect Control.
8(25)2019.PubMed/NCBI View Article : Google Scholar
|
|
43
|
Shrestha DK, Rajbhandari B, Pradhanang A,
Sedain G, Shilpakar SK and Pradhan S: Ventilator-associated
pneumonia in neurosurgical patients: A tertiary care center study.
J Inst Med. 41:40–44. 2019.
|
|
44
|
Teng G, Wang N, Nie X, Zhang L and Liu H:
Analysis of risk factors for early-onset ventilator-associated
pneumonia in a neurosurgical intensive care unit. BMC Infect Dis.
22(66)2022.PubMed/NCBI View Article : Google Scholar
|
|
45
|
Jiang W, Li L, Wen S, Song Y, Yu L and Tan
B: Gram-negative multidrug-resistant organisms were dominant in
neurorehabilitation ward patients in a general Hospital in
southwest China. Sci Rep. 12(11087)2022.PubMed/NCBI View Article : Google Scholar
|
|
46
|
Kourbeti IS, Vakis AF, Ziakas P,
Karabetsos D, Potolidis E, Christou S and Samonis G: Infections in
patients undergoing craniotomy: Risk factors associated with
post-craniotomy meningitis. J Neurosurg. 122:1113–119.
2015.PubMed/NCBI View Article : Google Scholar
|
|
47
|
Kesinger MR, Kumar RG, Wagner AK, Puyana
JC, Peitzman AP, Billiar TR and Sperry JL: Hospital-acquired
pneumonia is an independent predictor of poor global outcome in
severe traumatic brain injury up to 5 years after discharge. J
Trauma Acute Care Surg. 78:396–402. 2015.PubMed/NCBI View Article : Google Scholar
|
|
48
|
Shi MM, Monsel A, Rouby JJ, Xu YP, Zhu YG
and Qu JM: Inoculation pneumonia caused by coagulase negative
Staphylococcus. Front Microbiol. 10(2198)2019.PubMed/NCBI View Article : Google Scholar
|
|
49
|
Silva-Santana G, Silva CMF, Olivella JGB,
Silva IF, Fernandes LMO, Sued-Karam BR, Santos CS, Souza C and
Mattos-Guaraldi AL: Worldwide survey of Corynebacterium striatum
increasingly associated with human invasive infections, nosocomial
outbreak, and antimicrobial multidrug-resistance, 1976-2020. Arch
Microbiol. 203:1863–1880. 2021.PubMed/NCBI View Article : Google Scholar
|
|
50
|
Clariot S, Constant O, Lepeule R, Fihman
V, Razazi K, Cook F, Attias A, Merle JC, Hemery F, Levesque E, et
al: Clinical relevance and impact of Corynebacterium isolation in
lower respiratory tract of critically ill patients requiring
mechanical ventilation. Infection. 48:413–420. 2020.PubMed/NCBI View Article : Google Scholar
|
|
51
|
Milosavljevic MN, Milosavljevic JZ,
Kocovic AG, Stefanovic SM, Jankovic SM, Djesevic M and Milentijevic
MN: Antimicrobial treatment of Corynebacterium striatum invasive
infections: A systematic review. Rev Inst Med Trop Sao Paulo.
63(e49)2021.PubMed/NCBI View Article : Google Scholar
|
|
52
|
Shariff M, Aditi A and Beri K:
Corynebacterium striatum: An emerging respiratory pathogen. J
Infect Dev Ctries. 12:581–586. 2018.PubMed/NCBI View Article : Google Scholar
|
|
53
|
Erfani Z, Jelodari Mamaghani H, Rawling
JA, Eajazi A, Deever D, Mirmoeeni S, Azari Jafari A and Seifi A:
Pneumonia in nervous system injuries: An analytic review of
literature and recommendations. Cureus. 14(e25616)2022.PubMed/NCBI View Article : Google Scholar
|
|
54
|
Levin BR, Baquero F, Ankomah PP and McCall
IC: Phagocytes, antibiotics, and self-limiting bacterial
infections. Trends Microbiol. 25:878–892. 2017.PubMed/NCBI View Article : Google Scholar
|
|
55
|
Georgakopoulou VE, Mantzouranis K,
Damaskos C, Karakou E, Melemeni D, Mermigkis D, Petsinis G,
Sklapani P, Trakas N and Tsiafaki X: Correlation between serum
levels of 25-Hydroxyvitamin D and severity of community-acquired
pneumonia in hospitalized patients assessed by pneumonia severity
index: An observational descriptive study. Cureus.
12(e8947)2020.PubMed/NCBI View Article : Google Scholar
|
|
56
|
Yu L: Restoring good health in elderly
with diverse gut microbiome and food intake restriction to combat
COVID-19. Indian J Microbiol. 61:104–107. 2021.PubMed/NCBI View Article : Google Scholar
|
|
57
|
McFall-Ngai M, Hadfield MG, Bosch TC,
Carey HV, Domazet-Lošo T, Douglas AE, Dubilier N, Eberl G, Fukami
T, Gilbert SF, et al: Animals in a bacterial world, a new
imperative for the life sciences. Proc Natl Acad Sci USA.
110:3229–3236. 2013.PubMed/NCBI View Article : Google Scholar
|
|
58
|
Tanouchi Y, Lee AJ, Meredith H and You L:
Programmed cell death in bacteria and implications for antibiotic
therapy. Trends Microbiol. 21:265–270. 2013.PubMed/NCBI View Article : Google Scholar
|
|
59
|
Jorgensen I, Rayamajhi M and Miao EA:
Programmed cell death as a defence against infection. Nat Rev
Immunol. 17:151–164. 2017.PubMed/NCBI View Article : Google Scholar
|