Introduction
The anatomy of the nasal cavities and paranasal
sinuses exhibits substantial variability, making it one of the most
diverse regions in the human body. Given their intricate
three-dimensional structure and numerous morphological variations,
a comprehensive understanding of these anatomical features is
essential for sinus surgeons (1).
The maxillary sinus, pyramid-shaped and the largest of the
paranasal sinuses, is situated directly behind the anterior bony
surface of the midface and is encased by bone structures (2). This sinus was first described in 1651
by the English anatomist Nathaniel Highmore (3). Its development initiates in the 10th
week of intrauterine life, marked by primary extension, a phase in
which air fills the cavity to increase its volume. At the 20th week
of pregnancy, secondary pneumatization occurs, allowing the
maxillary sinus to expand into the maxilla, reaching a volume of
approximately 6-8 cm³ at birth. Thereafter, it continues to expand
laterally and inferiorly during two rapid growth phases: The first
from birth to 3 years and the second from 7 to 12 years. This
progressive inferior expansion correlates with the alveolar process
invasion, influenced by the eruption of permanent teeth, ultimately
extending 4 to 5 mm below the nasal floor and achieving an average
volume of 15 cm³ by age 18 to 20(4). Anatomical variations in the maxillary
sinuses are acknowledged to possess significant clinical
implications, although their distinctive presentation and
prevalence can vary widely (3). The
literature remains controversial regarding the factors directly
associated with the maxillary sinus volume (MSV), primarily due to
the challenges in tracking its development in individuals without
facial bone abnormalities. Additionally, measuring the sinus volume
in clinical practice is complicated by its position within the
middle third of the face (4).
Despite these, anatomical differences among ethnic groups challenge
the use of a standardized evaluation method. A cross-sectional
study showed that Chinese individuals have significantly larger
sinuses than Yemenis (5). A
multi-ethnic review also reported ethnic differences in sinonasal
anatomical variants, supporting that maxillary sinus anatomy varies
by demographic background (6).
Although some scholars from Middle Eastern countries, such as Saudi
Arabia, have characterized maxillary sinus anatomy, comprehensive
regional evaluations remain limited. Overall, reviews of sinonasal
variation report considerable population differences, emphasizing
that data from the Middle Eastern population are relatively sparse
compared with other ethnicities (7). Advanced three-dimensional imaging
techniques, such as computed tomography (CT) and cone beam CT
(CBCT), are the preferred methods for visualizing the maxillary
sinus and diagnosing sinus pathologies before surgical intervention
(1,8). The present study used multi-slice CT
scans to evaluate anatomical variations in the maxillary sinuses
and associated factors in the Sulaymaniyah population.
Patients and methods
Study design and ethical
considerations
This retrospective cross-sectional study was
conducted on 283 patients who visited Smart Health Tower
(Sulaymaniyah, Iraq) for paranasal sinus imaging over one year. The
study was approved (approval no. 62-6/1/2024) by the Research
Ethics Committee of the University of Sulaimani, College of
Medicine (Sulaymaniyah, Iraq). Written informed consent was
obtained from each participant before enrollment and for the
publication of this study and any accompanying images.
Data collection and anatomical
assessment
Due to the hazardous radiation exposure, the sample
was obtained from the hospital registry using a non-randomized
sampling method. A total of 283 multi-slice CT images were
acquired, of which 227 were included, while 56 were excluded based
on predetermined eligibility criteria. The thickness of the
multi-slice CT scans ranged from 1.0 to 1.5 mm. All measurements
and interpretations of the CT files were conducted using the
RadiAnt DICOM Viewer 2023.1 (Medixant; https://www.radiantviewer.com/) by a single expert
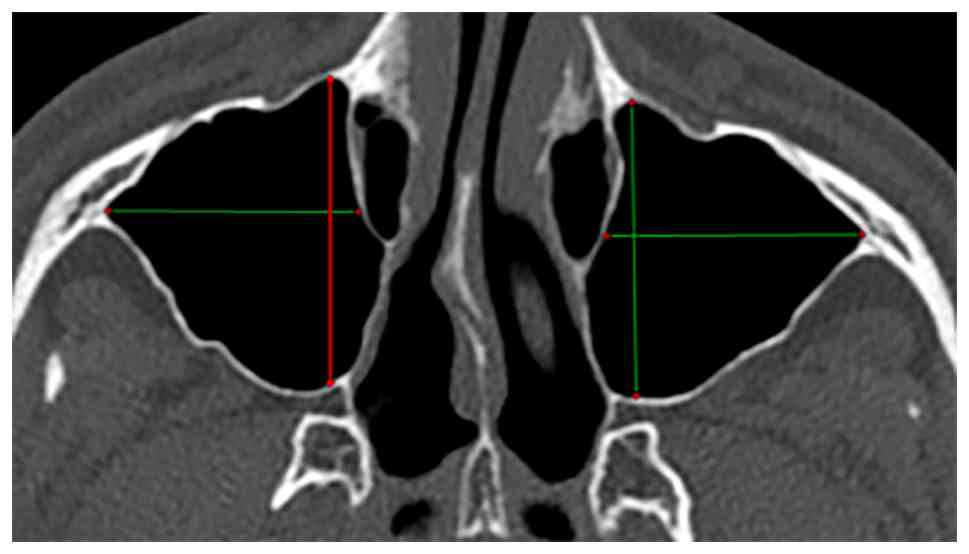
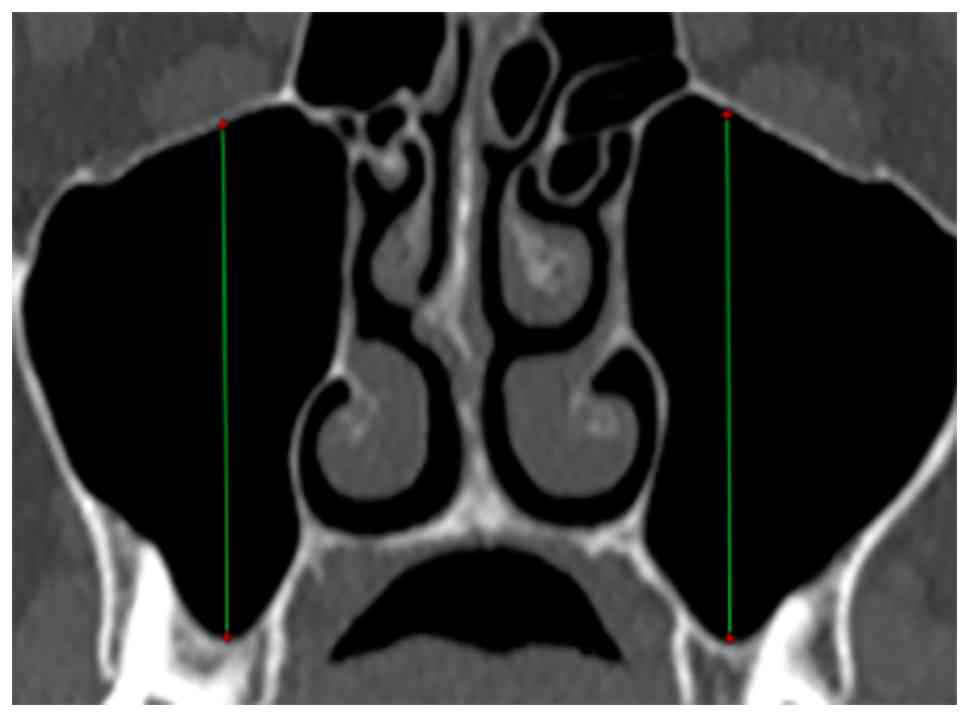
radiologist. Each sinus was assessed for variability in terms of
anteroposterior diameter, axial diameter, cranio-caudal diameter,
and volume, calculated using the ellipsoid approximation formula
(Figs. 1 and 2). Additionally, the presence and location
of infraorbital nerve (ION) protrusion, septation, Haller cells,
and hypoplasia were evaluated. The maximum diameter was determined
following a thorough review of all slices. Subsequently,
two-dimensional measurements were converted to three-dimensional
volume by multiplying them and applying a correction factor of
0.53. Furthermore, the percent difference formula was employed,
where the absolute difference was divided by the larger of the two
volumes and multiplied by 100. A result yielding a difference of
10% or more was classified as a significant asymmetry. Maxillary
sinus hypoplasia was diagnosed by comparing the length or width of
the sinus with that of the adjacent orbit. If either parameter of
the maxillary sinus was half or less than the corresponding orbit
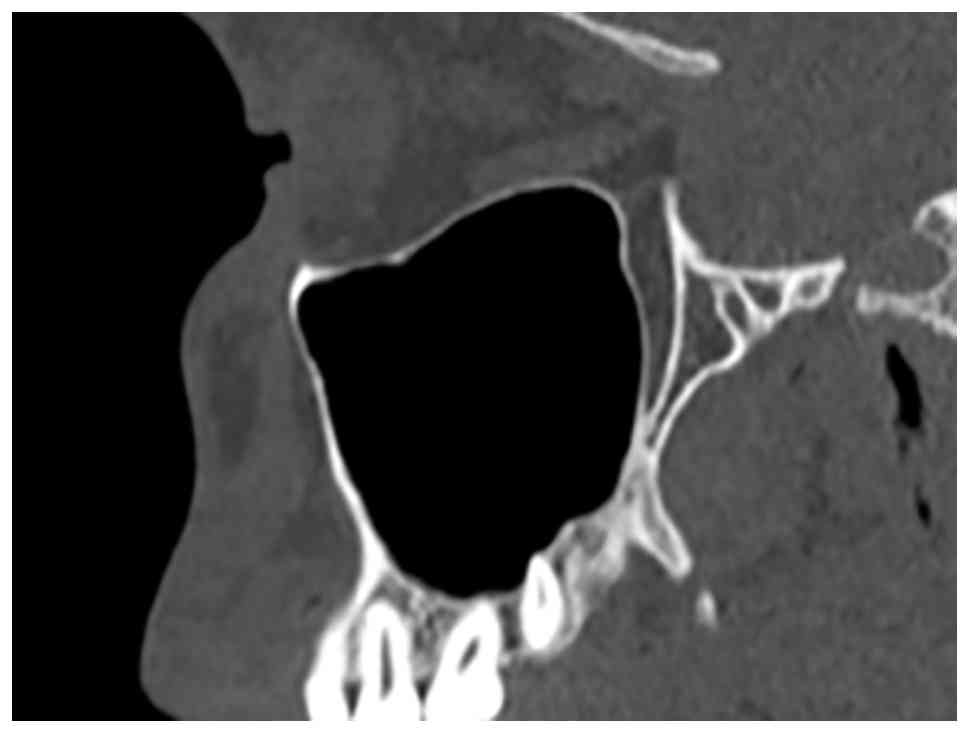
parameter, it indicated hypoplasia. While sagittal reconstruction
was not utilized for analyzing lengths and volumes, it was employed
for qualitative assessments to identify and exclude abnormalities
or variations (Fig. 3).
Eligibility criteria
The eligibility criteria for the study were
restricted to patients aged 14 years and older, with visible
pneumatization, and complete visualization of the inferior
maxillary bone, including the superior alveolar process. Cases with
any visible abnormalities or pathologies were excluded, such as
absent or inadequate maxillary sinus pneumatization, incomplete
visualization of the maxillary sinus, any maxillary sinus pathology
affecting volume (mucosal thickening > 2 mm, retention cyst,
polyps, air fluid levels, chronic sinusitis, space-occupying
lesions), dental or odontogenic conditions altering sinus anatomy,
history of sinus surgery, history of maxillofacial or craniofacial
trauma, and developmental or structural craniofacial abnormalities.
The references in this paper were verified for authenticity using
reputable blacklists (9).
Statistical analysis
The data were exported to an Excel sheet and entered
into the Statistical Package for Social Sciences (SPSS) version 27
(IBM Corp.). Categorical data were analyzed using the Chi-square
test, while numerical data were evaluated with the independent
samples t-test and one-way ANOVA. The results were presented as
frequencies, percentages, means with standard deviations, and
medians with ranges. P<0.05 was considered to indicate a
statistically significant difference.
Results
Baseline characteristics
The sample population included 128 males (56.4%) and
99 females (43.6%) with a median age of 39 years (range, 15 to 90
years). Regarding sinus volume, 20.2% of females exhibited a larger
right sinus, while 79.8% had a smaller right sinus. For the left
sinus, 24.0% of females had a larger sinus, and 76.0% had a smaller
one. Overall, sinus symmetry was observed in 37.4% of cases, while
62.6% were asymmetrical. Among asymmetrical cases, 58.5% were male
and 41.5% were female. Maxillary sinus septations were found in
19.8% of patients, with a greater prevalence among males (57.8%)
than females (42.2%). In terms of laterality, 42.2% of septations
were bilateral, 35.6% were right-sided, and 22.2% were left-sided.
ION protrusions were observed in 27.3% of cases, with a higher
occurrence in males (61.3%) than females (38.7%). Most protrusions
were bilateral (64.5%), followed by left-sided (19.4%) and
right-sided (16.1%). An accessory maxillary ostium (AMO) was
present in 48.0% of participants, with 57.8% occurring in males and
42.2% in females. The ostium was primarily bilateral (56%), with
28.4% on the right and 15.6% on the left. Haller cells were
identified in 10.1% of cases, with a higher prevalence in males
(60.9%) than in females (39.1%). Of the Haller cells, 13.0% were
bilateral, 52.2% were on the right side, and 34.8% were on the
left. Sinus hypoplasia was found in two cases (1%) (Table I).
 | Table IBaseline characteristics of the
study. |
Table I
Baseline characteristics of the
study.
| Variables |
Frequency/Percentage |
|---|
| Age, median
(range), year | 39 (15-90) |
| Sex | |
|
Male | 128 (56.4%) |
|
Female | 99 (43.6%) |
| Sinus volume | |
|
Right
sinus | |
|
Larger
in females | 20 (20.2%) |
|
Smaller
in females | 79 (79.8%) |
|
Left
sinus | |
|
Larger
in females | 24 (24.0%) |
|
Smaller
in females | 75 (76.0%) |
| Sinus symmetry | |
|
Symmetrical | 85 (37.4%) |
|
Asymmetrical | 142 (62.6%) |
|
Male | 83 (58.5%) |
|
Female | 59 (41.5%) |
| Septations | |
|
Yes | 45 (19.8%) |
|
No | 182 (80.2%) |
| Septations by
sex | |
|
Male | 26 (57.8%) |
|
Female | 19 (42.2%) |
| Septations
laterality | |
|
Bilateral | 19 (42.2%) |
|
Right | 16 (35.6%) |
|
Left | 10 (22.2%) |
| Infraorbital nerve
protrusions | |
|
Yes | 62 (27.3%) |
|
No | 165 (72.7%) |
| Infraorbital nerve
protrusions by gender | |
|
Male | 38 (61.3%) |
|
Female | 24 (38.7%) |
| Infraorbital nerve
protrusions laterality | |
|
Bilateral | 40 (64.5%) |
|
Right | 10 (16.1%) |
|
Left | 12 (19.4%) |
| Accessory maxillary
ostium | |
|
Yes | 109 (48.0%) |
|
No | 118 (52.0%) |
| Accessory maxillary
ostium by sex | |
|
Male | 63 (57.8%) |
|
Female | 46 (42.2%) |
| Accessory maxillary
ostium laterality | |
|
Bilateral | 61 (56.0%) |
|
Right | 31 (28.4%) |
|
Left | 17 (15.6%) |
| Haller cells | |
|
Yes | 23 (10.1%) |
|
No | 204 (89.9%) |
| Haller cells by
sex | |
|
Male | 14 (60.9%) |
|
Female | 9 (39.1%) |
| Haller cells
laterality | |
|
Bilateral | 3 (13.0%) |
|
Right | 12 (52.2%) |
|
Left | 8 (34.8%) |
| Sinus
hypoplasia | |
|
Yes | 2 (1.0%) |
|
No | 225 (99.0%) |
Right MSV by sex and age
Males generally exhibited a larger mean sinus volume
than females across most age ranges. The mean volume for the 14-29
age group was 21.90 cc in males vs. 16.72 cc in females
(P<0.001). This trend persisted, with significant differences
also observed in the 50-59 and >60 age groups, where males had
mean volumes of 19.58 and 20.17 cc, respectively, compared with
12.33 and 12.95 cc in females (P=0.004 and P=0.002,
respectively). Overall, the mean sinus volume was significantly
larger in males (20.12 cc) than in females (15.60 cc) (P<0.001).
For the anteroposterior dimension of the maxillary sinus, males had
an overall mean of 3.76 cm compared with 3.57 cm in females
(P<0.001). The cranio-caudal dimension was also significantly
greater in males (3.68 cm) than in females (3.29 cm) (P<0.001).
Significant sex differences in cranio-caudal length were observed
across several age groups, including 14-29 (P=0.015), 30-39
(P=0.002), and >60 (P=0.002). Transverse
measurements also revealed a larger mean dimension in males (2.68
cm) compared to females (2.43 cm) (P<0.001; Table II).
| Table IIComparison of sex regarding right
maxillary sinus volume based on age groups. |
Table II
Comparison of sex regarding right
maxillary sinus volume based on age groups.
| A, Right sinus
parameters |
|---|
| | Male | Female | |
|---|
| Age groups | Mean volume
(cc) | Standard
deviation | Mean volume
(cc) | Standard
deviation | P-value |
|---|
| 14-29 | 21.90 | 7.10 | 16.72 | 3.52 | <0.001 |
| 30-39 | 18.83 | 6.81 | 15.57 | 5.02 | 0.070 |
| 40-49 | 18.82 | 5.93 | 17.78 | 5.04 | 0.570 |
| 50-59 | 19.58 | 6.21 | 12.33 | 5.06 | 0.004 |
| >60 | 20.17 | 7.47 | 12.95 | 5.97 | 0.002 |
| Overall | 20.12 | 6.79 | 15.60 | 5.06 | <0.001 |
| B, Anteroposterior
dimension |
| | Male | Female | |
| Age groups | Mean diameter
(cm) | Standard
deviation | Mean diameter
(cm) | Standard
deviation | P-value |
| 14-29 | 3.88 | 0.33 | 3.58 | 0.34 | <0.001 |
| 30-39 | 3.73 | 0.45 | 3.66 | 0.31 | 0.540 |
| 40-49 | 3.64 | 0.28 | 3.71 | 0.40 | 0.560 |
| 50-59 | 3.83 | 0.27 | 3.32 | 0.46 | 0.010 |
| >60 | 3.66 | 0.57 | 3.39 | 0.69 | 0.200 |
| Overall | 3.76 | 0.39 | 3.57 | 0.45 | <0.001 |
| C, Cranio-caudal
dimension |
| | Male | Female | |
| Age groups | Mean diameter
(cm) | Standard
deviation | Mean diameter
(cm) | Standard
deviation | P-value |
| 14-29 | 3.75 | 0.61 | 3.46 | 0.34 | 0.015 |
| 30-39 | 3.64 | 0.57 | 3.28 | 0.47 | 0.002 |
| 40-49 | 3.61 | 0.62 | 3.37 | 0.52 | 0.170 |
| 50-59 | 3.60 | 0.50 | 3.08 | 0.47 | 0.018 |
| >60 | 3.75 | 0.72 | 2.99 | 0.69 | 0.002 |
| Overall | 3.68 | 0.60 | 3.29 | 0.51 | <0.001 |
| D, Transverse
dimension |
| | Male | Female | |
| Age groups | Mean diameter
(cm) | Standard
deviation | Mean diameter
(cm) | Standard
deviation | P-value |
| 14-29 | 2.81 | 0.33 | 2.58 | 0.32 | <0.001 |
| 30-39 | 2.52 | 0.48 | 2.39 | 0.40 | 0.340 |
| 40-49 | 2.63 | 0.38 | 2.55 | 0.47 | 0.560 |
| 50-59 | 2.61 | 0.50 | 2.23 | 0.42 | 0.054 |
| >60 | 2.72 | 0.60 | 2.26 | 0.48 | 0.010 |
| Overall | 2.68 | 0.51 | 2.43 | 0.44 | <0.001 |
Left MSV by sex and age
In the 14-29 age group, the mean volume was 23.16 cc
in males and 17.71 cc in females (P<0.001). Significant
differences were also observed in the 50-59 and >60 age groups,
with males having mean volumes of 19.17 and 19.92 cc, respectively,
compared with 13.66 and 13.83 cc in females (P=0.037 and
P=0.011, respectively). Overall, the left sinus volume was
significantly greater in males (21.08 cc) than in females (16.40
cc; P<0.001). The left maxillary sinus dimensions also exhibited
sex differences. In general, the mean anteroposterior dimension was
significantly larger in males (3.80 cm) than in females (3.61 cm;
P<0.001), with a notable difference in the 14-29 and 50-59 age
groups (P=0.005 and P=0.002, respectively).
Cranio-caudal measurements were also significantly greater in males
(3.81 cm) than in females (3.35 cm; P<0.001). For the transverse
dimension, males had a mean of 2.67 cm compared with 2.46 cm in
females (P<0.001) (Table
III).
| Table IIIComparison of sex regarding left
maxillary sinus volume based on age groups. |
Table III
Comparison of sex regarding left
maxillary sinus volume based on age groups.
| A, Left sinus
parameters |
|---|
| | Male | Female | |
|---|
| Age groups | Mean volume
(cc) | Standard
deviation | Mean volume
(cc) | Standard
deviation | P-value |
| 14-29 | 23.16 | 6.81 | 17.71 | 5.06 | <0.001 |
| 30-39 | 19.80 | 8.24 | 16.12 | 5.04 | 0.074 |
| 40-49 | 21.14 | 6.59 | 18.29 | 7.32 | 0.195 |
| 50-59 | 19.17 | 5.48 | 13.66 | 6.09 | 0.037 |
| >60 | 19.92 | 7.64 | 13.83 | 6.07 | 0.011 |
| Overall | 21.08 | 7.08 | 16.40 | 5.93 | <0.001 |
| B, Anteroposterior
dimension |
| | Male | Female | |
| Age groups | Mean diameter
(cm) | Standard
deviation | Mean diameter
(cm) | Standard
deviation | P-value |
| 14-29 | 3.92 | 0.36 | 3.66 | 0.38 | 0.004 |
| 30-39 | 3.75 | 0.50 | 3.70 | 0.30 | 0.626 |
| 40-49 | 3.78 | 0.26 | 3.81 | 0.32 | 0.751 |
| 50-59 | 3.80 | 0.35 | 3.31 | 0.33 | 0.002 |
| >60 | 3.66 | 0.40 | 3.35 | 0.71 | 0.126 |
| Overall | 3.80 | 0.38 | 3.61 | 0.45 | <0.001 |
| C, Cranio-caudal
dimension |
| | Male | Female | |
| Age groups | Mean diameter
(cm) | Standard
deviation | Mean diameter
(cm) | Standard
deviation | P-value |
| 14-29 | 3.90 | 0.54 | 3.46 | 0.33 | <0.001 |
| 30-39 | 3.74 | 0.59 | 3.35 | 0.40 | 0.011 |
| 40-49 | 4.85 | 0.52 | 3.45 | 0.62 | 0.029 |
| 50-59 | 3.66 | 0.49 | 3.22 | 0.63 | 0.091 |
| >60 | 3.75 | 0.64 | 3.12 | 0.65 | 0.005 |
| Overall | 3.81 | 0.55 | 3.35 | 0.50 | <0.001 |
| D, Transverse
dimension |
| | Male | Female | |
| Age groups | Mean diameter
(cm) | Standard
deviation | Mean diameter
(cm) | Standard
deviation | P-value |
| 14-29 | 2.80 | 0.37 | 2.59 | 0.39 | 0.023 |
| 30-39 | 2.54 | 0.52 | 2.40 | 0.42 | 0.331 |
| 40-49 | 2.67 | 0.40 | 2.52 | 0.51 | 0.284 |
| 50-59 | 2.56 | 0.46 | 2.29 | 0.45 | 0.154 |
| >60 | 2.65 | 0.64 | 2.31 | 0.53 | 0.081 |
| Overall | 2.67 | 0.47 | 2.46 | 0.46 | <0.001 |
Comparison of the right and left
maxillary sinuses
There was no significant difference in the right MSV
across age groups (P=0.123), while the left MSV varied
significantly (P=0.025). Regarding the anteroposterior,
craniocaudal, and transverse dimensions, the right maxillary sinus
showed no significant differences across age groups in the first
two dimensions; however, a significant difference was observed in
the transverse dimension (P=0.037). For the left maxillary
sinus, significant differences were noted in both the
anteroposterior and transverse dimensions among age groups
(P=0.006 and P=0.026, respectively) (Table IV). Additionally, ION protrusion
was significantly associated with increasing MSV on both the right
and left sides (P<0.001) (Table
V).
| Table IVComparison of right and left
maxillary sinus volumes based on age groups. |
Table IV
Comparison of right and left
maxillary sinus volumes based on age groups.
| A, Sinus
parameters |
|---|
| | Right maxillary
sinus | Left maxillary
sinus |
|---|
| Age groups | Mean volume
(cc) | Standard
deviation | P-value | Mean volume
(cc) | Standard
deviation | P-value |
|---|
| 14-29 | 19.67 | 6.35 | 0.123 | 20.82 | 6.66 | 0.025 |
| 30-39 | 17.16 | 6.12 | | 17.92 | 6.97 | |
| 40-49 | 18.43 | 5.54 | | 19.98 | 6.96 | |
| 50-59 | 17.16 | 6.73 | | 17.34 | 6.17 | |
| >60 | 16.85 | 7.65 | | 17.13 | 7.52 | |
| B, Anteroposterior
dimension |
| | Right maxillary
sinus | Left maxillary
sinus |
| Age groups | Mean diameter
(cm) | Standard
deviation | P-value | Mean diameter
(cm) | Standard
deviation | P-value |
| 14-29 | 3.75 | 0.37 | 0.149 | 3.81 | 0.39 | 0.006 |
| 30-39 | 3.70 | 0.38 | | 3.72 | 0.40 | |
| 40-49 | 3.67 | 0.33 | | 3.79 | 0.28 | |
| 50-59 | 3.66 | 0.41 | | 3.64 | 0.41 | |
| >60 | 3.53 | 0.63 | | 3.52 | 0.57 | |
| C, Cranio-caudal
dimension |
| | Right maxillary
sinus | Left maxillary
sinus |
| Age groups | Mean diameter
(cm) | Standard
deviation | P-value | Mean diameter
(cm) | Standard
deviation | P-value |
| 14-29 | 3.63 | 0.53 | 0.300 | 3.71 | 0.51 | 0.140 |
| 30-39 | 3.46 | 0.55 | | 3.54 | 0.54 | |
| 40-49 | 3.51 | 0.59 | | 3.69 | 0.59 | |
| 50-59 | 3.43 | 0.54 | | 3.52 | 0.57 | |
| >60 | 3.40 | 0.79 | | 3.46 | 0.71 | |
| D, Transverse
dimension |
| | Right maxillary
sinus | Left maxillary
sinus |
| Age groups | Mean diameter
(cm) | Standard
deviation | P-value | Mean diameter
(cm) | Standard
deviation | P-value |
| 14-29 | 2.71 | 0.39 | 0.037 | 2.71 | 0.39 | 0.026 |
| 30-39 | 2.44 | 0.44 | | 2.47 | 0.47 | |
| 40-49 | 2.58 | 0.46 | | 2.61 | 0.45 | |
| 50-59 | 2.49 | 0.58 | | 2.47 | 0.47 | |
| >60 | 2.52 | 0.66 | | 2.49 | 0.61 | |
| Table VEffect of ION protrusions on
maxillary sinus volumes. |
Table V
Effect of ION protrusions on
maxillary sinus volumes.
|
| Right sinus
volume | Left sinus
volume |
|---|
| Variable | Mean (cc) | Standard
deviation | P-value | Mean (cc) | Standard
deviation | P-value |
|---|
| With ION
protrusion | 20.93 | 5.62 | <0.001 | 21.20 | 6.18 | <0.001 |
| Without ION
protrusion | 17.36 | 6.52 | | 18.39 | 7.12 | |
Discussion
A comprehensive understanding of the anatomical
variations and pathologies of the maxillary sinus is essential for
clinical practice in dentistry, maxillofacial surgery, and
otolaryngology. Various imaging techniques, including CT and CBCT,
have been used to assess the nasal cavity and maxillary sinuses.
Conventional radiographs offer only a two-dimensional view of
anatomical structures. By contrast, CT and CBCT provide valuable
insights for imaging and identifying anatomical variations within
the bony structures of the paranasal sinuses (2,3). MSV
and sinus dimensions may vary by age and between individuals.
Additionally, even within the same individual, there may be
variations between the right and left sinus parameters (2). The relatively high prevalence of
maxillary sinus asymmetry (62.6%) and the variability in other
parameters in this study may be influenced by several anatomical,
developmental, and environmental factors. Craniofacial
morphological variations, particularly vertical skeletal growth
patterns, have been shown to affect sinus dimensions and contribute
to side-to-side differences in MSV (10). Ethnic and population-specific
variability further contributes to these differences, as studies in
other populations report wide variation in sinus asymmetry
prevalence, depending on methodology and population (5,6,11).
Developmental factors, including differential pneumatization and
sinus remodeling influenced by dental status, skeletal growth, and
sinonasal anatomy, may also play a role (12). Environmental and functional
influences, such as chronic sinonasal inflammation or differences
in mastication patterns, can contribute to asymmetric sinus
development over time (13).
Finally, methodological factors, including imaging modality, slice
orientation, and the threshold used to define asymmetry, may partly
explain differences in prevalence across studies. The prevalence of
AMO in the present study (~48%) has important anatomical and
clinical implications. AMO has been consistently associated with
impaired mucociliary clearance, mucus recirculation, and a higher
risk of recurrent or chronic maxillary sinusitis (14). Generally, AMO prevalence ranges from
35-56% and is significantly associated with abnormal maxillary
sinus mucosal changes, such as mucosal thickening or natural-ostium
obstruction (15). This
pathophysiological mechanism suggests that AMO may facilitate mucus
recirculation between the accessory and natural ostia, predisposing
the sinus to chronic inflammation and recurrent sinusitis (16). In our study population, the high
prevalence of AMO underscores the importance of careful
preoperative imaging assessment for ENT surgeons, radiologists, and
dental/maxillofacial clinicians to minimize procedural
complications and anticipate potential sinus drainage issues.
In the present cohort, maxillary sinus septations
were identified in approximately one-fifth of patients (~20%). This
finding aligns with reported prevalence rates from CBCT and CT
studies, which range from 21 to 25.6% of sinus segments and 25-37%
of individuals, depending on the population and imaging method
employed (17,18). Anatomically, these septa comprise
bony ridges that divide the sinus cavity, often oriented
bucco-palatally and located in the middle region, which complicates
surgical access (18). Clinically,
the presence of septa significantly increases the risk of
perforating the Schneiderian membrane during sinus lift procedures.
A meta-analysis across 1,865 patients (2,168 sinus lifts) found an
odds ratio of ~4.03 for perforation when septa were present,
compared with sinuses without septa (19).
Congenital maxillary sinus hypoplasia was identified
in 1% of the cases in this study, consistent with the low
prevalence reported in the literature (5.65%) (20). It is clinically significant because
it may mimic chronic maxillary sinusitis, present with nonspecific
symptoms, or lead to diagnostic confusion on routine imaging. In
addition, the altered anatomy may complicate endoscopic sinus
surgery, increase the risk of orbital penetration, and affect
surgical planning (20). Therefore,
even though its prevalence is low, awareness of this variation is
essential for accurate radiologic interpretation and safe surgical
management.
Certain studies indicated a significant association
between age and MSV, noting that MSV decreases with age (21,22).
By contrast, others reported no significant differences between the
right and left MSV values and MSV with age (21,23,24).
Sex differences in MSV have also been explored. Aşantoğrol and
Coşgunarslan (2) and Al-Rawi et
al (23) observed that males
had greater maxillary sinus width, height, and length than females,
with statistically significant differences. Conversely, Demir et
al (25) and Lessa et al
(4) reported no significant
correlation between MSV and sex. Despite these findings, numerous
studies support that MSV values are generally higher in males than
in females (21,23). In the present study, the right MSV
did not vary significantly with age, whereas the left MSV showed
differences across age groups. Concerning sex, the MSV on both
sides was significantly higher in males than in females, with this
difference evident across age categories.
Accurate identification of bony septa is essential
to enhance the safety of surgical procedures, particularly sinus
lift surgeries and implant placements, as septa have been
associated with an increased risk of sinus membrane perforation and
thinner sinus mucosa. This risk is heightened when the septa are
arranged longitudinally or are incomplete, as these configurations
can complicate membrane elevation compared with a transverse
arrangement (4). In terms of
anatomical variations, previous studies found no association
between the presence of septa and MSV. However, significant
increases in the maxillary sinus width on both the left and right
sides were noted when septa were present (2,21). The
prevalence of bony septa within the maxillary sinus has been
reported to range from 9.5 to 70%, varying according to the studied
population and diagnostic modality used (26). Lessa et al (4) observed that 47% of maxillary sinuses
presented with bony septa, although no significant difference was
noted in MSV related to the presence of septa. Şimşek Kaya et
al (27) identified septa in
32.9% of 228 evaluated sinuses, while Asan et al (3) reported a prevalence rate of 24%, with
septa more commonly located on the right side. Sex differences in
septa prevalence have been inconsistent in the literature. A study
found a higher prevalence of septa among females, with no
association between septa and age or dental status (28). Conversely, studies by Koymen et
al (29) and Hong et al
(30) reported a male predominance
in septa presence. This increased occurrence in males has been
postulated to relate to the typically higher mean maximum bite
force in males than females (29,30).
In the present study, maxillary sinus septation was identified in
45 cases (19.8%), comprising 26 males (57.8%) and 19 females
(42.2%). Bilateral septation was the most common in 19 cases
(42.2%).
Haller cells, or infra-orbital ethmoid cells, are
air-filled cavities inferolateral to the ethmoidal bulla (3). These cells can increase susceptibility
to sinus pathologies by accelerating inflammation, complicating
sinus surgery, and contributing to conditions such as
rhinosinusitis. Infection of Haller cells can lead to mucosal
swelling, which restricts secretion transport and creates a cycle
that may contribute to unilateral orbital cellulitis (3). Prevalence rates of Haller cells vary
widely in the literature, with reports ranging from 4.7 to 45.1% or
5.5 to 45.9% (31,32). Asan et al (3) observed Haller cells in 15.3% of
samples, identifying them as the second most significant anatomical
variation. Although there was no significant difference in
prevalence between sexes, a higher occurrence was noted on the
right side (3). Chaudhari et
al (32) found a prevalence of
10% (30 out of 300 individuals), with 18 males and 12 females,
yielding a male-to-female ratio of 3:2. Conversely, Ahmad et
al (33) reported a notably
higher prevalence of 38.2%, with a higher occurrence among females
(32). Regarding laterality,
Chaudhari et al (32)
reported that Haller cells appeared bilaterally in 16 cases and
unilaterally in 14, suggesting a tendency for bilateral occurrence.
This finding contrasts with a previous study that reported a
predominantly unilateral presentation of Haller cells (34). The current study identified Haller
cells in 23 cases (10.1%), comprising 14 males and 9 females. The
majority of these cases were unilateral (87%) and predominantly
located on the right side (52.2%), consistent with the findings of
Ramaswamy et al (34) and
Asan et al (3). The most
prevalent anatomical variation observed was sinus asymmetry,
identified in 142 cases (62.6%). Conversely, the presence of Haller
cells was the second least common variation. This finding contrasts
with the study by Asan et al (3), who identified Haller cells as the
second most frequent anatomical variation.
Lantos et al (35) defined infraorbital canal (IOC)
protrusion as occurring when the entire 360˚ circumference of the
IOC wall lacked contact with a maxillary sinus wall on at least one
axial CT image. Although reported prevalence rates for ION
protrusion range from 8 to 35%, there is no standardized definition
for protrusion despite efforts to establish a classification system
(35). In their study, Lantos et
al (35) observed a 10.8%
prevalence of IOC protrusion into the maxillary sinus, with a
bilateral protrusion rate of 5.6% (34). Eiid et al (36) found that the IOC most frequently
presented as the typical confined type, detected in 78.1% of
sinuses, while the suspended (or protruded) variant was identified
in 14.6% of cases. They emphasized that IOC protrusion, though not
uncommon, requires heightened caution from surgeons utilizing the
maxillary sinuses as access points, particularly in the upper
lateral areas of the sinus (36).
In the present study, ION protrusion into the maxillary sinus was
present in 62 cases (27.3%), with bilateral protrusions in 40 cases
(17.6%). On both sides, ION protrusion was significantly associated
with increased MSV. The observed association between ION protrusion
and increased MSV in our study has important anatomical and
clinical implications. Previous volumetric research demonstrated
that individuals with a ‘descending’ or protruding IOC Type 3
consistently exhibit significantly larger MSVs, suggesting that
extensive sinus pneumatization may progressively encompass or
suspend the canal within the sinus cavity. Since the developmental
trajectory of the ION canal is established prenatally, whereas
maxillary sinus pneumatization continues through adolescence and
adulthood, this relationship supports the concept that ION
protrusion is likely a pneumatization-driven variant rather than an
isolated anomaly (37). Clinically,
larger sinuses have been associated with a higher prevalence of
canal exposure or ‘suspension’ into the sinus lumen, reported in
~11% of cases in large CT-based series, underscoring the risk of
iatrogenic nerve injury during endoscopic sinus surgery, dental
implant placement, or transmaxillary procedures (35). Therefore, these findings reinforce
the importance of preoperative imaging, particularly volumetric
assessment, in patients exhibiting large maxillary sinuses, as the
likelihood of encountering a protruding or vulnerable IOC is
increased. This relationship also highlights the need for future
research to routinely incorporate sinus volume when evaluating ION
canal variants to improve anatomical understanding and surgical
planning.
The small sample size, non-random sampling, no
multiple comparison analysis, lack of assessment of interobserver
reliability, the use of ellipsoid volume estimates, and the data
being collected from only a single center are significant
limitations of this study that may affect the generalizability of
the findings.
In conclusion, anatomical variations of the
maxillary sinus were common within the study population, with
asymmetry present in 62.6%. The maxillary sinus was revealed to be
significantly larger in males than in females, exhibiting notable
differences in dimensions and volume. Additionally, this study
revealed an association between ION protrusion and sinus volume;
specifically, sinuses with protruded ION tended to have larger
volumes. These findings suggest the potential necessity for
preoperative assessments utilizing CT scans or other
three-dimensional imaging techniques.
Acknowledgements
Not applicable.
Funding
Funding: No funding was received.
Availability of data and materials
The data generated in the present study may be
requested from the corresponding author.
Authors' contributions
SHT was the major contributor to the conception of
the study, as well as to the literature search for related studies.
SHT and RS were involved in the literature review and the writing
of the manuscript. YF and BS were involved in the literature
review, the design of the study, the critical revision of the
manuscript, and the processing of the tables. SHT and RS acquired
the data, as well as performed the data analysis and
interpretation. In addition, SHT and RS confirm the authenticity of
all the raw data. All authors have read and approved the final
manuscript.
Ethics approval and consent to
participate
The study was approved (approval no 62-6/1/2024) by
the Research Ethics Committee of the University of Sulaimani,
College of Medicine (Sulaymaniyah, Iraq). Written informed consent
was obtained from each participant before enrollment.
Patient consent for publication
Written informed consent was obtained from the
patients for the publication of this study and any accompanying
images.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Papadopoulou AM, Chrysikos D, Samolis A,
Tsakotos G and Troupis T: Anatomical variations of the nasal
cavities and paranasal sinuses: A systematic review. Cureus.
13(e12727)2021.PubMed/NCBI View Article : Google Scholar
|
|
2
|
Aşantoğrol F and Coşgunarslan A: The
effect of anatomical variations of the sinonasal region on
maxillary sinus volume and dimensions: A three-dimensional study.
Braz J Otorhinolaryngol. 88 (Suppl 1):S118–S127. 2022.PubMed/NCBI View Article : Google Scholar
|
|
3
|
Asan MF, Castelino RL, Babu SG and Darwin
D: Anatomical variations of the maxillary sinus-a cone beam
computed tomography study. Acta Med Bulg. 49:33–37. 2022.
|
|
4
|
Lessa AMG, Oliveira VS, Costa RBA, Meneses
ATR, Crusoé-Rebello I, Costa FWG and Neves FS: Anatomical study of
the maxillary sinus: Which characteristics can influence its
volume? Surg Radiol Anat. 45:81–87. 2023.PubMed/NCBI View Article : Google Scholar
|
|
5
|
Albarakani AY, Zheng BW, Hong J,
Al-Somairi MAA, Abdulqader AA and Liu Y: A comparison of maxillary
sinus diameters in Chinese and Yemeni patients with skeletal
malocclusion. BMC Oral Health. 22(582)2022.PubMed/NCBI View Article : Google Scholar
|
|
6
|
Kulich M, Long R, Reyes Orozco F, Yi AH,
Hao A, Han JS and Hur K: Racial, ethnic, and gender variations in
sinonasal anatomy. Ann Otol Rhinol Laryngol. 132:996–1004.
2023.PubMed/NCBI View Article : Google Scholar
|
|
7
|
Madfa AA, Alshammari AF, Alenezi YE,
Alshammari BB, Al-Haddad A, Aledaili EA, Abobaker SH and Alkurdi
KA: Comprehensive analysis of maxillary sinus anatomical features
and associated characteristics: A CBCT-based study in a Saudi
subpopulation. BMC Oral Health. 25(1755)2025.PubMed/NCBI View Article : Google Scholar
|
|
8
|
Zhu J, Lin W, Yuan W and Chen L: New
insight on pathophysiology, diagnosis, and treatment of odontogenic
maxillary sinusitis. J Nanomater. 2021(9997180)2021.
|
|
9
|
Abdullah HO, Abdalla BA, Kakamad FH, Ahmed
JO, Baba HO, Hassan MN, Bapir R, Rahim HM, Omar DA, Kakamad SH, et
al: Predatory publishing lists: A review on the ongoing battle
against fraudulent actions. Barw Med J. 2:26–30. 2024.
|
|
10
|
Chunduru R, Rachel P, Kailasam V and
Padmanabhan S: The evaluation of maxillary sinus dimensions in
different craniofacial patterns: A systematic review and
meta-analysis. Turk J Orthod. 36:208–215. 2023.PubMed/NCBI View Article : Google Scholar
|
|
11
|
Aliu A, Ma'aji SM, Sirajo BS, Ibrahim AM
and Abdullahi ZD: Classification of anatomical variants of
maxillary sinus shapes and symmetry using computerized tomographic
imaging. Sub Saharan Afr J Med. 6:143–147. 2019.
|
|
12
|
Dinç K and İçöz D: Maxillary sinus volume
changes in individuals with different craniofacial skeletal
patterns: CBCT study. BMC Oral Health. 24(1516)2024.PubMed/NCBI View Article : Google Scholar
|
|
13
|
Lawson W, Patel ZM and Lin FY: The
development and pathologic processes that influence maxillary sinus
pneumatization. Anat Rec (Hoboken). 291:1554–1563. 2008.PubMed/NCBI View
Article : Google Scholar
|
|
14
|
Bani-Ata M, Aleshawi A, Khatatbeh A,
Al-Domaidat D, Alnussair B, Al-Shawaqfeh R and Allouh M: Accessory
maxillary ostia: Prevalence of an anatomical variant and
association with chronic sinusitis. Int J Gen Med. 13:163–168.
2020.PubMed/NCBI View Article : Google Scholar
|
|
15
|
Rudbarizade SH, Goudarzi F, Zadeh KM and
Afsa M: Accessory maxillary sinus ostium frequency and correlation
with anatomical variables and sinus mucosal status: A CBCT study. J
Dent (Shiraz). 26:302–308. 2025.PubMed/NCBI View Article : Google Scholar
|
|
16
|
Orhan Soylemez UP and Atalay B:
Investigation of the accessory maxillary ostium: A congenital
variation or acquired defect? Dentomaxillofac Radiol.
50(20200575)2021.PubMed/NCBI View Article : Google Scholar
|
|
17
|
Verma R, Dua N, Gupta R, Jain M, Mridula
and Gupta M: Evaluation of Maxillary sinus septa using cone
beam computed tomography (CBCT): A retrospective study. Cureus.
16(e68157)2024.PubMed/NCBI View Article : Google Scholar
|
|
18
|
Alhumaidan G, Eltahir MA and Shaikh SS:
Retrospective analysis of maxillary sinus septa-a cone beam
computed tomography study. Saudi Dental J. 33:467–473.
2021.PubMed/NCBI View Article : Google Scholar
|
|
19
|
Yang B, Wang T, Wen Y and Liu X:
Association between sinus septa and lateral wall thickness with
risk of perforation during maxillary sinus lift surgery: A
systematic review and meta-analysis. PLoS One.
19(e0308166)2024.PubMed/NCBI View Article : Google Scholar
|
|
20
|
Souza DA, Costa FW, de Mendonca DS,
Ribeiro EC, de Barros Silva PG and Neves FS: Computed tomography
assessment of maxillary sinus hypoplasia and associated anatomical
variations: A systematic review and meta-analysis of global
evidence. Oral Radiol. 40:124–137. 2024.PubMed/NCBI View Article : Google Scholar
|
|
21
|
Anbiaee N, Khodabakhsh R and Bagherpour A:
Relationship between anatomical variations of sinonasal area and
maxillary sinus pneumatization. Iran J Otorhinolaryngol.
31:229–234. 2019.PubMed/NCBI
|
|
22
|
Kalabalık F and Tarım Ertaş E:
Investigation of maxillary sinus volume relationships with nasal
septal deviation, concha bullosa, and impacted or missing teeth
using cone-beam computed tomography. Oral Radiol. 35:287–295.
2019.PubMed/NCBI View Article : Google Scholar
|
|
23
|
Al-Rawi NH, Uthman AT, Abdulhameed E, Al
Nuaimi AS and Seraj Z: Concha bullosa, nasal septal deviation, and
their impacts on maxillary sinus volume among Emirati people: A
cone-beam computed tomography study. Imaging Sci Dent. 49:45–51.
2019.PubMed/NCBI View Article : Google Scholar
|
|
24
|
Tassoker M, Magat G, Lale B, Gulec M,
Ozcan S and Orhan K: Is the maxillary sinus volume affected by
concha bullosa, nasal septal deviation, and impacted teeth? A CBCT
study. Eur Arch Otorhinolaryngol. 277:227–233. 2020.PubMed/NCBI View Article : Google Scholar
|
|
25
|
Demir UL, Akca ME, Ozpar R, Albayrak C and
Hakyemez B: Anatomical correlation between existence of concha
bullosa and maxillary sinus volume. Surg Radiol Anat. 37:1093–1098.
2015.PubMed/NCBI View Article : Google Scholar
|
|
26
|
Al-Zahrani MS, Al-Ahmari MM, Al-Zahrani
AA, Al-Mutairi KD and Zawawi KH: Prevalence and morphological
variations of maxillary sinus septa in different age groups: A CBCT
analysis. Ann Saudi Med. 40:200–206. 2020.PubMed/NCBI View Article : Google Scholar
|
|
27
|
Şimşek Kaya G, Daltaban Ö, Kaya M,
Kocabalkan B, Sindel A and Akdağ M: The potential clinical
relevance of anatomical structures and variations of the maxillary
sinus for planned sinus floor elevation procedures: A retrospective
cone beam computed tomography study. Clin Implant Dent Relat Res.
21:114–121. 2019.PubMed/NCBI View Article : Google Scholar
|
|
28
|
Benjaphalakron N, Jansisyanont P,
Chuenchompoonut V and Kiattavorncharoen S: Evaluation of the
maxillary sinus anatomical variations related to maxillary sinus
augmentation using cone beam computed tomography images. J Oral
Maxillofac Surg Med Pathol. 33:18–25. 2021.
|
|
29
|
Koymen R, Gocmen-Mas N, Karacayli U,
Ortakoglu K, Ozen T and Yazici AC: Anatomic evaluation of maxillary
sinus septa: Surgery and radiology. Clin Anat. 22:563–570.
2009.PubMed/NCBI View
Article : Google Scholar
|
|
30
|
Hong KL, Wong RCW, Lim AAT, Loh FC, Yeo JF
and Islam I: Cone beam computed tomographic evaluation of the
maxillary sinus septa and location of blood vessels at the lateral
maxillary sinus wall in a sample of the Singaporean population. J
Oral Maxillofac Surg Med Pathol. 29:39–44. 2017.
|
|
31
|
Kamdi P, Nimma V, Ramchandani A, Ramaswami
E, Gogri A and Umarji H: Evaluation of haller cell on CBCT and its
association with maxillary sinus pathologies. J Indian Acad Oral
Med Radiol. 30:41–45. 2018.
|
|
32
|
Chaudhari RS, Sagar K, Sagar N, Sanjeev O,
Abhay K and Pratik P: Prevalence of Haller's cells: A panoramic
study. Ann Maxillofac Surg. 9:72–77. 2019.PubMed/NCBI View Article : Google Scholar
|
|
33
|
Ahmad M, Khurana N, Jaberi J, Sampair C
and Kuba RK: Prevalence of infraorbital ethmoid (Haller's) cells on
panoramic radiographs. Oral Surg Oral Med Oral Pathol Oral Radiol
Endod. 101:658–661. 2006.PubMed/NCBI View Article : Google Scholar
|
|
34
|
Ramaswamy P, Sai Kiran CH, Santosh N,
Smitha B and Sudhakar S: Prevalence of Haller's cells in south
Indian population using digital panoramic radiographs. Int J
Stomatol Occlusion Med. 8:12–16. 2015.
|
|
35
|
Lantos JE, Pearlman AN, Gupta A, Chazen
JL, Zimmerman RD, Shatzkes DR and Phillips CD: Protrusion of the
infraorbital nerve into the maxillary sinus on CT: Prevalence,
proposed grading method, and suggested clinical implications. Am J
Neuroradiol. 37:349–353. 2016.PubMed/NCBI View Article : Google Scholar
|
|
36
|
Eiid SB and Mohamed AA: Protrusion of the
infraorbital canal into the maxillary sinus: A cross-sectional
study in Cairo, Egypt. Imaging Sci Dent. 52:359–364.
2022.PubMed/NCBI View Article : Google Scholar
|
|
37
|
Kedar E, Koren I, Medlej B and Hershkovitz
I: The associations between the maxillary sinus volume,
infraorbital ethmoid cells, and the infraorbital canal: A CT-based
study. Diagnostics (Basel). 13(3593)2023.PubMed/NCBI View Article : Google Scholar
|