Introduction
Dextrocardia with situs inversus, also known
as situs inversus totalis, is a rare congenital condition
where the major visceral organs are mirrored from their normal
positions. The heart is located on the right side of the thoracic
cavity instead of the left, and other organs, such as the liver,
spleen, stomach and intestines, are also reversed. This condition
occurs in ~1 in 10,000 live births (1). The exact cause of dextrocardia with
situs inversus is not fully understood; however, it is
believed to involve a combination of genetic and environmental
factors. Situs inversus is often inherited in an autosomal
recessive manner, meaning both parents must carry a copy of the
mutated gene to pass it on to their child (2). Specific genes associated with
laterality defects, such as zinc finger protein of the cerebellum
3, located on the X chromosome (Xq26); it encodes a transcription
factor critical for early embryonic patterning and regulates
signaling pathways (notably NODAL pathway) that establish the
left-right body axis. Dynein axonemal heavy chain 5 (DNAH5) encodes
a dynein arm motor protein in the outer dynein arm of motile cilia,
and DNAH11 is another outer dynein arm heavy chain essential for
effective ciliary beating, have been implicated in the development
of this condition (3). During
normal embryonic development, the organs undergo a complex process
of rotation and positioning. In individuals with situs
inversus, this process is altered, leading to the mirror-image
positioning of the organs. This reversal happens early in
embryogenesis, typically within the first few weeks of gestation.
People with dextrocardia with situs inversus usually do not
have any symptoms directly related to the positioning of their
organs and can lead normal, healthy lives (1). However, they may be at an increased
risk for certain complications, such as Kartagener syndrome (OMIM:
244400). Approximately 25% of individuals with situs
inversus have Kartagener syndrome, which includes chronic
sinusitis, bronchiectasis and infertility due to ciliary
dysfunction. While most individuals with situs inversus have
a structurally normal heart, there is an increased incidence of
congenital heart defects, such as transposition of the great
arteries, atrial septal defects (OMIM: 600747) or ventricular
septal defects (OMIM: 600996), and tetralogy of Fallot (4). Dextrocardia with situs inversus
is typically diagnosed through imaging studies, including chest
X-ray, which reveals the heart's position on the right side of the
chest, echocardiogram, which provides detailed images of the
heart's structure and function, and abdominal ultrasound or CT
scans, which confirm the reversed positioning of the abdominal
organs. Management of dextrocardia with situs inversus
focuses on monitoring for and addressing any associated conditions
or complications. Regular follow-up with a healthcare provider is
essential to ensure any potential issues are identified and treated
promptly. The prognosis for individuals with dextrocardia with
situs inversus is generally good, especially in the absence
of significant congenital heart defects or other associated
syndromes (5). With appropriate
medical care, most individuals can expect to live a normal
lifespan.
Case report
Presentation
A 27-year-old man presented to the Akash Institute
of Medical Sciences and Research Centre (Bengaluru, India) in May
2023 with a history of a cough with expectoration and fever with
chills that had persisted for 4 days. The patient had no known
comorbidities, no notable family history of congenital disorders
and was born of a non-consanguineous marriage. The patient reported
no history of smoking or alcohol consumption.
On examination, the patient's vital signs were as
follows: Pulse, 110 bpm (tachycardia); blood pressure, 122/74 mmHg;
respiratory rate, 20 cycles per min; SpO2, 96%; and
temperature, 99.8˚F. The apex beat was not palpable on the left
side and only faint heart sounds were heard in the left hemithorax.
Percussion revealed a tympanic note over the right thorax. On
abdominal examination, liver dullness was detected on the left
side, suggesting visceral transposition (Table I).
 | Table IClinical and diagnostic summary of the
patient with dextrocardia and situs inversus. |
Table I
Clinical and diagnostic summary of the
patient with dextrocardia and situs inversus.
| Parameter | Findings |
|---|
| Age, years | 27 |
| Sex | Male |
| Date of
presentation | May 2023 |
| Place of
presentation | Akash Institute of
Medical Sciences and Research Centre (Bengaluru, India) |
| Chief complaints | Cough with
expectoration, fever with chills (4 days duration) |
| Habits | Non-smoker and
non-drinker |
| Comorbidities | None |
| Vital signs | Pulse, 110 bpm
(tachycardia); blood pressure, 122/74 mmHg; respiratory rate, 20
cpm; SpO2, 96%; temperature, 99.8˚F |
| Cardiovascular
exam | Apex beat not
palpable on left; faint heart sounds on left |
| Respiratory exam | Tympanic percussion
note on the right thorax |
| Abdominal exam | Liver dullness on the
left side |
| ECG findings | Sinus rhythm; right
axis deviation; negative QRS in Lead 1; inverted P and T waves in
Lead 1; decreasing R wave amplitude from V1 to V6 |
| Imaging
investigations | Chest X-ray:
Dextrocardia suspected. 2D echocardiography: Dextrocardia with
normal cardiac function. Abdominal US: Liver and gallbladder on
left, spleen on right |
| Provisional
diagnosis | Dextrocardia with
situs inversus |
| Laboratory tests
conducted at | Akash Institute of
Medical Sciences and Research Centre, (Bengaluru, India) |
| Management | Symptomatic treatment
(for fever and coughing), referred to a cardiologist and
pulmonologist |
Investigations
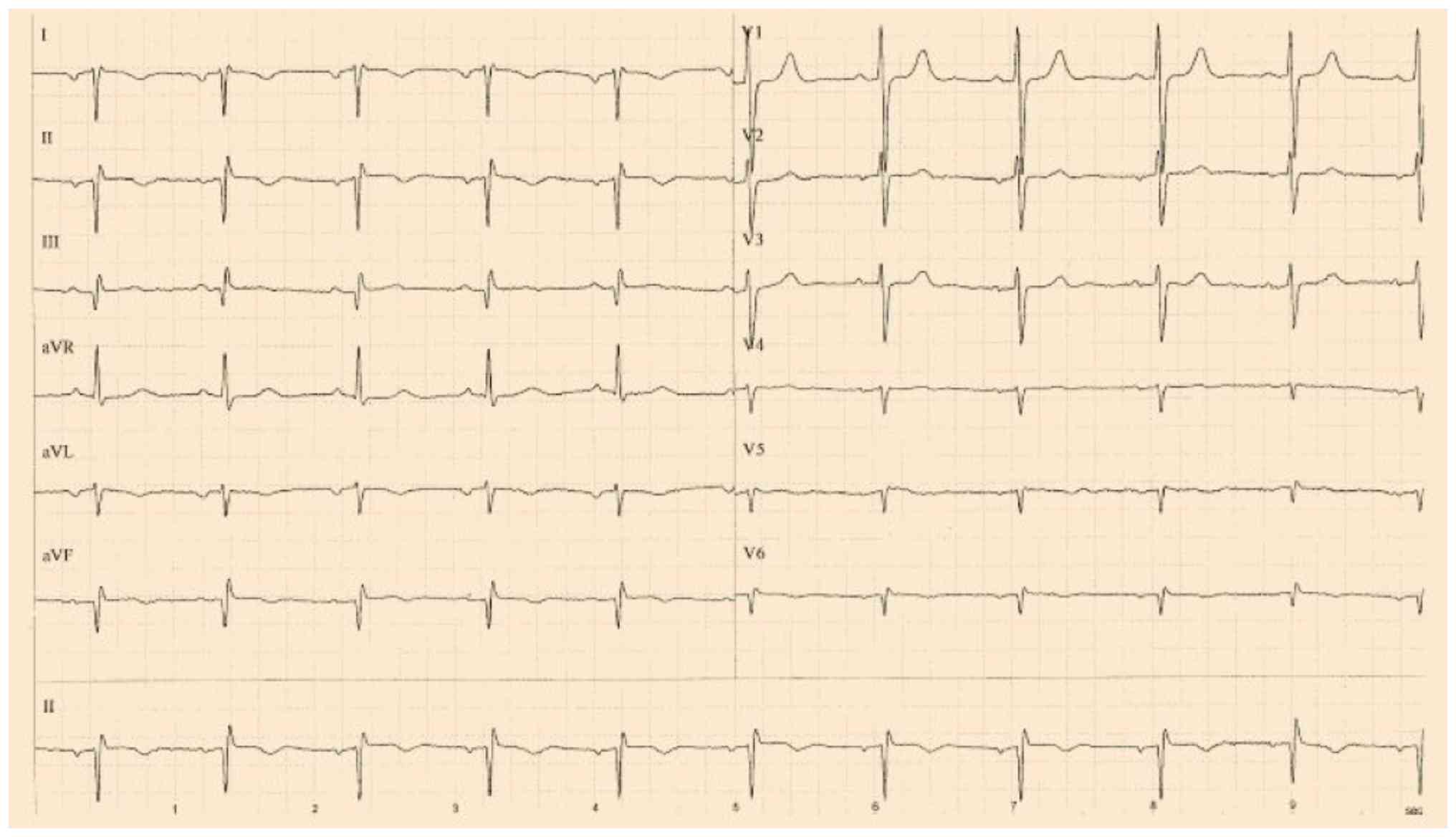
An electrocardiogram revealed sinus rhythm with
right axis deviation, a negative QRS complex in Lead 1, and
inverted P and T waves in Lead 1, with a progressively decreasing
R-wave amplitude from V1 to V6. A chest X-ray demonstrated a
right-sided cardiac shadow consistent with dextrocardia (Fig. 1). An electrocardiogram revealed
sinus rhythm with right axis deviation, a negative QRS complex in
Lead 1, and inverted P and T waves in Lead 1, with a progressively
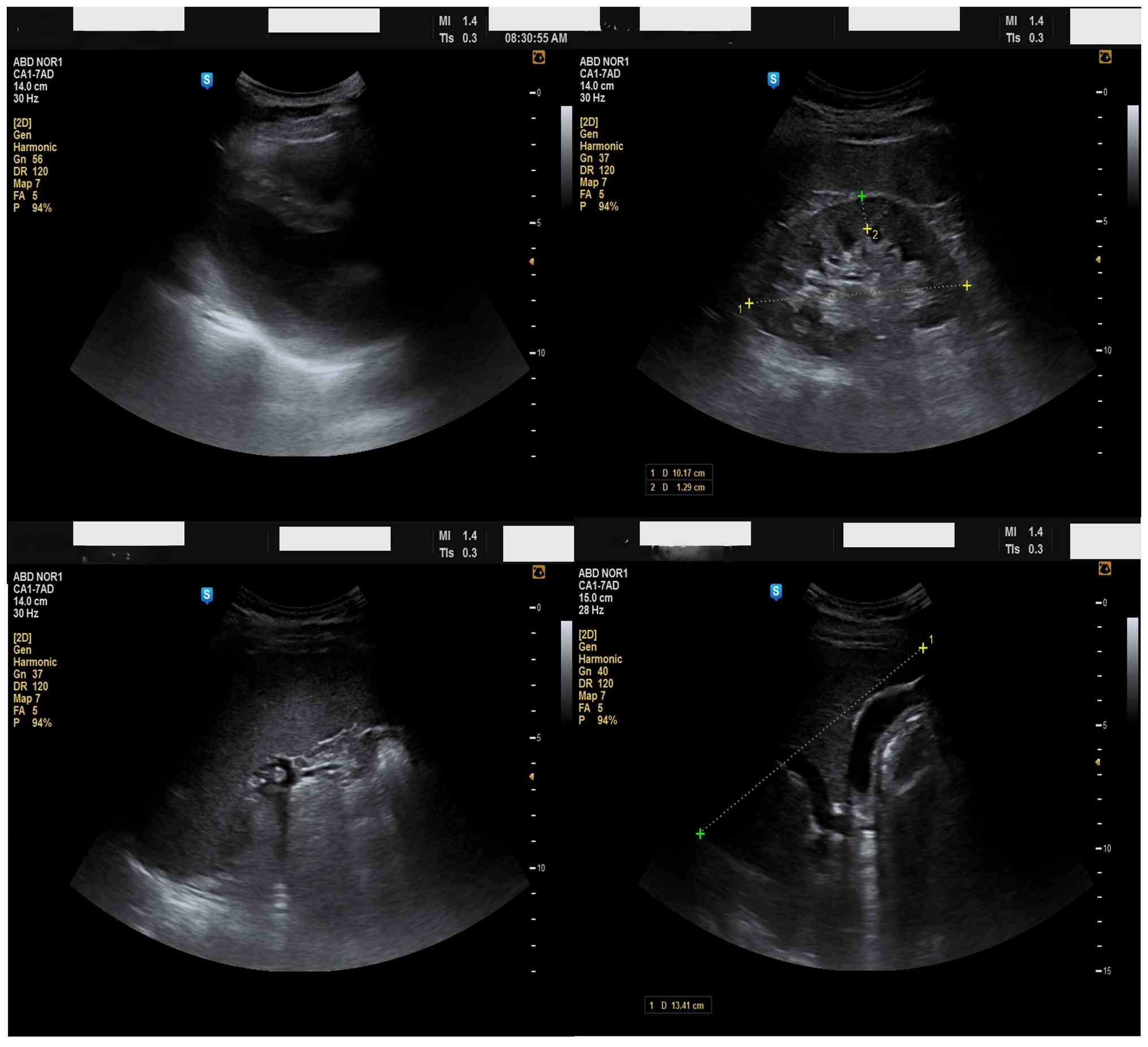
decreasing R-wave amplitude from V1 to V6 (Fig. 2). Ultrasonography showed the spleen
on the right (Fig. 3) (splenomegaly
14.5 cm), with normal kidneys, consistent with situs inversus
totalis.
Baseline laboratory investigations were also
performed. Hematology showed a white blood cell count of
4,910/mm3 (normal 4,000-10,500/mm3), a red
blood cell count of 4.29 million/mm3 (normal range,
4.5-5.9 million/mm3) hemoglobin 12.5 g/dl (normal range,
13.5-17.5 g/dl), a packed cell volume of 38.2% (normal range,
41-53%) and a platelet count of 1.64 lakh/mm3 (normal
range, 150-400 lakh/mm3). The differential count
revealed 65% neutrophils (normal range, 40-70%), 31% lymphocytes
(normal range, 20-40%) and 2% monocytes (normal range, 2-8%), with
absent eosinophils (normal range, 1-4%) and basophils (normal
range, 0-1%). Biochemical tests showed normal renal and liver
function, with 0.9 mg/dl serum creatinine (normal range, 0.7-1.3
mg/dl), 9.4 mg/dl urea (normal range, 20-40 mg/dl) and 3.2 mg/dl
uric acid (normal range, 3.5-7.2 mg/dl). Inflammatory markers,
including erythrocyte sedimentation rate and C-reactive protein,
were within normal limits, and troponin-I was negative, ruling out
myocardial ischemia.
Serological screening for infectious diseases was
negative, including hepatitis B surface antigen, human
immunodeficiency virus 1/2, hepatitis C virus and dengue virus
[non-structural protein 1 antigen, immunoglobulin (Ig)M and IgG
antibodies]. Urine analysis was normal, with no evidence of
proteinuria, hematuria or infection.
These electrocardiogram (ECG) findings are
characteristic of dextrocardia with situs inversus, which
helps in diagnosing the condition. The distinct ECG findings,
combined with clinical examination and imaging studies, allowed for
a comprehensive understanding of the patient's unique anatomical
and physiological presentation.
Outcome and follow-up
The patient was managed with symptomatic treatment,
including paracetamol for fever and expectorants for the cough.
Paracetamol was provided at 500 mg every 6 h for 3 days and
bromhexine was provided at 8 mg three times a day for 3 days. No
specific cardiac therapy was required, as echocardiography
confirmed normal cardiac function. The patient was referred to the
Departments of Cardiology and Pulmonology for further evaluation
and follow-up. The respiratory symptoms of the patient improved
during the hospital stay, and was discharged in stable condition.
At the 3-month follow-up in August 2023, the patient remained
asymptomatic and repeat echocardiography showed normal findings. No
features were present to suggest Kartagener syndrome, and genetic
testing was not pursued. The patient was educated about the
implications of situs inversus for emergency and surgical
care, and was advised to wear a medical alert bracelet.
Discussion
The present case emphasizes the importance of
combining physical examination with electrocardiographic and
imaging findings when diagnosing dextrocardia with situs
inversus, especially in patients who present with non-specific
symptoms. The present patient, a young adult with no known
comorbidities, showed normal cardiac anatomy and function despite a
complete mirror-image arrangement of the thoracoabdominal organs.
The present case highlights the significance of recognizing unique
ECG abnormalities that could otherwise lead to misinterpretation
and unnecessary testing. Such clinical vigilance is vital to
prevent diagnostic errors and overtreatment.
In the present study, differential diagnoses
considered at presentation included pneumonia, bronchitis,
tuberculosis, congenital heart disease, pericarditis,
gastroesophageal reflux disease and cholecystitis. These were
excluded based on normal inflammatory markers, negative serology
and supportive imaging studies, which confirmed situs inversus
totalis with dextrocardia and no structural cardiac
defects.
Dextrocardia with situs inversus presents a
unique diagnostic challenge due to its frequent association with
congenital cardiac anomalies. When dextrocardia is associated with
situs solitus, the incidence of notable cardiac defects,
such as atrial septal defects, ventricular septal defects and the
transposition of the great vessels, is high, reaching 90-95%
(6-8).
By contrast, patients with situs inversus totalis, as in the
present case, often have structurally normal hearts, although other
anomalies may still be present.
Associated defects in situs inversus may go
beyond the cardiovascular system and include duodenal atresia
(OMIM: 223400), asplenism (OMIM: 271400) or polysplenia, ectopic or
horseshoe kidneys and various pulmonary abnormalities, such as
chronic sinopulmonary infections and bronchiectasis (8). The presence of situs inversus
along with primary ciliary dyskinesia (OMIM: 613807) leads to
Kartagener syndrome, which is characterized by chronic sinusitis,
bronchiectasis and infertility caused by impaired ciliary function
(9,10).
The cause of laterality defects such as dextrocardia
with situs inversus remains multifactorial. Genetic factors,
including mutations in the DNAH5 gene, are essential in disrupting
left-right asymmetry during embryogenesis (11). Environmental influences such as
maternal diabetes, teratogenic exposure and rare cases of conjoined
twinning have also been linked (11,12).
Management requires a multidisciplinary approach
tailored to the patient's specific anatomical and functional
anomalies. A comprehensive cardiac evaluation using
echocardiography and ECG is essential for detecting structural or
electrical abnormalities (1,2).
Respiratory assessments and physiotherapy become particularly
important in patients with suspected or confirmed Kartagener
syndrome (9,10).
When surgical intervention is needed, careful
attention should be paid to reversed organ orientation to prevent
intraoperative errors. Genetic counseling should be provided to
affected individuals and their families, especially those planning
future pregnancies, to understand hereditary risks and implications
(11-13).
Advances in diagnostic imaging and genetic testing have greatly
improved early detection and enabled personalized treatment
strategies.
The present case report highlights the educational
importance of recognizing such rare congenital conditions and
stresses the need for a high index of suspicion in atypical
clinical cases. Early detection, proper referral and structured
follow-up are essential for improving outcomes in patients with
dextrocardia and situs inversus.
Acknowledgements
Not applicable.
Funding
Funding: No funding was received.
Availability of data and materials
The data generated in the present study may be
requested from the corresponding author.
Authors' contributions
ND contributed to the conception and design of the
study, participated in data collection, analysis and
interpretation, conducted the literature review, and drafted the
manuscript. MHS contributed to data collection, as well as the
analysis and interpretation of the patient data. SCMR contributed
to the conception and design of the study, participated in the
interpretation of clinical findings, and critically revised the
manuscript for important intellectual content, providing
substantial scientific input that shaped the discussion and
clinical interpretation. KHLG contributed to the interpretation of
patient data and clinical decision-making aspects of the case, and
critically revised the manuscript for important intellectual
content with significant academic and clinical input. ND and KHLG
confirm the authenticity of all the raw data. All authors have read
and approved the final manuscript and agree to be accountable for
all aspects of the work.
Ethics approval and consent to
participate
Not applicable.
Patient consent for publication
The patient consented to the publication of the case
report and the associated images.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Deshimo G, Abebe H, Damtew G, Demeke E and
Feleke S: A case report of dextrocardia with Situs inversus:
A rare condition and its clinical importance. Case Rep Med.
2024(2435938)2024.PubMed/NCBI View Article : Google Scholar
|
|
2
|
Karki S, Khadka N, Kashyap B, Sharma S,
Rijal S and Basnet A: Incidental finding of dextrocardia with
Situs inversus and absent left kidney: A case report. JNMA J
Nepal Med Assoc. 60:196–199. 2022.PubMed/NCBI View Article : Google Scholar
|
|
3
|
Bellchambers HM and Ware SM: ZIC3 in
heterotaxy. Adv Exp Med Biol. 1046:301–327. 2018.PubMed/NCBI View Article : Google Scholar
|
|
4
|
Balbino M, Montatore M, Masino F and
Guglielmi G: Kartagener's syndrome: A rare condition diagnosed in a
young male patient. Radiol Case Rep. 19:2741–2744. 2024.PubMed/NCBI View Article : Google Scholar
|
|
5
|
Rao PS and Rao NS: Diagnosis of
dextrocardia with a pictorial rendition of terminology and
diagnosis. Children (Basel). 9(1977)2022.PubMed/NCBI View Article : Google Scholar
|
|
6
|
Madan KK, Babu C, Chander S, Kumar A,
Balchander J and Nachipaan M: Complete A-V canal defect with
dextrocardia with CCTGA-A case report. IJTCVS. 19(55)2003.
|
|
7
|
Iino K, Watanabe G, Ishikawa N and Tomita
S: Total endoscopic robotic atrial septal defect repair in a
patient with dextrocardia and situs inversus totalis.
Interact CardioVasc Thorac Surg. 14:476–477. 2012.PubMed/NCBI View Article : Google Scholar
|
|
8
|
Piryani RM, Shukla A, Prasad DN, Kohli SC,
Shrestha G and Singh D: Situs inversus with dextrocardia
with multiple cardiac lesions in adult. Kathmandu Univ Med J
(KUMJ). 5:247–249. 2007.PubMed/NCBI
|
|
9
|
Ortega HA, Vega NDA, Santos BQ and Maia
GT: Primary ciliary dyskinesia: Considerations regarding six cases
of Kartagener syndrome. J Bras Pneumol. 33:602–608. 2007.PubMed/NCBI View Article : Google Scholar : (In English,
Portuguese).
|
|
10
|
Holzmann D, Ott PM and Felix H: Diagnostic
approach to primary ciliary dyskinesia: A review. Eur J Pediatr.
159:95–98. 2000.PubMed/NCBI View Article : Google Scholar
|
|
11
|
Olbrich H, Häffner K, Kispert A, Völkel A,
Volz A, Sasmaz G, Reinhardt R, Hennig S, Lehrach H, Konietzko N, et
al: Mutations in DNAH5 cause primary ciliary dyskinesia and
randomization of left-right asymmetry. Nat Gente. 30:143–144.
2002.PubMed/NCBI View
Article : Google Scholar
|
|
12
|
Agirbashi M, Hamid R, Jennings HS III and
Tiller GE: Situs inversus and hypertrophic cardiomyopathy in
identical twins. Am J Genet. 91:327–330. 2000.PubMed/NCBI
|
|
13
|
Distefano G, Romeo MG, Grasso S, Mazonne
D, Sciacca P and Mollica F: Dextrocardia with and without situs
viscerum inversus in two sibs. Am J Med Genet. 27:929–934.
1987.PubMed/NCBI View Article : Google Scholar
|