Introduction
Perioperative neurocognitive disorders (PNDs)
represent a spectrum of cognitive impairments that occur in
association with anesthesia and surgery. A multidisciplinary
consensus working group in 2018 recommended the term PND as an
overarching classification that includes pre-existing cognitive
impairment, postoperative delirium, delayed neurocognitive
recovery, and postoperative neurocognitive disorder (1). This updated nomenclature aligns
perioperative cognitive research with Diagnostic and Statistical
Manual of Mental Disorders-5 neurocognitive disorder terminology
and aims to standardize the description of cognitive changes
occurring before or following surgery (2).
Postoperative cognitive dysfunction (POCD), a term
historically used in perioperative research, refers to a measurable
decline in cognitive domains such as memory, attention, and
executive function following surgery and anesthesia (1). It is prevalent in older patients and
has been increasingly observed after major surgeries, including
cardiac surgery (1,3). The incidence of POCD following cardiac
surgery is 10-40% of patients at 6 weeks post-surgery, and recovery
is not always complete; ~45% of these patients achieve full
recovery within 1 year (1). POCD is
associated with delayed surgical recovery, prolonged hospital
stays, impaired activities of daily living, and a lower likelihood
of independent living (4). For
example, patients developing POCD following cardiac surgery have
over twice the relative risk of death (~2.04) compared with
non-POCD patients and experience an additional average hospital
stay of 1-2 days (4). These
findings underscore the health costs and morbidity associated with
POCD in patients undergoing cardiac surgery. As populations age and
more cardiac surgery is performed, the morbidity burden from POCD
is expected to rise.
Accurate POCD identification relies on standardized
neurocognitive testing (1,4). A comprehensive battery covering
multiple cognitive domains is ideal, but in practice, simpler
screening tools are typically used. The most widely used brief
cognitive test in perioperative literature is the Mini-Mental State
Examination (MMSE) (5). The
30-point MMSE is applied to measure global cognitive function
(orientation, memory, language, visuospatial), but was not designed
to detect the more subtle changes of POCD (6). The MMSE has limitations as a POCD
screen: it is not sensitive to mild impairment and under-identifies
cognitive decline in surgical patients (7). For example, 15% of elderly patients
were classified as cognitively impaired using the MMSE (cutoff
<24), whereas 33% were identified as impaired when applying the
more stringent Montreal Cognitive Assessment criteria (6-7).
Similarly, poor sensitivity and lack of validated cutoffs have been
found in other analyses for perioperative cognitive screening using
MMSE (6-7). Studies relying on the MMSE may
underestimate the true incidence of POCD, and comparisons between
trials are difficult because different studies use different
cognitive assessment tools.
Variations in reported POCD incidence have arisen
from differences in testing procedures (instruments used, follow-up
timing, and scoring criteria) (7-9).
To the best of our knowledge, few studies have employed a
consistent tool such as the MMSE to compare cognitive outcomes,
particularly in cardiac surgery, directly (10-16).
Therefore, the present systematic review and meta-analysis focusing
on MMSE-based cognitive outcomes following cardiac surgery aimed to
quantify changes in MMSE scores from preoperative baseline to
postoperative follow-up among patients undergoing cardiac surgery,
explore study-level factors associated with variability in
cognitive outcomes, and evaluate the methodological characteristics
of MMSE use across studies.
Materials and methods
Data sources and search strategy
The present systematic review was conducted in
accordance with the Preferred Reporting Items for Systematic
Reviews and Meta-Analyses (PRISMA 2020) guidelines (9). The study methods, inclusion criteria,
and analysis plan were defined a priori before the
literature search and data extraction.
MEDLINE/PubMed (pubmed.ncbi.nlm.nih.gov/), Embase (https://www.embase.com/), Cumulative Index to Nursing
& Allied Health Literature (about.ebsco.com/products/research-databases/cinahl-database),
the Cochrane Library (https://www.cochranelibrary.com/), PsycINFO
(https://www.apa.org/pubs/databases/psycinfo), Web of
Science (https://mjl.clarivate.com/home), and Scopus
(https://www.scopus.com/sources) were
searched for relevant literature from inception until May 2025
without regard to date or language. Search terms (Data S1) for ‘cardiac surgery’ [such as
coronary artery bypass grafting (CABG), valve, or aortic surgery],
‘postoperative cognitive dysfunction’, and ‘Mini-Mental State
Examination’ combined keywords and MeSH/Emtree terms. The reference
lists of relevant reviews, dissertations, and conference
proceedings were also searched.
Titles, abstracts, and full texts were independently
screened by two reviewers against the predefined inclusion
criteria. Inter-rater agreement during the screening process was
assessed using Cohen's κ statistic after the initial title-abstract
screening stage to quantify reviewer consistency. Any discrepancies
were resolved through discussion or consultation with a third
reviewer.
Inclusion and exclusion criteria
The inclusion criteria for the studies were as
follows: i) Adult patients (age ≥18 years) undergoing cardiac
surgery (CABG, valve, or aortic surgery); ii) cognitive function
assessed using the MMSE both before and after surgery; iii)
sufficient data reported (mean and SD or change scores) to
calculate the standardized mean difference (SMD) and iv) original
clinical studies (randomized trials or observational cohort
studies).
Studies that did not use the MMSE for cognitive
assessment, case reports, reviews, pediatric populations, or
non-cardiac procedures (thoracic surgery, cardiac transplantation,
or transcatheter valve replacement) were excluded. No restriction
on publication year was applied.
Because included studies reported postoperative MMSE
assessments at different follow-up intervals, data were extracted
from the longest postoperative follow-up reported in each study
when multiple time points were available. When studies reported
several clinically distinct follow-up windows (early and late
postoperative assessments), these were considered separate
comparisons in the meta-analysis provided that independent summary
statistics were available.
Data extraction
For subgroup analyses, patients were categorized as
having POCD or not (non-POCD) according to the definitions reported
in the original studies. In the perioperative literature, POCD is
generally defined as a decline in cognitive performance relative to
the patient's preoperative baseline measured using
neuropsychological tests (2).
However, there is currently no universally standardized diagnostic
threshold, and studies typically employ different statistical
approaches to determine cognitive decline (decreases of ≥1-2 SD
from baseline performance, percentage decline in test scores, or
composite indices derived from multiple cognitive tests) (1). POCD classification was therefore based
on the criteria used in the original publications, which typically
relied on postoperative deterioration in cognitive test
performance, assessed using the MMSE or broader neuropsychological
test batteries, relative to baseline values. Because diagnostic
thresholds, testing batteries, and timing of postoperative
assessments vary across studies, study-specific definitions were
used rather than attempting to retrospectively standardize the
classification using a single cutoff, which would not have been
feasible with the available summary data (9).
Data were independently extracted by two
investigators using a pre-piloted standardized form. Extracted
variables included study design (prospective or retrospective;
single-center or multicenter), country and setting, sample size,
patient demographic characteristics (age and sex distribution),
type of cardiac surgery, and timing of MMSE assessment. For each
eligible comparison, the number of participants and the mean MMSE
scores at baseline and postoperative time points or the reported
change in MMSE when available were extracted.
When information was missing or unclear, attempts
were made to contact the study authors for clarification. Any
discrepancies in data extraction were resolved through discussion
until consensus was reached. In addition, key study
characteristics, including differences in surgical procedures,
follow-up intervals, and study design, were recorded to facilitate
interpretation of heterogeneity across studies.
Evaluation of quality
A total of two reviewers independently evaluated
methodological quality using the Critical Appraisal Skills
Programme (CASP) checklist for cohort studies (8). The CASP tool includes 12 items
evaluating study validity, methodological rigor, and relevance
across domains such as selection bias, measurement of outcomes,
confounding control, and applicability. Each item was scored as
‘yes’, ‘no’, or ‘unclear’. Studies were categorized according to
the number of criteria fulfilled as follows: ≥10, good quality;
7-9, fair quality, and ≤6, low quality. Disagreements were resolved
through discussion until a consensus was reached.
Statistical analysis
All meta-analytic computations were conducted using
Comprehensive Meta-Analysis software, version 4 (Biostat, Inc.).
The effect size for postoperative change in cognitive performance
was estimated using SMD (Hedges' g) with corresponding 95%
confidence intervals (CIs). Effect sizes were calculated from the
reported preoperative and postoperative mean MMSE for each cohort.
This approach standardizes the mean difference using the pooled SD
of the two measurements and therefore does not require explicit
imputation of the within-subject association between pre- and
postoperative scores. Because the primary studies did not
consistently report change-score variances or pre-post association,
no fixed correlation coefficient was assumed in the analysis. Where
only medians with ranges or interquartile ranges were reported,
means and SD were estimated using established conversion formulas,
and SD was back-calculated from reported standard errors or CI when
necessary (17).
When primary studies reported >1 eligible
comparison (distinct postoperative follow-up time points or
separate patient strata), each comparison was treated as an
independent effect size when it represented a clinically distinct
contrast with separate summary statistics (means and SD). This
approach allows the meta-analysis to incorporate all available
evidence while preserving the specific clinical context of each
comparison.
To account for anticipated between-study
heterogeneity, a random-effects model was prespecified. Subgroup
analyses were conducted using a mixed-effects approach, in which
random-effects models were applied within each subgroup, while
differences between subgroups were assessed using a fixed-effect
Q_between statistic. Between-study variance (τ²) was estimated
using the DerSimonian-Laird method. Sensitivity analyses were
performed using the Paule-Mandel, Sidik-Jonkman, and restricted
maximum-likelihood estimators, and the Hartung-Knapp-Sidik-Jonkman
adjustment was applied to the pooled variance. Statistical
heterogeneity was quantified using Cochran's Q statistic
(P<0.10), I², τ², and τ. In addition to 95% CI, 95% prediction
interval (PI) was calculated for each pooled SMD to estimate the
range within which the true effect of a comparable future study was
likely to lie.
Robustness of the findings was assessed through
several sensitivity analyses, including leave-one-out influence
analysis, Baujat plots to identify influential comparisons,
comparison with a fixed-effect model, exclusion of studies at
higher risk of bias, and reanalysis using alternative effect-size
metrics (raw MMSE point change). Potential publication bias and
small-study effects were evaluated by visual inspection of funnel
plots of SMDs against their standard errors, Egger's weighted
regression test, and Begg's rank-correlation test (two-tailed
P<0.1) and Duval and Tweedie's trim-and-fill method when
asymmetry was detected to estimate the number of potentially
missing studies and generate an adjusted pooled effect size. In
addition, Rosenthal's and Orwin's fail-safe N statistics were
calculated to estimate how many null studies would be required to
overturn the overall result.
P<0.05 was considered to indicate a statistically
significant difference, and all tests were two-tailed unless
otherwise specified (P<0.10 for Cochran's Q and funnel-plot
asymmetry tests). CI, PI, and test statistics were based on the
t-distribution with k-1 degrees of freedom (df).
Results
Search strategy outcome
The systematic database search identified 1,564
records. Following removal of 312 duplicates, 1,252 titles and
abstracts were screened, of which 1,160 were excluded for not
meeting the criteria (non-cardiac surgery, pediatric populations or
absence of a cognitive outcome; Fig.
1). In total, 72 full-text articles were assessed for
eligibility and 64 were excluded for the following reasons: No MMSE
data (n=21), review, editorial or conference abstract (n=13),
ineligible study design (no original data; n=12), mixed surgical
cohorts without extractable cardiac subgroup data (n=10) and
duplicate or overlapping populations (n=8). In total, eight studies
met the eligibility criteria and were included in the qualitative
synthesis (10-16,18),
yielding 14 independent comparisons (distinct patient groups, time
points, or surgical strata).
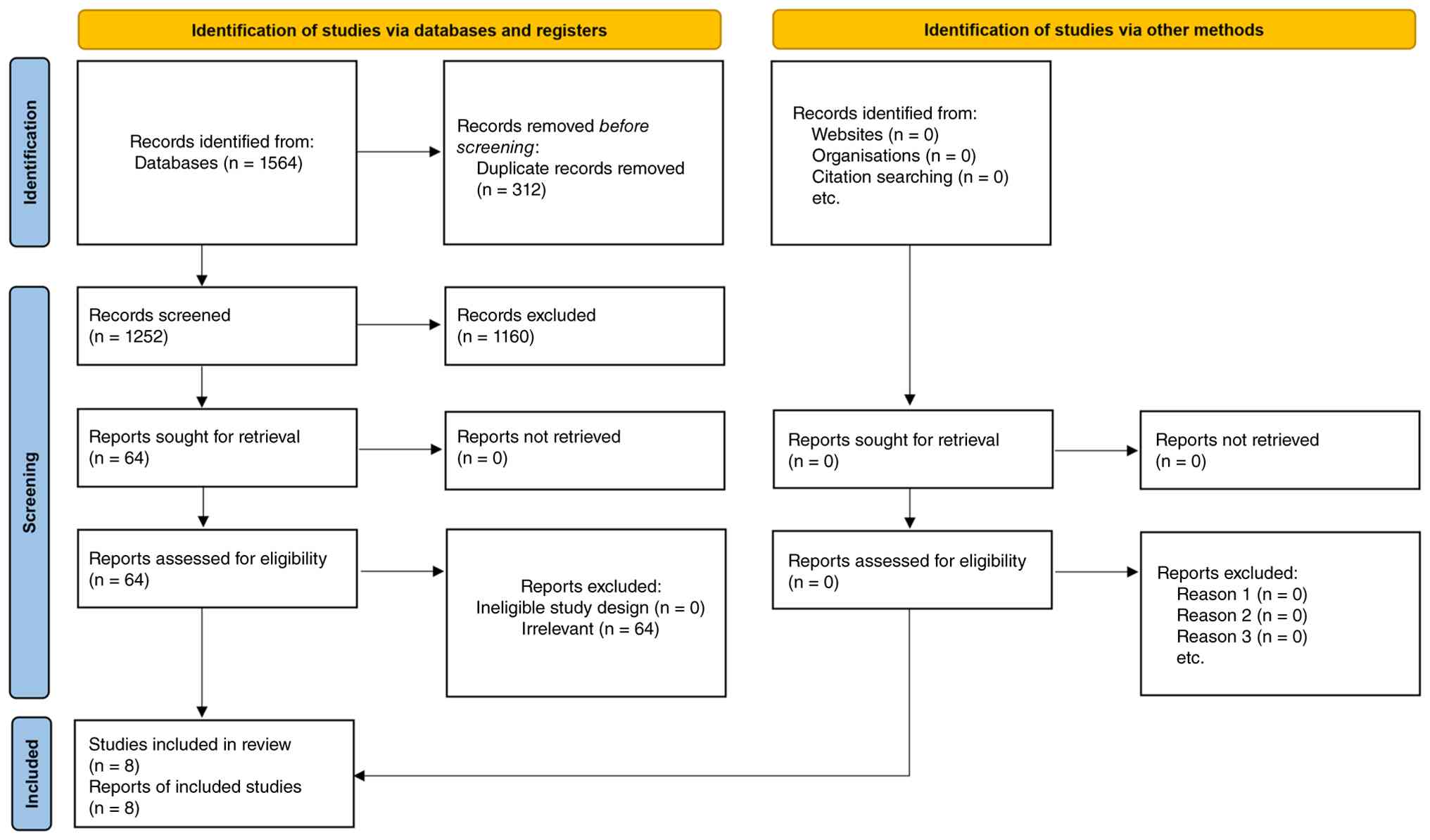 | Figure 1PRISMA flow diagram of study
selection. Of 1,564 records identified and 24 additional references
from manual search, 312 duplicates were removed, leaving 1,252
titles/abstracts for screening. Following exclusion of 1,160
ineligible citations, 72 full-text articles were assessed; 64 were
excluded for predefined reasons (no Mini-Mental State Examination
data, n=21; review/editorial/abstract, n=13; ineligible study
design, n=12; mixed cohorts without extractable cardiac subgroup,
n=10; overlapping populations, n=8). In total, eight studies met
all criteria and yielded 14 independent pre/post comparisons
included in qualitative and quantitative synthesis. |
General characteristics of the
included studies
All eight studies (10-16,18)
were prospective single-center cohorts published between 2005 and
2024; four were conducted in Japan (10-13),
with one each in India (16),
Sweden (14), China (18), and Malaysia (15). A total of 867 patients (sample size
range, 28-280) undergoing on-pump CABG or valve surgery were
analyzed. Mean or median age was between 60 and 65 in the Japanese
(10-13)
and Swedish (14) cohorts and ~50
years in the Chinese valve cohort (18); the overall proportion of male
patients was ~70%, but was lower (39%) in the study by Zhang et
al (18). All studies assessed
MMSE scores pre-operatively and at ≥1 early postoperative time
point [within the first postoperative week or at hospital discharge
in six studies, 2 weeks in Maekawa et al (13), and 6 weeks in Yazit et al
(15)]. Several cohorts also
included longer follow-up assessments up to 6 months (Table I) (10). Postoperative cognitive assessment
spanned the very early phase (≤1 week), an intermediate window (2
weeks), and a later window (6 weeks-6 months), yielding 14
independent comparisons included in the meta-analysis. Baseline
MMSE scores ranged from 26 to 29 points, indicating generally
preserved preoperative cognitive function across the
populations.
 | Table ICharacteristics of the studies
included in the systematic review and meta-analysis. |
Table I
Characteristics of the studies
included in the systematic review and meta-analysis.
| First author,
year | Design/setting | Country | Sample size | Mean age,
years | Male, % | Cardiac
procedure | Baseline MMSE | Post-operative
MMSE | (Refs.) |
|---|
| Kadoi and Goto,
2006 | Prospective cohort,
single center | Japan | 88 | NR | NR | On-pump CABG | NR | 6 mo: 41.5±4.1 | (10) |
| Kadoi et al,
2011 | Prospective cohort,
single center | Japan | 90 | 65±9 | 76 | On-pump CABG | 28.6±1.9 | POD7: 26.5±2.4; 6
mo: 27.9±2.1 | (11) |
| Kadoi et al,
2005 | Prospective cohort,
single center | Japan | 280 | 64±11 | 78 | On-pump CABG | 28.5±1.7 | POD7: 26.7±2.3; 6
mo: 27.9±2.0 | (12) |
| Maekawa et
al, 2014 | Prospective cohort,
single center | Japan | 28 | ≥60 | NR | CABG/valve | 26.8±1.9 | 2 wk: 24.4±2.1 | (13) |
| Veliz-Reissmüller
et al, 2007 | Prospective
cohort | Sweden | 103 | ≥60 | NR | CABG ± valve | Median, 29.0 (IQR
NR) | Discharge median,
26.5 (delirium group) | (14) |
| Yazit et al,
2024 | Prospective
cohort | Malaysia | 188 | NR | NR | Mixed cardiac
surgery | 27.5±2.5 | Discharge:
26.3±4.0; 6 wk: 27.4±3.6 | (15) |
| Shiraboina et
al, 2014 | Prospective
cohort | India | 62 | NR | 62 | CABG/AVR | NR | POD7 proportion
≤24 | (16) |
| Zhang et al,
2021 | Prospective
cohort | China | 71 | 51 (45-55) | 39 | Valve surgery with
CPB | 28.2±1.6 | POD7: 27.4±2.2 | (18) |
Quantitative synthesis of pre- vs.
postoperative cognitive function via MMSE
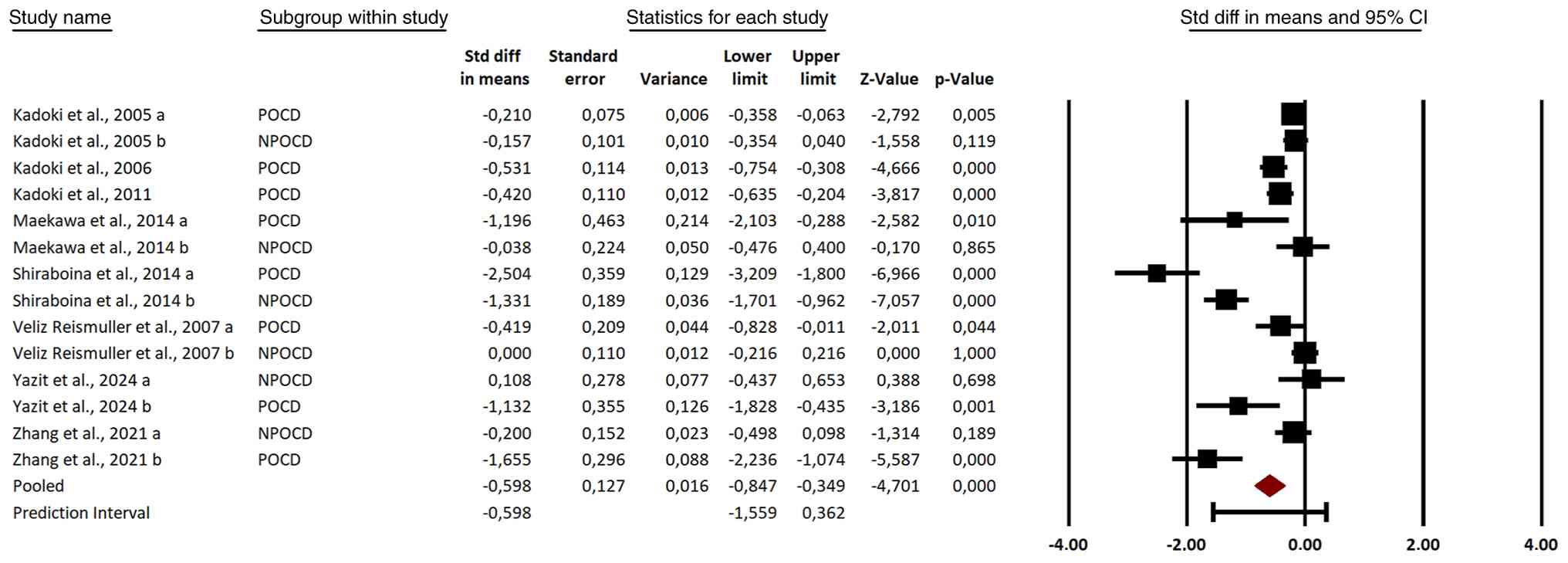
Cardiac surgery was associated with a significant
decline in MMSE (Hedges g=-0.60, 95% CI -0.85 to -0.35, P<0.001;
Fig. 2). For clinical
interpretability, the pooled standardized effect size was
translated into an approximate change in raw MMSE points. Using the
typical baseline SD reported across the included cohorts (~3 MMSE
points), the pooled effect size (g=-0.60) corresponded to an
estimated decline of 1-2 points on the 30-point MMSE scale.
Between-study heterogeneity was notable (τ²=0.178, τ=0.422;
Q=116.4, df=13, P<0.001; I²=88.8%). The 95% PI (-1.56 to 0.36)
spanned both negative and slightly positive values, indicating that
while most cohorts are expected to show cognitive decline, the
inclusion of values above zero suggests that small improvements
remain possible in some populations. A fixed-effect model yielded a
smaller but significant estimate (g=-0.35, 95% CI -0.43 to -0.27,
P<0.001).
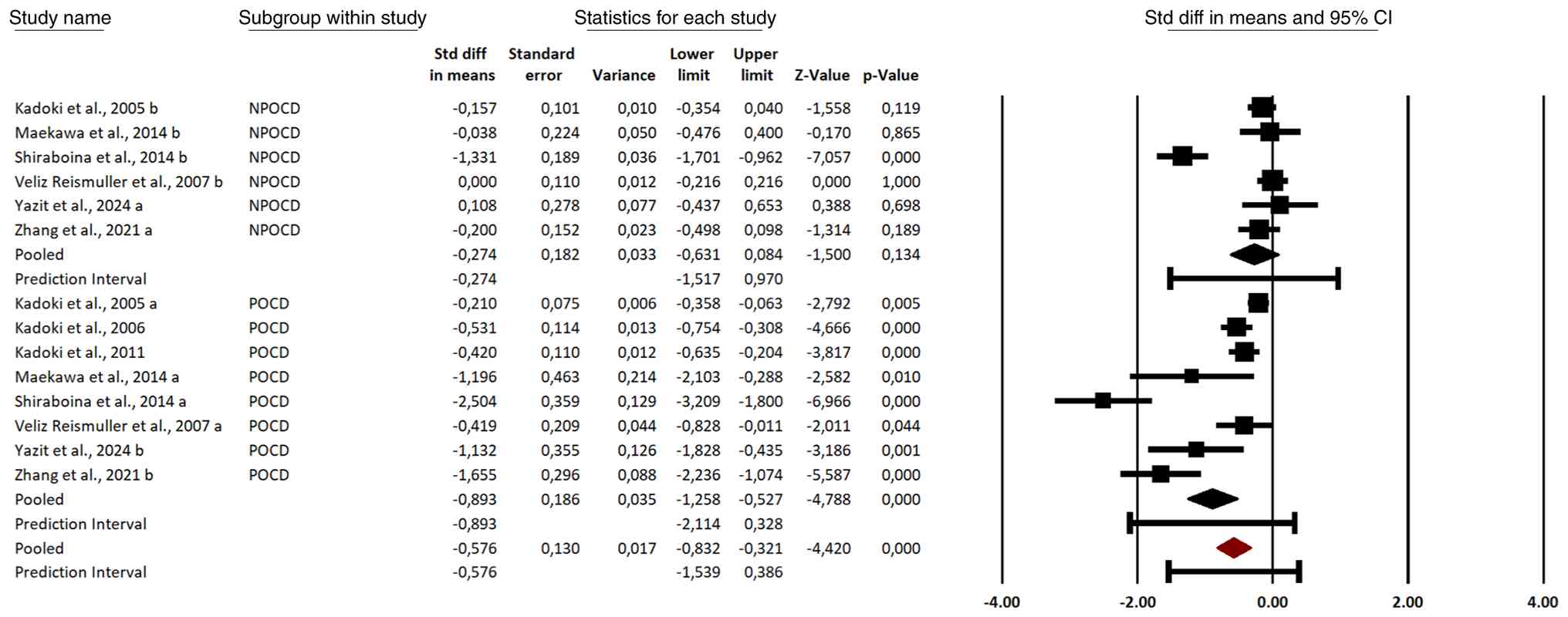
Subgroup analysis
Using the prespecified mixed-effects model, patients
who developed POCD (eight comparisons) showed a significant decline
in MMSE scores (Hedges' g=-0.893, 95% CI -1.258 to -0.527;
P<0.001; 95% PI -2.114 to 0.328), whereas patients without POCD
(six comparisons) showed a non-significant change (g=-0.274, 95% CI
-0.631 to 0.084; P=0.134; 95% PI, -1.517 to 0.970; Fig. 3). Heterogeneity was high in both
subgroups (I²=88-89%), but the between-group test showed a
significant difference in effect sizes (Q_between=9.08, df=1,
P=0.003). Across all 14 comparisons, the pooled mixed-effects
estimate was g=-0.576 (95% CI -0.832 to -0.321; P<0.001; 95% PI
-1.539 to 0.386), indicating that the overall postoperative decline
was driven primarily by the subgroup with clinical POCD.
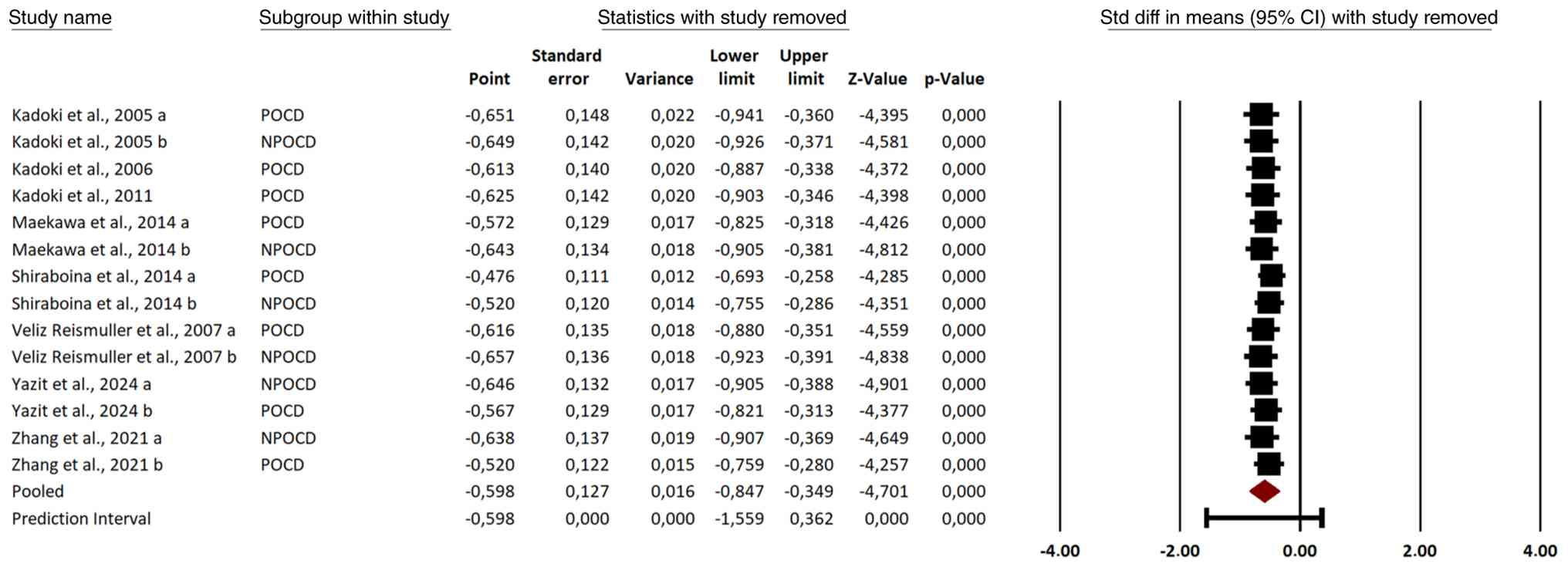
Sensitivity analysis
Sequential leave-one-out sensitivity analysis showed
that omission of any single comparison changed the pooled
standardized mean difference by <0.08. In every iteration, the
pooled estimate remained negative and significant (all P≤0.002),
indicating that the overall result was not driven by any individual
comparison (Fig. 4). Taken
together, these findings support the robustness of the conclusion
that cardiac surgery was associated with a significant
postoperative decline in MMSE score.
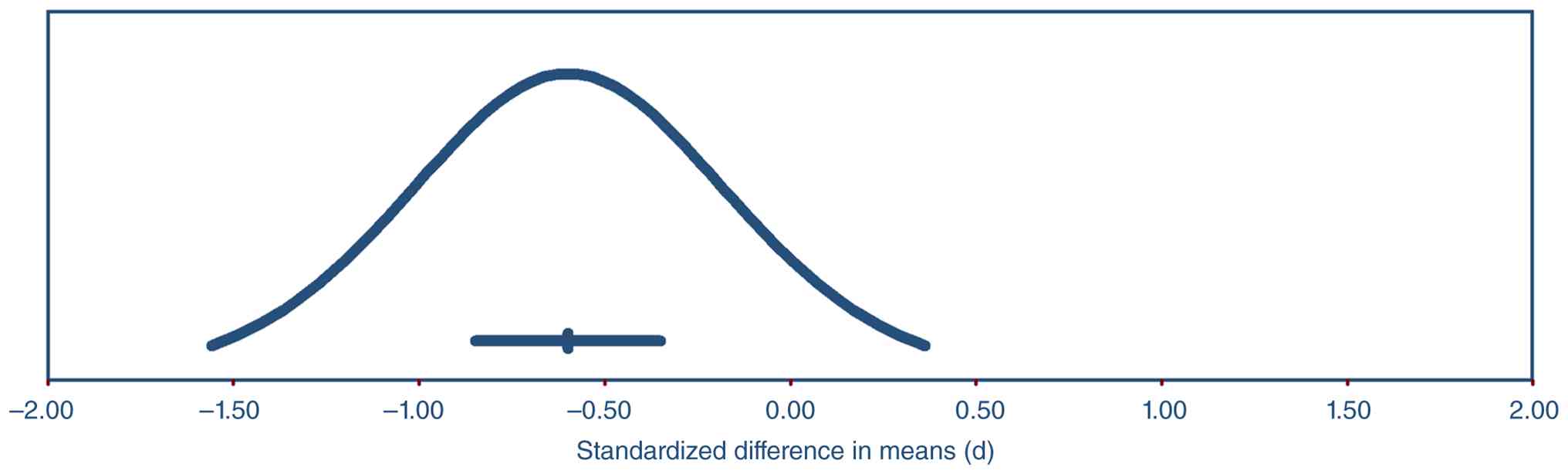
Heterogeneity assessment using PI
analysis
For the primary random-effects model (14
comparisons), the 95% PI ranged from -1.56 to 0.36 SMD units (with
the null value falling within the interval), indicating that most
future studies of similar design are likely to observe a
postoperative decline in MMSE, although a small improvement remains
possible in certain cohorts (Fig.
5). The subgroup analyses supported this pattern. Specifically,
cohorts consisting primarily of patients with POCD are expected to
report a marked cognitive decline, whereas studies including only
patients without POCD may plausibly observe outcomes ranging from a
modest decline to a modest improvement.
The range of the PI reflects substantial
between-study heterogeneity; its predominantly negative
distribution supports the overall conclusion that cognitive
performance, as measured by the MMSE, generally declined following
on-pump cardiac surgery.
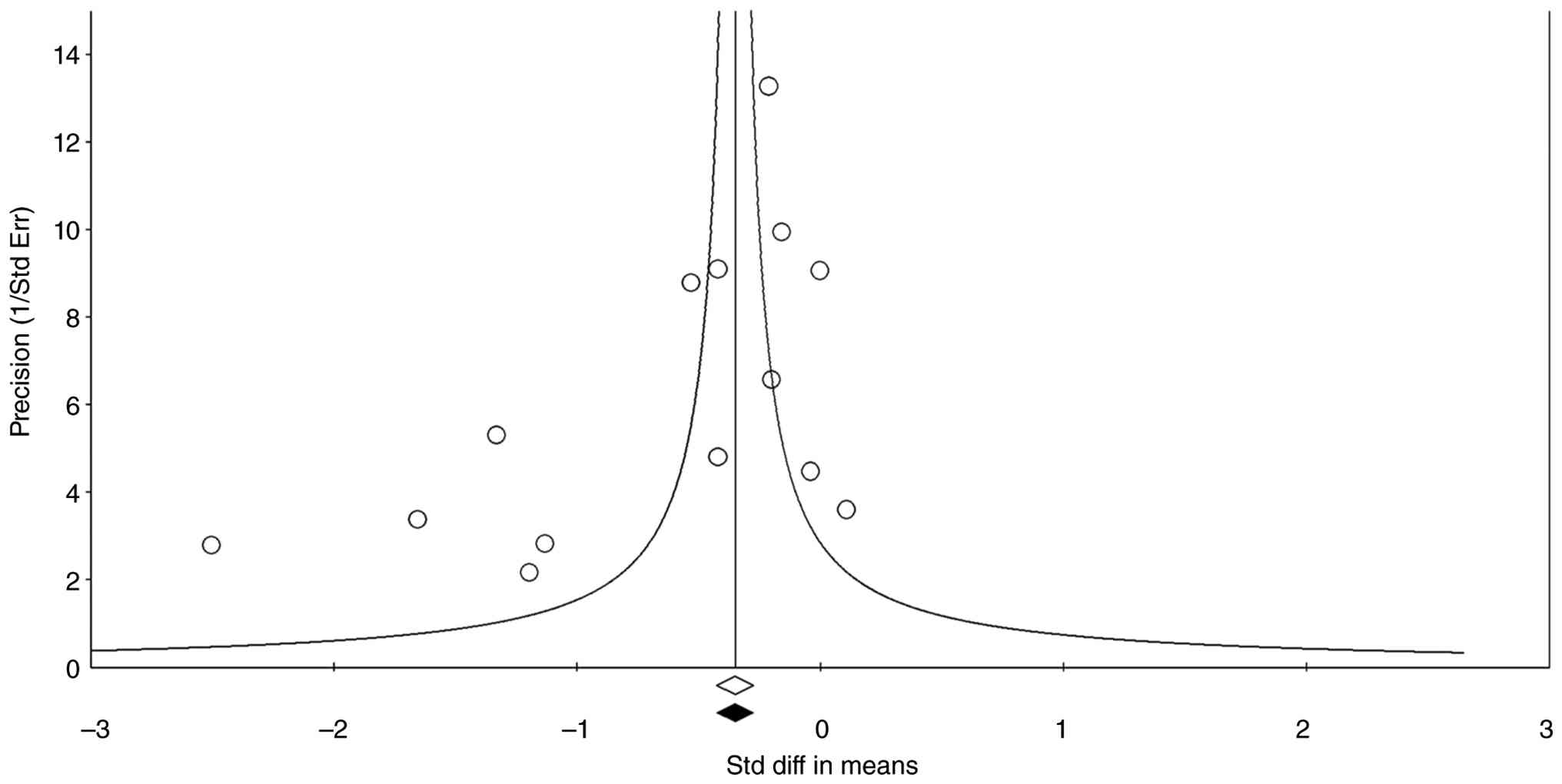
Publication bias assessment
Visual inspection of the funnel plot (Fig. 6) suggested an absence of large
studies reporting null effects, which was supported by statistical
tests. Egger's regression test yielded an intercept of -3.69 (95%
CI -6.81 to -0.58; P=0.024), and Begg and Mazumdar's
rank-correlation test indicated significant asymmetry (Kendall's
τ=-0.43, z=2.14; two-tailed P=0.033). Despite this asymmetry, Duval
and Tweedie's trim-and-fill procedure did not identify any
potentially missing studies (k_trimmed=0), and the bias-adjusted
random-effects estimate was unchanged compared with the original
pooled estimate (Hedges' g=-0.598, 95% CI -0.847 to -0.349).
Rosenthal's classic fail-safe N indicated that 431
additional null studies would be required to increase the pooled
P-value to >0.05, exceeding the conventional tolerance threshold
(5 x k + 10=80). Together, these analyses suggest that although
small-study effects may be present, they were unlikely to
materially alter the conclusion that cardiac surgery is associated
with a significant postoperative decline in MMSE score.
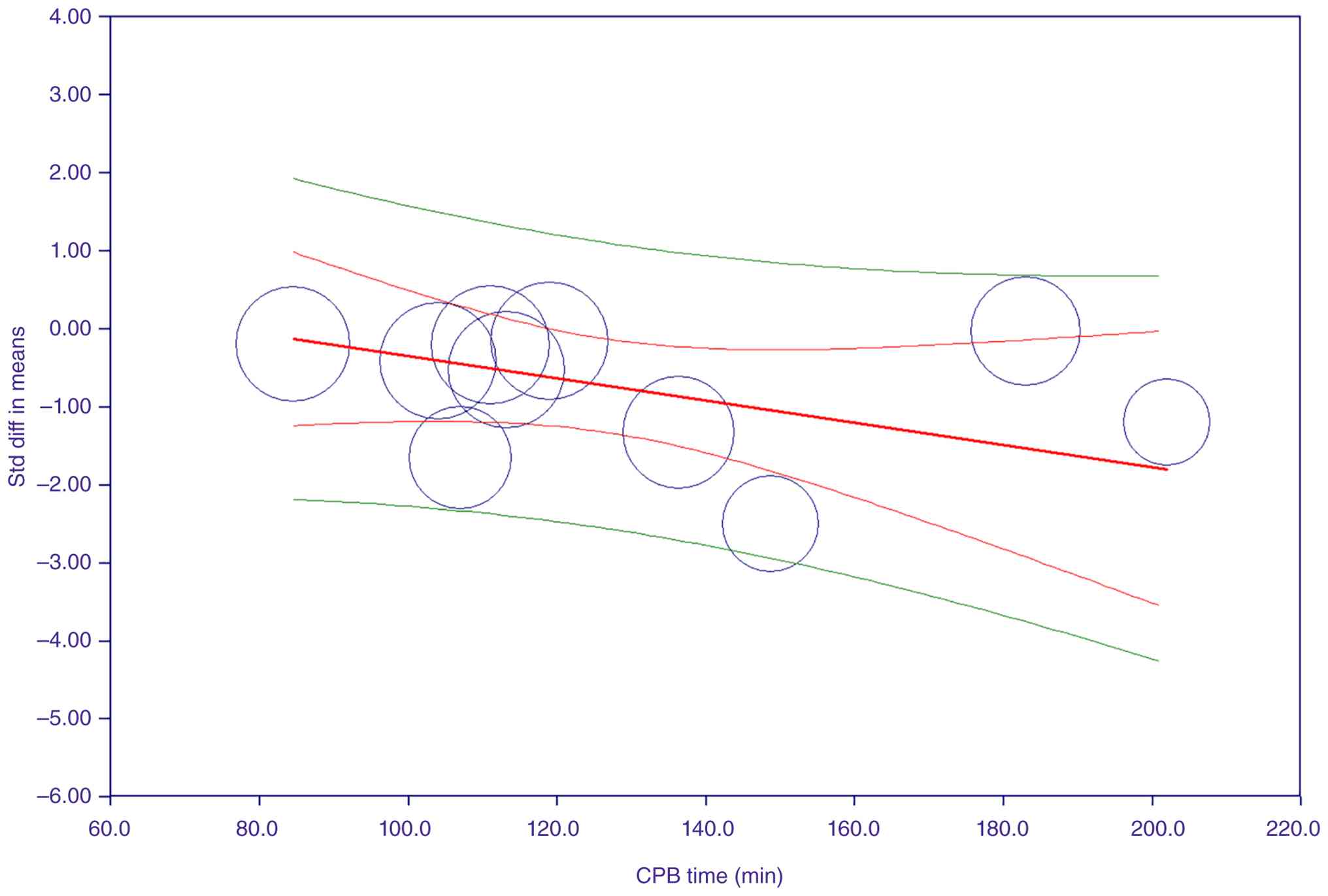
Meta-regression (moderator
analysis)
To explore sources of the large between-study
heterogeneity (τ²=0.178; I²=~89%), mixed-effects meta-regression
analysis was performed, including five a priori clinical
moderators: Mean age, cardiopulmonary bypass (CPB) time,
study-level prevalence of hypertension and diabetes mellitus, and
male sex. The simultaneous (multivariable) model was significant
(Q_model=11.22, df=5, P=0.047) and accounted for part of the
between-study heterogeneity, although only CPB time was an
independent predictor (Table II).
Specifically, each 1 min increase in CPB duration was associated
with an additional decline of 0.014 SD units in MMSE scores
(β=-0.014±0.006, Z=-2.27, P=0.023), corresponding to ~0.9 SD
greater decline for 1 h additional bypass time.
| Table IIMultivariable meta-regression of
mini-mental state examination change after cardiac surgery. |
Table II
Multivariable meta-regression of
mini-mental state examination change after cardiac surgery.
| Moderator
(k=14) | β (SMD-units) | 95% CI | Z-value | P-value |
|---|
| Intercept | -2.3838 | -6.673 to
1.905 | -1.09 | 0.276 |
| Age | +0.0642 | -0.016 to
0.145 | 1.56 | 0.118 |
| CPB time | -0.0143 | -0.0265 to
-0.0020 | -2.27 | 0.023 |
| Hypertension | +0.0079 | -0.030 to
0.046 | 0.40 | 0.686 |
| Diabetes | -0.0013 | -0.013 to
0.011 | -0.21 | 0.836 |
| Male | -0.0119 | -0.054 to
0.030 | -0.56 | 0.578 |
When each moderator was entered separately
(univariate models; Table III),
CPB time showed the strongest association and explained ~50% of the
between-study variance (R²_analog=0.50; τ² decreased from 0.198 to
0.100; Q=18.68, P=0.0001), whereas age explained ~29% of the
heterogeneity (Q=7.23, P=0.007). The remaining covariates
contributed little to explaining the variability across
studies.
| Table IIIExplained heterogeneity in separate
(one-predictor) models. |
Table III
Explained heterogeneity in separate
(one-predictor) models.
| Model | τ² | R² | Qmodel
(df=1) | P-value |
|---|
| Intercept only | 0.198 | - | - | - |
| Intercept +
age | 0.140 | 29 | 7.23 | 0.007 |
| Intercept + CPB
time | 0.100 | 50 | 18.68 | 0.001 |
| Intercept +
hypertension | 0.141 | 29 | 15.17 | 0.002 |
| Intercept +
diabetes | 0.204 | 0 | 12.17 | 0.016 |
| Intercept +
male | 0.237 | 0 | 11.22 | 0.047 |
Diagnostic plots and jackknife influence analyses
indicated that no single comparison exerted a disproportionate
influence on the regression estimates (largest studentized
residual=2.10; Cook's distance <1 for all points). Furthermore,
no problematic multicollinearity was detected among predictors; the
highest correlation was |r|=0.80 between age and hypertension, and
all variance inflation factors were ≤1.34 (Fig. 7).
Study quality assessment
In total, 5/8 studies achieved good methodological
quality. All of these were prospective single-center cohorts with
clearly stated aims, well-described recruitment, and rigorous
multivariable adjustment; for example, Kadoi et al (12) and Kadoi et al (11) used consensus neuropsychology
batteries and logistic regression. Maekawa et al (13) and Shiraboina et al (16) were graded as fair, chiefly because
short follow-up windows (≤2 weeks) or limited reporting made it
unclear whether all relevant confounders were handled;
nevertheless, both used validated cognitive outcomes (MMSE +
extended batteries) and prospective designs. No study was
downgraded for imprecision (every cohort reported effect sizes with
either CI or full regression output), and the absence of serious
loss to follow-up across studies supported internal validity.
External generalizability was highest for the larger cohorts [Yazit
et al (15), 188 patients;
Kadoi and Goto (10), 280
patients], whereas single-surgeon pilots require cautious
extrapolation. Overall, the evidence base was methodologically
sound, with minor limitations concentrated in the smaller
exploratory studies (Table
IV).
| Table IVCritical Appraisal Skills Program
cohort-study checklist applied to the included studies. |
Table IV
Critical Appraisal Skills Program
cohort-study checklist applied to the included studies.
| First author,
year | Focused issue | Acceptable
recruitment | Exposure
well-measured | Outcome
well-measured | Con-founders
considered | Adequat
follow-up | Clearly stated
results | Precision | Internal
validity | External
applicability | Consistent with
evidence | Practice
implication | Overall rating | (Refs.) |
|---|
| Kadoi and Goto,
2006 | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Good | (10) |
| Kadoi et al,
2011 | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Good | (11) |
| Kadoi et al,
2005 | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Good | (12) |
| Maekawa et
al, 2014 | Y | Y | Y | Y | U | Ua | Y | U | Y | U | Y | U | Fair | (13) |
| Veliz-Reissmüller
et al, 2007 | Y | Y | Y | Y | Y | Y | Y | Y | Y | U | Y | Y | Good | (14) |
| Yazit et al,
2024 | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Good | (15) |
| Shiraboina et
al, 2014 | Y | Y | U | Y | Y | Y | Y | Y | Y | U | Y | U | Fair | (16) |
| Zhang et al,
2021 | Y | Y | Y | Y | Y | Yb | Y | Y | Y | U | Y | U | Good | (18) |
Discussion
The present meta-analysis, which included 14
independent pre/postoperative comparisons and 867 patients,
demonstrated a moderate overall decline in MMSE score following
on-pump cardiac surgery. Although small improvements cannot be
excluded, the 95% PI suggested that most future cohorts may observe
some degree of POCD. Despite notable heterogeneity, the pooled
estimate remained robust across sensitivity analyses and
trim-and-fill procedures, together with a large fail-safe N (431
studies), suggesting that publication bias was unlikely to
meaningfully influence the results.
Cognitive outcomes differed markedly according to
POCD status. Patients meeting formal POCD criteria experienced a
significant decline in MMSE, whereas those without POCD showed only
a non-significant change. These findings indicate that the overall
POCD observed across studies was largely driven by patients who
develop clinically notable neurocognitive impairment.
The pooled standardized effect size corresponded to
a decrease of 1-2 points on the 30-point MMSE scale, which is
consistent with the magnitude of early postoperative cognitive
changes reported in previous studies (19,20).
Greaves et al (19) reported
cognitive impairment in ~43% of patients immediately following
coronary artery bypass surgery, declining to 19% at 6 months but
increasing again to 39% after 5 years. The present results,
therefore, align with the early POCD reported in large
observational cohorts. However, the PI indicated that outcomes may
vary across populations, and small improvements may occur in
certain cohorts, such as patients with impaired cerebral perfusion
who benefit from improved postoperative hemodynamics following
revascularization (21).
Several biological mechanisms have been proposed to
explain postoperative neurocognitive decline following cardiac
surgery (22-24).
Current evidence suggests that perioperative neurocognitive
disorder is multifactorial and involves interactions between
cerebral microembolism, systemic inflammatory activation, and
transient cerebral hypoperfusion during CPB (24). Microembolic particles, including air
bubbles, fat droplets, platelet aggregates, and fragments of
atherosclerotic plaque, may enter the cerebral circulation during
aortic manipulation or extracorporeal circulation, leading to
occlusion of small cerebral vessels and focal neuronal injury
(24). In addition, CPB activates
inflammatory pathways through contact between circulating blood and
artificial circuit surfaces, resulting in complement activation and
the release of pro-inflammatory cytokines such as interleukin-6 and
tumor necrosis factor-α. These inflammatory responses may disrupt
the blood-brain barrier and promote neuroinflammation, which is a
key contributor to POCD (24).
Transient cerebral hypoperfusion and ischemia-reperfusion injury
may exacerbate neuronal vulnerability and impair synaptic function,
contributing to POCD (22-24).
In addition to these established mechanisms,
mitochondrial dysfunction may represent a key downstream pathway in
postoperative neurocognitive decline (25-30).
Surgery, anesthesia, ischemia-reperfusion, and systemic
inflammation can impair mitochondrial respiration, decrease ATP
production, increase oxidative stress, disrupt calcium homeostasis,
and interfere with mitophagy and other mitochondrial
quality-control processes (25,30,31).
These changes may impair synaptic plasticity and neuronal
integrity, thereby contributing to POCD (25). Preclinical and narrative review data
further suggest that modulation of mitochondrial dynamics and
homeostasis may represent a promising therapeutic direction,
although such approaches remain investigational and have not been
established in routine perioperative practice (25-28).
Subgroup analysis confirmed that patients meeting
POCD criteria experienced notably greater cognitive decline than
those without POCD. Notably, the non-POCD subgroup demonstrated a
non-significant reduction in MMSE scores, suggesting that subtle
cognitive changes may occur in patients who do not meet formal
diagnostic thresholds. This is consistent with prior evidence
showing that patients undergoing cardiac surgery without overt
neurocognitive complications may experience modest postoperative
declines in cognitive performance (32). For example, Saczynski et al
(32) reported that patients who
did not develop postoperative delirium demonstrated an average MMSE
reduction of ~2 points in the early postoperative period.
Because the number of available comparisons was
relatively small, the present meta-regression analyses were
considered exploratory and interpreted with caution to minimize the
risk of overfitting. The analysis was conducted using study-level
covariates rather than individual patient data; therefore, the
observed associations represent ecological associations at the
study level and should not be interpreted as causal effects at the
individual level. The present meta-regression analysis identified
CPB duration as the only significant moderator associated with
variability in postoperative MMSE decline. Each additional minute
of CPB was associated with a small increase in cognitive impairment
(33). Prolonged CPB may increase
neurological vulnerability through mechanisms such as increased
embolic load, systemic inflammatory activation, and alterations in
cerebral perfusion (34). However,
CPB duration may also reflect surgical complexity, as longer bypass
times typically occur in patients undergoing more complicated
procedures or combined operations.
Beyond bypass duration, several patient-level and
procedural factors are associated with POCD. In particular,
advanced age has consistently been identified as an important risk
factor (35,36). Older patients may have decreased
cognitive reserve and greater cerebrovascular disease burden, which
may increase vulnerability to perioperative cerebral insult
(37).
From a clinical perspective, several perioperative
strategies have been proposed to mitigate postoperative
neurocognitive complications (38-41).
Multicomponent perioperative care pathways, typically referred to
as delirium prevention bundles, decrease postoperative delirium and
may improve broader neurocognitive outcomes (41). These interventions typically include
early mobilization, measures to promote normal sleep-wake patterns
and maintain patient orientation to their surroundings, adequate
pain control, minimization of sedative medications, and prompt
removal of unnecessary invasive devices (33). In addition, increasing attention has
been directed toward cognitive prehabilitation (42,43),
which aims to enhance cognitive reserve before surgery through
interventions such as cognitive training, optimization of vascular
risk factors, and patient education (38-43).
Intraoperative strategies, including monitoring of anesthetic depth
and cerebral oxygenation, may also contribute to decreasing
neurological injury during cardiac surgery (38-41).
The robustness of the present findings is supported
by methodological strengths, including independent dual data
extraction, high methodological quality among included studies, the
use of both CI and PI, and comprehensive sensitivity analyses.
Furthermore, the use of a uniform cognitive outcome measure (MMSE)
across all studies allowed direct comparison of cognitive changes
across cohorts and avoided the heterogeneity that arises when
different neuropsychological batteries are combined.
However, the present study had several limitations.
First, substantial residual heterogeneity remained despite
moderator analysis, suggesting that additional factors, such as
genetic susceptibility, anesthetic depth, and cerebral
autoregulation, may influence postoperative cognitive outcomes.
Second, follow-up durations were relatively limited, with the
longest postoperative assessment occurring at 6 months, preventing
evaluation of the long-term cognitive trajectory. Third, effect
sizes were derived from reported pre- and postoperative means and
SD; because most primary studies did not report the correlation
between paired measurements, assumptions regarding within-subject
dependence could not be directly verified, which may influence the
precision of standardized effect estimates. Fourth, reliance on the
MMSE may underestimate subtle cognitive impairments, as patients
with mild deficits achieve near-normal total scores, and the test
includes only limited assessment of executive function and
processing speed, which are commonly affected in POCD. In addition,
MMSE performance may be influenced by cultural and educational
factors, which may introduce measurement bias when comparing
heterogeneous populations across countries and healthcare settings.
Fifth, the included studies lacked non-surgical control groups,
making it difficult to distinguish cognitive changes attributable
specifically to cardiac surgery from those associated with aging,
comorbidities, or perioperative hospitalization. Finally,
meta-regression analyses were based on study-level data and a
relatively small number of comparisons, which limited statistical
power and introduced potential ecological bias and residual
confounding. The review protocol was not prospectively registered,
which may decrease transparency. Variability in diagnostic criteria
for POCD across studies may also have introduced misclassification
bias. Although publication bias analyses were performed, the small
number of included studies requires cautious interpretation because
statistical tests for funnel plot asymmetry have limited power when
<10 studies are available.
Overall, cardiac surgery is typically associated
with moderate postoperative cognitive decline, particularly among
patients who develop POCD. Awareness of this risk may support
perioperative cognitive monitoring and targeted prevention
strategies. Patients at higher risk, especially older adults or
those with pre-existing cognitive vulnerability, may benefit from
preoperative cognitive screening and structured postoperative
follow-up. Early cognitive rehabilitation may also be considered
for patients experiencing postoperative cognitive impairment.
The present analysis indicates that on-pump cardiac
surgery is associated with a moderate postoperative decline in MMSE
score, although cognitive outcomes vary across patients and study
populations. Patients who met formal criteria for POCD demonstrated
particularly pronounced declines, whereas individuals without POCD
showed non-significant changes. The present exploratory analyses
also identified longer CPB duration as a study-level factor
associated with greater postoperative cognitive decline, although
this should be interpreted cautiously given the observational
nature of the included studies and the potential for residual
confounding.
The present findings contribute to the growing body
of evidence that PNDs represent a key clinical concern following
cardiac surgery (44-46).
From a clinical perspective, awareness of potential postoperative
cognitive changes may support improved perioperative counseling,
cognitive monitoring, and early identification of patients at
higher risk for neurocognitive complications. More broadly, the
present study supported the integration of perioperative
neurocognitive assessment into cardiac surgical care pathways and
highlighted potentially modifiable intraoperative factors that may
inform future brain-protective strategies. Future research should
focus on strategies aimed at mitigating neurological injury during
cardiac surgery, including optimization of CPB management, improved
cerebral perfusion monitoring, and the evaluation of perioperative
neuroprotective approaches. In addition, longer-term prospective
studies, ideally including appropriate non-surgical control groups,
are needed to clarify whether postoperative cognitive changes
reflect surgery-associated effects, underlying patient
vulnerability, or the natural trajectory of cognitive aging. To the
best of our knowledge, evidence is still lacking regarding the
standardization of cognitive outcome assessment, the role of
mechanistic biomarkers and neuroimaging, and the real-world
feasibility and effectiveness of preventive interventions in
routine perioperative practice. Improved understanding of these
mechanisms and risk factors may facilitate better risk
stratification, targeted preventive interventions, and improved
neurological outcomes for patients undergoing cardiac surgery.
Supplementary Material
Data S1
Acknowledgements
Not applicable.
Funding
Funding: The present study was supported by Chronic Disease
Management Research Project of National Health Commission Capacity
Building and Continuing Education Center (grant no.
GWJJMB202510021111), the Tianshan Talents Program for the
Cultivation of High-Level Medical and Health Professionals (grant
no. TSYC202401B001), the Natural Science Foundation of Xinjiang
Province (grant no. 2024D01C176) and the Young Medical Science and
Technology Talent Project of Xinjiang Provincial Health Commission
(grant no. WJWY-202459).
Availability of data and materials
The data generated in the present study are included
in the figures and/or tables of this article.
Authors' contributions
XL and JWu designed the study, interpreted data, and
drafting of the manuscript. ZH interpreted the data. JWa conceived
and designed the study, interpretation, and critically revised and
finalized the manuscript. XC and JWa confirm the authenticity of
all the raw data. HC conceived and designed the study and
interpreted data. YY performed the literature review. XC and WY
analyzed data. XL and JWu wrote the manuscript. ZH revised the
manuscript. JWu supervised the study. JWa provided overall guidance
and finalized the manuscript. All authors have reviewed and
approved the final manuscript.
Ethics approval and consent to
participate
Not applicable.
Patient consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Evered L, Silbert B, Knopman DS, Scott DA,
DeKosky ST, Rasmussen LS, Oh ES, Crosby G, Berger M and Eckenhoff
RG: Nomenclature Consensus Working Group. Recommendations for the
nomenclature of cognitive change associated with anaesthesia and
surgery-2018. Anesthesiology. 129:872–879. 2018.PubMed/NCBI View Article : Google Scholar
|
|
2
|
Evered L, Silbert B, Knopman DS, Scott DA,
DeKosky ST, Rasmussen LS, Oh ES, Crosby G, Berger M and Eckenhoff
RG: Nomenclature Consensus Working Group. Recommendations for the
nomenclature of cognitive change associated with anaesthesia and
surgery-2018. Br J Anaesth. 121:1005–1012. 2018.PubMed/NCBI View Article : Google Scholar
|
|
3
|
Zhang L, Qiu Y, Zhang ZF, Zhao YF and Ding
YM: Current perspectives on postoperative cognitive dysfunction in
geriatric patients: Insights from clinical practice. Front Med
(Lausanne). 11(1466681)2024.PubMed/NCBI View Article : Google Scholar
|
|
4
|
Linassi F, Maran E, De Laurenzis A,
Tellaroli P, Kreuzer M, Schneider G, Navalesi P and Carron M:
Targeted temperature management in cardiac surgery: A systematic
review and meta-analysis on postoperative cognitive outcomes. Br J
Anaesth. 128:11–25. 2022.PubMed/NCBI View Article : Google Scholar
|
|
5
|
Pas MT, Olde Rikkert M, Bouwman A, Kessels
R and Buise M: Screening for mild cognitive impairment in the
preoperative setting: A narrative review. Healthcare (Basel).
10(1112)2022.PubMed/NCBI View Article : Google Scholar
|
|
6
|
Su Y, Dong J, Sun J, Zhang Y, Ma S, Li M,
Zhang A, Cheng B, Cai S, Bao Q, et al: Cognitive function assessed
by Mini-mental state examination and risk of all-cause mortality: A
community-based prospective cohort study. BMC Geriatr.
21(524)2021.PubMed/NCBI View Article : Google Scholar
|
|
7
|
Salis F, Costaggiu D and Mandas A:
Mini-mental state examination: Optimal cut-off levels for mild and
severe cognitive impairment. Geriatrics (Basel).
8(12)2023.PubMed/NCBI View Article : Google Scholar
|
|
8
|
Critical Appraisal Skills Programme: CASP
checklists, 2018. Available at: https://casp-uk.net/casp-tools-checklists/. Accessed
May 2, 2025.
|
|
9
|
Page MJ, McKenzie JE, Bossuyt PM, Boutron
I, Hoffmann TC, Mulrow CD, Shamseer L, Tetzlaff JM, Akl EA, Brennan
SE, et al: The PRISMA 2020 statement: An updated guideline for
reporting systematic reviews. BMJ. 372(n71)2021.PubMed/NCBI View
Article : Google Scholar
|
|
10
|
Kadoi Y and Goto F: Factors associated
with postoperative cognitive dysfunction in patients undergoing
cardiac surgery. Surg Today. 36:1053–1057. 2006.PubMed/NCBI View Article : Google Scholar
|
|
11
|
Kadoi Y, Kawauchi C, Ide M, Kuroda M,
Takahashi K, Saito S, Fujita N and Mizutani A: Preoperative
depression is a risk factor for postoperative short-term and
long-term cognitive dysfunction in patients with diabetes mellitus.
J Anesth. 25:10–17. 2011.PubMed/NCBI View Article : Google Scholar
|
|
12
|
Kadoi Y, Saito S, Fujita N and Goto F:
Risk factors for cognitive dysfunction after coronary artery bypass
graft surgery in patients with type 2 diabetes. J Thorac Cardiovasc
Surg. 129:576–583. 2005.PubMed/NCBI View Article : Google Scholar
|
|
13
|
Maekawa K, Baba T, Otomo S, Morishita S
and Tamura N: Low pre-existing gray matter volume in the medial
temporal lobe and white matter lesions are associated with
postoperative cognitive dysfunction after cardiac surgery. PLoS
One. 9(e87375)2014.PubMed/NCBI View Article : Google Scholar
|
|
14
|
Veliz-Reissmüller G, Agüero Torres H, van
der Linden J, Lindblom D and Eriksdotter Jönhagen M: Pre-operative
mild cognitive dysfunction predicts risk for post-operative
delirium after elective cardiac surgery. Aging Clin Exp Res.
19:172–177. 2007.PubMed/NCBI View Article : Google Scholar
|
|
15
|
Yazit NAA, Juliana N, Hafidz KM, Aziz
NASA, Maluin SM, Azmani S, Teng NIMF, Das S and Kadiman S:
Exploring cognitive changes in high-risk cardiac patients receiving
dexmedetomidine and evaluating the correlation between different
cognitive tools: A cohort study. Rev Cardiovasc Med.
25(273)2024.PubMed/NCBI View Article : Google Scholar
|
|
16
|
Shiraboina M, Ayya S, Srikanth Y, Kumar R,
Durga P and Gopinath R: Predictors of postoperative cognitive
dysfunction in adult patients undergoing elective cardiac surgery.
Indian J Anaesth. 58:334–336. 2014.PubMed/NCBI View Article : Google Scholar
|
|
17
|
Chi KY, Li MY, Chen C and Kang E: Cochrane
Taiwan. Ten circumstances and solutions for finding the sample mean
and standard deviation for meta-analysis. Syst Rev.
12(62)2023.PubMed/NCBI View Article : Google Scholar
|
|
18
|
Zhang Y, Duan B, Wang L, Ye Z, Pan Y, Guo
Q and Wang E: Association between the variability of cerebral
oxygen saturation during cardiopulmonary bypass and delayed
postoperative neurocognitive recovery in cardiac valve surgical
patients: A pilot study. Int J Clin Pract.
75(e13651)2021.PubMed/NCBI View Article : Google Scholar
|
|
19
|
Greaves D, Psaltis PJ, Ross TJ, Davis D,
Smith AE, Boord MS and Keage HAD: Cognitive outcomes following
coronary artery bypass grafting: A systematic review and
meta-analysis of 91,829 patients. Int J Cardiol. 289:43–49.
2019.PubMed/NCBI View Article : Google Scholar
|
|
20
|
Newman MF, Kirchner JL, Phillips-Bute B,
Gaver V, Grocott H, Jones RH, Mark DB, Reves JG and Blumenthal JA:
Neurological Outcome Research Group and the Cardiothoracic
Anesthesiology Research Endeavors Investigators. Longitudinal
assessment of neurocognitive function after coronary-artery bypass
surgery. N Engl J Med. 344:395–402. 2001.PubMed/NCBI View Article : Google Scholar
|
|
21
|
Smith PJ, Browndyke JN, Monge ZA,
Harshbarger TB, James ML, Gaca JG, Alexander JH, Berger MM, Newman
MF, Milano CA, et al: Longitudinal changes in regional cerebral
perfusion and cognition after cardiac operation. Ann Thorac Surg.
107:112–118. 2019.PubMed/NCBI View Article : Google Scholar
|
|
22
|
Zhang ZR, Li YZ, Wu XQ, Chen WJ, Xu J,
Zhao WH and Gong XY: Postoperative cognitive dysfunction in elderly
postcardiac surgery patients: Progress in rehabilitation
application research. Front Rehabil Sci. 5(1525813)2024.PubMed/NCBI View Article : Google Scholar
|
|
23
|
Hogue CW, Gottesman RF and Stearns J:
Mechanisms of cerebral injury from cardiac surgery. Crit Care Clin.
24:83–98, viii-ix. 2008.PubMed/NCBI View Article : Google Scholar
|
|
24
|
Xu X, Zhu D, Wu Y, Kuang X, Wang L, Wang X
and Shi H: Perioperative neurocognitive disorders in elderly
patients undergoing cardiac surgery: Mechanisms, biomarkers, and
prevention. J Cardiothorac Vasc Anesth: Jan 21, 2026 (Epub ahead of
print) doi: S1053-0770(26)00053-4, 2026.
|
|
25
|
Zhang Z, Yang W, Wang L, Zhu C, Cui S,
Wang T, Gu X, Liu Y and Qiu P: Unraveling the role and mechanism of
mitochondria in postoperative cognitive dysfunction: A narrative
review. J Neuroinflammation. 21(293)2024.PubMed/NCBI View Article : Google Scholar
|
|
26
|
Liu F, Wu X, Wang Z, Li A, Luo Y and Cao
J: Mitochondrial dysfunction in postoperative cognitive
dysfunction: From preclinical mechanisms to multimodal diagnostics
and precision intervention. Ageing Res Rev.
111(102845)2025.PubMed/NCBI View Article : Google Scholar
|
|
27
|
Yang Y, Liu Y, Zhu J, Song S, Huang Y,
Zhang W, Sun Y, Hao J, Yang X, Gao Q, et al:
Neuroinflammation-mediated mitochondrial dysregulation involved in
postoperative cognitive dysfunction. Free Radic Biol Med.
178:134–146. 2022.PubMed/NCBI View Article : Google Scholar
|
|
28
|
Ying J, Deng X, Du R, Ding Q, Tian H, Lin
Y, Zhou B and Gao W: Mitochondrial modulation treating
postoperative cognitive dysfunction neuroprotection via DRP1
inhibition by Mdivi1. Sci Rep. 14(26155)2024.PubMed/NCBI View Article : Google Scholar
|
|
29
|
Netto MB, de Oliveira Junior AN, Goldim M,
Mathias K, Fileti ME, da Rosa N, Laurentino AO, de Farias BX, Costa
AB, Rezin GT, et al: Oxidative stress and mitochondrial dysfunction
contributes to postoperative cognitive dysfunction in elderly rats.
Brain Behav Immun. 73:661–669. 2018.PubMed/NCBI View Article : Google Scholar
|
|
30
|
Ye F, Wei C and Wu A: The potential
mechanism of mitochondrial homeostasis in postoperative
neurocognitive disorders: An in-depth review. Ann Med.
56(2411012)2024.PubMed/NCBI View Article : Google Scholar
|
|
31
|
Pang B, Dong G, Pang T, Sun X, Liu X, Nie
Y and Chang X: Emerging insights into the pathogenesis and
therapeutic strategies for vascular endothelial injury-associated
diseases: Focus on mitochondrial dysfunction. Angiogenesis.
27:623–639. 2024.PubMed/NCBI View Article : Google Scholar
|
|
32
|
Saczynski JS, Marcantonio ER, Quach L,
Fong TG, Gross A, Inouye SK and Jones RN: Cognitive trajectories
after postoperative delirium. N Engl J Med. 367:30–39.
2012.PubMed/NCBI View Article : Google Scholar
|
|
33
|
Greaves D, Psaltis PJ, Davis DHJ, Ross TJ,
Ghezzi ES, Lampit A, Smith AE and Keage HAD: Risk factors for
delirium and cognitive decline following coronary artery bypass
grafting surgery: A systematic review and meta-analysis. J Am Heart
Assoc. 9(e017275)2020.PubMed/NCBI View Article : Google Scholar
|
|
34
|
Zhuang YM, Xu JY, Zheng K and Zhang H:
Research progress of postoperative cognitive dysfunction in cardiac
surgery under cardiopulmonary bypass. Ibrain. 10:290–304.
2023.PubMed/NCBI View Article : Google Scholar
|
|
35
|
Ntalouka MP, Arnaoutoglou E and Tzimas P:
Postoperative cognitive disorders: An update. Hippokratia.
22:147–154. 2018.PubMed/NCBI
|
|
36
|
Kotekar N, Kuruvilla CS and Murthy V:
Post-operative cognitive dysfunction in the elderly: A prospective
clinical study. Indian J Anaesth. 58:263–268. 2014.PubMed/NCBI View Article : Google Scholar
|
|
37
|
Goto T, Baba T, Yoshitake A, Shibata Y,
Ura M and Sakata R: Craniocervical and aortic atherosclerosis as
neurologic risk factors in coronary surgery. Ann Thorac Surg.
69:834–840. 2000.PubMed/NCBI View Article : Google Scholar
|
|
38
|
Milz S, Holaubek C, Siebel J, Hulde N,
Wefer F, Fruend A, Tigges-Limmer K, Gummert J and von Dossow V:
Implementation of evidence-based international recommendations
reduces postoperative delirium rate in patients undergoing cardiac
surgery or interventions: A system-based quality improvement study.
Rev Cardiovasc Med. 25(369)2024.PubMed/NCBI View Article : Google Scholar
|
|
39
|
Ahmadzadeh S, Duplechin DP, Haynes AT,
Hollander AV, Rieger R, Jean Baptiste C, Varrassi G, Shekoohi S and
Kaye AD: Evolving clinical management of postoperative delirium: A
narrative review. Cureus. 17(e92927)2025.PubMed/NCBI View Article : Google Scholar
|
|
40
|
Lau KT, Chiu LCS, Fong JSY, Chan AKM, Ho
KM and Lee A: Preoperative cognitive training for the prevention of
postoperative delirium and cognitive dysfunction: A systematic
review and meta-analysis. Perioper Med (Lond).
13(113)2024.PubMed/NCBI View Article : Google Scholar
|
|
41
|
Kotekar N, Shenkar A and Nagaraj R:
Postoperative cognitive dysfunction-current preventive strategies.
Clin Interv Aging. 13:2267–2273. 2018.PubMed/NCBI View Article : Google Scholar
|
|
42
|
He Y, Wang Z, Zhao Y, Han X, Guo K, Sun N
and Liu X: Cognitive prehabilitation for older adults undergoing
elective surgery: A systematic review and narrative synthesis.
Front Aging Neurosci. 16(1474504)2024.PubMed/NCBI View Article : Google Scholar
|
|
43
|
Humeidan ML, Reyes JC, Mavarez-Martinez A,
Roeth C, Nguyen CM, Sheridan E, Zuleta-Alarcon A, Otey A,
Abdel-Rasoul M and Bergese SD: Effect of cognitive prehabilitation
on the incidence of postoperative delirium among older adults
undergoing major noncardiac surgery: The neurobics randomized
clinical trial. JAMA Surg. 156:148–156. 2021.PubMed/NCBI View Article : Google Scholar
|
|
44
|
Ji L and Li F: Potential markers of
neurocognitive disorders after cardiac surgery: A bibliometric and
visual analysis. Front Aging Neurosci. 14(868158)2022.PubMed/NCBI View Article : Google Scholar
|
|
45
|
Ren X, Huiqiao L, Wu Y, Zhang T, Chen P,
Li L, Zhao G and Wang F: Perioperative neurocognitive disorders: A
comprehensive review of terminology, clinical implications, and
future research directions. Front Neurol.
16(1526021)2025.PubMed/NCBI View Article : Google Scholar
|
|
46
|
Paternò DS, Via L, Putaggio A, Piccolo A,
Scibilia G, Lentini M, Maniaci A, Luca F, Giudice ECL and Sorbello
M: Perioperative neurocognitive disorders: A narrative review of
pathophysiology, prevention, and management strategies. J Clin Med.
15(1253)2026.PubMed/NCBI View Article : Google Scholar
|