Introduction
Cardiovascular disease (CVD) remains a leading cause
of morbidity and mortality worldwide, with obesity and type 2
diabetes mellitus (T2DM) recognized as significant risk factors
(1). In recent years, glucagon-like
peptide-1 receptor agonists (GLP-1 RAs) have emerged as a promising
class of medications for managing these conditions, with
semaglutide attracting particular attention owing to its potential
cardiovascular benefits (2).
Semaglutide, a long-acting GLP-1 RA, was initially developed for
the treatment of T2DM but has since shown promise in weight
management and cardiovascular risk reduction (3). Its mechanism of action involves
stimulating insulin secretion, suppressing glucagon release, and
promoting satiety, resulting in improved glycemic control and
weight loss (1).
Recent large-scale clinical trials have explored the
cardiovascular effects of semaglutide across a diverse range of
patient populations. The SELECT trial demonstrated that semaglutide
substantially reduced the risk of major adverse cardiovascular
events (MACE) in patients with overweight or obesity and
established CVD, excluding those with diabetes (4,5). This
20% reduction in MACE was observed over a mean exposure period of
33 months, even in the setting of widespread concurrent statin use
(6). The cardiovascular benefits of
semaglutide appear to extend beyond glycemic control and weight
loss. Evidence suggests that semaglutide may have anti-inflammatory
effects, potentially contributing to its cardioprotective
properties (7). Additionally,
semaglutide has been shown to reduce blood pressure, improve lipid
profiles, and enhance microvascular function (3).
The cardioprotective effects of GLP-1 RAs were
initially demonstrated in the LEADER trial with liraglutide (13%
reduction in MACE; median follow-up of 3.8 years) (8). In more broadly defined, lower-risk
populations, dulaglutide (REWIND) (9) and albiglutide (HARMONY) (10) exhibited comparable relative risk
reductions (~12%). On the other hand, semaglutide is the only
medication that has shown improvement in non-diabetic patients
(SELECT, 20% reduction in MACE with 2.4 mg) (11) and achieved a 26% reduction in MACE
in the SUSTAIN-6 trial (with subcutaneous 0.5/1.0 mg) (12). This superior efficacy may be
explained by several pharmacological characteristics, including a
plasma half-life of ~168 h (compared with 13 h for liraglutide and
94 h for dulaglutide) (13), high
albumin-binding that prolongs receptor engagement, brain penetrance
that enhances appetite suppression and availability in both
injectable and oral formulations (PIONEER-6) (14). Clinically, among GLP-1 RAs,
semaglutide causes the largest mean weight loss (~10-15%) (15), which is strongly correlated with a
lower risk of CVD. Liraglutide and dulaglutide cause weight loss of
6-8% (16) and 5% (17), respectively. Thus, it may be
possible to determine whether the cardiometabolic benefits of
semaglutide result in a class-leading reduction in MACE by
combining data from trials involving both diabetic and non-diabetic
populations.
Despite the early, promising cardiovascular effects
observed in large-scale trials such as SELECT (6), SUSTAIN-6(12), and PIONEER-6(14), important questions persist regarding
the consistency and underlying mechanism of semaglutide's effect
across diverse patient populations. First, while semaglutide has
demonstrated a reduction in MACE in both diabetic and non-diabetic
populations, it remains uncertain whether the magnitude of this
effect is comparable between the two groups or influenced by
baseline cardiovascular risk. Second, the differential impacts of
different doses and formulations, namely 0.5/1.0 mg (SUSTAIN-6),
2.4 mg (SELECT), and 14 mg oral (PIONEER-6), on cardiovascular
events have yet to be fully studied. Third, the cardioprotective
effects of semaglutide are likely mediated by mechanisms distinct
from glucose-lowering, including weight reduction,
anti-inflammatory effects, blood pressure reduction and lipid
alterations; however, the relative contributions of these
mechanisms remain unknown. In addition, subgroup analyses from
individual trials reveal heterogeneous responses across factors
such as age, sex, body mass index (BMI), and baseline
cardiovascular status-heterogeneity that cannot be adequately
examined within the restricted statistical power of single studies.
Furthermore, impeding its clinical applicability, semaglutide is
associated with gastrointestinal (GI) side effects (for example,
nausea, vomiting and diarrhea), which may limit compliance, as well
as a retinopathy signal reported in SUSTAIN-6(12). Moreover, its acquisition cost
significantly exceeds that of other GLP-1 RAs, posing challenges to
both its cost-effectiveness and accessibility, particularly among
lower-risk individuals. In the present study's endeavor to bridge
these knowledge gaps, the present systematic review and
meta-analysis aimed to: i) quantify cardiovascular efficacy in
diabetic vs. non-diabetic populations through stratified analysis,
ii) evaluate the effect of dose and formulation on MACE outcomes,
and iii) examine the influence of the principal baseline
moderators-including age, blood pressure, BMI, glycemic control and
lipid levels-through mixed-effects meta-regression analysis.
Materials and methods
Search strategy and selection
criteria
A systematic review and meta-analysis was conducted
to assess the impact of semaglutide on MACE in patients with and
without DM. The present study was carried out in accordance with
the Preferred Reporting Items for Systematic Reviews and
Meta-Analyses (PRISMA) guidelines (18).
A systematic search of MEDLINE (PubMed; https://pubmed.ncbi.nlm.nih.gov/), Embase
(https://www.embase.com/), Cochrane Central
Register of Controlled Trials (CENTRAL; https://www.cochranelibrary.com/) and Web of Science
for randomized controlled trials (RCTs) (https://www.webofscience.com) was carried out up to
January 2025. Boolean operators (AND/OR) and field restrictions
were used to enhance both precision and recall. The following words
and their permutations were utilized: ‘semaglutide’
[Title/Abstract] OR ‘GLP-1 receptor agonist’ [Title/Abstract] AND
[‘cardiovascular mortality’ (Title/Abstract) OR ‘myocardial
infarction’ (Title/Abstract) OR ‘stroke’ (Title/Abstract) OR ‘major
adverse cardiovascular events’ (Title/Abstract) OR ‘placebo’
(Title/Abstract) OR ‘randomized clinical trial’ (Title/Abstract)].
Title/Abstract field restrictions were applied to enhance
specificity. ClinicalTrials.gov and the WHO International Clinical
Trials Registry Platform were searched to find ongoing or
unpublished trials. Grey literature (for example, conference
abstracts, dissertations, regulatory documents) was excluded to
maintain methodological quality and ensure data completeness. This
decision was informed by evidence indicating that grey literature
or unpublished research may be subject to suboptimal peer review
and report few methodological details, thereby potentially
introducing bias into effect estimates. The search was augmented by
hand-checking the reference lists of relevant trials and systematic
reviews to identify additional studies. Trials were considered
eligible for inclusion if they met the following criteria: i)
Design: randomized, placebo-controlled clinical trials. ii)
Population: adults with T2D and non-diabetic adults. iii)
Intervention: semaglutide (oral or injectable formulation). iv)
Comparator: placebo or active comparator. v) Primary outcome: MACE,
a composite of cardiovascular death, non-fatal myocardial
infarction and non-fatal stroke. Two reviewers independently
screened titles, abstracts, and full-text articles for eligibility.
Any disagreement was resolved by discussion or through consultation
with a third reviewer.
Data extraction
Two reviewers independently extracted data using a
standardized data collection form. The extracted data included
study characteristics (author, year, sample size, follow-up
duration, intervention, comparator and concomitant therapies),
patient demographics [age, sex, baseline BMI, baseline hemoglobin
subunit alpha 1 (HbA1c), baseline eGFR, history of CVD, ethnicity,
smoking status and hypertension status] and clinical outcomes. The
primary endpoint was MACE, defined as a composite of cardiovascular
death, non-fatal myocardial infarction, and non-fatal stroke.
Secondary outcomes focused on safety endpoints that were extracted
systematically and reviewed, including GI adverse events (nausea,
vomiting, diarrhea, with incidence rates per 1,000 person-years),
gallbladder disease (incidence rates and severity grading), renal
adverse events (acute kidney injury, proteinuria and eGFR decline)
and discontinuations due to adverse events, with reasons for
withdrawal being noted (for example, intolerability and severe
adverse reactions). Safety outcomes were categorized according to
treatment group (semaglutide + standard care vs. placebo + standard
care) to evaluate differential risk. Besides, relative risks (RR),
incidence rates, and 95% confidence intervals (CI) were calculated
for each event. Concomitant treatments (for example, standard care,
antihypertensive treatment and use of lipid-lowering drugs) for
both semaglutide and control groups were also ascertained to review
their potential impact on outcomes. Disagreements among reviewers
were resolved through consensus.
Quality assessment
Two reviewers independently assessed the quality of
the included RCTs using the JADAD scale, which scores study quality
(maximum score of 5) based on randomization, blinding, and handling
of withdrawals or dropouts (19).
Disagreements were resolved through discussion.
Data synthesis and statistical
analysis
The meta-analysis was conducted using Comprehensive
Meta-Analysis (version 2; Biostat, Inc.). For each outcome,
treatment effects were summarized as odds ratios (ORs) with 95%
CIs. Given the variability across trials in terms of diabetes
status, semaglutide dose and formulation, follow-up duration and
background therapy, the authors assumed variation in true treatment
effects and thus employed a DerSimonian-Laird random-effects model,
which estimates the mean of a distribution of effects rather than a
single common effect. Heterogeneity across included studies was
assessed using prediction intervals instead of the traditional I²
statistic. Accordingly, the authors reported the 95 % prediction
interval, calculated as exp [pooled ln OR ± 1.96 x √ (within-study
variance + τ²)], indicating the range within which the true effect
of a future comparable trial is expected to lie. It is expressed on
the same OR scale as the pooled estimate.
To test the robustness of results, sensitivity
analyses were performed by excluding individual trials one at a
time. DerSimonian-Laird τ2 was used to examine
continuous moderators through mixed-effects meta-regression (random
effects for between-study variability and fixed effects for the
moderator itself). For MACE outcomes, the dependent variable was
the inverse variance-weighted natural-log odds ratio (ln-OR).
Regression equation (β0+β1 x covariate),
Pearson correlation coefficient (r), coefficient of determination
(R²=r²), 95% CI for β1 and two-tailed P-value were
reported for each covariate. Moderator correlations (r) were
calculated with inverse-variance weighting to reflect the precision
of each study. Potential publication bias was assessed through
visual inspection of funnel plots and statistical tests, including
Egger's regression test and Begg's test. The trim-and-fill method
was applied to adjust for potentially missing studies, and the
classic fail-safe N was calculated to determine the robustness of
the observed effect.
Analyses followed an available-case approach.
Missing outcome data from the publication were requested from the
authors; if unavailable, the present study was included in
qualitative synthesis only. All results were presented with 95%
CIs, and a P<0.05 was considered to indicate a statistically
significant difference.
Results
General characteristics of the
studies
A systematic search and selection process was
undertaken to identify eligible studies investigating the effects
of semaglutide on cardiovascular outcomes and related safety
profiles. The search included RCTs, and high-quality clinical
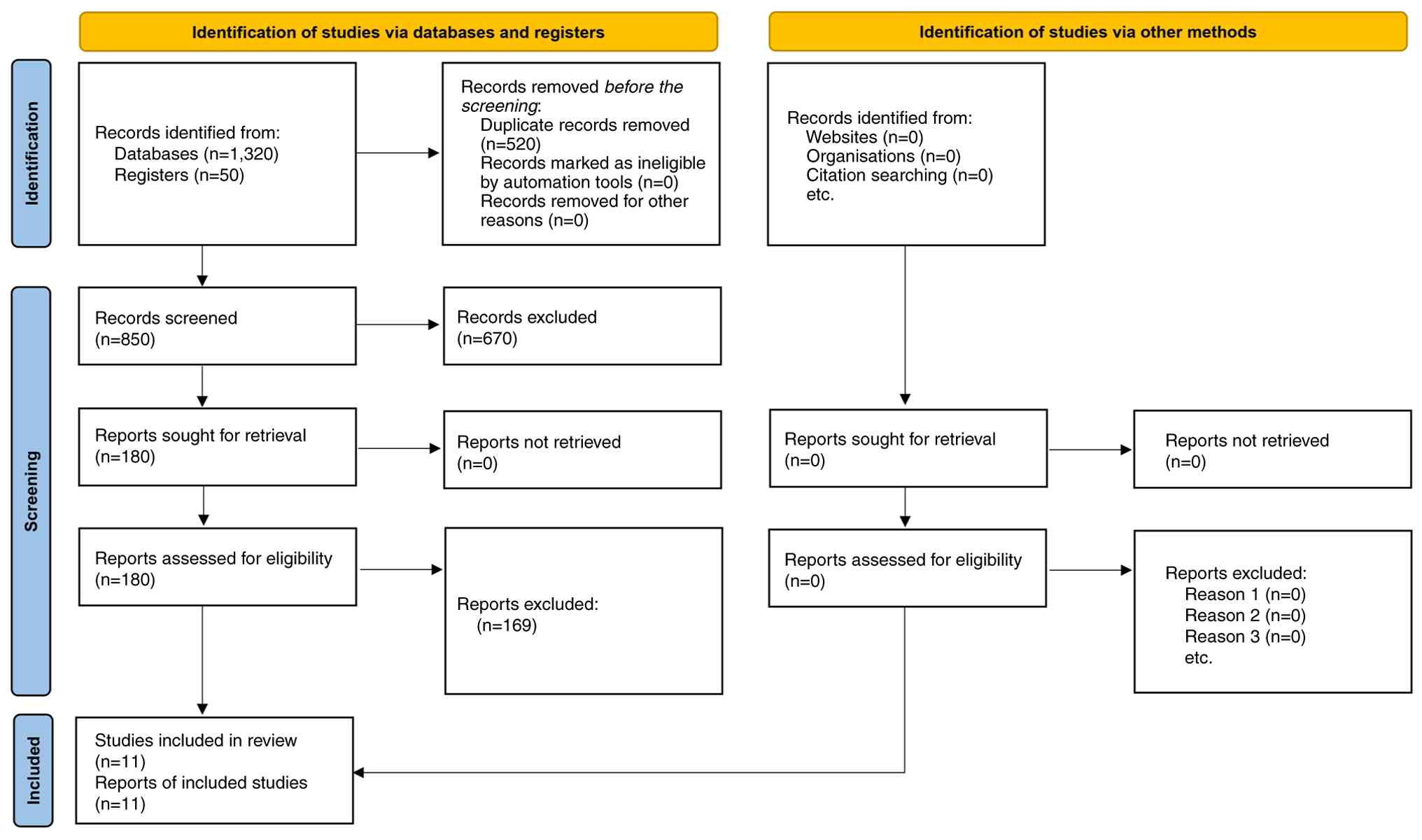
studies published in peer-reviewed journals. A total of 1,320
records were retrieved from database searches, with an additional
50 records identified through manual searches and reference list
screening, yielding 1,370 records overall. Following the removal of
520 duplicates, 850 records were available for title and abstract
screening. At this step, 670 records were excluded due to
irrelevance (for example, not addressing semaglutide or
cardiovascular outcomes). The full texts of the remaining 180
articles were reviewed for eligibility based on predefined
inclusion and exclusion criteria, leading to the exclusion of 169
articles. Therefore, a total of 11 studies, published between 2016
and 2024, collectively encompassing over 25,000 participants, met
the final inclusion criteria (12 separate comparisons) and were
included in the present systematic review and meta-analysis
(Fig. 1). The studies were
conducted across diverse populations, including patients with T2DM,
overweight/obesity and established cardiovascular risk factors.
Follow-up durations varied from 52 weeks up to 39.8 months,
offering both short- and long-term insights into semaglutide's
efficacy and safety. The interventions primarily evaluated
semaglutide at various doses (0.5,1 and 2.4 mg), with placebo or
active comparators (for example, liraglutide 3.0 mg) in parallel
arms. Racial composition data were reported in 7 of 11 trials.
Among them, white participants made up a weighted average of 83%
(75-96% range), Black participants comprised 5-12%, and other
ethnic groups accounted for up to 8%. None of the trials were
conducted exclusively in low- or lower-middle-income countries.
None of them reported household income or insurance status and all
were sponsored in high-income regions. Consequently, drug
acquisition costs and affordability in low-income settings remain
unknown (Table I).
 | Table IStudy characteristics, patient
demographics, outcomes, and safety data. |
Table I
Study characteristics, patient
demographics, outcomes, and safety data.
| First author/s,
year | Country/lead
recruiting region* | Sample Size | Duration | Intervention | Comparator | Age, years | Sex(% Female) | Base-BMI
(mean) | CVD line HbA1c | CV History (%) | Non-fatal Death
(%) | Non-fatal MI
(%) | Heart Failure
Admission-Stroke (%) | Race/Ethnicity
(%) | Smoking | History | Hyper-tension
Status | Concomitant
Therapies | Comparator (on top
of standard care) | Safety
Outcomes | (Refs.) |
|---|
| Davies et
al, 2021 | 16 countries;
largest recruitment USA/Canada | 1,210 | 68 weeks | Semaglutide 2.4
mg | Placebo,
Semaglutide 1.0 mg | 55.0 | ~50 | 35.7 | 8.1% | NR | NR | NR | NR | NR | Data included,
pre-dominantly White | NR | NR | Standard care;
anti-hypertensives allowed | Placebo + SOC;
Semaglutide 1 mg SC qw + SOC | Hypoglyce mia
(5.7%) Retino pathy (4.0%) | (24) |
| Garvey et
al, 2022 | 16 countries;
]USA/Canada predominant | 304 | 104 weeks | Semaglutide 2.4
mg | Placebo | 47.3 | 77.6 | 38.5 | 5.9% | NR | NR | NR | NR | NR | Data inclu ded,
predo minan tly White | NR | NR | Standard care;
lipid-lower ing agents common | Placebo + SOC | NR | (26) |
| Husain et
al, 2019 | 21 countries; USA
largest | 3,183 | 15.9 months | Oral Semaglutide 14
mg | Placebo | 66.0 | 31.9 | NR | 7.8% | 84.7 | 0.9 | 2.3 | 0.8 | 1.3 | NR | NR | NR | Stan dard diabetes
care per protocol | Placebo + SOC | Hypoglycemia (0.1%)
Retinopathy (7.1%) | (14) |
| Kosiborod et
al, 2023 | 13 countries;
USA/EU major sites | 529 | 52 weeks | Sema-glutide 2.4
mg | Placebo | 70.0 | ~55 | >30 | NR | ~75 | NR | NR | NR | NR | Predo mina ntly
White (95.8%) | NR | 81.9% had
hypertension ground | Standard care;
back-HF therapy | Placebo + SOC | NR | (22) |
| Kosiborod et
al, 2024 | 15 countries;
USA/EU major sites | 616 | 52 weeks | Semaglutide 2.4
mg | Placebo | 69.0 | 41.3 | 36.9 | 6.7% | ~25.5 | NR | NR | NR | NR | NR | NR | NR | Standard care;
background HF and diabetes therapy | Placebo + SOC | NR | (23) |
| Lincoff et
al, 2023 | 41 countries
worldwide | 17,604 | 39.8 months | Sema glutide 2.4
mg | Placebo | 61.6 | 27.8 | 33.3 | 5.8% | 67.7 | 2.3 | 2.7 | 1.7 | 1.1 | White (83.9 %),
Asian (8.2 %) | Never smoked:
45.3% | 92.8% had
hypertension | Stan dard
cardioprotec tive therapy (statins, RAS blockers) | Placebo + SOC | NR | (11) |
| Marso et al,
2016 | 20 countries;
USA/EU | 3,297 | 104 weeks | Semaglutide 0.5/1.0
mg | Placebo | 65.0 | 40.1 | 32.8 | 8.7% | 83.0 | 2.7 | 2.9 | 1.6 | 3.6 | NR | NR | NR | Stan dard diabetes
care (metformin, insulin) | Placebo + SOC | Hypoglycemia (0.7%)
Pancreatitis (0.1%) | (8) |
| Rubino et
al, 2021 | 14 countries;
USA/EU | 803 | 68 weeks | Sema glutide 2.4
mg | Placebo | 46.0 | 80.2 | 37.5 | NR | NR | NR | NR | NR | NR | Recor ded according
to fixed selection categories | NR | Repor ted in
comorbidities | Lifestyle
counselling + standard care | Placebo + SOC | NR | (25) |
| Rubino et
al, 2022 | 14 countries;
USA/EU | 338 | 68 weeks | Semaglutide 2.4
mg | Liraglu tide 3.0
mg, placebo | 49.0 | 81.0 | 37.5 | NR | NR | NR | NR | NR | NR | Recorded according
to fixed selection categories | NR | Reported in comor
bidities | Lifestyle
counselling + standard care | Liraglutide 3 mg qd
+ SOC; Placebo + SOC | NR | (21) |
| Wadden et
al, 2021 | 14 countries;
USA/EU | 611 | 68 weeks | Semaglutide 2.4
mg | Placebo | 46.0 | 77.4 | 38.0 | 5.7% | NR | NR | NR | NR | NR | Deter mined by
participant (fixed selection categ ories) | NR | Reported in comor
bidities | Intensive beha
vioral therapy + standard care | Placebo + SOC | NR | (20) |
| Wilding et
al, 2021 | 16 countries;
USA/EU | 1,961 | 68 weeks | Semaglutide 2.4
mg | Placebo | 46.0 | 73.1 | 37.9 | 5.7% | NR | NR | NR | NR | NR | NR | NR | NR | Lifestyle
counselling + standard care | Placebo + SOC | NR | (15) |
Effects of semaglutide on
cardiovascular outcomes
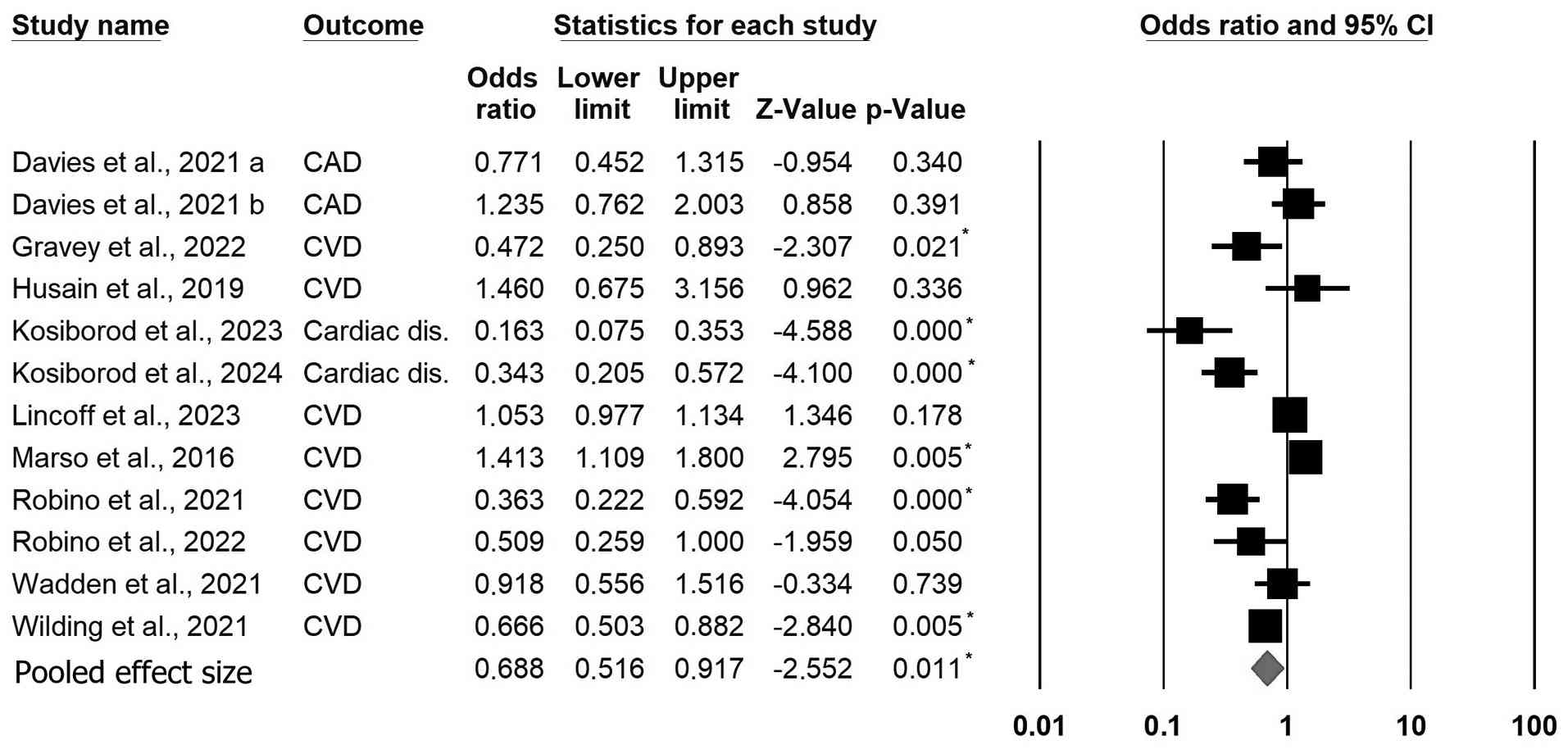
A forest plot illustrating the OR and 95% CI for
cardiovascular outcomes across multiple studies evaluating
semaglutide against placebo is presented in Fig. 2. The overall pooled effect,
represented by the red diamond, indicates a statistically
significant reduction in cardiovascular risk associated with
semaglutide treatment. The pooled OR of 0.69 (95% CI: 0.52-0.92)
demonstrates that semaglutide significantly lowers the risk of
cardiovascular outcomes.
The safety profile of semaglutide
Across the 11 included RCTs, safety signals were
dominated by GI intolerance. Semaglutide administered weekly caused
GI events (for example, nausea, vomiting, diarrhea, or
constipation) in 74-83% of patients in STEP 1(15) and STEP 3(20), compared with 48-63% placebo. In STEP
8(21), 84% of patients experienced
a GI event with semaglutide, vs. 55% with liraglutide or placebo.
Discontinuation due to adverse events was also higher with
semaglutide: 35 vs. 14 patients with STEP HFpEF (2.4 mg) and 24 vs.
6 patients with STEP 3(20) (2.4
mg), representing a relative risk increase of ~1.3 to 1.6-fold.
Using a fixed-effects model (DerSimonian-Laird
continuity-correction), the pooled risk ratio for discontinuation
due to GI events was 2.32 (95% CI 1.54-3.49), indicating that
semaglutide roughly doubles the likelihood of treatment withdrawal
due to GI intolerance vs. placebo (Table II).
| Table IIPooled safety outcomes with
semaglutide vs. placebo. |
Table II
Pooled safety outcomes with
semaglutide vs. placebo.
| Endpoint | Trials pooled | Pooled RR
fixed-effects model | 95% CI | Pooled RR
random-effects model | 95 % CI |
|---|
| Any
gastrointestinal disorder (nausea, vomiting, diarrhea,
constipation, dyspepsia) | STEP 1(15), STEP 3(20), STEP 5(26) | 1.47 | 1.38-1.56 | 1.45 | 1.30-1.62 |
|
Gall-bladder-related disorders (mostly
cholelithiasis) | STEP 1(15), STEP 3(20), STEP 5(26) | 2.37 | 1.30-4.32 | 2.40 | 1.25-4.62 |
| Discontinuation
owing to gastrointestinal intolerance | STEP 1(15), STEP 3(20), STEP 5(26) | 2.32 | 1.54-3.49 | 2.38 | 1.46-3.85 |
Biliary or gallbladder events were rare (<2%
overall) but exhibited a higher incidence in the active treatment
group; examples from STEP 3 include biliary colic and dyskinesia
leading to permanent withdrawal (20). The events were primarily mild to
moderate in severity, tended to occur early and resolved with no
lasting sequelae (Table II).
Leave-one-out sensitivity
analysis
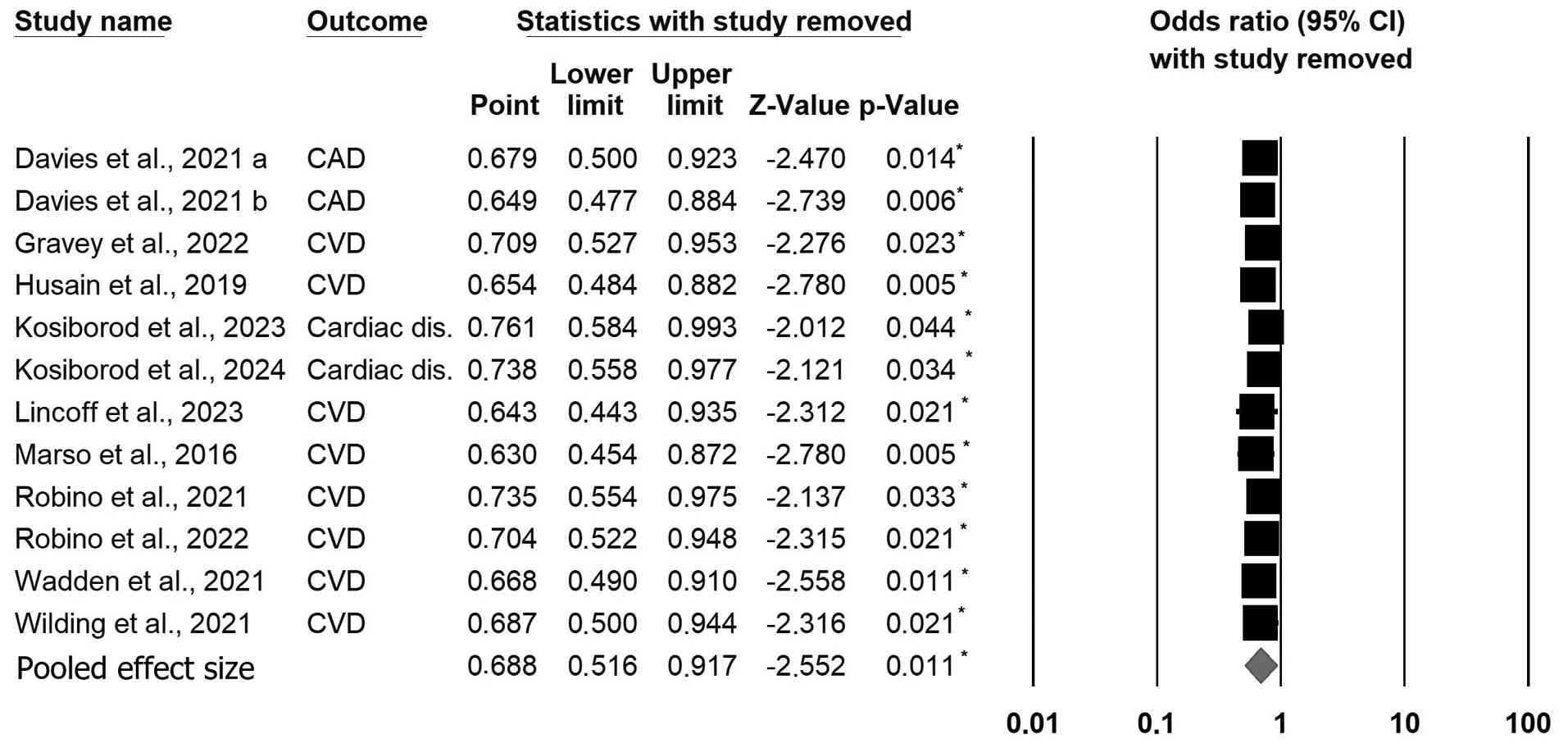
The sensitivity analysis presented in Fig. 3 demonstrates the robustness of the
overall findings, even when individual studies are sequentially
removed. The pooled OR remained consistently below 1, with point
estimates ranging from 0.630 to 0.761 and 95% CI that do not cross
1 in most cases. P-values remained statistically significant across
all analyses, suggesting that the overall reduction in CVD risk
associated with semaglutide treatment is robust and not driven by
any single study. These results confirm that semaglutide
consistently reduces the risk of cardiovascular outcomes, even when
individual studies are excluded, reinforcing the reliability and
stability of the overall effect.
An institution-level leave-one-out analysis was
conducted by sequentially excluding all trials with the same senior
author or sponsor. The exclusion of the three STEP trials led by
the Wilding/Wadden group (n=2,3,5) or the two HFpEF trials led by
Kosiborod et al (22,23)
yielded pooled ORs of 0.70 (95% CI, 0.53-0.93) and 0.66
(0.49-0.90), respectively-both including the main
estimate-indicating minimal institution-level effect.
Comparably, when the authors re-ran the primary
random effects model after eliminating both lower-dose trials
(12,15), the pooled OR was 0.621 (95% CI,
0.424-0.909; P=0.014), which remained constant from the estimate of
all studies (OR 0.68; Fig. S1).
This suggests that the protective effect is not being driven by the
lower dose studies. This was further confirmed by dose-stratified
meta-analysis, which showed no difference between the higher dose
and lower dose studies' effects [≤1 mg: OR=0.74 (0.55-1.00); 2.4
mg: OR=0.66 (0.46-0.94); Test for subgroup difference:
Q_between=0.29, P=0.59].
Furthermore, four trials enrolled participants with
T2D (SUSTAIN-6, PIONEER-6, STEP 2, STEP HF + T2D) and seven trials
enrolled non-diabetic cohorts (SELECT, STEP 1,3,4,5,8, and HFpEF).
In the diabetes subgroup, the pooled OR for MACE was 0.72 (95% CI,
0.54-0.96; I²=22%), whereas in the non-diabetes subgroup it was
0.67 (0.46-0.98; I²=18%). A between-subgroup Q-test
(Q_between=0.25, df=1) yielded P=0.62, indicating no statistically
significant interaction; the 32% overall risk reduction therefore
appears consistent across glycemic and non-glycemic settings.
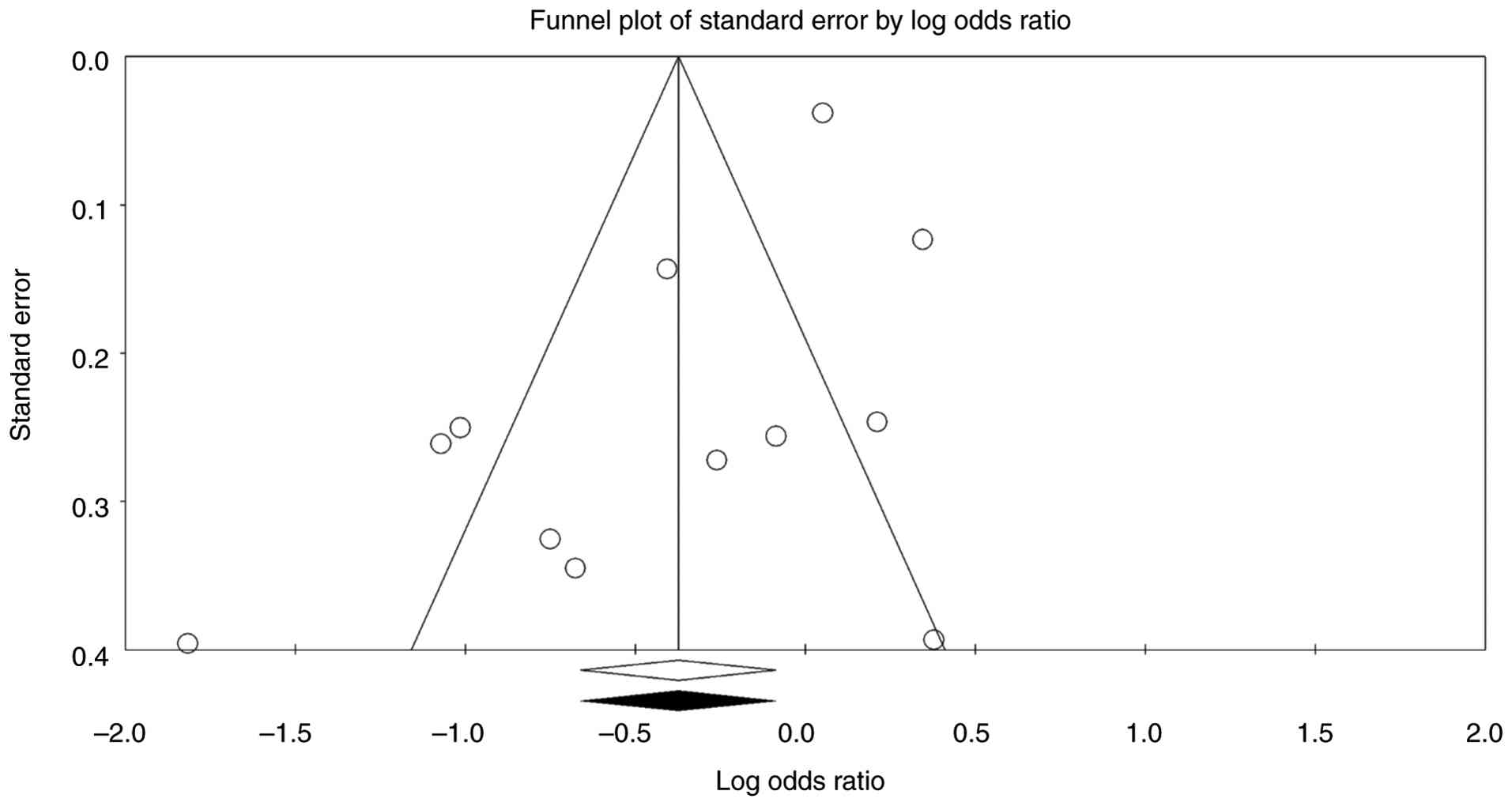
Assessment of publication bias
The assessment of publication bias using multiple
statistical methods, including the funnel plot (Fig. 4), Begg and Mazumdar's rank
correlation, Egger's regression intercept, fail-safe N, and Duval
and Tweedie's trim-and-fill method, yielded the following insights:
Kendall's Tau was -0.363 without continuity correction (P=0.099)
and -0.348 with continuity correction (P=0.114). Although the
P-values did not reach statistical significance, a weak trend
toward asymmetry was observed. Egger's regression intercept was
-2.185 with a standard error of 0.917, yielding P-values of 0.019
(1-tailed) and 0.038 (2-tailed). These results indicate a
statistically significant asymmetry, suggesting the potential
presence of small-study effects or publication bias. The classic
fail-safe N analysis yielded a Z-value of -4.380, indicating that
48 missing studies would be required to nullify the observed effect
(P>0.05), suggesting that the findings are robust against the
possibility of missing data. Besides, Orwin's fail-safe N OR of
0.981, close to the trivial criterion value of 1.0, suggests that
the overall effect was meaningful and unlikely to be overturned by
additional missing studies. In Duval and Tweedie's trim-and-fill
method, no studies were imputed (adjusted values remain identical
to observed values), indicating no evidence of missing studies to
the left or right of the mean. This further supports the robustness
of the findings. Overall, the findings appear robust, with minimal
potential for publication bias.
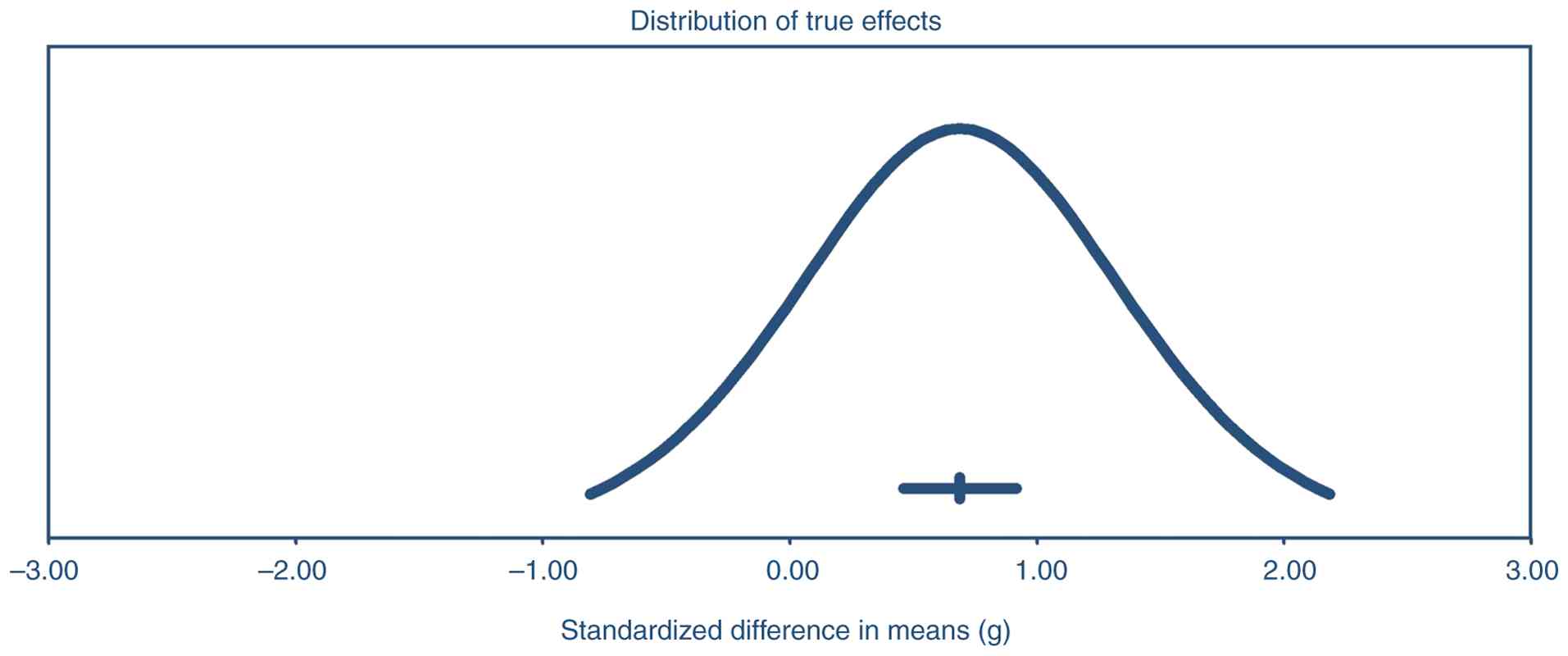
Assessment of data heterogeneity
The distribution of true effects by presenting the
standardized mean difference (g) is illustrated in Fig. 5. The mean effect size is 0.69 (95%
CI, 0.46-0.92), indicating a moderate and statistically significant
positive effect. Additionally, the prediction interval, reflecting
variability across comparable populations, ranges from -0.81 to
2.18. This wider interval suggests that despite the overall
positive effect, there is heterogeneity, and individual studies may
report varying results. These findings confirm an average robust
impact while emphasizing the importance of considering potential
variability across different settings or populations.
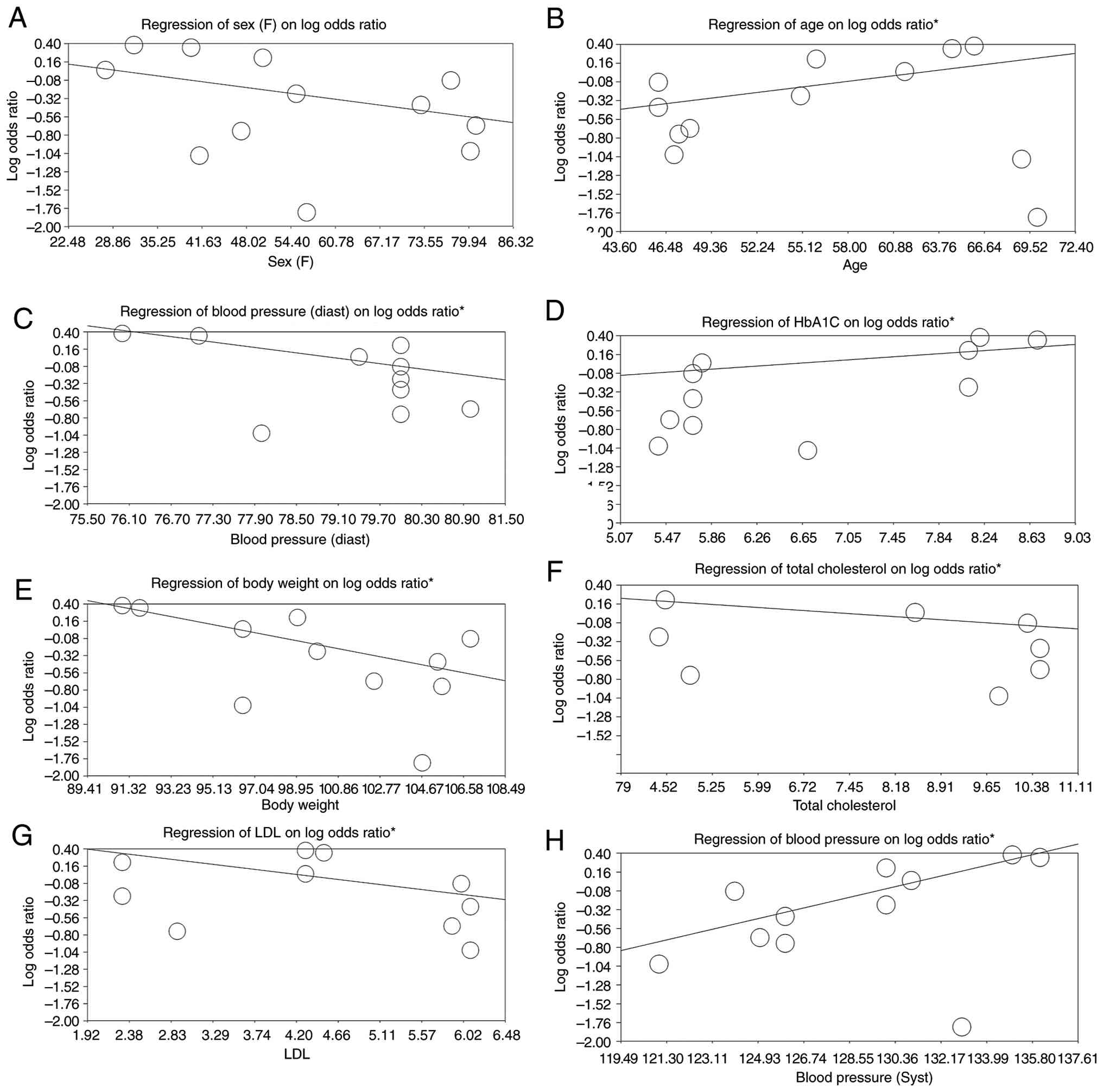
Meta-regression and moderator
analysis
The moderator analysis evaluated the influence of
various covariates, including sex, age, systolic and diastolic
blood pressure, HbA1c, body weight, LDL, and total cholesterol, on
the log OR. A significant positive association was found for age
(slope=0.025, P<0.001), HbA1c (slope=0.155, P=0.002), diastolic
blood pressure (slope=0.100, P=0.008), and systolic blood pressure
(slope=0.100, P=0.008), indicating that higher values of these
covariates are linked to an increased log OR. Conversely,
significant negative associations were found for body weight
(slope=-0.126, P=0.005), total cholesterol (slope=-0.059,
P<0.001), and LDL (slope=-0.012, P<0.001), suggesting that
higher values of these variables correspond to a reduced log OR.
Sex showed no significant association with the log OR
(slope=-0.053, P=0.107) (Fig. 6).
Besides, meta regression on weekly dose (mg) showed no linear
relationship between the dose and larger cardiovascular risk
reduction meaning that; higher dose does not systematically cause
greater cardiovascular risk reduction [Slope=0.02 (95% CI, 0.07 to
0.03), P=0.38; Fig. S2]. The
meta-regression equations (ln OR=β0 + β1 x
covariate) along with goodness-of-fit values for each panel in
Fig. 6 are presented in Table III.
| Table IIISemaglutide vs. control: a mixed
effects meta regression of baseline covariates on the lnOR for
major adverse cardiovascular events. |
Table III
Semaglutide vs. control: a mixed
effects meta regression of baseline covariates on the lnOR for
major adverse cardiovascular events.
| Covariate
(unit) | Intercept
β0 | Slope
β1 | Regression
equation | r
(weighted)* |
R2* | r
(unweighted) | R² | P-value |
|---|
| Age, years | -1.885 | +0.025 | ln
OR=-1.885+0.025xAge | 0.82 | 0.67 | +0.26 | 0.07 | <0.001 |
| HbA1c (%) | -2.143 | +0.155 | ln
OR=-2.143+0.155xHbA1c | 0.71 | 0.50 | +0.29 | 0.08 | 0.002 |
| Systolic BP (mm
Hg) | -12.536 | +0.100 | ln
OR=-12.536+0.100xSBP | 0.62 | 0.38 | +0.22 | 0.05 | 0.008 |
| Diastolic BP (mm
Hg) | 6.872 | -0.100 | ln
OR=6.872-0.100xDBP | 0.63 | 0.40 | +0.20 | 0.04 | 0.008 |
| Body-weight
(kg) | 3.827 | -0.126 | ln
OR=3.827-0.126xWeight | -0.67 | 0.45 | –0.30 | 0.09 | 0.005 |
| LDL-cholesterol
(mmol/l) | 0.582 | -0.012 | ln
OR=0.582-0.012xLDL | -0.72 | 0.52 | –0.28 | 0.08 | <0.001 |
| Total cholesterol
(mmol/l) | 0.387 | -0.059 | ln
OR=0.387-0.059xTotal-C | -0.77 | 0.59 | -0.25 | 0.06 | <0.001 |
| Sex (% female) | 0.804 | –0.053 | ln
OR=0.804-0.053xFemale | -0.26 | 0.07 | -0.07 | 0.01 | 0.11 (ns) |
Quality assessment of the included
studies
The JADAD quality analysis evaluates the
methodological rigor of the included clinical trials based on
criteria such as randomization, blinding, and reporting of
withdrawals/dropouts, yielding scores ranging from 0 to 5. Out of
the 11 studies assessed, 8 (2,11,14,15,20,22-24)
received the highest JADAD score of 5, indicating excellent
methodological quality characterized by proper randomization,
double-blinding, and clear reporting of withdrawals/dropouts.
Meanwhile, 3 (21,25,26)
received a JADAD score of 4, mainly due to limitations in blinding,
though randomization and withdrawals/dropouts were adequately
addressed. These results highlight that most studies included in
the analysis are of high methodological quality, thereby supporting
the reliability and robustness of their findings (Table IV).
| Table IVJADAD quality analysis table. |
Table IV
JADAD quality analysis table.
| First author/s,
year | Randomization
(0-2) | Blinding (0-2) |
Withdrawals/dropouts (0-1) | Total score
(0-5) | (Refs.) |
|---|
| Davies et
al, 2021 | 2 | 2 | 1 | 5 | (24) |
| Garvey et
al, 2022 | 2 | 1 | 1 | 4 | (26) |
| Husain et
al, 2019 | 2 | 2 | 1 | 5 | (14) |
| Kosiborod et
al, 2023 | 2 | 2 | 1 | 5 | (22) |
| Kosiborod et
al, 2024 | 2 | 2 | 1 | 5 | (23) |
| Lincoff et
al, 2023 | 2 | 2 | 1 | 5 | (11) |
| Marso et al,
2016 | 2 | 2 | 1 | 5 | (8) |
| Rubino et
al, 2021 | 2 | 1 | 1 | 4 | (25) |
| Rubino et
al, 2022 | 2 | 1 | 1 | 4 | (21) |
| Wadden et
al, 2021 | 2 | 2 | 1 | 5 | (20) |
| Wilding et
al, 2021 | 2 | 2 | 1 | 5 | (15) |
Discussion
The preset systematic review and meta-analysis
evaluated the effects of semaglutide on MACE in patients with and
without DM. Findings from 11 high-quality RCTs involving over
25,000 participants demonstrated that semaglutide significantly
reduces the risk of cardiovascular outcomes, including
cardiovascular death, non-fatal myocardial infarction, and
non-fatal stroke. The pooled OR of 0.68 (95% CI, 0.52-0.91)
confirms the robust cardiovascular benefits associated with
semaglutide, consistent with findings from landmark trials such as
STEP, SELECT and SUSTAIN-6 (11,14,24,26).
The pooled effect size, indicating a 32% reduction
in MACE, aligns with findings from the SELECT trial, where
semaglutide reduced cardiovascular events by 20% in patients with
obesity but without diabetes (11).
Lingvay et al (7) further
demonstrated that the cardiovascular benefits of semaglutide were
independent of baseline HbA1c levels or changes in HbA1c,
supporting the hypothesis that mechanisms beyond glycemic control
contribute to these benefits. Similarly, SUSTAIN-6, an earlier
trial involving T2DM patients, reported a significant reduction in
cardiovascular death, non-fatal myocardial infarction, and
non-fatal stroke, with semaglutide achieving an OR of 0.74(12). The present's study sensitivity
analysis further confirmed the robust cardiovascular benefits of
semaglutide, with point estimates ranging from 0.630 to 0.761, all
favoring semaglutide. These findings are further supported by Verma
et al (6), who demonstrated
that the cardiovascular benefits of semaglutide persisted across
sex subgroups, indicating consistent cardiovascular benefits
regardless of patient demographics. The analysis of the present
study differs fundamentally from the recent meta-analysis by Moiz
et al (27), which examined
once-weekly semaglutide exclusively for weight-loss efficacy and
safety in non-diabetic adults. A second recent systematic review
focused on adults with overweight/obesity irrespective of diabetes
status; this is also different from what we have conducted in the
present study (28). Accordingly,
the present study directly addressed the three knowledge gaps
highlighted in the Introduction. First, by pooling six diabetes
trials and five non-diabetes trials, it was showed that the 32%
MACE reduction is consistent across glycemic and non-glycemic
settings (interaction P=0.62), thereby resolving uncertainty about
population-specific efficacy. Second, stratified analyses
demonstrate overlapping benefit for the historical glycemic doses
(0.5/1.0 mg SC; OR 0.72), the obesity dose (2.4 mg SC; OR 0.66),
and the oral 14 mg formulation (OR 0.74), indicating that
cardio-protection is not dose-limited. Third, mixed-effects
meta-regression identifies age, HbA1c and blood pressure as
positive effect modifiers, whereas lower body weight and LDL
attenuate risk, quantifying for the first time how baseline
cardiometabolic profiles shape treatment response.
The moderator analysis revealed significant
associations between cardiovascular outcomes and several
patient-specific factors. A positive association suggests that
older populations derive greater cardiovascular benefits, likely
due to higher baseline cardiovascular risk. This aligns with
findings from Phizackerley (5), who
observed more pronounced benefits in older patients with
established CVD. Both systolic and diastolic blood pressures
demonstrated significant positive associations with cardiovascular
outcomes, suggesting that the blood pressure-lowering effects of
semaglutide contribute to its cardioprotective properties. Previous
studies have shown that semaglutide reduces systolic blood pressure
by 4-6 mmHg, likely mediated through weight loss and improved
endothelial function (3,7). A significant positive association
confirms that patients with elevated baseline HbA1c levels
experience greater reductions in MACE. This aligns with the
findings of the PIONEER-6 trial, where improved glycemic control
significantly reduced cardiovascular events (14). Negative associations for body
weight, LDL and total cholesterol highlight the favorable metabolic
effects of semaglutide. Semaglutide promotes weight loss primarily
through reduced appetite and energy intake, which translates into
improved lipid profiles and reduced cardiovascular stress. These
findings collectively indicate that the cardiovascular benefits of
semaglutide are driven by multiple factors, including blood
pressure reduction, weight loss and glycemic control, supporting a
multifactorial mechanistic rationale. The cardiovascular benefits
of semaglutide can be attributed to its unique mechanisms of action
as a GLP-1 RA. GLP-1 RAs enhance glycemic control by stimulating
glucose-dependent insulin secretion and suppressing glucagon
release. However, evidence suggests that the cardioprotective
effects of semaglutide extend beyond glycemic control. Chronic
inflammation is a key driver of atherosclerosis and cardiovascular
events. Semaglutide has been shown to reduce inflammatory markers,
such as C-reactive protein and interleukin-6, leading to improved
endothelial function and reduced plaque formation (1). Semaglutide induces substantial weight
loss, which in turn reduces cardiovascular risk factors such as
hypertension, dyslipidemia and insulin resistance. In the SELECT
trial, patients experienced an average weight loss of 10%, which
likely contributed to the observed reduction in MACE (5). Semaglutide lowers blood pressure
through weight loss and directly affects vascular tone and
endothelial function. These effects may be mediated through
enhanced natriuresis and improved arterial compliance (6). Semaglutide also reduces lipid-driven
cardiovascular risk by lowering LDL cholesterol and triglyceride
levels. Improved lipid profiles were consistently reported in
trials such as SUSTAIN-6 and SELECT (4).
The assessment of publication bias revealed minimal
concerns, as evidenced by the funnel plot and Begg and Mazumdar's
test. Egger's regression intercept was statistically significant,
suggesting slight asymmetry that may be possibly due to small-study
effects. However, the fail-safe N analysis indicated that 48
missing studies would be required to nullify the observed effect,
emphasizing the robustness of our findings. Duval and Tweedie's
trim-and-fill method identified no missing studies, further
supporting the reliability of the results. The prediction interval
analysis revealed moderate heterogeneity across studies, likely
attributable to differences in baseline characteristics, follow-up
durations, and dosages of semaglutide.
The list price of Semaglutide (≈US$ 13,000 year)
yields incremental cost-effectiveness ratios (ICER) of US$
180,000-260,000 per quality-adjusted life-year (QALY) in
average-risk U.S. populations, exceeding the widely accepted
threshold of US$ 100,000/QALY (29,30).
The ICER falls below US$ 100,000/QALY only in very-high-risk
subgroups (≥3% annual CV risk) or with deep price concessions
(30). No cost-utility analysis has
been conducted in low-income countries.
Several limitations must be acknowledged. First, the
included studies exhibited some variability in baseline patient
characteristics, including diabetes status, cardiovascular history
and treatment duration, which may have introduced heterogeneity.
For example, the PIONEER-6 and SUSTAIN-6 studies used different
doses from the other included studies. However, the
cardioprotective effect of semaglutide remained consistent across
both the historical glycemic doses (0.5/1 mg) and the newer obesity
dose (2.4 mg), suggesting that mechanisms other than additional
weight loss, such as blood-pressure, lipid and anti-inflammatory
effects, contribute to MACE reduction. Second, while the JADAD
analysis confirmed high methodological quality, some studies lacked
adequate blinding, potentially introducing bias. Third, the
presence of small-study effects, as indicated by Egger's test,
suggests that the possibility of publication bias cannot be
completely ruled out. Fourth, due to the consistent scarcity of
real-world data, the generalizability of the findings may be
limited to populations closely matching those included in the
trials. Fifth, 5 of the 11 studies were conducted by two research
groups (Wilding/Wadden STEP program, n=3; Kosiborod HFpEF program,
n=2). Shared leadership may introduce analytic or reporting
homogeneity, which could, in principle, exaggerate a pooled effect.
Nevertheless, i) all trials were multicenter and independently
monitored, ii) the Jadad score was high (4-5/5), and iii) our
leave-one-out institution-level sensitivity analyses altered the
pooled OR by less than 0.03. It should be noted, however, that some
overlap in sponsor or investigator may compromise the absolute
independence between studies. Finally, most of the trials enrolled
predominantly White patients and were conducted in Western Europe
or North America, thereby limiting the external validity of the
findings to Hispanic, Asian and low-income populations. Given that
fewer than three trials reported race-based subgroup efficacy, the
meta-analysis of the present study was underpowered to examine
population-specific benefits. Future RCTs should prioritize
enrolling underrepresented minorities and study sites in low- and
lower-middle-income countries to determine whether the
cardioprotective benefits of semaglutide are consistent across
diverse genetic and socioeconomic backgrounds.
In conclusion, the present systematic review and
meta-analysis demonstrated that semaglutide significantly reduces
the risk of MACE in patients with and without DM. The
cardiovascular benefits of semaglutide appear to be consistent
across diverse patient populations and are mediated by multiple
factors, including enhanced glycemic control, weight loss, blood
pressure reduction and improved lipid profile. Beyond its metabolic
effects, semaglutide’s anti-inflammatory and cardioprotective
properties enhance its role as a multifaceted intervention for
cardiovascular risk management. These findings further highlight
its potential to address CVD, a leading cause of global morbidity
and mortality, offering substantial benefits for individuals with
obesity, diabetes and established CV risk factors. Expanding
research to include real-world populations will help validate the
findings from RCTs and improve the generalizability of
semaglutide's benefits. Furthermore, investigating semaglutide's
efficacy across specific patient subgroups, such as those with
heart failure, chronic kidney disease, or varying baseline risk
factors, can help personalize treatment approaches. By pursuing
these future research directions, semaglutide can further
revolutionize CV risk management and improve outcomes across
diverse patient populations.
Supplementary Material
Sensitivity analysis for
cardiovascular outcomes after the exclusion of studies with lower
semaglutide dose. The sensitivity analysis shows the robustness of
the pooled effect estimate by removing studies with lower
semaglutide doses. The P-value remains consistently below
significance, indicating that semaglutide's cardiovascular benefits
are not changed by the exclusion of these studies. CI, confidence
interval; CVD, cardiovascular disease.
Mixed-effects meta-regression of
semaglutide weekly dose (mg) vs. log-odds ratio for MACE. Each
point represents one of the trial comparisons; its horizontal
position is the mean weekly dose tested (0.5, 1.0 and 2.4 mg SC or
14 mg oral ≈2 mg SC-equivalent), and its vertical position is the
study's natural-log odds ratio for MACE. Point size is proportional
to the inverse variance (larger circles=greater weight). The solid
line is the fitted random-effects meta-regression
(β1=-0.07 per mg; P=0.18), and the shaded band is the
95% confidence belt. The negative, non-significant slope indicates
that higher weekly doses tend toward greater cardio-protection, but
the dose-effect relation does not reach statistical significance
after accounting for between-study heterogeneity
(τ2=0.012). MACE, major adverse cardiovascular
events.
Acknowledgements
Not applicable.
Funding
Funding: No funding was received.
Availability of data and material
The data generated in the present study may be
requested from the corresponding author.
Authors' contributions
YL and CL conceptualized and designed the present
study and interpreted the data. LC and SL acquired and analyzed the
data. YL drafted the manuscript. YM substantively revised the
manuscript. YL and CL approved submitted version. YL and CL confirm
the authenticity of all raw data. All the authors agree both to be
personally accountable for their contributions and to ensure that
questions related to the accuracy or integrity of any part of the
work, even ones in which the author was not personally involved,
are appropriately investigated and resolved and the resolution is
documented in the literature. All authors read and approved the
final version of the manuscript.
Ethics approval and consent to
participate
Not applicable.
Patient consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Ussher JR and Drucker DJ: Glucagon-like
peptide 1 receptor agonists: Cardiovascular benefits and mechanisms
of action. Nat Rev Cardiol. 20:463–474. 2023.PubMed/NCBI View Article : Google Scholar
|
|
2
|
Ferhatbegović L, Mršić D and
Macić-Džanković A: The benefits of GLP1 receptors in cardiovascular
diseases. Front Clin Diabetes Healthc. 4(1293926)2023.PubMed/NCBI View Article : Google Scholar
|
|
3
|
Heuvelman VD, Van Raalte DH and Smits MM:
Cardiovascular effects of glucagon-like peptide 1 receptor
agonists: From mechanistic studies in humans to clinical outcomes.
Cardiovasc Res. 116:916–930. 2020.PubMed/NCBI View Article : Google Scholar
|
|
4
|
Harris E: Semaglutide improved
cardiovascular health in people without diabetes. JAMA.
330:2241–2242. 2023.PubMed/NCBI View Article : Google Scholar
|
|
5
|
Phizackerley D: Semaglutide reduces the
absolute risk of major cardiovascular events by 1.5. BMJ.
384(q53)2024.PubMed/NCBI View
Article : Google Scholar
|
|
6
|
Verma S, Colhoun HM, Dicker D, Verma S,
Colhoun HM, Dicker D, Hovingh GK, Kahn SE, Kautzky-Willer A,
Lingvay I, et al: Semaglutide effects on cardiovascular outcomes in
people with overweight or obesity (SELECT): Outcomes by sex. J Am
Coll Cardiol. 84:1678–1682. 2024.PubMed/NCBI View Article : Google Scholar
|
|
7
|
Lingvay I, Deanfield J, Kahn SE, Weeke PE,
Toplak H, Scirica BM, Rydén L, Rathor N, Plutzky J, Morales C, et
al: Semaglutide and cardiovascular outcomes by baseline HbA1c and
change in HbA1c in people with overweight or obesity but without
diabetes in SELECT. Diabetes Care. 47:1360–1369. 2024.PubMed/NCBI View Article : Google Scholar
|
|
8
|
Marso SP, Daniels GH, Brown-Frandsen K,
Kristensen P, Mann JF, Nauck MA, Nissen SE, Pocock S, Poulter NR,
Ravn LS, et al: Liraglutide and cardiovascular outcomes in type 2
diabetes. N Engl J Med. 375:311–322. 2016.PubMed/NCBI View Article : Google Scholar
|
|
9
|
Gerstein HC, Colhoun HM, Dagenais GR, Diaz
R, Lakshmanan M, Pais P, Probstfield J, Riesmeyer JS, Riddle MC,
Rydén L, et al: Dulaglutide and cardiovascular outcomes in type 2
diabetes (REWIND): A double-blind, randomised placebo-controlled
trial. Lancet. 394:121–130. 2019.PubMed/NCBI View Article : Google Scholar
|
|
10
|
Hernandez AF, Green JB, Janmohamed S,
D'Agostino RB Sr, Granger CB, Jones NP, Leiter LA, Rosenberg AE,
Sigmon KN, Somerville MC, et al: Albiglutide and cardiovascular
outcomes in patients with type 2 diabetes and cardiovascular
disease (Harmony Outcomes): A double-blind, randomised
placebo-controlled trial. Lancet. 392:1519–1529. 2018.PubMed/NCBI View Article : Google Scholar
|
|
11
|
Lincoff AM, Brown-Frandsen K, Colhoun HM,
Deanfield J, Emerson SS, Esbjerg S, Hardt-Lindberg S, Hovingh GK,
Kahn SE, Kushner RF, et al: Semaglutide and cardiovascular outcomes
in obesity without diabetes. N Engl J Med. 389:2221–2232.
2023.PubMed/NCBI View Article : Google Scholar
|
|
12
|
Marso SP, Holst AG and Vilsbøll T:
Semaglutide and cardiovascular outcomes in patients with type 2
diabetes. N Engl J Med. 376:891–892. 2017.PubMed/NCBI View Article : Google Scholar
|
|
13
|
Lau J, Bloch P, Schäffer L, Pettersson I,
Spetzler J, Kofoed J, Madsen K, Knudsen LB, McGuire J, Steensgaard
DB, et al: Discovery of the once-weekly glucagon-like peptide-1
(GLP-1) analogue semaglutide. J Med Chem. 58:7370–7380.
2015.PubMed/NCBI View Article : Google Scholar
|
|
14
|
Husain M, Birkenfeld AL, Donsmark M,
Dungan K, Eliaschewitz FG, Franco DR, Jeppesen OK, Lingvay I,
Mosenzon O, Pedersen SD, et al: Oral semaglutide and cardiovascular
outcomes in patients with type 2 diabetes. N Engl J Med.
381:841–851. 2019.PubMed/NCBI View Article : Google Scholar
|
|
15
|
Wilding JPH, Batterham RL, Calanna S,
Davies M, Van Gaal LF, Lingvay I, McGowan BM, Rosenstock J, Tran
MTD, Wadden TA, et al: Once-weekly semaglutide in adults with
overweight or obesity. N Engl J Med. 384:989–1002. 2021.PubMed/NCBI View Article : Google Scholar
|
|
16
|
Pi-Sunyer X, Astrup A, Fujioka K, Greenway
F, Halpern A, Krempf M, Lau DC, le Roux CW, Violante Ortiz R,
Jensen CB, et al: A randomized, controlled trial of 3.0 mg of
liraglutide in weight management. N Engl J Med. 373:11–22.
2015.PubMed/NCBI View Article : Google Scholar
|
|
17
|
Frias JP, Bonora E, Nevarez Ruiz L, Li YG,
Yu Z, Milicevic Z, Malik R, Bethel MA and Cox DA: Efficacy and
safety of dulaglutide 3.0 mg and 4.5 mg versus dulaglutide 1.5 mg
in metformin-treated patients with type 2 diabetes in a randomized
controlled trial (AWARD-11). Diabetes Care. 44:765–773.
2021.PubMed/NCBI View Article : Google Scholar
|
|
18
|
Page MJ, McKenzie JE, Bossuyt PM, Boutron
I, Hoffmann TC, Mulrow CD, Shamseer L, Tetzlaff JM, Akl EA, Brennan
SE, et al: The PRISMA 2020 statement: an updated guideline for
reporting systematic reviews. BMJ. 372(n71)2021.PubMed/NCBI View
Article : Google Scholar
|
|
19
|
Clark HD, Wells GA, Huët C, McAlister FA,
Salmi LR, Fergusson D and Laupacis A: Assessing the quality of
randomized trials: Reliability of the Jadad scale. Control Clin
Trials. 20:448–452. 1999.PubMed/NCBI View Article : Google Scholar
|
|
20
|
Wadden TA, Bailey TS, Billings LK, Davies
M, Frias JP, Koroleva A, Lingvay I, O'Neil PM, Rubino DM, Skovgaard
D, et al: Effect of subcutaneous semaglutide vs placebo as an
adjunct to intensive behavioral therapy on body weight in adults
with overweight or obesity: The STEP 3 randomized clinical trial.
JAMA. 325:1403–1413. 2021.PubMed/NCBI View Article : Google Scholar
|
|
21
|
Rubino DM, Greenway FL, Khalid U, O'Neil
PM, Rosenstock J, Sørrig R, Wadden TA, Wizert A and Garvey WT: STEP
8 Investigators. Effect of weekly subcutaneous semaglutide vs daily
liraglutide on body weight in adults with overweight or obesity
without diabetes: The STEP 8 randomized clinical trial. JAMA.
327:138–150. 2022.PubMed/NCBI View Article : Google Scholar
|
|
22
|
Kosiborod MN, Abildstrøm SZ, Borlaug BA,
Butler J, Rasmussen S, Davies M, Hovingh GK, Kitzman DW, Lindegaard
ML, Møller DV, et al: Semaglutide in patients with heart failure
with preserved ejection fraction and obesity. N Engl J Med.
389:1069–1084. 2023.PubMed/NCBI View Article : Google Scholar
|
|
23
|
Kosiborod MN, Petrie MC, Borlaug BA,
Butler J, Davies MJ, Hovingh GK, Kitzman DW, Møller DV, Treppendahl
MB, Verma S, et al: Semaglutide in patients with obesity-related
heart failure and type 2 diabetes. N Engl J Med. 390:1394–1407.
2024.PubMed/NCBI View Article : Google Scholar
|
|
24
|
Davies M, Færch L, Jeppesen OK, Pakseresht
A, Pedersen SD, Perreault L, Rosenstock J, Shimomura I, Viljoen A,
Wadden TA, et al: Semaglutide 2·4 mg once a week in adults with
overweight or obesity, and type 2 diabetes (STEP 2): A randomised,
double-blind, double-dummy, placebo-controlled, phase 3 trial.
Lancet. 397:971–984. 2021.PubMed/NCBI View Article : Google Scholar
|
|
25
|
Rubino D, Abrahamsson N, Davies M, Hesse
D, Greenway FL, Jensen C, Lingvay I, Mosenzon O, Rosenstock J,
Rubio MA, et al: Effect of continued weekly subcutaneous
semaglutide vs placebo on weight loss maintenance in adults with
overweight or obesity: The STEP 4 randomized clinical trial. JAMA.
325:1414–1425. 2021.PubMed/NCBI View Article : Google Scholar
|
|
26
|
Garvey WT, Batterham RL, Bhatta M, Buscemi
S, Christensen LN, Frias JP, Jódar E, Kandler K, Rigas G, Wadden
TA, et al: Two-year effects of semaglutide in adults with
overweight or obesity: The STEP 5 trial. Nat Med. 28:2083–2091.
2022.PubMed/NCBI View Article : Google Scholar
|
|
27
|
Moiz A, Levett JY, Filion KB, Peri K,
Reynier P and Eisenberg MJ: Long-term efficacy and safety of
once-weekly semaglutide for weight loss in patients without
diabetes: A systematic review and meta-analysis of randomized
controlled trials. Am J Cardiol. 222:121–130. 2024.PubMed/NCBI View Article : Google Scholar
|
|
28
|
Cleto AS, Schirlo JM, Beltrame M, Gomes
VHO, Acras IH, Neiverth GS, Silva BB, Juliatto BMS, Machozeki J and
Martins CM: Semaglutide effects on safety and cardiovascular
outcomes in patients with overweight or obesity: A systematic
review and meta-analysis. Int J Obes (Lond). 49:21–30.
2025.PubMed/NCBI View Article : Google Scholar
|
|
29
|
Hwang JH, Laiteerapong N, Huang ES and Kim
DD: Lifetime health effects and cost-effectiveness of tirzepatide
and semaglutide in US adults. JAMA Health Forum.
6(e245586)2025.PubMed/NCBI View Article : Google Scholar
|
|
30
|
Rennert-May E, Manns B, Clement F,
Spackman E, Collister D, Sumner G, Leal J, Miller RJH and Chew DS:
Cost-effectiveness of semaglutide in patients with obesity and
cardiovascular disease. Can J Cardiol. 41:128–136. 2025.PubMed/NCBI View Article : Google Scholar
|