Introduction
Primary pulmonary tumors are extremely rare in
children, with an annual incidence of <2 per million (1). The ratio of primary to metastatic to
inflammatory/congenital tumors is reported to be 1:5:60 (2-4).
The pathological spectrum of primary pulmonary tumors is complex
and diverse (5). According to the
histological origin, there are five main categories: Mesenchymal
tumors (rhabdomyosarcoma and inflammatory myofibroblastic tumor),
epithelial tumors (alveolar carcinoma), lymphoid tumors (Langerhans
cell histiocytosis and lymphoma), embryonic tumors (hamartoma and
pleuropulmonary blastoma) and neuroendocrine tumors (small cell
carcinoma and large cell neuroendocrine carcinoma).
The clinical manifestations often present with
nonspecific symptoms, including fever, persistent coughing,
dyspnea, chest pain and recurrent pulmonary infections, depending
on the type of tumor (6-7). Some cases are asymptomatic and
detected incidentally on imaging studies (4,8). Due
to the lack of characteristic clinical features, these conditions
are frequently misdiagnosed as asthma, foreign body aspiration,
infectious diseases, or reactive airway disorders, leading to
diagnostic delays (9).
Despite the rarity, ~65-76% of these tumors are
malignant (7,10). The overall mortality rate for
primary malignant tumors is ~30%, while the mortality rate for
primary benign pulmonary tumors in children is 8.7% (4). However, they continue to have an
improved prognosis compared with those encountered in adulthood.
Early diagnosis and prompt treatment are critical for optimal
outcomes in children with primary pulmonary tumors (9). The differential diagnosis of primary
pulmonary tumors in children is complex, as it requires the
differentiation of these tumors from both metastatic pulmonary
lesions and more prevalent non-tumorous conditions. The prognosis
and treatment approaches of these three conditions are markedly
different.
In the medical literature, the incidence data on
primary pulmonary tumors in children are limited due to the
predominance of individual case reports and diagnosis-specific case
series. The present study analyzed the clinical and pathological
data of pediatric patients diagnosed with primary pulmonary tumors
by the Pathology Department of the Children's Hospital of Zhejiang
University School of Medicine between January 2016 and October
2024. The objective was to investigate the clinical and
pathological characteristics, diagnosis and therapy of primary
pulmonary tumors in children, to highlight the diagnosis and
therapy of primary pulmonary tumors.
Materials and methods
Study population
A retrospective case series review was conducted.
Clinical and pathological data were collected from 36 pediatric
patients diagnosed with primary pulmonary tumors by the Pathology
Department at the Children's Hospital of Zhejiang University School
of Medicine between January 2016 and October 2024. The age, sex,
signs and symptoms on admission, tumor localization, imaging
findings, pathology, surgical procedure, complications and
postoperative follow-up were recorded for each patient.
The present study was approved by the Ethics
Committee of Children's Hospital of Zhejiang University School of
Medicine (approval no. 2024-IRB-0397-P-01).
Pathology
All specimens were fixed with 10% formalin at room
temperature for 12 h. After gross examination and sampling, tissues
were placed in cassettes and processed in an automatic tissue
processor for postfixation, dehydration, clearing, and paraffin
infiltration as follows: Postfixation in neutral buffered formalin
(pH 7.4) at room temperature for 4 h, rinsing under running tap
water for 30 min, dehydration through graded ethanol at room
temperature (80% ethanol for 30 min, 95% ethanol for 1 h x2, and
100% ethanol for 1 h x2), clearing in xylene at room temperature
for 20 min x2, paraffin infiltration at 58-60˚C for 3 h, and
embedding at 60-62˚C. Serial sections were cut at 3-4 µm, mounted
onto slides, and baked in an oven at 60-62˚C for 2 h. The sections
were then subjected to hematoxylin and eosin (H&E) staining and
immunohistochemical staining, respectively. Images were captured
under a light microscope (bright-field; Leica Microsystems
GmbH).
H&E staining
Sections were dewaxed in xylene for 10 min x2,
rehydrated through graded ethanol series (absolute ethanol for 3
min x2, 95% ethanol for 2 min x2, 80% ethanol for 2 min, and 70%
ethanol for 2 min), and rinsed in running tap water. The sections
were stained with Gill's hematoxylin for 10 min, rinsed under
running tap water for 2 min, differentiated with 0.5% acid alcohol
for several seconds under microscopic observation when necessary,
rinsed under running water, and blued in warm water. After
immersion in 95% ethanol for 1 min, the sections were stained with
0.5% alcoholic eosin for 1 min, briefly differentiated in 80%
ethanol, dehydrated through 95% ethanol for 3 min x2 and 100%
ethanol for 3 min x2, cleared in xylene for 5 min x2, and finally
mounted with neutral balsam. All procedures were performed at room
temperature.
Immunohistochemistry
Immunohistochemical analysis was performed on
formalin-fixed paraffin-embedded tissue sections. The
immunostaining was performed on a Leica Biosystems BOND3 instrument
with a Bond Polymer Refine Detection kit (cat. no. DS9800; Leica
Microsystems GmbH). Heat-mediated antigen retrieval was performed
with Tris-EDTA buffer (pH 9.0; BOND Epitope Retrieval Solution 2;
Leica Microsystems GmbH) at 100˚C for 20 min. Endogenous peroxidase
activity was blocked using the kit-supplied Peroxide Block (3-4%
hydrogen peroxide) at room temperature for 5 min. Primary
antibodies were incubated for 15 min at room temperature. Detection
was performed using the kit-supplied Post Primary reagent (mouse
IgG linker, containing 10% animal serum) followed by the Polymer
reagent (rabbit anti-Poly-HRP-IgG); both reagents are ready-to-use
without dilution and were incubated at room temperature for 8 min
each. Chromogenic visualization was achieved using Mixed DAB Refine
at room temperature for 10 min. All sections were counterstained
with the kit-supplied Hematoxylin (<0.1%) at room temperature
for 5 min. The primary antibodies used in the present study are
listed in Table SI.
Statistical analysis
Statistical analysis was conducted using the
Statistical Package for the Social Sciences software (version 26.0;
IBM Corp.). Normally distributed data are described by mean ±
standard deviation (SD) and analyzed using the independent t-test.
Non-normally distributed data are described by median and quartile
ranges [medians, (P25, P75)] and analyzed using the Mann-Whitney
test. Categorical data are expressed as frequencies (%) and were
compared using the χ2 test or Fisher's exact test.
Graphics were generated through Microsoft Excel 2021 (Microsoft
Corporation). P<0.05 was considered to indicate a statistically
significant difference.
Results
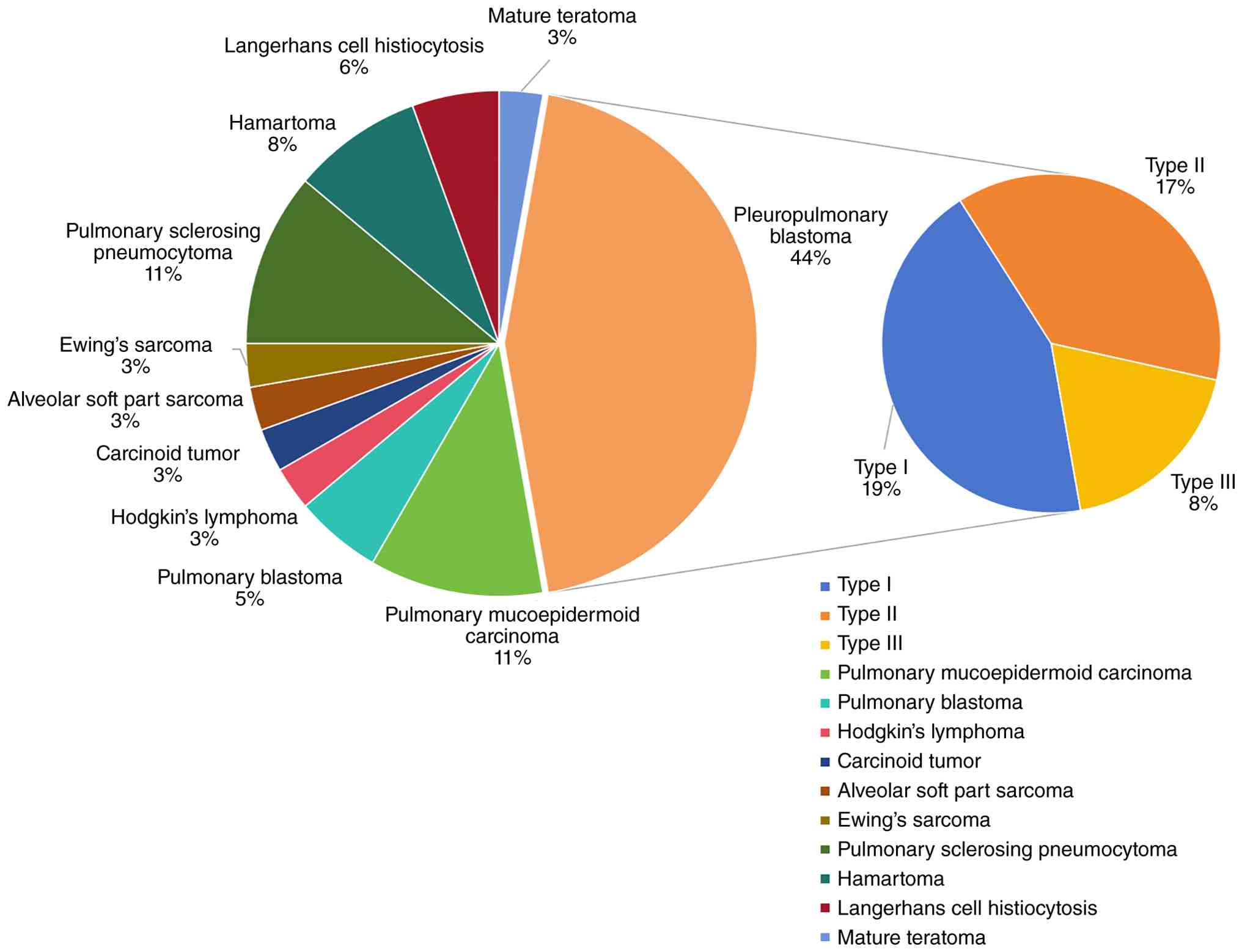
Among 36 pediatric patients with primary pulmonary
tumors, 19 were girls and 17 were boys. The age at diagnosis ranged
from 2.0 to 9.8 years, with a median age of 4.0 years. A total of
11 distinct histopathologic tumor types were identified.
Pleuropulmonary blastoma (PPB) was the most prevalent tumor type,
comprising 44.44% (16/36; 7 of type I, 6 of type II and 3 of type
III). Pulmonary mucoepidermoid carcinoma and pulmonary sclerosing
pneumocytoma each accounted for 11.11% (4/36; Table I). The remaining 12 patients
exhibited eight separate morphologies, including pulmonary
hamartoma, Langerhans cell histiocytosis, pulmonary blastoma,
mature teratoma, Hodgkin's lymphoma, carcinoid, pulmonary alveolar
soft tissue sarcoma and Ewing's sarcoma (Fig. 1).
 | Table IThe clinical and pathological
characteristics of all patients (n=36). |
Table I
The clinical and pathological
characteristics of all patients (n=36).
| Characteristic | All patients |
|---|
| Demographics | |
|
Age (year),
[median, (P25, P75)] | 4, (2, 9.75) |
|
Sex
(F:M) | 19:17 |
| Clinical
manifestations | |
|
Fever, n
(%) | 17 (47.22) |
|
Cough, n
(%) | 25 (69.44) |
|
Dyspnea, n
(%) | 6 (16.67) |
|
Chest pain,
n (%) | 6 (16.67) |
|
Hemoptysis,
n (%) | 2 (5.56) |
|
Swollen
lymph nodes, n (%) | 1 (2.78) |
| Localization | |
|
Tracheal, n
(%) | 6 (16.67) |
|
Multiplicity,
n (%) | 7 (19.44) |
| Imaging features | |
|
Maximum
diameter (cm), [median, (P25, P75)] | 4, (2, 7) |
|
Atelectasis,
n (%) | 7 (19.44) |
|
Pleural
effusion, n (%) | 8 (22.22) |
|
Pneumothorax,
n (%) | 1 (2.78) |
| Pathological
Features | |
|
Morphological
characteristicsa, n
(%) | 15 (41.67) |
|
Hemorrhage
necrosis/Calcification, n (%) | 18(50) |
|
Ki-67 index
(%), [median, (P25, P75)] | 25, (5.88, 60) |
| Treatments | |
|
Surgery, n
(%) | 35 (97.22) |
|
Chemotherapy,
n (%) | 18(50) |
|
Radiation, n
(%) | 2 (5.56) |
| Outcomes | |
|
Follow up
time (years), [median, (P25, P75)] | 1.25, (0.71,
3.00) |
|
Metastasis,
n (%) | 2 (5.56) |
|
Recurrence,
n (%) | 3 (8.33) |
The most prevalent symptoms at the time of diagnosis
were respiratory symptoms, including 25 (69.44%) patients with
cough, six (16.67%) with dyspnea and two (5.56%) with hemoptysis.
Other symptoms included fever in 17 (47.22%) and chest pain in six
(16.67%). The imaging findings at the time of diagnosis included
associated complications, including pleural effusion in 8 (22.22%),
atelectasis in seven (19.44%) and pneumothorax in one (2.78%;
Table I).
The maximum diameter of tumors ranged from 2.0-7.0
cm with a median of 4.0 cm. The imaging findings indicated that 32
(88.89%) patients had unilateral lesions, with 19 (59.38%) in the
left lung and 13 (40.62%) in the right lung. The other three
patients exhibited bilateral involvement and one presented with a
lesion located in the mid-trachea. In total, tumors in 29 (80.56%)
patients were solitary, with 11 located in the upper lobe of the
left lung, eight in the lower lobe of the left lung, two in the
upper lobe of the right lung, four in the middle lobe of the right
lung, three in the lower lobe of the right lung and one in the
mid-trachea. Other tumors in seven (19.44%) patients were multiple,
including three bilateral and four unilateral. There were 11
(30.56%) patients with cystic lesions, 10 (27.78%) with
cystic-solid lesions and 15 (41.67%) with solid lesions.
Furthermore, six patients presented with intratracheal tumors and
two had metastases to other sites (Fig.
1).
The immunohistochemical results were as follows:
Desmin was positive in 66.67% (16/24), vimentin in 100% (14/14),
Myogenic Differentiation 1 in 55.56% (10/18), myogenin in 76.92%
(10/13), smooth muscle actins in 44.44% (4/9), epithelial membrane
antigen in 75.0% (15/20), integrase interactor 1 in 100% (14/14),
S-100 in 36.36% (8/22), chromogranin A in 44.44% (4/9),
synaptophysin in 35.71% (5/14), CD34 in 100% (11/11), CD99 in
90.91% (10/11), tumor protein p53 (p53) in 100% (2/2) and thyroid
transcription factor-1 (TTF-1) in 100% (2/2).
According to the classification of tumor malignancy,
10 were benign tumors and 26 were malignant tumors (Table II). A comparison of the clinical
and pathological characteristics between benign and malignant
tumors is presented in Table
III.
| Table IIPathological types of primary
pulmonary tumors in the present study. |
Table II
Pathological types of primary
pulmonary tumors in the present study.
| A, Benign (n) |
|---|
| Pulmonary sclerosing
pneumocytoma | 4 |
| Hamartoma | 3 |
| Langerhans cell
histiocytosis | 2 |
| Mature teratoma | 1 |
| Total | 10 (27.78%) |
| B, Malignant (n) |
| Pleuropulmonary
blastoma | |
|
Type I | 7 |
|
Type II | 6 |
|
Type
III | 3 |
| Pulmonary
mucoepidermoid carcinoma | 4 |
| Pulmonary
blastoma | 2 |
| Hodgkin's
lymphoma | 1 |
| Carcinoid tumor | 1 |
| Alveolar soft part
sarcoma | 1 |
| Ewing's sarcoma | 1 |
| Total | 26 (72.22%) |
| Table IIIComparison between benign and
malignant tumors. |
Table III
Comparison between benign and
malignant tumors.
| Characteristic | Benign (n=10) | Malign (n=26) | Z/χ² | P-value |
|---|
| Demographic | | | | |
|
Age (year),
[median, (P25, P75)] | 6.5, (3.5,
10.5) | 4, (2, 9.5) | 1.193 | 0.241 |
|
Sex
(F:M) | 5:5 | 14:12 | 0 | 1 |
| Clinical
manifestation | | | | |
|
Fever, n
(%) | 4(40) | 13(50) | 0.027 | 0.868 |
|
Cough, n
(%) | 6(60) | 19 (73.08) | 0.129 | 0.720 |
|
Dyspnea, n
(%) | 0 (0) | 6 (23.08) | 1.357 | 0.244 |
|
Chest pain,
n (%) | 1(10) | 5 (19.23) | 0.028 | 0.868 |
|
Hemoptysis,
n (%) | 0 (0) | 2 (7.69) | | 1 |
|
Swollen
lymph nodes, n (%) | 0 (0) | 1 (3.85) | | 1 |
| Localization | | | | |
|
Tracheal, n
(%) | 0 (0) | 6 (23.08) | 1.357 | 0.244 |
|
Multiplicity,
n (%) | 2(20) | 5 (19.23) | 0 | 1 |
| Imaging
feature | | | | |
|
Maximum
diameter (cm) | 1.7 (2.5, 3.5) | 5.5 (3, 7) | -2.26 | 0.022 |
|
Atelectasis,
n (%) | 1(10) | 6 (23.08) | 0.175 | 0.676 |
|
Pleural
effusion, n (%) | 0 (0) | 8 (30.77) | 2.376 | 0.123 |
|
Pneumothorax,
n (%) | 1(10) | 0 (0) | | 0.278 |
| Pathological
feature | | | | |
|
Morphological
characteristicsa, n
(%) | 0 (0) | 15 (41.67) | 7.659 | 0.006 |
|
Hemorrhage
necrosis/Calcification, n (%) | 4(40) | 14 (38.89) | 0.554 | 0.457 |
|
Ki-67 index
(%) | 2 (1.38,
26.25) | 37.5 (9.63,
70) | -2.466 | 0.012 |
| Treatment | | | | |
|
Surgery, n
(%) | 10(100) | 25 (96.15) | | 1 |
|
Chemotherapy,
n (%) | 0 (0) | 18 (69.23) | 13.846 | <0.001 |
|
Radiation, n
(%) | 0 (0) | 2 (7.69) | | 1 |
| Outcome | | | | |
|
Follow up
time (years) | 0.27 (1, 1.38) | 1.5 (0.71,
3.04) | -1.243 | 0.220 |
|
Metastasis,
n (%) | 1(10) | 1 (3.85) | | 0.484 |
|
Recurrence,
n (%) | 0 (0) | 3 (11.54) | | 0.545 |
The results indicated that there were no
statistically significant differences (P>0.05) between benign
and malignant pulmonary tumors in terms of demographic
characteristics, clinical manifestations and tumor locations.
However, regarding imaging findings, the maximum diameter of
malignant tumors ranged from 3.0-7.0 cm (median: 5.5 cm), which was
markedly larger than that of benign tumors, with a range of 1.7-3.5
cm (median: 2.5 cm). The incidence of associated pleural effusion
in malignant tumors was 30.77%, markedly higher than in benign
tumors (0%). All eight patients with pleural effusion were
diagnosed with malignant tumors, including six patients of PPB, one
of pulmonary mucoepidermoid carcinoma and one of Ewing's sarcoma.
Pathologically, 41.67% of malignant tumors exhibited significant
cellular atypia or mitotic activity, compared to 0% in benign
tumors. The Ki-67 index for malignant tumors (9.63-70.0%; median:
37.5%) was markedly higher than that of benign tumors (1.38-26.25%;
median: 2.0%). The specific histological features and typical
immunohistochemical results of benign and malignant tumors are
presented in Figs. 2 and 3. Regarding treatment, 69.23% of patients
with malignant tumors received chemotherapy, a proportion markedly
higher than the 0% observed in patients with benign tumors. All
differences were statistically significant (P<0.05).
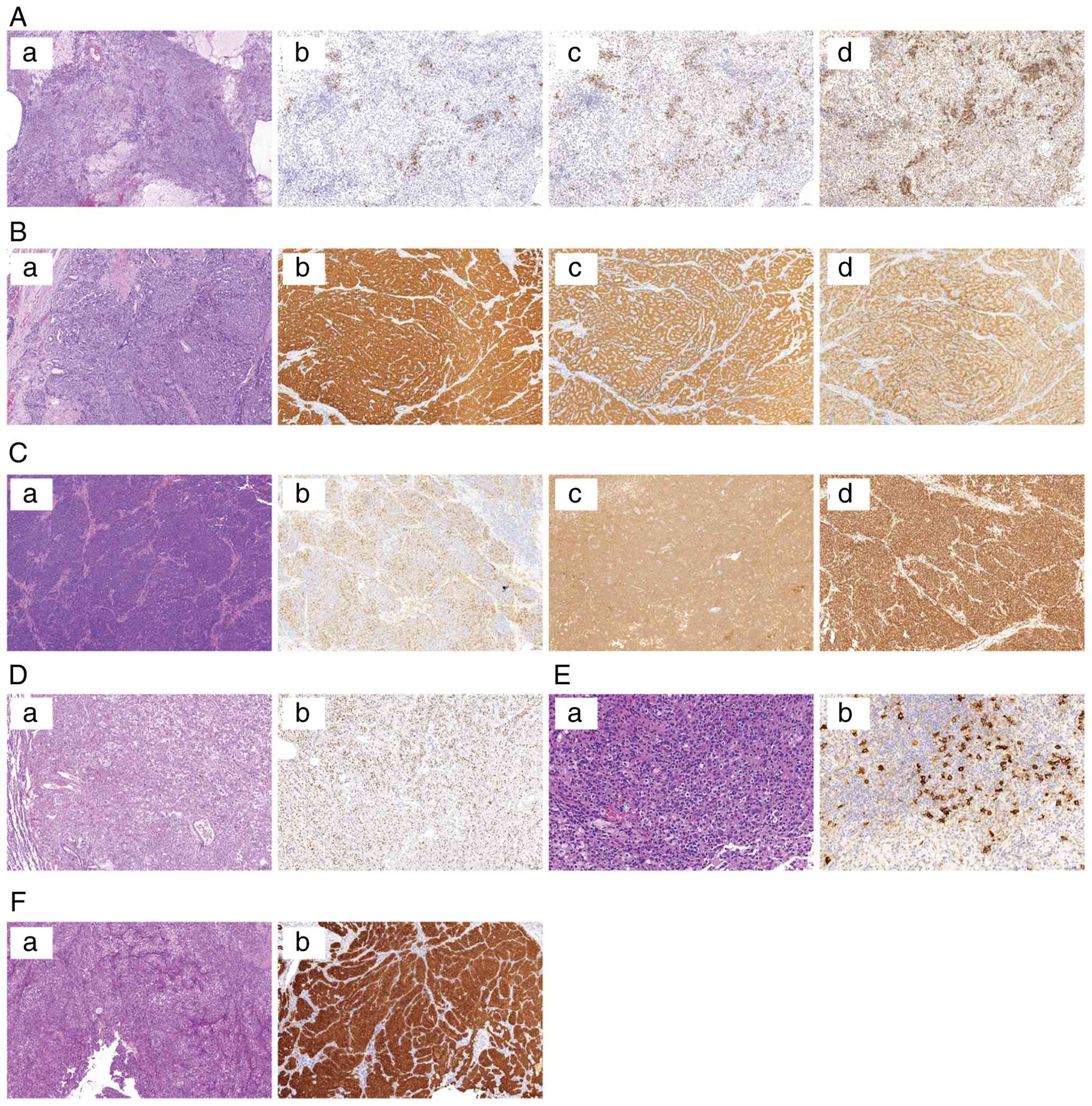 | Figure 2Six types of primary malignant
pulmonary tumors and their typical immunohistochemical positive
markers. (A) Pleuropulmonary blastoma. Tumor cells were diffusely
distributed in oval and spindle shapes with significant atypia.
Giant cells, mitotic figures, chondroid and striated muscle
differentiation were observed. (Aa; magnification, x5) The stroma
exhibited mucinous degeneration, hemorrhage and necrosis. Positive
expression of (Ab; magnification, x10) myogenin, (Ac;
magnification, x10) MyoD1 and (Ad; magnification, x10) desmin. (B)
Carcinoid tumor. (Ba; magnification, x10) Tumor cells were arranged
in a glandular pattern, with round nuclei and eosinophilic
cytoplasm. (Bb; magnification, x10) Positive expression of
synaptophysin, (Bc; magnification, x10) CK and (Bd; magnification,
x10) chromogranin A. (C) Ewing's sarcoma. (Ca; magnification, x10)
Tumor cells were round with deeply stained nuclei and certain cells
exhibited pleomorphism. Multiple mitotic figures were observed. The
cells were distributed in sheets, with some forming rosette-like
clusters. Focal areas exhibited calcification and necrosis.
Positive expression of (Cb; magnification, x10) NKX2-2, (Cc;
magnification, x10) CD99 and (Cd; magnification, x10) FLI-1. (D)
Alveolar soft part sarcoma. (Da; magnification, x10) Tumor cells
were arranged in nests and acinar patterns, with abundant
cytoplasm. Certain cells exhibited eosinophilic and clear
cytoplasm. (Db; magnification, x10) Positive for TFE3. (E)
Hodgkin's lymphoma. (Ea; magnification, x45) The tumor cells were
round or oval, with some depicting binucleation. Nucleoli were
prominent and the stroma exhibited significant eosinophilic
granulocyte infiltration. (Eb; magnification, x30) Positive for
CD30. (F) Pulmonary mucoepidermoid carcinoma. Tumor cells were
arranged in nests or glandular patterns, with abundant cytoplasm.
(Fa; magnification, x10) The regions were rich in mucin and mitotic
bodies were readily observed. (Fb; magnification, x10) Positive for
CK7. MyoD1, Myogenic Differentiation 1; CK Cytokeratin; NKX2-2, NK2
Homeobox 2; CD99, Cluster of differentiation 99; FLI-1, Friend
leukemia integration 1; TFE3, Transcription Factor Enhancer 3. |
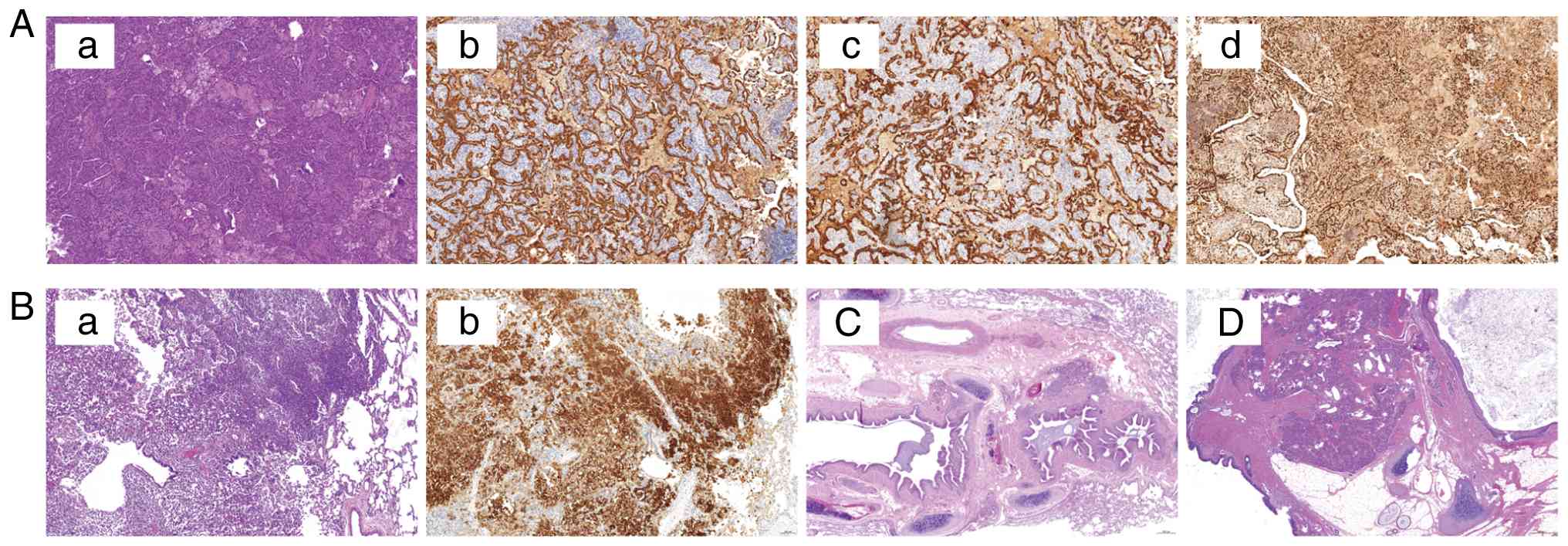 | Figure 3Four types of primary benign pulmonary
tumors and their typical immunohistochemical positive markers. (A)
Pulmonary sclerosing pneumocytoma. Tumor cells were arranged in a
papillary pattern, covered by cuboidal epithelium. The stroma
contained round and spindle-shaped cells, with certain cells
exhibiting clear cytoplasm. (Aa; magnification, x10) Focal collagen
degeneration was observed and foamy histiocytes were scattered in
localized areas. Positive expression of (Ab; magnification, x10)
CK, (Ac; magnification, x10) CK7 and (Ad; magnification, x10)
TTF-1. (B) Langerhans cell histiocytosis. (Ba; magnification, x10)
The tissue revealed sheets of eosinophilic cytoplasm, tumor cell
proliferation with nuclear grooves and infiltration by numerous
eosinophils, lymphocytes and histiocytes. Positive expression of
(Bb; magnification, x10) CD1a. (C; magnification, x2.5) Hamartoma.
Multiple dilated and distorted bronchi were observed, with mucus
plugs inside. Surrounding structures included cartilage, bone-like
tissue and adipose tissue. (D; magnification, x3.5) Mature
teratoma. (D) Tissue components, including skin and its appendages,
respiratory epithelium, pancreas and cartilage, were observed. CK
Cytokeratin; TTF-1, Thyroid Transcription Factor-1; CD, Cluster of
differentiation. |
PPB constituted the largest proportion in the
present study. A comparative analysis of the clinical and
pathological characteristics of type II and III (non-cystic) PPB
vs. other malignant non-cystic pulmonary tumors is presented in
Table IV. The age at diagnosis for
pediatric patients with PPB (range: 2.0-4.0 years; median: 3.0
years) was markedly younger than that for patients with other
malignant pulmonary tumors (range: 7.5-13.0 years; median: 10.0
years). The mean maximum tumor diameter in PPB was 7.86 cm (SD:
2.19), which was markedly larger than that of other malignant
pulmonary tumors (mean: 2.44 cm, SD: 1.76). The proportion of
multiple lesions was lower in PPB (0% vs. 62.50%). PPB exhibited a
markedly higher Ki-67 index (mean: 66.67%, SD: 17.50) compared to
other malignant pulmonary tumors (mean: 13.88%; SD: 12.88).
Furthermore, PPB had a markedly higher chemotherapy rate (88.89%
vs. 37.50%). All differences were statistically significant
(P<0.05).
| Table IVComparison between type II and III
(non-cystic) PPB and other malignant non-cystic pulmonary
tumors. |
Table IV
Comparison between type II and III
(non-cystic) PPB and other malignant non-cystic pulmonary
tumors.
| | PPB type II and Ⅲ
(n=9) | Other tumors
(n=8) | Total (n=17) | Z/χ² | P-value |
|---|
| Demographic | | | | | |
|
Age
(year) | 3 (2, 4) | 10 (7.5, 13) | 4 (2.5, 10) | -3.344 | <0.001 |
|
Sex
(F:M) | 5:4 | 4:4 | 9:8 | 0 | 1 |
| Clinical
manifestation | | | | | |
|
Fever, n
(%) | 5 (55.56) | 4(50) | 9 (52.94) | 0 | 1 |
|
Cough, n
(%) | 6 (66.67) | 7 | 13 (76.47) | 0.192 | 0.661 |
|
Dyspnea, n
(%) | 2(22.22) | 1 (12.50) | 3 (17.65) | 0 | 1 |
|
Chest pain,
n (%) | 3 (33.33) | 1 (12.50) | 4 (23.53) | 0.192 | 0.661 |
|
Hemoptysis,
n (%) | 0 (0) | 2(25) | 2 (11.76) | | 0.206 |
|
Swollen
lymph nodes, n (%) | 0 (0) | 1 (12.50) | 1 (5.88) | | 0.471 |
| Imaging
feature | | | | | |
|
Multiplicity,
n (%) | 0 (0) | 5 (62.50) | 5 (29.41) | 5.243 | 0.022 |
|
Maximum
diameter (cm) | 7.86±2.19 | 2.44±1.76 | 5.15±3.40 | 0.597 | <0.001 |
|
Pleural
effusion, n (%) | 4 (44.44) | 2(25) | 6 (35.29) | 0.108 | 0.742 |
|
Atelectasis,
n (%) | 1 (11.11) | 4(50) | 5 (29.41) | 1.496 | 0.221 |
| Pathological
feature | | | | | |
|
Ki-67 index
(%) | 66.67±17.50 | 13.88±12.88 | 41.82±31.04 | 7.002 | 0 |
| Treatment | | | | | |
|
Surgery, n
(%) | 9(100) | 7 | 16 (94.12) | | 0.471 |
|
Chemotherapy,
n (%) | 8 (88.89) | 3 (37.50) | 11 (64.71) | 2.906 | 0.088 |
|
Radiation, n
(%) | 0 (0) | 2(25) | 2 (11.76) | | 0.206 |
A patient with Hodgkin's lymphoma was confirmed by
ultrasound-guided biopsy and chemotherapy was administered. Another
35 patients underwent surgical intervention. Among them, 18
(51.43%) patients were treated with thoracoscopy and 11 (31.43%)
with thoracotomy. Notably, six (17.14%) patients were initially
treated with fiberoptic bronchoscopy and four of them subsequently
required thoracotomy, while one required thoracoscopy. A total of
34 lobectomy or segmentectomy specimens, six bronchoscopy biopsy
specimens (five of which were accompanied by lobectomy or
segmentectomy specimens) and one specimen from an ultrasound-guided
biopsy were obtained. Chemotherapy was administered to 16 (44.44%)
patients, while two (5.56%) patients received a combination of
chemotherapy and radiotherapy.
Follow-up data were available in 33 of the 36
patients, with a median follow-up duration of 15.0 months (range:
8.5-36 months). Three patients experienced recurrences, which
occurred between 9 and 13 months following the initial diagnosis.
The conditions of three patients with tumor recurrence were as
follows: The first pediatric patient of Type III PPB was diagnosed
6 years and 8 months ago, with recurrence 5 years and 7 months
later. After initial surgery and four cycles of chemotherapy, the
patient underwent a second surgery followed by eight additional
cycles of chemotherapy. Computed tomography (CT) follow-up scans
indicated a growing solid lesion in the lower right lobe. The
parents refused further surgery and the child remains under
follow-up. The second pediatric patient with Ewing sarcoma with
EWSR1-FLI1 gene fusion was diagnosed 17 months ago and experienced
recurrence for eight months. The patient received preoperative
cyclophosphamide, doxorubicin, vincristine chemotherapy, followed
by alternating ifosfamide, etoposide/vincristine, doxorubicin,
cyclophosphamide chemotherapy and surgery. The presence of new
lesions on follow-up CT scans nine months after treatment suggests
the possibility of metastasis. The third patient was diagnosed with
pulmonary blastoma and experienced recurrence one year after the
initial diagnosis. The patient received chemotherapy and
subsequently lost to follow-up. No fatalities were found among the
pediatric patients.
Discussion
Primary pulmonary tumors are rare in children and
their diagnosis and treatment can be challenging due to their
nonspecific symptoms at the time of presentation (10). Studies have reported that the most
prevalent primary malignant pulmonary tumors in children are
carcinoid tumors and PPB (4,11).
However, the histologic distribution of tumors has been markedly
altered since the previous analysis, with an increased proportion
of patients exhibiting the blastoma and mucoepidermoid histological
subtypes (12-13). The distribution of pathological
types of primary pulmonary tumors in the present study was
consistent with this trend, with PPB being the most prevalent,
accounting for 44.44%, followed by mucoepidermoid carcinoma, which
constitutes 11.11%.
In this cohort of primary pulmonary tumors,
malignant tumors accounted for 72.22%, consistent with the
previously reported range of 65-76% (2). These primary tumors, which
predominantly present as pulmonary nodules, pose a significant
diagnostic challenge in children due to their diverse appearances
and the absence of established criteria to distinguish benign from
malignant lesions. The present study compared the demographic
characteristics, clinical manifestations, imaging findings,
pathological findings, treatment approaches and prognosis of benign
and malignant primary pulmonary tumors in children. The results
indicated that differentiating between benign and malignant tumors
is challenging when based solely on demographic characteristics and
clinical manifestations. However, imaging findings, including tumor
size and the presence of pleural effusion, can provide valuable
diagnostic insights. Studies have demonstrated that pleural
effusion is prevalent in pulmonary tumors and is frequently
indicative of malignant spread to pleural membranes, which is
associated with a poor prognosis (14-15).
Therefore, in clinical practice, when pleural effusion is observed
in association with pulmonary tumors, it should be closely
monitored for potential malignant progression and given due
clinical attention. Pathologically, tumors characterized by
significant cellular atypia, prominent mitotic activity and a high
Ki-67 index are strongly associated with a higher likelihood of
malignancy.
In the present study, PPB was the most prevalent
malignant pulmonary tumor; however, its misdiagnosis rate remains
high in clinical practice. A study demonstrates that up to 51.2% of
patients are initially misdiagnosed with non-tumorous conditions,
with misdiagnosis rates of 100, 58.3 and 39.1% for type I, II and
III PPB, respectively (16).
Therefore, it is important to summarize and refine the differential
diagnosis of PPB. The present study specifically compared type II
and III PPB with other non-cystic malignant pulmonary tumors due to
the substantial proportion of non-cystic malignant tumors. The
findings revealed that a younger age at diagnosis (median: 36
months), solitary tumor presentation (100%), larger tumor diameter
(7.857±2.193 cm) and higher Ki-67 index (66.67±17.5) are
distinguishing features of PPB when compared to other non-cystic
malignant pulmonary tumors. In a report involving 350 PPB patients,
the median age at diagnosis for type II and III PPB was 37 months
(17). Additionally, 62.76% of
patients presented with tumors larger than 10.0 cm and 85.47% had
unifocal type II or type III PPB. In the present study, all
pediatric patients of PPB were unifocal, which can be attributed to
the smaller sample size. Other findings were consistent with the
results of the present study. Accordingly, it can be inferred that,
prior to pathological diagnosis, in children suspected of having a
non-cystic pulmonary tumor, a younger diagnostic age and a solitary
larger-diameter tumor are more indicative of PPB.
Recent advances in molecular biology have markedly
improved the diagnosis and classification of pulmonary tumors
(18). The 2021 World Health
Organization Classification of Lung Tumors underscored that while
morphology remains the foundation of diagnosis,
immunohistochemistry and molecular techniques are essential
adjuncts (19). It highlighted the
critical need to integrate molecular characteristics and genetic
mutations with histopathology to improve diagnostic accuracy and
prognostic evaluation. A study involving 74 patients with pulmonary
tumors found that all patients exhibited genetic mutations,
suggesting that these alterations play a key role in tumor
progression (8). Furthermore, p53
expression varies across different types of pulmonary tumors, with
high levels markedly associated with tumor progression and poor
prognosis (20). Notably, in the
present study, a Type III PPB case with recurrence exhibited strong
p53 positivity (++); however, given that p53 immunohistochemistry
was performed in only two cases (100% positive), no statistically
significant correlation can be established between p53 expression
and prognosis. Definitive assessment of TP53 mutational status
requires sequencing confirmation, which was not available in the
present study. Therefore, a multidisciplinary approach to
personalized treatment and improved outcomes is necessary for the
accurate diagnosis of pulmonary tumors, which includes the
integration of molecular pathology in addition to clinical and
imaging findings.
The present study had several limitations. First,
the median follow-up period of 15 months (range: 8.5-36 months) is
relatively short for pediatric oncology studies and long-term
survival outcomes require further investigation. Second, the lack
of comprehensive molecular diagnostics is a significant limitation
of the present study. Future studies should incorporate DICER1
mutation analysis for all PPB cases and TP53 sequencing to
correlate with p53 immunohistochemistry expression patterns.
In summary, primary pulmonary tumors in children
lack specific clinical manifestations. Imaging and pathological
characteristics are valuable in the differential diagnosis of
benign and malignant tumors. Younger age at diagnosis, solitary
lesions and larger non-cystic tumors are indicative of a higher
likelihood of PPB. The integration of molecular diagnostics is an
important direction for future research to improve early detection
and treatment outcomes.
Supplementary Material
Primary antibodies used in the present
study.
Acknowledgements
Not applicable.
Funding
Funding: The present study was supported by the National Natural
Science Foundation of China (grant nos. 82070028 and 82200027),
Innovation Team for the Diagnosis and Treatment of Childhood Asthma
(2022), Key R & D Projects of Zhejiang Provincial Science and
Technology Agency (grant no. 2023C03042) and Special Fund for the
Incubation of Young Clinical Scientist, The Children's Hospital of
Zhejiang University School of Medicine (grant no.
CHZJU2023YS005).
Availability of data and materials
The data generated in the present study are included
in the figures and/or tables of this article.
Authors' contributions
LFT, WGZ and CY conceived and designed the study and
reviewed the manuscript. YC drafted the initial manuscript. WZG, CY
and TYY analyzed the data and improved the later revision of the
article. YH, SJM, ML and XZW participated in the data collection.
LFT, WZG and CY confirm the authenticity of all the raw data. All
authors read and approved the final manuscript.
Ethics approval and consent to
participate
The present study complied with the Declaration of
Helsinki and was approved by the Ethics Committee of the Children's
Hospital of Zhejiang University School of Medicine.
Patient consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Ferrari A, Brecht IB, Gatta G, Schneider
DT, Orbach D, Cecchetto G, Godzinski J, Reguerre Y, Bien E,
Stachowicz-Stencel T, et al: Defining and listing very rare cancers
of paediatric age: Consensus of the Joint Action on Rare Cancers in
cooperation with the European Cooperative Study Group for pediatric
rare tumors. Eur J Cancer. 110:120–126. 2019.PubMed/NCBI View Article : Google Scholar
|
|
2
|
Cohen MC and Kaschula RO: Primary
pulmonary tumors in childhood: A review of 31 years' experience and
the literature. Pediatr Pulmonol. 14:222–232. 1992.PubMed/NCBI View Article : Google Scholar
|
|
3
|
Hancock BJ, Di Lorenzo M, Youssef S,
Yazbeck S, Marcotte JE and Collin PP: Childhood primary pulmonary
neoplasms. J Pediatr Surg. 28:1133–1136. 1993.PubMed/NCBI View Article : Google Scholar
|
|
4
|
Dishop MK and Kuruvilla S: Primary and
metastatic lung tumors in the pediatric population: A review and
25-year experience at a large children's hospital. Arch Pathol Lab
Med. 132:1079–1103. 2008.PubMed/NCBI View Article : Google Scholar
|
|
5
|
Yu DC, Grabowski MJ, Kozakewich HP,
Perez-Atayde AR, Voss SD, Shamberger RC and Weldon CB: Primary lung
tumors in children and adolescents: A 90-year experience. J Pediatr
Surg. 45:1090–1095. 2010.PubMed/NCBI View Article : Google Scholar
|
|
6
|
McCahon E: Lung tumours in children.
Paediatr Respir Rev. 7:191–196. 2006.PubMed/NCBI View Article : Google Scholar
|
|
7
|
Weldon CB and Shamberger RC: Pediatric
pulmonary tumors: Primary and metastatic. Semin Pediatr Surg.
17:17–29. 2008.PubMed/NCBI View Article : Google Scholar
|
|
8
|
Özcan HN, Atak F, Oğuz B, Kutluk T and
Haliloğlu M: Imaging findings of primary lung tumors in children.
Diagn Interv Radiol. 30:419–426. 2024.PubMed/NCBI View Article : Google Scholar
|
|
9
|
Özkan M: Pulmonary tumors in childhood.
Turk Gogus Kalp Damar Cerrahisi Derg. 32 (Suppl 1):S73–S77.
2024.PubMed/NCBI View Article : Google Scholar
|
|
10
|
Chen Q, Cheng J, Wang L, Lv X and Hu J:
Primary lung cancer in children and adolescents. J Cancer Res Clin
Oncol. 150(225)2024.PubMed/NCBI View Article : Google Scholar
|
|
11
|
Neville HL, Hogan AR, Zhuge Y, Perez EA,
Cheung MC, Koniaris LG, Thompson WR and Sola JE: Incidence and
outcomes of malignant pediatric lung neoplasms. J Surg Res.
156:224–230. 2009.PubMed/NCBI View Article : Google Scholar
|
|
12
|
Smith NJ, Mukherjee D, Wang Y, Brazauskas
R, Nelson AA and Cortina CS: Epidemiology and outcomes of primary
pediatric lung malignancies: Updates from the SEER database. Am J
Surg. 222:861–866. 2021.PubMed/NCBI View Article : Google Scholar
|
|
13
|
Rojas Y, Shi YX, Zhang W, Beierle EA,
Doski JJ, Goldfarb M, Goldin AB, Gow KW, Langer M, Vasudevan SA and
Nuchtern JG: Primary malignant pulmonary tumors in children: A
review of the national cancer data base. J Pediatr Surg.
50:1004–1008. 2015.PubMed/NCBI View Article : Google Scholar
|
|
14
|
Porcel JM: Malignant pleural effusions
because of lung cancer. Curr Opin Pulm Med. 22:356–361.
2016.PubMed/NCBI View Article : Google Scholar
|
|
15
|
Yang Y, Du J, Wang YS, Kang HY, Zhai K and
Shi HZ: Prognostic impact of pleural effusion in patients with
malignancy: A systematic review and meta-analysis. Clin Transl Sci.
15:1340–1354. 2022.PubMed/NCBI View Article : Google Scholar
|
|
16
|
Zhang N, Zeng Q, Ma X, Chen C, Yu J, Zhang
X, Yan D, Xu C, Liu D and Zhang Q: Diagnosis and treatment of
pleuropulmonary blastoma in children: A single-center report of 41
cases. J Pediatr Surg. 55:1351–1355. 2020.PubMed/NCBI View Article : Google Scholar
|
|
17
|
Messinger YH, Stewart DR, Priest JR,
Williams GM, Harris AK, Schultz KA, Yang J, Doros L, Rosenberg PS,
Hill DA and Dehner LP: Pleuropulmonary blastoma: A report on 350
central pathology-confirmed pleuropulmonary blastoma cases by the
International pleuropulmonary blastoma registry. Cancer.
121:276–285. 2015.PubMed/NCBI View Article : Google Scholar
|
|
18
|
Voggel S, Abele M, Seitz C, Agaimy A,
Vokuhl C, Dirksen U, Bier A, Flaadt T, Classen CF, Claviez A, et
al: Primary lung carcinoma in children and adolescents-clinical
characteristics and outcome of 12 cases from the German registry
for rare paediatric tumours (STEP). Lung Cancer. 160:66–72.
2021.PubMed/NCBI View Article : Google Scholar
|
|
19
|
Nicholson AG, Tsao MS, Beasley MB, Borczuk
AC, Brambilla E, Cooper WA, Dacic S, Jain D, Kerr KM, Lantuejoul S,
et al: The 2021 WHO classification of lung tumors: Impact of
advances since 2015. J Thorac Oncol. 17:362–387. 2022.PubMed/NCBI View Article : Google Scholar
|
|
20
|
Oduah EI and Grossman SR: Harnessing the
vulnerabilities of p53 mutants in lung cancer-focusing on the
proteasome: A new trick for an old foe. Cancer Biol Ther.
21:293–302. 2020.PubMed/NCBI View Article : Google Scholar
|