Introduction
Mechanical ventilation is the standard treatment for
patients with acute respiratory distress syndrome (ARDS). However,
a high tidal volume (Vt) may overstretch alveoli, cause
ventilator-associated lung injury (1) and increase mortality (2), partly through proinflammatory mediator
release induced by biotrauma and volutrauma (3). In ARDS patients, lung-protective
ventilation with low Vt has been firmly established as the standard
of care based on landmark trials.
By contrast, the protective effect of low Vt
ventilation in patients who received mechanical ventilation but do
not have ARDS remains controversial. Driving pressure (∆P) is also
important for the optimization of mechanical ventilation
parameters. Unlike the well-defined benefits in ARDS, the optimal
Vt strategy in non-ARDS patients is less clear, as these patients
have relatively healthy lungs and may be more tolerant of higher
Vt, but are also potentially at risk of developing
ventilator-induced lung injury. Certain studies have reported
increased morbidity and mortality with high Vt in non-ARDS patients
(4,5) and meta-analyses have demonstrated
reduced mortality, ventilation duration (6) and pulmonary complications (7) with low Vt in non-ARDS patients.
Conversely, a previous randomized control trial (RCT) reported no
mortality or ventilation benefit of low Vt compared with that of
intermediate Vt in patients without ARDS (8). These conflicting findings highlight a
knowledge gap that may require large RCTs to resolve (9).
To address this gap, the present study performed a
meta-analysis evaluating low compared with high Vt in patients
without ARDS. As outcomes are also influenced by positive
endexpiratory pressure (PEEP) (10), ΔP (11) and maximum airway pressure (Pmax)
(12), subgroup analyses stratified
by these parameters were performed. Additionally, trial sequential
analysis (TSA) was applied to assess the robustness and
conclusiveness of the evidence. Thus, the present study not only
compared low vs. high Vt in non-ARDS patients, but also explored
whether confounding factors such as Pmax, PEEP and ΔP modified the
relationship between Vt and clinical outcomes, providing a more
comprehensive evidence base for bedside ventilation management.
Materials and methods
Study design and registration
The present systematic review and meta-analysis was
performed according to the Preferred Reporting Items for Systematic
Reviews and Meta-analyses (PRISMA) guidelines (13) and the recommendations of the
Meta-analysis of Observational Studies in Epidemiology Group
(14).
Data sources and search
strategies
The PubMed, Cochrane Library and EMBASE databases
were searched from inception to February 2025 using the following
Medical Subject Headings and keywords (‘low Vt’ OR ‘protective
ventilation’ OR ‘lower Vt’). No limits were applied for language.
The reference lists of eligible studies were also searched to
identify additional relevant articles.
Inclusion and exclusion criteria
The inclusion criteria were as follows: i) RCTs or
observational studies that reported Vt; ii) patients without ARDS
at the start of ventilation (patients without ARDS were defined as
mechanically ventilated adults who did not meet the Berlin
definition criteria for ARDS (15),
consistent with the inclusion criteria of the major trials included
in this meta-analysis) (8); and
iii) adult patients (aged ≥18 years) undergoing uninterrupted
ventilation. The exclusion criteria were as follows: i) Patients
who underwent one-lung ventilation; ii) patients with ARDS at the
start of ventilation; and iii) reviews, letters, abstracts or
editorials. RCTs and observational studies were both included as
observational studies can provide real-world evidence and larger
sample sizes when RCTs are limited; a sensitivity analysis was
employed to assess the effect of including observational studies on
the overall findings.
Study selection
A total of two reviewers (MG and FX) independently
assessed titles and abstracts to select eligible studies. Full text
records were retrieved and reviewed to determine study eligibility.
Reviewers were blinded to authors' names, year of publication and
journal. Disagreements regarding study selection were resolved by
discussion and consensus.
Data extraction and study
endpoints
The reviewers independently extracted data from
eligible studies, including the author, sample size, study design,
patient history of chronic pulmonary disease, study limitations and
outcome measures.
The primary outcome was short-term mortality,
defined as 28- or 30-day mortality in the intensive care unit (ICU)
or hospital. Secondary outcomes were the number of days of
ventilation, incidence of pulmonary complications and length of
hospital stay.
Assessment of the quality of evidence
in included studies
The reviewers independently assessed the
methodological quality and risk of bias of each included study.
RCTs were assessed using the Cochrane risk of bias tool (16), cohort studies were assessed using
the Newcastle-Ottawa scale and cross-sectional studies were
assessed using the Agency for Healthcare Research and Quality
methodology checklist (17,18). The presence of publication bias was
evaluated by visual inspection of funnel plots (19). The strength of evidence was
determined using GRADE (20).
Disagreements regarding quality of evidence were resolved by
discussion and consensus.
Data synthesis and statistical
analysis
Statistical analysis was performed using RevMan (v.
5.3; The Cochrane Collaboration) and STATA (v. 12.0; StataCorp LP)
software. Odds ratios (ORs) and corresponding 95% confidence
intervals (CIs) were calculated using the inverse-variance weighted
approach. Heterogeneity between studies was assessed using the
I2 statistic (I2 ≥50% indicating substantial
heterogeneity).
Low Vt was defined as <8 ml/kg predicted body
weight, and high Vt was defined as >9 ml/kg of predicted body
weight. The effects of PEEP, ∆P and Pmax were assessed as
confounding factors. The subgroup analysis stratified by Pmax was
prespecified in the PROSPERO registration (registration no.
CRD42019119453). The following subgroup analyses were predefined:
Stratification by PEEP, ΔP and Pmax, based on their known influence
on outcomes in mechanically ventilated patients. Specifically, Pmax
was categorized as low (≤25 cmH2O) or high (>25
cmH2O) based on previously published thresholds
(6,7). Pmax was defined as peak airway
pressure in pressure assist-control ventilation and plateau
pressure in volume assist-control ventilation. Although peak
pressure and plateau pressure are physiologically distinct, both
are indicators of Pmax exposure, and limited primary studies
reported both values separately. Furthermore, in
pressure-controlled ventilation modes commonly used in
intraoperative settings, peak pressure approximates plateau
pressure in the absence of significant airway resistance (4,10).
Given the exploratory nature of this subgroup analysis, studies
were pooled using either definition while acknowledging this as a
limitation. Data describing PEEP, ∆P and Pmax were extracted, when
available. A meta-regression analysis was performed to evaluate the
associations between low vs. high Vt and PEEP, ∆P and Pmax.
Subgroup analysis was stratified by low Vt and low compared with
high Pmax. TSA was applied to control the risk of type I and type
II errors due to sparse data and repeated significance testing. TSA
calculated the required information size and monitored whether the
cumulative evidence crossed the monitoring boundaries, thereby
assessing the conclusiveness of the findings (21). P<0.05 was considered to indicate
a statistically significant difference.
Results
Study characteristics
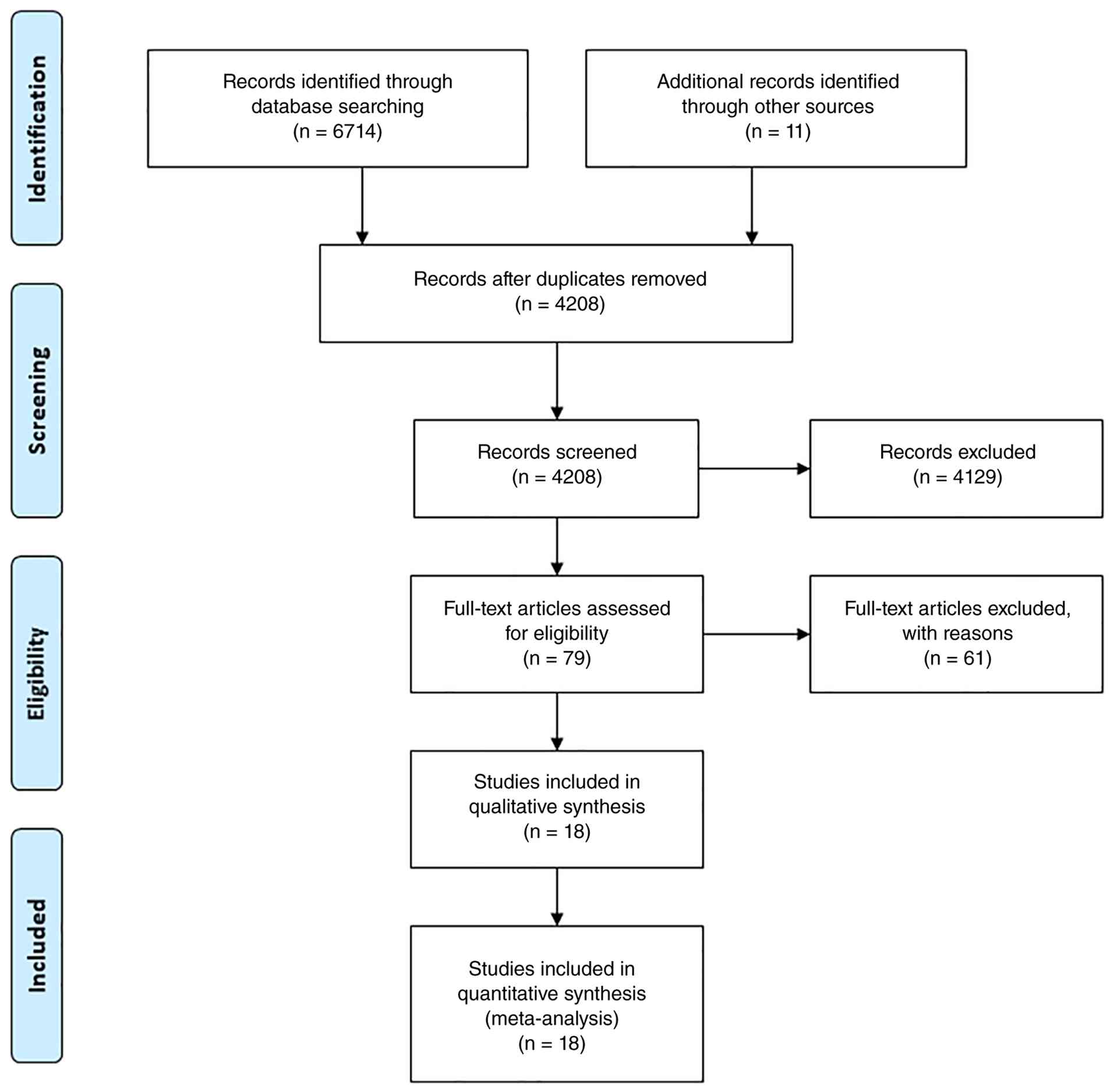
The searches identified 6,725 citations, and the
full text articles of 79 studies were reviewed. Finally, 18 studies
(8,22-38),
comprising 2 observational studies (23,37)
and 16 RCTs, were included in the meta-analysis (Fig. 1). The characteristics of the
included studies are presented in Table
I. A total of 3,042 adult patients [low Vt, 1,530 (50.3%); high
Vt, 1,512 (49.7%)] were included in the analyses. Of these, 11
studies were ICU-based and 7 were intraoperative; the mixture of
these two settings may have increased clinical heterogeneity and
this represents a limitation of the meta-analysis. The two settings
were included as they represent the two main populations of
mechanically ventilated patients without ARDS, and inclusion was
restricted to those meeting the same eligibility criteria. Although
the mixture of ICU and intraoperative studies may introduce
clinical heterogeneity, consistent inclusion and exclusion criteria
were applied across both settings to maximize patient homogeneity.
Moreover, subgroup analyses and meta-regression were performed to
explore potential sources of heterogeneity.
 | Table ICharacteristics of the included
studies. |
Table I
Characteristics of the included
studies.
| | | Low Vt | High Vt | |
|---|
| First author/s,
year | No. | Cause of
ventilation | PEEP
(cmH2O) | ΔP
(cmH2O) | Pmax
(cmH2O) | PEEP
(cmH2O) | ΔP
(cmH2O) | Pmax
(cmH2O) | Main outcome | (Refs.) |
|---|
| Determann et
al, 2010 | 150 | ICU patients | 7 | - | - | 7 | - | - | Cytokine levels in
BLF and plasma | (22) |
|
Fernandez-Bustamante et al,
2011 | 429 | Abdominal
surgery | 7 | - | 20.9 | 7 | - | 23.6 | Tidal volume
setting | (23) |
| Futier et
al, 2013 | 400 | Abdominal
surgery | 6-8 | 9.2 | 15.2 | 0 | 16.6 | 16.1 | Pulmonary and
extrapulmonary complications | (24) |
| Ge et al,
2013 | 60 | Spinal fusion | 10 | - | - | 7 | - | - | Pulmonary
Complication | (25) |
| Kuzkov et
al, 2016 | 40 | Pancreatoduodenal
surgery | 4 | 4.6 | 12.0 | 4 | 5.4 | 16.4 | Oxygenation and the
incidence of atelectases | (26) |
| Lee et al,
1990 | 103 | Surgery | 7 | - | 28.9 | 7 | - | 38.8 | The incidence of
pulmonary infection | (27) |
| Park et al,
2016 | 40 | Laparoscopic
surgery | 5 | - | - | 0 | - | - | Pulmonary
complications | (28) |
| Pi et al,
2015 | 63 | Abdominal
surgery | 9 | 6.7 | 12.0 | 0 | 10.9 | 16.4 |
PaO2/FiO2 ratio and
pulmonary compliance | (29) |
| Pinheiro de
Oliveira et al, 2010 | 20 | Scheduled
surgery | 5 | 12.2 | 17.9 | 5 | 24.3 | 29.8 | Pulmonary
inflammation | (30) |
| Severgnini et
al, 2013 | 53 | Abdominal
surgery | 10 | 8.7 | - | 0 | 16.0 | - | Pulmonary Infection
Score | (31) |
| Shen et al,
2015 | 120 | Surgery | 6 | - | - | 0 | - | - | Pulmonary
compliance | (32) |
| Simonis et
al, 2018 | 961 | ICU patients | 7 | 11.2 | - | 7 | 13.0 | - | Ventilator-free
days | (8) |
| Soh et al,
2018 | 78 | Spinal surgery | 6 | 9.5 | 16.4 | 0 | 15.2 | 16.3 | Pulmonary
complications | (33) |
| Sundar et
al, 2011 | 149 | Cardiac
surgery | 5-6 | 13.9 | - | 5-6 | 15.2 | - | Time to
extubation. | (34) |
| Treschan et
al, 2012 | 101 | Abdominal
surgery | 5 | - | 15.0 | 5 | - | 17.0 | Lung function | (35) |
| Weingarten et
al, 2010 | 40 | Abdominal
surgery | 12 | - | 14.6 | 0 | - | 16.8 | Oxygenation,
respiratory system mechanics | (36) |
| Yilmaz et
al, 2007 | 375 | ICU patients | 5 | - | 25.0 | 5 | - | 30.9 | The frequency of
acute lung injury | (37) |
| Zamani et
al, 2017 | 61 | CABG surgery | 10 | - | - | 0 | - | - | Postoperative
pulmonary complications | (38) |
The risk of bias assessment for RCTs is presented in
Fig. S1. Among the 16 RCTs, nine
trials were assessed as high risk of performance bias and detection
bias (8,25-29,32,34,37)
and two trials were assessed as unclear risk of performance bias
and detection bias as the authors considered that the outcomes were
not influenced by a lack of blinding or that blinding of
participants was impossible (30,31).
Trials were assessed as low risk of all other biases. The high risk
of bias in these nine trials may influence the reliability of the
findings; however, these trials represent the best available
evidence given the inherent challenge of blinding ventilator
settings. Future trials with blinded outcome assessment are
warranted to confirm these results. The cohort study (37) scored nine stars (Table SI) and the cross-sectional study
(23) scored seven (Table SII) according to Newcastle-Ottawa
scale and Agency for Healthcare Research and Quality methodology
checklist separately (17,18).
Low Vt ventilation does not decrease
short-term mortality in patients without ARDS
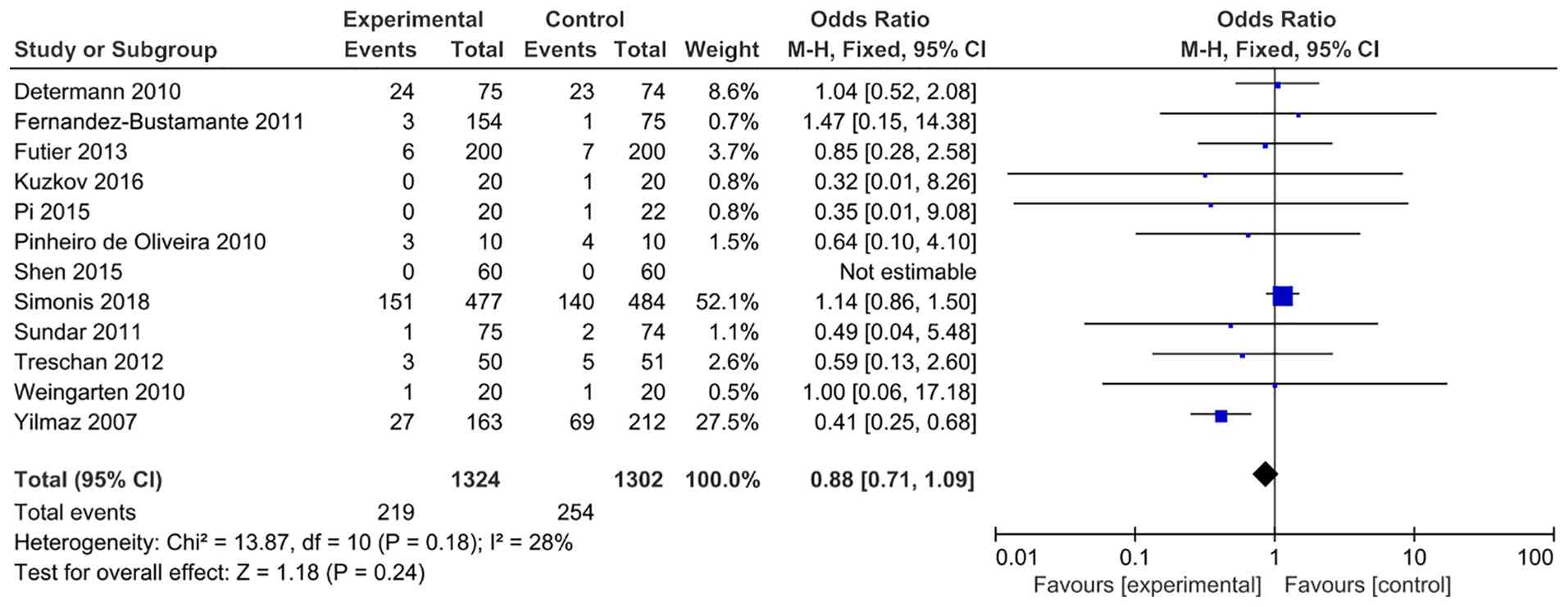
Short-term mortality was reported in 12 studies
(8,22-24,26,29,30,32,34-37)
(patients n=2,620). The short-term mortality rate was 16.4%
(219/1,324) in patients ventilated with a low Vt and 19.5%
(254/1,302) in patients ventilated with a high Vt. The
meta-analysis revealed no significant difference in short term
mortality between patients ventilated with a low Vt and those
ventilated with a high Vt (OR, 0.88; 95% CI, 0.71-1.09; P=0.24;
Fig. 2). Thus, low Vt alone did not
reduce short-term mortality in patients without ARDS. Moreover,
there was no evidence of publication bias (Fig. S2), but the overall strength of
evidence was low (Table SIII),
suggesting that further investigation may influence the
estimate.
Low Vt and low Pmax decreases
short-term mortality in patients without ARDS
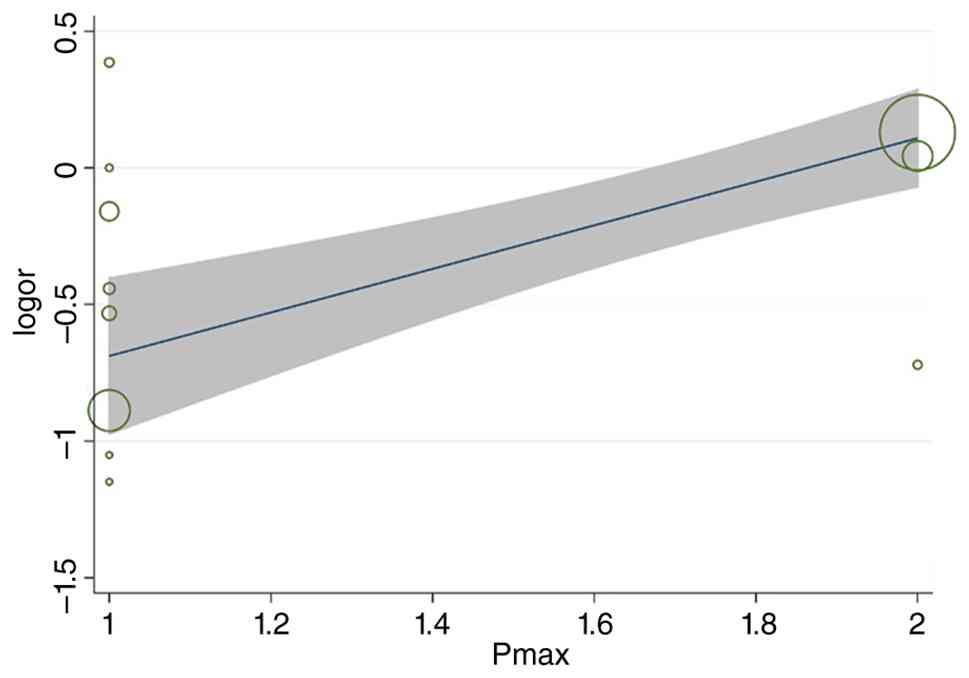
Meta-regression analyses identified Pmax (P=0.01) as
a confounding factor in the analysis of short-term mortality
(Figs. 3 and S3). Subgroup analysis stratified by Pmax
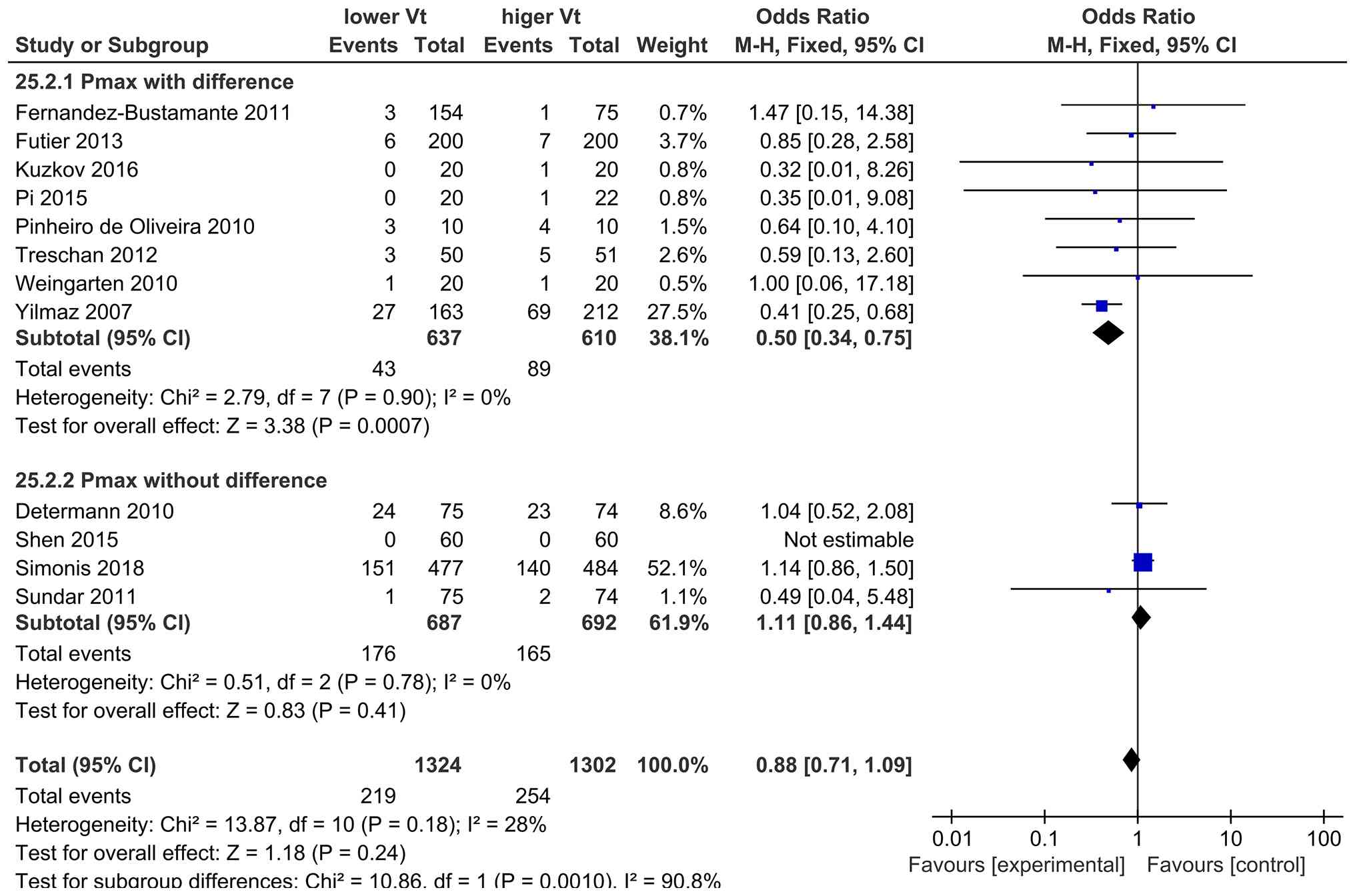
level in patients receiving low Vt ventilation demonstrated that
short-term mortality was significantly decreased in those with low
Pmax compared with those with high Pmax (OR, 0.50; 95% CI,
0.34-0.75; P=0.0007; Fig. 4). There
was no significant difference in short term mortality between
patients ventilated with a low Vt and those ventilated with a high
Vt in studies with the same or an undefined Pmax (OR, 1.11; 95% CI,
0.86-1.44; P=0.41; Fig. 4). These
findings suggested that a low Vt combined with an appropriate Pmax
may improve the outcomes of ventilated patients without ARDS.
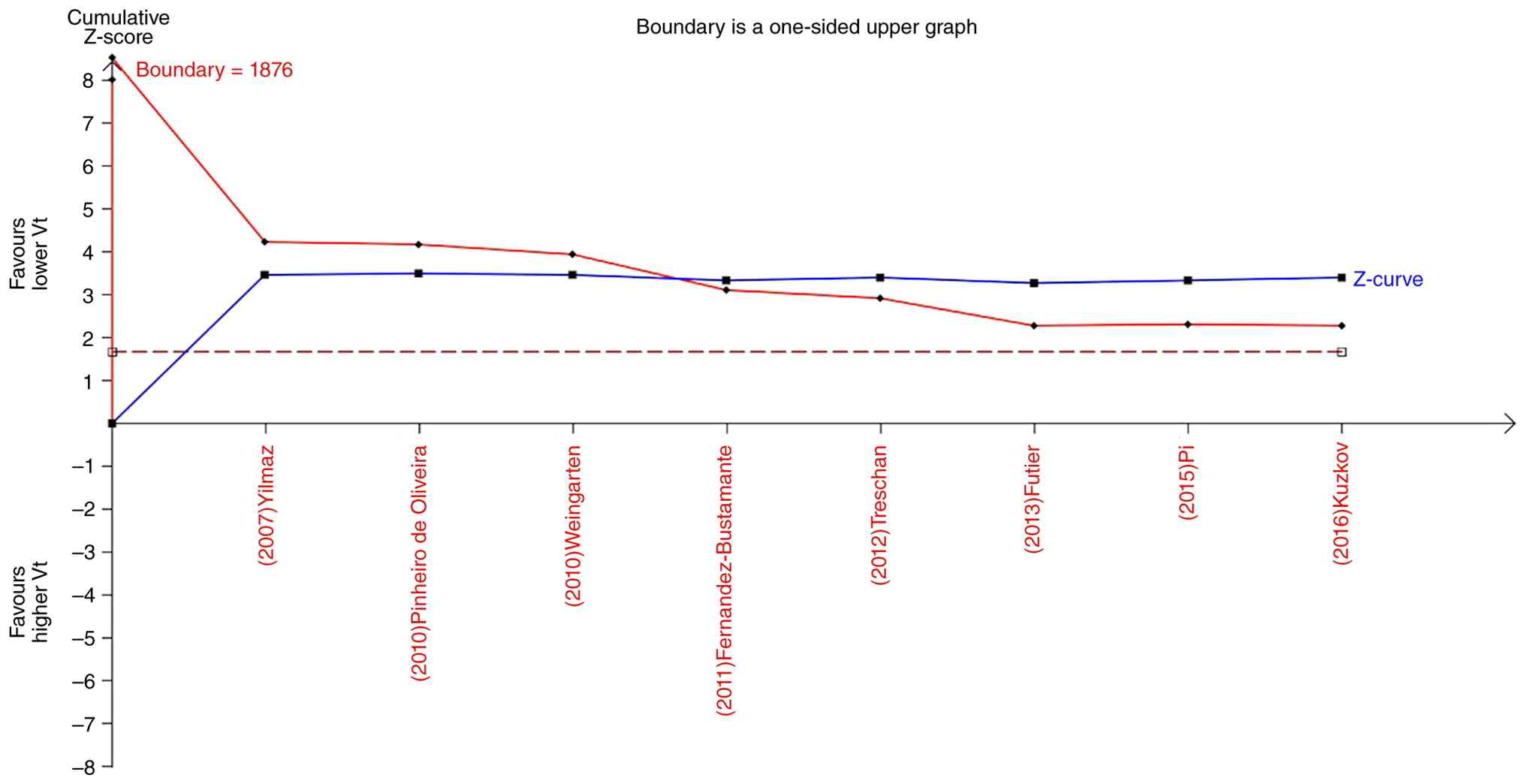
TSA revealed that the diversity-adjusted required
information size was 1,876. The cumulative z-curve crossed the
trial sequential monitoring boundary for benefit and the
conventional boundary for benefit, but did not reach the estimated
required information size (Fig. 5).
These findings should be interpreted with caution, as the required
information size was not reached. Nevertheless, the crossing of the
monitoring boundary suggests a potential benefit that warrants
confirmation in future larger trials.
Low Vt ventilation decreases the
number of days of ventilation, incidence of pulmonary complications
and hospital length of stay in patients without ARDS
The number of days of ventilation [mean difference
(MD), -1.00; 95% CI, -1.76--0.24; P=0.01; Fig. S4], the incidence of pulmonary
complications (studies, n=11; OR, 0.40; 95% CI, 0.30-0.54;
P<0.00001; Fig. S5) (24-26,28,29,31-33,35,36,38)
and hospital length of stay (studies, n=11; MD, -1.49; 95% CI,
-2.54--0.44; P=0.006; Fig. S6)
(8,23,24,26,28,29,32-36)
were significantly decreased in patients ventilated with a low Vt
compared with a high Vt. There was evidence of publication bias
among studies reporting the number of days of ventilation.
Discussion
The present systematic review and meta-analysis
evaluated the effects of low compared with high Vt ventilation in
patients without ARDS. A ventilation strategy combining low Vt with
low Pmax was associated with a significant reduction in short-term
mortality compared with low Vt combined with high Pmax.
Additionally, low Vt ventilation was associated with a reduced
duration of ventilation, incidence of pulmonary complications and
length of hospital stay compared with high Vt.
The results of the present study demonstrated that
low Vt ventilation was not associated with a reduction in
short-term mortality in patients without ARDS. Similar to the
findings from our previous study (8), the PRoVENT trial reported no
significant difference in 28- or 90-day mortality in ICU patients
without ARDS who were expected not to be extubated within 24 h of
randomization and were ventilated with a low vs. intermediate Vt
strategy (39). By contrast, a
meta-analysis of 20 articles reported that ventilation with lower
Vt was associated with reduced mortality in patients without ARDS
(40).
Potentially modifiable factors other than Vt may
affect outcomes in patients both with and without ARDS. Decreases
in ΔP resulting from changes in ventilator settings have been
reported to be strongly associated with increased survival in
patients with ARDS (41). ΔP and
plateau pressure were risk factors for mortality and ARDS in one
cohort study of mechanically ventilated patients without ARDS
(11), while ΔP was not associated
with hospital mortality in another cohort study of patients without
ARDS (42). A secondary analysis of
the PRoVENT study reported that a higher Pmax was independently
associated with higher in-hospital mortality in critically ill
patients under mechanical ventilatory support for reasons other
than ARDS (12). Accordingly, in
the present meta-analysis, the effects of PEEP, ∆P and Pmax were
assessed as confounding factors in short term mortality among
ventilated patients without ARDS using meta-regression. Results
identified Pmax as a confounding factor and pooled data showed that
a ventilation strategy including a low Vt and a low Pmax was
associated with a significant reduction in short-term mortality
compared with low Vt combined with high Pmax. However, the TSA
results should be interpreted with caution, as the required
information size was not reached. Nevertheless, the cumulative
Z-curve crossed the monitoring boundary for benefit, suggesting a
potential survival advantage of low Vt combined with low Pmax that
warrants confirmation in future larger trials. Notably, pooled data
demonstrated that a ventilation strategy combining low Vt with low
Pmax was associated with a significant reduction in short-term
mortality compared with low Vt with high Pmax. This finding
highlights that limiting both Vt and airway pressure is likely
necessary to achieve a survival benefit in patients without ARDS,
whereas low Vt alone is insufficient. Ventilation strategies that
use a high Vt and a high Pmax may lead to overstretching of
alveoli, local production and release of inflammatory mediators,
recruitment of neutrophils and ventilator-associated lung injury
(1-3).
The findings from the meta-analysis in the present
study suggested that duration of ventilation, incidence of
pulmonary complications and length of hospital stay may be
decreased in patients without ARDS who are ventilated with a low Vt
compared with a high Vt. In a post-hoc analysis of a large,
randomized trial of low Vt ventilation it was found that during
laparoscopic surgeries, low Vt was associated with a markedly
reduced pulmonary complications (43). The effect of a low Vt on duration of
ventilation is consistent with a previous individual patient data
meta-analysis which reported that use of low Vt (≤6 ml/kg of
predicted body weight) vs. high Vt (≥10 ml/kg of predicted body
weight) in patients without ARDS at the onset of mechanical
ventilation was associated with shorter duration of ventilation
(6). By contrast, a previously
published RCT (8) indicated that a
low Vt ventilation strategy was not more effective than an
intermediate Vt strategy for decreasing the number of
ventilator-free days in patients in the ICU without ARDS. The
findings in the present study regarding the effect of a low Vt on
the incidence of pulmonary complications and length of hospital
stay are consistent with two previous studies (7,40) but
contrast with the findings from a third study (8). Consequently, more adequately powered
RCTs are needed to evaluate the effect of a low Vt on duration of
ventilation, incidence of pulmonary complications and length of
hospital stay in patients without ARDS.
Moreover, recent studies support the findings of the
present study. For example, one RCT reported that low Vt alone
provided no clinical benefit in patients without ARDS (44) and two network meta-analyses both
demonstrated that low Vt combined with individualized PEEP reduces
pulmonary complications (45,46),
which is consistent with the conclusion in the present study that a
combination strategy, rather than low Vt alone, is required to
improve outcomes.
However, the present meta-analysis has several
limitations, including substantial heterogeneity among the included
studies; therefore, the results should be interpreted with caution.
Specifically, the included studies comprised both ICU-based (11
studies) and intraoperative (seven studies) settings. This mixture
may have introduced clinical heterogeneity, as the baseline
characteristics, duration of ventilation and severity of illness
differ between these two populations. First, data from RCTs and
observational studies were pooled; however, the observational
studies were of high methodological quality. Second, Pmax varied
between studies, and the Pmax setting required for protective
mechanical ventilation in patients without ARDS has not been
defined. Third, the duration of mechanical ventilation varied
across studies. Fourth, Pmax was defined as either peak or plateau
pressure across the included studies, and these two variables are
physiologically distinct. This heterogeneity in definition may have
influenced the results of the Pmax subgroup analysis, and therefore
the findings should be interpreted with caution.
In summary, the results of the present study
demonstrated that a ventilation strategy combining low Vt with low
Pmax was associated with a significant reduction in short-term
mortality in patients without ARDS compared with a ventilation
strategy combining low Vt with high Pmax. Furthermore, ventilation
with a low Vt was associated with a reduced duration of
ventilation, incidence of pulmonary complications and length of
hospital stay compared with ventilation with a high Vt. Ventilation
with a low Vt alone also did not improve short-term mortality.
Moreover, the present meta-analysis was limited by heterogeneity
between studies.
Supplementary Material
Risk of bias for included randomized
control trials. Red (-) indicates a high risk of bias; yellow (?)
indicates unclear risk, and green (+) indicates a low risk of
bias.
Funnel plot for the effect of low Vt
on short-term mortality in patients without ARDS. Vt, tidal volume;
ARDS, acute respiratory distress syndrome.
Meta-regression analyses exploring
PEEP and ΔP as potential sources of heterogeneity. (A)
Meta-regression analyses of PEEP. (B) Meta-regression analyses of
ΔP. PEEP, positive endexpiratory pressure; ΔP, driving
pressure.
Number of days of ventilation in
patients without ARDS. ARDS, acute respiratory distress
syndrome.
Incidence of pulmonary complications
in patients without ARDS. ARDS, acute respiratory distress
syndrome; M-H, Mantel-Haenszel.
Hospital length of stay in patients
without ARDS. ARDS, acute respiratory distress syndrome. CI,
confidence intervals.
Newcastle-Ottawa quality assessment
scale.
Cross-sectional study quality
assessment.
GRADE evidence profile for the studies
in the meta-analysis.
Acknowledgements
Not applicable.
Funding
Funding: The present work was supported by the National Natural
Science Foundation of China (grant no. 81871602).
Availability of data and materials
The data generated in the present study are included
in the figures and/or tables of this article.
Authors' contributions
FX and FG conceived and designed the study. ZL, FX
and FG developed the methodology. SM assessed the methodological
quality and risk of bias of the included studies. MG performed the
formal analysis. MG, FX and FG provided resources and curated the
data. MG wrote the original draft of the manuscript. All authors
reviewed and edited the manuscript. FG supervised the project and
acquired the funding. MG and FX confirm the authenticity of all the
raw data. All authors read and approved the final manuscript.
Ethics approval and consent to
participate
Not applicable.
Patient consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Costa A, Sakho B, Gomez S, Khanyan B,
Leybengrub P and Bergese S: Ventilator-associated lung injury:
Pathophysiology, prevention, and emerging therapeutic strategies.
Int J Mol Sci. 26(10448)2025.PubMed/NCBI View Article : Google Scholar
|
|
2
|
Acute Respiratory Distress Syndrome
Network. Brower RG, Matthay MA, Morris A, Schoenfeld D, Thompson BT
and Wheeler A: Ventilation with lower tidal volumes as compared
with traditional tidal volumes for acute lung injury and the acute
respiratory distress syndrome. N Engl J Med. 342:1301–1308.
2000.PubMed/NCBI View Article : Google Scholar
|
|
3
|
Merola R, Vargas M and Battaglini D:
Ventilator-induced lung injury: The unseen challenge in acute
respiratory distress syndrome management. J Clin Med.
14(3910)2025.PubMed/NCBI View Article : Google Scholar
|
|
4
|
Gajic O, Frutos-Vivar F, Esteban A,
Hubmayr RD and Anzueto A: Ventilator settings as a risk factor for
acute respiratory distress syndrome in mechanically ventilated
patients. Intensive Care Med. 31:922–926. 2005.PubMed/NCBI View Article : Google Scholar
|
|
5
|
Hager DN, Krishnan JA, Hayden DL and
Brower RG: ARDS Clinical Trials Network. Tidal volume reduction in
patients with acute lung injury when plateau pressures are not
high. Am J Respir Crit Care Med. 172:1241–1245. 2005.PubMed/NCBI View Article : Google Scholar
|
|
6
|
Serpa Neto A, Simonis FD, Barbas CS, Biehl
M, Determann RM, Elmer J, Friedman G, Gajic O, Goldstein JN, Horn
J, et al: Association between tidal volume size, duration of
ventilation, and sedation needs in patients without acute
respiratory distress syndrome: An individual patient data
meta-analysis. Intensive Care Med. 40:950–957. 2014.PubMed/NCBI View Article : Google Scholar
|
|
7
|
Neto AS, Simonis FD, Barbas CS, Biehl M,
Determann RM, Elmer J, Friedman G, Gajic O, Goldstein JN, Linko R,
et al: Lung-protective ventilation with low tidal volumes and the
occurrence of pulmonary complications in patients without acute
respiratory distress syndrome: A systematic review and individual
patient data analysis. Crit Care Med. 43:2155–2163. 2015.PubMed/NCBI View Article : Google Scholar
|
|
8
|
Writing Group for the PReVENT
Investigators. Simonis FD, Serpa Neto A, Binnekade JM, Braber A,
Bruin KCM, Determann RM, Goekoop GJ, Heidt J, Horn J, Innemee G, et
al: Effect of a low vs intermediate tidal volume strategy on
ventilator-free days in intensive care unit patients without ARDS:
A randomized clinical trial. JAMA. 320:1872–1880. 2018.PubMed/NCBI View Article : Google Scholar
|
|
9
|
Schultz MJ, Haitsma JJ, Slutsky AS and
Gajic O: What tidal volumes should be used in patients without
acute lung injury? Anesthesiology. 106:1226–1231. 2007.PubMed/NCBI
|
|
10
|
Serpa Neto A, Filho RR, Cherpanath T,
Determann R, Dongelmans DA, Paulus F, Tuinman PR, Pelosi P, de
Abreu MG and Schultz MJ: PROVE Network Investigators. Associations
between positive end-expiratory pressure and outcome of patients
without ARDS at onset of ventilation: A systematic review and
meta-analysis of randomized controlled trials. Ann Intensive Care.
6(109)2016.PubMed/NCBI View Article : Google Scholar
|
|
11
|
Fuller BM, Page D, Stephens RJ, Roberts
BW, Drewry AM, Ablordeppey E, Mohr NM and Kollef MH: Pulmonary
mechanics and mortality in mechanically ventilated patients without
acute respiratory distress syndrome: A cohort study. Shock.
49:311–316. 2018.PubMed/NCBI View Article : Google Scholar
|
|
12
|
Simonis FD, Barbas CSV, Artigas-Raventós
A, Canet J, Determann RM, Anstey J, Hedenstierna G, Hemmes SNT,
Hermans G, Hiesmayr M, et al: Potentially modifiable respiratory
variables contributing to outcome in ICU patients without ARDS: A
secondary analysis of PRoVENT. Ann Intensive Care.
8(39)2018.PubMed/NCBI View Article : Google Scholar
|
|
13
|
Moher D, Liberati A, Tetzlaff J and Altman
DG: PRISMA Group. Preferred reporting items for systematic reviews
and meta-analyses: The PRISMA statement. Ann Intern Med.
151:264–269, W264. 2009.PubMed/NCBI View Article : Google Scholar
|
|
14
|
Stroup DF, Berlin JA, Morton SC, Olkin I,
Williamson GD, Rennie D, Moher D, Becker BJ, Sipe TA and Thacker
SB: Meta-analysis of observational studies in epidemiology: A
proposal for reporting. Meta-analysis of observational studies in
epidemiology (MOOSE) group. JAMA. 283:2008–2012. 2000.PubMed/NCBI View Article : Google Scholar
|
|
15
|
ARDS Definition Task Force. Ranieri VM,
Rubenfeld GD, Thompson BT, Ferguson ND, Caldwell E, Fan E,
Camporota L and Slutsky AS: Acute respiratory distress syndrome:
The Berlin definition. JAMA. 307:2526–2533. 2012.PubMed/NCBI View Article : Google Scholar
|
|
16
|
Higgins JP, Altman DG, Gøtzsche PC, Jüni
P, Moher D, Oxman AD, Savovic J, Schulz KF, Weeks L and Sterne JA:
Cochrane Bias Methods Group; Cochrane Statistical Methods Group.
The cochrane collaboration's tool for assessing risk of bias in
randomised trials. BMJ. 343(d5928)2011.PubMed/NCBI View Article : Google Scholar
|
|
17
|
Stang A: Critical evaluation of the
Newcastle-Ottawa scale for the assessment of the quality of
nonrandomized studies in meta-analyses. Eur J Epidemiol.
25:603–605. 2010.PubMed/NCBI View Article : Google Scholar
|
|
18
|
Shamliyan TA, Kane RL, Ansari MT, Raman G,
Berkman ND, Grant M, Janes G, Maglione M, Moher D, Nasser M, et al:
Development of quality criteria to evaluate nontherapeutic studies
of incidence, prevalence, or risk factors of chronic diseases:
Pilot study of new checklists [Internet]. Rockville (MD): Agency
for Healthcare Research and Quality (US): Report No.: 11-EHC008-EF,
2011.
|
|
19
|
Egger M, Davey Smith G, Schneider M and
Minder C: Bias in meta-analysis detected by a simple, graphical
test. BMJ. 315:629–634. 1997.PubMed/NCBI View Article : Google Scholar
|
|
20
|
Guyatt GH, Oxman AD, Vist GE, Kunz R,
Falck-Ytter Y, Alonso-Coello P and Schünemann HJ: GRADE Working
Group. GRADE: An emerging consensus on rating quality of evidence
and strength of recommendations. BMJ. 336:924–926. 2008.PubMed/NCBI View Article : Google Scholar
|
|
21
|
Pogue JM and Yusuf S: Cumulating evidence
from randomized trials: Utilizing sequential monitoring boundaries
for cumulative meta-analysis. Control Clin Trials. 18:580–593;
discussion 661-6. 1997.PubMed/NCBI View Article : Google Scholar
|
|
22
|
Determann RM, Royakkers A, Wolthuis EK,
Vlaar AP, Choi G, Paulus F, Hofstra JJ, de Graaff MJ, Korevaar JC
and Schultz MJ: Ventilation with lower tidal volumes as compared
with conventional tidal volumes for patients without acute lung
injury: A preventive randomized controlled trial. Crit Care.
14(R1)2010.PubMed/NCBI View
Article : Google Scholar
|
|
23
|
Fernandez-Bustamante A, Wood CL, Tran ZV
and Moine P: Intraoperative ventilation: Incidence and risk factors
for receiving large tidal volumes during general anesthesia. BMC
Anesthesiol. 11(22)2011.PubMed/NCBI View Article : Google Scholar
|
|
24
|
Futier E, Constantin JM, Paugam-Burtz C,
Pascal J, Eurin M, Neuschwander A, Marret E, Beaussier M, Gutton C,
Lefrant JY, et al: A trial of intraoperative low-tidal-volume
ventilation in abdominal surgery. N Engl J Med. 369:428–437.
2013.PubMed/NCBI View Article : Google Scholar
|
|
25
|
Ge Y, Yuan L, Jiang X, Wang X, Xu R and Ma
W: Effect of lung protection mechanical ventilation on respiratory
function in the elderly undergoing spinal fusion. Zhong Nan Da Xue
Xue Bao Yi Xue Ban. 38:81–85. 2013.PubMed/NCBI View Article : Google Scholar : (In Chinese).
|
|
26
|
Kuzkov VV, Rodionova LN, Ilyina YY,
Ushakov AA, Sokolova MM, Fot EV, Duberman BL and Kirov MY:
Protective ventilation improves gas exchange, reduces incidence of
atelectases, and affects metabolic response in major
pancreatoduodenal surgery. Front Med (Lausanne).
3(66)2016.PubMed/NCBI View Article : Google Scholar
|
|
27
|
Lee PC, Helsmoortel CM, Cohn SM and Fink
MP: Are low tidal volumes safe? Chest. 97:430–434. 1990.PubMed/NCBI View Article : Google Scholar
|
|
28
|
Park SJ, Kim BG, Oh AH, Han SH, Han HS and
Ryu JH: Effects of intraoperative protective lung ventilation on
postoperative pulmonary complications in patients with laparoscopic
surgery: Prospective, randomized and controlled trial. Surg Endosc.
30:4598–4606. 2016.PubMed/NCBI View Article : Google Scholar
|
|
29
|
Pi X, Cui Y, Wang C, Guo L, Sun B, Shi J,
Lin Z, Zhao N, Wang W, Fu S and Li E: Low tidal volume with PEEP
and recruitment expedite the recovery of pulmonary function. Int J
Clin Exp Pathol. 8:14305–14314. 2015.PubMed/NCBI
|
|
30
|
Pinheiro de Oliveira R, Hetzel MP, dos
Anjos Silva M, Dallegrave D and Friedman G: Mechanical ventilation
with high tidal volume induces inflammation in patients without
lung disease. Crit Care. 14(R39)2010.PubMed/NCBI View
Article : Google Scholar
|
|
31
|
Severgnini P, Selmo G, Lanza C, Chiesa A,
Frigerio A, Bacuzzi A, Dionigi G, Novario R, Gregoretti C, de Abreu
MG, et al: Protective mechanical ventilation during general
anesthesia for open abdominal surgery improves postoperative
pulmonary function. Anesthesiology. 118:1307–1321. 2013.PubMed/NCBI View Article : Google Scholar
|
|
32
|
Shen Zi-Jin and Dong R: Value of
protective mechanical ventilation for alleviating symptoms of
general anesthesia patients with high risk of postoperative
pulmonary complications. J Shanghai Jiaotong University.
35:1632–1636. 2015.
|
|
33
|
Soh S, Shim JK, Ha Y, Kim YS, Lee H and
Kwak YL: Ventilation with high or low tidal volume with PEEP does
not influence lung function after spinal surgery in prone position:
A randomized controlled trial. J Neurosurg Anesthesiol. 30:237–245.
2018.PubMed/NCBI View Article : Google Scholar
|
|
34
|
Sundar S, Novack V, Jervis K, Bender SP,
Lerner A, Panzica P, Mahmood F, Malhotra A and Talmor D: Influence
of low tidal volume ventilation on time to extubation in cardiac
surgical patients. Anesthesiology. 114:1102–1110. 2011.PubMed/NCBI View Article : Google Scholar
|
|
35
|
Treschan TA, Kaisers W, Schaefer MS,
Bastin B, Schmalz U, Wania V, Eisenberger CF, Saleh A, Weiss M,
Schmitz A, et al: Ventilation with low tidal volumes during upper
abdominal surgery does not improve postoperative lung function. Br
J Anaesth. 109:263–271. 2012.PubMed/NCBI View Article : Google Scholar
|
|
36
|
Weingarten TN, Whalen FX, Warner DO, Gajic
O, Schears GJ, Snyder MR, Schroeder DR and Sprung J: Comparison of
two ventilatory strategies in elderly patients undergoing major
abdominal surgery. Br J Anaesth. 104:16–22. 2010.PubMed/NCBI View Article : Google Scholar
|
|
37
|
Yilmaz M, Keegan MT, Iscimen R, Afessa B,
Buck CF, Hubmayr RD and Gajic O: Toward the prevention of acute
lung injury: Protocol-guided limitation of large tidal volume
ventilation and inappropriate transfusion. Crit Care Med.
35:1660–1666; quiz 1667. 2007.PubMed/NCBI View Article : Google Scholar
|
|
38
|
Zamani MM, Najafi A, Sehat S, Janforooz Z,
Derakhshan P, Rokhtabnak F, Mesbah Kiaee M, Kholdebarin A,
Ghorbanlo M, Hemadi MH and Ghodraty MR: The effect of
intraoperative lung protective ventilation vs conventional
ventilation, on postoperative pulmonary complications after
cardiopulmonary bypass. J Cardiovasc Thorac Res. 9:221–228.
2017.PubMed/NCBI View Article : Google Scholar
|
|
39
|
Neto AS, Barbas CSV, Simonis FD,
Artigas-Raventós A, Canet J, Determann RM, Anstey J, Hedenstierna
G, Hemmes SNT, Hermans G, et al: Epidemiological characteristics,
practice of ventilation, and clinical outcome in patients at risk
of acute respiratory distress syndrome in intensive care units from
16 countries (PRoVENT): An international, multicentre, prospective
study. Lancet Respir Med. 4:882–893. 2016.PubMed/NCBI View Article : Google Scholar
|
|
40
|
Serpa Neto A, Cardoso SO, Manetta JA,
Pereira VG, Espósito DC, Pasqualucci Mde O, Damasceno MC and
Schultz MJ: Association between use of lung-protective ventilation
with lower tidal volumes and clinical outcomes among patients
without acute respiratory distress syndrome: a meta-analysis. JAMA.
308:1651–1659. 2012.PubMed/NCBI View Article : Google Scholar
|
|
41
|
Amato MB, Meade MO, Slutsky AS, Brochard
L, Costa EL, Schoenfeld DA, Stewart TE, Briel M, Talmor D, Mercat
A, et al: Driving pressure and survival in the acute respiratory
distress syndrome. N Engl J Med. 372:747–755. 2015.PubMed/NCBI View Article : Google Scholar
|
|
42
|
Schmidt MFS, Amaral ACKB, Fan E and
Rubenfeld GD: Driving pressure and hospital mortality in patients
without ARDS: A cohort study. Chest. 153:46–54. 2018.PubMed/NCBI View Article : Google Scholar
|
|
43
|
Karalapillai D, Weinberg L, Neto AS,
Peyton PJ, Ellard L, Hu R, Pearce B, Tan CO, Story D, O'Donnell M,
et al: Low tidal volume ventilation for patients undergoing
laparoscopic surgery: A secondary analysis of a randomised clinical
trial. BMC Anesthesiol. 23(71)2023.PubMed/NCBI View Article : Google Scholar
|
|
44
|
Tadié JM, Ouattara A, Laviolle B,
Lesouhaitier M, Esvan M, Rousseau C, Grégoire M, Gaudriot B,
Nesseler N, Labaste F, et al: Maintaining ventilation with very low
tidal volume and positive-end expiratory pressure versus no
ventilation during cardiopulmonary bypass for cardiac surgery in
adults: A randomized clinical trial. Intensive Care Med.
51:849–860. 2025.PubMed/NCBI View Article : Google Scholar
|
|
45
|
Mo J, Wang D, Xiao J, Chen Q, An R and Liu
HL: Effects of lung protection ventilation strategies on
postoperative pulmonary complications after noncardiac surgery: A
network meta-analysis of randomized controlled trials. BMC
Anesthesiol. 24(346)2024.PubMed/NCBI View Article : Google Scholar
|
|
46
|
Jivraj NK, Lakbar I, Sadeghirad B, Müller
MM, Sohn SY, Peel JK, Jaffer A, Phoophiboon V, Trivedi V, Chaudhuri
D, et al: Intra-operative ventilation strategies and their impact
on clinical outcomes: A systematic review and network meta-analysis
of randomised trials. Anaesthesia. 80:973–987. 2025.PubMed/NCBI View Article : Google Scholar
|