Introduction
Dental implants have become one of the primary
methods for tooth replacement and have gained widespread global
application in recent years (1-3).
Compared with traditional restorative methods, implant-supported
restorations not only markedly improve masticatory function,
speech, and comfort but also enhance aesthetic outcomes, Patients
achieve higher satisfaction in these parameters, including an
overall aesthetic satisfaction rate of 96.67% (4-10).
Furthermore, implant-supported restorations boost patient
self-confidence and life quality (11,12).
As a result, dental implant rehabilitation has become the preferred
method for tooth replacement in modern dentistry. The survival rate
(SR) of dental implants is associated with osseointegration;
successful osseointegration is influenced by multiple factors,
including implant design, surgical technique, systemic metabolic
status and immune function (13).
Diabetic patients, due to metabolic dysregulation, may experience
secondary vascular and bone tissue complications, which interfere
with osseointegration and long-term implant stability, increasing
the risk of peri-implantitis (14).
Additionally, microvascular complications in diabetic patients may
decrease the release of repair cells and growth factors, impair
collagen synthesis and hinder soft tissue regeneration (1). Consequently, diabetic patients are
typically considered unsuitable for implant rehabilitation
(4,15).
Diabetes mellitus (DM) has seen a notable increase
in prevalence over the past decades, with the number of affected
individuals worldwide exceeding 800 million (16). Diabetic patients typically exhibit
poorer oral health, with a markedly higher prevalence of edentulism
compared with non-diabetic populations. Adults with diabetes
exhibit approximately twice the tooth loss rate as those without
diabetes (17). This disparity is
primarily attributed to their increased susceptibility to oral
disease, such as periodontitis and dental caries, and experience
accelerated alveolar bone resorption following tooth loss (14,18,19).
As a result, implant-supported restorations have become a key
option for diabetic patients to restore masticatory function and
improve life quality. Well-controlled diabetic patients do not
experience a significant decrease in implant SR following implant
placement (20,21) For example, Diehl et al
(22) observed that implant SR
reached 100% in both diabetic and normoglycemic groups, with no
significant differences in probing depth (PD), marginal bone loss
(MBL), and bleeding on probing (BOP). Similarly, Tulbah et
al (23) conducted a 5-year
follow-up study and observed that, despite a higher incidence of
complications in diabetic patients, implant SR did not markedly
decline, further supporting the hypothesis that diabetic patients
can achieve long-term implant success. These findings have led to
the increasing application of implant-supported restoration in the
dental treatment of diabetic patients (24,25).
Research on implant rehabilitation in diabetic
patients has primarily focused on delayed implant placement
strategies. Most studies indicate that, with well-controlled blood
glucose levels, the implant SR in diabetic patients is comparable
with those in non-diabetic patients (26,27).
However, rapid alveolar bone resorption following tooth extraction
may lead to insufficient bone volume, necessitating bone
augmentation procedures, which not only increase surgical risk but
also impose additional financial burdens on patients (8,28-30).
Moreover, the extended treatment duration may compromise
masticatory efficiency, negatively impacting patient quality of
life. Compared with delayed implantation, immediate implant
placement (IIP) simplifies the repair process by placing implants
during tooth extraction, reducing the number of surgeries and
overall waiting time for the final prosthesis. In addition, this
method helps to maintain the size of the alveolar ridge, thereby
supporting the overlying soft tissue (31-34).
To date, there is limited research on IIP in diabetic patients, and
existing meta-analyses exhibit limitations (35). For example, Andrade et al
(35) found no significant
differences in implant SR between diabetic and healthy individuals.
However, the aforementioned meta-analysis included seven studies,
with only five being utilized for quantitative synthesis. In the
analysis of MBL, the comparison was limited to immediate vs.
conventional loading in diabetic patients, without a thorough
exploration of differences compared with healthy patients.
Additionally, key soft tissue indicators such as probing depth (PD)
and BOP were not analyzed. In conclusion, the limitations of
existing meta-analyses include a small number of included studies,
incomplete observation indicators and a lack of comprehensive
evaluation of both hard and soft tissue health. It was hypothesized
that IIP could be applied in diabetes patients. The present study
aimed to determine whether IIP could be adopted in diabetic
patients by assessing its feasibility and safety in diabetic
patients.
Materials and methods
Data retrieval and collection
According to the Population/Patient, Intervention;
C: Comparison; O: Outcome principle, PubMed (https://pubmed.ncbi.nlm.nih.gov), Embase (embase.com), Web of science (https://www.webofscience.com), Cochrane (https://www.cochranelibrary.com), Google
(scholar.google.com) and China National
Knowledge Infrastructure (CNKI) (https://www.cnki.net) databases were searched from
January 2000 to March 2025. Key words were as follows: ‘Diabetic
patients’ or ‘DM’ or ‘type 2 diabetes’ or ‘glycemic control’ or
‘hyperglycemia’ and ‘IIP’ or ‘immediate dental implant’ or
‘immediate implant restoration’ or ‘immediate loading’ and ‘healthy
patients’ or ‘non-diabetic patients’ or ‘systemically healthy’ and
‘implant survival rate’ or ‘implant success rate’ or ‘implant
failure’ or ‘MBL’ or ‘bone resorption’ or ‘peri-implant bone level’
or ‘PD’ or ‘peri-implant probing depth’ or ‘BOP’ or ‘peri-implant
bleeding’ or ‘safety’ or ‘complications’ or ‘adverse events’.
Inclusion criteria were as follows: i) Studies
involving diabetic (including those with well- and poorly
controlled diabetes) and healthy patients who underwent IIP for
single or multiple teeth (age, ≥18 years); ii) intervention measure
is IIP, with healthy patients serving as the control group
receiving the same intervention; iii) studies that reported key
outcome measures such as implant SR, MBL, PD, BOP or complications,
with a follow-up period ≥6 months.
Exclusion criteria were as follows: i) Case reports,
reviews and meta-analyses; ii) animal-related research; iii)
studies with a sample size <10; and iv) studies with incomplete
data.
Data extraction
A total of two independent researchers
systematically performed the literature screening and data
extraction according to the inclusion/exclusion criteria. Titles
and abstracts were screened, followed by full-text assessment of
eligible studies. Discrepancies between the two researchers were
resolved through discussion, and if consensus could not be reached,
a third senior researcher was consulted. Extracted data included
first author, year of publication, study design, number of patients
and implants, follow-up time and outcome measures such as MBL, PD,
BOP and SR. The follow-up durations were categorized into three
subgroups according to the time points available in the included
studies: ≤6 months, 12 and ≥24 months, representing short-term,
mid-term, and long-term follow-up, respectively.
Quality evaluation of included
literature
Newcastle-Ottawa Scale (NOS) was adopted to evaluate
the quality of literature (36).
Statistical analysis
Meta-analysis was conducted using RevMan 5.4
software (cochranelibrary.com/). For continuous
variables (MBL, PD and BOP), the mean difference (MD) and 95%
confidence interval (CI) were calculated. For dichotomous variables
(implant SR), the risk ratio (RR) and 95% CI were determined.
Heterogeneity between studies was assessed using the Cochrane Q
test and the I² statistic, with I²≥50% indicating substantial
heterogeneity, in which case a random-effects model was applied.
Subgroup analyses were performed based on glycemic control levels
in diabetic patients and follow-up duration. Sensitivity analysis
was performed using the leave-one-out method. Publication bias was
assessed using a funnel plot. P<0.05 was considered to indicate
a statistically significant difference.
Results
Study characteristics
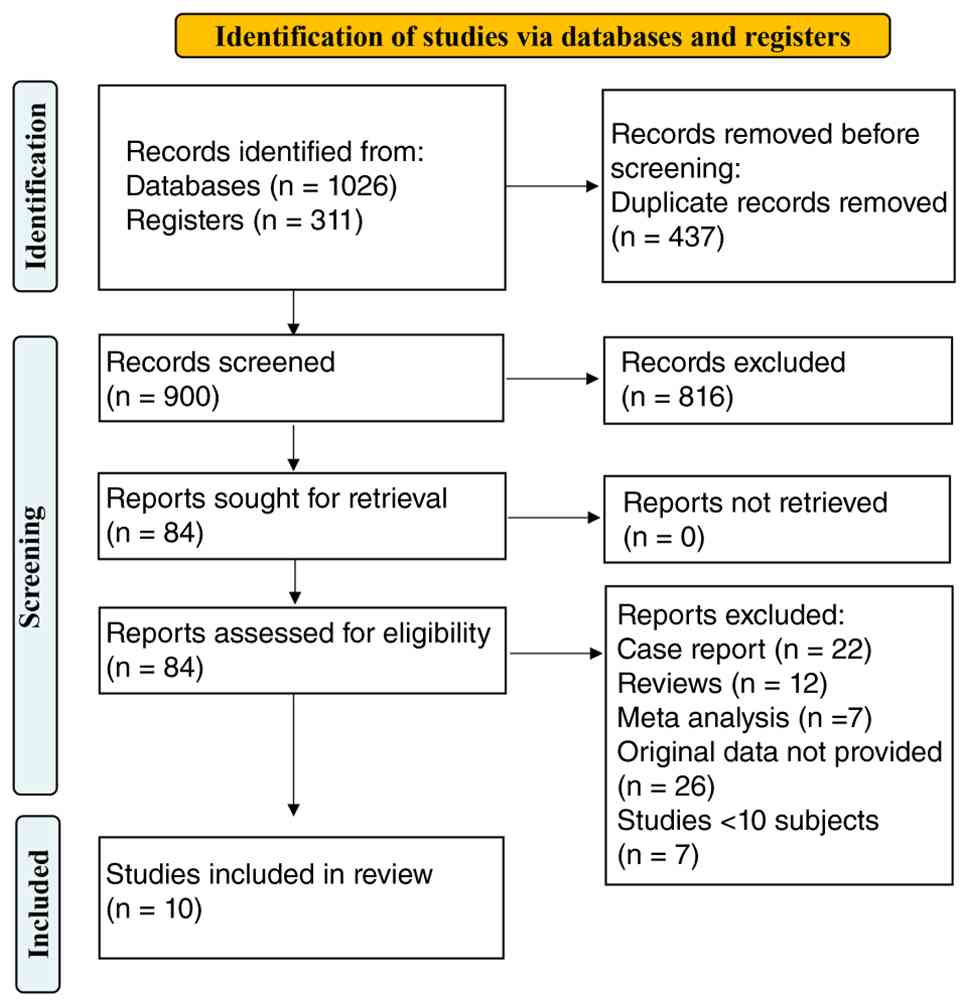
A total of 1,337 relevant studies were initially
retrieved. After removing 437 duplicate records, 900 studies
remained. Title and abstract screening excluded 816 studies. The
full text of the remaining 84 studies was further reviewed, leading
to the exclusion of 74 studies. A total of 10 studies meeting the
eligibility criteria were included (Fig. 1) (37-46).
Among the 10 included studies, most had a follow-up period ranging
from 6 to 24 months (37,39-41,43,45,46),
while some extended to 10 and 15 years (38,44).
The sample sizes varied from 23 patients (168 implants) to 655
patients (922 implants). Implant placement approaches included
single-tooth restoration, full-arch rehabilitation and the
all-on-four concept, though some studies did not specify detailed
implant strategies (40,44). The methodological quality was
assessed using the NOS. The median Ottawa score was 7 (range, 6-9),
indicating that the overall quality of the included studies was
high (Table I).
 | Table IBasic information and relevant
efficacy indicators of included studies. |
Table I
Basic information and relevant
efficacy indicators of included studies.
| | | Patients/total
implants | | Marginal bone loss,
mm | Probing depth,
mm | Bleeding on
probing, % | Survival rate | |
|---|
| First author,
year | Study design | Poorly controlled
DM | Well-controlled
DM | Healthy | Follow-up time,
months | Poorly controlled
DM | Well-controlled
DM | Healthy | Poorly controlled
DM | Well-controlled
DM | Healthy | Poorly controlled
DM | Well-controlled
DM | Healthy | Poorly controlled
DM | Well-controlled
DM | Healthy | NOS score |
|---|
| Agliardi et
al, 2023(38) | RCS | NR | 19/76 | 154/616 | 180 | NR | NR | NR | NR | NR | NR | NR | NR | NR | NR | 71/76 | 602/616 | 6 |
| Aguilar-Salvatierra
et al, 2016(39) | PCS | 22/22 | 30/30 | 33/33 | 6 | 1.33±0.29 | 0.71±0.31 | 0.51±0.19 | 3.43±0.23 | 2.54±0.32 | 2.43±0.25 | 0.59±0.07 | 0.41±0.04 | 0.36±0.06 | 19/22 | 28/29 | 33/33 | 8 |
| | | | | | 12 | 1.54±0.43 | 0.86±0.25 | 0.64±0.23 | 3.57±0.37 | 2.66±0.27 | 2.60±0.18 | 0.65±0.06 | 0.45±0.07 | 0.39±0.04 | NR | NR | NR | |
| | | | | | 24 | 1.92±0.38 | 0.98±0.27 | 0.72±0.27 | 3.68±0.48 | 2.79±0.24 | 2.67±0.14 | 0.74±0.05 | 0.51±0.05 | 0.44±0.07 | NR | NR | NR | |
| Al Amri et
al, 2016(40) | PCS | 31/31 | 30/30 | 30/30 | 6 | 0.55±0.06 | 0.52±0.02 | 0.33±0.11 | 3.30±0.21 | 2.50±0.18 | 2.00±0.50 | 0.71±0.05 | 0.63±0.06 | 0.42±0.05 | 31/31 | 30/30 | 30/30 | 8 |
| | | | | | 12 | 0.57±0.07 | 0.54±0.12 | 0.45±0.06 | 2.40±0.35 | 2.30±0.26 | 1.90±0.04 | 0.63±0.02 | 0.60±0.04 | 0.40±0.02 | NR | NR | NR | |
| | | | | | 24 | 0.59±0.20 | 0.58±0.15 | 0.46±0.16 | 2.30±0.62 | 2.30±0.15 | 1.60±0.05 | 0.62±0.05 | 0.62±0.07 | 0.40±0.06 | NR | NR | NR | |
| Alves et al,
2010(41) | PCS | NR | 4/28 | 19/140 | 36 | NR | NR | NR | NR | NR | NR | NR | NR | NR | NR | 28/28 | 138/140 | 6 |
| Bell et al,
2011(42) | RCS | NR | 23/83 | 632/839 | 3-93 | NR | NR | NR | NR | NR | NR | NR | NR | NR | NR | 83/83 | 824/839 | 6 |
| D'Orto et
al, 2022(43) | RCS | NR | 22/114 | 25/122 | 6 | NR | 0.63±0.54 | 0.57±0.52 | NR | NR | NR | 0.62±0.06 | 0.52±0.06 | 0.43±0.05 | NR | 108/114 | 118/122 | 8 |
| | | | | | 12 | NR | 0.94±0.75 | 0.99±0.82 | NR | NR | NR | 0.63±0.07 | 0.54±0.06 | 0.47±0.05 | NR | NR | NR | |
| | | | | | 24 | NR | 0.82±0.64 | 0.84±0.73 | NR | NR | NR | 0.72±0.06 | 0.56±0.07 | 0.45±0.06 | NR | NR | NR | |
| | | | | | 36 | NR | 0.90±0.76 | 0.86±0.79 | NR | NR | NR | NR | NR | NR | NR | NR | NR | |
| Gómez-Moreno et
al, 2015(37) | PCS | 22/22 | 24/24 | 21/21 | 12 | 0.54±0.12 | 0.45±0.15 | 0.41±0.18 | 2.23±0.28 | 2.24±0.20 | 2.19±0.22 | NR | NR | NR | NR | NR | NR | 8 |
| | | | | | 24 | 0.63±0.16 | 0.52±0.18 | 0.48±0.15 | 2.37±0.26 | 2.27±0.23 | 2.21±0.20 | NR | NR | NR | NR | NR | NR | |
| | | | | | 36 | 0.70±0.19 | 0.57±0.16 | 0.53±0.17 | 2.40±0.25 | 2.30±0.23 | 2.26±0.19 | NR | NR | NR | NR | NR | NR | |
| Han et al,
2021(45) | RCS | 15/15 | 15/15 | 30/30 | 3 | NR | NR | NR | 2.55±0.51 | 1.65±0.46 | 1.71±0.27 | NR | NR | NR | NR | NR | NR | 7 |
| | | | | | 6 | NR | NR | NR | 2.33±0.51 | 1.72±0.44 | 1.76±0.20 | NR | NR | NR | NR | NR | NR | |
| Tawil et al,
2008(44) | PCS | 1/11 | 10/47 | 12/59 | 12-144 | NR | NR | NR | NR | NR | NR | NR | NR | NR | 11/11 | 47/47 | 58/59 | 7 |
| Zhao et al,
2022(46) | RCS | NR | 21/24 | 135/161 | 6 | NR | 0.68±0.38 | 0.77±0.31 | NR | NR | NR | NR | NR | NR | NR | NR | NR | 8 |
| | | | | | 12 | NR | 0.97±0.39 | 1.09±0.49 | NR | NR | NR | NR | NR | NR | NR | NR | NR | |
| | | | | | 24 | NR | 1.10±0.39 | 1.23±0.54 | NR | NR | NR | NR | NR | NR | NR | NR | NR | |
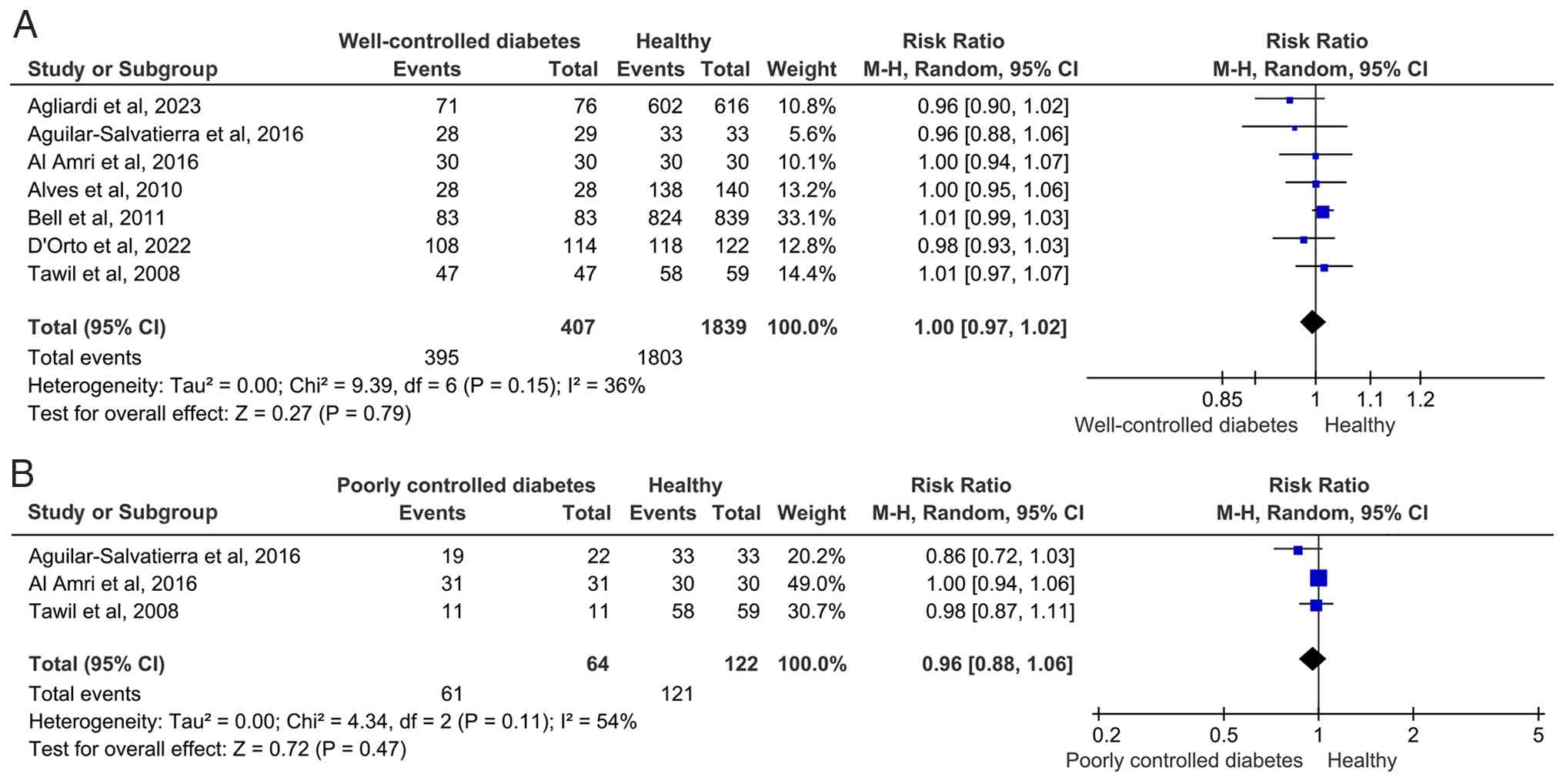
Implant SR between diabetic and
healthy patients
No significant difference was observed in implant SR
between well-controlled diabetic patients and healthy individuals
(RR=1.00, 95% CI: 0.97-1.02), with moderate heterogeneity among
studies (I²=36%). Similarly, no significant decrease in implant SR
was observed in poorly controlled diabetic patients (RR=0.96, 95%
CI: 0.88-1.06), although heterogeneity was relatively high (I²=54%;
Fig. 2). In well-controlled
diabetic patients, individual studies consistently showed implant
SR comparable with those of healthy individuals (RR: 0.96-1.01)
(38-44),
with no significant differences. In poorly controlled diabetic
patients, individual studies reported similar implant SR to healthy
individuals (RR range: 0.86-1.00) (39,40,44),
with no significant differences. Although the overall implant SR
did not differ markedly between diabetic patients and healthy
individuals, the pooled effect size for poorly controlled diabetic
patients was lower than that for healthy individuals (RR=0.96),
suggesting that glycemic control impacts implant SR.
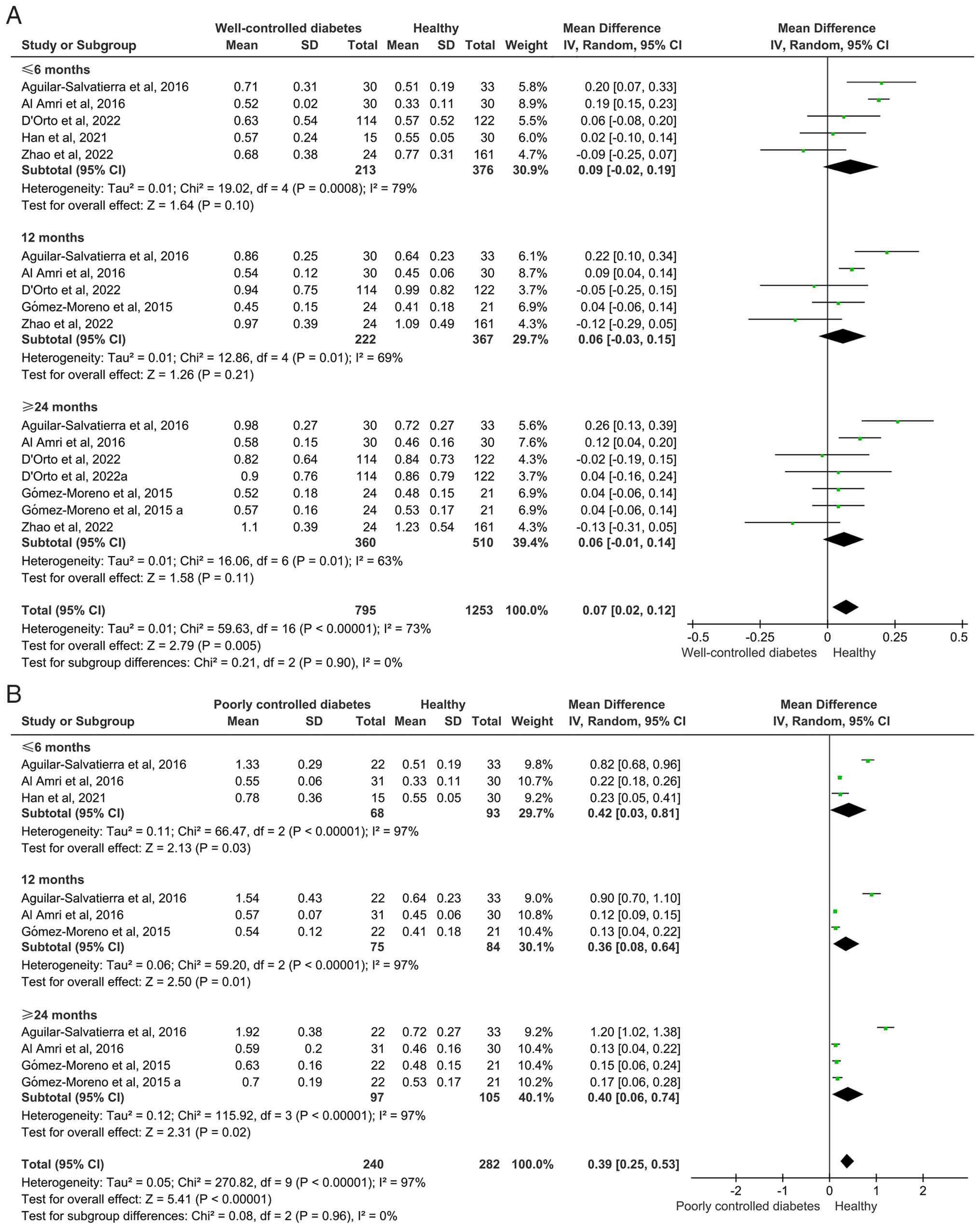
Diabetic patients undergoing IIP have
higher MBL
Well-controlled diabetic patients exhibited higher
MBL than healthy individuals (MD=0.07, 95% CI: 0.02-0.12). Poorly
controlled diabetic patients showed a more pronounced increase in
MBL (MD=0.39, 95% CI: 0.25-0.53). Subgroup analysis indicated that
in poorly controlled diabetic patients, MBL was significantly
higher at all time points (≤6, 12 and ≥24 months; Fig. 3). Although well-controlled diabetic
patients exhibited higher MBL than healthy individuals, this was
not significant in any individual follow-up subgroup but achieved
statistical significance in the pooled overall analysis, likely
because of the increased statistical power from combining the
subgroups. Among well-controlled diabetic patients,
Aguilar-Salvatierra (39) and Al
Amri (40) reported markedly higher
MBL compared with healthy individuals, whereas other studies found
no significant difference (37,43,45,46).
In poorly controlled diabetic patients, all studies consistently
showed markedly greater MBL than in healthy individuals. High
heterogeneity was observed in MBL analyses (I²=73-97%). Despite the
notable heterogeneity, the results from the random-effects model
consistently supported the conclusion that diabetic patients,
especially those with inadequate glycemic control, experience
markedly greater MBL following IIP.
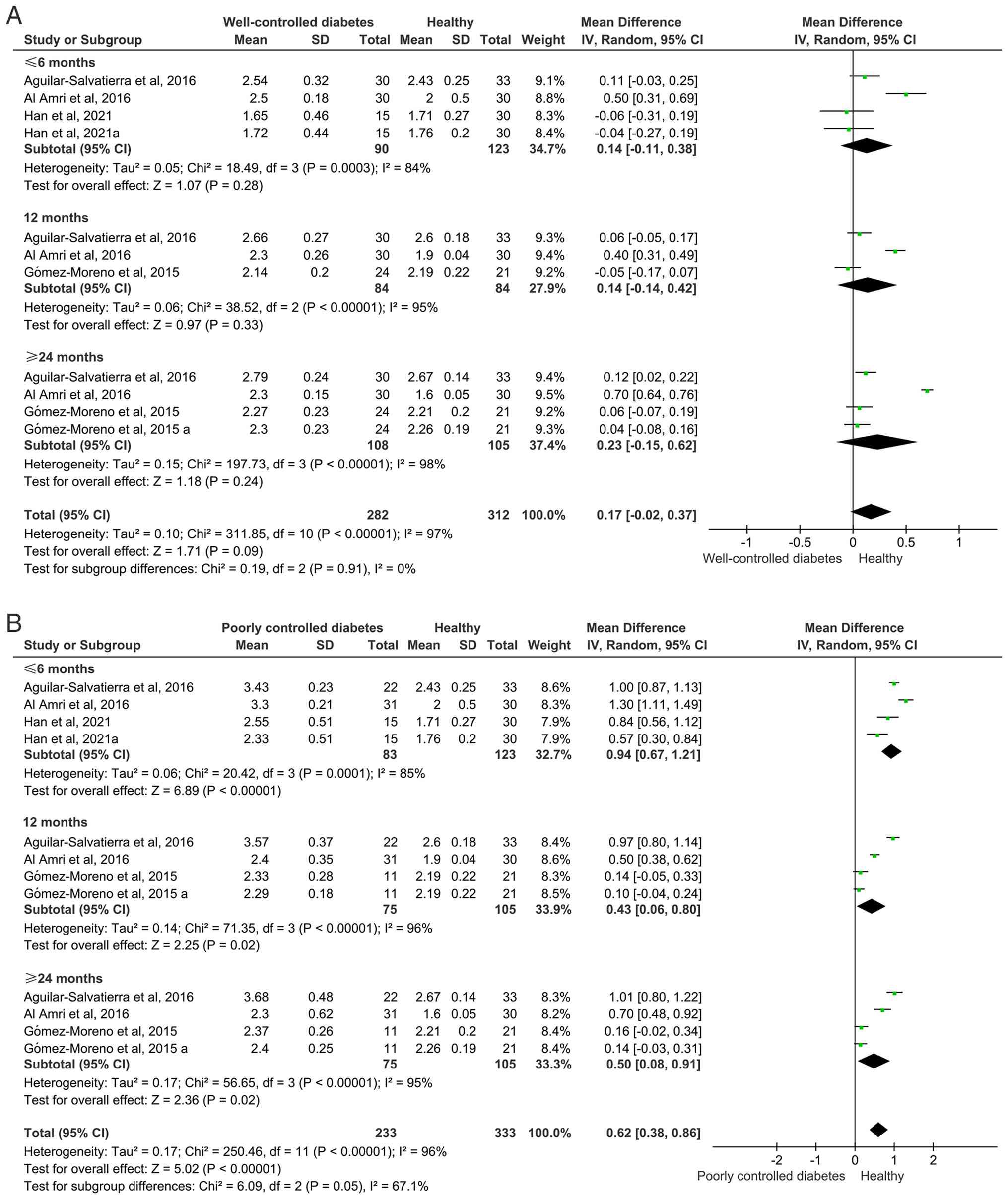
Diabetic patients undergoing IIP
experience greater PD
No significant difference was observed in PD between
well-controlled diabetic patients and healthy individuals (MD=0.17,
95% CI: -0.02-0.37). However, poorly controlled diabetic patients
exhibited significantly greater PD than healthy individuals
(MD=0.62, 95% CI: 0.38-0.86). Subgroup analysis revealed that in
poorly controlled diabetic patients, PD was significantly higher at
all time points (≤6, 12 and ≥24 months; Fig. 4). In well-controlled diabetic
patients, although PD was slightly higher than in healthy
individuals, the difference was significant only in a few
individual studies (39,40). Among well-controlled diabetic
patients, Al Amri (40) reported
markedly higher PD than in healthy individuals, while other studies
found no significant difference (37,45).
In poorly controlled diabetic patients, both Aguilar-Salvatierra
(39) and Al Amri (40) reported markedly greater PD compared
with healthy individuals. High heterogeneity was observed in PD
analyses (I²=96-97%). Despite the notable heterogeneity, the
results from the random-effects model consistently supported the
conclusion that poorly controlled diabetic patients experienced
markedly greater PD following IIP.
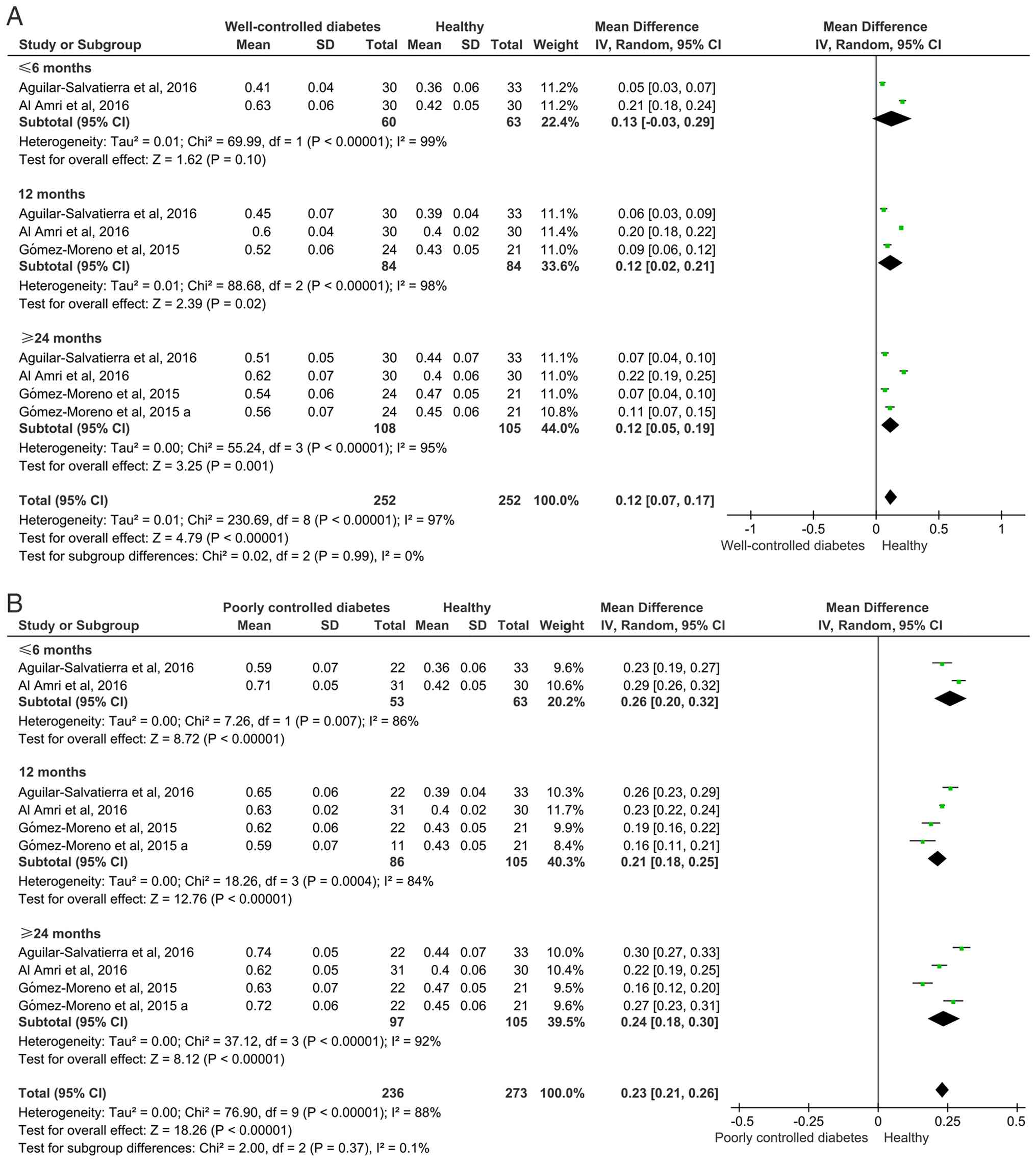
Diabetic patients undergoing IIP
experience higher BOP
Well-controlled diabetic patients exhibited
significantly higher BOP than healthy individuals (MD=0.12, 95% CI:
0.07-0.17); poorly controlled diabetic patients also exhibited a
significant increase in BOP compared with healthy individuals
(MD=0.23, 95% CI: 0.21-0.26). Subgroup analysis revealed that in
poorly controlled diabetic patients, BOP was markedly higher at all
time points (≤6, 12 and ≥24 months; Fig. 5). In well-controlled diabetic
patients, while BOP was also higher than in healthy individuals,
the difference was significant only at 12 and ≥24 months. A high
degree of heterogeneity was observed in the BOP forest plot
(I²=88-97%). Despite the notable heterogeneity, the results from
the random-effects model consistently supported the conclusion that
diabetic patients, particularly those with inadequate glycemic
management, experience markedly higher BOP following IIP.
Safety
A total of two studies (42,43)
compared the incidence of complications following immediate implant
placement, primarily focusing on edema, bleeding and wound
infection. The results indicated no significant increase in
complication rates compared with healthy patients (data not
shown).
Sensitivity analysis
To evaluate the robustness of the meta-analysis
results, sensitivity analysis was performed using the leave-one-out
method. The pooled effect size and 95% CI remained stable across
all iterations, indicating that the findings were not notably
influenced by any single study (data not shown). For example, in
the analysis of implant SR, the exclusion of Agliardi et al
(38) yielded a RR of 1.01 (95% CI:
0.90-1.02) for well-controlled diabetic patients. Similarly, the
exclusion of Aguilar-Salvatierra (39) resulted in an RR of 1 (95% CI:
0.97-1.02). These results were consistent with the overall pooled
effect size (RR=1, 95% CI: 0.97-1.02). The stability of the effect
estimates across all sensitivity analyses underscored the
robustness of the meta-analysis findings and suggests that the
results are not driven by any individual study.
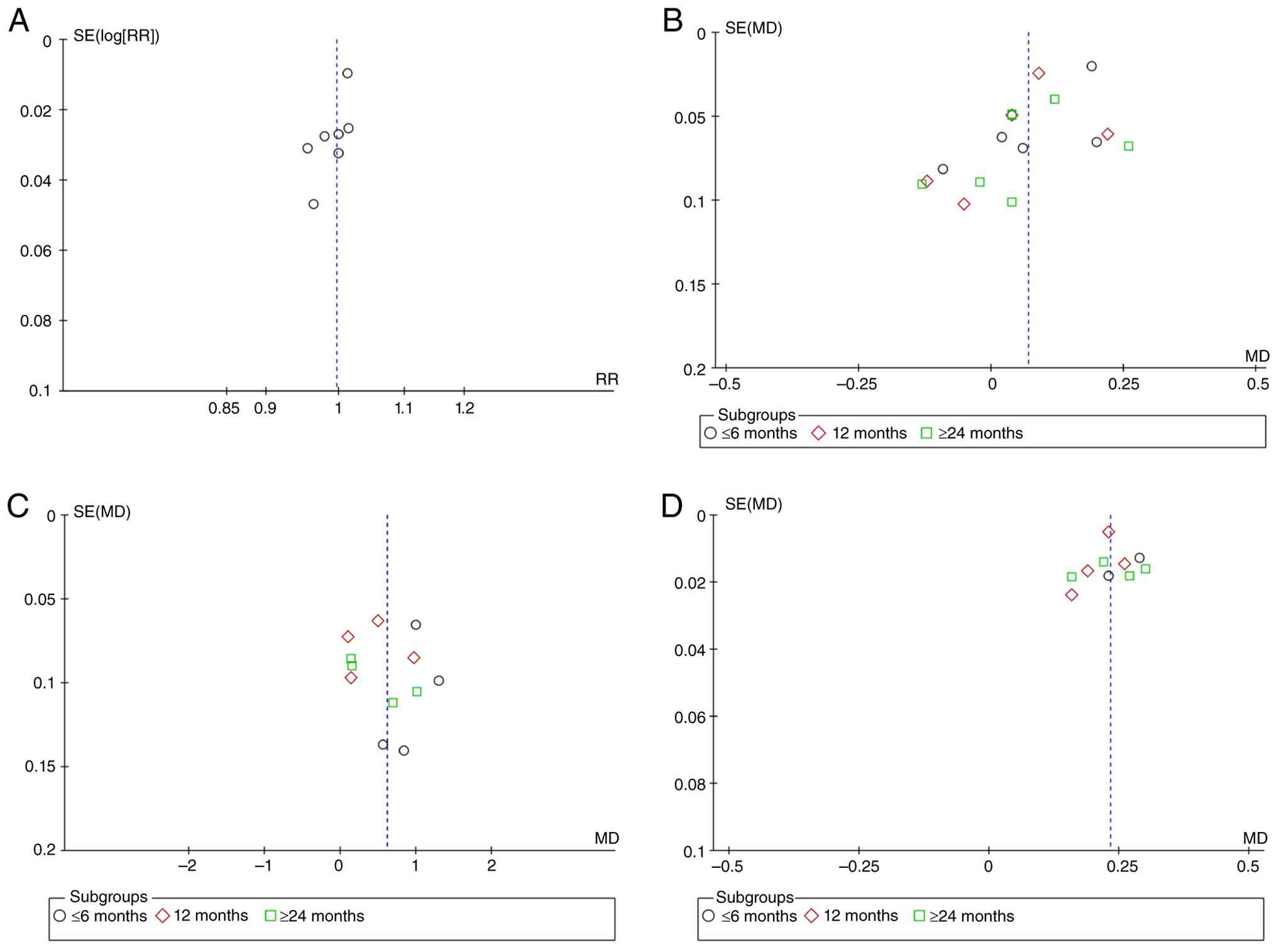
Publication bias
To assess the potential publication bias, funnel
plot analysis was performed for the outcomes of SR, MBL, PD and
BOP. Visual inspection of the funnel plots for SR, MBL, PD and BOP
revealed a symmetrical distribution (Fig. 6), indicating no apparent publication
bias. This suggested that the results of the meta-analysis are not
markedly influenced by publication bias and have high
reliability.
Discussion
IIP offers the advantages of decreasing treatment
duration, minimizing the number of surgical procedures and
maintaining the contour of the alveolar ridge. This is beneficial
in the maxillary anterior region, where good soft tissue profiles
and aesthetic outcomes can be achieved (31,32).
However, IIP demands high initial stability; patients with acute
infection, severe bone defect or high occlusal loads may face
increased risk of early failure (33,34).
By contrast, delayed implantation is typically performed 3-6 months
after tooth extraction, allowing healing of the extraction socket
and sufficient bone regeneration before implant placement. This
approach improves the success rate of osseointegration and
long-term stability. However, delayed implantation results in a
longer treatment timeline, requiring patients to wear temporary
dentures, which may affect chewing efficiency and life quality and
increase psychological burden (47-50).
For diabetic patients, particularly those with well-controlled
diabetes, the question of whether IIP can be performed is a key
issue in clinical practice. The present meta-analysis demonstrated
no obvious difference was in implant SR between diabetic patients
and healthy individuals who undergo IIP. However, obvious
differences were observed between in terms of MBL, PD and BOP
Diabetic patients, particularly those with inadequate glycemic
management, exhibited worse outcomes.
The primary evaluation criterion for survival in the
present study was implant retention. The present findings indicated
that, when glycemic control was good, implant SR did not differ
markedly between diabetic patients and healthy individuals.
Although hyperglycemia can affect the blood supply to the implant
area, impair soft and bone tissue healing and increase the risk of
peri-implantitis, maintaining strict blood sugar control and
enhancing oral hygiene guidance improve long-term implant success
(40,51-53).
However, the present results also showed that diabetic patients
with poor glycemic control did not experience a markedly lower SR
compared with healthy individuals, which is inconsistent with
current research. Ayele et al (54) provided further evidence on the
impact of diabetes on implant survival, indicating that
uncontrolled type 2 DM leads to increased peri-implant bone loss
and decreased implant SR. The discrepancy in the present study may
be attributed to the fact that Tawil et al (44) only enrolled one patient with poorly
controlled blood sugar, who received 11 implants, all of which
remained intact. Al Amri et al (40) reported that all patients had a 100%
implant SR during the follow-up period, resulting in consistent
data. Aguilar-Salvatierra et al (39) reported that diabetic patients with
high hemoglobin A1c (HbA1C) levels initially showed good glycemic
control, with HbA1C levels markedly decreasing after 24 months
follow-up. Therefore, satisfactory blood sugar control in diabetic
patients following IIP is a key factor influencing implant SR.
Diabetes may induce secondary vascular and osseous
complications, which interfere with the osseointegration of
implants. This affects the success rate of implants and the healing
of peri-implant bone tissue. Therefore, the present meta-analysis
investigated MBL in diabetic patients and healthy individuals to
evaluate bone tissue healing. MBL is an effective indicator of
peri-implant bone integration and bone healing and one of the key
metrics for assessing long-term implant success (55,56).
Diabetic patients exhibited slightly higher MBL compared with
healthy individuals. This may be attributed to abnormal bone
metabolism and heightened inflammatory responses induced by the
hyperglycemic states in diabetic patients. Alsahhaf et al
(57) observed that, compared with
well-controlled diabetic patients and healthy individuals, poorly
controlled diabetic patients experience markedly greater bone loss
around the implants. The hyperglycemic environment promotes
oxidative stress and the accumulation of advanced glycation
end-products, which inhibit osteoblast activity and stimulate
osteoclast formation, leading to increased bone resorption
(8). Moreover, diabetic patients
typically have microvascular complications, which may impair blood
supply and healing capacity of peri-implant bone tissue (39). However, in the present study, the
actual bone loss in well-controlled diabetic patients was
relatively small (0.07 mm); in clinical practice, bone loss of 0.07
mm is almost negligible (55). The
actual bone loss in patients with poorly controlled diabetes was
0.39 mm, which remains within an acceptable range (bone loss
<0.2 mm/year is considered normal) (56). Therefore, such levels of bone loss
are unlikely to have a notable impact on the long-term survival of
implants. As previously noted, the similarity in implant SR between
diabetic patients and healthy individuals further indicated that
bone damage in diabetic patients does not affect implant survival.
Therefore, diabetic patients can undergo IIP.
BOP and PD are key clinical indicators for assessing
the health of peri-implant soft tissue. The present study found no
significant difference in PD between well-controlled diabetic
patients and healthy individuals, while BOP was markedly higher in
diabetic patients. PD and BOP were markedly increased in patients
with poor blood glucose control, suggesting more pronounced
inflammation around the peri-implant tissue in diabetic
individuals. For example, Gómez-Moreno et al (37) showed that poorly controlled diabetic
patients (HbA1c ≥10.0%) have a significant increase in BOP during a
3-year follow-up after implant placement. Additionally, Lv et
al (58) found that as HbA1c
levels increased, the levels of bone metabolism negative regulators
such as IL-6, TNF-α and RANKL also markedly increased, accompanied
by a notable increase in PD around the implant. Hyperglycemia may
decrease the resistance of periodontal tissues to bacterial
infections, leading to microvascular changes in the gums and
increased release of inflammatory mediators, thus exacerbating the
inflammatory response in peri-implant tissues (59,60).
Furthermore, impaired immune function in diabetic patients
intensifies the inflammation around the implant (61). In the present study, PD for poorly
controlled diabetic patients was 0.62 mm higher than in healthy
patients. In clinical practice, a 0.62 mm increase in PD typically
indicates mild inflammation, which usually does not have a notable
impact on implant stability or success rates (62). While the differences in BOP were
significant, the actual values were relatively small (0.12 and
0.23). It is typically considered that BOP <10% is indicative of
healthy peri-implant tissue (63).
Therefore, although diabetes increased the risk of inflammation in
peri-implant soft tissues, effective glycemic control prevented
severe inflammatory infections.
The included studies exhibited significant
heterogeneity. Numerous factors may contribute to this variability.
Firstly, the cohort studies may have been influenced by
confounders, such as differences in implant types. Certain studies
utilized Straumann Bone Level implants (Straumann AG), Brånemark
System® MKIV (Nobel Biocare AB), or NobelSpeedy Groovy® (Nobel
Biocare AB, Göteborg, Sweden) (37-40,44),
which may impact the outcomes. Additionally, patients had varying
HbA1c levels, and in certain cases, HbA1c levels decreased during
follow-up (38). The follow-up
duration also differed: Certain studies had follow-up periods <6
months (45), while others had
follow-up durations of 24 or 36 months (37,43).
The type of implants also varied, including single teeth, full-arch
and all-on-four approaches. Furthermore, there were differences in
the imaging methods used to measure MBL, such as intra-oral x-rays
(38,39,43)
and panoramic radiograph (41) or
cone beam CT (46), which may lead
to discrepancies in precision and consistency. Despite these
differences, the main results remained consistent in subgroup and
sensitivity analyses, indicating the robustness of the findings.
Moreover, the use of a random-effects model mitigated the impact of
heterogeneity on the results. Nevertheless, the presence of
heterogeneity suggests that caution should be exercised when
interpreting the findings, especially when extrapolating to a
broader population. Future research should investigate the sources
of heterogeneity and decrease its impact through standardized study
designs and measurement techniques.
The present meta-analysis has several limitations.
Firstly, certain studies included had small sample sizes,
particularly the group of patients with poorly controlled diabetes
(44,45). Small sample sizes may lead to
insufficient statistical power, potentially failing to detect
underlying differences and affecting the stability of the results.
Secondly, due to the limited number of studies available for funnel
plot analysis in some outcome measures, statistical tests such as
Egger's test were not performed, as they would have low power and
potentially yield misleading results (64). Therefore, publication bias was
assessed qualitatively based on visual inspection of funnel plot
symmetry. Future studies with larger sample sizes are needed to
validate the robustness of our findings. Thirdly, while the studies
categorized diabetic patients into well- and poorly controlled
groups, there was a lack of detailed analysis of HbA1c levels. The
precise level of blood glucose control may have a notable impact on
implant success rates and the health of surrounding tissue, but the
included studies did not fully explore this aspect. Furthermore,
although the present study examined indicators such as MBL, PD and
BOP, it lacked a detailed assessment of peri-implantitis, which is
one of the primary causes of implant failure (53). Future research should investigate
the incidence and risk factors of peri-implantitis in diabetic
patients. Finally, the type of implants and surgical techniques
varied, which could affect the comparability of the results. Future
studies should aim to standardize implant types and surgical
techniques to decrease the influence of confounding factors.
The present meta-analysis indicated that diabetic
patients with good blood glucose control showed no significant
difference in implant SR compared with healthy individuals,
suggesting that IIP is feasible in diabetic patients. However,
diabetic patients, especially those with poor blood glucose
control, exhibit significant differences in MBL, PD and BOP,
indicating that they may face a higher risk of peri-implant
inflammation and tissue destruction following implant placement.
Clinicians should pay particular attention to preoperative blood
glucose control and postoperative peri-implant maintenance in
diabetic patients. Regular monitoring of MBL, PD and BOP around the
implant, along with personalized oral hygiene instructions and
periodontal maintenance plans, may decrease the risk of
peri-implantitis and improve the long-term SR of implants.
Acknowledgements
Not applicable.
Funding
Funding: The present study was supported by the 2024 Research
Innovation and Translation Fund of Peking University Binhai
Hospital (grant no. 2024-CX-05.
Availability of data and materials
The data generated in the present study may be
requested from the corresponding author.
Authors' contributions
ZL, HY and XZ conceived the study. HL and XZ
analyzed the data. ZL and HY confirm the authenticity of all the
raw data. ZL and HY wrote the manuscript. All authors have read and
approved the final manuscript.
Ethics approval and consent to
participate
Not applicable.
Patient consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Anolik RA, Nelson JA, Rosen EB, Disa J,
Matros E and Allen RJ Jr: Immediate dental implant placement in the
oncologic setting: A conceptual framework. Plast Reconstr Surg Glob
Open. 9(e3671)2021.PubMed/NCBI View Article : Google Scholar
|
|
2
|
Soldini MC, Arroyo I, Peragine R, Roldán
E, Valles C and Pons R: Long-Term evaluation of narrow-diameter
dental implants in posterior sites in patients with history of
periodontitis: A retrospective study with an 11.5-year mean
follow-up. Clin Oral Implants Res. 36:1535–1550. 2025.PubMed/NCBI View Article : Google Scholar
|
|
3
|
Zohary M, Malekzadeh M, Salari A, Afzali A
and Maleki D: Platelet-rich fibrin and concentrated growth factor
in the treatment of immediate implants in teeth with periapical
lesions: A clinical trial with two-year follow-up. J Dent Res Dent
Clin Dent Prospects. 19:89–96. 2025.PubMed/NCBI View Article : Google Scholar
|
|
4
|
Aldhohrah T, Qin G, Liang D, Song W, Ge L,
Mashrah MA and Wang L: Does simultaneous soft tissue augmentation
around immediate or delayed dental implant placement using
sub-epithelial connective tissue graft provide better outcomes
compared to other treatment options? A systematic review and
meta-analysis. PLoS One. 17(e0261513)2022.PubMed/NCBI View Article : Google Scholar
|
|
5
|
Raffat EM, Shady M, Elkashty AAR and Syad
ME: Comparative analysis of implant survival, peri-implant health,
and patient satisfaction among three treatment modalities in
atrophic posterior mandibles: A randomized clinical study. BMC Oral
Health. 25(939)2025.PubMed/NCBI View Article : Google Scholar
|
|
6
|
Bajaj V, Kolte AP, Kolte R and Bawankar
PV: Comparative evaluation of immediate implant placement and
provisionalization (IIPP) with and without a concentrated growth
factor-enriched bone graft: A randomized controlled trial. Dent Med
Probl. 62:449–459. 2025.PubMed/NCBI View Article : Google Scholar
|
|
7
|
Parihar AS, Nandanan N, Kurien VTV,
Bandgar S, Patri G, Laddha R and Kumar S: Impact of periodontal
biotype on the long-term esthetics of implant-supported
restorations: A 5-year prospective study. J Pharm Bioallied Sci. 17
(Suppl 1):S555–S557. 2025.PubMed/NCBI View Article : Google Scholar
|
|
8
|
Sghaireen MG, Alduraywish AA, Srivastava
KC, Shrivastava D, Patil SR, Al Habib S, Hamza M, Ab Rahman S,
Lynch E and Alam MK: Comparative evaluation of dental implant
failure among healthy and well-controlled diabetic patients-A
3-Year retrospective study. Int J Environ Res Public Health.
17(5253)2020.PubMed/NCBI View Article : Google Scholar
|
|
9
|
Heng S, Arunjaroensuk S, Pozzi A,
Damrongsirirat N, Pimkhaokham A and Mattheos N: Comparing medium to
long-term esthetic, clinical, and patient-reported outcomes between
freehand and computer-assisted dental implant placement: A
cross-sectional study. J Esthet Restor Dent. 37:834–843.
2025.PubMed/NCBI View Article : Google Scholar
|
|
10
|
Liu F, Wang YH, Xiong YJ and Ni YL:
Modified oral implant restoration improves dental aesthetics,
function, and patient satisfaction in maxillary anterior tooth
loss. Am J Transl Res. 17:983–991. 2025.PubMed/NCBI View Article : Google Scholar
|
|
11
|
Tanır KÖ, Avağ C, Tosun E and Akkocaoğlu
M: Evaluation of the quality of life and the satisfaction level
after reconstruction with anterior iliac crest graft and
implant-supported fixed prosthesis treatment. J Prosthodont.
32:801–806. 2023.PubMed/NCBI View Article : Google Scholar
|
|
12
|
Kalyoncuoğlu ÜT and Samur Ergüven S:
Social appearance anxiety and oral health-related quality of life
in middle-aged adults with implant therapy. Folia Med (Plovdiv).
65:277–282. 2023.PubMed/NCBI View Article : Google Scholar
|
|
13
|
Thomas DC, Bellani D, Piermatti J and
Kodaganallur Pitchumani P: Systemic factors affecting prognosis of
dental implants. Dent Clin North Am. 68:555–570. 2024.PubMed/NCBI View Article : Google Scholar
|
|
14
|
Ghorbani H, Minasyan A, Ansari D, Ghorbani
P, Wood DA, Yeremyan R, Ghorbani S and Minasian N: Anti-diabetic
therapies on dental implant success in diabetes mellitus: A
comprehensive review. Front Pharmacol. 15(1506437)2024.PubMed/NCBI View Article : Google Scholar
|
|
15
|
Enteghad S, Shirban F, Nikbakht MH,
Bagherniya M and Sahebkar A: Relationship between diabetes mellitus
and periodontal/peri-implant disease: A contemporaneous review. Int
Dent J. 74:426–445. 2024.PubMed/NCBI View Article : Google Scholar
|
|
16
|
He Y, Wang X, Wu Y, Li L, Liu M, Chen R,
He J, Mai W and Li X: Three decades of CKD due to diabetes mellitus
type 2 in China, with projections of disease burden from 2022 to
2036: A systematic analysis for the Global Burden of disease study
2021. Clin Kidney J. 18(sfaf265)2025.PubMed/NCBI View Article : Google Scholar
|
|
17
|
Luo H, Pan W, Sloan F, Feinglos M and Wu
B: Forty-year trends in tooth loss among American adults with and
without diabetes mellitus: An age-period-cohort analysis. Prev
Chronic Dis. 12(E211)2015.PubMed/NCBI View Article : Google Scholar
|
|
18
|
Rotim Ž, Pelivan I, Sabol I, Sušić M,
Ćatić A and Bošnjak AP: The effect of local and systemic factors on
dental implant failure-analysis of 670 patients with 1260 implants.
Acta Clin Croat. 60:367–372. 2022.PubMed/NCBI View Article : Google Scholar
|
|
19
|
Chen A, Ng ST, Goh V, Siu SC, Yeung K,
Tsang YC, Wang Q and Leung WK: Assessing oral health and the
minimally important differences in oral health-related quality of
life of non-diabetic and diabetic patients: A cross-sectional
study. Aust Dent J. 69:206–218. 2024.PubMed/NCBI View Article : Google Scholar
|
|
20
|
Sharma A, Deo A, Sharma A, Kumar D, Gupta
P and Cheema M: Assessment of prognosis of dental implants in
diabetic patients: A clinical study. J Pharm Bioallied Sci. 15
(Suppl 2):S920–S922. 2023.PubMed/NCBI View Article : Google Scholar
|
|
21
|
Yum H, Han HS, Kim K, Kim S and Cho YD:
The cumulative survival rate of sandblasted, large-grit,
acid-etched dental implants: A retrospective analysis. J
Periodontal Implant Sci. 54:122–135. 2024.PubMed/NCBI View Article : Google Scholar
|
|
22
|
Diehl D, Bespalov A, Yildiz MS and
Friedmann A: Restoration of posterior teeth by narrow diameter
implants in hyperglycemic and normoglycemic patients - 4-year
results of a case-control study. Clin Oral Investig.
28(392)2024.PubMed/NCBI View Article : Google Scholar
|
|
23
|
Tulbah HI, Alsahhaf A, AlRumaih HS, Vohra
F and Abduljabbar T: Clinical evaluation of short tuberosity
implants among type 2 diabetic and non-diabetic patients: A 5 year
follow-up. Medicina (Kaunas). 58(1487)2022.PubMed/NCBI View Article : Google Scholar
|
|
24
|
Tomar S, Sahani A and Kumar A: Implant
survival and peri-implant health in prediabetic and healthy
patients with adjacent implants over 5 years: A systematic review.
J Prosthet Dent. 135:579.e1–579.e7. 2026.PubMed/NCBI View Article : Google Scholar
|
|
25
|
Kaushik M, Srivastava A and Khattri S:
Long-term survival of dental implants in a patient with
periodontitis and diabetes mellitus: An eight-year follow-up case
report. Cureus. 16(e75852)2024.PubMed/NCBI View Article : Google Scholar
|
|
26
|
Herrero F, de Souza RF, Feine JS,
Alexander PP, Green AV and Oates TW: The impact of implant-retained
overdentures on type-2 diabetic and non-diabetic edentulous
patients: Satisfaction and quality of life in a prospective cohort
study. J Dent. 127(104357)2022.PubMed/NCBI View Article : Google Scholar
|
|
27
|
Friedmann A, Winkler M, Diehl D, Yildiz MS
and Bilhan H: One-year performance of posterior narrow diameter
implants in hyperglycemic and normo-glycemic patients-a pilot
study. Clin Oral Investig. 25:6707–6715. 2021.PubMed/NCBI View Article : Google Scholar
|
|
28
|
Do TA, Le HS, Shen YW, Huang HL and Fuh
LJ: Risk factors related to late failure of dental implant-A
systematic review of recent studies. Int J Environ Res Public
Health. 17(3931)2020.PubMed/NCBI View Article : Google Scholar
|
|
29
|
Huang N, Liu P, Yan Y, Xu L, Huang Y, Fu
G, Lan Y, Yang S, Song J and Li Y: Predicting the risk of dental
implant loss using deep learning. J Clin Periodontol. 49:872–883.
2022.PubMed/NCBI View Article : Google Scholar
|
|
30
|
Nyland AN, Lie SA and Gjerde CG: Risk
factors for early dental implant failure. Int J Oral Maxillofac
Implants. 39:164–172. 2024.PubMed/NCBI View Article : Google Scholar
|
|
31
|
In 't Veld M, Schulten EAJM and Leusink
FKJ: Immediate dental implant placement and restoration in the
edentulous mandible in head and neck cancer patients: A systematic
review and meta-analysis. Curr Opin Otolaryngol Head Neck Surg.
29:126–137. 2021.PubMed/NCBI View Article : Google Scholar
|
|
32
|
Zhai QK, Gao C, Shen ML, Shui YH, Tang T
and Liu K: Local risk factors for one-year dental implant loss and
late loss in 287 failed implants caused by peri-implantitis or
infection after prosthesis loading: a retrospective study. Br J
Oral Maxillofac Surg. 62:545–550. 2024.PubMed/NCBI View Article : Google Scholar
|
|
33
|
Zhang Q, Guo S, Li Y, Li Z, Wang D and
Zhang K: Analysis of risk indicators for implant failure in
patients with chronic periodontitis. BMC Oral Health.
24(1051)2024.PubMed/NCBI View Article : Google Scholar
|
|
34
|
Cheng Y, Lai Z and Yu W: Influencing
factors and survival rates in immediate vs. delayed dental implant
placement: A six-year retrospective analysis. Front Dent Med.
6(1563641)2025.PubMed/NCBI View Article : Google Scholar
|
|
35
|
Andrade CAS, Paz JLC, de Melo GS,
Mahrouseh N, Januário AL and Capeletti LR: Survival rate and
peri-implant evaluation of immediately loaded dental implants in
individuals with type 2 diabetes mellitus: A systematic review and
meta-analysis. Clin Oral Investig. 26:1797–1810. 2022.PubMed/NCBI View Article : Google Scholar
|
|
36
|
Stang A: Critical evaluation of the
Newcastle-Ottawa scale for the assessment of the quality of
nonrandomized studies in meta-analyses. Eur J Epidemiol.
25:603–605. 2010.PubMed/NCBI View Article : Google Scholar
|
|
37
|
Gómez-Moreno G, Aguilar-Salvatierra A,
Rubio Roldán J, Guardia J, Gargallo J and Calvo-Guirado JL:
Peri-implant evaluation in type 2 diabetes mellitus patients: A
3-year study. Clin Oral Implants Res. 26:1031–1035. 2015.PubMed/NCBI View Article : Google Scholar
|
|
38
|
Agliardi EL, Pozzi A, Romeo D and Del
Fabbro M: Clinical outcomes of full-arch immediate fixed prostheses
supported by two axial and two tilted implants: A retrospective
cohort study with 12-15 years of follow-up. Clin Oral Implants Res.
34:351–366. 2023.PubMed/NCBI View Article : Google Scholar
|
|
39
|
Aguilar-Salvatierra A, Calvo-Guirado JL,
González-Jaranay M, Moreu G, Delgado-Ruiz RA and Gómez-Moreno G:
Peri-implant evaluation of immediately loaded implants placed in
esthetic zone in patients with diabetes mellitus type 2: A two-year
study. Clin Oral Implants Res. 27:156–161. 2016.PubMed/NCBI View Article : Google Scholar
|
|
40
|
Al Amri MD, Kellesarian SV, Al-Kheraif AA,
Malmstrom H, Javed F and Romanos GE: Effect of oral hygiene
maintenance on HbA1c levels and peri-implant parameters around
immediately-loaded dental implants placed in type-2 diabetic
patients: 2 years follow-up. Clin Oral Implants Res. 27:1439–1443.
2016.PubMed/NCBI View Article : Google Scholar
|
|
41
|
Alves CC, Correia AR and Neves M:
Immediate implants and immediate loading in periodontally
compromised patients-a 3-year prospective clinical study. Int J
Periodontics Restorative Dent. 30:447–455. 2010.PubMed/NCBI
|
|
42
|
Bell CL, Diehl D, Bell BM and Bell RE: The
immediate placement of dental implants into extraction sites with
periapical lesions: A retrospective chart review. J Oral Maxillofac
Surg. 69:1623–1627. 2011.PubMed/NCBI View Article : Google Scholar
|
|
43
|
D'Orto B, Polizzi E, Nagni M, Tetè G and
Capparè P: Full arch implant-prosthetic rehabilitation in patients
with type I diabetes mellitus: Retrospective clinical study with 10
year follow-up. Int J Environ Res Public Health.
19(11735)2022.PubMed/NCBI View Article : Google Scholar
|
|
44
|
Tawil G, Younan R, Azar P and Sleilati G:
Conventional and advanced implant treatment in the type II diabetic
patient: Surgical protocol and long-term clinical results. Int J
Oral Maxillofac Implants. 23:744–752. 2008.PubMed/NCBI
|
|
45
|
Han LP: Clinical observation of immediate
implantation of central incisors in patients with type 2 diabetes
mellitus at different glycated hemoglobin levels. Master's thesis.
Inner Mongolia Medical University, 2021 (In Chinese). Available at:
Wanfang Data (wanfangdata.com.cn).
|
|
46
|
Zhao GQ, Ding F, Liu Y, Shi SJ, Liu XD,
Zhao WB, Wang XX, Zhang SJ and Song YL: Prognosis and influencing
factors of immediate implantation in T2DM patients:A retrospective
study. Practical Journal of Stomatology. 38:74–79. 2022.(In
Chinese). Available at: CNKI (cnki.net).
|
|
47
|
Carpentieri J and Greenstein G: Guidelines
for immediate vs delayed dental implant placement in the esthetic
zone. Compend Contin Educ Dent. 45:340–347; quiz 348.
2024.PubMed/NCBI
|
|
48
|
Slagter KW, Meijer HJA, Hentenaar DFM,
Vissink A and Raghoebar GM: Immediate single-tooth implant
placement with simultaneous bone augmentation versus delayed
implant placement after alveolar ridge preservation in bony defect
sites in the esthetic region: A 5-year randomized controlled trial.
J Periodontol. 92:1738–1748. 2021.PubMed/NCBI View Article : Google Scholar
|
|
49
|
Puisys A, Auzbikaviciute V,
Vindasiute-Narbute E, Pranskunas M, Razukevicus D and Linkevicius
T: Immediate implant placement vs. early implant treatment in the
esthetic area. A 1-year randomized clinical trial. Clin Oral
Implants Res. 33:634–655. 2022.PubMed/NCBI View Article : Google Scholar
|
|
50
|
Chatzopoulos GS and Wolff LF: Assessing
the long-term survival of dental implants in a retrospective
Analysis: Immediate versus delayed placement. Clin Exp Dent Res.
11(e70096)2025.PubMed/NCBI View Article : Google Scholar
|
|
51
|
Nourah D, Aldahlawi S and Andreana S:
Should the quality of glycemic control guide dental implant therapy
in patients with diabetes? Focus on implant survival. Curr Diabetes
Rev. 18(e060821195367)2022.PubMed/NCBI View Article : Google Scholar
|
|
52
|
Monje A, Kan JY and Borgnakke W: Impact of
local predisposing/precipitating factors and systemic drivers on
peri-implant diseases. Clin Implant Dent Relat Res. 25:640–660.
2023.PubMed/NCBI View Article : Google Scholar
|
|
53
|
Lang L and Saponaro PC, Hammoudeh H,
Barnett SD, Nassani LM, Hsieh YL, Azer SS and Saponaro PC:
Evaluation endosseous dental implants success rate, adverse events,
and associated risk factors: A retrospective study. Int J Oral
Maxillofac Implants. 0:1–30. 2025.
|
|
54
|
Ayele S, Sharo N and Chrcanovic BR:
Marginal bone loss around dental implants: Comparison between
diabetic and non-diabetic patients-a retrospective clinical study.
Clin Oral Investig. 27:2833–2841. 2023.PubMed/NCBI View Article : Google Scholar
|
|
55
|
Abi Rached S, Chakar C, Samarani R,
Menassa G, Sembronio S, Pucci R, Calabrese L, Cantore S, Malcangi
A, Spirito F and DI Cosola M: Radiographic marginal bone level
evaluation around two different tissue-level implant systems: A
one-year prospective study. Minerva Dent Oral Sci. 72:298–311.
2023.PubMed/NCBI View Article : Google Scholar
|
|
56
|
Geraets W, Zhang L, Liu Y and Wismeijer D:
Annual bone loss and success rates of dental implants based on
radiographic measurements. Dentomaxillofac Radiol.
43(20140007)2014.PubMed/NCBI View Article : Google Scholar
|
|
57
|
Alsahhaf A, Alali Y, Albeshri S, Subayt
AKA, Alomayri A, Abduljabbar T and Vohra F: Clinical, radiographic,
and inflammatory peri-implant parameters around narrow diameter
implant crowns among prediabetic and non-diabetic subjects.
Medicina (Kaunas). 58(1839)2022.PubMed/NCBI View Article : Google Scholar
|
|
58
|
Lv X, Zou L, Zhang X, Zhang X, Lai H and
Shi J: Effects of diabetes/hyperglycemia on peri-implant biomarkers
and clinical and radiographic outcomes in patients with dental
implant restorations: A systematic review and meta-analysis. Clin
Oral Implants Res. 33:1183–1198. 2022.PubMed/NCBI View Article : Google Scholar
|
|
59
|
Shang R and Gao L: Impact of hyperglycemia
on the rate of implant failure and peri-implant parameters in
patients with type 2 diabetes mellitus: Systematic review and
meta-analysis. J Am Dent Assoc. 152:189–201.e1. 2021.PubMed/NCBI View Article : Google Scholar
|
|
60
|
de Oliveira PGFP, Bonfante EA, Bergamo
ETP, de Souza SLS, Riella L, Torroni A, Benalcazar Jalkh EB, Witek
L, Lopez CD, Zambuzzi WF and Coelho PG: Obesity/metabolic syndrome
and diabetes mellitus on peri-implantitis. Trends Endocrinol Metab.
31:596–610. 2020.PubMed/NCBI View Article : Google Scholar
|
|
61
|
Ali D, Baskaradoss JK and Joseph BK:
cortisol levels in the peri-implant sulcular fluid of type-2
diabetic and non-diabetic patients with peri-implantitis. Oral
Health Prev Dent. 20:219–226. 2022.PubMed/NCBI View Article : Google Scholar
|
|
62
|
Jervøe-Storm PM, Bunke J, Worthington HV,
Needleman I, Cosgarea R, MacDonald L, Walsh T, Lewis SR and Jepsen
S: Adjunctive antimicrobial photodynamic therapy for treating
periodontal and peri-implant diseases. Cochrane Database Syst Rev.
7(CD011778)2024.PubMed/NCBI View Article : Google Scholar
|
|
63
|
Herrera D, Berglundh T, Schwarz F, Chapple
I, Jepsen S, Sculean A, Kebschull M, Papapanou PN, Tonetti MS and
Sanz M: EFP workshop participants and methodological consultant.
Prevention and treatment of peri-implant diseases-The EFP S3 level
clinical practice guideline. J Clin Periodontol. 50 (Suppl
26):S4–S76. 2023.PubMed/NCBI View Article : Google Scholar
|
|
64
|
Sterne JA, Sutton AJ, Ioannidis JP, Terrin
N, Jones DR, Lau J, Carpenter J, Rücker G, Harbord RM, Schmid CH,
et al: Recommendations for examining and interpreting funnel plot
asymmetry in meta-analyses of randomised controlled trials. BMJ.
343(d4002)2011.PubMed/NCBI View Article : Google Scholar
|