Introduction
Stevens-Johnson syndrome (SJS) and toxic epidermal
necrolysis (TEN) are acute drug-induced hypersensitivity adverse
reactions that predominantly involve the skin and mucous membranes.
Although rare, with an incidence of ~5.76 cases per million
person-years (1), these conditions
are life-threatening. Subsequent to its onset, the diseases
progress rapidly, follow a severe clinical course and are
associated with a relatively high mortality rate (2). Carbamazepine (CBZ) is a widely used
broad-spectrum antiepileptic drug in clinical practice and it can
also be used for the treatment of other diseases, including
trigeminal neuralgia, glossopharyngeal neuralgia, bipolar disorder
and manic episodes. Due to its definite efficacy and good
tolerability, it is widely applied in clinical practice. However,
with the increase in clinical application, cases of
carbamazepine-induced SJS have been frequently reported in the
literature (3-5).
The role of genetic factors in the pathogenesis of CBZ-related
SJS/TEN has attracted widespread attention, among which the
polymorphism of human leukocyte antigen (HLA) genes is closely
related to the occurrence of the disease. Studies have shown that
major histocompatibility complex, class I, A
(HLA-A)*3101 and HLA-B*1502 genotypes are
important genetic risk factors for CBZ-induced SJS/TEN (6). The HLA-B*1502 genotype has
the strongest correlation with CBZ-related SJS/TEN in Asian
populations (7,8), while the HLA-A*3101
genotype is significantly associated with CBZ-related SJS/TEN
worldwide, especially in Europe (9). At present, clinical guidelines
recommend that before using CBZ, HLA-B*1502 genotype
screening should be performed for Asian populations and
HLA-A*3101 genotype screening should be performed for
Caucasian populations to reduce the risk of CBZ-related SJS/TEN
(10). However, clinical practice
has found that certain patients with CBZ-related SJS/TEN have
negative screening results for both HLA-A*3101 and
HLA-B*1502 genotypes. Such cases suggest that the
pathogenesis of CBZ-induced SJS is not only determined by the above
two HLA genotypes, but may also involve the synergistic effect of
various factors, including other genetic factors, environmental
factors (such as combined medication, infection) and individual
metabolic differences (11). The
present study reported a case of CBZ-induced SJS in a Chinese
patient with negative HLA-A*3101 and
HLA-B*1502 genotypes. The innovation and uniqueness of
the present study are mainly reflected in three aspects: Case
specificity, research perspective and clinical value. In terms of
case specificity, this study supplemented a rare case type and
enriching the clinical spectrum of the disease. From the research
and clinical perspective, this study analyzed a rare HLA
double-negative case, and summarized the clinical features and core
management strategies. It is helpful to deepen the clinical
understanding of CBZ-induced SJS and offer a certain reference for
rational clinical medication.
Case report
A 34-year-old female patient with blepharospasm
started taking CBZ upon the recommendation of a neurologist to
relieve the symptoms. The initial oral dosage was 100 mg twice
daily, which was increased to 200 mg twice daily after 3 days.
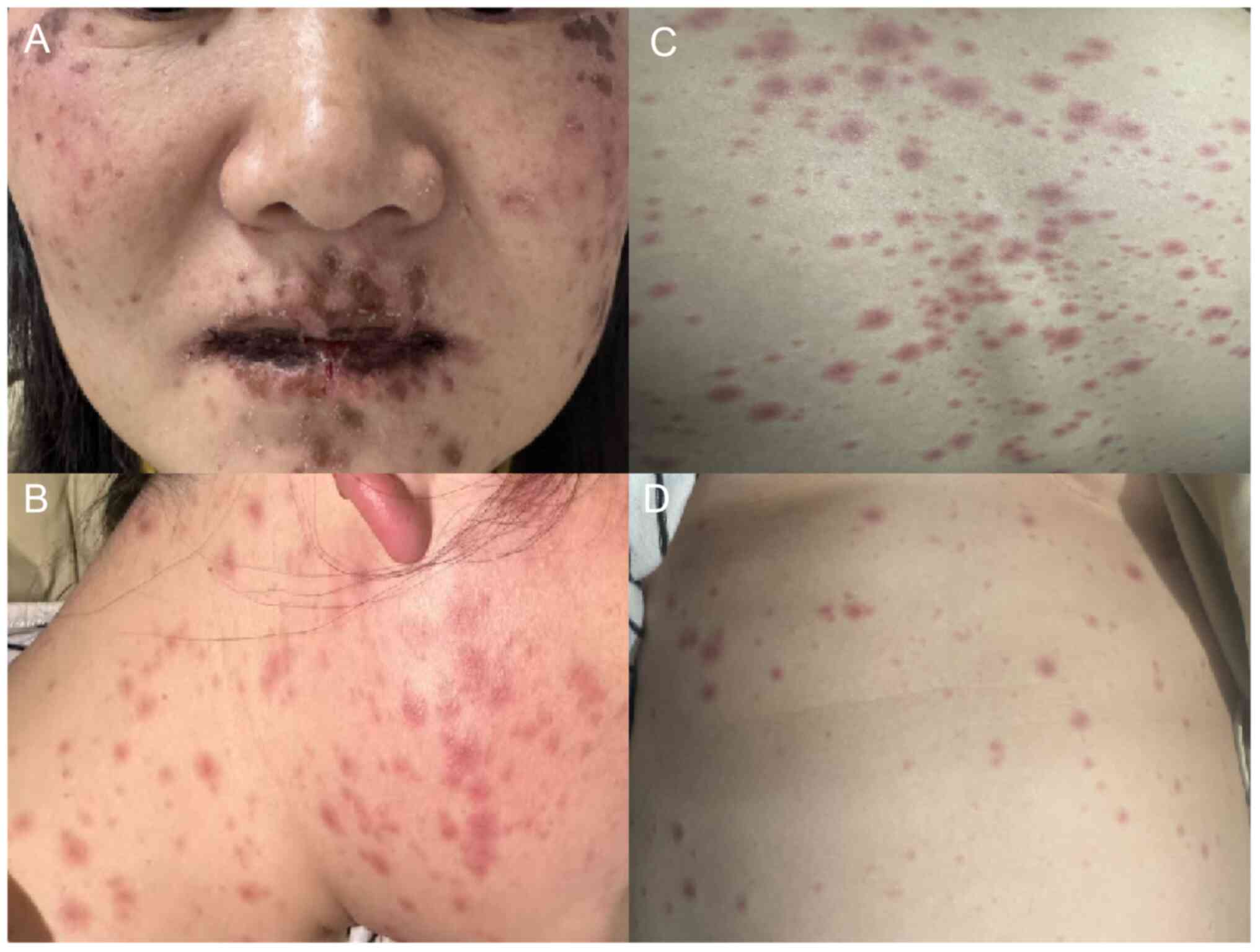
Following 2 weeks of CBZ treatment, the patient developed a
generalized rash with pruritus, which was followed by the gradual
emergence of macular erythema on the chest, back, oral cavity and
lips, along with oral herpes lesions (Fig. 1). After 7 days, as the condition had
progressed, the herpes vesicles ruptured and exuded fluid, leading
to difficulty in opening the mouth and subsequent inability to eat.
During the onset of symptoms, the patient did not present with any
fever or other systemic manifestations, and prior to this episode,
the patient had not taken any other medications or consumed any
special foods. Upon admission to Wufeng Tujia Autonomous County
People's Hospital in November 2025, based on the clinical
manifestations, the patient was diagnosed with SJS. The Severity of
Illness Score for TEN (SCORTEN) (12) was adopted to evaluate the patient,
who obtained a score of 1, indicating a low risk of mortality.
Genetic testing revealed a negative status for both the
HLA-A*3101 and HLA-B*1502 genes. The genetic
testing was performed using a real-time PCR with sequence-specific
primer method. Genomic DNA was extracted from the patient's
peripheral blood sample using a commercial DNA extraction kit
(HiPure blood DNA mini kit; cat. no. D3111; Guangzhou Magen
Biotechnology Co., Ltd.). The kit used for amplification and
detection was TargetSeq® Target Probes (T216V1),
manufactured by iGeneTech Biotech (Beijing) Co., Ltd. (cat. no.
PT1001832; batch no. 69136402); the procedures were carried out on
a real-time fluorescent quantitative PCR instrument (ABI 9700;
Thermo Fisher Scientific, Inc.) following the manufacturer's
standard protocol. Genotypes were determined based on the presence
or absence of specific amplification signals for the target
alleles. All the genetic testing work was performed by CRED
Diagnostics in Wuhan (China). CBZ was immediately discontinued and
the patient was administered 10 mg of dexamethasone via intravenous
infusion. After 3 days, the patient's pain symptoms had improved.
The dose of dexamethasone was then tapered to 5 mg for a further 3
days, after which the herpes lesions began to resolve and no new
rashes or erythematous changes appeared across the patient's body.
The dose of dexamethasone was then tapered to 3 mg for another 3
days before complete discontinuation. During the treatment, in
addition to dexamethasone, analgesic drugs (oral ibuprofen 300 mg
three times daily) were also intermittently administrated, the
patient was supplemented with vitamin C, energy supplements, fluids
and electrolytes and the patient was instructed to use mouthwash to
maintain oral hygiene. After 10 days of treatment, the patient was
discharged with significant improvement. The patient was advised to
have adequate rest and follow a light diet within two weeks after
discharge. Daily normal saline gargling was performed to keep the
oral cavity clean. The skin and mucous membranes were maintained
clean and dry to prevent wound damage and secondary infection.
Regular hospital follow-up was arranged once a week.
Discussion
SJS, also known as erythema multiforme major drug
eruption, is a rare type IV delayed hypersensitivity reaction
primarily induced by drug factors (95%). In addition to
characteristic bullous skin reactions and epidermal detachment, it
often involves mucosal tissues, such as the oral cavity, eyes and
genitourinary tract, and may also be accompanied by fever (13,14).
The disease has an acute onset, rapid progression and potential for
recurrence. It is highly prone to infections and systemic
complications, and severe cases may even develop multiple organ
failure leading to death. There are significant ethnic differences
in the incidence of SJS, with Asians having twice the risk of
developing the disease compared to Caucasians (15). Currently, the pathogenesis of SJS is
not fully understood. Studies have confirmed that SJS is mainly
caused by drugs (14,15), such as sulfonamides, antiepileptic
drugs, non-steroidal anti-inflammatory drugs, allopurinol and
nevirapine. Additionally, immune factors and genetic factors of the
body also have a certain impact on the onset of the disease.
The major histocompatibility complex (MHC) is a
group of highly conserved cell surface proteins. In humans, MHC is
also referred to as HLA. The primary functions of the HLA gene
system include participating in self-recognition, regulating immune
responses and mediating rejection of allogeneic transplants
(16). It is generally recognized
that both humoral immunity and cellular immunity are involved in
allergic reactions. Humoral immunity is dominated by immunoglobulin
E-mediated allergic reactions, while cellular immunity is initiated
through the T cell receptor-antigen peptide-MHC complex. In rare
cases, certain drugs can induce immune responses by interacting
with HLA molecules, resulting in adverse drug reactions (ADRs).
Polymorphism in HLA genes increases the likelihood of off-target
binding between HLA molecules and small-molecule drugs. These
potential off-target interactions are associated with T
cell-mediated ADRs; however, the mechanisms underlying most
HLA-related drug interactions remain poorly understood. Immune
responses triggered by different HLA-B genes may lead to
dose-independent ADRs (17), such
as SJS and TEN. Numerous studies have confirmed an association
between the HLA-B*1502 gene and CBZ-induced SJS/TEN
(18,19). In a study involving 44 patients with
CBZ-induced SJS/TEN, all participants were found to carry the
HLA-B*1502 allele. Subsequent studies verified this
association between CBZ-induced SJS/TEN and HLA-B*1502
across diverse Asian populations, including those in China,
Thailand, Malaysia and India (19).
A meta-analysis across multiple populations revealed a significant
association between HLA-A*3101 and CBZ-induced
drug-induced hypersensitivity syndrome, however no significant
association with CBZ-induced SJS/TEN (20). Another study indicated that
HLA-A*3101 is a predictive marker for CBZ-induced
allergic reactions in Europeans (5).
These findings suggest that the type of cutaneous
adverse drug reactions may be determined by genetic variations.
Consequently, guidelines and drug labels recommend
HLA-B*1502 genotyping for high-risk populations prior to
CBZ administration. CBZ should not be used in individuals positive
for this allele unless the potential benefits outweigh the risks
(10). In the present case, the
patient did not undergo genotyping before administration of CBZ.
HLA-B*1502 and HLA-A*3101 genes were tested
during the treatment and the results showed that both were
negative. This result holds significant clinical significance,
suggesting that the pathogenesis of CBZ-induced SJS is complex and
diverse. In current clinical practice, positive HLA gene screening
indicates a significantly increased risk of SJS following CBZ
administration; however, negative gene screening cannot completely
rule out the possibility of SJS occurrence. This case exemplified
the following clinical scenario: Despite the absence of relevant
risk gene carriers, the patient still developed SJS after CBZ
treatment. This indicates that in addition to HLA-A*3101
and HLA-B*1502 genes, other genetic factors,
environmental factors or individual metabolic differences may be
involved in the pathogenesis of CBZ-related SJS. It also dispels
the misconception that ‘negative gene results ensure safe CBZ use’
and provides important practical insights for clinical medication
risk assessment.
The SCORTEN is widely used to predict the mortality
of patients with SJS/TEN (21).
SCORTEN should be assessed within 24 h of admission and
re-evaluated on the 3rd day. This scoring system is based on seven
independent risk factors: Age, malignant tumor, tachycardia,
epidermal detachment rate, serum urea, serum glucose and
bicarbonate levels (Table SI). The
more risk factors present, the higher the mortality rate (Table SII).
Currently, there is no standard treatment protocol
for SJS, and symptomatic and supportive care remains the mainstay
of management. Intravenous immunoglobulin (IVIg) has been widely
used in patients with SJS/TEN. Previously, the clinical benefit of
IVIg in patients with SJS was controversial; however, recent
studies have demonstrated that high-dose IVIg (<2 g/kg) exerts a
positive effect on reducing the mortality of SJS/TEN (22). Similarly, the efficacy of systemic
corticosteroids in SJS treatment is controversial. A major concern
is that corticosteroid use in patients with SJS/TEN may increase
the risk of infection, although some studies have also reported
positive therapeutic effects (23,24). A
growing body of evidence indicates that combined treatment with
IVIg and corticosteroids, rather than IVIg monotherapy, can improve
the prognosis of SJS/TEN (25-27).
In addition, therapeutic plasma exchange (PE) and the double plasma
molecular adsorption system (DPMAS) are also potential treatments
in SJS/TEN. The mechanism of PE is removal of drug, drug
metabolites and cytokines from the patient. The Japanese guidelines
recommend systematic steroids, IVIg and PE as the three first-line
treatments of choice. Although certain studies have shown PE was
effective in the treatment of SJS/TEN (28-30),
its efficacy has been found to be controversial in clinical
practice (31,32). A recent study showed no benefit of
PE for reducing in-hospital mortality or the length of hospital
stay (33). The DPMAS is a blood
purification technique that employs various adsorbents to
non-selectively bind and eliminate toxins or inflammatory mediators
in the blood, thereby alleviating inflammation and regulating
immune responses. A study reported that the levels of TNF-α and
IFN-γ were elevated in patients with SJS/TEN and decrease
significantly following DPMAS treatment (34). It is speculated that the adsorption
effect of DPMAS is similar to that of TNF inhibitors, as it can
reduce pro-inflammatory factors and thus inhibit the progression of
SJS/TEN. Cyclosporine, a calcineurin inhibitor, can regulate T
lymphocyte-mediated cytotoxicity and inhibit key molecules such as
Fas ligand, NF-κB and TNF-α. Multiple case reports and
meta-analyses have confirmed that cyclosporine treatment can
improve the survival rate of patients with SJS/TEN (35,36).
The complex pathogenesis and rarity of SJS/TEN pose significant
challenges to its treatment. Although the aforementioned
therapeutic approaches have demonstrated certain efficacy,
limitations such as small sample sizes and the lack of randomized
controlled trials have compromised the quality of relevant studies.
Consequently, a definitive standard treatment for this disease
remains unavailable to date.
Therapeutic intervention for the patient in the
present case was the discontinuation of CBZ, combined with stepwise
administration of dexamethasone (10 mg intravenously for 3
consecutive days, followed by 5 mg for 3 days and 3 mg for 2 days).
Other supportive measures included analgesia, energy support,
maintenance of water-electrolyte balance, keeping skin wounds dry
and using mouthwash to maintain oral hygiene. The treatment
achieved a significant effect: The systemic symptoms improved
markedly after 10 days of hospitalization and was the patient was
discharged successfully. The patient was treated with intravenous
dexamethasone alone, without IVIg, for two reasons: Symptoms had
peaked at admission (SCORTEN score 1) with no subsequent
progression, reflecting low mortality risk, and the patient opted
for monotherapy due to financial difficulties. Nevertheless, it may
be reasonable to assume that IVIg should be prioritized in
combination therapy when clinically indicated to ensure therapeutic
efficacy.
Since this present study is a retrospective case
study, it is necessary to point out that it has certain
limitations. First, the present study is a single-case report,
which only reports one Chinese patient with CBZ-induced SJS who is
negative for both HLA-A*3101 and HLA-B*1502
genotypes. The small sample size limits the generalizability and
representativeness of the research conclusions, making it
impossible to fully reflect the overall clinical characteristics
and pathogenic rules for such cases. Second, the present study only
detected two genotypes, HLA-A*3101 and
HLA-B*1502, and did not further explore the specific
roles of other potential genetic factors involved in the
pathogenesis, such as other HLA subtypes, environmental factors or
individual metabolic differences. In the future, more cases of
CBZ-related SJS with negative HLA-A*3101 and
HLA-B*1502 genotypes will be collected, and integrated
basic and clinical research will be further carried out to screen
and verify other genetic factors, environmental factors and
metabolism-related factors that may be involved in the pathogenesis
of CBZ-induced HLA-negative SJS, so as to improve the pathogenesis
system of CBZ-related SJS.
In summary, SJS is a severe disease primarily
induced by drugs, and can be life-threatening. Genotyping for
HLA-A*3101 and HLA-B*1502 should be conducted
before initiating CBZ therapy, so as to assess the risk of SJS. It
is still necessary to keep close clinical monitoring during and
after CBZ administration even if the patient tests negative for
HLA-A*3101 and HLA-B*1502 genes. On the one
hand, SJS has an acute onset and rapid progression, and early
identification and timely intervention are key to improving
prognosis and reducing mortality. On the other hand, as shown in
the present case, negative gene screening cannot completely avoid
the onset risk; clinicians should not lower their vigilance, but
inform patients to closely observe symptoms during medication
(especially within 2-8 weeks, the high-incidence period of SJS) and
seek medical attention immediately with drug withdrawal if abnormal
manifestations occur to avoid delayed treatment.
Supplementary Material
SCORTEN scoring system to assess
severity and predict mortality in Stevens-Johnson
syndrome/TEN.
Interpretation of the SCORTEN
score.
Acknowledgements
Not applicable.
Funding
Funding: No funding was received.
Availability of data and materials
All data generated in the study are included in the
article.
Authors' contributions
All authors were involved in the patient's care. ZY
and JL contributed to the conception, design and data collection.
FY drafted the manuscript. ZY and JL confirmed the authenticity of
all raw data. All authors read and approved the final
manuscript.
Ethics approval and consent to
participate
The present study was conducted according to the
principles of the Declaration of Helsinki. The patient agreed to
receive relevant clinical examinations including genetic
testing.
Patient consent for publication
Written consent was obtained from the patient for
the publication of clinical data and images in this academic
paper.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Frey N, Jossi J, Bodmer M, Bircher A, Jick
SS, Meier CR and Spoendlin J: The epidemiology of stevens-johnson
syndrome and toxic epidermal necrolysis in the UK. J Invest
Dermatol. 137:1240–1247. 2017.PubMed/NCBI View Article : Google Scholar
|
|
2
|
Sunaga Y, Kurosawa M, Ochiai H, Watanabe
H, Sueki H, Azukizawa H, Asada H, Watanabe Y, Yamaguchi Y, Aihara
M, et al: The nationwide epidemiological survey of Stevens-Johnson
syndrome and toxic epidermal necrolysis in Japan, 2016-2018. J
Dermatol Sci. 100:175–182. 2020.PubMed/NCBI View Article : Google Scholar
|
|
3
|
Subramanian A, Haitharali R, Nirenjen S,
Tamilanban T, Dhanasekaran S, Gnanasekaran S, Manavalan M and Raja
S: Carbamazepine-induced Stevens-Johnson syndrome: A case report
with review of the literature. Curr Drug Saf. 20:382–387.
2025.PubMed/NCBI View Article : Google Scholar
|
|
4
|
Khoo ABS, Ali FR, Yiu ZZN and Ferguson JE:
Carbamazepine induced Stevens-Johnson syndrome. BMJ Case Rep.
2016(bcr2016214926)2016.PubMed/NCBI View Article : Google Scholar
|
|
5
|
Xu YY, Sun ZL, Zhang XL, Liu ZL, Liu W and
Guan X: Carbamazepine induced Stevens-Johnson syndrome in Han
Chinese with positive HLA-A * 3101 gene: A case report. Beijing Da
Xue Xue Bao Yi Xue Ban. 55:755–757. 2023.PubMed/NCBI View Article : Google Scholar : (In Chinese).
|
|
6
|
Marks ME, Botta RK, Abe R, Beachkofsky TM,
Boothman I, Carleton BC, Chung WH, Cibotti RR, Dodiuk-Gad RP,
Grimstein C, et al: Updates in SJS/TEN: Collaboration, innovation,
and community. Front Med (Lausanne). 10(1213889)2023.PubMed/NCBI View Article : Google Scholar
|
|
7
|
Yang SC, Chen CB, Lin MY, Zhang ZY, Jia
XY, Huang M, Zou YF and Chung WH: Genetics of severe cutaneous
adverse reactions. Front Med (Lausanne). 8(652091)2021.PubMed/NCBI View Article : Google Scholar
|
|
8
|
Tempark T, John S, Rerknimitr P,
Satapornpong P and Sukasem C: Drug-induced severe cutaneous adverse
reactions: Insights into clinical presentation, immunopathogenesis,
diagnostic methods, treatment, and pharmacogenomics. Front
Pharmacol. 13(832048)2022.PubMed/NCBI View Article : Google Scholar
|
|
9
|
Zhou Y, Krebs K, Milani L and Lauschke VM:
Global frequencies of clinically important HLA alleles and their
implications for the cost-effectiveness of preemptive
pharmacogenetic testing. Clin Pharmacol Ther. 109:160–174.
2021.PubMed/NCBI View
Article : Google Scholar
|
|
10
|
Phillips EJ, Sukasem C, Whirl-Carrillo M,
Müller DJ, Dunnenberger HM, Chantratita W, Goldspiel B, Chen YT,
Carleton BC, George AL Jr, et al: Clinical pharmacogenetics
implementation consortium guideline for HLA genotype and use of
carbamazepine and oxcarbazepine: 2017 update. Clin Pharmacol Ther.
103:574–581. 2018.PubMed/NCBI View
Article : Google Scholar
|
|
11
|
Cheng L: Current pharmacogenetic
perspective on Stevens-Johnson syndrome and toxic epidermal
necrolysis. Front Pharmacol. 12(588063)2021.PubMed/NCBI View Article : Google Scholar
|
|
12
|
Dobry AS, Himed S, Waters M and
Kaffenberger BH: Scoring assessments in Stevens-Johnson syndrome
and toxic epidermal necrolysis. Front Med (Lausanne).
9(883121)2022.PubMed/NCBI View Article : Google Scholar
|
|
13
|
Sharma N, Venugopal R, Maharana PK,
Chaniyara M, Agarwal T, Pushker N, Pandey RM, Sangwan S, Sen S,
Kashyap S, et al: Multistep grading system for evaluation of
chronic ocular sequelae in patients with Stevens-Johnson syndrome.
Am J Ophthalmol. 203:69–77. 2019.PubMed/NCBI View Article : Google Scholar
|
|
14
|
Hasegawa A and Abe R: Stevens-Johnson
syndrome and toxic epidermal necrolysis: Updates in pathophysiology
and management. Chin Med J (Engl). 137:2294–2307. 2024.PubMed/NCBI View Article : Google Scholar
|
|
15
|
Oakley AM and Krishnamurthy K:
Stevens-Johnson syndrome. StatPearls Publishing, Treasure Island,
FL, 2023.
|
|
16
|
Lenz TL: HLA genes: A hallmark of
functional genetic variation and complex evolution. Methods Mol
Biol. 2809:1–18. 2024.PubMed/NCBI View Article : Google Scholar
|
|
17
|
Illing PT, Purcell AW and McCluskey J: The
role of HLA genes in pharmacogenomics: Unravelling HLA associated
adverse drug reactions. Immunogenetics. 69:617–630. 2017.PubMed/NCBI View Article : Google Scholar
|
|
18
|
Biswas M, Ershadian M, Shobana J, Nguyen
AH and Sukasem C: Associations of HLA genetic variants with
carbamazepine-induced cutaneous adverse drug reactions: An updated
meta-analysis. Clin Transl Sci. 15:1887–1905. 2022.PubMed/NCBI View Article : Google Scholar
|
|
19
|
Schneider JA and Cohen PR: Stevens-Johnson
syndrome and toxic epidermal necrolysis: A concise review with a
comprehensive summary of therapeutic interventions emphasizing
supportive measures. Adv Ther. 34:1235–1244. 2017.PubMed/NCBI View Article : Google Scholar
|
|
20
|
Ozeki T, Mushiroda T, Yowang A, Takahashi
A, Kubo M, Shirakata Y, Ikezawa Z, Iijima M, Shiohara T, Hashimoto
K, et al: Genome-wide association study identifies
HLA-A*3101 allele as a genetic risk factor for
carbamazepine-induced cutaneous adverse drug reactions in Japanese
population. Hum Mol Genet. 20:1034–1041. 2011.PubMed/NCBI View Article : Google Scholar
|
|
21
|
Hasegawa A and Abe R: Recent advances in
managing and understanding Stevens-Johnson syndrome and toxic
epidermal necrolysis. F1000Res 9: F1000 Faculty Rev-612, 2020.
|
|
22
|
Jacobsen A, Olabi B, Langley A, Beecker J,
Mutter E, Shelley A, Worley B, Ramsay T, Saavedra A, Parker R, et
al: Systemic interventions for treatment of Stevens-Johnson
syndrome (SJS), toxic epidermal necrolysis (TEN), and SJS/TEN
overlap syndrome. Cochrane Database Syst Rev.
3(CD013130)2022.PubMed/NCBI View Article : Google Scholar
|
|
23
|
Morita K, Matsui H, Michihata N, Fushimi K
and Yasunaga H: Association of early systemic corticosteroid
therapy with mortality in patients with Stevens-Johnson syndrome or
toxic epidermal necrolysis: A retrospective cohort study using a
nationwide claims database. Am J Clin Dermatol. 20:579–592.
2019.PubMed/NCBI View Article : Google Scholar
|
|
24
|
Zimmermann S, Sekula P, Venhoff M,
Motschall E, Knaus J, Schumacher M and Mockenhaupt M: Systemic
immunomodulating therapies for Stevens-Johnson syndrome and toxic
epidermal necrolysis: A systematic review and meta-analysis. JAMA
Dermatol. 153:514–522. 2017.PubMed/NCBI View Article : Google Scholar
|
|
25
|
Barron SJ, Del Vecchio MT and Aronoff SC:
Intravenous immunoglobulin in the treatment of Stevens-Johnson
syndrome and toxic epidermal necrolysis: A meta-analysis with
meta-regression of observational studies. Int J Dermatol.
54:108–115. 2015.PubMed/NCBI View Article : Google Scholar
|
|
26
|
Tsai TY, Huang IH, Chao YC, Li H, Hsieh
TS, Wang HH, Huang YT, Chen CY, Cheng YC, Kuo PH, et al: Treating
toxic epidermal necrolysis with systemic immunomodulating
therapies: A systematic review and network meta-analysis. J Am Acad
Dermatol. 84:390–397. 2021.PubMed/NCBI View Article : Google Scholar
|
|
27
|
Yang L, Shou YH, Li F, Zhu XH, Yang YS and
Xu JH: Intravenous immunoglobulin combined with corticosteroids for
the treatment of Stevens-Johnson syndrome/toxic epidermal
necrolysis: A propensity-matched retrospective study in China.
Front Pharmacol. 12(750173)2022.PubMed/NCBI View Article : Google Scholar
|
|
28
|
Liao SQ, Yan ZR, Lin LW, Deng M, Xiao GJ
and Gao PY: Plasmapheresis for refractory toxic epidermal
necrolysis unresponsive to conventional therapy: A case report and
literature review. Front Immunol. 16(1579349)2025.PubMed/NCBI View Article : Google Scholar
|
|
29
|
Watari T, Sato S, Uojima H and Tokuda Y:
Successful combination therapy including plasma exchange for severe
toxic epidermal necrolysis. J Gen Fam Med. 17:232–237. 2016.
|
|
30
|
Aihara Y, Oyama Y, Ichikawa K, Takeshita
S, Takahashi Y, Kambara T and Aihara M: Toxic epidermal necrolysis
in a 4-year-old boy successfully treated with plasma exchange in
combination with methylprednisolone and i.v. immunoglobulin. J
Dermatol. 39:951–952. 2012.PubMed/NCBI View Article : Google Scholar
|
|
31
|
Furubacke A, Berlin G, Anderson C and
Sjöberg F: Lack of significant treatment effect of plasma exchange
in the treatment of drug-induced toxic epidermal necrolysis?
Intensive Care Med. 25:1307–1310. 1999.PubMed/NCBI View Article : Google Scholar
|
|
32
|
Miyamoto Y, Ohbe H, Kumazawa R, Matsui H,
Fushimi K, Yasunaga H and Ohta B: Evaluation of plasmapheresis vs
immunoglobulin as first treatment after ineffective systemic
corticosteroid therapy for patients with stevens-johnson syndrome
and toxic epidermal necrolysis. JAMA Dermatol. 159:481–487.
2023.PubMed/NCBI View Article : Google Scholar
|
|
33
|
Senda A and Fushimi K: Effectiveness of
early treatment with plasma exchange in patients with
Stevens-Johnson syndrome and toxic epidermal necrolysis. Sci Rep.
14(2893)2024.PubMed/NCBI View Article : Google Scholar
|
|
34
|
Tan YW, Liu LP and Zhang K: Double plasma
molecular adsorption system for Stevens-Johnson syndrome/toxic
epidermal necrolysis: A case report. World J Clin Cases.
12:1371–1377. 2024.PubMed/NCBI View Article : Google Scholar
|
|
35
|
Ng QX, De Deyn MLZQ, Venkatanarayanan N,
Ho CYX and Yeo WS: A meta-analysis of cyclosporine treatment for
Stevens-Johnson syndrome/toxic epidermal necrolysis. J Inflamm Res.
11:135–142. 2018.PubMed/NCBI View Article : Google Scholar
|
|
36
|
Shah R, Chen ST and Kroshinsky D: Use of
cyclosporine for the treatment of Stevens-Johnson syndrome/toxic
epidermal necrolysis. J Am Acad Dermatol. 85:512–513.
2021.PubMed/NCBI View Article : Google Scholar
|