Introduction
The liver is anatomically divided into eight
independent segments, each supplied by its own portal and hepatic
venous systems (1). Segment I (the
caudate lobe) is located between the ligamentum venosum and the
inferior vena cava. The middle hepatic vein separates the remaining
portion of the liver into right and left lobes. The right lobe
comprises segments V, VI, VII and VIII, while the left lobe
includes segments II, III and IV. The left lobe is further
subdivided by the umbilical fissure and falciform ligament into
lateral (segments II and III) and medial (IV, the quadrate lobe)
segments (2).
The hepatobiliary tree consists of both intrahepatic
ducts (IHDs) and extrahepatic ducts (EHDs). The intrahepatic
biliary system is formed by the right hepatic duct (RHD) and left
hepatic duct (LHD). The RHD arises from the confluence of the right
posterior duct (RPD), which drains segments VI and VII, and the
right anterior duct (RAD), which drains segments V and VIII.
Typically, the RPD follows a relatively horizontal course, whereas
the RAD is more vertically oriented. The LHD is formed by the
biliary ducts of segments II, III and IV. The RHD and LHD join to
form the common hepatic duct (CHD), which is then joined by the
cystic duct (CD) from the gallbladder. The CD most commonly inserts
into the middle third of the CHD on its right-lateral side, forming
the common bile duct (CBD). The CBD empties the main pancreatic
duct into the major duodenal papilla in the second part of the
duodenum (2-4).
This conventional biliary anatomy is present in 55-65% of the
general population worldwide (3-5).
Although anatomical variations of the IHD and CD
have been well described in other populations, such as Asian,
European and American, their prevalence within Middle Eastern
populations, as well as their interrelationship and clinical
significance with biliary conditions, such as gallstone disease,
cholecystitis and obstructive jaundice, remain insufficiently
explored. Importantly, previous studies (6-12)
have evaluated IHD and CD variations separately, with limited data
addressing their combined occurrence and impact on biliary
pathology. A thorough understanding of biliary anatomy is crucial
for anatomists, radiologists and surgeons, as unrecognized
variations can increase the risk of postoperative complications,
such as bile duct injury, biliary peritonitis, jaundice and sepsis
(2,5,13-17).
Therefore, the present study aimed to investigate the coexistence
of IHD and CD variations and evaluate their effect on biliary
pathology in a Middle Eastern population using magnetic resonance
cholangiopancreatography (MRCP).
Materials and methods
Study design and setting
The present retrospective, cross-sectional,
single-center, observational study included 259 patients who met
the following inclusion criteria: Referral for MRCP for a
biliary-related indication; adequate image quality allowing full
visualization of the biliary tree; and availability of complete
medical record at King Abdullah University Hospital (KAUH; Irbid,
Jordan), a tertiary referral center in Northern Jordan, between
January 2019 and December 2023. The mean age of the cohort was
48.2±18.0 years, and female patients comprised 44.0% of the cohort
(n=114/259). KAUH is a referral and teaching hospital affiliated
with Jordan University of Science and Technology, serving >3
million individuals across four governorates. The present study was
approved by the Institutional Review Board of Jordan University of
Science and Technology and KAUH (approval no. 10/163/2023; Irbid,
Jordan) and conducted in accordance with the principles of The
Declaration of Helsinki. Exclusion criteria included poor image
quality, insufficient visualization of the IHD or CD and incomplete
medical records.
Data collection
Demographic data, including age, sex and prior
diagnoses associated with the biliary system, such as the presence
of gallbladder or biliary tract stones, cholecystitis and
obstructive jaundice, were systematically extracted from the
hospital database. Patient data were accessed and extracted in
stages between September 2023 and May 2024. Clinical variables were
determined based on documented clinical diagnoses and imaging
findings, with relevant laboratory investigations reviewed when
necessary to support the diagnosis of biliary obstruction.
Imaging technique
All MRCP examinations were performed using a
standardized protocol on a 1.5-T MR system (Ingenia; Philips
Healthcare). The imaging parameters were as follows: Repetition
time of 401 msec, echo time of 80 msec, flip angle of 90 degrees
and field of view of 343x343 mm. Thick oblique coronal and axial
slices of ~8 mm interval were acquired during breath-hold. Patients
fasted for 6 h prior to the examination, and no intravenous or oral
contrast agents were administered. The protocol included three
sequences: The T2-weighted axial single-shot turbo spin-echo
sequences, T2-weighted spectral attenuated inversion recovery
coronal fast spin-echo sequences and 3D respiratory-triggered
heavily T2-weighted MRCP sequences. Furthermore, the heavily
T2-weighted thick-slab MRCP images, the axial and coronal source
images from the 3D respiratory-triggered heavily T2-weighted MRCP
sequences, and the maximum intensity projection images were
analyzed together to identify any possible anatomic variations. All
patients were scanned in the supine position. Scans with notable
technical limitations, such as poor image quality or incomplete
visualization of the biliary tree were excluded to maintain
diagnostic accuracy.
Image analysis
Two radiology residents independently assessed MRCP
images and documented the biliary tree anatomy, including the
presence of anatomical variants. The collected data were
classified, and cases with poor image quality were excluded.
Discrepancies were resolved by consensus with a senior consultant
radiologist. All evaluations were conducted using the Picture
Archiving and Communication System (PACS; Synapse PACS; FUJIFILM
Corporation). The type of IHD anatomy was classified according to
the system described by Huang et al (18). Conventional anatomy (type 1) was
specified as the RPD joining the posterior RAD to form the RHD,
which subsequently joins the LHD to form the CHD. Anatomical
variations were classified as follows: i) Type 2, when there was a
common confluence of the RPD, RAD and LHD (trifurcation); ii) type
3a, when the RPD drained into the LHD; iii) type 3b, when the RPD
drained into the CHD; and iv) type 4, when other variants of the
IHD were identified and sequentially numbered. Among these, a
single case in which two LHDs drained into the CHD was recorded
(Fig. 1A). The CD insertion into
the CHD was defined based on its circumferential association with
conventional anatomy as type 1, where the CD was inserted into the
CHD through the right-lateral aspect. Anatomical variations were
classified as follows: i) Type 2, when the CD coursed a distinctive
anterior spiral pattern to the CHD, thus leading to its insertion
into the left medial side of the CHD; and ii) type 3, when the CD
coursed a distinctive posterior spiral pattern to the CHD,
eventually resulting into its insertion into the left medial side
of the CHD (Fig. 1B).
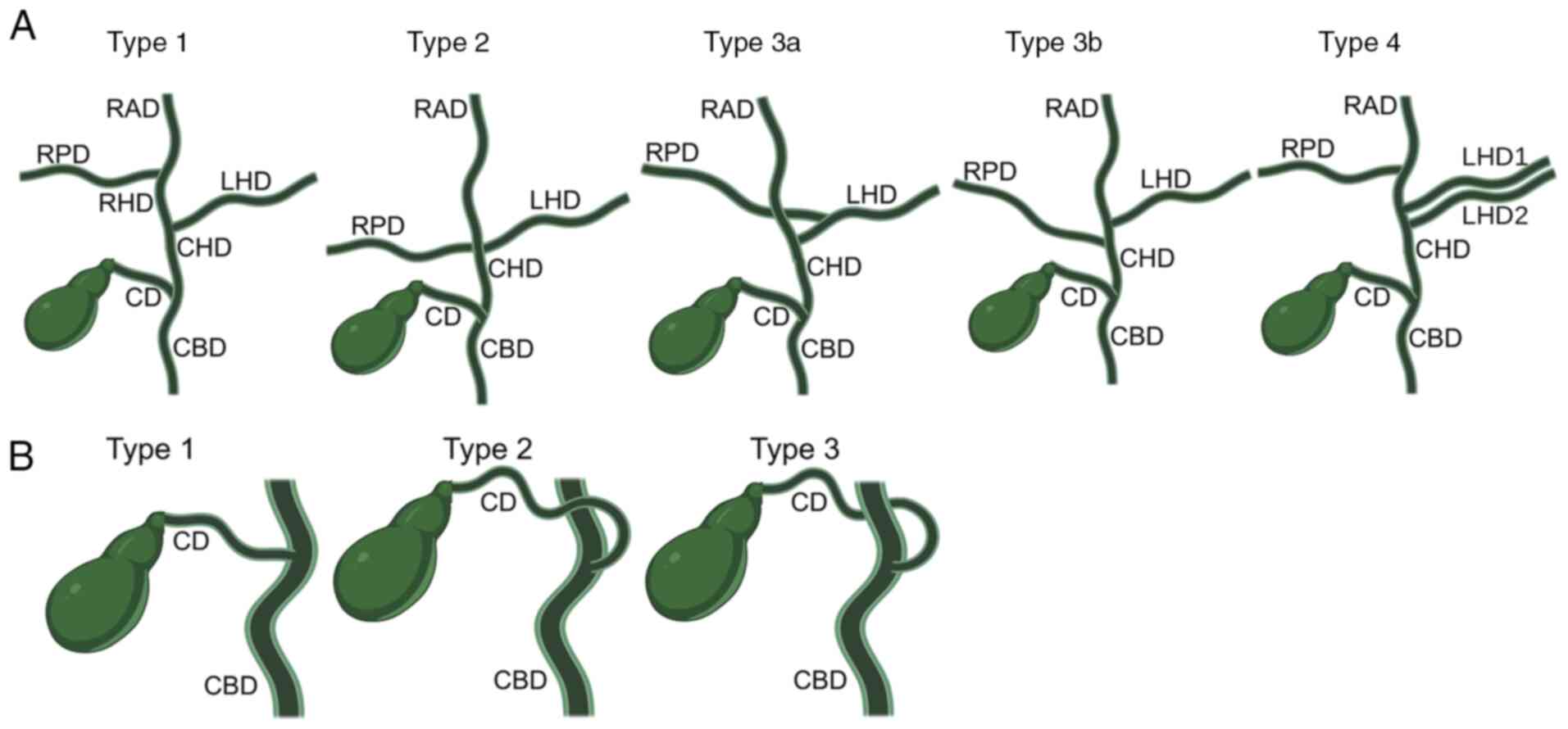 | Figure 1Schematic illustration of IHD and CD
anatomical variations. (A) IHD anatomical patterns: i) Type 1,
conventional anatomy, in which the RHD is formed by the confluence
of the RAD and RPD, and then joins the LHD to form the CHD; ii)
type 2, trifurcation pattern including the RAD, RPD and LHD; iii)
type 3a, the RPD drains into the LHD; iv) type 3b, the RPD drains
into the CHD; and v) type 4, presence of two LHDs draining into the
CHD. (B) CD anatomical patterns: i) Type 1, lateral insertion into
the CHD; ii) type 2, anterior spiral course with medial insertion
into the CHD; and iii) type 3, posterior spiral course with medial
insertion into the CHD. IHD, intrahepatic duct; CD, cystic duct;
RAD, right anterior duct; RPD, right posterior duct; RHD, right
hepatic duct; LHD, left hepatic duct; CHD, common hepatic duct;
CBD, common bile duct. Created with BioRender (https://www.biorender.com/). |
Statistical analysis
All statistical analyses were performed using Stata
16.0 (StataCorp LP). Continuous variables, such as age, are
presented as the mean ± SD and were compared across anatomical
groups using one-way ANOVA. Categorical variables, presented as
numbers and percentages, including sex, ductal variants, lithiasis,
cholecystitis and obstructive jaundice, were compared using
Fisher's exact test. Univariable logistic regression analyses were
carried out to identify factors associated with IHD variations and
uncommon CD variations. Candidate variables were selected a
priori based on demographic relevance, anatomical plausibility,
clinical significance and availability within the retrospective
MRCP dataset. Age and sex were retained as core demographic
covariates. Additional variables included the corresponding ductal
anatomical pattern, the composite ‘any biliary stone’,
cholecystitis and obstructive jaundice due to their clinical and
anatomical relevance. Effect estimates were reported as odds ratios
(ORs) and adjusted odds ratios (aORs) with 95% confidence intervals
(CIs). aORs were estimated using multivariable logistic regression
models adjusted for age, sex, the corresponding ductal anatomical
variation, any biliary stone, cholecystitis and obstructive
jaundice. Site-specific stone variables were excluded to avoid
structural collinearity with the composite variable ‘any biliary
stone’, which was retained as the primary indicator of biliary
lithiasis. Model adequacy was verified using the Hosmer-Lemeshow
test, and a two-sided P<0.05 was considered to indicate a
statistically significant difference.
Results
Branching patterns of the IHD
Conventional IHD anatomy (type 1) was observed in
61.4% of cases, whereas anatomical variants were recorded in 38.6%
of cases (type 2=22.0%, type 3a=7.7%, type 3b=8.5% and type 4=0.4%;
Fig. 2). The differences in the
study variables across IHD categories are summarized in Table I. Neither mean age nor sex
distribution differed significantly across IHD categories. By
contrast, CD anatomy was notably associated with the IHD pattern
(P<0.05). CD variants were only identified in 29.6% of type 1
cases, with ~50.0% of cases presenting with type 2 (49.1%) and type
3a (55.0%) configurations. Furthermore, anterior-spiral CD
insertion (CD type 2) was more common in IHD type 2 (28.1%),
whereas posterior-spiral insertion (CD type 3) predominated in IHD
type 3a (40.0%) (P<0.05 based on comparison across all CD
variation types; Table I), thus
indicating concordant developmental variation between IHD and EHD.
Biliary stone disease was present in 40.9% of patients but was not
associated with IHD pattern or other clinical variables (all
P>0.05). Specifically, age (P=0.900), sex (P=0.199), cystic duct
stones (P=0.201), CBD stones (P=0.283), gallbladder stones
(P=0.120), any biliary stone (P=0.052), cholecystitis (P=0.568) and
obstructive jaundice (P=0.174) did not differ significantly across
IHD categories (Table I).
Univariable and multivariable logistic regression analyses
identifying factors associated with IHD variations are listed in
Table II. CD variation was the
strongest predictor, doubling the odds of harboring an IHD variant
in univariable analysis (OR=2.20; 95% CI, 1.31-3.70; P=0.003) and
remained significant after adjustment for age, sex, any biliary
stone, cholecystitis and obstructive jaundice (aOR=1.95; 95% CI,
1.13-3.35; P=0.016). Consistently, the presence of any biliary
stone in the gallbladder, CD or CBD was also independently
associated with a ~2-fold increase in the odds of an IHD variant
(OR=1.97; 95% CI, 1.18-3.28; P=0.009; aOR=2.00; 95% CI, 1.16-3.46;
P=0.013). Age, sex, individual stone locations, cholecystitis and
obstructive jaundice were not significantly associated (all
P>0.05). Individual stone locations were not included in the
multivariable model due to collinearity with the composite variable
‘any biliary stone’.
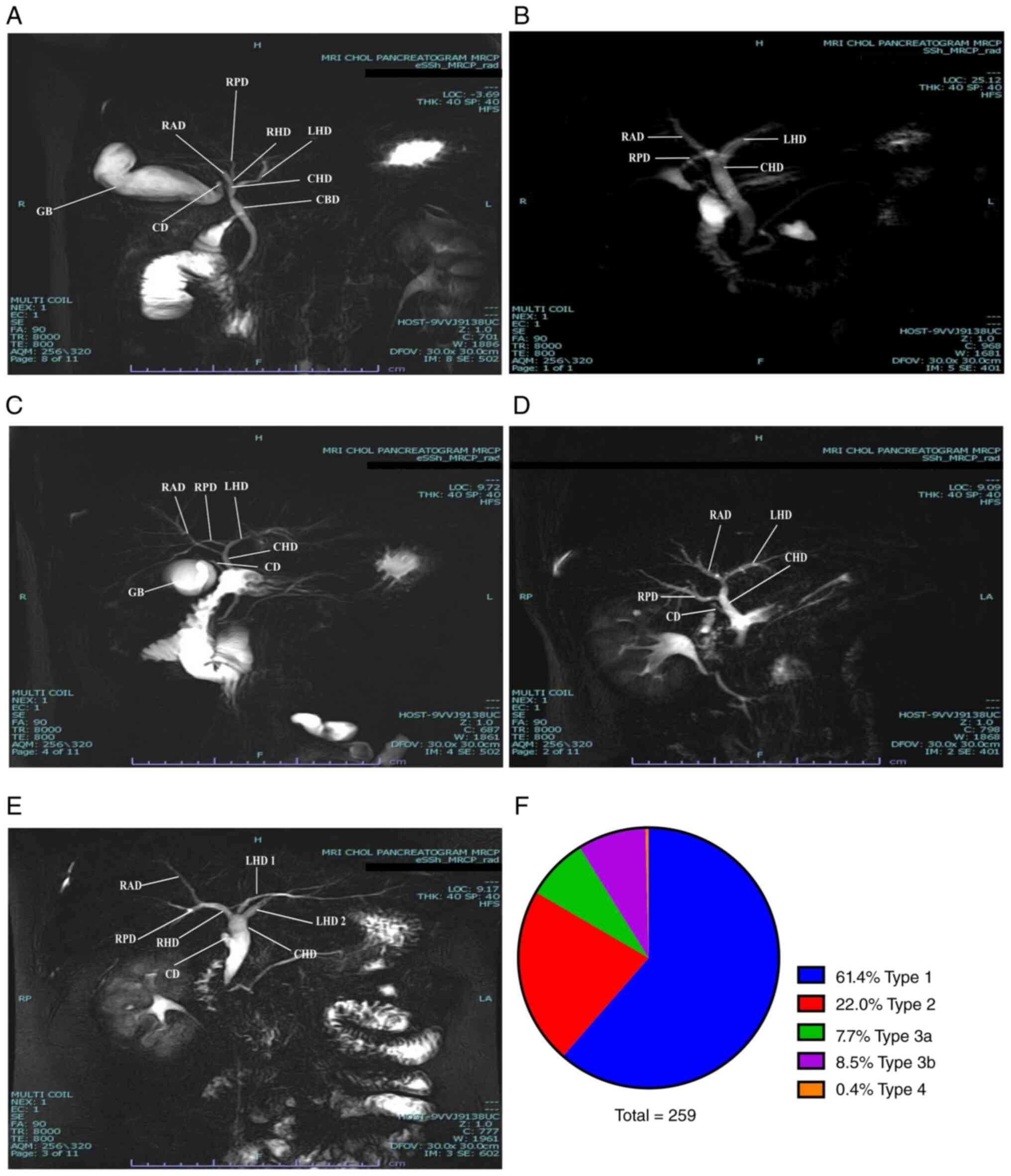 | Figure 2Representative magnetic resonance
cholangiopancreatography images showing IHD anatomical variation
patterns. (A) Type 1, the RAD and RPD form the RHD, which joins the
LHD to form the CHD. Furthermore, the CD inserts laterally into the
CHD (type 1 CD). (B) Type 2, trifurcation pattern involving the
RAD, RPD and LHD. (C) Type 3a, the RPD drains into the LHD. (D)
Type 3b, the RPD drains into the CHD. (E) Type 4, presence of two
LHDs draining into the CHD. (F) Distribution of IHD types (n=259).
IHD, intrahepatic duct; RAD, right anterior duct; RPD, right
posterior duct; RHD, right hepatic duct; LHD, left hepatic duct;
CHD, common hepatic duct; CD, cystic duct; GB, gallbladder; H,
head; F, feet; R, right; L, left; RP, right posterior; LA, left
anterior. |
 | Table IDifferences in the study variables
across intrahepatic duct types. |
Table I
Differences in the study variables
across intrahepatic duct types.
| Variable | Total (n=259) | Type 1 (n=159;
61.4%) | Type 2 (n=57;
22.0%) | Type 3a (n=20;
7.7%) | Type 3b (n=22;
8.5%) | Type 4 (n=1;
0.4%) | P-value |
|---|
| Age, years | 48.2±18.0 | 48.2±18.4 | 50.0±19.2 | 41.0±13.9 | 49.4±13.5 | 60.0±0.0 | 0.900 |
| Sex, n (%) | | | | | | | 0.199 |
|
Female | 114 (44.0) | 76 (47.8) | 18 (31.6) | 10 (50.0) | 10 (45.5) | 0 (0.0) | |
|
Male | 145 (56.0) | 83 (52.2) | 39 (68.4) | 10 (50.0) | 12 (54.5) | 1 (100.0) | |
| CD variation, n
(%) | | | | | | | 0.019 |
|
No | 164 (63.3) | 112 (70.4) | 29 (50.9) | 9 (45.0) | 13 (59.1) | 1 (100.0) | |
|
Yes | 95 (36.7) | 47 (29.6) | 28 (49.1) | 11 (55.0) | 9 (40.9) | 0 (0.0) | |
| CD variation type,
n (%) | | | | | | | 0.031 |
|
Type 1 | 164 (63.3) | 112 (70.4) | 29 (50.9) | 9 (45.0) | 13 (59.1) | 1 (100.0) | |
|
Type 2 | 46 (17.8) | 24 (15.1) | 16 (28.1) | 3 (15.0) | 3 (13.6) | 0 (0.0) | |
|
Type 3 | 49 (18.9) | 23 (14.5) | 12 (21.0) | 8 (40.0) | 6 (27.3) | 0 (0.0) | |
| CD stones, n
(%) | | | | | | | 0.201 |
|
No | 255 (98.5) | 157 (98.7) | 57 (100.0) | 19 (95.0) | 21 (95.5) | 1 (100.0) | |
|
Yes | 4 (1.5) | 2 (1.3) | 0 (0.0) | 1 (5.0) | 1 (4.5) | 0 (0.0) | |
| CBD stones, n
(%) | | | | | | | 0.283 |
|
No | 225 (86.9) | 143 (89.9) | 45 (78.9) | 17 (85.0) | 19 (86.4) | 1 (100.0) | |
|
Yes | 34 (13.1) | 16 (10.1) | 12 (21.1) | 3 (15.0) | 3 (13.6) | 0 (0.0) | |
| Gallbladder stones,
n (%) | | | | | | | 0.120 |
|
No | 168 (64.9) | 110 (69.2) | 30 (52.6) | 13 (65.0) | 15 (68.2) | 0 (0.0) | |
|
Yes | 91 (35.1) | 49 (30.8) | 27 (47.4) | 7 (35.0) | 7 (31.8) | 1 (100.0) | |
| Any biliary stone,
n (%) | | | | | | | 0.052 |
|
No | 153 (59.1) | 104 (65.4) | 26 (45.6) | 11 (55.0) | 12 (54.5) | 0 (0.0) | |
|
Yes | 106 (40.9) | 55 (34.6) | 31 (54.4) | 9 (45.0) | 10 (45.5) | 1 (100.0) | |
| Cholecystitis, n
(%) | | | | | | | 0.568 |
|
No | 253 (97.7) | 156 (98.1) | 55 (96.5) | 19 (95.0) | 22 (100.0) | 1 (100.0) | |
|
Yes | 6 (2.3) | 3 (1.9) | 2 (3.5) | 1 (5.0) | 0 (0.0) | 0 (0.0) | |
| Obstructive
jaundice, n (%) | | | | | | | 0.174 |
|
No | 138 (53.3) | 83 (52.2) | 26 (45.6) | 12 (60.0) | 16 (72.7) | 1 (100.0) | |
|
Yes | 121 (46.7) | 76 (47.8) | 31 (54.4) | 8 (40.0) | 6 (27.3) | 0 (0.0) | |
| Table IIFactors associated with the presence
of IHD variation (IHD types 2, 3a, 3b and 4). |
Table II
Factors associated with the presence
of IHD variation (IHD types 2, 3a, 3b and 4).
| | Univariable
regression | Multivariable
regression |
|---|
| Variable | OR (95% CI) | P-value | aOR (95% CI) | P-value |
|---|
| Age | 1.00 (0.99,
1.01) | 0.980 | 1.00 (0.98,
1.01) | 0.688 |
| Female (vs.
male) | 0.67 (0.40,
1.11) | 0.123 | 0.67 (0.39,
1.14) | 0.142 |
| CD variation
(present vs. absent) | 2.20 (1.31,
3.70) | 0.003 | 1.95 (1.13,
3.35) | 0.016 |
| CD
stonesa (present vs.
absent) | 1.60 (0.22,
11.56) | 0.640 | - | - |
| CBD
stonesa (present vs.
absent) | 1.96 (0.95,
4.06) | 0.069 | - | - |
| Gallbladder
stonesa (present vs.
absent) | 1.63 (0.97,
2.74) | 0.067 | - | - |
| Any biliary stone
(present vs. absent) | 1.97 (1.18,
3.28) | 0.009 | 2.00 (1.16,
3.46) | 0.013 |
| Cholecystitis
(present vs. absent) | 1.61 (0.32,
8.13) | 0.565 | 0.85 (0.15,
4.89) | 0.860 |
| Obstructive
jaundice (present vs. absent) | 0.89 (0.54,
1.48) | 0.70 | 0.73 (0.42,
1.24) | 0.242 |
Anatomical variations of CD insertion
into the CBD
Conventional CD right-lateral insertion (type 1) was
observed in 63.3% (n=164) of all cases (Fig. 2A), whereas CD variants were
identified in 36.7%, including anterior spiral (type 2, 17.8%) and
posterior spiral patterns (type 3, 18.9%) (Fig. 3). As shown in Table III, age did not differ
significantly across CD patterns (P=0.680), and although female
patients were less common among spiral variants, this difference
did not reach statistical significance (P=0.077). Furthermore, a
significant association between the IHD and EHD anatomy was
evident. Particularly, IHD variants were present in approximately
one-third of patients with conventional right-lateral CD insertion
(type 1, 31.7%), compared with roughly half of patients with
anterior (type 2, 47.8%) or posterior (type 3, 53.1%) spiral
variants (P=0.010). Consistently, CD pathology followed the same
hierarchy, with posterior spiral CD variants showing the highest
prevalence of CD stones (P=0.047). However, it should be noted that
the vast majority of patients were negative for CD stones (98.5%;
255/259), and the observed P-value should be interpreted with
caution given its borderline significance. The composite variable
‘any biliary stone’ increased step-wise from 34.8% in type 1 to
47.8% in type 2 and 55.1% in type 3 (P=0.022). A similar trend was
found for cholecystitis (0.6 vs. 4.4 vs. 6.1%; P=0.039). However,
it should be noted that the vast majority of patients were negative
for cholecystitis (97.7%; 253/259), and these findings should
therefore be interpreted with caution. By contrast, CBD stones and
obstructive jaundice were not significantly associated with CD
orientation (P=0.898 and P=0.179, respectively). These results
suggested that spiral (medial) CD variants were associated with
both IHD variations and a higher risk of lithiasis and
cholecystitis. Univariable and multivariable logistic regression
analyses were performed to identify factors associated with the
presence of uncommon CD variants (spiral insertions; types 2 and
3). As shown in Table IV, IHD
variation was the strongest independent variable associated with CD
variants (OR=2.20; 95% CI, 1.31-3.70; P=0.003), and remained
significant after adjustment for age, sex, any biliary stone,
cholecystitis and obstructive jaundice (aOR=1.95; 95 % CI,
1.14-3.35; P=0.015). Similarly, the presence of lithiasis was also
independently associated with spiral CD variants (OR=2.00; 95% CI,
1.19-3.35; P=0.008; aOR=1.79; 95% CI, 1.03-3.12; P=0.041). In
addition, female sex showed a modest protective effect against
uncommon CD variants in the univariable analysis (OR=0.59; 95% CI,
0.35-0.98; P=0.043). However, this association was not retained
after adjustment (aOR=0.60; 95% CI, 0.35-1.04; P=0.070).
Cholecystitis exhibited a univariable association, although the
wide 95% CI (1.04-78.71) and borderline P-value (P=0.046) indicate
that this result should be interpreted with caution (OR=9.06; 95%
CI, 1.04-78.71; P=0.046), but was attenuated in the multivariable
model (aOR=8.31; 95% CI, 0.88-78.02; P=0.064). Age, site-specific
stone location and obstructive jaundice were not significantly
associated with spiral CD insertions (all P>0.05). Notably,
gallbladder stone showed a significant association in the
univariable analysis (OR=1.86; 95% CI, 1.10-3.14; P=0.021);
however, site-specific stone variables were excluded from the
multivariable model due to collinearity with the composite variable
‘any biliary stone’.
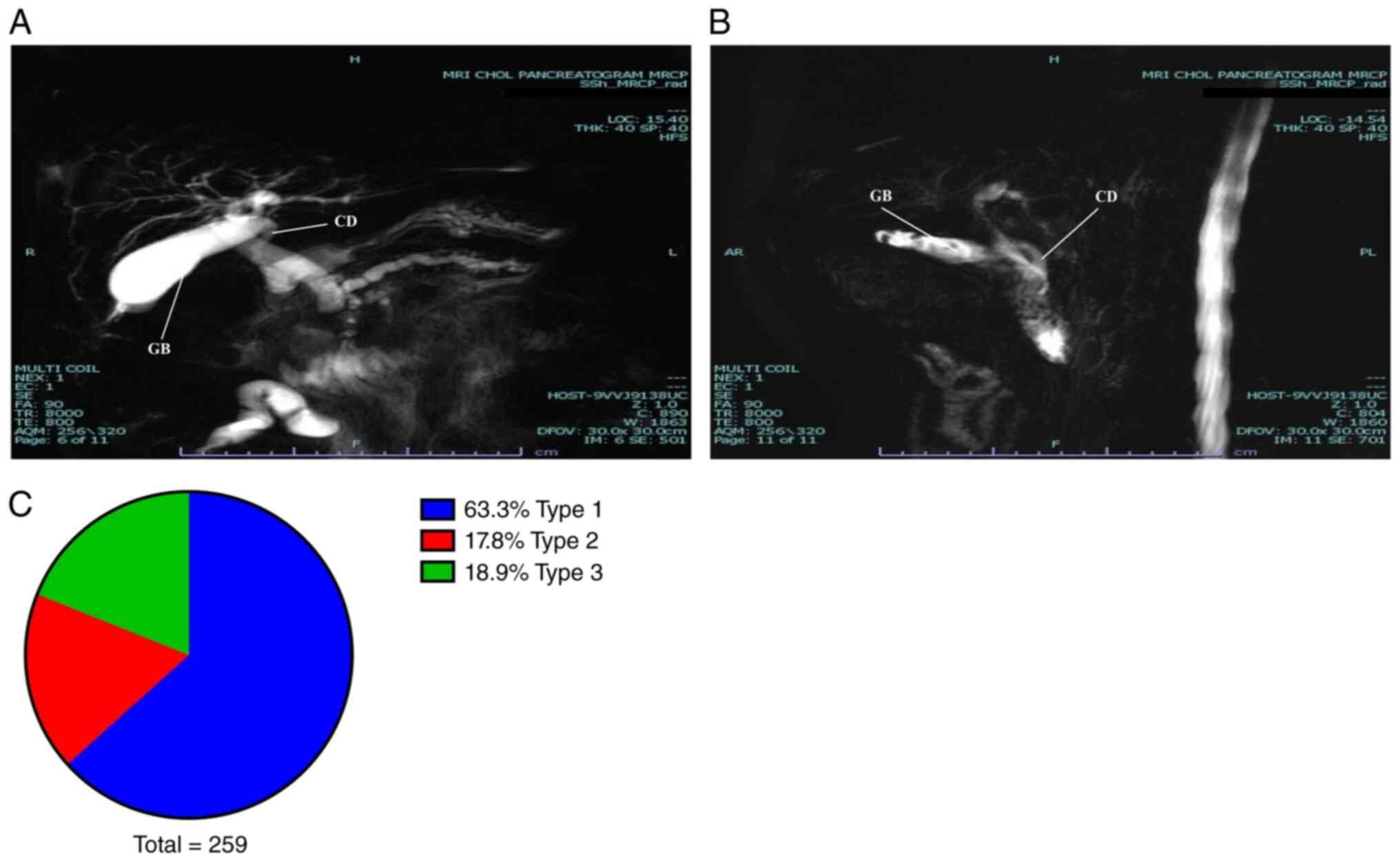 | Figure 3Representative magnetic resonance
cholangiopancreatography images showing CD anatomical variation
patterns. (A) Type 2, anterior spiral course with medial insertion
into the CHD. (B) Type 3, posterior spiral course with medial
insertion into the CHD. (C) Distribution of CD anatomical types
(n=259). CD, cystic duct; CHD, common hepatic bile duct; GB,
gallbladder; H, head; F, feet; R, right; L, left; AR, anterior
right; PL, posterior left. |
| Table IIIDifferences in the study variables
across CD types. |
Table III
Differences in the study variables
across CD types.
| Variable | Total (n=259) | Type 1 (n=164;
63.3%) | Type 2 (n=46;
17.8%) | Type 3 (n=49;
18.9%) | P-value |
|---|
| Age, years | 48.2±18.0 | 47.9±17.3 | 48.4±16.4 | 49.0±21.6 | 0.680 |
| Sex, n (%) | | | | | 0.077 |
|
Female | 114 (44.0) | 80 (48.8) | 14 (30.4) | 20 (40.8) | |
|
Male | 145 (56.0) | 84 (51.2) | 32 (69.6) | 29 (59.2) | |
| IHD variation, n
(%) | | | | | 0.010 |
|
No | 159 (61.4) | 112 (68.3) | 24 (52.2) | 23 (46.9) | |
|
Yes | 100 (38.6) | 52 (31.7) | 22 (47.8) | 26 (53.1) | |
| IHD variation type,
n (%) | | | | | 0.031 |
|
Type 1 | 159 (61.4) | 112 (68.3) | 24 (52.2) | 23 (46.9) | |
|
Type 2 | 57 (22.0) | 29 (17.7) | 16 (34.8) | 12 (24.5) | |
|
Type 3a | 20 (7.7) | 9 (5.5) | 3 (6.5) | 8 (16.3) | |
|
Type 3b | 22 (8.5) | 13 (7.9) | 3 (6.5) | 6 (12.3) | |
|
Type 4 | 1 (0.4) | 1 (0.6) | 0 (0.0) | 0 (0.0) | |
| CD stones, n
(%) | | | | | 0.047 |
|
No | 255 (98.5) | 163 (99.4) | 46 (100.0) | 46 (93.9) | |
|
Yes | 4 (1.5) | 1 (0.6) | 0 (0.0) | 3 (6.1) | |
| CBD stones, n
(%) | | | | | 0.898 |
|
No | 225 (86.9) | 142 (86.6) | 41 (89.1) | 42 (85.7) | |
|
Yes | 34 (13.1) | 22 (13.4) | 5 (10.9) | 7 (14.3) | |
| Gallbladder stones,
n (%) | | | | | 0.066 |
|
No | 168 (64.9) | 115 (70.1) | 26 (56.5) | 27 (55.1) | |
|
Yes | 91 (35.1) | 49 (29.9) | 20 (43.5) | 22 (44.9) | |
| Any biliary stone,
n (%) | | | | | 0.022 |
|
No | 153 (59.1) | 107 (65.2) | 24 (52.2) | 22 (44.9) | |
|
Yes | 106 (40.9) | 57 (34.8) | 22 (47.8) | 27 (55.1) | |
| Cholecystitis, n
(%) | | | | | 0.039 |
|
No | 253 (97.7) | 163 (99.4) | 44 (95.7) | 46 (93.9) | |
|
Yes | 6 (2.3) | 1 (0.6) | 2 (4.3) | 3 (6.1) | |
| Obstructive
jaundice, n (%) | | | | | 0.179 |
|
No | 138 (53.3) | 90 (54.9) | 19 (41.3) | 29 (59.2) | |
|
Yes | 121 (46.7) | 74 (45.1) | 27 (58.7) | 20 (40.8) | |
| Table IVFactors associated with the presence
of uncommon CD variation (CD variation types 2 and 3). |
Table IV
Factors associated with the presence
of uncommon CD variation (CD variation types 2 and 3).
| | Univariable
regression | Multivariable
regression |
|---|
| Variable | OR (95% CI) | P-value | aOR (95% CI) | P-value |
|---|
| Age | 1 (0.99, 1.02) | 0.723 | 1 (0.99, 1.02) | 0.817 |
| Female (vs.
male) | 0.59 (0.35,
0.98) | 0.043 | 0.6 (0.35,
1.04) | 0.070 |
| IHD variation
(present vs. absent) | 2.2 (1.31,
3.7) | 0.003 | 1.95 (1.14,
3.35) | 0.015 |
| CD
stonesa (present vs.
absent) | 5.32 (0.54,
51.84) | 0.151 | - | - |
| CBD
stonesa (present vs.
absent) | 0.93 (0.44,
1.98) | 0.857 | - | - |
| Gallbladder
stonesa (present vs.
absent) | 1.86 (1.1,
3.14) | 0.021 | - | - |
| Any biliary stone
(present vs. absent) | 2 (1.19, 3.35) | 0.008 | 1.79 (1.03,
3.12) | 0.041 |
| Cholecystitis
(present vs. absent) | 9.06 (1.04,
78.71) | 0.046 | 8.31 (0.88,
78.02) | 0.064 |
| Obstructive
jaundice (present vs. absent) | 1.19 (0.72,
1.98) | 0.499 | 1.06 (0.62,
1.83) | 0.832 |
Discussion
The present study investigated the prevalence and
clinical associations of biliary ductal anatomical variations in a
Jordanian population using MRCP. Conventional IHD anatomy (type 1)
was observed in 61.4% of cases, whereas 38.6% exhibited variant
branching patterns. Consistently, the right-lateral CD insertion
(type 1) was present in 63.3% of patients, while medial insertions
accounted for 36.7%. A significant association between IHD and CD
variations was identified, thus indicating a potentially
coordinated developmental association. Compared with the majority
of previous studies (6-12)
that had evaluated these anatomical systems independently, in the
present study a combined analysis of IHD and CD variations was
performed, which demonstrated a statistically significant
interrelationship. Furthermore, variant CD insertions were
associated with a higher prevalence of biliary lithiasis and
cholecystitis, highlighting their clinical relevance. These
findings extended prior work, such as that by Renzulli et al
(19) by confirming the coexistence
of IHD and CD variations and further highlighting the clinical
relevance of CD variations. Whereas Renzulli et al focused
primarily on IHD anatomy with EHD as a secondary aim, the present
study specifically characterized CD insertion variants as the
primary outcome and their independent clinical predictors using
multivariable analysis. In addition, the present study is the first
to evaluate these associations in a Middle Eastern population,
directly addressing the limitation acknowledged by Renzulli et
al regarding the generalizability of their findings beyond an
almost exclusively European series from a single Italian center. A
comprehensive understanding of biliary anatomy is essential for
accurate preoperative planning and for minimizing complications
during hepatobiliary procedures (2,20). It
has been reported that anatomical variations can increase the risk
of bile duct injury during laparoscopic cholecystectomy, with an
incidence of 0.5-1.7% as reported across multiple international
studies (14,15,21),
thus resulting in severe complications, including jaundice, biliary
peritonitis, sepsis and secondary biliary cirrhosis (16,17).
Certain IHD variations carry important surgical implications. The
trifurcation pattern (type 2), in which the RPD, RAD and LHD share
a common confluence point, is considered a contraindication for
safe right hepatectomy in living donor liver transplantation, as it
necessitates additional biliary anastomoses in the recipient,
increasing the risk of postoperative biliary complications
(22). The type 3a IHD variant, in
which the RPD drains into the LHD, are important, as they can
complicate liver transplantation and increase donor risk (22). Unrecognized type 3a anatomy during
left hepatectomy can also result in bile leakage, biliary stasis,
recurrent infections or cirrhosis due to RPD transection or
ligation (9). A previous study
demonstrated that in percutaneous transhepatic drainage,
obstruction of the LHD could lead to cholestasis in the right
posterior lobe (7). Therefore,
particular variants, such as types 2 and 3a, are considered
relative contraindications for liver donation in some centers
(22,23).
Several classification systems have described IHD
variations (24). In the present
study, the Huang classification (18) was adopted due to its simplicity and
clinical applicability. The prevalence of conventional anatomy
varies across populations, with higher rates reported in Asian
populations (~65%) compared with European and American ones (~60%)
(25). Consistent with prior
studies (7,9,18,19,22,24,26-28),
in the present study no significant sex-based differences were
observed, although certain reports suggested a higher prevalence of
IHD variants among women (25,29).
The proportion of conventional IHD anatomy in the
current study (61.4%) lied within the range reported in the
literature (41.0-87.0%) (5-9,11,12,19,20,25-27,29-42).
The most common variation was type 2 trifurcation (22.0%), although
its prevalence varied widely in previous studies (3.0-44.0%)
(5,19,25,27,30,37,40,42).
Types 3a and 3b occurred in 7.7 and 8.5% of cases, respectively,
which were also within previously reported ranges (2.2-27.8% and
1.5-10%, respectively) (5-9,11,12,19,20,25-27,29-42).
A rare variant involving draining of two separate LHDs into the CHD
was identified in one case (0.4%), which was consistent with prior
reports of low prevalence of this variant (0.2-2.4%) (7,20,27,30,40).
Other rare variations, such as drainage of the RPD or RHD into the
CD, or the presence of accessory hepatic ducts, which have been
reported in previous studies (5-8,20,26,27,30-32,34,37,40),
were not observed in the present study.
A key finding of the present study was the strong
association between CD insertion patterns and IHD variations, an
observation that has been previously noted (19). For example, type 2 CD insertion was
most commonly associated with type 2 IHD, while type 3 CD
frequently co-occurred with type 3a IHD. Preoperative
identification of EHD anatomy could therefore help anticipate
corresponding variations in IHD. The aforementioned association
could likely reflect a shared embryologic origin from the hepatic
diverticulum, where the pars hepatica forms the IHD, while the pars
cystica gives rise to the CD, CBD and gallbladder (43). Disruptions in this developmental
process could account for the concurrent occurrence of variations
in both systems (19,43,44).
By contrast, CD anatomy lacks a standardized
classification system (10).
Existing studies have described CD variants using descriptive
anatomical classifications and imaging-based approaches that
categorize variations by insertion site, course and morphology
(6,10,11,23,45,46).
These descriptive and imaging-based strategies collectively
highlight the heterogeneity in the characterization of CD
variations. Therefore, the present study employed a simplified
MRCP-based classification system focusing on insertion patterns and
course, as these features are consistently identifiable and
clinically relevant. The distinction between conventional lateral
insertion and medial spiral insertions represents a well-reported
and clinically important pattern across MRCP-based studies
(6,10,11,46-48).
In contrast to existing systems that variably emphasize insertion
level, duct length or complex morphological configurations, the
present classification focused on parameters consistently
visualized on MRCP and directly applicable to surgical planning and
radiological reporting. Specifically, classification according to
CD insertion pattern and course enables consistent identification
and reporting of anatomical variants on MRCP. For example,
recognition of anterior or posterior spiral CD insertion can be
explicitly communicated in radiological reports and considered
during preoperative assessment, thereby improving awareness of
atypical biliary anatomy and facilitating surgical planning for
hepatobiliary procedures. Accordingly, the current classification
was intended as a pragmatic and reproducible reporting framework
aligned with routine MRCP practice, rather than as a substitute for
more comprehensive anatomical classification systems.
CD variations are considered to arise from
embryologic malrotation during duodenal development, resulting in
anterior or posterior spiral courses around the CHD (49). In the present study, conventional CD
anatomy was observed in 63.3% of cases, slightly lower than rates
reported in previous studies (76.1-89%) (6,10,11,46).
These variants can increase the risk of bile duct injury and
intraoperative bile leakage during laparoscopic cholecystectomy
(50).
Although IHD variations were not directly associated
with specific clinical conditions, they frequently co-occurred with
atypical CD insertions. Spiral CD variants, particularly posterior
types, were more commonly associated with biliary stones and
inflammation, potentially due to impaired bile flow and stasis
(10,51). Multivariable analysis revealed that
both IHD variations and biliary stones independently predicted CD
variants, while CD variants were strongly associated with IHD
variations. These findings supported the interrelationship between
intrahepatic and extrahepatic biliary anatomy and their combined
contribution to disease pathology.
The observed association between CD variations,
biliary lithiasis and cholecystitis further supports the clinical
importance of recognizing biliary anatomical variants during
preoperative evaluation. From a practical perspective, current
evidence supports a selective rather than routine application of
MRCP prior to cholecystectomy. The American Society for
Gastrointestinal Endoscopy guidelines (52) advocate a risk-stratified approach,
categorizing patients into low-, intermediate- and high-probability
groups for CBD stones. To verify the diagnosis, the American
Society for Gastrointestinal Endoscopy recommends that patients
with an intermediate risk (10-50%) of choledocholithiasis should
undergo endoscopic ultrasound or MRCP (53). A subsequent study further supported
this strategy, suggesting that intermediate-risk classification
could guide the use of additional imaging, including MRCP or
endoscopic ultrasound, rather than performing routine imaging in
all patients (53). Furthermore,
the American Society for Gastrointestinal Endoscopy guidelines have
been associated with a reduced number of unnecessary diagnostic
endoscopic retrograde cholangiopancreatographies, thus minimizing
procedure-related complications (52,53).
Particularly, identification of CD variations or complex biliary
anatomy is clinically important, as it can alert the surgeon to an
increased risk of misidentification and warrant a more cautious
dissection strategy. When anatomical variation is identified or
suspected, a cautious operative approach is essential (54), involving careful dissection to
achieve the critical view of safety; a method of target
identification requiring: Clearance of the hepatocystic triangle of
fat and fibrous tissue, separation of the lower third of the
gallbladder from the cystic plate, and confirmation that only the
CD and cystic artery remain attached to the gallbladder before
clipping and division (54). When
these criteria cannot be safely met, bail-out strategies such as
subtotal fenestrating cholecystectomy should be employed, and
intraoperative imaging considered when anatomy remains unclear, as
part of a broader strategy to improve operative safety (54). Given that EHD and IHD variants may
coexist, identification of any variation should prompt a systematic
search for additional ductal variations (19). In this context, preoperative
identification of complex biliary anatomy should be incorporated
into patient counseling, informed consent and operative planning
for possible intraoperative imaging or endoscopic procedures.
The present study has several limitations. Firstly,
its retrospective, cross-sectional design limits inference of
causal relationships between biliary anatomical variations and
associated clinical conditions. In addition, several potential
confounders, including body mass index, metabolic syndrome,
diabetes, dyslipidemia and medication history, were not
consistently available in the present retrospective imaging-based
study and therefore could not be included in the multivariable
analyses. Consequently, the aORs should be interpreted as
associations adjusted for the available demographic, anatomical and
radiological variables, rather than as fully adjusted causal
estimates accounting for all metabolic or systemic clinical risk
factors. Furthermore, the single-center design could limit the
generalizability of the results, as the study population was
derived from a tertiary referral center that typically manages more
complex or symptomatic cases. This could introduce referral bias,
potentially leading to an overrepresentation of patients with
biliary pathology compared with the general population. Consistent
with this possibility, the relatively high prevalence of biliary
stones (40.9%) likely reflects selection bias, given that MRCP is
more commonly performed in patients with suspected biliary disease
rather than in asymptomatic individuals. Consequently, the observed
associations between anatomical variations and biliary pathology
could be overestimated and should therefore be interpreted with
caution. Additionally, patients referred for MRCP may not
accurately reflect the true distribution of biliary anatomical
variations in the general population. Therefore, future multicenter
prospective studies, including more representative populations, are
needed to externally validate these findings. Lastly, although MRCP
is a reliable, non-invasive imaging tool for evaluation of the
biliary system, its spatial resolution can occasionally fail to
identify rare anatomical variations.
In conclusion, IHD and CD variations are common and
strongly associated, supporting a shared developmental origin.
Their identification is of clinical importance for surgical
planning and risk stratification, particularly given the
association of CD variants with biliary lithiasis and inflammation.
Identification of a variation in one component should prompt
careful evaluation for concurrent variations in the other. Patients
with such variations may also benefit from closer monitoring due to
their potentially increased susceptibility to stone formation and
cholecystitis.
Acknowledgements
Not applicable.
Funding
Funding: This present study was supported by Jordan University
of Science and Technology, Deanship of Research (grant no.
484-2023).
Availability of data and materials
The data generated in the present study may be
requested from the corresponding author.
Authors' contributions
WM and NO contributed to the conceptualization and
design of the study. WM, NO, AA and HAJ wrote the manuscript. Image
acquisition and analysis were performed by AM, AAD, HAJ and NO.
Data analysis and interpretation were carried out by WM, AA and SM.
WM and NO confirm the authenticity of all the raw data. All authors
read and approved the final manuscript.
Ethics approval and consent to
participate
The present study was approved by the Institutional
Review Board of Jordan University of Science and Technology and
KAUH (approval no. 10/163/2023). The study adhered to all
applicable national regulations and institutional policies
regarding human research and was conducted in accordance with the
ethical principles outlined in The Declaration of Helsinki. The
Institutional Review Board waived the requirement for informed
consent due to the retrospective design of the study, as all
personal identifiers were removed to ensure that no patient could
be identified, either directly or indirectly.
Patient consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Gazelle GS, Lee MJ and Mueller PR:
Cholangiographic segmental anatomy of the liver. Radiographics.
14:1005–1013. 1994.PubMed/NCBI View Article : Google Scholar
|
|
2
|
Mortelé KJ and Ros PR: Anatomic variants
of the biliary tree: MR cholangiographic findings and clinical
applications. AJR Am J Roentgenol. 177:389–394. 2001.PubMed/NCBI View Article : Google Scholar
|
|
3
|
Mortelé KJ, Rocha TC, Streeter JL and
Taylor AJ: Multimodality imaging of pancreatic and biliary
congenital anomalies. Radiographics. 26:715–731. 2006.PubMed/NCBI View Article : Google Scholar
|
|
4
|
Turner MA and Fulcher AS: The cystic duct:
Normal anatomy and disease processes. Radiographics. 21:3–22,
288-294. 2001.PubMed/NCBI View Article : Google Scholar
|
|
5
|
Nayman A, Özbek O, Erol S, Karakuş H and
Kaya HE: Magnetic resonance cholangiopancreatography evaluation of
intrahepatic bile duct variations with updated classification.
Diagn Interv Radiol. 22:489–494. 2016.PubMed/NCBI View Article : Google Scholar
|
|
6
|
Aljiffry M, Abbas M, Wazzan MAM,
Abduljabbar AH, Aloufi S and Aljahdli E: Biliary anatomy and
pancreatic duct variations: A cross-sectional study. Saudi J
Gastroenterol. 26:188–193. 2020.PubMed/NCBI View Article : Google Scholar : (Epub ahead of
print).
|
|
7
|
Li X, Duan R, He Y, Qin J, Liu R, Dai S,
Zhou J, Zeng X, Duan J, Gao P, et al: Application of
three-dimensional visualization technology in the anatomical
variations of hilar bile ducts in Chinese population. Front Surg.
9(934183)2022.PubMed/NCBI View Article : Google Scholar
|
|
8
|
Shrestha P, Mansur DI, Karki S, Shrestha
S, Maskey S and Chaudary R: Atypical pattern of the intrahepatic
biliary duct on magnetic resonance cholangiopancreatography in a
tertiary care centre: A descriptive cross-sectional study. JNMA J
Nepal Med Assoc. 60:955–958. 2022.PubMed/NCBI View Article : Google Scholar
|
|
9
|
Cawich SO, Sinanan A, Deshpande RR,
Gardner MT, Pearce NW and Naraynsingh V: Anatomic variations of the
intra-hepatic biliary tree in the Caribbean: A systematic review.
World J Gastrointest Endosc. 13:170–183. 2021.PubMed/NCBI View Article : Google Scholar
|
|
10
|
Zhu JH, Zhao SL, Kang Q, Zhu Y, Liu LX and
Zou H: Classification of anatomical morphology of cystic duct and
its association with gallstone. World J Gastrointest Surg.
16:307–317. 2024.PubMed/NCBI View Article : Google Scholar
|
|
11
|
Vidal V, Hardwigsen J, Jacquier A, Le
Corroller T, Gaubert JY, Moulin G, Bartoli JM, Petit P and
Champsaur P: Anatomic variants of the biliary tree with MR
cholangiography: Feasibility and surgical applications. J Chir
(Paris). 144:505–507. 2007.PubMed/NCBI View Article : Google Scholar : (In French).
|
|
12
|
Sirvanci M, Duran C, Ozturk E, Balci D,
Dayangaç M, Onat L, Yüzer Y, Tokat Y and Killi R: The value of
magnetic resonance cholangiography in the preoperative assessment
of living liver donors. Clin Imaging. 31:401–405. 2007.PubMed/NCBI View Article : Google Scholar
|
|
13
|
Varotti G, Gondolesi GE, Goldman J, Wayne
M, Florman SS, Schwartz ME, Miller CM and Sukru E: Anatomic
variations in right liver living donors1. J Am Coll Surg.
198:577–582. 2004.
|
|
14
|
Ishii H, Noguchi A, Fukami T, Sugimoto R,
Tada H, Takeshita H, Umehara S, Izumi H, Tani N, Yamaguchi M and
Yamane T: Preoperative evaluation of accessory hepatic ducts by
drip infusion cholangiography with CT. BMC Surg.
17(52)2017.PubMed/NCBI View Article : Google Scholar
|
|
15
|
Perini RF, Uflacker R, Cunningham JT,
Selby JB and Adams D: Isolated right segmental hepatic duct injury
following laparoscopic cholecystectomy. Cardiovasc Intervent
Radiol. 28:185–195. 2005.PubMed/NCBI View Article : Google Scholar
|
|
16
|
Keulemans YC, Bergman JJ, de Wit LT, Rauws
EA, Huibregtse K, Tytgat GN and Gouma DJ: Improvement in the
management of bile duct injuries? J Am Coll Surg. 187:246–254.
1998.PubMed/NCBI View Article : Google Scholar
|
|
17
|
Connor S and Garden OJ: Bile duct injury
in the era of laparoscopic cholecystectomy. Br J Surg. 93:158–168.
2006.PubMed/NCBI View
Article : Google Scholar
|
|
18
|
Huang TL, Cheng YF, Chen CL, Chen TY and
Lee TY: Variants of the bile ducts: Clinical application in the
potential donor of living-related hepatic transplantation.
Transplant Proc. 28:1699–1670. 1996.PubMed/NCBI
|
|
19
|
Renzulli M, Brandi N, Brocchi S, Balacchi
C, Lanza C, Pettinari I, Stefanini B, Carrafiello G, Piscaglia F,
Golfieri R and Marasco G: Association between anatomic variations
of extrahepatic and intrahepatic bile ducts: Do look up! J. Anat.
242:683–694. 2023.PubMed/NCBI View Article : Google Scholar
|
|
20
|
Sharma V, Saraswat VA, Baijal SS and
Choudhuri G: Anatomic variations in intrahepatic bile ducts in a
north Indian population. J Gastroenterol Hepatol. 23:e58–e62.
2008.PubMed/NCBI View Article : Google Scholar
|
|
21
|
Nijssen MAJ, Schreinemakers JMJ, Meyer Z,
Van Der Schelling GP, Crolla RMPH and Rijken AM: Complications
after laparoscopic cholecystectomy: A video evaluation study of
whether the critical view of safety was reached. World J Surg.
39:1798–1803. 2015.PubMed/NCBI View Article : Google Scholar
|
|
22
|
Catalano OA, Singh AH, Uppot RN, Hahn PF,
Ferrone CR and Sahani DV: Vascular and biliary variants in the
liver: Implications for liver surgery. Radiographics. 28:359–378.
2008.PubMed/NCBI View Article : Google Scholar
|
|
23
|
Hyodo T, Kumano S, Kushihata F, Okada M,
Hirata M, Tsuda T, Takada Y, Mochizuki T and Murakami T: CT and MR
cholangiography: Advantages and pitfalls in perioperative
evaluation of biliary tree. Br J Radiol. 85:887–896.
2012.PubMed/NCBI View Article : Google Scholar
|
|
24
|
Deka P, Islam M, Jindal D, Kumar N, Arora
A and Negi SS: Analysis of biliary anatomy according to different
classification systems. Indian J Gastroenterol. 33:23–30.
2014.PubMed/NCBI View Article : Google Scholar
|
|
25
|
Cucchetti A, Peri E, Cescon M, Zanello M,
Ercolani G, Zanfi C, Bertuzzo V, Di Gioia P and Pinna AD: Anatomic
variations of intrahepatic bile ducts in a European series and
meta-analysis of the literature. J Gastrointest Surg. 15:623–630.
2011.PubMed/NCBI View Article : Google Scholar
|
|
26
|
Al-Muhanna AF, Lutfi AM, Al-Abdulwahhab
AH, Al-Sharydah AM, Al-Quorain A, Al-Muhanna AF and Al-Dhaferi BF:
Magnetic resonance and retrograde endoscopic
cholangiopancreatography-based identification of biliary tree
variants: Are there type-related variabilities among the Saudi
population? Surg Radiol Anat. 41:869–877. 2019.PubMed/NCBI View Article : Google Scholar
|
|
27
|
Gupta A, Rai P, Singh V, Gupta RK and
Saraswat VA: Intrahepatic biliary duct branching patterns, cystic
duct anomalies, and pancreas divisum in a tertiary referral center:
A magnetic resonance cholangiopancreaticographic study. Indian J
Gastroenterol. 35:379–384. 2016.PubMed/NCBI View Article : Google Scholar
|
|
28
|
Song GW, Lee SG, Hwang S, Sung GB, Park
KM, Kim KH, Ahn CS, Moon DB, Ha TY, Kim BS, et al: Preoperative
evaluation of biliary anatomy of donor in living donor liver
transplantation by conventional nonenhanced magnetic resonance
cholangiography. Transpl Int. 20:167–173. 2007.PubMed/NCBI View Article : Google Scholar
|
|
29
|
Uysal F, Obuz F, Uçar A, Seçil M, Igci E
and Dicle O: Anatomic variations of the intrahepatic bile ducts:
Analysis of magnetic resonance cholangiopancreatography in 1011
consecutive patients. Digestion. 89:194–200. 2014.PubMed/NCBI View Article : Google Scholar
|
|
30
|
Gürsoy Çoruh A, Gülpınar B, Baş H and
Erden A: Frequency of bile duct confluence variations in subjects
with pancreas divisum: An analysis of MRCP findings. Diagn Interv
Radiol. 24:72–76. 2018.PubMed/NCBI View Article : Google Scholar
|
|
31
|
Swain B, Sahoo RK, Sen KK, G MK, Parihar
SS and Dubey R: Evaluation of intrahepatic and extrahepatic biliary
tree anatomy and its variation by magnetic resonance
cholangiopancreatography in Odisha population: A retrospective
study. Anat Cell Biol. 53:8–14. 2020.PubMed/NCBI View Article : Google Scholar
|
|
32
|
Sarawagi R, Sundar S, Raghuvanshi S, Gupta
SK and Jayaraman G: Common and uncommon anatomical variants of
intrahepatic bile ducts in magnetic resonance
cholangiopancreatography and its clinical implication. Pol J
Radiol. 81:250–255. 2016.PubMed/NCBI View Article : Google Scholar
|
|
33
|
De Filippo M, Calabrese M, Quinto S,
Rastelli A, Bertellini A, Martora R, Sverzellati N, Corradi D,
Vitale M, Crialesi G, et al: Congenital anomalies and variations of
the bile and pancreatic ducts: Magnetic resonance
cholangiopancreatography findings, epidemiology and clinical
significance. Radiol Med. 113:841–859. 2008.PubMed/NCBI View Article : Google Scholar : (In English,
Italian).
|
|
34
|
Kim SY, Byun JH, Hong HS, Choi EK, Lee SS,
Park SH and Lee MG: Biliary tract depiction in living potential
liver donors at 3.0-T magnetic resonance cholangiography. Invest
Radiol. 43:594–602. 2008.PubMed/NCBI View Article : Google Scholar
|
|
35
|
Karakas HM, Celik T and Alicioglu B: Bile
duct anatomy of the anatolian caucasian population: Huang
classification revisited. Surg Radiol Anat. 30:539–545.
2008.PubMed/NCBI View Article : Google Scholar
|
|
36
|
Cho A, Asano T, Yamamoto H, Nagata M,
Takiguchi N, Kainuma O, Soda H, Mori M, Narumoto S, Okazumi S, et
al: Relationship between right portal and biliary systems based on
reclassification of the liver. Am J Surg. 193:1–4. 2007.PubMed/NCBI View Article : Google Scholar
|
|
37
|
Macdonald DB, Haider MA, Khalili K, Kim
TK, O'Malley M, Greig PD, Grant DR, Lockwood G and Cattral MS:
Relationship between vascular and biliary anatomy in living liver
donors. AJR Am J Roentgenol. 185:247–252. 2005.PubMed/NCBI View Article : Google Scholar
|
|
38
|
Chen JS, Yeh BM, Wang ZJ, Roberts JP,
Breiman RS, Qayyum A and Coakley FV: Concordance of second-order
portal venous and biliary tract anatomies on MDCT angiography and
MDCT cholangiography. AJR Am J Roentgenol. 184:70–74.
2005.PubMed/NCBI View Article : Google Scholar
|
|
39
|
Ohkubo M, Nagino M, Kamiya J, Yuasa N, Oda
K, Arai T, Nishio H and Nimura Y: Surgical anatomy of the bile
ducts at the hepatic hilum as applied to living donor liver
transplantation. Ann Surg. 239:82–86. 2004.PubMed/NCBI View Article : Google Scholar
|
|
40
|
Choi JW, Kim TK, Kim KW, Kim AY, Kim PN,
Ha HK and Lee MG: Anatomic variation in intrahepatic bile ducts: An
analysis of intraoperative cholangiograms in 300 consecutive donors
for living donor liver transplantation. Korean J Radiol. 4:85–90.
2003.PubMed/NCBI View Article : Google Scholar
|
|
41
|
Kitagawa Y, Nimura Y, Hayakawa N, Kamiya
J, Nagino M, Uesaka K, Oda K, Ohta A, Jan YY, Cheng LP, et al:
Intrahepatic segmental bile duct patterns in hepatolithiasis: A
comparative cholangiographic study between Taiwan and Japan. J
Hepatobiliary Pancreat Surg. 10:377–381. 2003.PubMed/NCBI View Article : Google Scholar
|
|
42
|
Nakamura T, Tanaka K, Kiuchi T, Kasahara
M, Oike F, Ueda M, Kaihara S, Egawa H, Ozden I, Kobayashi N and
Uemoto S: Anatomical variations and surgical strategies in right
lobe living donor liver transplantation: Lessons from 120 cases.
Transplantation. 73:1896–1903. 2002.PubMed/NCBI View Article : Google Scholar
|
|
43
|
Priya A, Ghosh SK, Walocha JA, Pasternak
A, Iwanaga J and Loukas M: Variations in extra-hepatic biliary tree
morphology and morphometry: A narrative review of literature with
focus on cystohepatic triangle. Folia Morphol (Warsz). 82:498–506.
2023.PubMed/NCBI View Article : Google Scholar
|
|
44
|
Lamah M, Karanjia ND and Dickson GH:
Anatomical variations of the extrahepatic biliary tree: Review of
the world literature. Clin Anat. 14:167–172. 2001.PubMed/NCBI View Article : Google Scholar
|
|
45
|
Taourel P, Bret PM, Reinhold C, Barkun AN
and Atri M: Anatomic variants of the biliary tree: Diagnosis with
MR cholangiopancreatography. Radiology. 199:521–527.
1996.PubMed/NCBI View Article : Google Scholar
|
|
46
|
Renzulli M, Brocchi S, Marasco G, Spinelli
D, Balacchi C, Barakat M, Pettinari I and Golfieri R: A new
quantitative classification of the extrahepatic biliary tract
related to cystic duct implantation. J Gastrointest Surg.
25:2268–2279. 2021.PubMed/NCBI View Article : Google Scholar
|
|
47
|
Sarawagi R, Sundar S, Gupta SK and
Raghuwanshi S: Anatomical variations of cystic ducts in magnetic
resonance cholangiopancreatography and clinical implications.
Radiol Res Pract. 2016(3021484)2016.PubMed/NCBI View Article : Google Scholar
|
|
48
|
Taghavi A, Azizi M, Rasekhi A and Gholami
Z: Anatomic variations of the cystic duct in magnetic resonance
cholangiopancreatography in shiraz: A cross-sectional study. Iran J
Med Sci. 47:48–52. 2022.PubMed/NCBI View Article : Google Scholar
|
|
49
|
Shaw MJ, Dorsher PJ and Vennes JA: Cystic
duct anatomy: An endoscopic perspective. Am J Gastroenterol.
88:2102–2106. 1993.PubMed/NCBI
|
|
50
|
Gupta R, Kumar A, Hariprasad CP and Kumar
M: Anatomical variations of cystic artery, cystic duct, and gall
bladder and their associated intraoperative and postoperative
complications: An observational study. Ann Med Surg (Lond).
85:3880–3886. 2023.PubMed/NCBI View Article : Google Scholar
|
|
51
|
Pitt HA, Doty JE, DenBesten L and
Kuchenbecker SL: Stasis before gallstone formation: Altered
gallbladder compliance or cystic duct resistance? Am J Surg.
143:144–149. 1982.PubMed/NCBI View Article : Google Scholar
|
|
52
|
ASGE Standards of Practice Committee.
Buxbaum JL, Abbas Fehmi SM, Sultan S, Fishman DS, Qumseya BJ,
Cortessis VK, Schilperoort H, Kysh L, Matsuoka L, et al: ASGE
guideline on the role of endoscopy in the evaluation and management
of choledocholithiasis. Gastrointest Endosc. 89:1075–1105.e15.
2019.PubMed/NCBI View Article : Google Scholar
|
|
53
|
Ko C and Buxbaum J: Do the 2019 ASGE
choledocholithiasis guidelines reduce diagnostic ERCP? Gastrointest
Endosc. 93:1360–1361. 2021.PubMed/NCBI View Article : Google Scholar
|
|
54
|
Strasberg SM and Brunt LM: The critical
view of safety: Why it is not the only method of ductal
identification within the standard of care in laparoscopic
cholecystectomy. Ann Surg. 265:464–465. 2017.PubMed/NCBI View Article : Google Scholar
|














