Introduction
Positron emission tomography (PET) continues to gain
acceptance as a valuable tool in the diagnosis and staging of
non-small cell lung cancer (NSCLC) (1–4). Its
sensitivity and specificity with respect to the detection of
malignancy in solitary pulmonary nodules have been estimated at 97
and 78%, respectively (5), and PET
has been shown to be superior to computed tomography (CT) in
staging of the mediastinum (6–21).
There has also been much interest in the incorporation of PET into
radiation treatment planning, particularly with the opportunities
afforded by 3-D conformal radiation therapy and intensity-modulated
radiation therapy, which improve dose conformality and allow for
dose escalation. The utilization of PET imaging in treatment
planning could conceivably alter target volumes in two ways:
exclusion of suspicious, but PET-negative, tissue volumes and
inclusion of previously undetected tumor burden (22). Classically, target volumes in NSCLC
include a combination of the primary site, with or without the
ipsilateral hilum and/or mediastinum. While many studies have been
conducted which evaluate the accuracy of PET in lung cancer, few
have separated the data with respect to these areas, limiting the
confidence with which PET can be employed in radiation planning.
For this reason, this study was performed to evaluate the accuracy
of PET imaging according to these regions of interest.
Materials and methods
A University of Pennsylvania Institutional Review
Board-approved retrospective study was undertaken to assess the
diagnostic accuracy of PET based on surgical pathology
confirmation. Between January 2003 and July 2005, 351 patients with
suspicion of lung cancer underwent pre-operative PET imaging
followed by surgical resection. The dates listed were based on the
date of surgery, and all surgical procedures were performed at the
Hospital of the University of Pennsylvania. From this population,
257 (73%) patients with a pathologic diagnosis of NSCLC who did not
undergo neoadjuvant therapy were assessed. Pre-operative clinical
stage was estimated based on pre-operative PET and CT imaging via
the American Joint Committee on Cancer Staging System (6th edition)
(23). Postoperative pathologic
stage was based on surgical pathologic findings.
PET findings were documented separately with respect
to the primary site, ipsilateral hilum and mediastinum. The PET
results were then correlated with surgical pathology at the time of
resection. Measures, including accuracy, sensitivity, specificity,
positive predictive value (PPV) and negative predictive value
(NPV), were determined. PET findings were scored as positive,
suspicious or negative based solely on the original radiology
report, and suspicious findings were ultimately considered positive
as there would be a tendency to treat those regions of suspicion. A
secondary radiology review of the original PET films was not
conducted by the investigators, as it was decided to reflect
utilization of PET reports and films in a typical radiation
oncology clinic. PET studies were performed at both academic (30%)
and community (70%) centers, and patients did not undergo combined
PET/CT studies.
Statistical analysis
The χ2 (24) and Fisher's exact (24) tests were employed to test for
associations of PET accuracy with clinical and surgical factors.
All tests were two-sided, and statistical significance was defined
as p≤0.05. Concordance between clinical staging and pathologic
staging was determined via a weighted Kappa statistic (24). Statistical analyses were performed
with Statistical Package for Social Sciences statistical software
(version 11.5 for Windows; SPSS Inc., Chicago, IL, USA) and
StatXact statistical software (version 5.0 for Windows; Cytel
Software Corporation, Cambridge, MA, USA).
Results
The characteristics of the patients included in the
study are summarized in Table I.
The median patient age was 68 years (range 35–86), and most
presented with early clinical stage disease (63% stage I and 14%
stage II). Similar numbers of males and females were included, and
the majority of patients were Caucasian (90%).
 | Table I.Baseline clinical factors of all study
patients (n=257). |
Table I.
Baseline clinical factors of all study
patients (n=257).
| Clinical factor | No. | % |
|---|
| Gender | | |
| Male | 131 | 51 |
| Female | 126 | 49 |
| Age (years) | | |
| ≤65 | 105 | 41 |
| >65 | 152 | 59 |
| Median (range) | 68 (35–86) | |
| Race | | |
| Caucasian | 232 | 90 |
| Non-caucasian | 21 | 8 |
| Unknown | 4 | 2 |
| Clinical T stage | | |
| T0 | 3 | 1 |
| T1 | 154 | 60 |
| T2 | 78 | 30 |
| T3 | 3 | 1 |
| T4 | 19 | 7 |
| Clinical N stage | | |
| N0 | 182 | 71 |
| N1 | 34 | 13 |
| N2 | 33 | 13 |
| N3 | 8 | 3 |
| Clinical stage | | |
| IA | 118 | 46 |
| IB | 43 | 17 |
| IIA | 17 | 7 |
| IIB | 17 | 7 |
| IIIA | 24 | 9 |
| IIIB | 22 | 9 |
| IV | 16 | 6 |
| Primary tumor
location | | |
| Left lung | 104 | 40 |
| Right lung | 146 | 57 |
| Not
applicable/unknown | 7 | 3 |
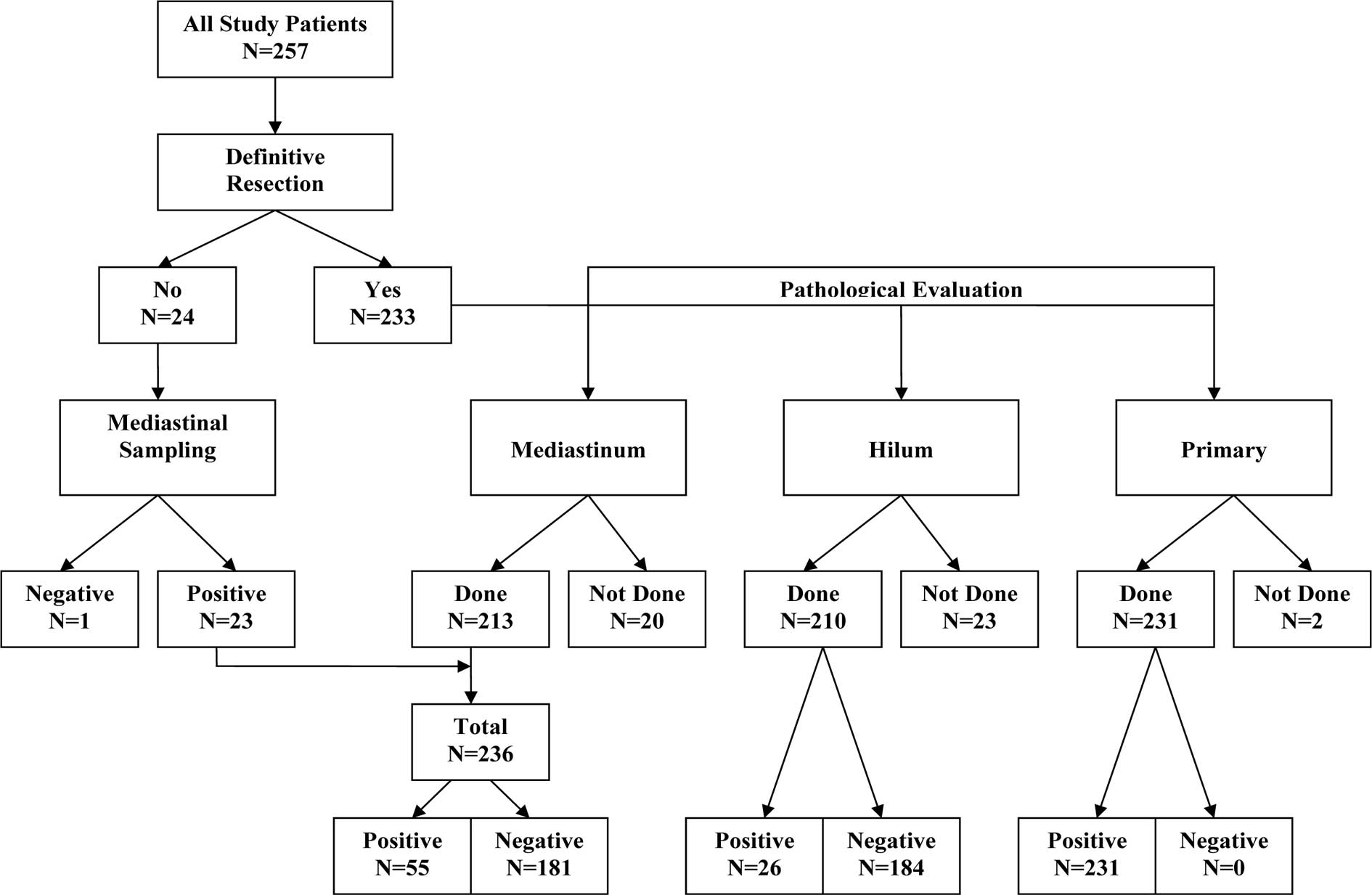
A diagram demonstrating the pathologic evaluation of
the study patients is listed in Fig.
1. Nearly all patients underwent definitive surgical resection
(91%), with the remainder undergoing mediastinal sampling alone.
The characteristics of the patients who underwent definitive
resection are summarized in Table
II. The median time between pre-operative PET and definitive
resection was 41 days (range 2–333), and a majority of patients
underwent lobectomy (77%). Most tumors were either adenocarcinoma
(45%) or squamous cell carcinoma (30%), and 92% of resected primary
tumors were >1 cm on pathologic measurement. Pre-operative
clinical measurement of tumor diameter could not be documented, as
primary tumor size was not always noted on the original radiology
report.
| Table II.Characteristics of definitive
resection patients (n=233). |
Table II.
Characteristics of definitive
resection patients (n=233).
| No. | % |
|---|
| Time from CT/PET to
surgery (days) | | |
| ≤30 | 95 | 41 |
| >30 | 138 | 59 |
| Median (range) | 41 (2–333) | |
| Surgical
procedure | | |
| Pneumonectomy | 9 | 4 |
| Bilobectomy | 7 | 3 |
| Lobectomy | 180 | 77 |
| Wedge
resection | 30 | 13 |
| Other | 7 | 3 |
| Pathologic primary
tumor size (cm) | | |
| ≤1 | 19 | 8 |
| >1 | 214 | 92 |
| Median
(range) | 2.5 (0.5–13.5) | |
| Histology | | |
| Squamous | 70 | 30 |
|
Adenocarcinoma | 105 | 45 |
| Large cell | 9 | 4 |
|
Bronchoalveolar | 36 | 16 |
| Poorly
differentiated | 12 | 5 |
| Non-small
cell | 1 | <1 |
The accuracy and prediction measures for the study
patients with respect to PET imaging are shown in Table III. The accuracy of PET imaging was
relatively high at the primary site (95%), ipsilateral hilum (80%)
and mediastinum (84%). Although the specificity of the hilum (84%)
and mediastinum (95%) was likewise high, the sensitivity with
regard to both was lower than the primary site (50 and 49%,
respectively, vs. 95%). The specificity of the primary site was not
evaluated, as all patients had pathologic evidence of disease at
the primary site. The negative prediction measures of the
ipsilateral hilum (92%) and mediastinum (86%) were again high, but,
as with sensitivity, the positive prediction measures of the
ipsilateral hilum and mediastinum were lower (31 and 75%,
respectively). The PPV and NPV of the primary site were not
calculated, as all patients had pathologic evidence of disease at
the primary site.
| Table III.Accuracy and prediction measures of
PET findings vs. pathology findings. |
Table III.
Accuracy and prediction measures of
PET findings vs. pathology findings.
A, Correlation of
PET to pathology findings by subsite.
|
|---|
| Pathology finding
|
|---|
| + | − | Total |
|---|
| Primary | | | |
| PET finding | | | |
| + | 219 | 0 | 219 |
| − | 12 | 0 | 12 |
| Total | 231 | 0 | 231 |
| Hilum | | | |
| PET finding | | | |
| + | 13 | 29 | 42 |
| − | 13 | 155 | 168 |
| Total | 26 | 184 | 210 |
| Mediastinum | | | |
| PET finding | | | |
| + | 27 | 9 | 36 |
| − | 28 | 172 | 200 |
| Total | 55 | 181 | 236 |
B, Accuracy of PET
by subsite.
|
|---|
| Site | PET accuracy
measure | No. with
finding | Total no. | % |
|---|
| Primary
(n=231) | | | | |
| Sensitivity | 219 | 231 | 94.8 |
| Specificity | 0 | 0 | NEa |
| Overall
accuracy | 219 | 231 | 94.8 |
| Hilum (n=210) | | | | |
| Sensitivity | 13 | 26 | 50.0 |
| Specificity | 155 | 184 | 84.2 |
| Overall
accuracy | 168 | 210 | 80.0 |
| Mediastinum
(n=236) | | | | |
| Sensitivity | 27 | 55 | 49.1 |
| Specificity | 172 | 181 | 95.0 |
| Overall
accuracy | 199 | 236 | 84.3 |
C, Predictive value
of PET by subsite.
|
|---|
| Site | PET prediction
measure | No. with
finding | Total no. | % |
|---|
| Primary
(n=231) | | | | |
| PPV | 219 | 219 | NEa |
| NPV | 0 | 12 | NEb |
| Hilum (n=210) | | | | |
| PPV | 13 | 42 | 31.0 |
| NPV | 155 | 168 | 92.3 |
| Mediastinum
(n=236) | | | | |
| PPV | 27 | 36 | 75.0 |
| NPV | 172 | 200 | 86.0 |
Additionally, association tests were performed
between PET accuracy and various clinical and pathologic factors. A
comparison of PET accuracy with respect to bronchoalveolar tumors
is shown in Table IV. There was
decreased PET accuracy for bronchoalveolar primary tumors vs. other
histologies (86 vs. 96%, p=0.02), but no difference was noted with
regards to accuracy within the ipsilateral hilum (85 vs. 79%,
p=0.64) or mediastinum (94 vs. 85%, p=0.27).
| Table IV.PET overall accuracy for
bronchoalveolar tumors vs. other histologies. |
Table IV.
PET overall accuracy for
bronchoalveolar tumors vs. other histologies.
| Site | Brochoalveolar
| Other histologies
| P-value |
|---|
Pathology
| Pathology
|
|---|
| + | − | + | − |
|---|
| Primary | | | | | |
|
PET+ | 31 | 0 | 188 | 0 | |
|
PET− | 5 | 0 | 7 | 0 | |
| Accuracy | 31/36 (86%) | 188/195 (96%) | 0.02 |
| Hilum | | | | | |
|
PET+ | 0 | 4 | 13 | 25 | |
|
PET− | 1 | 28 | 12 | 127 | |
| Accuracy | 28/33 (85%) | 140/177 (79%) | 0.64 |
| Mediastinum | | | | | |
|
PET+ | 0 | 1 | 12 | 8 | |
|
PET− | 1 | 30 | 19 | 142 | |
| Accuracy | 30/32 (94%) | 154/181 (85%) | 0.27 |
PET accuracy within the ipsilateral hilum and
mediastinum in patients in whom PET accurately evaluated the
primary tumor was compared to those in whom the primary tumor was
inaccurately evaluated. No difference was found in accuracy at
either site. In the ipsilateral hilum, PET was accurate in 79% of
patients with accurate PET at the primary site vs. 100% in those
with false negative PET of the primary site (p=0.36). In the
mediastinum, PET was accurate in 86% of patients with accurate PET
at the primary site vs. 100% in those with false negative PET of
the primary site (p=0.61).
PET accuracy at the primary site was decreased in
primary tumors ≤1 cm on pathologic evaluation vs. those >1 cm
(78 vs. 96%, p=0.01), and there was no difference in PET accuracy
at either the primary site (93 vs. 96%, p=0.44), ipsilateral hilum
(75 vs. 81%, p=0.44) or mediastinum (82 vs. 85%, p=0.73) when
comparing studies interpreted at academic centers (n=42) vs. those
interpreted at community facilities (n=215).
Table V depicts
concordance between clinical and pathologic staging of patients in
the study. Thirty-five percent of patients were upstaged at
surgery, 51% had no change in stage at surgery and 14% were
downstaged at surgery. A weighted Kappa analysis demonstrated
statistical concordance between clinical and pathologic staging
(p<0.0001).
| Table V.Concordance between clinical and
pathologic staging. |
Table V.
Concordance between clinical and
pathologic staging.
A, Comparison
between clinical and pathologic stage.
|
|---|
| Clinical stage | Pathologic stage
|
|---|
| IA (n=67) | IB (n=57) | IIA + IB
(n=34) | IIIA (n=27) | IIIB (n=18) | IV (n=12) |
|---|
| IA (n=108) | 56 | 19 | 15 | 3 | 9 | 6 |
| IB (n=42) | 2 | 26 | 5 | 6 | 3 | 0 |
| IIA + IIB
(n=31) | 5 | 7 | 12 | 7 | 0 | 0 |
| IIIA (n=13) | 0 | 3 | 0 | 7 | 1 | 2 |
| IIIB (n=13) | 3 | 1 | 2 | 3 | 4 | 0 |
| IV (n=8) | 1 | 1 | 0 | 1 | 1 | 4 |
B, Change in
staging based on operative findings.
|
|---|
| Pathologic vs.
clinical staging | No. | % |
|---|
| ↑ Stage | | |
| Pathologic stage
> clinical stage (to the right of the bold area) | 76 | 35 |
| = Stage | | |
| Pathologic stage
= clinical stage (bold area) | 109 | 51 |
| ↓ Stage | | |
| Pathologic stage
< clinical stage (below bold area) | 30 | 14 |
Discussion
Radiation treatment planning for lung cancer has
evolved with the introduction of new diagnostic and imaging
modalities and with increasing capacity for delivering conformal
radiotherapy. Traditional radiation portals typically included the
mediastinum and ipsilateral hilum electively, in addition to the
primary tumor. Newer techniques omit elective coverage of the
entire mediastinum and ipsilateral hilum, treating instead an
‘involved field’, which limits the treatment portals to only the
primary tumor and nodal areas deemed to be positive on
pre-treatment staging and evaluation. Single institution studies of
involved field radiation suggest that elective nodal failures are
rare, occurring in approximately 6% of patients (25,26);
this may lead to the underestimation of the true incidence of
elective nodal relapse, as isolated nodal relapses are rare and
nodal relapses in the setting of hematogenous metastases are
typically excluded. A phase III randomized trial of 200 patients
(in whom staging did not include PET) comparing elective nodal
radiation and involved field radiation demonstrated no difference
in overall survival between the groups at 5 years (27). However, a potential limitation of
involved field radiation is in the accuracy of staging and
diagnostic studies to detect pathologic disease. PET is a modality
which might provide such enhanced target delineation. While the
role of PET or PET/CT in addition to conventional workup to prevent
unnecessary surgery has been previously studied in randomized
trials (28–30), the role of PET in radiation field
design is an equally relevant, yet less examined, issue. This study
sought to evaluate PET imaging by region of interest as it applies
to radiation treatment planning in NSCLC.
To our knowledge, the present study constitutes one
of the largest published series comparing PET to surgical
pathologic data. We analyzed PET accuracy at several distinct sites
relevant for radiation treatment planning: primary tumor,
ipsilateral hilum and mediastinum. We found a relatively high
overall accuracy of PET with regard to staging of the primary site
(95%), ipsilateral hilum (80%) and mediastinum (84%), which is
similar to other published series investigating PET-based staging
and higher than the accuracy rates obtained with CT staging
(17,18,20,21).
Even with bronchoalveolar tumors, where PET demonstrated decreased
accuracy and instances where the primary site was inaccurately
evaluated, PET retained a high accuracy in the ipsilateral hilum
and mediastinum. This supports the use of PET in combination with
other imaging and staging modalities as a potentially important
tool for radiation field design.
The specificity and negative predictive values
associated with PET evaluation of nodal regions from our study were
relatively high. These findings could be utilized in deciding to
treat with involved field radiation techniques, excluding large,
elective treatment volumes in selected cases. Conversely, the
sensitivity and positive predictive values noted in our study were
relatively low; however, these results should be interpreted with
caution and may simply reflect the smaller numbers of patients with
positive hilar and mediastinal disease, as the majority had early
stage disease.
It is important to note that clinical and pathologic
stage were in agreement only half of the time, with 35% of patients
being upstaged at the time of surgery. Previous studies have
reported a level of agreement between 35 and 55% for clinical and
pathologic staging (31–35), with deterioration in agreement as
stage increases (31).
Subclinical, microscopic disease, not visualized on CT or PET,
often accounts for this upstaging. Nomori et al (16), in a study of 80 patients comparing
pre-operative PET and CT vs. surgical pathology, found that PET was
unable to distinguish foci of disease less than 4 mm and that 32%
of all resected lymph nodes with disease involvement had foci of
disease less than 4 mm. The presence of subclinical disease
involvement illustrates the limitations of clinical staging in
NSCLC, especially in those treated with definitive radiation
therapy. The use of involved field radiation, with target
delineation based on PET and CT alone, could therefore potentially
lead to erroneous underdosing or non-treatment of microscopic
disease foci. Incorporation of pathologic assessment of lymph
nodes, via mediastinoscopy or endobronchial ultrasound, in addition
to conventional staging with imaging and PET, may improve the
overall accuracy of staging and further assist in radiation
treatment planning.
There are strengths and limitations to the present
study. More than three-quarters of the patients had clinical stage
I or II disease, which may account for the lower than expected
sensitivity and PPV for PET detection of lymph node involvement.
Further evaluation of PET accuracy in more advanced stage patients
is warranted, as this would better reflect the typical lung cancer
patient referred for definitive radiation therapy. Additionally,
this study focused specifically on the role of PET alone, whereas
PET/CT is now more commonly used for staging. Despite these
limitations, our results constitute one of the largest collected
series on PET staging, and the study presented here is one of the
few examining accuracy by specific disease subsites. In addition,
our findings that there was no compromise in accuracy of lymph node
staging, even with bronchoalveolar histology or when PET
inaccurately staged the primary site, are novel to our
knowledge.
In conclusion, PET is a useful tool in the clinical
assessment and staging of lung cancer, and should be incorporated
as part of standard staging. With respect to radiation treatment
planning, it is helpful in delineating disease-affected sites and
in determining which areas to incorporate and which to exclude in
the radiation portals. However, given the rates of upstaging
observed between clinical and pathologic staging and the risk of
subclinical disease involvement, caution must be exercised during
the delineation of limited fields, and pathologic assessment of
nodes should be performed whenever possible. Lung cancer remains
one of the most common causes of cancer-related death in both men
and women, and local failure is a common occurrence. Refinements in
target delineation, radiation planning and delivery are potential
avenues by which outcomes may be improved, which will ultimately
require the incorporation of multimodal staging evaluations,
including PET.
Acknowledgements
The authors would like to acknowledge
Dr Eli Glatstein for his continuing guidance and mentorship,
without which this manuscript would not have been possible.
References
|
1.
|
Albes JM, Lietzenmayer R, Schott U,
Schülen E, Wehrmann M and Ziemer G: Improvement of non-small-cell
lung cancer staging by means of positron emission tomography.
Thorac Cardiovasc Surg. 47:42–47. 1999. View Article : Google Scholar : PubMed/NCBI
|
|
2.
|
Bury T, Paulus P, Dowlati A, Corhay JL,
Weber T, Ghaye B, Schoffers J, Limet R, Albert A, Rigo P and
Radermecker M: Staging of the mediastinum: value of positron
emission tomography imaging in non-small cell lung cancer. Eur
Respir J. 9:2560–2564. 1996. View Article : Google Scholar : PubMed/NCBI
|
|
3.
|
Coleman RE: PET in lung cancer. J Nucl
Med. 40:814–820. 1999.PubMed/NCBI
|
|
4.
|
Sachs S and Bilfinger TV: The impact of
positron emission tomography on clinical decision making in a
university-based multidisciplinary lung cancer practice. Chest.
128:698–703. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
5.
|
Gould MK, Maclean CC, Kuschner WG, Rydzak
CE and Owens DK: Accuracy of positron emission tomography for
diagnosis of pulmonary nodules and mass lesions: a meta-analysis.
JAMA. 285:914–924. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
6.
|
Gould MK, Kuschner WG, Rydzak CE, Maclean
CC, Demas AN, Shigemitsu H, Chan JK and Owens DK: Test performance
of positron emission tomography and computed tomography for
mediastinal staging in patients with non-small-cell lung cancer: a
meta-analysis. Ann Intern Med. 139:879–892. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
7.
|
Toloza EM, Harpole L and McCrory DC:
Noninvasive staging of non-small cell lung cancer: a review of the
current evidence. Chest. 123:S137–S146. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
8.
|
Sasaki M, Ichiya Y, Kuwabara Y, Akashi Y,
Yoshida T, Fukumura T, Murayama S, Ishida T, Sugio K and Masuda K:
The usefulness of FDG positron emission tomography for the
detection of mediastinal lymph node metastases in patients with
non-small cell lung cancer: a comparative study with X-ray computed
tomography. Eur J Nucl Med. 23:741–747. 1996. View Article : Google Scholar : PubMed/NCBI
|
|
9.
|
Sazon DA, Santiago SM, Soo Hoo GW,
Khonsary A, Brown C, Mandelkern M, Blahd W and Williams AJ:
Fluorodeoxyglucose-positron emission tomography in the detection
and staging of lung cancer. Am J Respir Crit Care Med. 153:417–421.
1996. View Article : Google Scholar : PubMed/NCBI
|
|
10.
|
Vansteenkiste JF and Stroobants SG: The
role of positron emission tomography with
18F-fluoro-2-deoxy-D-glucose in respiratory oncology. Eur Respir J.
17:802–820. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
11.
|
Valk PE, Pounds TR, Hopkins DM, Haseman
MK, Hofer GA, Greiss HB, Myers RW and Lutrin CL: Staging non-small
cell lung cancer by whole-body positron emission tomographic
imaging. Ann Thorac Surg. 60:1573–1582. 1995. View Article : Google Scholar : PubMed/NCBI
|
|
12.
|
Vansteenkiste JF, Stroobants SG, De Leyn
PR, Dupont PJ, Bogaert J, Maes A, Deneffe GJ, Nackaerts KL,
Verschakelen JA, Lerut TE, Mortelmans LA and Demedts MG: Lymph node
staging in non-small-cell lung cancer with FDG-PET scan: a
prospective study on 690 lymph node stations from 68 patients. J
Clin Oncol. 16:2142–2149. 1998.PubMed/NCBI
|
|
13.
|
Patz EF Jr, Lowe VJ, Goodman PC and
Herndon J: Thoracic nodal staging with PET imaging with 18FDG in
patients with bronchogenic carcinoma. Chest. 108:1617–1621. 1995.
View Article : Google Scholar : PubMed/NCBI
|
|
14.
|
Pieterman RM, van Putten JW, Meuzelaar JJ,
Mooyaart EL, Vaalburg W, Koëter GH, Fidler V, Pruim J and Groen HJ:
Preoperative staging of non-small-cell lung cancer with
positron-emission tomography. N Engl J Med. 343:254–261. 2000.
View Article : Google Scholar : PubMed/NCBI
|
|
15.
|
Scott WJ, Gobar LS, Terry JD, Dewan NA and
Sunderland JJ: Mediastinal lymph node staging of non-small-cell
lung cancer: a prospective comparison of computed tomography and
positron emission tomography. J Thorac Cardiovasc Surg.
111:642–648. 1996. View Article : Google Scholar : PubMed/NCBI
|
|
16.
|
Nomori H, Watanabe K, Ohtsuka T, Naruke T,
Suemasu K and Uno K: The size of metastatic foci and lymph nodes
yielding false-negative and false-positive lymph node staging with
positron emission tomorgraphy in patients with lung cancer. J
Thorac Cardiovasc Surg. 127:1087–1092. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
17.
|
Steinert HC, Hauser M, Allemann F, Engel
H, Berthold T, von Schulthess GK and Weder W: Non-small cell lung
cancer: nodal staging with FDG PET versus CT with correlative lymph
node mapping and sampling. Radiology. 202:441–446. 1997. View Article : Google Scholar : PubMed/NCBI
|
|
18.
|
Wahl RL, Quint LE, Greenough RL, Meyer CR,
White RI and Orringer MB: Staging of mediastinal non-small cell
lung cancer with FDG PET, CT, and fusion images: preliminary
prospective evaluation. Radiology. 191:371–377. 1994. View Article : Google Scholar : PubMed/NCBI
|
|
19.
|
Hagberg RC, Segall GM, Stark P, Burdon TA
and Pompili MF: Characterization of pulmonary nodules and
mediastinal staging of bronchogenic carcinoma with F-18
fluorodeoxyglucose positron emission tomography. Eur J Cardiothorac
Surg. 12:92–97. 1997. View Article : Google Scholar
|
|
20.
|
Gupta NC, Tamim WJ, Graeber GG, Bishop HA
and Hobbs GR: Mediastinal lymph node sampling following positron
emission tomography with fluorodeoxyglucose imaging in lung cancer
staging. Chest. 120:521–527. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
21.
|
Dunagan D, Chin R Jr, McCain T, Case L,
Harkness B, Oaks T and Haponik E: Staging by positron emission
tomography predicts survival in patients with non-small cell lung
cancer. Chest. 119:333–339. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
22.
|
Lavrenkov K, Partridge M, Cook G and Brada
M: Positron emission tomography for target volume definition in the
treatment of non-small cell lung cancer. Radiother Oncol. 77:1–4.
2005.PubMed/NCBI
|
|
23.
|
Greene FL; American Joint Committee on
Cancer, American Cancer Society: AJCC Cancer Staging Manual. 6th
edition. Springer-Verlag; New York: 2002, View Article : Google Scholar
|
|
24.
|
Fleiss JL: Statistical Methods for Rates
and Proportions. 2nd edition. John Wiley and Sons, Inc; New York:
1981
|
|
25.
|
Bradley JD, Wahab S, Lockett MA, Perez CA
and Purdy JA: Elective nodal failures are uncommon in medically
inoperable patients with stage I non-small-cell lung carcinoma
treated with limited radio-therapy fields. Int J Radiat Oncol Biol
Phys. 56:342–347. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
26.
|
Rosenzweig KE, Sura S, Jackson A and Yorke
E: Involved-field radiation therapy for inoperable non small-cell
lung cancer. J Clin Oncol. 25:5557–5561. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
27.
|
Yuan S, Sun X, Li M, Yu J, Ren R, Yu Y, Li
J, Liu X, Wang R, Li B, Kong L and Yin Y: A randomized study of
involved-field irradiation versus elective nodal irradiation in
combination with concurrent chemotherapy for inoperable stage III
nonsmall cell lung cancer. Am J Clin Oncol. 30:239–244. 2007.
View Article : Google Scholar : PubMed/NCBI
|
|
28.
|
Van Tinteren H, Hoekstra OS, Smit EF, van
den Bergh JH, Schreurs AJ, Stallaert RA, van Velthoven PC, Comans
EF, Diepenhorst FW, Verboom P, van Mourik JC, Postmus PE, Boers M
and Teule GJ: Effectiveness of positron emission tomography in the
preoperative assessment of patients with suspected non-small-cell
lung cancer: the PLUS multi-centre randomized trial. Lancet.
359:1388–1393. 2002.PubMed/NCBI
|
|
29.
|
Viney RC, Boyer MJ, King MT, Kenny PM,
Pollicino CA, McLean JM, McCaughan BC and Fulham MJ: Randomized
controlled clinical trial of the role of positron emission
tomography in the management of stage I and II non-small-cell lung
cancer. J Clin Oncol. 22:2357–2362. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
30.
|
Fischer B, Lassen U, Mortensen J, et al:
Preoperative staging of lung cancer with combined PET-CT. N Engl J
Med. 361:32–39. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
31.
|
López-Encuentra A, García-Luján R, Rivas
JJ, Rodríguez-Rodríguez J, Torres-Lanza J and Varela-Simo G;
Bronchogenic Carcinoma Cooperative Group of the Spanish Society of
Pneumology and Thoracic Surgery: Comparison between clinical and
pathologic staging in 2,994 cases of lung cancer. Ann Thorac Surg.
79:974–979. 2005.PubMed/NCBI
|
|
32.
|
Fernando HC and Goldstraw P: The accuracy
of clinical evaluative intrathoracic staging in lung cancer as
assessed by postsurgical pathologic staging. Cancer. 65:2503–2506.
1990. View Article : Google Scholar : PubMed/NCBI
|
|
33.
|
Gdeedo A, van Schil P, Corthouts B, van
Mieghem F, van Meerbeeck J and van Marck E: Comparison of imaging
TNM [(i)TNM] and pathological TNM [pTNM] in staging of bronchogenic
carcinoma. Eur J Cardiothorac Surg. 12:224–227. 1997.
|
|
34.
|
Bülzebruck H, Bopp R, Drings P, Bauer E,
Krysa S, Probst G, van Kaick G, Müller KM and Vogt-Moykopf I: New
aspects in the staging of lung cancer. Prospective validation of
the International Union Against Cancer TNM classification. Cancer.
70:1102–1110. 1992.PubMed/NCBI
|
|
35.
|
Bülzebruck H, Drings P, Kayser K, Schulz
V, Tuengerthal S and Vogt-Moykopf I: Classification of lung cancer:
first experiences with the new TNM classification (4th edition).
Eur Respir J. 4:1197–1206. 1991.PubMed/NCBI
|