Introduction
Essential hypertension is the leading cause of
cardiovascular morbidity and mortality worldwide, affecting ∼20% of
the adult population (1). Many
drugs are effective in treating hypertension, although individuals
can respond differently to the same drug. Interindividual variation
in the efficacy of medications may be influenced by genetic
variations (2). Hypertension
pharmacogenetics seeks to find genetic predictors of response to
drugs that lower blood pressure. More and more studies have
investigated associations between genetic polymorphisms and
response to drugs (3–6).
KATP (ATP-sensitive potassium channel)
channels have important functions through their coupling of
cellular energetic networks and their ability to decode metabolic
signals, and they are implicated in diseases of many organs.
KATP is formed by the physical association between the
inward-rectifier potassium channels (Kir6.x) and the regulatory
sulfonylurea receptor subunit (SUR), which forms a hetero-octameric
complex (7). Iptakalim is a novel
KATP opener with antihypertensive properties targeting
small arteries of hypertensive status in different models of
hypertension in rats and dogs. Iptakalim can produce long-lasting
hypotensive effects without tolerance. At the same time it exerted
a protective effect against hypertensive damage to target organs.
Iptakalim has preferentially selective effects on SUR2B/Kir6.1 and
it is a more potent activator of the SUR2B/Kir6.1 subtype of
KATP channels than diazoxide and pinacidil, the two most
commonly studied KATP channel openers (8–14).
Iptakalim is an effective antihypertensive drug for the treatment
of mild to moderate essential hypertension (15). Yet, individual variations for its
antihypertensive effects have been observed. Genetic variations
that alter the structure, configuration, activity, or quantity of
the drug target receptors or target-related regulation factors may
contribute to individual variations in drug response (16). Thus, genetic variations of the
Kir6.1 gene may contribute to individual variations in drug
response.
In the present study, we investigated polymorphisms
of the Kir6.1 gene in 162 Chinese Han hypertensive patients and
their possible association with the antihypertensive response to
iptakalim treatment.
Materials and methods
Patients
All of the material studied was obtained from
subjects who completed the protocol at 5 centers of the phase III
clinical trial of iptakalim which was a randomized double-blind
trial performed at 14 centers in 11 cities in China. We studied 162
non-related Chinese Han patients with essential hypertension (81
men, 81 women) (mean age ± SD, 55±9 years; range, 26–74). Patients
met the World Health Organization-International Society of
Hypertension criteria for hypertension [systolic BP (SBP) ≥140 mmHg
or diastolic BP (DBP) ≥90 mmHg]. Trained investigators assessed the
blood pressure (BP) of the patients on at least three different
occasions. All patients underwent a complete physical examination.
Secondary causes of hypertension and heart, liver, and kidney
diseases were excluded by patient history and by physical and
laboratory examinations. After a 2-week, single-blind, placebo
run-in period, all patients were treated orally with iptakalim
(Thadweik Academy of Medicine, Beijing, China) at a single daily
fixed dosage of 5 mg (one tablet per day) for 4 consecutive weeks.
Subsequently, patients whose BP was <140/90 mmHg continued the
same dose regimen for another 4 weeks. In patients whose BP was not
adequately controlled (≥140/90 mmHg), the dose was doubled for the
following 4 weeks. Patients were required to take their dose of
iptakalim at approximately 9 a.m. and carefully record the time
they took the tablet. Blood pressure was measured before taking the
medicine on the first day and 24 h after 8 weeks of treatment.
Three consecutive measurements were carried out on the right arm of
quietly seated participants with a 1-min interval between
replicates. When the difference between the measurements was >4
mmHg, the patient was asked to rest for 5 min, and then repeated
measurements were carried out. In all of our analyses, an average
of three consecutive blood pressure readings was used. Written
informed consent was obtained from all patients enrolled in the
study in accordance with principles of the Declaration of Helsinki.
The protocol of the study was approved by the institutional Ethics
Committee.
DNA studies
Genomic DNA was extracted from peripheral blood
leukocytes using standard procedures (Promega genomic DNA
purification kit, USA). The Kir6.1 gene was amplified by PCR and
screened using the PCR-SSCP method (17,18).
Primers of the Kir6.1 gene were designed using Primer3 (http://frodo.wi.mit.edu/primer3/) (Table I). The amplification was performed
as follows: initial denaturation at 95°C for 5 min followed by 35
cycles of denaturation at 95°C for 30 sec, annealing at 58°C for 30
sec, and extension at 72°C for 1 min, and final extension at 72°C
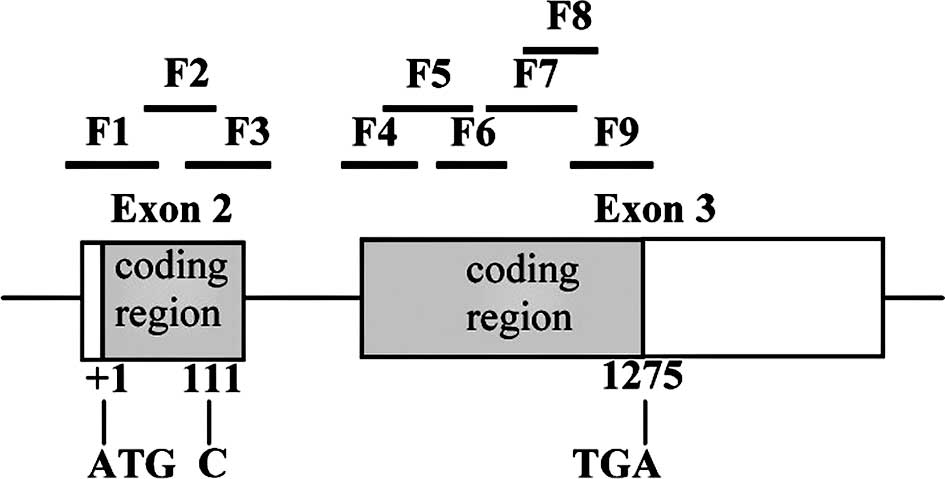
for 5 min. cDNA and protein sequences were numbered according to
GenBank NM_004982 with nucleotide numbering beginning with the
first Met (Fig. 1). The samples
were heated at 100°C for 10 min and immediately chilled on ice. PCR
products (5 μl) were electrophoresed on a 8% non-denaturing
acrylamide:bisacrylamide (29:1) gel in 1X TBE buffer. Gels were run
overnight at a constant 5 W at 4°C, and SSCP bands were visualized
on the gels by silver staining. Direct sequencing (ABI 3730XL
sequencer, Applied Biosystem) was used to confirm the results.
 | Table I.Primers and parameters for the PCR
procedure used in this study. |
Table I.
Primers and parameters for the PCR
procedure used in this study.
| Fragment | | Sequence | Amplicon size
(bp) |
|---|
| F1 | Sense |
5′-GGTGAGGATAGGGTGGGTTT-3′ | 297 |
| Antisense |
5′-CCTGTAGAAAGCGTCCTTGC-3′ | |
| F2 | Sense |
5′-ACCTGGCGCATAAGAACATC-3′ | 229 |
| Antisense |
5′-CACACAGTGGACTCCAAACC-3′ | |
| F3 | Sense |
5′-CTATCATGTGGTGGCTGGTG-3′ | 272 |
| Antisense |
5′-TGTTAGGTGTTGTTCTTTATTGTGC-3′ | |
| F4 | Sense |
5′-TCAAAATGTGACCTGATGGTG-3′ | 242 |
| Antisense |
5′-GTTTCTGCCCTTCTGTGAGC-3′ | |
| F5 | Sense |
5′-GCCATCACGGTTTTGATTCT-3′ | 286 |
| Antisense |
5′-CAGGAATGTCCAGTTGGTGA-3′ | |
| F6 | Sense |
5′-GAGTGGGTGACCTGAGGAAA-3′ | 226 |
| Antisense |
5′-GCCAGGTCAGTTGCTGAGAT-3′ | |
| F7 | Sense |
5′-GATCATCTGCCACGTGATTG-3′ | 291 |
| Antisense |
5′-GGTTTCTCATCCAGCTCTCG-3′ | |
| F8 | Sense |
5′-ATCACCACACAAGCACGAAC-3′ | 238 |
| Antisense |
5′-TGCGCTTCCTCAGAGAATTT-3′ | |
| F9 | Sense |
5′-CGAGAGCTGGATGAGAAACC-3′ | 264 |
| Antisense |
5′-CCCAGCATAAACCGTCAAAA-3′ | |
Statistical analysis
Values are expressed as the mean ± SD. The means for
continuous variables in the two groups were compared using the
t-test. The prevalence of categorical variables was compared using
the χ2 test. The blood pressure (BP) response was
defined as the blood pressure before treatment minus the blood
pressure at the end of the 8-week treatment. All tests were
two-tailed, and P<0.05 was considered statistically significant.
The SPSS 13.0 statistical package (SPSS, Chicago, IL, USA) was used
for analysis.
Results
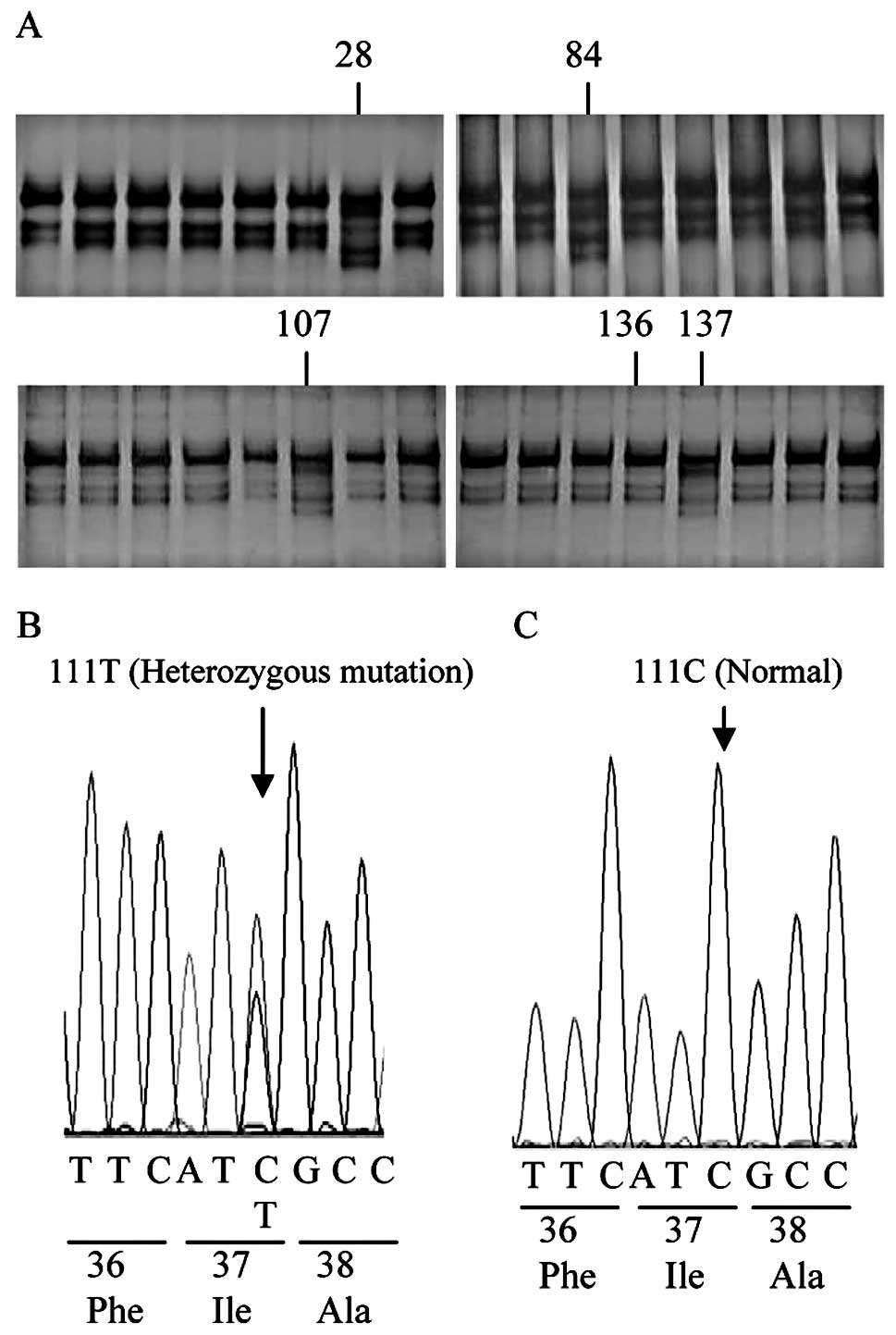
PCR-SSCP and DNA sequencing were used to detect
mutation of the Kir6.1 gene in 162 Chinese Han hypertensive
patients treated by iptakalim. As shown in Fig. 2, single base pair substitution (C
to T) at nucleotide position 111 in exon 2 of the coding region was
detected in one female and three male patients. This substitution
in four patients was heterozygous and did not result in an amino
acid substitution (Ile37Ile, silent mutation). The I37I
polymorphism was found to have a low prevalence in the Chinese Han
hypertensive patients. The frequencies of the CC and CT genotypes
were 97.5 and 2.5%, respectively. The TT genotype was not found in
this population. For the 162 patients in this study, there were no
significant differences in age, gender, body mass index (BMI),
baseline SBP and DBP between patients with the CC and patients with
the CT genotype before iptakalim treatment (Table II). The BP of the four patients
with the CT genotype was well controlled by iptakalim treatment.
Comparison of the reductions in BP at 8 weeks post treatment in the
patients with the I37I polymorphism showed that there was no
significant difference in the SBP and DBP response between the
patients with the CC and CT genotypes (Table II).
| Table II.Clinical characteristics of the
patients and evaluation of the reduction in blood pressure (BP) at
8 weeks post treatment with iptakalim in patients with the I37I
polymorphism. |
Table II.
Clinical characteristics of the
patients and evaluation of the reduction in blood pressure (BP) at
8 weeks post treatment with iptakalim in patients with the I37I
polymorphism.
| Characteristics | Kir6.1 gene I37I
genotype
|
|---|
| CC (n=158) | CT (n=4) | P-valuea |
|---|
| Age, mean (SD),
years | 55 (9) | 59 (12) | 0.395 |
| Gender
(male/female) | 78/80 | 1/3 | 0.314 |
| Body mass index, mean
(SD), kg/m2 | 25.3 (2.7) | 24.7 (1.8) | 0.627 |
| Blood pressure, mean
(SD), mmHg | | | |
| SBP | 152.7 (12.6) | 149.3 (16.6) | 0.587 |
| DBP | 100.0 (4.1) | 99.7 (4.2) | 0.876 |
| BP reduction, mean
(SD), mmHg | | | |
| ΔSBP | 11.0 (13.4) | 12.9 (24.4) | 0.787 |
| ΔDBP | 11.0 (7.8) | 16.4 (14.3) | 0.191 |
Discussion
During screening of the entire coding region and
partial screening of the intron of the Kir6.1 gene in 162 patients,
a low prevalence of the I37I polymorphism in the exon 2 coding
region was noted. Frequencies of the CC and CT genotypes were
158/162 (97.5%) and 4/162 (2.5%), respectively. The TT genotype was
not found in this population. There were no significant differences
in BP response to iptakalim between the patients with the CC
genotype and those with the CT genotype. No other mutations or
polymorphisms were detected in the remaining patients. The results
indicate that abnormality in the primary structure of Kir6.1 may
not be involved in the genetic pathogenesis of essential
hypertension and the BP response to iptakalim in Chinese Han
hypertensive patients.
The I37I mutation was previously detected in one
female Japanese patient with coronary spastic angina (CSA). No
other mutation was detected in the genetic analysis of the Kir6.1
gene in 19 Japanese patients with CSA (19). A complete mutational analysis of
the Kir6.1 gene was performed in a series of 18 Italian patients
with impaired coronary vasomotility, and no mutations were detected
in the sample analyzed, thus suggesting that Kir6.1 gene
aberrations are not a common cause of abnormal coronary
vasomotility in Italians (20). A
rare missense variant in exon 3 of the Kir6.1 gene was found to be
associated with ventricular fibrillation with prominent early
repolarization (21). The
mutational analysis of the Kir6.1 gene among various ethnic groups
showed that it may be so important that no mutations or
polymorphisms that alter the primary structure of Kir6.1 are
allowed. This is in agreement with the result of a Kir6.1 gene
knockout experiment which found that deficiency of the Kir6.1
KATP channel imparts fatal susceptibility to endotoxemia
(22).
To our knowledge, this study is the first to
investigate polymorphisms of the Kir6.1 gene and the association of
the I37I polymorphism with BP and BP response to antihypertensive
drugs in a Chinese Han hypertensive population. One limitation of
our study is that, even though our sample size (162 patients) was
larger than previous Kir6.1 gene mutation studies (19–21),
our study population may be too small to confirm an association of
the I37I polymorphism and BP response to iptakalim due to the low
prevalence of this polymorphism in our study. Therefore a larger
sample is needed to more accurately determine whether or not the
I37I polymorphism is associated with BP response to iptakalim
treatment. Iptakalim preferentially activates the SUR2B/Kir6.1
subtype of KATP channels (13,23),
and the SUR2B gene may be an important candidate gene for
pharmacogenetics research of iptakalim.
In conclusion, we demonstrated that abnormality in
the primary structure of Kir6.1 is not involved in the genetic
pathogenesis of essential hypertension in Chinese Han hypertensive
patients and the I37I polymorphism may have no effect on the BP
response to iptakalim treatment.
Acknowledgements
This study was supported by grants
from the National Key Technologies R&D Program of China (no.
2008ZXJ09004-018). We thank the patients for their
participation.
References
|
1.
|
Zhang S, Mao G, Zhang Y, et al:
Association between human atrial natriuretic peptide Val7Met
polymorphism and baseline blood pressure, plasma trough irbesartan
concentrations, and the antihypertensive efficacy of irbesartan in
rural Chinese patients with essential hypertension. Clin Ther.
27:1774–1784. 2005. View Article : Google Scholar
|
|
2.
|
Trotta R, Donati MB and Iacoviello L:
Trends in pharmacogenomics of drugs acting on hypertension.
Pharmacol Res. 49:351–356. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
3.
|
Arnett DK and Claas SA: Pharmacogenetics
of antihypertensive treatment: detailing disciplinary dissonance.
Pharmacogenomics. 10:1295–1307. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
4.
|
Sherva R, Ford CE, Eckfeldt JH, Davis BR,
Boerwinkle E and Arnett DK: Pharmacogenetic effect of the
stromelysin (MMP3) polymorphism on stroke risk in relation to
antihypertensive treatment: the genetics of hypertension associated
treatment study. Stroke. 42:330–335. 2011. View Article : Google Scholar
|
|
5.
|
Duarte JD, Lobmeyer MT, Wang Z, et al:
Lack of association between polymorphisms in STK39, a putative
thiazide response gene, and blood pressure response to
hydrochlorothiazide. Pharmacogenet Genomics. 20:516–519. 2010.
View Article : Google Scholar : PubMed/NCBI
|
|
6.
|
Suonsyrjä T, Donner K, Hannila-Handelberg
T, Fodstad H, Kontula K and Hiltunen TP: Common genetic variation
of beta1- and beta2-adrenergic receptor and response to four
classes of antihypertensive treatment. Pharmacogenet Genomics.
20:342–345. 2010.PubMed/NCBI
|
|
7.
|
Nichols CG: KATP channels as molecular
sensors of cellular metabolism. Nature. 440:470–476. 2006.
View Article : Google Scholar : PubMed/NCBI
|
|
8.
|
Wang H, Zhang YL and Chen YP: Targeting
small arteries of hypertensive status with novel ATP-sensitive
potassium channel openers. Curr Vasc Pharmacol. 3:119–124. 2005.
View Article : Google Scholar : PubMed/NCBI
|
|
9.
|
Wang H, Long CL and Zhang YL: A new
ATP-sensitive potassium channel opener reduces blood pressure and
reverses cardiovascular remodeling in experimental hypertension. J
Pharmacol Exp Ther. 312:1326–1333. 2005. View Article : Google Scholar
|
|
10.
|
Gao S, Long CL, Wang RH and Wang H:
KATP activation prevents progression of cardiac
hypertrophy to failure induced by pressure overload via protecting
endothelial function. Cardiovasc Res. 83:444–456. 2009.
|
|
11.
|
Wang H, Tang Y, Wang L, Long CL and Zhang
YL: ATP-sensitive potassium channel openers and
2,3-dimethyl-2-butylamine derivatives. Curr Med Chem. 14:133–155.
2007. View Article : Google Scholar : PubMed/NCBI
|
|
12.
|
Chen YP, Qiu CR and Wang H: Cardiovascular
pharmacological characterization of novel 2,3-dimethyl-2-butylamine
derivatives in rats. Life Sci. 75:2131–2142. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
13.
|
Chen YP, Cui WY and Wang H: Selective
actions of iptakalim on the subtypes of KATP channels.
Chin Pharmacol Bull. 22:278–284. 2006.
|
|
14.
|
Long CL, Qin XC, Pan ZY, et al: Activation
of ATP-sensitive potassium channels protects vascular endothelial
cells from hypertension and renal injury induced by hyperuricemia.
J Hypertens. 26:2326–2338. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
15.
|
Duan RF, Cui WY, Gao HY, et al:
Correlation between ACE gene I/D polymorphism and clinical efficacy
of iptakalim in Chinese Han hypertensive population. Chin J Clin
Pharmacol Ther. 15:961–966. 2010.
|
|
16.
|
Evans WE and Relling MV: Pharmacogenomics:
translating functional genomics into rational therapeutics.
Science. 286:487–491. 1999. View Article : Google Scholar : PubMed/NCBI
|
|
17.
|
Bettinaglio P, Galbusera A, Caprioli J, et
al: Single strand conformation polymorphism (SSCP) as a quick and
reliable method to genotype M235T polymorphism of angiotensinogen
gene. Clin Biochem. 35:363–368. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
18.
|
Lu Jun, Jiang Shan, Ye Song and Li
Chaopin: Detecting drug resistant genetic mutation among
pneumoconiosis patients complicated with tuberculosis in
Mycobacterium tuberculosis L-forms application of PCR-SSCP
technique in Huainan mining district. J Nanjing Med Univ.
3:180–184. 2007.
|
|
19.
|
Tomita H, Sasaki S, Osanai T, et al:
Mutational analysis of Kir6.1 in Japanese patients with coronary
spastic angina. Int J Mol Med. 18:589–591. 2006.
|
|
20.
|
Emanuele E, Falcone C, Carabela M, et al:
Absence of Kir6.1/ KCNJ8 mutations in Italian patients with
abnormal coronary vasomotion. Int J Mol Med. 12:509–512.
2003.PubMed/NCBI
|
|
21.
|
Haïssaguerre M, Chatel S, Sacher F, et al:
Ventricular fibrillation with prominent early repolarization
associated with a rare variant of KCNJ8/KATP channel. J Cardiovasc
Electrophysiol. 20:93–98. 2009.PubMed/NCBI
|
|
22.
|
Kane GC, Lam CF, O’Cochlain F, et al: Gene
knockout of the KCNJ8-encoded Kir6.1 K(ATP) channel imparts fatal
susceptibility to endotoxemia. FASEB J. 20:2271–2280. 2006.
View Article : Google Scholar : PubMed/NCBI
|
|
23.
|
Pan Z, Huang J, Cui W, Long C, Zhang Y and
Wang H: Targeting hypertension with a new adenosine
triphosphate-sensitive potassium channel opener iptakalim. J
Cardiovasc Pharmacol. 56:215–228. 2010. View Article : Google Scholar : PubMed/NCBI
|