Introduction
The number of hypertensive subjects in Japan is
estimated to be 40 million. Since the proportion of elderly people
in the population is increasing and the incidence of hypertension
increases with age, management of hypertension is an important
problem in our country. Lifestyle factors, particularly excess
dietary salt intake, play major roles in the onset as well as the
development of hypertension (1–5).
Salt intake of the Japanese population was among the highest for
countries that participated in the INTERSALT study (6), and thus salt restriction is the most
important lifestyle modification for the Japanese.
Hypertension prevention is one of the important
outcomes of ‘Healthy Japan 21’, which is a project designed to
create a healthy nation in the 21st century.
In ‘Healthy Japan 21’, the goal is a daily salt
intake of less than 10 g in males and less than 8 g in females.
However, according to this interim report, the goal seems to be
very difficult to achieve (7,8).
Thus, it is important to develop strategies for educating people
about the need to reduce their salt intake.
One strategy is the self-monitoring of urinary salt
excretion; this was recommended as a useful strategy by the Working
Group for Dietary Salt Reduction of the Japanese Society of
Hypertension (9). A device that
may be useful with this strategy is a self-monitoring device that
was recently developed and estimates 24-h urinary salt excretion
from overnight urine samples (10). However, the usefulness of this
medical device as an educational tool has not yet been established.
The purpose of this study, therefore, was to determine the
usefulness of this urinary salt self-monitoring device for
educating healthy adults regarding their levels of salt intake and
the dangers of excessive salt use.
Materials and methods
Study protocol
The study protocol was approved by the Ethics
Committee of Nishikyushu University. Informed written consent was
obtained from each subject, and the study protocol conformed to the
ethical guidelines of the 1975 Declaration of Helsinki. We
prospectively enrolled healthy adult volunteers between March and
April of 2009 in Saga, Japan. Exclusion criteria included physical,
psychic and social difficulties, subjects under medical treatment
and those ≥65 years of age. A total of 30 subjects (15 males and 15
females) were enrolled in the study.
Participant occupations included administrative
officials (n=22) and public health nurses (n=8).
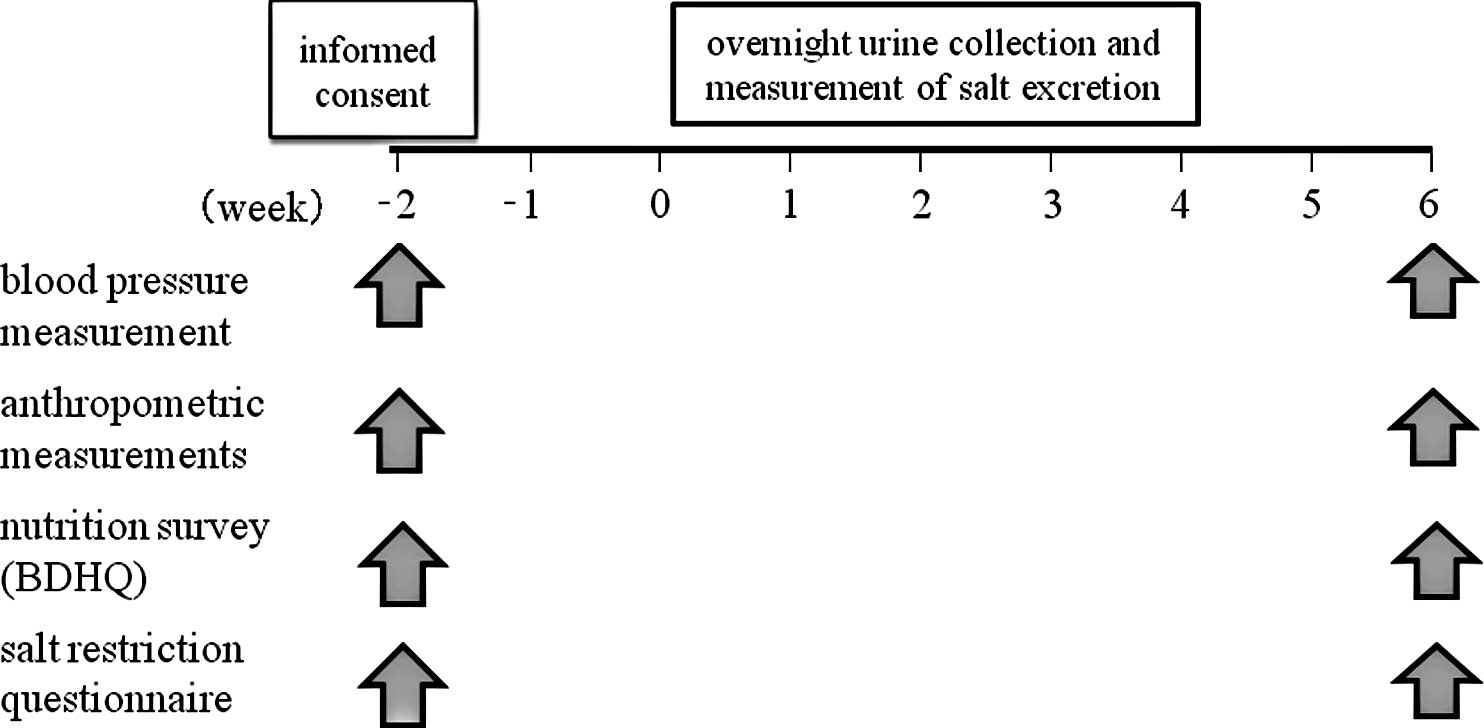
The intervention schedule is shown in Fig. 1. At baseline and 8 weeks later we
measured blood pressure (BP), anthropometric variables and
nutritional variables (by a dietary habits questionnaire). BP was
measured with a sphygmomanometer by a public health nurse while
subjects were sitting quietly at a room temperature of 25°C.
Anthropometric measurements, including waist circumference, were
prformed by a dietitian. Survey of nutritional variables was
carried out using a brief self-administered dietary history
questionnaire (BDHQ) that was able to evaluate the nutrient intake
of the previous month (11). The
BDHQ was developed based on a self-administered dietary history
questionnaire (DHQ) (12,13). The practice of salt restriction was
investigated using a salt restriction questionnaire. This included
awareness of salt restriction and of the salt content of food,
frequency of the use of seasoning, frequencies of eating pickles,
noodles and soup, and opportunities to eat out. In this survey, the
salt awareness was obtained based on the participant’s
self-evaluation. Scores for these items were added and the total
score was used to investigate the relationship between awareness of
salt restriction and actual urinary salt excretion. Subjects were
asked to measure daily salt excretion at home for 4 weeks using the
self-monitoring device.
Outcome markers
The main outcome measures were salt excretion levels
and changes in systolic blood pressure (SBP) and diastolic blood
pressure (DBP).
Statistical analysis
Values are presented as the means ± standard
deviation (SD). Differences in variables were compared by paired
t-tests. A Chi-square test was also utilized when appropriate.
Correlations between variables were analyzed using Pearson’s
product moment correlation coefficient and multiple linear
regression analysis. All data were statistically analyzed with the
assistance of the JMP software program (ver. 8; SAS Institute,
Cary, NC, USA). The α-level was set at P=0.05.
Results
Baseline characteristics and urinary salt
excretion
The mean age of the subjects was 43.2±8.8 years. The
mean salt excretion for all subjects (averaged over 4 weeks) was
8.05±1.61 g/day and the range (maximum-minimum value) was 5.58±2.15
g/day in all subjects (Table I).
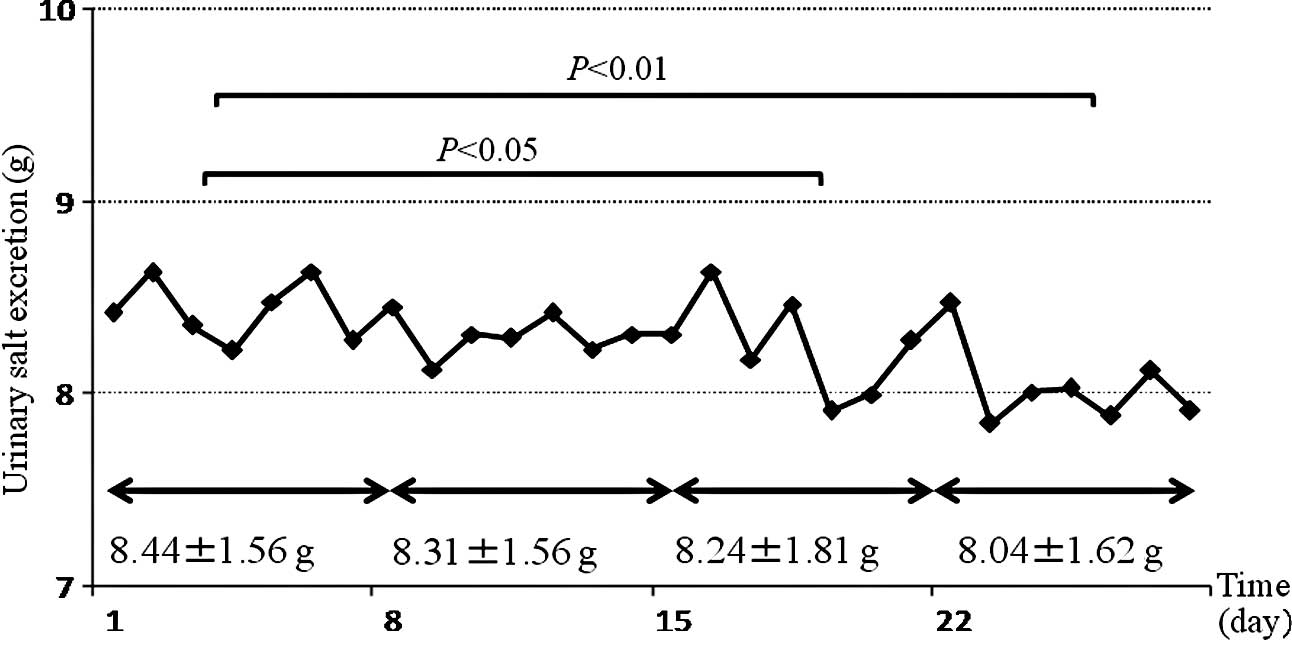
Fig. 2 demonstrates the trend of
daily salt excretion for all subjects throughout the 4 weeks. The
average urinary salt excretion significantly decreased from week 1
to weeks 3 and 4 (P<0.05 and P<0.01, respectively).
 | Table I.Background of participants and urinary
salt excretion. |
Table I.
Background of participants and urinary
salt excretion.
| Participants
(no.) | 30 |
| (male/female) | 15/15 |
| Age (years) | 43.20±8.8 |
| Urinary salt
excretion for 4 weeks (g/day) | 8.05±1.61 |
| Maximal value
(g/day) | 11.05±2.10 |
| Minimum value
(g/day) | 5.47±1.86 |
| Range (g/day) | 5.58±2.15 |
| Urinary salt
excretion of 1st week (g/day) | 8.44±1.56 |
| Urinary salt
excretion of 2nd week (g/day) | 8.31±1.56 |
| Urinary salt
excretion of 3rd week (g/day) | 8.24±1.81a |
| Urinary salt
excretion of 4th week (g/day) | 8.04±1.62b |
Clinical parameters
Table II shows the
changes in BP and anthropometric measures from baseline to the end
of week 8. The decrease in DBP was significant, but the decreases
in SBP and in the anthropometric variables were not. Urinary salt
excretion was significantly correlated with SBP (r= 0.54,
P<0.005), DBP (r= 0.55, P<0.005), body weight (BW) (r= 0.63,
P<0.005), body mass index (r= 0.41, P<0.05) and waist
circumference (WC) (r= 0.37, P<0.05). Multiple linear regression
analysis showed that DBP, body weight and WC were significantly and
independently associated with urinary salt excretion
(R2=0.5399 for total of DBP, BW and WC).
| Table II.Changes in blood pressure,
anthropometrics and nutritional intake. |
Table II.
Changes in blood pressure,
anthropometrics and nutritional intake.
| Baseline | End of week 8 |
|---|
| SBP (mmHg) | 123.0±20.7 | 122.1±18.8 |
| DBP (mmHg) | 77.7±14.3 | 74.3±13.3 |
| BW (kg) | 60.8±11.0 | 60.6±11.3 |
| BMI
(kg/m2) | 22.8±3.3 | 22.7±3.5 |
| Waist circumference
(cm) | 81.1±9.1 | 80.7±8.7 |
| Total energy
(kJ) | 7,800±3,073 | 7,155±2,801a |
| Protein (g) | 62.3±21.2 | 58.3±20.2 |
| Fat (g) | 53.8±21.0 | 50.8±18.7 |
| Carbohydrate (g) | 245.2±90.7 | 229.5±96.4 |
| Potassium (mg) | 2,269±905 | 2,234±868 |
| Calcium (mg) | 416±180 | 420±180 |
| Magnesium (mg) | 231±87 | 221±82 |
| Salt (g) | 9.1±2.8 | 8.5±3.1b |
Dietary intake
Table II shows the
changes in nutritional intake from baseline to the end of the 8th
week. Energy and salt intakes decreased significantly, while intake
of other nutritional variables did not significantly change during
this period. Energy intake was significantly correlated with salt
intake both at baseline (r=0.85, P<0.0001) and at the end of the
study (r=0.90, P<0.0001). Furthermore, changes in both variables
during the observation period were correlated with each other
(r=0.40, P=0.0286).
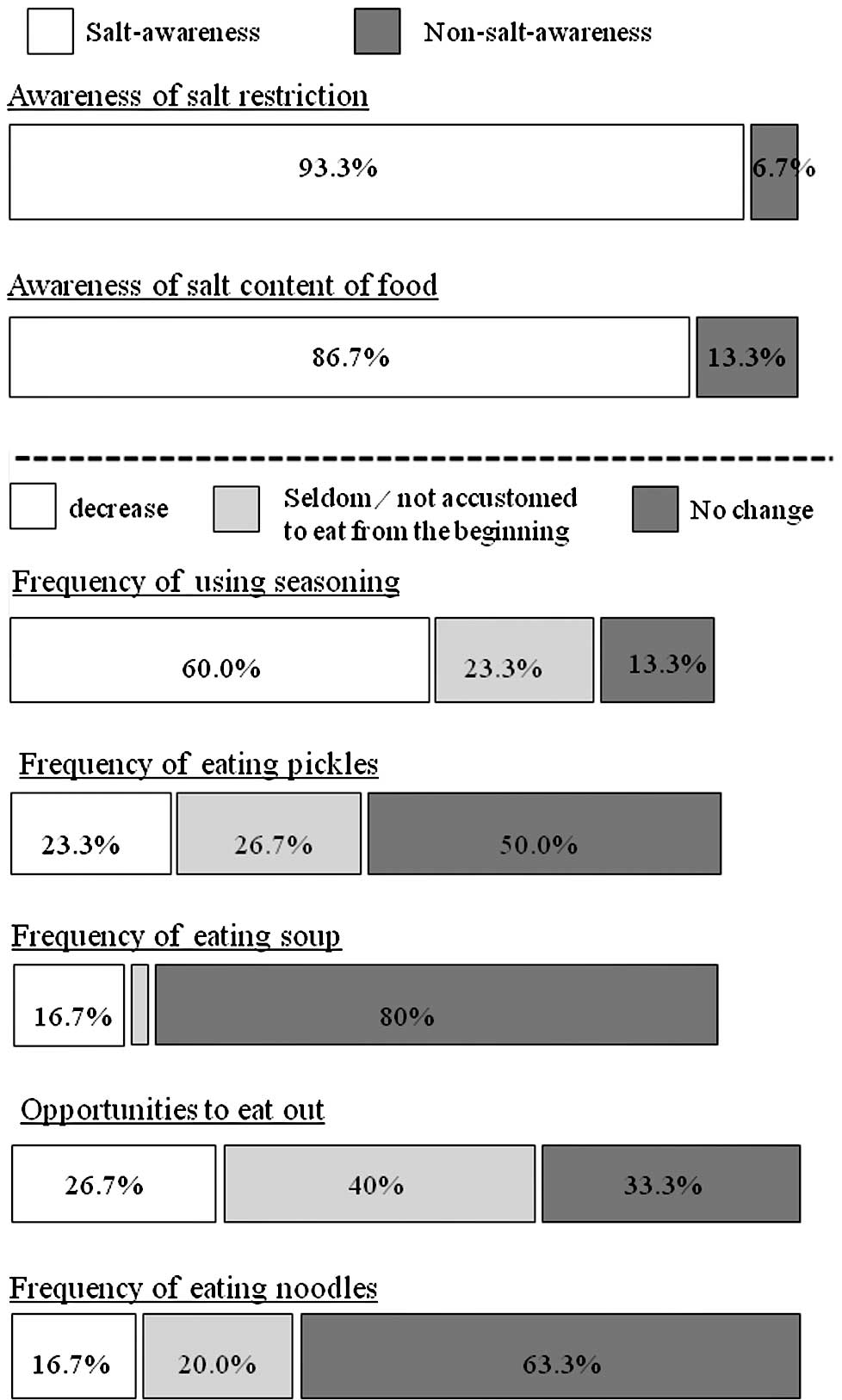
Salt restriction questionnaire
The proportion of those who were aware of salt
restriction increased from 47% at baseline to 90% after 8 weeks.
Among the items investigated, awareness of the salt content of food
increased and the use of seasoning decreased, while other items
failed to show significant changes (Fig. 3). When urinary salt excretion was
compared between the high- (>6 points) and low-score (≤6 points)
groups, subjects in the high-score group showed significantly lower
salt excretion (7.07±0.80 g/day) compared to those in the low-score
group (8.46±1.70 g/day, P<0.01).
Discussion
There were two main findings of the present study.
i) Self-monitoring of urinary salt excretion at home for 4 weeks
significantly reduced urinary salt excretion in healthy adults. ii)
DBP, BW and WC were correlated with urinary salt excretion.
Ohta et al reported that urinary salt
excretion is reduced by the use of a self-monitoring device by
hypertensive patients, and that BW is significantly correlated with
salt excretion (14). Meland et
al also reported that during a randomized controlled trial for
12 weeks, BP decreased significantly in hypertensive patients who
were using self-monitoring of urine for Cl− in addition
to receiving nutritional instruction (15). These reports are consistent with
our results showing the short-term usefulness of the
self-monitoring of urinary salt excretion, and the relationship
between salt excretion and BW. The present observation that
self-monitoring of urinary salt excretion effectively decreases
salt excretion even in healthy adults clearly indicates the
potential usefulness of this method as an educational tool that
will increase salt restriction and lead to the prevention of
hypertension. However, salt restriction and weight control may not
last long, as suggested by our TOHP II study (16). Thus, future studies are necessary
to investigate long-term effectiveness of our salt-excretion
self-monitoring method for decreasing salt intake.
The decrease in salt intake was observed not only in
those engaged in self-monitoring of urinary salt excretion, but
also by results from our nutrition survey. In the nutrition survey,
there was a significant and strong correlation between energy and
salt intakes. Since salt intake of obese subjects was reported to
be high compared to normal weight subjects (17), the restriction of energy intake may
lead to salt reduction.
It is intriguing that self-monitoring of urinary
salt excretion improved the awareness of salt restriction in
normotensive subjects. However, there was no significant
association between urinary salt excretion and awareness of salt
restriction at baseline (data not shown). This observation is
compatible with previous findings by Ohta et al that there
is no relationship between awareness of salt restriction and the
actual salt intake evaluated by 24-h urine collection (18). Since subjective awareness of salt
restriction may not necessarily be reflected in actual salt
reduction, monitoring of salt excretion seems extremely important
to educate the population about the health benefits of salt
restriction.
Concerning the validity of the self-monitoring
device, Yamasue et al reported a significant correlation
between i) salt excretion values estimated using overnight urine
and a self-monitoring device, and ii) salt excretion measured by
24-h urine collection (r=0.72, P<0.001) (10). Ohta et al also reported that
salt excretion measured with a self-monitoring device correlated
well with that determined by 24-h home urine evaluation in
hypertensive subjects (r=0.63, P<0.01) (14). Since the self-monitoring device can
be used at home to evaluate daily urinary salt excretion, it can be
used as a strong motivational tool to help individuals reduce salt
intake. As a matter of fact, in this study urinary salt excretion
by itself, without any specific educational program, reduced salt
intake. Therefore, it seems more practical to use this device
rather than 24-h urine collections for educating people about their
need for salt restriction.
Several potential limitations of the present study
include its non-randomized observational design, use of a small
number of subjects and a short duration. Another limitation is that
subjects were relatively young and of above average intelligence.
Therefore, it is not yet clear whether the present findings can be
extrapolated to the general population.
In conclusion, the use of a self-monitoring device
leads to a decrease in salt excretion, which indicates that
subjects reduced their salt intake. Use of the device thus seems to
be an effective tool for educating healthy adults about the health
benefits of salt restriction.
Acknowledgements
The present study was supported by
funds from the Nishikyushu University. The authors greatly
appreciate the technical assistance received from the staff of the
Department of Health promotion, Tosu Health Center.
References
|
1.
|
Intersalt: an international study of
electrolyte excretion and blood pressure. Results for 24 hour
urinary sodium and potassium excretion. Intersalt Cooperative
Research Group. BMJ. 297:319–328. 1988. View Article : Google Scholar
|
|
2.
|
Antonios TF and MacGregor GA: Salt intake:
potential deleterious effects excluding blood pressure. J Hum
Hypertens. 9:511–515. 1995.PubMed/NCBI
|
|
3.
|
Du Cailar G, Ribstein J and Mimran A:
Dietary sodium and target organ damage in essential hypertension.
Am J Hypertens. 15:222–229. 2002.
|
|
4.
|
Espeland MA, Whelton PK, Kostis JB, et al:
Predictors and mediators of successful long-term withdrawal from
antihypertensive medications. TONE Cooperative Research Group.
Trial of Nonpharmacologic Interventions in the Elderly. Arch Fam
Med. 8:228–236. 1999. View Article : Google Scholar
|
|
5.
|
Obarzanek E, Proschan MA, Vollmer WM, et
al: Individual blood pressure responses to changes in salt intake:
results from the DASH-Sodium trial. Hypertension. 42:459–467. 2003.
View Article : Google Scholar : PubMed/NCBI
|
|
6.
|
The INTERSALT Co-operative Research Group:
appendix tables: Centre-specific results by age and sex. J Hum
Hypertens. 3:331–407. 1989.PubMed/NCBI
|
|
7.
|
Nakagawa H, Morikawa Y, Okayama A, et al:
Trends in blood pressure and urinary sodium and potassium excretion
in Japan: reinvestigation in the 8th year after the Intersalt
Study. J Hum Hypertens. 13:735–741. 1999.PubMed/NCBI
|
|
8.
|
Stamler J, Elliott P, Dennis B, et al:
INTERMAP: background, aims, design, methods, and descriptive
statistics (nondietary). J Hum Hypertens. 17:591–608. 2003.
View Article : Google Scholar : PubMed/NCBI
|
|
9.
|
Kawano Y, Tsuchihashi T, Matsuura H, Ando
K, Fujita T and Ueshima H: Report of the Working Group for Dietary
Salt Reduction of the Japanese Society of Hypertension: (2)
assessment of salt intake in the management of hypertension.
Hypertens Res. 30:887–893. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
10.
|
Yamasue K, Tochikubo O, Kono E and Maeda
H: Self-monitoring of home blood pressure with estimation of daily
salt intake using a new electrical device. J Hum Hypertens.
20:593–598. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
11.
|
Sasaki S: Development and evaluation of
dietary assessment methods using biomarkers and diet history
questionnaire for individuals. Research for Evaluation Methods of
Nutrition and Dietary Lifestyle Programs Held on Healthy Japan 21.
Summary Report. Ministry of Health, Welfare and Labor; pp. 10–44.
2004
|
|
12.
|
Sasaki S, Ushio F, Amano K, et al: Serum
biomarker-based validation of a self-administered diet history
questionnaire for Japanese subjects. J Nutr Sci Vitaminol.
46:285–296. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
13.
|
Sasaki S, Yanagibori R and Amano K:
Self-administered diet history questionnaire developed for health
education: a relative validation of the test-version by comparison
with 3-day diet record in women. J Epidemiol. 8:203–215. 1998.
View Article : Google Scholar : PubMed/NCBI
|
|
14.
|
Ohta Y, Tsuchihashi T, Miyata E and Onaka
U: Usefulness of self-monitoring of urinary salt excretion in
hypertensive patients. Clin Exp Hypertens. 31:690–697. 2009.
View Article : Google Scholar : PubMed/NCBI
|
|
15.
|
Meland E, Laerum E and Ulvik RJ: Salt
restriction in hypertension – the effect of dietary advice and self
monitoring of chloride concentration in urine. Scand J Clin Lab
Invest. 54:399–404. 1994.
|
|
16.
|
The Trials of Hypertension Prevention,
phase II. The Trials of Hypertension Prevention Collaborative
Research Group: Effects of weight loss and sodium reduction
intervention on blood pressure and hypertension incidence in
overweight people with high-normal blood pressure. Arch Intern Med.
157:657–667. 1997.
|
|
17.
|
Frackiewicz J, Hamulka J, Wawrzyniak A and
Gornicka M: [Students nutrients intake and risk of cardiovascular
diseases]. Rocz Panstw Zakl Hig. 60:269–274. 2009.
|
|
18.
|
Ohta Y, Tsuchihashi T, Ueno M, et al:
Relationship between the awareness of salt restriction and the
actual salt intake in hypertensive patients. Hypertens Res.
27:243–246. 2004. View Article : Google Scholar : PubMed/NCBI
|