Introduction
Approximately 500,000 cases of head and neck
squamous cell carcinoma (HNSCC) are diagnosed worldwide each year
(1). The main treatment for
localized (stages I and II) HNSCC is surgical resection. However,
for loco-regionally advanced stage HNSCC (stages III and IV), the
benefits of surgery are much less apparent as most patients
eventually present with recurrence (2). Moreover, approximately two-thirds of
these patients have advanced disease with large primary tumors
and/or regional lymph node involvements (T3–4/N2–3 and M0–1) at the
time of diagnosis (3). Thus, the
conventional treatment for these patients is chemotherapy or
radiotherapy. However, broad resistance, termed multidrug
resistance (MDR), to chemotherapy has been found to be a major
cause for the failure of HNSCC treatment (4). Among the many reasons for MDR, it has
been reported that the family of ATP-binding cassette (ABC)
transporters plays a critical role (5).
ATP-binding cassette, subfamily G, member 2 (ABCG2),
is a member of the ABC transporter family, which was first cloned
from doxorubicin-resistant human MCF-7 breast cancer cells and was
named breast cancer resistance protein (BCRP) (6). ABCG2 overexpression has been observed
in many cell lines and tumor types (7–16),
where it functions to pump a wide variety of endogenous and
exogenous compounds out of cells (17–21).
ABCG2 was demonstrated to be associated with cancer stem cells and
multidrug resistance (22,23). However, the levels of ABCG2
expression in laryngeal, hypopharyngeal and nasopharyngeal cancers
are not known. In addition, the correlation between the level of
expression and clinical characteristics also remains to be
determined. In the present study, to explore the role of ABCG2 in
HNSCC, we examined ABCG2 expression at the protein and mRNA levels,
as well as the function of ABCG2 in cell cultures by Western
blotting, real-time quantitative reverse transcription-polymerase
chain reaction (RT-PCR) and flow cytometry.
Positive ABCG2 expression was observed in HNSCC
tissues by immunohistochemistry. The level of ABCG2 expression was
associated with TNM stage and lymph node metastasis. Furthermore,
the level of ABCG2 protein and mRNA expression varied among the
Hep-2, Hep-2T, CNE and FaDu cell lines. Due to the negligible
expression and function of ABCG2 in the FaDu cell line, it is
suggested as a negative control cell line in HNSCC study.
Additionally, consistent with previous studies, fumitremorgin C
(FTC), a specific inhibitor of ABCG2, altered the sensitivity of
ABCG2-overexpressing cell lines to mitoxantrone.
Materials and methods
Cell lines and reagents
The CNE, Hep-2 and FaDu cell lines from human
nasopharyngeal, laryngeal and hypopharyngeal cancers, were obtained
from the American Type Culture Collection (ATCC). A taxol-resistant
cell line (Hep-2T) was developed by continuous exposure of Hep-2
cells to stepwise escalating concentrations of taxol for 12 months
(24). All of the cell lines were
cultured in Dulbecco's modified Eagle's medium (DMEM), supplemented
with 10% fetal bovine serum, 100 U/ml penicillin and 100 μg/ml
streptomycin at 37°C in a humidified atmosphere composed of 5%
CO2.
Mitoxantrone and FTC were purchased from
Sigma-Aldrich (USA). The monoclonal anti-ABCG2 antibody, BXP-21,
was purchased from Abcam (USA).
Immunohistochemistry
A panel of untreated HNSCC tissue samples, including
98 cases of laryngeal cancer, 40 cases of hypopharyngeal cancer and
34 cases of nasopharyngeal cancer tissues, was obtained from the
Shanghai Jiao Tong University Affiliated First People's Hospital,
with approval from the Research Ethics Committee of Shanghai Jiao
Tong University Affiliated First People's Hospital. Tissues were
fixed in formalin and embedded in paraffin. Serial sections (4-μm)
were cut and dried for 3 h at 60°C. Sections were then
deparaffinized with xylene and rehydrated through a graded series
of alcohol. Endogenous peroxidase was blocked with 3%
H2O2, and incubation was carried out with
normal goat serum for 30 min at room temperature. The sections were
incubated with BXP-21 (1:40 dilution) overnight at 4°C. After
washing with PBS, sections were incubated for 30 min with a
horseradish peroxidase-labeled polymer anti-mouse secondary
antibody. DAB was applied for 40 min to visualize immunolabeling,
resulting in a brown precipitate. After washing, the sections were
counterstained with hematoxylin. Negative controls involved
substitution of the primary antibody with PBS at the same
concentration.
Western blot analysis of ABCG2
Exponentially growing cells were washed two times
with ice-cold PBS, and lysed in RIPA buffer with protease inhibitor
PMSF for 30 min with occasional rocking followed by centrifugation
at 12,000 x g at 4°C for 15 min. Protein concentration of the
lysates was quantified by the BCA protein assay. Equal amounts of
protein (40 μg) were electrophoresed in 8% SDS-PAGE and transferred
to PVDF membranes (Millipore, Bedford, MA, USA). The membranes were
blocked for 1 h with 5% skim milk in PBS, and incubated with
anti-ABCG2 mouse monoclonal antibody BXP-21 diluted 1:20 in skim
milk at 4°C overnight. After washing, membranes were incubated with
the corresponding horseradish peroxidase-conjugated secondary
antibody (Pierce) diluted 1:20,000 in skim milk. The
immunocomplexes were visualized with an enhanced chemiluminescence
detection kit according to the manufacturer's instructions
(Pierce).
Real-time quantitative RT-PCR
Total cellular RNA was isolated from the Hep-2,
Hep-2T, CNE and FaDu cells using TRIzol reagent (Invitrogen).
Single-stranded oligo(dT)-primed cDNA was generated from 2 μg of
total RNA in a 20-μl reaction mixture. The primers used for the
analysis of ABCG2 were sense 5′-CTCAGTTTATCCGTGGTG-3′ and antisense
5′-AGATGATTGTTCGTCCCT-3′ (180 bp), and β-actin was used as an
internal standard (sense primer 5′-ATCATGTTTGAGACCTTCAA-3′ and
antisense primer 5′-CATCTCTTGCTCGAAGTCCA-3′; 318 bp). The
amplification reaction was carried out with 2 μl of cDNA product
for 27 cycles and each cycle consisted of 95°C for 45 sec, 56°C for
45 sec and 72°C for 45 sec, followed by a final 5-min elongation at
72°C. The final PCR products were electrophoresed on a 1.5% agarose
gel. Real-time RT-PCR was performed using a LightCycler rapid
thermal cycler system (Roche Diagnostics Ltd., Lewes, UK) according
to the manufacturer's instructions. Complementary DNA obtained from
2 μg RNA and 0.3 μl primers were included in the
LightCycler-FastStart DNA Master SYBR Green I mix (Roche
Diagnostics). The reaction condition was 40 cycles with
denaturation for 10 min at 95°C, annealing for 30 sec at 58°C and
extention for 45 sec at 72°C. To represent the ABCG2 expression
level, the ABCG2 mRNA expression index was used as calculated from
the following formula: Value of the ABCG2 gene copy/value of the
β-actin gene copy.
Cytotoxicity assay of cell survival
3-4,5-Dimethylthiazol-2-yl-2,5-diphenyltetrazolium
bromide (MTT) assay was employed to assess cell viability. MTT
assay is based on the ability of viable cells to reduce soluble
yellow MTT to blue formazan crystals. In this assay, the optical
density (OD) values represented the absorption of formazan
dissolved by dimethyl sulfoxide (DMSO) at 570 nm. Cells
(5x103 per well) were seeded in quintuplicate in a
96-well plate containing 150 μl culture complete medium. After 24 h
of incubation, different concentrations of mitoxantrone were added
to the designated wells after the addition of FTC (5 and 10 μM).
After 48 h of incubation, 20 μl of MTT (5 mg/ml) was added to each
well and the cells were further incubated for 4 h at 37°C. The
medium was removed and the product was dissolved in DMSO.
Absorbance was measured at 570 nm with a spectrophotometer. DMSO
(10%) was selected as a positive control for the cytotoxicity
studies.
IC50 values were calculated using SPSS
16.0 software. Each study was performed in triplicate and repeated
three times.
Drug accumulation assays
Cellular mitoxantrone accumulation was determined
according to the procedure originally reported by Allen et
al (25), with some
modifications. Briefly, 4×105 cells were seeded in
6-well plates 24 h prior to the experiment. Incubation with
mitoxantrone (0, 0.5, 1, 5 and 10 μg/ml) was performed for 60 min
at 37°C and 70–80% cellular confluency was achieved. Cells were
washed with ice-cold PBS, trypsinized and resuspended in medium at
a concentration of 4×105 cells/ml. Intracellular
fluorescence of mitoxantrone was determined by flow cytometry
(Becton Dickinson). To measure drug accumulation, cells were then
incubated with 0.5 μg/ml mitoxantrone for 1 h at 37°C in the
presence or absence of FTC (5 and 10 μM), which was used as an
inhibitor of ABCG2 in the four cell lines. The cells were excited
at 480 nm and emission was measured at 630 nm. A minimum of
104 cells was analyzed for each sample. All assays were
performed in at least three independent experiments, each time with
triplicate wells.
Statistical analysis
Categorical variables were evaluated by Pearson
Chi-square, continuity correction or Fisher's exact tests.
Spearman's rank correlation test was conducted to assess the
correlation between ordinal variables. The statistical software
SPSS 16.0 was used in data processing and analyzing the
significance using the Student's t-test, and a P-value <0.05
indicated the presence of a significant difference.
Results
ABCG2 expression in human HNSCC tissues
by immunohistochemistry
Patient epidemiological data, such as median age,
gender, tumor grade and stage and lymph node metastasis, were
summarized and analyzed (Table I).
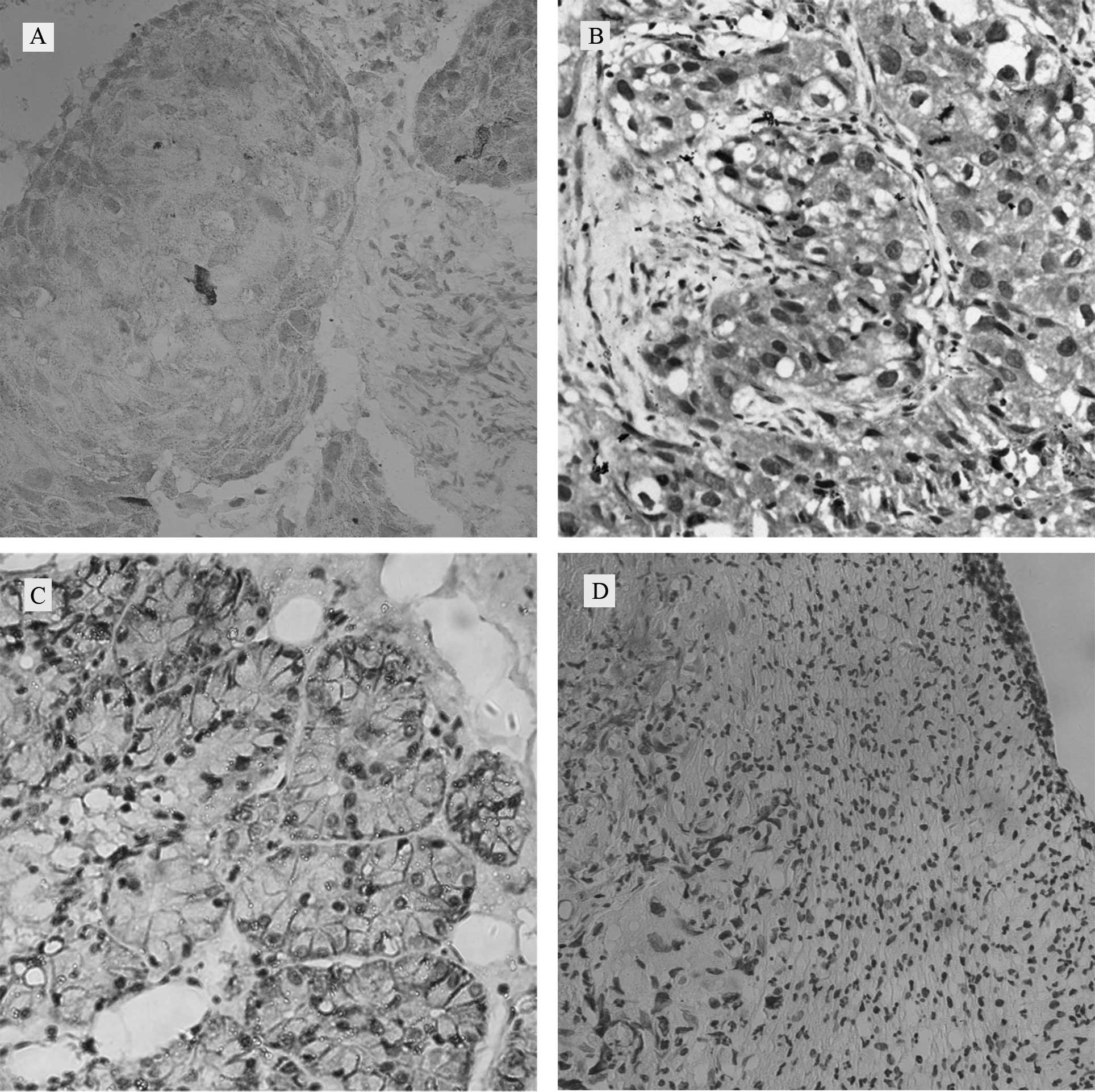
Positive protein expression of ABCG2 was noted in 52.04% of the
laryngeal, 65% of the hypopharyngeal and 58.82% of the
nasopharyngeal cancer specimens by immunohistochemistry.
ABCG2-positive tumors showed a mixed membranous and cytoplasmic
pattern of staining in HNSCC cells (Fig. 1A–C) compared to the negative
control of laryngeal cancer (Fig.
1D). Correlations between ABCG2 expression and patient
demographic data, as well as various prognostic factors, were also
investigated (Table I). High
expression of ABCG2 was significantly associated with TNM stage
(P<0.05) and lymph node metastasis (P<0.01) in the laryngeal
and nasopharyngeal cancers, while ABCG2 expression in
hypopharyngeal cancer was significantly associated only with lymph
node metastasis (P<0.01). In addition, an increasing trend
between ABCG2 expression and clinical TNM stage was noted in the
hypopharyngeal cancer.
 | Table ICorrelation between
clinicopathological parameters and ABCG2 expression in HNSCC. |
Table I
Correlation between
clinicopathological parameters and ABCG2 expression in HNSCC.
| Laryngeal cancer
(n=98) | Hypopharyngeal cancer
(n=40) | Nasopharyngeal cancer
(n=34) |
|---|
|
|
|
|
|---|
| Clinicopathological
parameter | n | ABCG2
| χ2 | P-value | n | ABCG2
| χ2 | P-value | n | ABCG2
| P-value |
|---|
| P | N | P | N | P | N |
|---|
| Gender | | | | 2.126 | 0.145 | | | | | 0.583 | | | | 0.551 |
| Female | 7 | 6 | 1 | | | 2 | 1 | 1 | | | 4 | 2 | 2 | |
| Male | 91 | 45 | 46 | | | 38 | 25 | 13 | | | 30 | 18 | 12 | |
| Age (years) | | | | 0.095 | 0.758 | | | | 3.095 | 0.079 | | | | 0.322 |
| <60 | 62 | 33 | 29 | | | 24 | 13 | 11 | | | 24 | 13 | 11 | |
| ≥60 | 36 | 18 | 18 | | | 16 | 13 | 3 | | | 10 | 7 | 3 | |
| Histological
grade | | | | 5.081 | 0.079 | | | | 1.849 | 0.397 | | | | 0.071 |
| I | 31 | 11 | 20 | | | 5 | 2 | 3 | | | 11 | 4 | 7 | |
| II | 51 | 31 | 20 | | | 23 | 15 | 8 | | | II + 23 | 16 | 7 | |
| III | 16 | 9 | 7 | | | 12 | 9 | 3 | | | III | | | |
| Clinical stage | | | | 5.587 | 0.018a | | | | 3.077 | 0.079 | | | | 0.018a |
| I–II | 68 | 30 | 38 | | | 5 | 1 | 4 | | | 21 | 9 | 12 | |
| III–IV | 30 | 21 | 9 | | | 35 | 25 | 10 | | | 13 | 11 | 2 | |
| Lymph node
status | | | | 10.078 | 0.002b | | | | 7.081 | 0.008b | | | | 0.007b |
| Positive | 22 | 18 | 4 | | | 33 | 25 | 8 | | | 29 | 20 | 9 | |
| Negative | 76 | 33 | 43 | | | 7 | 1 | 6 | | | 5 | 0 | 5 | |
Western blot analysis and real-time
RT-PCR analysis
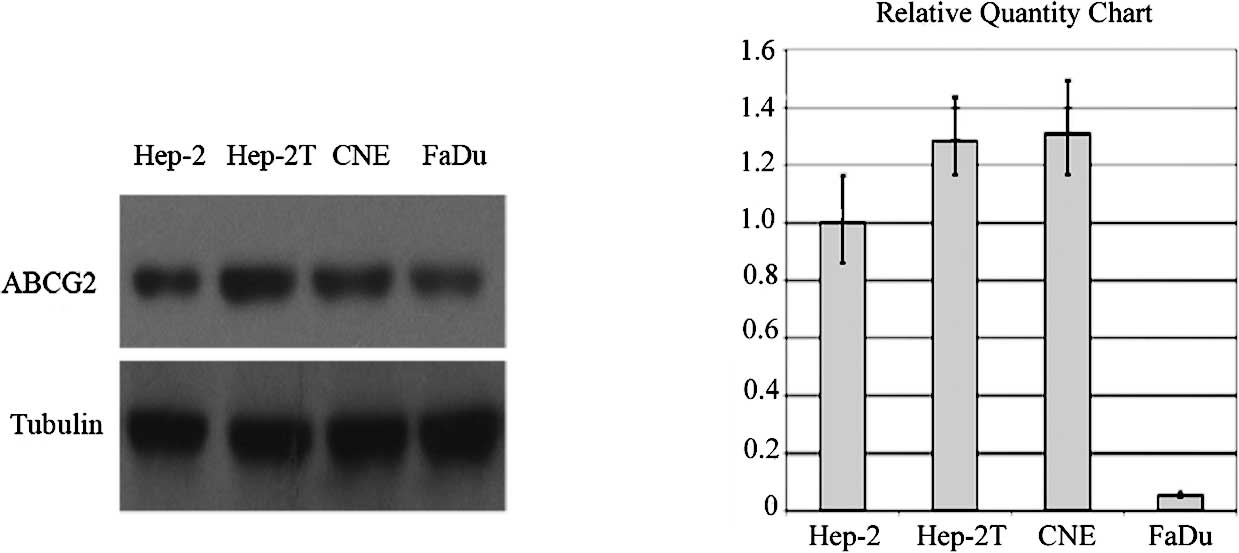
Fig. 2A illustrates
the results of the Western blot analysis of ABCG2 protein
expression in the Hep-2, Hep-2T, CNE and FaDu cell lines. Bands
detected by chemiluminescence were observed at ∼72 kDa
corresponding to ABCG2. The levels of ABCG2 markedly varied in the
four cell lines (Fig. 2A).
Real-time RT-PCR revealed that the relative
expression levels of ABCG2 mRNA in Hep-2, Hep-2T and CNE cells were
significantly higher than that in the FaDu cells (Fig. 2B).
The levels of ABCG2 mRNA were consistent with the
protein expression in the four cell lines. The taxol-resistant cell
line Hep-2T, which was verified by overexpression of P-gp,
presented a cross-resistance characteristic corresponding to a much
higher expression of ABCG2 than the Hep-2 cells. However, the FaDu
cell line exhibited a very low ABCG2 expression at both the protein
and mRNA level.
Cytotoxicity assay of cell survival
The sensitivity of the Hep-2, Hep-2T, CNE and FaDu
cell lines to mitoxantrone was assessed by MTT assay. The
IC50 values of mitoxantrone in the four HNSCC cell lines
during treatment alone or in combination with different FTC
concentrations are shown in Table
II. The fold-reversal value of mitoxantrone by 5 μM FTC in
Hep-2, Hep-2T and CNE cells was 2.75, 6.58 and 9.05, respectively.
By contrast, FTC did not increase the chemosensitivity of the FaDu
cells. As shown in Table II, FTC
at the indicated concentrations potently stimulated the activity of
mitoxantrone in the Hep-2, Hep-2T and CNE cell lines.
| Table IIEffect of FTC on ABCG2-mediated
resistance to mitoxantrone in the HNSCC cell lines. |
Table II
Effect of FTC on ABCG2-mediated
resistance to mitoxantrone in the HNSCC cell lines.
| Compounds | IC50 ±
SD μM
|
|---|
| Hep-2 | Hep-2T | CNE | FaDu |
|---|
| Mitoxantrone | 1.753±0.244
(1.00) | 1.817±0.259
(1.00) | 1.149±0.060
(1.00) | 1.133±0.540
(1.00) |
| +5 μM FTC | 0.638±0.016
(2.75)a | 0.276±0.047
(6.58)a | 0.127±0.053
(9.05)a | 1.126±0.620
(1.00) |
| +10 μM FTC | 0.632±0.032
(2.77)a | 0.289±0.054
(6.29)a | 0.093±0.048
(12.35)a | 1.265±0.427
(1.01) |
Mitoxantrone accumulation
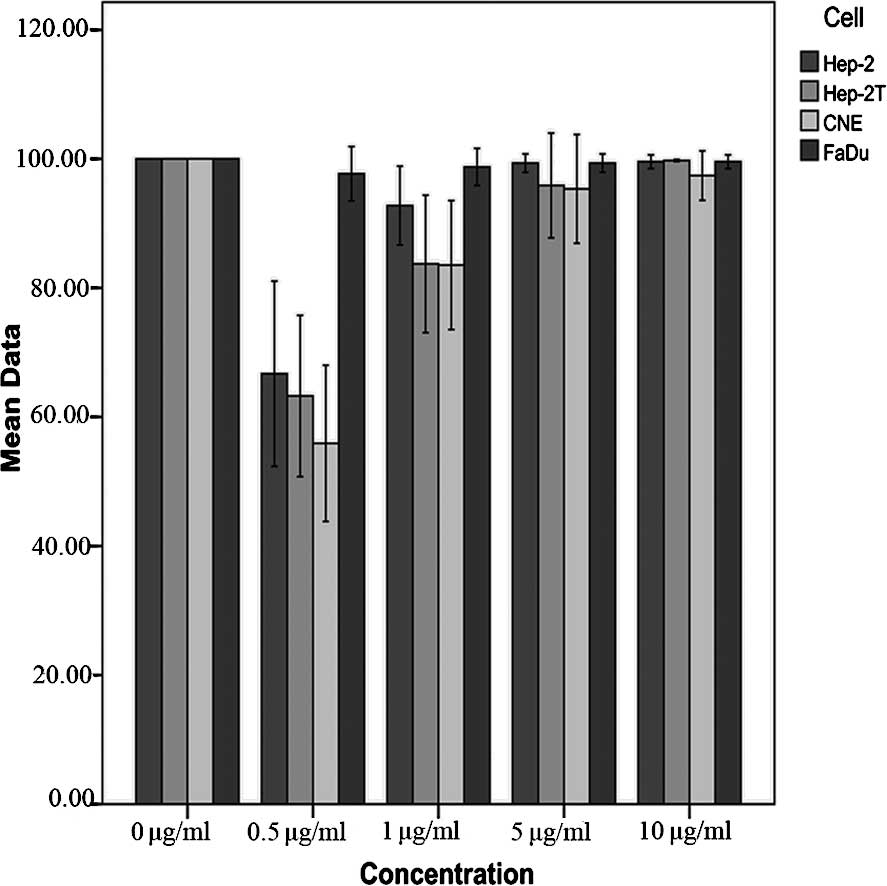
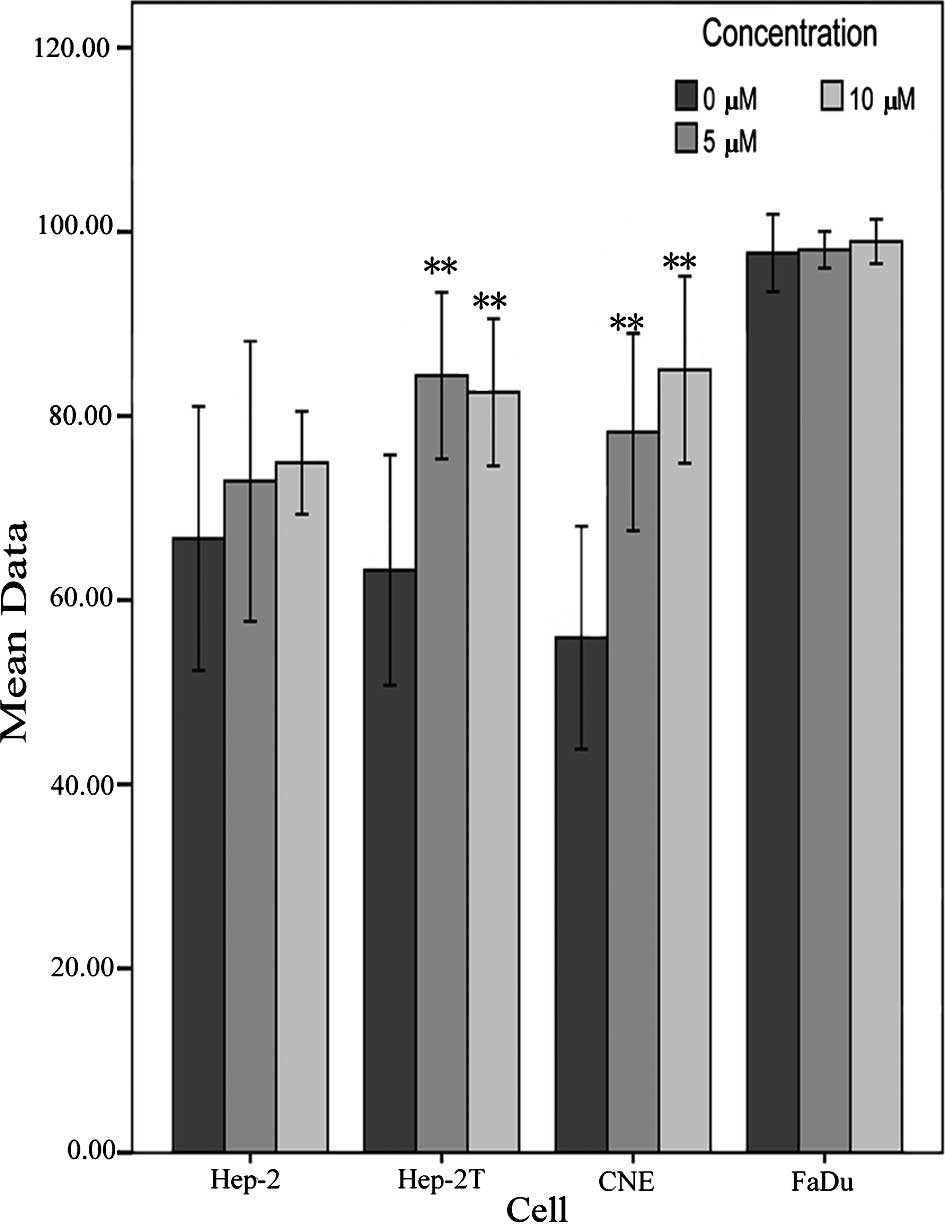
For the drug accumulation assay, a dose-dependent
profile was noted in the Hep2, Hep2T and CNE cells, while the FaDu
cell line showed a high level of mitoxantrone uptake. As shown in
Fig. 3, the mitoxantrone
fluorescence values were inversely correlated with ABCG2 mRNA
expression levels. When cells were treated in the presence of 5 and
10 μM FTC, the intracellular accumulation of mitoxantrone was 1.09-
and 1.12-fold higher in the Hep-2, 1.33- and 1.31-fold higher in
the Hep-2T, and 1.4- and 1.5-fold higher in the CNE cells. There
was no significant change in the intracellular accumulation of
mitoxantrone in the FaDu cells (Fig.
4).
Discussion
ABCG2 was discovered a decade ago and has been
extensively studied in laboratories worldwide, yielding a wealth of
knowledge akin to that gathered for P-gp (26). ABCG2 is a transmembrane transporter
that carries out the important biological function of the efflux of
multiple endogenous and exogenous substances out of cells. On
account of its ability to efflux multiple drugs, overexpression of
this protein has been associated with drug-resistant cancers
(5), including HNSCC.
In the present study, we first determined the
expression of ABCG2 in HNSCC tissues, and similar to the expression
in other cancer types, ABCG2-positive tumors showed a mixed
membranous and cytoplasmic pattern of staining in HNSCC cells
(Fig. 1A–C). In the 98 cases of
laryngeal carcinoma, 40 cases of hypopharyngeal carcinoma and 34
cases of nasopharyngeal carcinoma, the ABCG2-positive rate was 52,
65 and 58.8%, respectively. A significant correlation was found
between ABCG2 expression and clinical stage and lymph node
metastasis. In accordance with research in acute myeloid leukemia
(11,27,28),
adult acute lymphoblastic leukemia (29), non-small cell lung cancer (15) and esophageal squamous cell
carcinoma (14), positive
expression of ABCG2 may accelerate progression and metastasis in
HNSCC. However, no significant correlation, only an increasing
trend between ABCG2 expression and histological grade, was observed
in the tumor tissues of the laryngeal and nasopharyngeal cancers.
Theoretically, the chemosensitivity of carcinomas usually increases
with increasing histological grade. Thus, our results revealed that
the drug sensitivity of HNSCC cells is a multifactorial phenomenon,
which is determined not only by ABCG2, but by other ABC
transporters, such as P-gp. As stated above, it has been
demonstrated that ABCG2 may have an effect on disease progression
and drug resistance, and it may be an unfavorable prognostic factor
of HNSCC. Although the use of targeted molecular agents to cure
cancer is promising, one challenge involves the discovery of
biomarkers of tumors (30). To our
knowledge, this is the first study to investigate the prognostic
value of ABCG2 expression in three HNSCC cell lines,
simultaneously.
In vitro, ABCG2 confers drug resistance
against a variety of anticancer drugs and isolates stem cell-like
side population cells, which may both act as an efflux pump.
However, the level of expression of ABCG2 in HNSCC cell lines is
not known. In the present study, we evaluated the expression of
ABCG2 in four HNSCC cell lines by Western blotting and real-time
quantitative RT-PCR (Fig. 2A and
B). According to the molecular biological results, the Hep-2T
cell line exhibited the highest expression level of ABCG2 protein,
followed by CNE, Hep-2 and FaDu cells (Fig. 2A). Consistent with other reports
(31,32), the levels of mRNA expression were
correlated with the levels of protein expression (Fig. 2B). Based on the above results, we
infer that the drug resistance of Hep-2T cells to taxol is not
mainly caused by an increased gene and protein level of P-gp
expression, but simultaneously by an increased level of ABCG2
expression. Consequently, we found that resistance to a single
chemotherapeutic agent may result in cross-resistance to various
structurally and functionally dissimilar drugs, as well as elevated
expression of different ABC transporters.
In an attempt to evaluate the contribution of
resistance-related molecule ABCG2, we examined the anticancer drug
sensitivity of Hep-2, Hep-2T, CNE and FaDu cell lines to
mitoxantrone, as well as the effect of FTC, a specific inhibitor of
ABCG2, on the drug sensitivity of the above four HNSCC cell lines
(Table II). The results revealed
that the ABCG2 protein and mRNA levels reflect the functional
activity of ABCG2, and the ability of FTC to reverse these effects
may be specific to ABCG2 in HNSCC cell lines. The inhibitor of FTC
was not toxic in the four cell lines tested in this study (data not
shown). These results clearly demonstrate that inhibition of FTC is
more effective in drug-resistance cell lines than in their parental
cells. Consistent with cytotoxicity data, the results of the drug
accumulation studies showed that FTC strongly enhanced the
intracellular accumulation of mitoxantrone in the
ABCG2-overexpressing cells. The results confirmed that mitoxantrone
is a specific substrate for ABCG2 and FTC is a specific inhibitor
of ABCG2 in HNSCC cell lines.
Moreover, the FaDu cell line did not show obvious
expression and function of ABCG2. These results indicate that the
FaDu cell line may be suitable as a negative control for the study
of ABCG2 in HNSCC cell lines in further investigations.
It is well known that tumors are composed of
heterogeneous cell types. Evidence suggests that carcinoma is a
disease of stem cells and, similar to normal organs, contains a
small population of cells with high proliferative capacity,
self-renewing potential, multidifferentiation ability and
resistance to chemotherapy and radiotherapy. This has catalyzed a
shift towards using targeted therapies for cancer. To date,
side-population phenotype cells, which exhibit many characteristics
of stem cells, were selected in a wide variety of normal tissues
and tumors in an attempt to understand the biological properties of
cell types in HNSCC (33,34). Distinct molecular markers of cancer
stem cells were absent in these cells, and there is increasing
evidence suggesting that they may play an important role in
tumorigenesis and cancer therapy.
In conclusion, the results of the present study
confirmed that ABCG2 is widely present in untreated HNSCC cells,
raising the possibility that ABCG2 may be a simple independent
unfavorable prognostic factor for HNSCC, and may be a clinically
relevant mechanism of anticancer drug resistance. We also confirmed
ABCG2 expression and its efflux pump function in HNSCC cell lines;
the specific inhibitor of FTC decreased the expression of ABCG2,
resulting in an increase in the intracellular concentration of
mitoxantrone. Moreover, the FaDu cell line is potentially a
suitable negative control for further study of the role of ABCG2 in
HNSCC. In future studies, we will focus on the function and
characteristics of side-population cells in HNSCC.
Acknowledgments
The authors are grateful to Dr Jiawei Chen and Dr
Honghui Hu of the Department of Pathology, Shanghai Jiaotong
University Affiliated First People's Hospital, for the database of
clinical indices and the technical assistance. They also thank Ms.
Yu-Ying Chen of the Morphology and Cell Chemistry Laboratory of
Shanghai Jiao Tong University School of Medicine, for her
assistance in the immunohistochemistry. This study was supported by
the Shanghai Science and Technology Development Fund (no.
09411951000) and the Resource Sharing Platform for Clinical
Research (no. SHDC12007206), China.
References
|
1
|
Greenlee RT, Murray T, Bolden S and Wingo
PA: Cancer statistics, 2000. CA Cancer J Clin. 50:7–33. 2000.
View Article : Google Scholar
|
|
2
|
Vokes EE, Weichselbaum RR, Lippman SM and
Hong WK: Head and neck cancer. N Engl J Med. 328:184–194. 1993.
View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Clark JI, Hofmeister C, Choudhury A, et
al: Phase II evaluation of paclitaxel in combination with
carboplatin in advanced head and neck carcinoma. Cancer.
92:2334–2340. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Dean M, Hamon Y and Chimini G: The human
ATP-binding cassette (ABC) transporter superfamily. J Lipid Res.
42:1007–1017. 2001.PubMed/NCBI
|
|
5
|
Ross DD and Nakanishi T: Impact of breast
cancer resistance protein on cancer treatment outcomes. Methods Mol
Biol. 596:251–290. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Doyle LA, Yang W, Abruzzo LV, et al: A
multidrug resistance transporter from human MCF-7 breast cancer
cells. Proc Natl Acad Sci USA. 95:15665–15670. 1998. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Diestra JE, Condom E, del Muro XG, et al:
Expression of multidrug resistance proteins P-glycoprotein,
multidrug resistance protein 1, breast cancer resistance protein
and lung resistance-related protein in locally advanced bladder
cancer treated with neoadjuvant chemotherapy: biological and
clinical implications. J Urol. 170:1383–1387. 2003.
|
|
8
|
Sauerbrey A, Sell W, Steinbach D, Voigt A
and Zintl F: Expression of the BCRP gene (ABCG2/MXR/ABCP) in
childhood acute lymphoblastic leukaemia. Br J Haematol.
118:147–150. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Abbott BL, Colapietro AM, Barnes Y, Marini
F, Andreeff M and Sorrentino BP: Low levels of ABCG2 expression in
adult AML blast samples. Blood. 100:4594–4601. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Plasschaert SL, van der Kolk DM, de Bont
ES, et al: The role of breast cancer resistance protein in acute
lymphoblastic leukemia. Clin Cancer Res. 9:5171–5177.
2003.PubMed/NCBI
|
|
11
|
Benderra Z, Faussat AM, Sayada L, et al:
Breast cancer resistance protein and P-glycoprotein in 149 adult
acute myeloid leukemias. Clin Cancer Res. 10:7896–7902. 2004.
View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Nakayama K, Kanzaki A, Ogawa K, Miyazaki
K, Neamati N and Takebayashi Y: Copper-transporting P-type
adenosine triphosphatase (ATP7B) as a cisplatin-based
chemoresistance marker in ovarian carcinoma: comparative analysis
with expression of MDR1, MRP1, MRP2, LRP and BCRP. Int J Cancer.
101:488–495. 2002. View Article : Google Scholar
|
|
13
|
Faneyte IF, Kristel PM, Maliepaard M, et
al: Expression of the breast cancer resistance protein in breast
cancer. Clin Cancer Res. 8:1068–1074. 2002.PubMed/NCBI
|
|
14
|
Tsunoda S, Okumura T, Ito T, et al: ABCG2
expression is an independent unfavorable prognostic factor in
esophageal squamous cell carcinoma. Oncology. 71:251–258. 2007.
View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Yoh K, Ishii G, Yokose T, et al: Breast
cancer resistance protein impacts clinical outcome in
platinum-based chemotherapy for advanced non-small cell lung
cancer. Clin Cancer Res. 10:1691–1697. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Jin Y, Bin ZQ, Qiang H, et al: ABCG2 is
related with the grade of glioma and resistance to mitoxantone, a
chemotherapeutic drug for glioma. J Cancer Res Clin Oncol.
135:1369–1376. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Polgar O, Robey RW and Bates SE: ABCG2:
structure, function and role in drug response. Expert Opin Drug
Metab Toxicol. 4:1–15. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Honjo Y, Hrycyna CA, Yan QW, et al:
Acquired mutations in the MXR/BCRP/ABCP gene alter substrate
specificity in MXR/BCRP/ABCP-overexpressing cells. Cancer Res.
61:6635–6639. 2001.PubMed/NCBI
|
|
19
|
Robey RW, Honjo Y, Morisaki K, et al:
Mutations at amino-acid 482 in the ABCG2 gene affect substrate and
antagonist specificity. Br J Cancer. 89:1971–1978. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Ejendal KFK, Diop NK, Schweiger LC and
Hrycyna CA: The nature of amino acid 482 of human ABCG2 affects
substrate transport and ATP hydrolysis but not substrate binding.
Protein Sci. 15:1597–1607. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Miwa M, Tsukahara S, Ishikawa E, Asada S,
Imai Y and Sugimoto Y: Single amino acid substitutions in the
transmembrane domains of breast cancer resistance protein (BCRP)
alter cross resistance patterns in transfectants. Int J Cancer.
107:757–763. 2003. View Article : Google Scholar
|
|
22
|
Song J, Chang I, Chen Z, Kang M and Wang
CY: Characterization of side populations in HNSCC: highly invasive,
chemoresistant and abnormal Wnt signaling. PloS One. 5:e114562010.
View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Schwabedissen HE and Kroemer HK: In vitro
and in vivo evidence for the importance of breast cancer resistance
protein transporters (BCRP/MXR/ABCP/ABCG2). Handb Exp Pharmacol.
201:325–371. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Li L, Jiang AC, Dong P, Wan Y and Yu ZW:
The characteristics of Hep-2 cells with multiple drug resistance
induced by Taxol. Otolaryngol Head Neck Surg. 137:659–664. 2007.
View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Allen JD, van Loevezijn A, Lakhai JM, et
al: Potent and specific inhibition of the breast cancer resistance
protein multidrug transporter in vitro and in mouse intestine by a
novel analogue of fumitremorgin C. Mol Cancer Ther. 1:417–425.
2002.
|
|
26
|
Robey RW, To KK, Polgar O, et al: ABCG2: a
perspective. Adv Drug Deliv Rev. 61:3–13. 2009. View Article : Google Scholar
|
|
27
|
Benderra Z, Faussat AM, Sayada L, et al:
MRP3, BCRP, and P-glycoprotein activities are prognostic factors in
adult acute myeloid leukemia. Clin Cancer Res. 11:7764–7772. 2005.
View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Uggla B, Stahl E, Wagsater D, et al: BCRP
mRNA expression v. clinical outcome in 40 adult AML patients. Leuk
Res. 29:141–146. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Suvannasankha A, Minderman H, O'Loughlin
KL, et al: Breast cancer resistance protein (BCRP/MXR/ABCG2) in
acute myeloid leukemia: discordance between expression and
function. Leukemia. 18:1252–1257. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Sawyers CL: The cancer biomarker problem.
Nature. 452:548–552. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Maliepaard M, Scheffer GL, Faneyte IF, et
al: Subcellular localization and distribution of the breast cancer
resistance protein transporter in normal human tissues. Cancer Res.
61:3458–3464. 2001.PubMed/NCBI
|
|
32
|
Young LC, Campling BG, Cole SPC, Deeley RG
and Gerlach JH: Multidrug resistance proteins MRP3, MRP1, and MRP2
in lung cancer: correlation of protein levels with drug response
and messenger RNA levels. Clin Cancer Res. 7:1798–1804.
2001.PubMed/NCBI
|
|
33
|
Hirschmann-Jax C, Foster AE, Wulf GG, et
al: A distinct ‘side population’ of cells with high drug efflux
capacity in human tumor cells. Proc Natl Acad Sci USA.
101:14228–14233. 2004.
|
|
34
|
Haraguchi N, Utsunomiya T, Inoue H, et al:
Characterization of a side population of cancer cells from human
gastrointestinal system. Stem Cells. 24:506–513. 2006. View Article : Google Scholar : PubMed/NCBI
|