Introduction
Meningiomas are abundant in the blood supply.
Manelfe et al (1) divided
meningiomas (based mainly on the external or internal carotid
artery) into four types according to the arterial blood supply.
Several scholars (2–4) have performed studies on the blood
supply of meningiomas through digital subtraction angiography
(DSA). In meningiomas fed by a single internal or external carotid
artery, DSA imaging clearly reveals the staining and arteriovenous
branches of the tumor, but those fed by both an internal and
external carotid artery cannot be displayed well as the image does
not show both sides simultaneously. Multi-slice spiral CT vascular
imaging involves a contrast injection to the full arterial and
venous phases to fully stain the tumor and display dual feeding
arteries and reflux veins, and has received attention from a number
of researchers (3,5,6). To
understand the advantages and disadvantages of multi-slice CT
angiography (MSCTA) and DSA in the angiography of meningiomas, a
comparative study of the two methods in the detection of meningioma
blood supply was performed.
Materials and methods
General materials
Twenty inpatients in our hospital diagnosed with
meningioma by CT or MR underwent MSCTA and DSA at the same time.
The inspection interval was 1 week. Among 20 patients, 11 tumors
were convex, 3 in the midline falx and 6 in the infratentorial
(including the saddle, anterior and posterior cranial fossa and
cerebellopontine angle area), including 3 cases in the near side of
venous sinuses. Patients included 8 men and 12 women, aging from 17
to 74 years. The size of the largest tumor was 120×110×800 mm,
while that of the smallest was 35×32×27 mm.
Equipment and contrast agent
The CT machine used was the Somatom Sensation
16-slice spiral CT machine. DSA was performed using the Advantx
Lc/Lp DLX Dual C-arm DSA machine (GE, USA). The contrast agent used
was iopamidol (370 mg/ml).
Examination methods
Multi-slice spiral CT examination and
three-dimensional reconstruction: Informed consent was obtained
from all patients prior to the study. We then succesfully
eliminated their emotional tension. Patients were placed in the
supine position on the check-bed and initially plain-scanned to
determine the scan range. The scan field generally ranged from the
skull base to the calvaria. Patients underwent a contrast-enhanced
scan. Scan parameters were 120 kv, 200 mAs, slice thickness 2 mm
and collimation 16×0.75 mm. Contrast agent automatic tracking
technology was used. A high pressure injector was applied to inject
80–100 ml (370 mg/ml) iopamidol through the elbow vein at the rate
of 3 ml/sec. Reconstruction slice was 0.75 mm, with a spacing of
0.75 mm. Reconstruct multiplanar reformations (MPR), maximum
intensity projection (MP), shaded surface display (SSD) and volume
rendering technique (VRT) were conducted on the Wizard
workstation.
DSA inspection
Informed consent was obtained from all patients
prior to the study. We then succesfully eliminated their emotional
tension. Tranquilizers were used in agitated patients prior to the
examination. Using the Seldinger technique, a 4F VER angiography
catheter was inserted via the right femoral arterial approach, and
placed in a 5F arterial sheath. The left and right carotid arteries
and the left and right vertebral arteries were selected to perform
contrast radiography. The high-pressure injection method was used
and we selected iopamidol (370 mg/ml) as the contrast agent.
Contrast agent dosage was as follows: carotid angiography flow rate
of 5 ml/sec, with a total of 7 ml each time; vertebral angiography
flow rate of 4 ml/sec, with a total volume of 6 ml each time. The
orthophoric and lateral images were taken.
Data analysis
Two veteran radiologists analyzed two types of
imaging data. One radiologist knew the medical history, but did not
know the DSA results. The other took DSA as the ‘gold standard’ to
evaluate the diagnostic sensitivity and specificity of CTA, and
assessed the differences between the two imaging methods in the
meningiomas’ feeding arteries, draining veins and the adjacent
sinus invasion or extent of invasion, as well as the spatial
relationship between the tumor and great intracranial blood
vessels. The specific observation methods were: i) the performance
of the two techniques in displaying the feeding arteries of the
tumor and the main branches of the brain arteries adjacent to the
tumor, including the clarity of display of the arteries (comparison
between tumor body and arteries in density and signal differences),
the displayed number of arteries, artery embedding, compression and
erosion and the existence of dissimilar observation results due to
different pathogenic sites. ii) Comparative evaluation of draining
veins, including the number of displayed draining veins, displaying
clarity, characteristics of the joint between the draining veins
and the tumor body, flow direction of the draining veins and the
richness of the peripheral compensatory perforator veins. iii)
Comparative evaluation of venous sinuses, including the clarity of
the display of the relationship between parasagittal sinus
meningiomas and venous sinuses, sinus damage, indicating violation
of the integrity of the sinus. iv) Comparative evaluation of
surrounding tissues, including the contrast of the degree of
enhancement of the tumor body, the degree of the tumor compression
and invasion of the surrounding brain tissues, and the effect of
the tumor on the adjacent bones.
Results
Arterial blood supply of tumors
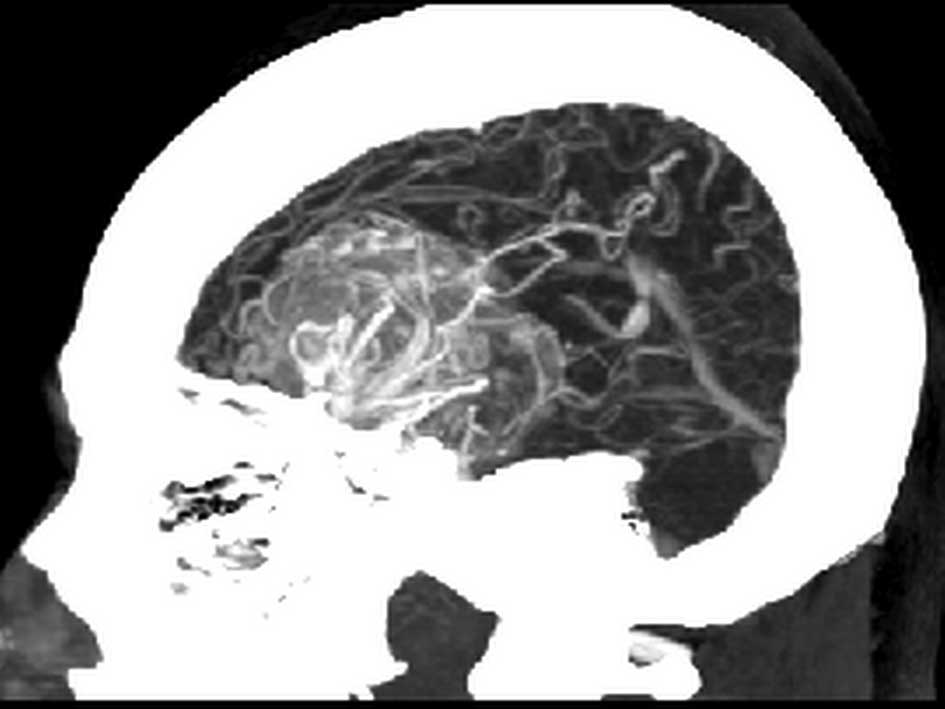
In 20 cases of meningiomas, MSCTA and DSA images
were both clear in displaying the feeding arteries of the tumor.
The feeding arteries around the tumor were connected to the body in
clusters or arcuses, and then branched into the tumor body
(Fig. 1). MSCTA achieved the DSA
imaging effects by adjusting displaying angles, clearly displaying
intracranial branches of class IV or above. DSA displayed more
peritumoral minor arteries than MSCTA. Both examination methods
revealed that the intracranial arteries were involved in blood
supply in 12 cases.
Relationship between tumor and its
peripheral vessels
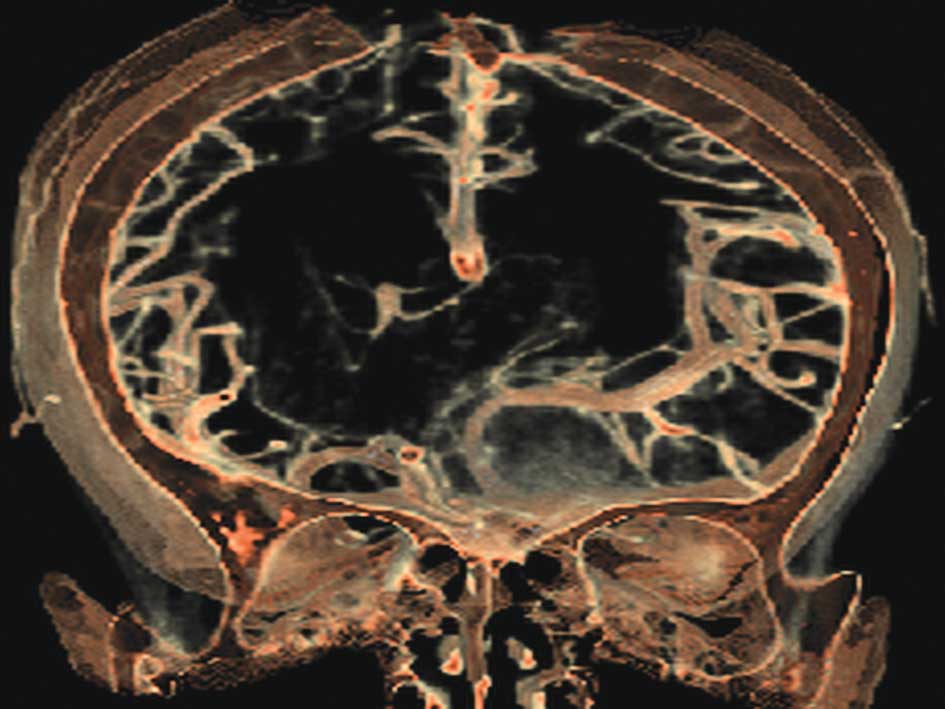
In this study, tumor body in 16 cases was closely
related to its adjacent intracranial arteries (including the
oppression and embedding of the tumor on the main arterial
branches). The first-class branches of Willis’ arteries were
compressed and shifted in 7 cases. The middle cerebral artery was
shifted and distorted by temporal meningiomas in 4 cases, and
certain branches turned into significant distortion (Fig. 2). The anterior cerebral artery was
shifted to the opposite side by arched compression in 2 cases. The
anterior cerebral artery was shifted under the pressure in 1 case
and some branches were involved in feeding the tumor. The MPR
reconstruction technology of MSCTA was good at displaying the
three-dimensional relationship between the tumor and other blood
vessels.
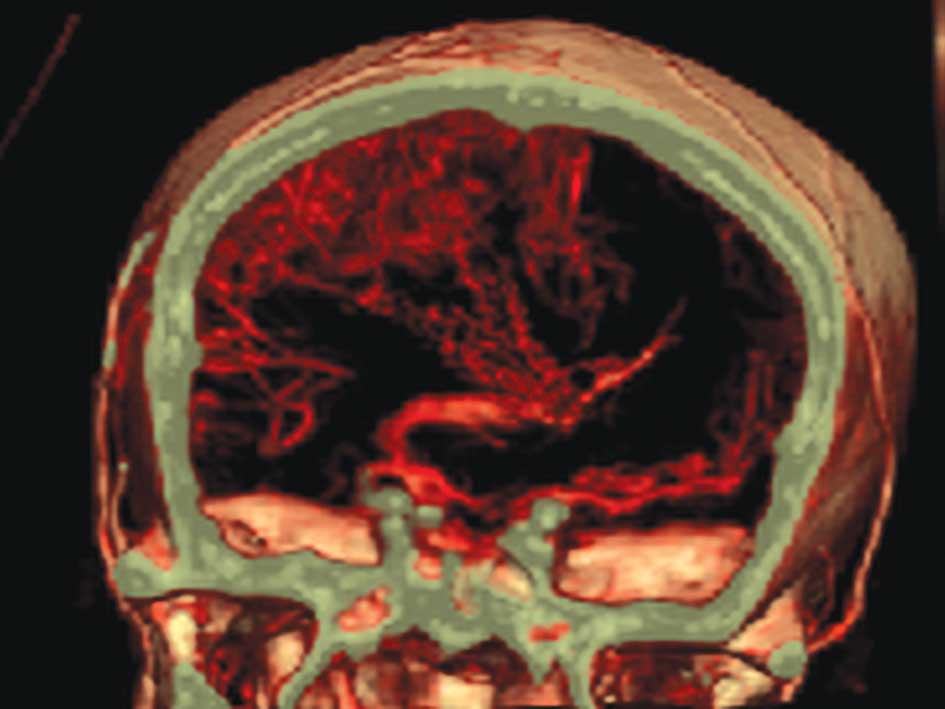
Draining veins of the tumor
DSA provided information regarding venous drainage,
especially small reflux veins. The MSCTA examination of 20 cases
was also able to clearly display the morphology, abundance,
drainage of the reflux veins of the tumor and the relationship
between veins and venous sinuses. Veins surrounded the tumor or
connected it in clusters, and therefore provided important clinical
information, such as venous drainage into the adjacent sagittal
sinus or the superficial and deep cranial veins (Fig. 3).
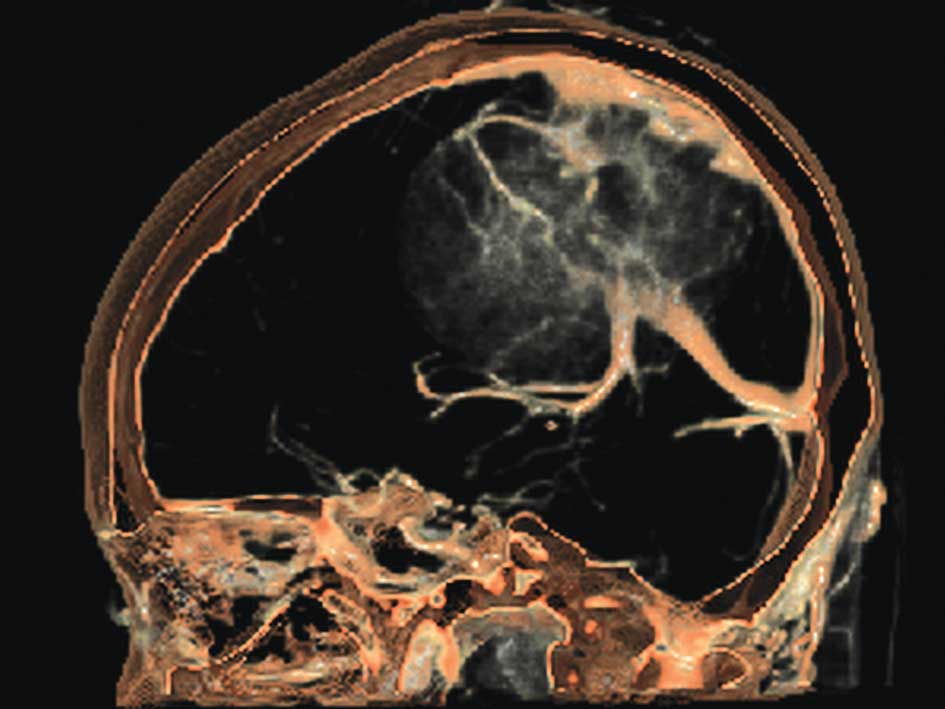
Displaying situation of venous sinus in
parasagittal sinus meningiomas
Of the 20 cases, 8 were parasagittal sinus
meningiomas. Both DSA and MSCTA showed the relationship between
tumor body and venous sinus, as well as clinical information, such
as the violation, stenosis and truncation of the venous sinus,
including 5 cases near the superior sagittal sinus (3 cases of
invasion), and 1 sigmoid sinus. However, in 4 cases of invasion,
the invasion of the sinus cavity of 1 case was overestimated by
MSCTA due to the impact of bone structure (Fig. 4).
Relationship between the tumor and its
adjacent bone
In 20 cases, MSCTA completely displayed the
anatomical relationship between the tumor and its adjacent skull,
as well as the impact of the tumor on the bone structure. Eight
cases showed thickening of bone structure, while 3 cases displayed
thinning. Both thinning and thickening of bone structure existed in
2 cases, while 7 cases were not affected. In contrast to MSCTA, DSA
provided little useful information on the relationship between the
tumor and its adjacent bone.
Imaging of MSCTA compared to DSA
Tumor staining, arterial display, venous sinus
invasion and the relationship between the tumor and its peripheral
vessels are shown in Table I. A
good display of arteries was one which revealed arteries of class
IV or above. Venous display involved showing the superior veins
above the reflux veins, the good clarity of venous sinuses and the
depiction of the changes of peritumoral vessels involved in the
tumor’s compression, pushing and violation.
 | Table IComparison of the tumor displaying
between the two methods. |
Table I
Comparison of the tumor displaying
between the two methods.
| Methods | Complete tumor
staining (N1=20) No. (%) | Arterial display
(N1=20) No. (%) | Venous display
(N1=20) No. (%) | Venous sinus display
(N1=8) No. (%) | Changes of
peritumoral vessels (N1=16) No. (%) |
|---|
| MSCTA | 20 (100) | 19 (95.5) | 18 (90) | 7 (87.5) | 16 (100) |
| DSA | 8 (25) | 20 (100) | 15 (75) | 8 (100) | 10 (62.5) |
Discussion
Importance of angiography in
meningiomas
The primary treatment method for meningioma is
surgery, although inadequate preparation often causes massive
hemorrhage, leading to unnecessary risks. Angiography of
meningiomas provides clinical information, such as the tumor’s
feeding arteries, the fate of venous drainage, changes of venous
sinuses and its adjacent main cerebral arteries before surgery,
enabling surgeons to fully understand the circumstances that may be
encountered during surgery, thus making sure that they have a well
thought-out plan, avoiding accidents due to a lack of preparedness.
Therefore, increasing attention is being paid to angiography in
clinical practice. Previously, DSA was mainly used for the
angiography of meningiomas, but DSA had obvious disadvantages, such
as iatrogenic vascular injury, radiation exposure, side-effects and
complications of contrast agents, as well as high cost, and thus
was not very easily accepted by patients. With the emergence and
development of multi-slice spiral CT, this relatively non-invasive
examination technology is being approved by more and more doctors
and patients. The application of DSA for the vascular diagnosis of
meningioma is decreasing (4),
although in some respects, DSA continues to play an irreplaceable
role. In this study, we applied multi-slice spiral CT to image the
blood supply of meningiomas and compared MSCTA and DSA in various
aspects, to explore the application value and advantages of the two
methods in imaging the blood supply of meningiomas.
Application of DSA in meningiomas
As the ‘gold standard’ of angiography, DSA still
plays an important role as it is able to directly and faithfully
observe the narrow, fine branches and the existence of invasion,
stretch and embedding in blood vessels. According to the DSA
imaging of meningiomas, we can analyze whether the blood supply is
abundant, and whether there is risky intracranial-extracranial
anastomosis in different parts of the tumor and its feeding
arteries. Based on such observation, pre-operative embolization
treatment can be implemented in selected suitable cases. Therefore,
DSA enables us to better grasp the indications of selective
external carotid artery embolization, improve efficacy and reduce
complications. However, the shortcomings of DSA are also evident.
Among the cases in our study, 12 out of 20 cases presented with
dual arterial blood supply by the internal and external carotid
artery. During DSA imaging, the catheter was first placed in the
external carotid artery and then into the internal carotid artery
for imaging. Such a time lag meant that we could not reveal the
dual arterial blood supply simultaneously. Singly-displaying the
infusion of contrast agent in the arteries while being unable to
display the other set of arteries supplying the blood caused
insufficient tumor staining (Fig.
1D). A similar problem occurred in the veins. DSA cannot
display the full view of the tumor and its exact location or the
relationship between the tumor and the skull. Invasion, radiation
and high cost also affect the acceptance by the examinees.
Application of MSCTA in meningiomas
The multi-slice spiral CT is receiving more and more
acceptance from doctors and patients. At present, MSCTA is being
widely used in clinical practice. Vascular imaging applied to all
parts of the body provides important information for clinicians,
and vascular imaging of meningiomas has been widely used at home
and abroad (5,7). MSCTA has certain advantages, such as
its non-invasiveness, and has fewer complications. After one
enhanced scan, an arbitrary point can be chosen to reconstruct the
multi-dimensional image of the lesion, to determine the causes of
vascular compression and the extent of compression. In particular,
three-dimensional helical CT angiography (3D-CTA) applies a
continuous, rapid, non-interval spatial data scanning technique to
obtain high-quality three-dimensional images. Because of the faster
scanning speed, the ion radiation and the contrast agent use is
significantly reduced, while the application of the contrast agent
tracking trigger technique renders the scan delay time more
accurate, thus obtaining higher quality images. In this study, 20
cases of meningiomas underwent MSCTA examination. Contrast medium
intelligent tracking technology was applied, ordering the scanning
to be automatically triggered 5 sec after the threshold (set as the
carotid artery, generally 100 Hu) was reached, starting from the
extracranial parts of the common carotid artery, including the
whole brain. This method has proven to be clinically feasible
(8). MSCTA scans in the arterial
phase and the venous phase and displays the tumor staining and
blood supply in the different phases. It can also reveal the
relationship between the tumor body and peripheral vessels and
skull by adjusting different thresholds (Fig. 2E), providing comprehensive clinical
information.
Contrast between MSCTA and DSA
MSCTA has a relatively high spatial resolution. It
can reveal intracranial arterial circles of class IV and above, and
can clearly display abnormal meningeal and intracranial feeding
branches, which is sufficient to meet the clinical requirements for
displaying vessels of interest. The results are consistent with the
DSA imaging. MSCTA also has a high temporal resolution. Scanning
time from the base of the skull to the calvaria was not more than
10 sec. Additionally, contrast medium intelligent tracking
technology was adopted. Therefore, there were fewer opportunities
for venous pollution: there were only 2 cases among 20 patients
that had arteriovenous hybrid imaging. However, this did not affect
the clinical diagnosis. As the cerebral veins have high imaging
speed, the venous phase can be obtained by scanning immediately
after the arterial phase. MSCTA imaging in cerebral veins has been
widely recognized by clinicians (5,7),
which can clearly display the shape, abundance and drainage fate of
draining veins (Fig. 4). In this
study, 18 out of 20 cases showed a clear-cut venous system, while
in the remaining 2 cases, the tumors’ lack of blood supply proved
to be a rare arteriovenous blood supply by later surgery.
In this study, when performing DSA with unilateral
and one-leg angiography, we found that certain parts of the tumor
were not stained, particularly when the branches of the internal
and external carotid arteries were all involved in feeding the
tumor. MSCTA scans with the contrast agent completely infiltrated
into the interstitial tissue of the tumor by delayed scan.
Therefore, the extent of tumor staining in MSCTA is stronger than
in DSA. It reflects the blood abundance of the tumor body, thus
providing a reference for the clinical understanding of the tumor
blood supply, as well as judgments of pre-operative embolization.
To obtain the complete staining of the tumor, dual angiography
should be implemented by scanning the internal and external carotid
artery at the same time, although this increases the damage and
dosage of the contrast agent.
As there is no bone structure impact in parasagittal
sinus meningiomas, DSA shows obvious superioriy in displaying
circumstances, such as the changes of sinus cavity and
establishment and the improvement of the collateral venous
circulation path, as well as the complete display of vessels
adjacent to the skull. In this study, among 8 cases of parasagittal
sinus meningiomas, 5 cases revealed sinus cavity invasion. DSA
provided accurate and three-dimensional information about sinus
cavity invasion. MSCTA only displays the general profile of the
venous sinus. Due to the sinus bone structure, it is difficult to
assess the narrow sinuses at the bone side, assaults and the tumor
thrombus. The bone subtraction algorithm not only is time
consuming, but also affects the venous sinuses, as enhanced vessels
have similar density to bones, while other factors also exist. In
this study, among 8 cases of venous sinus invasion, 1 case of
meningioma that MSCTA had difficulties in diagnosing was due to the
extent of the damage of the venous sinuses, the size of the tumor
thrombus and stenosis of the sinus, as well as bone artifacts and
partial volume effects. Meanwhile, DSA shows clear superiority in
displaying vessels adjacent to the skull. In the same plane, it can
provide a complete and three-dimensional image of the running
characteristics of blood vessels near the skull side. In this
study, DSA completely showed 26 blood vessels near the skull side
in the same plane, but MSCTA showed only 12 due to the bony
interference. Therefore, when no surrounding tissues are
interfering, DSA does better in displaying vascular change features
near the skull side than MSCTA (including vascular courses, the
extent of compression and three-dimensional information). With
regard to the relationship between tumor body and its peripheral
vessels, MSCTA shows better performance. It provides stereoscopic
imaging of displacement and compression between the tumor and
vessels by MPR, VRT and other three-dimensional reconstruction
technology, so as to provide clear and visible data for
clinicians.
Compared to DSA, MSCTA is more invasive, faster,
less expensive and with relatively fewer contraindications.
Additionally, MSCTA displays the three-dimensional relationship
between the tumor, blood vessels and the skull. It also simulates
surgical approaches for clinicians from multiple perspectives and
avoids destroying the adjacent massive vessels and important
tissues. However, CTA also has limitations, including: i) the
spatial resolution of CTA is lower than DSA, but there was no
diagnostic difference in the requirements of clinically interesting
vessels in this group; ii) CTA cannot dynamically observe the blood
flow, so that it cannot correctly judge the direction of blood
flow; iii) there are relatively more influential factors in CTA
imaging. Both examination methods have advantages in the evaluation
of blood supply in meningiomas, and are to some extent
complementary. We should select a reasonable method to measure the
characteristics of tumors in clinical practice.
References
|
1.
|
C ManelfeP LasjauniasJ
RuscalledaPreoperative embolization of intracranial meningiomasAm J
Neuroradiol796319863096121
|
|
2.
|
X FanQ FangL HuangThe meningioma
diagnostic value with digital subtraction cerebral angiographyJ
Intervent Radiol154304312006
|
|
3.
|
J MaW RenP ChenThe diagnostic value of
digital subtraction angiography of intracranial meningiomaJ
Intervent Radiol134834852006
|
|
4.
|
R LiD WangZ ZengDigital subtraction
angiography of meningioma and preoperative embolotherapyJ Practical
Radiol219499512005
|
|
5.
|
X HanT WangH GaoClinical study on
nurturing vessels of menigioma by multi-slice CT angiography and 3D
reconstructionChin J Intervent Imaging Ther31721742006
|
|
6.
|
M LellK AndersE KlotzH DittW BautzBF
TomandlClinical evaluation of bone-subtraction CT angiography
(BSCTA) in head and neck imagingEur
Radiol16889897200610.1007/s0330-005-0032-116267665
|
|
7.
|
SG WetzelE KirschKW StockCerebral veins:
comparative study of CT venography with intraarterial digital
subtraction angiographyAm J Neuroradiol20249255199910094346
|
|
8.
|
MM LellK AndersU MichaelNew techniques in
CT
angiographyRadioGraphics26S45S62200610.1148/rg.26si06550817050518
|