Introduction
Pancreatic carcinoma causes more than 20,000 deaths
every year in Japan and overall five-year survival is less than 5%
(1,2). For patients with localized disease,
radical surgery may be of long-term benefit. Therefore, we usually
perform radical pancreatic resection, comprising wide lymph node
dissection and complete removal of the extrapancreatic nerve plexus
of the superior mesenteric artery or celiac axis for patients with
carcinoma of the pancreas, to improve outcomes (3–5).
However, even in patients who undergo resection, five-year survival
remains only 7–24% and median survival is only approximately one
year in most series, indicating that surgery alone is usually
inadequate. These disappointing results are likely attributable to
early vascular dissemination; i.e. subclinical metastases are
present at the time of diagnosis in most patients (6). This hypothesis underpins the
investigation of adjuvant chemotherapy after surgery. Oettle et
al reported that adjuvant chemotherapy with gemcitabine
produced a statistically significant improvement in overall
survival (OS) (7).
A major drawback of adjuvant therapy for pancreatic
cancer is the marked and consistent failure of 20–30% of patients
to receive the designated therapy as a result of post-operative
complications, delayed surgical recovery, patient refusal,
comorbidity, or early disease recurrence (8–10).
These challenges can be overcome in certain cases by administering
preoperative therapy, in order that more patients receive
potentially beneficial adjuvant treatment. Other theoretical
advantages of this approach include the early treatment of
micrometastases, delaying surgery and thereby sparing those who
already have occult metastases the morbidity and mortality of major
surgery if disseminated disease becomes apparent at the time of
reassessment; reduced risk of intraoperative tumor seeding; better
treatment tolerance than with postoperative therapy; and reduced
overall treatment time.
Potential disadvantages of preoperative therapy
include the requirement for biliary decompression before
chemotherapy with the potential for complications associated with
biliary stents; delayed surgery allowing progression to a
non-resectable stage in patients whose disease did not respond to
therapy; lack of preoperative tissue diagnosis (risk of seeding if
a preoperative biopsy is performed); and more postoperative
complications.
Gemcitabine is a deoxycytidine analogue that
competes for incorporation into DNA, thereby inhibiting its
synthesis. Gemcitabine is currently the standard treatment for
advanced pancreatic cancer on the basis of a randomized study
comparing gemcitabine with 5-fluorouracil (5-FU) in 126 patients in
which a small but clinically important survival advantage and
greater clinical benefit favoring gemcitabine were observed.
S-1 is an oral fluorinated pyrimidine developed by
Taiho Pharmaceutical Co., Ltd. (Tokyo, Japan). This agent contains
tegafur (FT), 5-chloro-2,4-dihydroxypyridine (CDHP), and potassium
oxonate (Oxo) at a molar ratio (FT:CDHP:Oxo) of 1:0.4:1, based on a
biochemical modulation of 5-FU (11). FT, a prodrug of 5-FU, is gradually
converted into 5-FU and is rapidly catabolized by dihydropyrimidine
dehydrogenase (DPD) in the liver. 5-Chloro-2,4-dihydroxypyridine is
a competitive inhibitor of 5-FU catabolism, being about 180 times
more potent than uracil in inhibiting DPD (12). When FT is combined with CDHP, the
resulting high 5-FU levels are maintained in both plasma and the
tumor. In addition, it has been suggested that CDHP has the
potential to enhance the antitumor activity of 5-FU against
subcutaneous tumors in nude mice, using human pancreatic carcinoma
cells with highly malignant DPD activity (13). Oxo inhibits the enzyme orotate
phosphoribosyltransferase, the major enzyme responsible for 5-FU
activation in colon cancer (14).
Oxo preferentially localizes in the gut rather than in the tumor
and appears to have a biochemical effect on orotate
phosphoribosyltransferase, thereby selectively inhibiting the
formation of 5-FU nucleotides in the gut and theoretically reducing
gastrointestinal side effects (15). Oral administration of S-1 is more
convenient and simulates the effect of continuous infusion of 5-FU.
The safety and usefulness of combination chemotherapy with
gemcitabine and S-1 for advanced pancreatic cancer were previously
reported (16–18) and a phase III trial was conducted
in Japan.
The usefulness of preoperative (neoadjuvant)
gemcitabine-based chemotherapy or chemoradiotherapy for prolonging
survival in patients with resectable pancreatic cancer was also
previously reported (19–22). As yet, the combination regimen of
gemcitabine and S-1 for patients with preoperatively resectable
pancreatic cancer has not been investigated. Therefore, we
conducted a pilot study of neoadjuvant chemotherapy (NAC) with a
combination of gemcitabine plus S-1 for patients with resectable
pancreatic cancer.
Materials and methods
Patient selection
Between January 2006 and June 2009, 35 patients who
had radiologically diagnosed pancreatic cancer regarded as
potentially resectable underwent pancreatic resection with
lymphadenectomy at Kanazawa University Hospital. A total of 34 of
the 35 resected tissue specimens were pathologically proven to be
ductal adenocarcinoma of the pancreas. NAC was administered to 13
(NAC group) of the 34 patients. The other 21 patients were
surgically treated without preoperative chemotherapy (control
group). The study was non-randomized.
Written informed consent was obtained from each
patient prior to enrollment, and the local ethics committee
approved the study.
Eligibility criteria included being 20–79 years of
age, Eastern Cooperative Oncology Group (ECOG) performance status
of one or less (ambulatory and capable of self-care), adequate
renal function (normal serum creatinine and blood urea nitrogen
levels), adequate liver function (total bilirubin level <2.5
times upper normal limit (UNL) or <3 times UNL after biliary
drainage if the patient had jaundice and serum transaminases (GOT,
GPT) levels <2.5 or 3 times UNL), bone marrow reserve (white
blood cell count between 4000 and 12,000 mm3, neutrophil
count >2000 mm3, platelet count >100,000
mm3, hemoglobin >9.5 g/dl), and adequate pulmonary
function (PaO2>65 mmHg). Any prior cancer treatments
(tumor resection, chemotherapy, immunotherapy, or radiotherapy) had
to have been discontinued at least four weeks prior to study
entry.
The exclusion criteria included pulmonary fibrosis
or interstitial pneumonia, marked pleural or pericardial effusion
or marked peripheral edema, most forms of heart disease, difficult
to control diabetes mellitus, active infection, pregnancy or
lactation, being a woman of childbearing age unless using effective
contraception, severe drug hypersensitivity, appearance of distant
metastases during preoperative chemotherapy, severe neurological
impairment or mental disorder, active concomitant malignancy, and
other serious medical conditions.
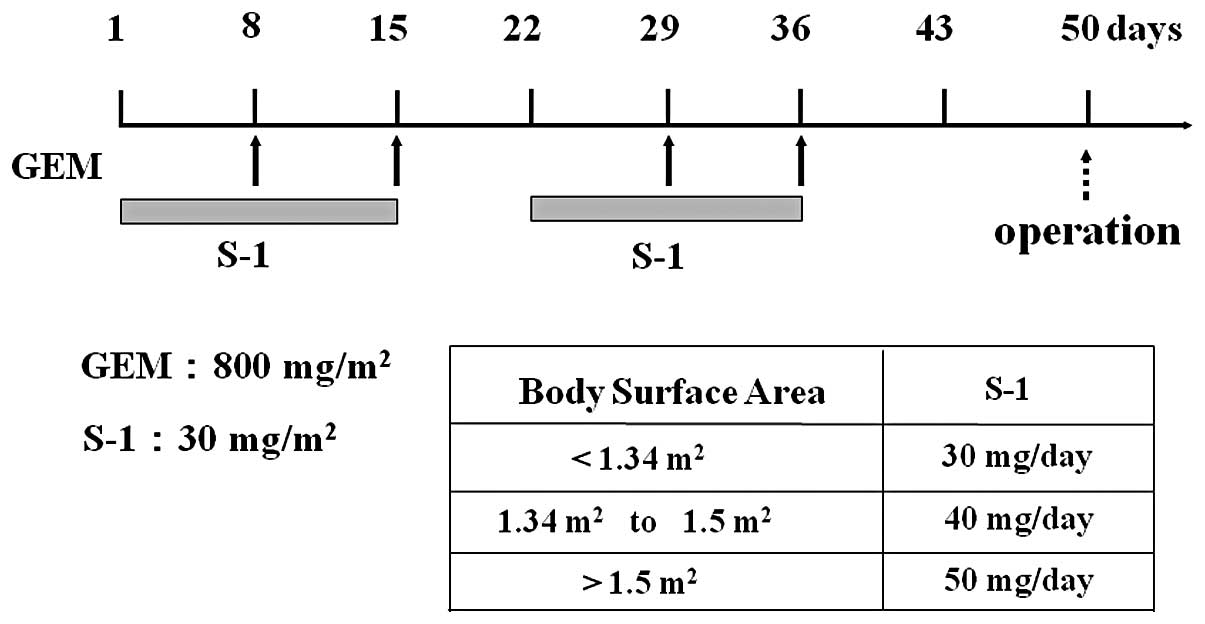
Treatment protocol
The laboratory tests required to assess eligibility
had to be completed within seven days prior to the start of
treatment; S-1 was administered orally after a meal for 14
consecutive days (from the evening of day 1 to the morning of day
15), followed by a one-week break. Each capsule of S-1 contained 20
or 25 mg of FT. Individual doses were rounded down to the nearest
pill size less than the calculated dose, given the available
formulation. Gemcitabine was administered as a 30-min intravenous
infusion on days 8 and 15 of each cycle. The cycle was repeated
twice. This schedule was based on an in vitro study, which
showed maximum synergy when fluoropyrimidine precedes exposure to
gemcitabine (23). The planned
drug doses in this study were as follows: S-1 30 mg/m2
day and gemcitabine 800 mg/m2 (Fig. 1). The two groups received
pancreatectomy with lymphadenectomy. In cases with suspected tumor
infiltration into the portal vein, resection of the vein with
reconstruction was performed. In the NAC group, the operation was
performed more than two weeks after chemotherapy.
Assessment of efficacy
Tumor responses were evaluated according to Response
Evaluation Criteria In Solid Tumors (RECIST). A complete response
(CR) was defined as the disappearance of all clinical evidence of
the measurable tumor. A partial response (PR) was defined as a ≥30%
reduction in the sum of the products of two perpendicular diameters
of all measurable lesions compared to the base-line with no
evidence of new lesions. Stable disease (SD) was defined as a
<30% reduction or <20% increase in the sum of the products of
two perpendicular diameters of all measurable lesions compared to
the base-line, with no evidence of new lesions. Progressive disease
(PD) was defined as an increase of ≥20% in the sum of the products
of two perpendicular diameters of all measurable lesions compared
to the base-line, the appearance of any new lesion, or
deterioration in clinical status consistent with disease
progression. To assess objective responses, patients were evaluated
following two cycles of chemotherapy, i.e., prior to surgery.
Pathological diagnosis
Surgically resected specimens were immediately fixed
in a 10% neutral-buffered formaldehyde solution. After the
specimens had been cut horizontally into 5-mm tissue blocks and
corresponding computerized tomographic (CT) images taken (24), they were dehydrated and embedded in
paraffin. Sections (5-μm) were cut and stained with
hematoxylin and eosin. Each section was carefully examined by light
microscopy. The tumors were evaluated according to the General
Rules for the Clinical and Pathological Study of Pancreatic Cancer
proposed by the Japanese Pancreatic Cancer Group. The grading
system of Evans et al was used to assess the pathological
effects of preoperative chemotherapy (25). The degrees of cytological change
and tumor destruction were graded on a scale of I–IV, as follows:
grade I, characteristic cytologic changes of malignancy are
present, but little (<10%) or no tumor cell destruction is
evident; grade IIa, destruction of 10–50% of tumor cells; grade
IIb, destruction of 51–90% of tumor cells; grade III, few (<10%)
viable-appearing tumor cells are present; grade IIIM, sizable pools
of mucin are present; grade IV, no viable tumor cells are present;
grade IVM, acellular pools of mucin are present.
Follow-up
Adjuvant chemotherapy with bi-weekly gemcitabine was
administered following surgery, if possible. Patients were
evaluated by physical examination and laboratory data bi-weekly and
by CT every three months.
Statistical analysis
Categorical variables were compared using the
Chi-square test. The OS and disease-free survival (DFS) rates were
calculated from the start of the study or study treatment until
death or the final date of follow-up and determined by the
Kaplan-Meier method. Data for surviving patients at the time of the
study report were censored. The log-rank test was applied for
comparison of survival rates between groups. Results were
considered significant at p<0.05.
Results
Clinical data of patients
From 2006 to June 2009, 13 patients (7 males and 6
females) diagnosed as having resectable pancreatic ductal
adenocarcinoma were treated with NAC using S-1 and gemcitabine.
Their mean age was 62.6 years (range, 51–77). There were 21
patients (14 males and 7 females) in the control group, with a mean
age of 66.0 years (range, 52–80). No differences were found between
the groups in terms of age, gender, status of lymph node
metastases, tumor stage or tumor size (Table I). Following chemotherapy, no
patients were judged to be incapable of undergoing laparotomy.
Neither distant metastasis nor tumor progression was observed.
 | Table I.Patient characteristics. |
Table I.
Patient characteristics.
| Characteristics | NAC group | Control group | p-value |
|---|
| Patients (n) | 13 | 21 | |
| Gender (n) | | | |
| Male | 7 | 14 | NS |
| Female | 6 | 7 | |
| Age (years) | | | |
| Median | 62.6 | 66.0 | NS |
| Range | 51–77 | 52–80 | |
| Location (n) | | | |
| Head of
pancreas | 9 | 11 | NS |
| Pancreas body and
tail | 3 | 10 | |
In the NAC group, comprising 13 ductal
adenocarcinoma patients, nine with pancreatic head cancer were
treated by pancreaticoduodenectomy with portal resection and five
with pancreatic body-to-tail cancer underwent distal
pancreatectomy. In the control group, comprising 21 ductal
adenocarcinoma patients, 11 patients with pancreatic head cancer
were treated by pancreaticoduodenectomy with portal resection, and
10 with pancreatic body-to-tail cancer underwent distal
pancreatectomy. Of the 13 patients (69.2%), 9 completed both
courses of preoperative chemotherapy.
Response to chemotherapy
The 13 NAC patients exhibited SD. The radiological
findings showed the average rate of tumor shrinkage was 8.1% (−5.7
to 25.8%). None of the patients showed an increase in tumor size
during preoperative chemotherapy, but in half of the patients the
tumor size was unchanged. In the NAC group, the tumor specimens
exhibited histopathological evidence of tumor cell injury, although
none of the patients exhibited a pathological CR. The treatment
effect, as judged by the Evans grading system, was grade IIa in 11
patients and grade IIb in two.
Surgical results
Intraoperative blood loss during pancreatic cancer
resection was 487.3±326.8 ml in the NAC group and 487.6±390.0 ml in
the control group. No significant difference was found between the
two groups in terms of tumor location (Table II). The overall postoperative
mortality rate was 0%. In the NAC group, eight patients (61.5%) had
complications. One case each developed pancreatic fistula, delayed
gastric empty (DGE) and intra-abdominal infections, which were
treated conservatively. In the control group, 12 patients (57.1%)
suffered complications. There were four intra-abdominal infections,
five DGE, two pancreatic fistulas, and one case each of ileus and
wound infection, both of which were treated conservatively.
However, one case with a pancreatic fistula complicated by hepatic
arterial bleeding required interventional radiology.
| Table II.Histopathological
characteristics. |
Table II.
Histopathological
characteristics.
| NAC group
(n=13) | Control group
(n=21) | p-value |
|---|
| Tumor size
(mm) | | | |
| Average | 30.1 | 30.6 | NS |
| Range | 16–55 | 17–53 | |
| Serosal
invasion | 53.8% | 40.0% | NS |
| Retroperitoneal
invasion | 84.6% | 61.9% | NS |
| Vascular
invasion | 84.6% | 90.5% | NS |
| Lymph node
metastasis | 76.9% | 57.1% | NS |
| Perineural
invasion | 100.0% | 90.5% | NS |
Efficacy
Median resected tumor specimen size was 30.1 mm in
the NAC group, with no patients demonstrating a pathological CR
(Table II). Tumor size in the
control group was 30.6 mm, not significantly larger than in the NAC
group. The NAC and control groups did not differ significantly in
the frequency of lymph node metastasis or infiltration of vessels,
nerve plexuses and the retroperitoneum. Moreover, the frequency of
pathologically curative resection (R0) in the NAC group was not
significantly higher than that in the control group (R0/1/2%,
84.6/15.4/0.0 versus 85.7/14.3/0.0).
Toxicity
Eleven of the 13 NAC patients were evaluated for
toxicity. The most common side effects are shown in Table III. A substantial percentage of NAC
patients experienced grades I–III hematological toxicities, i.e.,
leucopenia (grades I–II, 46.2%; grade III, 7.7%), anemia (grades
I–II, 53.8%), and thrombocytopenia (grades I–II, 38.5%; grade III,
15.4%). Other side effects were liver injury (grade I, 8.3%) and
eruption (grade I, 8.3%).
| Table III.Toxicities of preoperative
chemotherapy. |
Table III.
Toxicities of preoperative
chemotherapy.
| Grade I–II (%) | Grade III (%) |
|---|
| Leucopenia | 6 (46.2) | 1 (7.7) |
| Anemia | 7 (53.8) | 0 (0.0) |
|
Thrombocytopenia | 5 (38.5) | 2 (15.4) |
| Eruption | 1 (7.7) | 0 (0.0) |
| Liver injury | 1 (7.7) | 0 (0.0) |
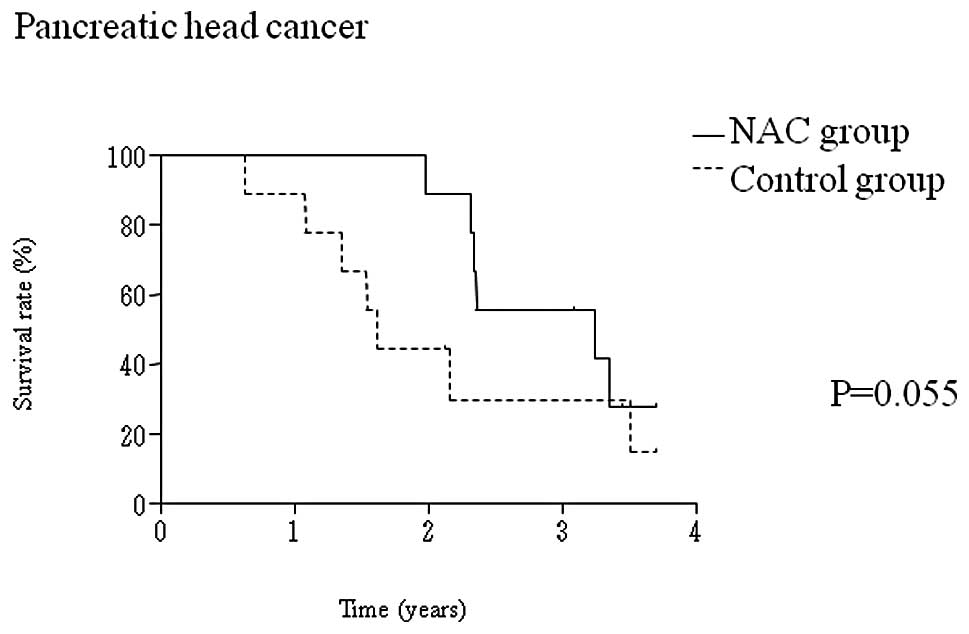
OS and DFS rates
Of the 34 patients, 17 (50.0%) patients were
followed up with adjuvant chemotherapy with bi-weekly gemcitabine
administration following surgery. The median follow-up time after
the operation was 30.0 months (range, 24–48) for all patients.
Although the one- and three-year OS rates of pancreatic head cancer
patients in the NAC group were 88.9 and 55.6%, superior to the 88.9
and 29.6% in the control group (p=0.055), the differences did not
reach statistical significance (Fig.
2A). OS rates for pancreatic body and tail cancer patients did
not differ significantly between the two groups (Fig. 2B).
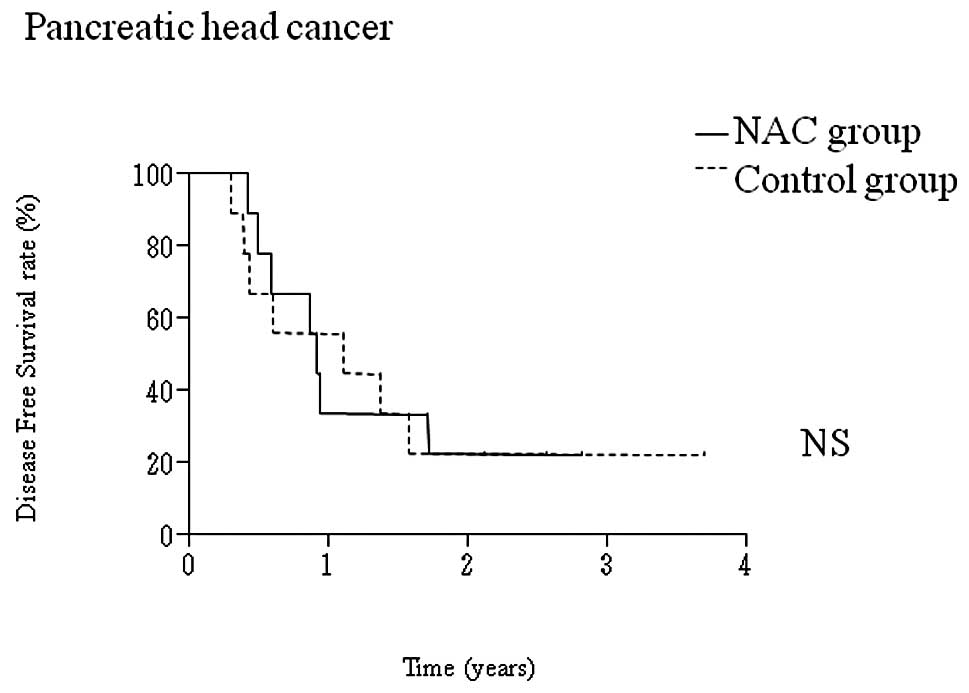
No significant differences were observed in the DFS
rates of pancreatic head cancer versus pancreatic body-to-tail
cancer patients, and between the NAC and control groups (Fig. 3A and B). Sites of recurrence are
shown in Table IV. There were
significant differences between the two groups. However, the number
of liver metastases tended to be lower in the NAC (1.7±0.6) than in
the control (5.8±4.3) group (p=0.065).
| Table IV.Patterns of recurrence in resected
patients. |
Table IV.
Patterns of recurrence in resected
patients.
| NAC group (n=7,
%) | Control (n=13,
%) | p-value |
|---|
| Local | 1 (14.3) | 1 (7.7) | NS |
| Liver | 4 (57.1) | 10 (76.9) | NS |
| Peritoneum | 1 (14.3) | 4 (30.8) | NS |
| Lung | 3 (42.9) | 0 (0.0) | NS |
| Lymph node | 1 (14.3) | 1 (7.7) | NS |
Discussion
Curative surgical resection is the only means of
curing pancreatic cancer. However, the majority of pancreatic
cancer resections are reportedly R1 (26) and, even after undergoing curative
resection, patients with pancreatic cancer face a 50–80% local
recurrence rate and a 25–50% chance of developing distant
metastases (6). We reported that
for patients with localized pancreatic cancer, radical pancreatic
resection, consisting of wide lymph node dissection and complete
removal of the extrapancreatic nerve plexus of the superior
mesenteric artery or celiac axis, improves outcomes (3–5).
However, the long-term results are not satisfactory due to the high
frequency of distant metastasis. Given the unsatisfactory outcomes
obtained to date, adjuvant chemotherapy is required. In particular,
pancreatic head cancer, partly due to surgical stress, requires a
long postoperative recovery period before chemotherapy is
administered. Preoperative chemotherapy is expected to reduce the
risk of distant metastasis.
Nakamura et al conducted a phase II clinical
trial of S-1 combined with gemcitabine for metastatic pancreatic
cancer (16). In that trial, S-1
was administered for 14 consecutive days prior to gemcitabine.
Moreover, Nakahira et al reported that pretreatment with S-1
enhances gemcitabine effects in pancreatic cancer xenografts
(27). The mechanism of these
enhanced effects is considered to be 5-FU upregulation of the major
mediator of cell uptake of gemcitabine, the human equilibrative
nucleoside transporter 1 (hENT1). In this study, we adopted the
regimen of Nakamura et al (16). However, due to the high incidence
of side effects with this preoperative chemotherapy, the S-1 dose
was reduced. In other words, S-1 was used only as a biochemical
modulator of gemcitabine.
Identifying an objective response following
chemotherapy for localized pancreatic cancer is extremely
difficult. Pancreatic cancer can be responsive to treatment even if
the histological response to chemotherapy, the radiological
findings, and tumor size were only minimally altered. Therefore,
the viability of tumors, as measured by positron emission
tomography-CT, has been used for response evaluation.
The effectiveness of preoperative chemoradiotherapy
has previously been reported (25,28,29).
Chemoradiotherapy is superior for local control of pancreatic
cancer, but one report described a higher rate of distant
metastases compared to chemotherapy alone (30). Based on these factors, we performed
radical resection for local control of pancreatic cancer, rather
than administering radiation therapy preoperatively.
In the nine NAC-group patients with pancreatic head
cancer, OS was prolonged compared to the control group. Although
the difference did not reach statistical significance, there were
no deaths within a two-year postoperative period in the NAC-group
patients with pancreatic head cancer. Notably,
pancreaticoduodenectomy for pancreatic head cancer is highly
invasive. Therefore, a few months are required to recover from
surgery, before adjuvant chemotherapy can be administered.
Furthermore, chemotherapy dose reductions are required for patients
who are not able to tolerate full doses of anticancer drugs.
Preoperative chemotherapy may be advantageous in allowing time for
postoperative chemotherapy. In addition, fewer liver metastases
were evident in the NAC compared to the control group. These
factors may have contributed to prolonged DFS.
Of the 13 NAC patients, 11 (84.6%) patients were
evaluated for toxicity. No severe toxicities were observed. In
addition, incidences of perioperative complications did not differ
significantly between the two groups.
In conclusion, NAC with gemcitabine and S-1 is well
tolerated and may be effective, particularly against pancreatic
head cancer. However, the appropriate doses of anticancer drugs
should be deteremined in a future study. A phase I study of NAC
with gemcitabine and S-1 is currently under way in patients with
resectable pancreatic cancer.
References
|
1.
|
Ministry of Health, Labour and Welfare:
The Dynamic Statistics of the Population in 2005. http://www.mhlw.go.jp/toukei/saikin/hw/jinkou/kakutei05/hyo7/htmluri
(11 June 2009, data last accepted).
|
|
2.
|
Ishii H, Furuse J, Boku N, et al: Phase II
study of gemcitabine chemotherapy alone for locally advanced
pancreatic carcinoma: JCOG0506. Jpn J Clin Oncol. View Article : Google Scholar : 2010. View Article : Google Scholar : PubMed/NCBI
|
|
3.
|
Nagakawa T, Kurachi M, Konishi K, et al:
Translateral retroperitoneal approach in radical surgery for
pancreatic carcinoma. Jpn J Surg. 12:229–233. 1982. View Article : Google Scholar : PubMed/NCBI
|
|
4.
|
Nagakawa T, Nagamori M, Futakami F, et al:
Result of extensive surgery for pancreatic carcinoma. Cancer.
77:640–645. 1996. View Article : Google Scholar : PubMed/NCBI
|
|
5.
|
Miwa K, Ohta T, Shimizu K, et al:
Augmented regional pancreatoduodenectomy for pancreas head cancer:
combined resection of pancreas head and superior mesenteric artery
and vein. In: American College of Surgeons 90th Annual Clinical
Congress; Chicago. Isis 190. 2004
|
|
6.
|
Evans DB, Abbruzzese JL and Willett CG:
Cancer of the pancreas. Cancer: Principles and Practice of
Oncology. 6th edition. De Vita Hellman S and Rosenberg SA:
Lippincott, Williams and Wilkins; Philadelphia: pp. 1126–1161.
2001
|
|
7.
|
Oettle H, Post S, Neuhaus P, et al:
Adjuvant chemotherapy with gemcitabine vs observation in patients
undergoing curative-intent resection of pancreatic cancer: a
randomized controlled trial. JAMA. 297:267–277. 2007. View Article : Google Scholar
|
|
8.
|
Klinlenbijl JH, Jeekel J, Sahmoud T, et
al: Adjuvant radiotherapy and 5-fluorouracil after curative
resection of cancer of the pancreas and periampullary region: phase
III trial of the EORTC Gastrointestinal Tract Cancer Cooperative
Group. Ann Surg. 230:776–782. 1999. View Article : Google Scholar
|
|
9.
|
Spitz FR, Abbruzzese JL, Lee JE, et al:
Preoperative and postoperative chemoradiation strategies in
patients treated with pancreaticoduodenectomy for adenocarcinoma of
the pancreas. J Clin Oncol. 15:928–937. 1997.PubMed/NCBI
|
|
10.
|
Yeo CJ, Abrams RA, Grochow LB, et al:
Pancreaticoduodenectomy for pancreatic adenocarcinoma:
postoperative adjuvant chemoradiation improves survival. A
prospective, single-institution experience. Ann Surg. 225:621–633.
1997. View Article : Google Scholar
|
|
11.
|
Shirasaka T, Shimamoto Y, Ohshimo H, et
al: Development of a novel form of an oral 5-fluorouracil
derivative (S-1) directed to the potentiation of the tumor
selective cytotoxicity of 5-fluorouracil by two biochemical
modulators. Anticancer Drugs. 7:548–557. 1996. View Article : Google Scholar : PubMed/NCBI
|
|
12.
|
Tatsumi K, Fukushima M, Shirasaki T and
Fujii S: Inhibitory effects of pyrimidine, barbituric acid and
pyrimidine derivatives on 5-fluorouracil degradation in rat liver
extracts. Jpn J Cancer Res. 78:748–755. 1987.PubMed/NCBI
|
|
13.
|
Takechi T, Fujioka A, Matssushima E, et
al: Enhancement of the antitumor activity of 5-fluorouracil (5-FU)
by inhibiting dihydropyrimidine dehydrogenase activity (DPD) using
5-chloro-2,4-dihydroxypyridine (CDHP) in human tumor cells. Eur J
Cancer. 38:1271–1277. 2002. View Article : Google Scholar
|
|
14.
|
Peters GJ, van Groeningen CJ, Laurensse EJ
and Pinedo HM: A compression of 5-fluorouracil metabolism in human
colorectal cancer and colon mucosa. Cancer. 68:1903–1909. 1991.
View Article : Google Scholar : PubMed/NCBI
|
|
15.
|
Takechi T, Nakano K, Uchida J, et al:
Antitumor activity and low intestinal toxicity of S-1, a new
formulation of oral tegafur, in experimental tumor models in rats.
Cancer Chemother Pharmacol. 39:205–211. 1997. View Article : Google Scholar : PubMed/NCBI
|
|
16.
|
Nakamura K, Yamaguchi T, Ishihara T, et
al: Phase I trial of oral S-1 combined with gemcitabine in
metastatic pancreatic cancer. Br J Cancer. 92:2134–2139. 2005.
View Article : Google Scholar : PubMed/NCBI
|
|
17.
|
Ueno H, Okusaka T, Ikeda M, et al: A phase
I study of combination chemotherapy with gemcitabine and oral S-1
for advanced pancreatic cancer. Oncology. 69:421–427. 2005.
View Article : Google Scholar : PubMed/NCBI
|
|
18.
|
Nakamura K, Yamaguchi T, Ishihara T, et
al: Phase II trial of oral S-1 combined with gemcitabine in
metastatic pancreatic cancer. Br J Cancer. 1–5. 2006.PubMed/NCBI
|
|
19.
|
Vento P, Mustonen H, Joensuu T, et al:
Impact of preoperative chemoradiotherapy on survival in patients
with resectable pancreatic cancer. World J Gastroenterol.
21:2945–2951. 2007.PubMed/NCBI
|
|
20.
|
Palmer DH, Stocken DD, Hewitt H, et al: A
randomized phase 2 trial of neo-adjuvant chemotherapy in resectable
pancreatic cancer: gemcitabine alone versus gemcitabine combined
with cisplatin. Ann Surg Oncol. 14:2088–2096. 2007. View Article : Google Scholar
|
|
21.
|
Sato N, Kurashima K, Nagai H, et al: The
effect of adjuvant and neoadjuvant chemo (radio) therapy on
survival in 1,679 resected pancreatic carcinoma cases in Japan:
report of the national survey in the 34th annual meeting of
Japanese Society of Pancreatic Surgery. J Hepatobiliary Pancreat
Surg. 16:485–492. 2009. View Article : Google Scholar
|
|
22.
|
Satoi S, Yanagimoto H, Toyokawa H, et al:
Surgical result after preoperative chemoradiation therapy for
patients with pancreatic cancer. Pancreas. 38:282–288. 2008.
View Article : Google Scholar : PubMed/NCBI
|
|
23.
|
Rauchwerger DR, Firby PS, Hedley DW and
Moore MJ: Equilibrative-sensitive nucleoside transporter and its
role in gemcitabine sensitivity. Cancer Res. 60:6075–6079.
2000.PubMed/NCBI
|
|
24.
|
Makino I, Kitagawa H, Ohta T, et al: Nerve
plexus invasion in pancreatic cancer. Spread patterns on
histopathologic and embryological analysis. Pancreas. 37:358–365.
2008. View Article : Google Scholar : PubMed/NCBI
|
|
25.
|
Evans DB, Rich TA, Byrd DR, et al:
Preoperative chemoradiation and pancreaticoduodenectomy for
adenocarcinoma of the pancreas. Arch Surg. 127:1335–1339. 1992.
View Article : Google Scholar : PubMed/NCBI
|
|
26.
|
Esposito I, Kleeff J, Bergmann F, et al:
Most pancreatic cancer resections are R1 resections. Ann Surg
Oncol. 15:1651–1660. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
27.
|
Nakahira S, Nakamori S, Tsujie M, et al:
Pretreatment with S-1, an oral derivative of 5-fluorouracil,
enhances gemcitabine effect in pancreatic cancer xenografts.
Anticancer Res. 28:179–186. 2008.PubMed/NCBI
|
|
28.
|
Takai S, Satoi S, Yanagimoto H, et al:
Neoadjuvant chemoradiation in patients with potentially resectable
pancreatic cancer. Pancreas. 36:26–32. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
29.
|
Golcher H, Brunner T, Grabenbauer G, et
al: Preoperative chemoradiation in adenocarcinoma of the pancreas.
A single centre experience advocating a new treatment strategy.
EJSO. 34:756–764. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
30.
|
Van Laethem JL, Hammel P, Mornex F, et al:
Adjuvant gemcitabine alone versus gemcitabine-based
chemoradiotherapy after curative resection for pancreatic cancer: A
randomized EORTC-40013-22012/FFCD-9203/GERCOR phase II study. J
Clin Oncol. 28:4450–4456. 2010.
|