Introduction
Historically, most cancer research has been focused
on studying the biology of either primary tumors or metastases.
However, the intermediate steps of the process, including events
such as cell departure from the tumor mass, intravasation,
lymphatic and circulatory dissemination and extravasation, have
been less studied. In recent years, there has been an increasing
interest in understanding thoroughly all processes involved in the
metastatic cascade, including the transit journey of tumor cells in
the circulatory and lymphatic systems (1). Moreover, it is acknowledged that a
thorough understanding of the biology of circulating tumor cells
(CTCs) may open new paths for the future development of potential
anticancer strategies (2,3).
The systemic nature of breast cancer is
characterized by the migration of tumor cells even at early stages
of the disease when the primary tumor shows a relatively small size
(4). Thus, CTCs in peripheral
blood could be regarded as the pre-stadium of clinically manifest
distant metastases (5,6). A considerable number of studies have
been accomplished on the determination of CTCs as a prognostic
and/or predictive biomarker for different types of cancers
(7). In contrast to studies in
bone marrow (BM), only a few studies on peripheral blood (PB)
screening have been conducted to date (8,9).
Additionally, the size of the patient cohorts analyzed and the
applied detection methods vary considerably between these studies.
Such experimental and analytical diversity insinuates that the
available knowledge on this topic is in certain cases contradictory
and controversial. Consequently, although some groups have found an
association between the presence of CTCs and a worse prognosis,
others have not demonstrated such an association, making the
prognostic significance of CTCs still uncertain (10,11).
For most patients affected with primary breast
cancer, the standard of care is systemic neoadjuvant therapy (NAT),
followed by surgical resection of the malignant tissue. NAT may
result in local tumor regression or even in a complete tumor
response, which may directly influence the surgical procedure of
choice, going from radical mastectomy to some type of
breast-conserving surgery – without risking patient survival
(12). Even though at early stages
tumors are clinically restricted to loco-regional tissue, there is
often early dissemination of viable tumor cells. One of the
purposes of systemic NAT is to attack these circulating and/or
disseminating tumor cells. This fact has potentiated the interest
in the use of NAT (13).
A potential use of the detection CTCs could be to
optimize treatment strategies that may increase the cure rate of
breast cancer patients. Several studies have reported that
metastatic breast cancer patients (MBC) with decreasing CTCs after
the initiation of antitumor therapy tend to enjoy a prolonged
benefit from their current regimens (14). In early breast cancer, however, it
remains necessary to consuct more studies to correlate the presence
or persistence of CTCs with overall survival (OS) and with
progression-free disease (PFS). We designed a study to assess the
potential of CTCs to predict risk of death in a cohort of patients
with primary breast cancer, evaluating the presence of CTCs both
prior to and after neoadjuvant treatment.
Patients and methods
Patient characteristics
Twenty-six patients were enrolled in the study from
April 2000 until December 2002, but 2 patients were excluded due to
problems originating during the sample processing. Follow-up time
was extended until the end of 2005 or until death, with a median
follow-up time of 56 months. Eligibility criteria for the study
were female breast cancer with age ranging from 26 to 71 years,
with early breast cancer (stages T2 to T3), without a familial
history of cancer and without previous chemotherapy treatment at
the entry of the study. Tumor types of the patients were classified
by pathologists according to the World Health Organization scheme
for typing breast tumors. Immunostaining of primary tumor samples
was assessed by the Department of Pathology (University Hospital of
Jaén) on routinely processed paraffin sections upon
antigen-retrieval. Sections were examined with monoclonal
antibodies (mAbs) recognizing estrogen receptor (ER) (clone 6F11;
Master Diagnostica, Granada, Spain); and HER2 c-erbB2 (clone CB11;
Master Diagnostica), using immunoperoxidase staining with
monoclonal antibodies, and considering the ER positive cut-off
level at >10% stained nuclei. The receptor status of the
patients was 59% for positive ER and 41% for negative ER. The
clinical characteristics of the patients at the time of primary
diagnosis are outlined in Table
I.
 | Table I.Tumor characteristics for the studied
population and correlation with CTC detection prior to and after
neoadjuvant chemotherapy. |
Table I.
Tumor characteristics for the studied
population and correlation with CTC detection prior to and after
neoadjuvant chemotherapy.
| Basal status (n=24)
| Post-chemotherapy
(n=24)
|
|---|
| No. (%) | CTCs+
(n=17) | p-value | No. (%) | CTCs+
(n=13) | p-value |
|---|
| Age (years;
55.38)a | | | 0.048a | | | 0.500 |
| <50 | 9/24 (37.5) | 8 | | 8/24 (33) | 5 | |
| ≥50 | 15/24 (62.5) | 9 | | 16/24 (67) | 8 | |
| Stage | | | 0.430 | | | 0.240 |
| IIA–IIB | 9/23 (39.1) | 8 | | 9/24 (37.5) | 6 | |
| IIIA–IIIB | 14/23 (60.9) | 8 | | 15/24 (62.5) | 7 | |
| Histology | | | 0.802 | | | 0.600 |
| Ductal | 11/23 (48) | 8 | | 12/23 (52.2) | 7 | |
| Lobular | 6/23 (26) | 4 | | 5/23 (21.7) | 3 | |
| Other | 6/23 (26) | 4 | | 6/23 (26.1) | 2 | |
| Lymph node status
(N) | | | 0.100 | | | 0.150 |
| N0 | 7/23 (30.4) | 6 | | 3/21 (14) | 1 | |
| N1 | 11/23 (47.9) | 7 | | 13/21 (62) | 7 | |
| N2 | 5/23 (21.7) | 3 | | 5/21 (24) | 2 | |
| Estrogen receptor
(ER) | | | 0.093b | | | 0.097b |
| ER-positive | 13/22 (59) | 11 | | 13/22 (59.1) | 9 | |
| ER-negative | 9/22 (41) | 4 | | 9/22 (40.9) | 2 | |
Neoadjuvant chemotherapy
All of the patients received anthracyclines and
taxol followed by tamoxifen aromatase inhibitors for patients with
hormone receptor-positive tumors. All evaluations were performed
with informed consent of the patients and with no knowledge of the
patients’ clinical status.
Circulating tumor cell detection
Prior to the first cycle of chemotherapy and 1 month
after the end of the treatment, 10 ml of anti-coagulated PB were
collected. Samples were maintained at room temperature and
processed within 4 h after collection. Blood samples were processed
according to the protocol established for our group (15). Briefly, the samples were processed
initially in a double density gradient (Histopaque 1077 over
Histopaque 1119). Enrichment of epithelial cells after Ficoll
gradient was performed by selective immunomagnetic cell separation,
using magnetic beads labelled with a multi-cytokeratin-specific
antibody (CK3-11D5; Miltenyi Biotec) which recognizes cytokeratin
7, 8, 18 and 19. Cytokeratin-positive cells were further
characterized by immunocytochemical staining using a highly
specific anti-cytokeratin-FITC antibody (CK3-6H5-FITC; Miltenyi
Biotec), on slides prepared by cytospin. Additionally,
cytokeratin-expressing cells were revealed by incubation with
freshly prepared Fast Red TR/Naphthol AS-MX substrate solution
(Sigma) for 15 min in a humidity chamber at room temperature.
Slides were washed once with PBS and stained with Mayer’s
hematoxylin solution (Sigma) for 30 sec at room temperature.
Epithelial tumor cells can quickly and easily be identified and
enumerated based on their strong coloration. The efficiency of the
method was tested using positive controls prepared by spiking blood
samples of healthy volunteers with varying numbers of MDA-MB-231
and MCF-7 mammary epithelial cancer cell lines (15).
Statistical analysis
The clinical characteristics of the patients were
related to the presence of CK+ cells in PB by means of a
Fisher’s exact test. When a variable was ordered, a trend analysis
was applied. Actuarial curves for OS were calculated by the
Kaplan-Meier method. The magnitude of the association was assessed
in terms of hazard ratios with 95% confidence intervals (CI),
estimated by a Cox regression analysis. OS was calculated from the
date of the detection of CK cells in PB to the date of death. All
statistical calculations were carried out using the STATA 8-SE
(Stata Inc., College Station, TX, USA) statistical analysis
program. The cut-off point for significance was set as
p<0.05.
Results
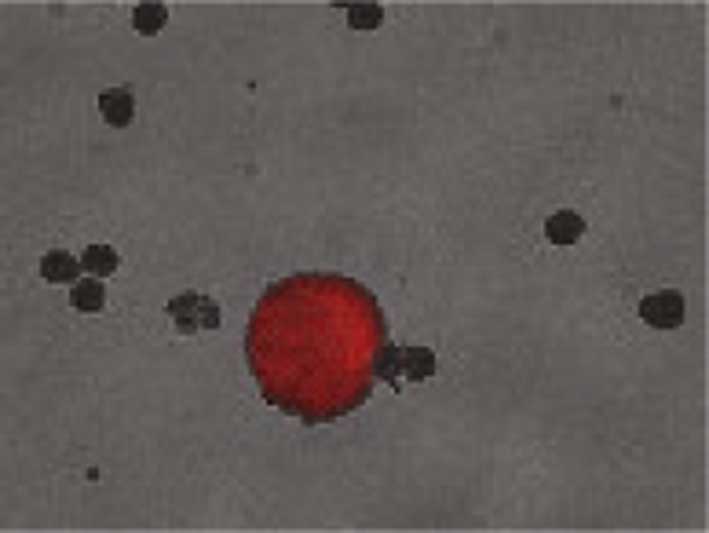
From April 2000 until December 2002, pre- and
post-neoadjuvant chemotherapy blood samples were obtained from 24
patients. CTCs detected by immunocytochemistry in the PB of breast
cancer patients showed a strong cytoplasmic staining pattern, and
the surrounding hematopoietic cells showed no expression of
cytokeratins (Fig. 1).
Identification of at least 1 CTC in the sample was considered as
positive. Correlation of CTCs in PB with patient characteristics is
outlined in Table I.
In the samples collected prior to neoadjuvant
chemotherapy, one or more CTCs were detected in 17 patients
(detection rate 70.08%; 95% CI 0.11–2.33). The mean (SD) number of
CK+ cells detected was 4.3 (±6.3), ranging from 1 to 28
cells (Tables I and II). There were significant differences
between the presence of CK+ cells and age groups
(p=0.048), in favor of patients <50 years of age. No
correlations were found with lymph node status (p=0.1),
histological type (p=0.802) or tumor stage (p=0.43). Regarding the
relationship between ER and the presence of CTCs, a borderline, but
significant trend was observed (p=0.093). Univariate analyses,
including all patients, revealed that the presence of CTCs was not
related to the OS (p=0.599).
| Table II.Number of CTCs detected in 24 breast
cancer patients. |
Table II.
Number of CTCs detected in 24 breast
cancer patients.
| Patient | CTCs basal
status | CTCs
post-chemotherapy | Patient status |
|---|
| 1 | 14 | 2 | Exitus |
| 2 | 6 | 3 | Exitus |
| 3 | 0 | 1 | Alive |
| 4 | 0 | 0 | Exitus |
| 5 | 2 | 0 | Alive |
| 6 | 28 | 1 | Exitus |
| 7 | 2 | 0 | Alive |
| 8 | 0 | 8 | Alive |
| 9 | 0 | 1 | Alive |
| 10 | 0 | 3 | Alive |
| 11 | 7 | 0 | Alive |
| 12 | 1 | 0 | Alive |
| 13 | 6 | 2 | Exitus |
| 14 | 3 | 0 | Alive |
| 15 | 2 | 0 | Alive |
| 16 | 3 | 1 | Exitus |
| 17 | 3 | 0 | Alive with
metatastic disease |
| 18 | 2 | 0 | Alive with
metatastic disease |
| 19 | 0 | 8 | Alive |
| 20 | 15 | 6 | Exitus |
| 21 | 0 | 0 | Alive |
| 22 | 0 | 8 | Alive |
| 23 | 8 | 0 | Alive |
| 24 | 6 | 0 | Alive |
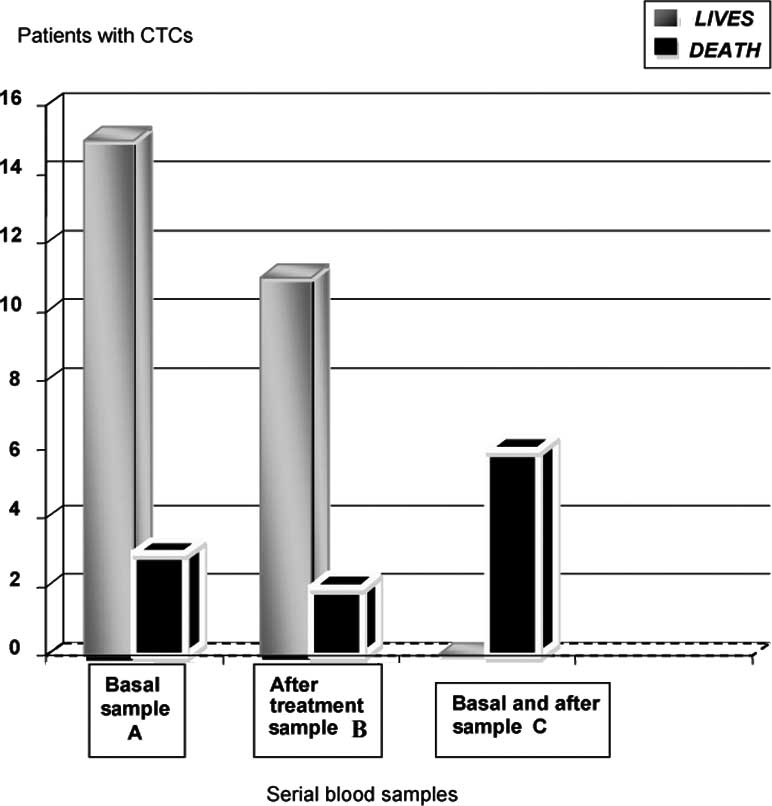
In the post-neoadjuvant chemotherapy sample group,
13 out of 24 patients were CTC-positive (detection rate 54.1%;
range 1–8 cells, median 2.1) (Tables
I and II). Comparing the rate
of CTCs present in samples from patients prior to and after NAT,
persistent detection of CTCs was achieved in 6 of 24 patients
(Fig. 2).
There were no significant differences in the
presence of CK+ cells between the age groups (p=0.5),
the lymph node status (p=0.15) or histological type (p=0.6)
(Table I) when compared to the
presence of CTC at both pre- and post-NAT. In regards to the ER, a
borderline significant trend was observed (p=0.097).
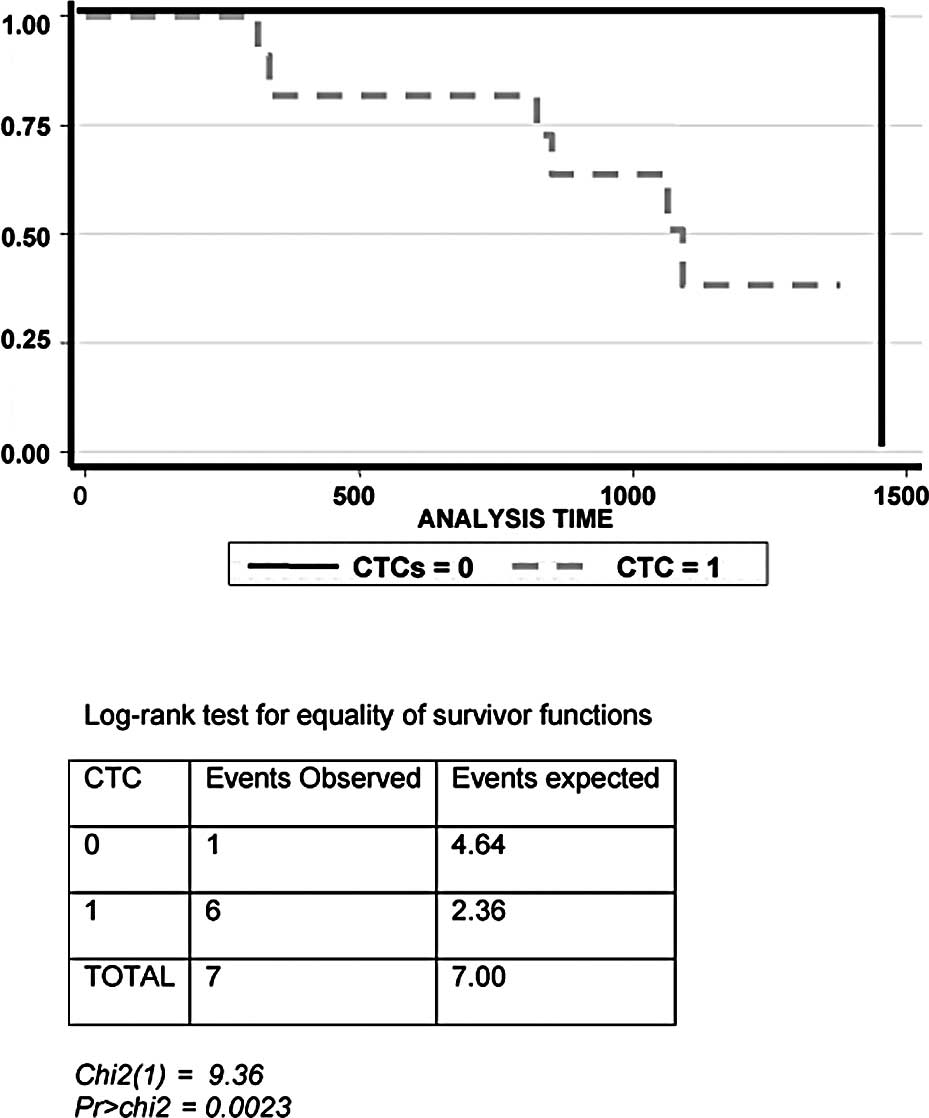
Prognostic analysis
Kaplan-Meier analysis of the OS in connection with
the detection of CK+ cells is presented in Fig. 3. Follow-up time covered the period
between last sample collection and the end time-point of the study
or until the date of death (median follow-up 56 months). Complete
data were available from 24 patients. From the initial 24 patients
included in the study, 7 patients had disease progression despite
treatment and died within the follow-up time. Within this group, 6
of them presented persistence of CTCs during follow-up and 1 of
them was negative for CTCs. Patients with negative result for CTCs,
in any of the excisions obtained during the follow-up, remain alive
and without evidence of clinical disease, except 1 individual.
Univariate and multivariate analyses revealed that the presence of
CTCs was related to OS, but only when the detection of CTC was
positive prior to and after treatment. Hence, only in the
double-positive patients can CTC detection be regarded as an
independent prognostic factor. Likewise, the Kaplan-Meier survival
analysis showed that the persistence of CK+ cells in PB
was associated with short survival (p=0023).
Discussion
Mounting evidence during recent years suggests that
the presence of CTCs correlates with disease progression in
patients with breast cancer (16).
The prognostic value of CTCs has been validated in MBC, but the
clinical significance of CTCs at early stages of breast cancer
remains controversial. In the present study, we demonstrated a
significant correlation between CTC detection and disease
progression when the CTC count was positive (≥1 cells/10 ml blood)
at both pre- and post-neoadjuvant treatment.
Similar studies to ours have been previously
conducted In a recent report by Bidard et al (17), detection of CTCs in non-MBC
patients was correlated with OS when neoadjuvant chemotherapy was
chosen as a treatment modality. In that study, after applying
CellSearch system for CTC separation, the group reported that
detection of 1 or more CTCs/7.5 ml prior to NAT predicted OS. Here,
we reinforced the notion that the presence of CTCs in the
neoadjuvant context can be used as a prognostic factor when 1 or
more cells are detected in PB. However, in our study this clinical
significance was only valid when a persistent detection of CTCs
after treatment occurred. Only patients with remaining CTCs in the
blood after treatment clearly showed a shorter OS. Similar to our
findings, the authors showed that in multivariate analysis the
presence of CTCs after NAT was found to be of less significance for
OS. Contrary to our data, their results for OS demonstrated that
the presence of CTCs before chemotherapy was a strong independent
prognostic factor along with tumor size and triple
receptor-negative phenotype.
Other groups have also made attempts to explore the
prognostic value of CTC detection in the context of breast cancer.
Riethdorf et al in the GepartQuatro study observed no
significant correlation between CTC detection and primary tumor
characteristics, such as tumor stage, histologic type, node lymph
stage or homone receptor status (18). Comparable outcomes were shown by
Pierga et al (9) in a
smaller cohort of patients in the REMAGUS 02 trial. In this study,
we also observed no significant correlation between CTC detection
and most characteristics presented in the primary tumor. To note, a
close to significant correlation between CTC detection and ER
status was observed in our study (p=0.097), which could be relevant
considering that we presented results with a smaller cohort of
patients.
The potential of CTCs to accurately predict the risk
of relapse and OS may depend on the optimal timing for sampling,
the frequency of performing blood collection and the cell
separation system used. The positive immunomagnetic isolation used
here was performed using mAb-labelled magnetic microbeads and a
basic magnet (MACS™ magnetic activated cell sorting system-Miltenyi
Biotec). This methodology allows efficient sorting of CTCs from
leukocytes. In previous reports from our laboratory, we
demonstrated that this methodology holds high reproducibility and
accuracy (19). In fact,
CellSearch™ system (Veridex) is the only FDA approved and leading
automated immnunomagnetic separation system for clinical routines
to detect and analyze CTCs in patients with MBC. Nevertheless, the
efficacy of this system in samples collected from early breast
cancer patients still needs to be confirmed. Other important points
for consideration are the timing of sample collection and the
definition of positivity in regard to the number of cells.
Cristofanilli et al observed that in MBC, detection of CTCs
at relative high numbers (≥5) at any subsequent time point (3 weeks
onwards) appears to be an indicator of poor clinical outcome, and
they concluded that determinations of CTCs up to 15–20 weeks after
initiation of therapy predicts more discriminately for survival
outcome. In their study, patients showing a persistence of CTC
counts (≥5 CTCs at the beginning and follow-up) exhibited
significantly worse OS compared to patients with persistently low
CTC counts (<5 at baseline and follow-up). On the other hand,
patients who changed from an elevated CTC count (≥5) at baseline to
a low CTC count (<5) at follow-up survived significantly longer
than those patients who changed from a low baseline CTC count to an
elevated CTC count at follow-up (20). However, such correlations are not
as evident in early breast cancer. In this regard, Riethdorf et
al (18) established CTC
positivity at 1 or more CTCs/7.5 ml before treatment, while
analyzing blood samples from pre-operated non-metastatic breast
cancer patients. In that study, only 5% of pre-operative samples
carried 5 or more CTCs/sample. In our study, we observed that the
majority of patients with fatal outcome presented 5 or more CTCs/10
ml prior to NAT. However, the numbers of cells in positive samples
in average diminished considerably in blood collected after
treatment. Still, our results were obtained from a small cohort of
patients; therefore interpretation of the data should be carried
out with caution.
We did not find correlations between CTCs and the
pathological characteristics of tumors at diagnosis. In early
breast cancer cases, Pachman et al (21) suggested the existence of a strong
correlation between the presence of CTCs and a decrease in tumor
size after neoadjuvant chemotherapy. The authors theorized that the
reduction in the tumor size during treatment could be a consequence
of the release of CTCs from the primary tumor mass. Moreover,
another study revealed that escalating numbers of CTCs during
tamoxifen treatment, although associated to primary tumor mass
reduction, was a strong predictor of relapse (22). In this later study, the observed
enhancement in CTC positivity was also predictive of a subsequent
relapse after aromatase inhibitor treatment. Additionally, other
groups exploring similar associations also found an inverse
correlation between CK-19 mRNA positivity in samples pre- and
post-tamoxifen treatment and disease-free interval and OS (23). The overall conclusion of all these
observations is that, in most cases, the CTCs found after
treatments are refractory to therapy. We hypothesize that these
CTCs could represent poorly differentiated cells. A reasonable
possibility is that NAT may eliminate more efficiently highly
differentiated tumor cells, and less efficiently the poorly
differentiated CTCs or/and in a dormant state (24). Experiments in pre-clinical models
suggest that dormant cancer cells are common in that they may get
reactivated under specific circumstances, and that they represent
an interesting but difficult therapeutic target (25).
In summary, we show that CTC determination in early
breast cancer patients can be used as a biomarker for prognosis
when the detection persists several weeks after treatment. This
methodology, applied at the parameters that we have chosen, serves
to identify patients with a high risk of death after treatment. Our
data also suggest that most CTCs found after treatment may
represent poorly differentiated cells refractory to treatment,
since it is associated with a higher degree of relapse. Although
significant, the power of our analyses is limited by the number of
patients enrolled in the study, despite the relatively long
follow-up period. Furthermore, the potential loss of epithelial
markers suffered by tumor cells released to the circulation or by
tumor cells going through partial or full epithelial-mesenchymal
transdifferentiation may lead to erroneous outcomes and still
stands as one of the main drawbacks of this methodology.
Standardization of the methodology between
laboratories remains as a mandatory goal to reach a sound
communication and the universal acceptance of data among scholars
in the field.
Traslational relevance
In recent years, the perspective of the study of
breast cancer has changed considerably, and the importance of
curative local treatments has declined in favor of administering
chemotherapy treatments or hormonal, even in the absence of lymph
node involvement or small-size tumors. The identification of new
prognostic factors that allow us to discriminate and stratify
patients for individualized treatment is one of the most important
avenues of research in this field. Among these new markers, the
presence of CTCs is considered indicative of hematogenous spread. A
factor with considerable potential prognostic significance in
metastasis formation could allow the characterization of patients
with primary breast cancer into subgroups that require more
intensive clinical monitoring. Lastly, with molecular and genetic
characterization of CTCs, chemoresistance profiles should also be
able to advise the clinician regarding the most efficacious
chemotherapy regimens. In terms of tumor biology, it is clear that
circulating tumor cells are present in early breast cancer, thus
supporting the theory of early metastasis.
Abbreviations:
|
CTCs
|
circulating tumor cells
|
|
ER
|
estrogen receptor
|
|
CK
|
cytokeratin
|
|
NAT
|
neoadjuvant therapy
|
|
OS
|
overall survival
|
Acknowledgements
The authors gratefully acknowledge all
patients who took part in this study and would like to thank Miguel
Rivero, Jesus Ruiz, Ivan Álvarez and Carlos García (Miltenyi Biotec
Spain) for the unconditional support in cancer research. The study
was supported by the Ministerio de Sanidad y Consumo grant; grant
no. FIS 02/1879; grant sponsor: COFIMAN S.L. and Fundación Pública
Progreso y Salud, Consejería y Salud, Junta de Andalucía.
References
|
1
|
Klein CA: The metastasis cascade. Science.
321:1841–1844. 2008. View Article : Google Scholar
|
|
2
|
Mego M, Mani SA and Cristofanilli M:
Molecular mechanisms of metastasis in breast cancer – clinical
applications. Nat Rev Clin Oncol. 7:693–701. 2010.
|
|
3
|
Graves H and Czerniecki BJ: Circulating
tumor cells in breast cancer patients: an evolving role in patient
prognosis and disease progression. Pathol Res Int. 2011:6210902011.
View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Pantel K and Brakenhoff RH: Dissecting the
metastatic cascade. Nat Rev Cancer. 4:448–456. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Serrano MJ, Sánchez-Rovira P,
Delgado-Rodriguez M and Gaforio JJ: Detection of circulating tumor
cells in the context of treatment: prognostic value in breast
cancer. Cancer Biol Ther. 8:671–675. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Botteri E, Sandri MT, Bagnardi V, Munzone
E, Zorzino L, Rotmensz N, Casadio C, Cassatella MC, Esposito A,
Curigliano G, et al: Modeling the relationship between circulating
tumour cell number and prognosis of metastatic breast cancer.
Breast Cancer Res Treat. 122:211–217. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Lin H, Balic M, Zheng S, Datar R and Cote
R: Disseminated and circulating tumor cells: role in effective
cancer management. Crit Rev Oncol Hematol. 77:1–11. 2011.
View Article : Google Scholar : PubMed/NCBI
|
|
8
|
García-Sáenz JA, Martín M, Maestro ML,
Vidaurreta M, Veganzones S, Rafael S, Casado A, Bobokova J, Sastre
J, de la Orden V, et al: Circulating tumour cells in locally
advanced breast cancer. Clin Transl Oncol. 11:544–547. 2009.
|
|
9
|
Pierga JY, Bidard FC, Mathiot C, Brain E,
Delaloge S, Giachetti S, de Cremoux P, Salmon R, Vincent-Salomon A
and Marty M: Circulating tumor cell detection predicts early
metastatic relapse after neoadjuvant chemotherapy in large operable
and locally advanced breast cancer in a phase II randomized trial.
Clin Cancer Res. 14:7004–7010. 2008. View Article : Google Scholar
|
|
10
|
Nakagawa T, Martinez SR, Goto Y, Koyanagi
K, Kitago M, Shingai T, Elashoff DA, Ye X, Singer FR, Giuliano AE
and Hoon DSB: Detection of circulating tumor cells in early-stage
breast cancer metastasis to axillary lymph nodes. Clin Cancer Res.
13:4105–4110. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Wong NS, Kahn HJ, Zhang L, Oldfield S,
Yang LY, Marks A and Trudeau ME: Prognostic significance of
circulating tumour cells enumerated after filtration enrichment in
early and metastatic breast cancer patients. Breast Cancer Res
Treat. 99:63–69. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Langer R, Ott K, Feith M, Lordick F,
Siewert JR and Becker K: Prognostic significance of
histopathological tumor regression after neoadjuvant chemotherapy
in esophageal adenocarcinomas. Mod Pathol. 22:1555–1563. 2009.
View Article : Google Scholar
|
|
13
|
Makhoul I and Kiwan E: Neoadjuvant
systemic treatment of breast cancer. J Surg Oncol. 103:348–357.
2011. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Pierga JY, Hajage D, Bachelot T, Delaloge
S, Brain E, Campone M, Dieras V, Rolland E, Mignot L, Mathiot C and
Bidard FC: High independent prognostic and predictive value of
circulating tumor cells compared with serum tumor markers in a
large prospective trial in first-line chemotherapy for metastatic
breast cancer patients. Ann Oncol. 2011. View Article : Google Scholar : 2011.
|
|
15
|
Riethdorf S and Pantel K: Disseminated
tumor cells in bone marrow and circulating tumor cells in blood of
breast cancer patients: current state of detection and
characterization. Pathobiology. 75:140–148. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Gaforio JJ, Serrano MJ, Sanchez-Rovira P,
Sirvent A, Delgado-Rodriguez M, Campos M, de la Torre N, Algarra I,
Duenas R and Lozano A: Detection of breast cancer cells in the
peripheral blood is positively correlated with estrogen-receptor
status and predicts for poor prognosis. Int J Cancer. 107:984–990.
2003. View Article : Google Scholar
|
|
17
|
Bidard FC, Mathiot C, Delaloge S, Brain E,
Giachetti S, de Cremoux P, Marty M and Pierga JY: Single
circulating tumor cell detection and overall survival in
nonmetastatic breast cancer. Ann Oncol. 21:729–733. 2010.
View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Riethdorf S, Müller V, Zhang L, Rau T,
Komor M, Roller M, Huober J, Fehm T, Schrader I, Hilfrich J, et al:
Detection and HER2 expression of circulating tumor cells:
prospective monitoring in breast cancer patients treated in the
neoadjuvant geparquattro trial. Clin Cancer Res. 16:2634–2645.
2010. View Article : Google Scholar
|
|
19
|
Serrano MJ, Lorente JA, Delgado Rodríguez
M, Fernández A, Fernández M, de la Torre C, Fernández Izquierdo J
and Sánchez Rovira P: Circulating tumour cells in peripheral blood:
potential impact on breast cancer outcome. Clin Trans Oncol.
13:204–208. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Cristofanilli M, Budd GT, Ellis MJ,
Stopeck A, Matera J, Miller MC, Reuben JM, Doyle GV, Allard WJ,
Terstappen LW and Hayes DF: Circulating tumor cells, disease
progression, and survival in metastatic breast cancer. N Engl J
Med. 351:781–791. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Pachmann K, Camara O, Kavallaris A,
Krauspe S, Malarski N, Gajda M, Kroll T, Jörke C, Hammer U,
Altendorf-Hofmann A, et al: Monitoring the response of circulating
epithelial tumor cells to adjuvant chemotherapy in breast cancer
allows detection of patients at risk of early relapse. J Clin
Oncol. 26:1208–1215. 2008. View Article : Google Scholar
|
|
22
|
Pachmann K, Camara O, Kohlhase A, et al:
Assessing the efficacy of targeted therapy using circulating
epithelial tumor cells (CETC): the example of SERM therapy
monitoring as a unique tool to individualize therapy. J Cancer Res
Clin Oncol. 137:821–828. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Meng S, Tripathy D, Frenkel EP, Shete S,
Naftalis EZ, Huth JF, Beitsch PD, Leitch M, Hoover S, Euhus D, et
al: Circulating tumor cells in patients with breast cancer
dormancy. Clin Cancer Res. 10:8152–8162. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Aguirre-Ghiso JA: Models, mechanisms and
clinical evidence for cancer dormancy. Nat Rev Cancer. 7:834–846.
2007. View
Article : Google Scholar : PubMed/NCBI
|
|
25
|
Mani SA, Guo W, Liao MJ, Eaton EN, Ayyanan
A, Zhou AY, Brooks M, Reinhard F, Zhang CC, Shipitsin M, et al: The
epithelial-mesenchymal transition generates cells with properties
of stem cells. Cell. 133:704–715. 2008. View Article : Google Scholar : PubMed/NCBI
|