Introduction
Ulcerative colitis (UC) is chronic colitis of
unknown etiology. Traditionally, patients who have severe attacks
requiring hospitalization are treated with intravenous
corticosteroids. Their response rate is approximately 60%.
Recently, calcineurin inhibitors (CNIs) have been used as
alternative treatments for steroid-refractory or steroid-dependent
UC. There are two main options for CNI induction therapy:
intravenous cyclosporin A (CSA) and oral tacrolimus (FK506).
CSA blocks the calcium-dependent signal transduction
pathway emanating from the T-cell receptor, thereby inhibiting the
action of helper T cells. CSA is also administered to patients with
graft-versus-host disease following allogeneic bone marrow
transplantation or to patients undergoing renal transplant. With
respect to steroid-refractory or steroid-dependent UC, CSA
induction therapy provides an effective medical alternative for
patients previously faced with only surgical options. Uncontrolled
trials (1,2) and controlled trials (3) established the efficacy of short-term
CSA use as a ‘rescue therapy’ in severe UC. Lichtiger et al
reported that intravenous CSA followed by oral therapy demonstrated
an initial response rate of 82% within a mean of 7 days versus 0%
in the group that received steroids alone (3).
On the other hand, tacrolimus (FK506) has similar
pharmacological mechanisms of action to CSA. Fellermann et
al reported the effectiveness of FK506 for refractory UC
patients. FK506 was initiated either intravenously at a dose of
0.01–0.02 mg/kg/day or 0.1–0.2 mg/kg/day orally. They concluded
that peroral dosing is equivalent to intravenous administration
(4). Ogata et al reported
the results of a placebo-controlled, double-blind study which
revealed that oral FK506 improved disease activity for 68.4% of the
patients in the high trough group as compared with 10.0% in the
placebo group (5).
As described above, these two CNIs are powerful
agents in bringing about remission of active UC. However, even
where CNIs are administered, a consequent colectomy may be required
in certain cases. We previously reported the factors affecting the
efficacy of CSA therapy for refractory ulcerative colitis (6). In the present study, we conducted a
retrospective study to investigate the prognostic factors for
colectomy in the era of CNI treatment.
Patients and methods
Patients
We reviewed the medical charts and recent follow-up
of 60 consecutive UC patients (35 men and 25 women) who had been
initially treated with CNIs for disease flare-ups between December
1999 and March 2011 at the Shiga University of Medical Science
Hospital. One case with concomitant psychological disorders was
excluded due to a suspension of the CNI treatment (Table I). In general, the CNIs were
administered to patients resistant to systemic corticosteroids. The
cytomegalovirus infections were validated from blood samples by
cytomegalovirus antigenemia (C7-HRP). Twelve out of 17 patients
also received concurrent ganciclovir treatment due to
cytomegalovirus infection. The average patient age was 33.6 years
[standard deviation (SD) 12.5, range 16–62], and the disease type
included one attack in only 8 cases, chronic continuous attacks in
14 cases and relapse remitting attacks in 37 cases. The disease
extent was pancolitis in 39 cases and left-sided colitis in 20
cases. To prevent Pneumocystis carinii infection,
sulfamethoxazole/trimethoprim was administered to all cases treated
with the CNIs.
 | Table I.Clinical background of the study
participants. |
Table I.
Clinical background of the study
participants.
| Clinical
characteristic | CSA | FK506 |
|---|
| Total no. of patients
(M/F) | 48 (28/20) | 11 (7/4) |
| Age, in years; mean ±
SD (range) | 33.4±12.7
(17–62) | 34.5±12.3
(16–59) |
| Disease duration, in
years; mean ± SD (range) | 3.9±4.0
(0.05–15.7) | 5.2±5.0
(0.15–16.4) |
| Seo’s CIDAI; mean ±
SD (range) | 221.1±24.7
(166.0–275.5) | 213.2±34.8
(143.0–265.7) |
| Undermining ulcer
(present/absent) | 52.0% (25/23) | 36.3% (4/7) |
| Disease extent
(pancolitis/left-sided) | 66.6% (32/16) | 63.6% (7/4) |
| C7-HRP
(positive/negative) | 31.2% (15/33) | 18.0% (2/9) |
| Total PSL used before
CNI treatment (mg)a;
mean ± SD (range) | 5,213±7,172
(140–36,500) | 4,517±4,816
(0–11,330) |
| CNI response rate
(responders/all) | 66.6% (32/48) | 63.6% (7/11) |
| Colectomy rate
(number) | 52% (25/48) | 36.3% (4/11) |
CSA administration
CSA was administered by continuous infusion with
starting doses of 2–4 mg/kg/day for a maximum of 14 days. The serum
CSA levels were monitored three times per week during the infusion
therapy, and the infusion dose was altered by aiming for 350–450
ng/ml. Following successful continuous CSA infusion, we switched to
peroral dosing. The total peroral daily doses were double those of
the continuous daily infusions. The trough serum levels were
monitored, and the dose of CSA was adjusted to trough serum levels
of 100–200 ng/ml. The average duration of the peroral CSA
administration was 145 days.
FK506 administration
FK506 treatment was started at a dose of 0.1
mg/kg/day, divided in two portions since a total oral daily dose of
approximately 0.1 mg/kg/ day was necessary to achieve a high trough
level of 10–15 ng/ml. The serum FK506 levels were monitored three
times per week during admission. The dose was altered by aiming for
a high trough level of 10–15 ng/ml for the first week, and then for
a low trough level of 5–10 ng/ml for the following week. The
absorption of FK506 is known to decrease by 38% following meals
(7). To minimize the effect of
meals, FK506 was prescribed to be taken one hour before food. The
average duration of FK506 administration was 127 days.
Definitions of outcome
The disease activity was assessed by using Seo’s
complex integrated disease activity index (CIDAI)(8). Scores below 150 indicated cases in
‘remission’. ‘CNI responders’ were defined as those with a 50-point
decrease two weeks following CNI administration. Following the
successful induction of remission, those patients who required
hospitalization or additional induction therapy such as steroids,
cytophoresis, infliximab and CNIs were defined as in ‘relapse’.
Statistical analyses
The patient characteristics of the responders were
then compared to the non-responders to elucidate the
characteristics of the responders. For evaluating the prognostic
factors of efficacy, categorical data analyses were performed on
gender, age (≥40 years, <40 years), disease duration (≥4 years,
<4 years), Seo’s CIDAI upon initiation of CSA treatment (≥220
points, <220 points), endoscopic findings of undermining ulcers,
disease extent (total colitis type or left-sided colitis), C7-HRP,
and total prednisolone (PSL) used prior to CNI treatment (≥10,000
mg, <10,000 mg). The overall colectomy-free survival was
calculated using the Kaplan-Meier method. The log-rank test was
used to determine the statistical difference between groups.
Receiver operating characteristic (ROC) curves were plotted to
compare the prognostic yield of these factors. All statistical
analyses were performed with StatView v5.0 (SAS Institute, Cary,
NC, USA), GraphPad Prism v4.03 and SPSS v16.0.1 (SPSS, Chicago, IL,
USA) software.
Results
Comparison between CNIs
The baseline characteristics of the study population
are described in Table I. The
patients’ backgrounds, the effectiveness of the CNIs and the
colectomy rate did not differ significantly between these two CNI
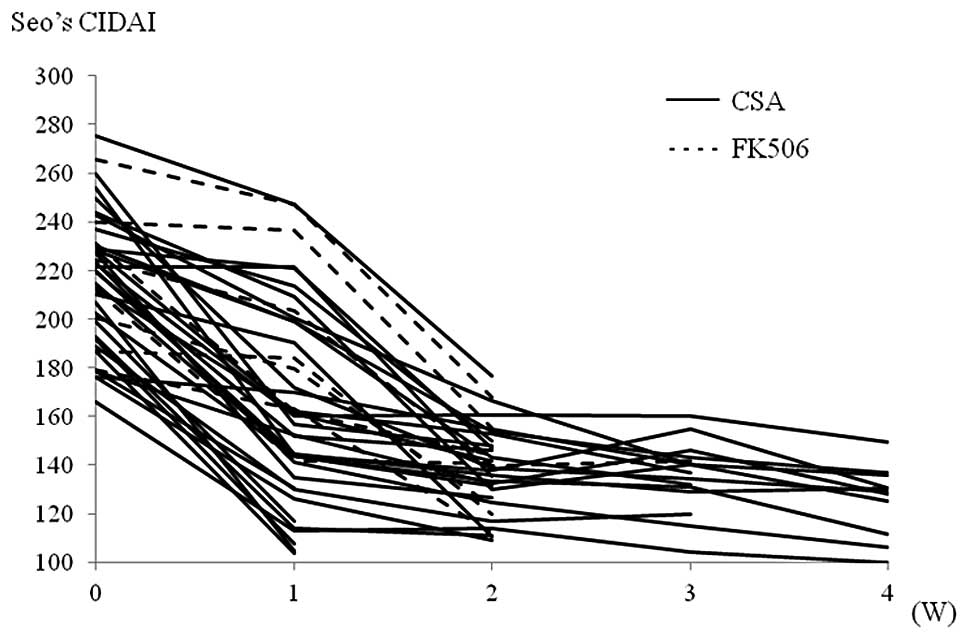
groups. The only difference was the onset of action following
initiation of CNI treatment. As shown in Fig. 1, the FK506 responders had a slower
onset as compared to the CSA responders. The prevalence of CNI
responders within one week following CNI administration was 56%
(18/32) in the CSA responder group as compared with 28% (2/7) in
the FK506 responder group (Fig.
1). Seo’s CIDAI decreased 53.1 points (SD 31.8) in the CSA
responder group as compared with 28.8 points (SD 28.8) in the FK506
responder group (P=0.035). To achieve a high trough level of FK506,
an average of 8.5 days was required.
The switching of CNI administration during single
induction therapy was not effective in two cases; one from CSA to
FK506, the other from FK506 to CSA. These two cases required urgent
colectomies.
Factors affecting CNI treatment and
colectomy
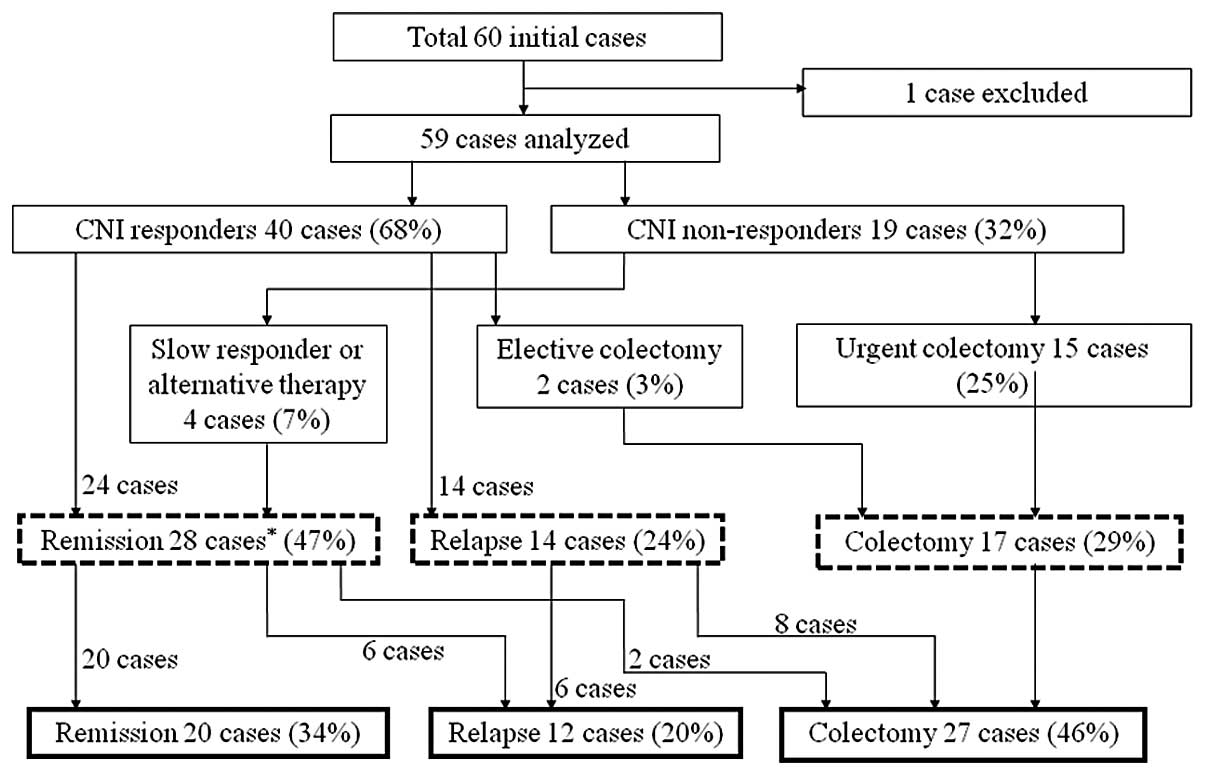
An overview of the outcome of patients treated with
the CNIs is shown in Fig. 2. The
response rate to the CNIs was 68%. Forty-seven percent of all cases
analyzed stayed in remission at one year following CNI
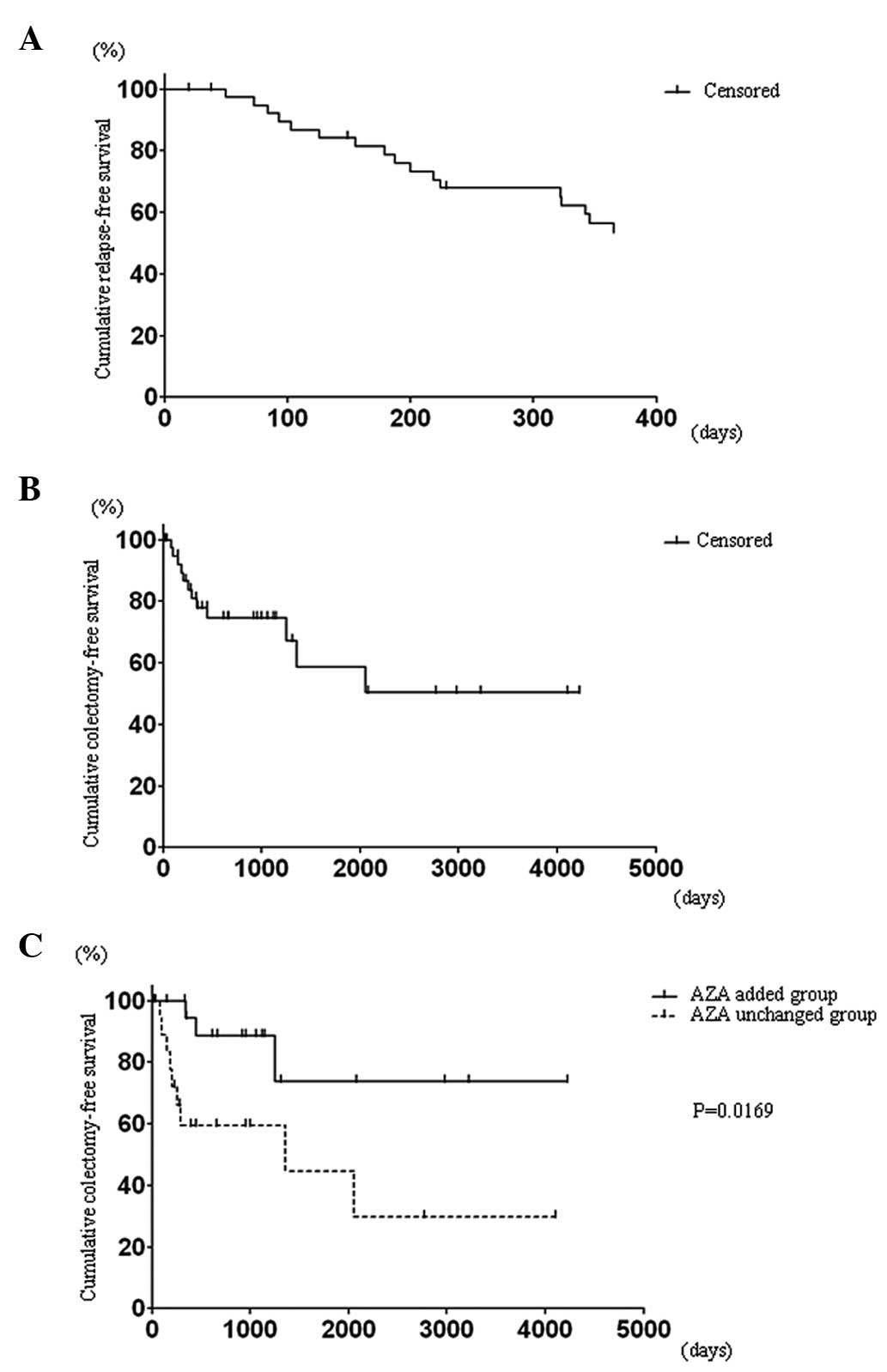
administration. The Kaplan-Meier survival analysis revealed a 53.5%
relapse-free survival rate among the CNI responders at one year
following the CNI administration (Fig.
3A). On the other hand, 46% of all cases analyzed underwent a
subsequent colectomy during the observation period. The
Kaplan-Meier analysis revealed that the overall colectomy-free
survival rate among the CNI responders was 50.3% during an average
observation period of 3.7 years (Fig.
3B). A stratified analysis revealed that the addition of
azathioprine (AZA) following the CNI treatment significantly
reduced the colectomy rate (73.3% vs. 29.7%, P=0.0169) (Fig. 3C).
As shown in Table
II, the factors that lessen the efficacy of CNIs were: i)
positivity for C7-HRP, and ii) more than 10,000 mg of PSL being
used prior to starting CNI treatment. Furthermore, those factors
predictive of a colectomy at one year following CNI treatment were:
i) CNI unresponsiveness, ii) positivity for C7-HRP and iii) more
than 10,000 mg of PSL being used prior to starting the CNIs
(Table III). The same results were
obtained subsequent to analyzing the prognostic factors for a
consequent colectomy (Table
IV).
| Table II.Risk estimates of CNI
non-responsiveness. |
Table II.
Risk estimates of CNI
non-responsiveness.
| | 95% CI
|
|---|
| Characteristic | Risk estimate | Lower | Upper |
|---|
| Male gender | 1.267 | 0.412 | 3.896 |
| Age ≥40 years | 1.538 | 0.481 | 4.916 |
| Disease duration ≥4
years | 2.308 | 0.755 | 7.055 |
| Seo’s CIDAI ≥220
points | 1.061 | 0.336 | 3.070 |
| Prior AZA
treatment | 1.385 | 0.416 | 4.612 |
| Undermining ulcer
present | 0.900 | 0.302 | 2.685 |
| Pancolitis | 2.500 | 0.701 | 8.915 |
| C7-HRP
positivity | 12.000 | 3.200 | 44.988 |
| PSL ≥10,000 mg | 12.375 | 3.122 | 49.048 |
| Table III.Risk estimates of a colectomy at one
year after CNI administration. |
Table III.
Risk estimates of a colectomy at one
year after CNI administration.
| | 95% CI
|
|---|
| Characteristic | Risk estimate | Lower | Upper |
|---|
| Male gender | 1.773 | 0.561 | 5.602 |
| Age ≥40 years | 1.077 | 0.331 | 3.506 |
| Disease duration ≥4
years | 0.875 | 0.284 | 2.699 |
| Seo’s CIDAI ≥220
points | 2.800 | 0.848 | 9.245 |
| Prior AZA
treatment | 1.385 | 0.416 | 4.612 |
| Undermining ulcer
present | 0.477 | 0.156 | 1.464 |
| Pancolitis | 2.500 | 0.701 | 8.915 |
| C7-HRP
positivity | 3.600 | 1.097 | 11.809 |
| PSL ≥10,000 mg | 3.429 | 1.010 | 11.643 |
| CNI
non-responder | 33.750 | 7.447 | 152.951 |
| Table IV.Risk estimates of a consequent
colectomy. |
Table IV.
Risk estimates of a consequent
colectomy.
| | 95% CI
|
|---|
| Characteristic | Risk estimate | Lower | Upper |
|---|
| Male gender | 0.944 | 0.334 | 2.670 |
| Age ≥40 years | 0.762 | 0.250 | 2.319 |
| Disease duration ≥4
years | 0.514 | 0.177 | 1.491 |
| Seo’s CIDAI ≥220
points | 1.083 | 0.386 | 3.044 |
| Prior AZA
treatment | 2.105 | 0.648 | 6.835 |
| Undermining ulcer
present | 0.711 | 0.255 | 1.981 |
| Pancolitis | 2.403 | 0.788 | 7.335 |
| C7-HRP
positivity | 3.529 | 1.051 | 11.855 |
| PSL ≥10,000 mg | 3.972 | 1.091 | 14.467 |
| CNI
non-responder | 19.833 | 3.950 | 99.590 |
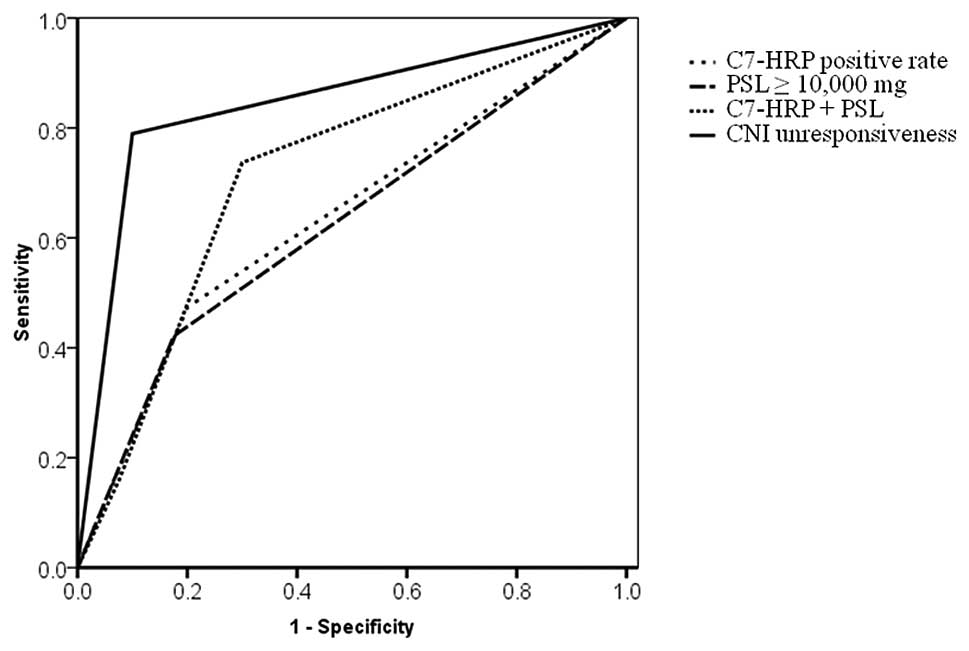
To evaluate the prognostic yield, ROCs were plotted
for a colectomy within 1 year following CNI administration
(Fig. 4). The area under the curve
(AUC), sensitivity and specificity were as follows: i) positivity
for C7-HRP (AUC, 63.7%; sensitivity, 47.4%; specificity, 80%); ii)
PSL ≥10,000 mg (AUC, 62.3%; sensitivity, 42.1%, specificity,
82.5%); iii) positivity for C7-HRP + PSL ≥10,000 mg (AUC, 71.4%;
sensitivity, 73.7%; specificity, 92.5%); and iv) CNI
non-responsiveness (AUC, 84.5%; sensitivity, 78.9%; specificity,
90%). As compared to positivity for C7-HRP alone or PSL ≥10,000 mg
alone, the combination of these two factors improved the prognostic
yield (AUC 71.4%). CNI non-responsiveness was the strongest factor
for predicting a colectomy within 1 year following CNI
administration.
Factorial analyses for cytomegalovirus antigenemia
and cumulative steroid dose were also conducted. Positivity for
C7-HRP was strongly related to older age and endoscopic findings
(Table V). On the other hand,
cumulative steroid dose was affected by disease duration and
severity (Table VI).
| Table V.Risk estimates of positivity for
C7-HRP. |
Table V.
Risk estimates of positivity for
C7-HRP.
| | 95% CI
|
|---|
| Characteristic | Risk estimate | Lower | Upper |
|---|
| Male gender | 0.436 | 0.120 | 1.584 |
| Age ≥40 years | 4.125 | 1.237 | 13.754 |
| Disease duration ≥4
years | 0.802 | 0.249 | 2.585 |
| Seo’s CIDAI ≥220
points | 1.514 | 0.472 | 4.858 |
| Prior AZA
treatment | 0.769 | 0.209 | 2.838 |
| Undermining ulcer
present | 3.529 | 1.051 | 11.855 |
| Pancolitis | 1.429 | 0.425 | 4.801 |
| PSL ≥10,000 mg | 2.000 | 0.580 | 6.898 |
| Table VI.Risk estimates of PSL ≥10,000 mg. |
Table VI.
Risk estimates of PSL ≥10,000 mg.
| | 95% CI
|
|---|
| Characteristic | Risk estimate | Lower | Upper |
|---|
| Male gender | 2.292 | 0.631 | 8.317 |
| Age ≥40 years | 0.269 | 0.054 | 1.348 |
| Disease duration ≥4
years | 7.333 | 1.954 | 27.528 |
| Seo’s CIDAI ≥220
points | 0.170 | 0.046 | 0.628 |
| Prior AZA
treatment | 3.403 | 0.974 | 11.891 |
| Undermining ulcer
present | 0.417 | 0.122 | 1.421 |
| Pancolitis | 0.700 | 0.208 | 2.353 |
| C7-HRP
positive | 2.000 | 0.580 | 6.898 |
Ganciclovir for cytomegalovirus
antigenemia and multiple administrations of CNIs
Of the 17 patients, 12 were administered ganciclovir
due to cytomegalovirus antigenemia. However, ganciclovir treatment
did not improve CNI responsiveness. The response rate for CNIs were
25% (3/9) in the ganciclovir-treated group and 40% (2/5) in the
ganciclovirnon-treated group.
Although most patients responded to CNI induction
therapy with a single course, 9 patients required multiple CNI
administrations due to relapse. Seven out of these 9 patients
underwent induction therapy by using CSA twice. However, none of
them became quiescent following the second CSA administration,
resulting in colectomies. On the other hand, 2 of these 9 patients
had induction therapy by first receiving CSA and secondarily FK506.
These two patients stayed in remission by taking oral FK506 as a
maintenance therapy. Infliximab was used in 4 patients to treat
relapses, resulting in three patients going into remission and one
patient undergoing a colectomy.
Adverse events
No serious bacterial infections occurred during CNI
treatment. The administration of CSA was discontinued in four
cases: two cases due to liver dysfunction, and one due to renal
dysfunction. An antihypertensive drug was started in the last case
during CSA treatment. A magnesium agent was administered in four
cases due to hypomagnesemia. FK506 was discontinued in one case due
to renal dysfunction.
Discussion
Prospective and retrospective studies have already
reported the prognostic factors for colectomy, such as clinical,
laboratory, radiological, endoscopic and genetic findings (9). In this study, the disease extent
(10–13), disease duration (14,15),
gender (16,17) and endoscopic findings (14,15,18,19)
were not significant predictive factors for a colectomy as well as
CNI non-responsiveness, although previous reports have identified
these factors to predict the outcome. Most of these previous
reports investigated the prognostic factors of patients treated
with corticosteroids. On the other hand, our study focused on the
predictive outcomes of CNIs used to treat steroid-refractory or
steroid-dependent UC. Our study population and the therapeutic
agents used may have affected the results of our investigation.
Almost all of our study participants were steroid-refractory or
steroid-dependent. Furthermore CNIs were reported to be effective
in patients with steroid-refractory or steroid-dependent UC. As the
strength of treatment increases, predictive factors previously
reported are thought to become insignificant.
It is natural that CNI non-responsiveness is the
best predictor for a colectomy within one year following start of
CNI treatment. It is particularly notable that the ROC demonstrated
a moderate accuracy for colectomy prediction within one year by
combining positivity for C7-HRP plus PSL ≥10,000 mg, since these
two factors may be obtained prior to or shortly following start of
the CNI treatment.
Cytomegalovirus (CMV) reactivation is known as an
important exacerbating factor (20–22).
However, the clinical significance of CMV reactivation remains
controversial. Matsuoka et al claimed that the clinical
significance of CMV reactivation was limited, showing that
cytomegalovirus was frequently reactivated in active UC patients;
however, it disappeared without antiviral agents. Therefore, they
concluded that if cytomegalovirus antigenemia is low, antiviral
therapies may not be necessary for most UC patients (23). On the other hand, Yoshino et
al claimed that antiviral therapy was essential if CMV is
monitored by mucosal quantitative real-time polymerase chain
reaction (PCR), showing that 10 (83.3%) of the 12 patients with
CMV-DNA positivity in the inflamed mucosa went into remission after
applying antiviral therapy and modulating immunosuppressive
therapies, and that 12 (92.3%) of the 13 CMV-DNA-negative UC
patients went into remission following treatment with more intense
immunosuppressive therapies (24).
Our results revealed that ganciclovir treatment did not improve the
CNI responsiveness, and that C7-HRP may be used as a predictive
marker for CNI non-responsiveness and for a colectomy. In this
context, C7-HRP does not provide sufficient information for making
a decision whether or ganciclovir should be started; however,
positivity for C7-HRP indicates poor prognosis. In accordance with
a previous report (25), our
results also demonstrated that the patients of older age have
higher risk of cytomegalovirus reactivation.
Corticosteroids are the standard therapeutic drug
for UC. Our results revealed the strong connection between the
longer disease duration and cumulative steroid dose. Of course, it
should be taken into account that an enormous cumulative
corticosteroid dose is indirectly selecting a refractory patient
population. However, large amounts of steroid use may exacerbate
the refractory properties of UC. Yoshiyama et al reported
that cumulative steroid-overdosed UC patients may have a functional
deficit in neutrophils (26).
Although our study cannot determine whether the results reflect the
refractory characteristics of the patients themselves or support a
dysfunction of neutrophil-related immunity in steroid-overdosed
patients, a prior overdose of corticosteroids was also a
significant marker for CNI non-responsiveness and a colectomy.
The response rate to CSA and FK506 was similar in
our results. However, FK506 had a slower onset of action than
intravenous CSA. This is due to the fact that peroral FK506
required an average of 8.5 days to reach a high trough level (10–15
ng/ml) in our patients. Those patients who need urgent induction
should be treated with intravenous CSA rather than oral FK506. On
the other hand, once successful induction was obtained, oral FK506
may be better for maintenance therapy than oral CSA from the
viewpoint of keeping stable drug serum levels. AZA is a crucial
agent that maintains disease quiescence. Our results highlighted
the importance of a bridging therapy to avoid a colectomy.
In conclusion, the prognostic factors for CNI
efficacy and a colectomy were as follows: i) more than 10,000 mg
PSL used prior to starting the CNI treatment; and ii) positivity
for C7-HRP. Although the efficacy of CSA and FK506 was similar, the
onset of action in induction therapy was earlier for CSA than
FK506. Furthermore, the addition of AZA following successful
induction therapy is important in order to avoid a colectomy.
References
|
1
|
Sandborn W: A critical review of
cyclosporin therapy in inflammatory bowel disease. Inflamm Bowel
Dis. 1:48–63. 1995.
|
|
2
|
Actis GC, Ottobrelli A, Pera A, et al:
Continuously infused cyclosporine at low dose is sufficient to
avoid emergency colectomy in acute attacks of ulcerative colitis
without the need for high-dose steroids. J Clin Gastroenterol.
17:10–13. 1993. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Lichtiger S, Present DH, Kornbluth A, et
al: Cyclosporine in severe ulcerative colitis refractory to steroid
therapy. N Engl J Med. 330:1841–1845. 1994. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Fellermann K, Tanko Z, Herrlinger KR, et
al: Response of refractory colitis to intravenous or oral
tacrolimus (FK506). Inflamm Bowel Dis. 8:317–324. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Ogata H, Matsui T, Nakamura M, et al: A
randomised dose finding study of oral tacrolimus (FK506) therapy in
refractory ulcerative colitis. Gut. 55:1255–1262. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Bamba S, Tsujikawa T, Inatomi O, et al:
Factors affecting the efficacy of cyclosporin A therapy for
refractory ulcerative colitis. J Gastroenterol Hepatol. 25:494–498.
2010. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
http://www.info.pmda.go.jp/downfiles/ph/PDF/800126_3999014M1022_3_18.pdfuri
|
|
8
|
Seo M, Okada M, Yao T, Ueki M, Arima S and
Okumura M: An index of disease activity in patients with ulcerative
colitis. Am J Gastroenterol. 87:971–976. 1992.PubMed/NCBI
|
|
9
|
Travis S, Satsangi J and Lemann M:
Predicting the need for colectomy in severe ulcerative colitis: a
critical appraisal of clinical parameters and currently available
biomarkers. Gut. 60:3–9. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Meyers S, Lerer PK, Feuer EJ, Johnson JW
and Janowitz HD: Predicting the outcome of corticoid therapy for
acute ulcerative colitis. Results of a prospective, randomized,
double-blind clinical trial. J Clin Gastroenterol. 9:50–54. 1987.
View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Truelove SC and Jewell DP: Intensive
intravenous regimen for severe attacks of ulcerative colitis.
Lancet. 1:1067–1070. 1974. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Oshitani N, Kitano A, Fukushima R, et al:
Predictive factors for the response of ulcerative colitis patients
during the acute-phase treatment. Digestion. 46:107–113. 1990.
View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Chakravarty BJ: Predictors and the rate of
medical treatment failure in ulcerative colitis. Am J
Gastroenterol. 88:852–855. 1993.PubMed/NCBI
|
|
14
|
Turner D, Mack D, Leleiko N, et al: Severe
pediatric ulcerative colitis: a prospective multicenter study of
outcomes and predictors of response. Gastroenterology.
138:2282–2291. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Carbonnel F, Gargouri D, Lemann M, et al:
Predictive factors of outcome of intensive intravenous treatment
for attacks of ulcerative colitis. Aliment Pharmacol Ther.
14:273–279. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Kumar S, Ghoshal UC, Aggarwal R, Saraswat
VA and Choudhuri G: Severe ulcerative colitis: prospective study of
parameters determining outcome. J Gastroenterol Hepatol.
19:1247–1252. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Elloumi H, Ben Abdelaziz A, Derbel F, et
al: Predictive factors of glucocorticosteroid treatment failure in
severe acute idiopathic colitis. Acta Gastroenterol Belg.
68:226–229. 2005.PubMed/NCBI
|
|
18
|
Oshitani N, Matsumoto T, Jinno Y, et al:
Prediction of short-term outcome for patients with active
ulcerative colitis. Dig Dis Sci. 45:982–986. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Cacheux W, Seksik P, Lemann M, et al:
Predictive factors of response to cyclosporine in
steroid-refractory ulcerative colitis. Am J Gastroenterol.
103:637–642. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Vega R, Bertran X, Menacho M, et al:
Cytomegalovirus infection in patients with inflammatory bowel
disease. Am J Gastroenterol. 94:1053–1056. 1999. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Loftus EV Jr, Alexander GL and Carpenter
HA: Cytomegalovirus as an exacerbating factor in ulcerative
colitis. J Clin Gastroenterol. 19:306–309. 1994. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Cottone M, Pietrosi G, Martorana G, et al:
Prevalence of cytomegalovirus infection in severe refractory
ulcerative and Crohn’s colitis. Am J Gastroenterol. 96:773–775.
2001.
|
|
23
|
Matsuoka K, Iwao Y, Mori T, et al:
Cytomegalovirus is frequently reactivated and disappears without
antiviral agents in ulcerative colitis patients. Am J
Gastroenterol. 102:331–337. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Yoshino T, Nakase H, Ueno S, et al:
Usefulness of quantitative real-time PCR assay for early detection
of cytomegalovirus infection in patients with ulcerative colitis
refractory to immunosuppressive therapies. Inflamm Bowel Dis.
13:1516–1521. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Kuwabara A, Okamoto H, Suda T, Ajioka Y
and Hatakeyama K: Clinicopathologic characteristics of clinically
relevant cytomegalovirus infection in inflammatory bowel disease. J
Gastroenterol. 42:823–829. 2007. View Article : Google Scholar
|
|
26
|
Yoshiyama S, Miki C, Okita Y, Araki T,
Uchida K and Kusunoki M: Neutrophil-related immunoinf lammatory
disturbance in steroid-overdosed ulcerative colitis patients. J
Gastroenterol. 43:789–797. 2008. View Article : Google Scholar : PubMed/NCBI
|