Introduction
Malignant ascites, an abnormal accumulation of fluid
in the peritoneal cavity caused by tumor infiltration or secretion,
is a recognized indication of end-stage events in various types of
cancer. The local fluid accumulation of ascites may cause abdominal
pain, bowel obstruction, loss of appetite, nausea, fatigue,
anorexia and cachexia, which deteriorate the quality of life of
patients. The mean survival rate of patients following the
diagnosis of malignant ascites is approximately 20 weeks (1). Therefore, palliating the symptoms and
prolonging survival have become the foremost goal. The treatment of
malignant ascites remains a difficult problem to solve. The
established approaches include salt restriction, diuresis,
peritoneovenous shunts, paracentesis and chemotherapy via
intraperitoneal injection in selected cases. However, these
conventional methods occasionally relieve symptoms but only for a
short while, and do not prolong survival. Their effects are
variable and unreliable. Since there are no generally accepted and
evidence-based guidelines for the management of malignant ascites
(2), novel methods are required
for its treatment in the clinic.
The increased peritoneal microvascular permeability
is one of the main factors which contributes to the development of
malignant ascites. Vascular endothelial growth factor (VEGF) is
believed to be a primary influence in stimulating vessel formation
and increasing vascular permeability, which is related to the
formation of malignant metastases (3). Therefore, anti-VEGF is a promising
candidate for the clinical treatment of malignant ascites.
Endostatin, a 20-kDa C-terminal fragment of collagen
XVIII identified by O'Reilly in 1997, significantly inhibits
VEGF-induced endothelial cell proliferation and decreases
angiogenesis and tumor growth (4).
However, the poor stability, low biochemical activity and high
production costs limit the clinical application of collagen XVIII.
The Chinese scientist Luo Yongzhang developed Endostar, a novel
recombinant human endostatin containing an additional 9-amino acid
sequence at the N-terminus to improve its stability and biological
activity, and produced Endostar in E. coli to reduce the
production costs (5). Endostar was
approved in 2005 by the State Food and Drug Administration of China
(SFDA) for the treatment of non-small cell lung cancer (NSCLC)
following phase I–III clinical trials in China (6). Currently, the drug is used to treat
different types of tumors combined with chemotherapy in the clinic
(7). Endostar is provided to treat
malignant ascites and significantly improve quality of life with
high efficiency and low toxicity (8).
β-elemene, extracted from Chinese medicinal herbs,
including Curcuma wenyujin YH Chen & C Ling, has
broad-spectrum antitumor activity by inhibiting proliferation and
inducing apoptosis in several types of solid tumor cells (9). Curcuma wenyujin inhibits tumor
growth and metastasis by suppressing VEGF-mediated angiogenesis
(10), and demonstrates
synergistic effects on lung cancer cells when combined with taxanes
(11). In phase III clinical
trials, it was observed that intraperitoneal injection of β-elemene
relieved the symptoms of malignant ascites and improved quality of
life with minor side effects (12).
Although Endostar and β-elemene are effective agents
for the treatment of malignant ascites, it is always difficult to
control refractory and recurrent malignant ascites by
administration of a single drug. Therefore, a combination therapy
for obstinate ascites is likely to be valuable in the clinic. In
the present study, we evaluated the effects of Endostar and
β-elemene, alone and combined, on malignant ascites in an H22
ascitic mouse model. The peritoneal microvascular permeability and
the underlying mechanism was also investigated.
Materials and methods
Cell culture and animal model
H22 hepatoma ascitic cells were purchased from the
Institute of Biochemistry and Cell Biology of the Chinese Academy
of Sciences (Shanghai, China). H22 cells were cultured in RPMI-1640
medium containing 10% fetal bovine serum in a Forma Series II
water-jacketed incubator (Thermo Fisher Scientific, Rockford, IL,
USA) at 37°C under a humidified atmosphere of 5% CO2.
The expression of VEGF mRNA and protein in H22 cells was verified
by quantitative real-time polymerase chain reaction (RT-qPCR) and
western blot analysis, respectively. Female ICR mice (6 weeks old,
18–20 g) were purchased from Shanghai Laboratory Animal Center, CAS
(SLACCAS, Shanghai, China) and maintained in pathogen-free cages at
the Animal Experimental Center. Animal quality was controlled
(Certification #2007000523797).
To establish the mouse model of malignant ascites,
cultured H22 cells were harvested and prepared as a cell suspension
at a concentration of 1×107 cells/ml in
phosphate-buffered saline (PBS). Mice were intraperitoneally
injected with 0.2 ml of cell suspension (total, 2×106
cells/mouse). The procedure was not associated with mortality or
morbidity.
All possible steps were taken to avoid animal
suffering at each stage of the experiment. The procedures used in
this study had the approval of the Institutional Animal Care and
Use Committee of Jiangsu Simcere Pharmaceutical Research
Institute.
Reagents
Endostar solution (10 g/l, batch #YY2011008) was
provided by Simcere Pharmaceutical Research (Nanjing, China).
β-elemene (l-methyl-l-vinyl-2,4-diisopropenyl-cyclohexane) solution
(5 g/l, batch #0909221) was purchased from Jingang Pharmaceutical
(Dalian, China).
RPMI-1640 culture medium and fetal bovine sera were
purchased from Gibco (Grand Island, NY, USA). Primary antibodies
for VEGF, MMP-2 and β-actin were obtained from Abcam (Cambridge,
MA, USA). Enzyme-linked immunosorbent assay (ELISA) kits for VEGF,
matrix metalloproteinase-2 (MMP-2) and hypoxia inducible factor 1α
(HIF1α) were purchased from R&D (Minneapolis, MN, USA). Evans
blue dye was purchased from Sigma (St. Louis, MO, USA).
Animal treatment
The doses of Endostar and β-elemene used to treat
malignant ascites in the clinic are 30 mg/m2 (8) and 200–300 mg/m2 (12) via intraperitoneal injection, and
the translated dose from human to mouse is approximately 8 mg/kg
and 50–75 mg/m2, respectively. Therefore, the dose range
of Endostar and β-elemene used in this research was 4, 8 and 16
mg/kg and 50, 75 and 100 mg/kg, respectively. The safety of these
doses (Endostar 16 mg/kg, β-elemene 100 mg/ kg and their
combination) was evaluated in our previous study, and no
drug-induced hematological toxicity, hepatotoxicity or liver and
kidney injury were observed (unpublished data).
To determine the most effective dose of Endostar and
β-elemene, we evaluated the effects of different doses on malignant
ascites in the mouse model. The mice were randomly divided into
seven treatment groups (n=20, each) 24 h after intraperitoneal
injection of H22 cells. The control group received the vehicle used
in all treatments, i.e., 0.9% normal saline (NS); the Endostar
treatment groups received 4, 8 and 16 mg/kg of Endostar in NS; and
the β-elemene treatment groups received 50, 75 and 100 mg/kg of
β-elemene in NS. Mice were administered the respective drug
treatment once a day for eight days via intraperitoneal injection.
A total of 10 mice from each group were euthanized by
CO2 inhalation 24 h after the final drug administration
and ascites were collected to measure the volume. The remaining 10
mice were maintained until death to determine the survival
rate.
To determine the optimal dose combination of
Endostar and β-elemene, we combined the most effective dose of
Endostar with the other doses of β-elemene, and combined the most
effective dose of β-elemene with the other doses of Endostar.
Different dose combinations were used to treat ascitic mice. The
treatments were the same as those previously mentioned.
Other therapeutic effects and the underlying
mechanisms were investigated with the optimal dose combination. The
mice were randomly divided into four treatment groups (n=20, each)
24 h after intraperitoneal injection of H22 cells. The control
group received NS, the Endostar group and β-elemene group received
their single doses which were used in the combination group and the
combination group received the optimal dose combination. The
treatments were the same as previously mentioned and 10 mice of
each group were euthanized to collect ascites samples for further
detection. A remaining 10 mice per group were used for Evans blue
extravasation detection.
Physical, cellular and biochemical
examinations
To measure the ascites volume, ascites fluid was
collected and measured via syringe from the opened abdominal wall
following euthanasia.
The ascites fluid samples were diluted 10-fold prior
to analysis. The tumor cells were counted under a microscope
(CKX41, Olympus, Tokyo, Japan). Each sample was counted three times
and the average was calculated.
The ascitic protein was examined by clinical
biochemical analyzer (7020, Hitachi, Tokyo, Japan).
Evans blue extravasation detection
To determine whether the drugs decreased the
peritoneal microvascular permeability, the leakage of Evans blue
dye into the ascites fluid was analyzed (13). A total of 10 mice from each group
were injected with 0.2 ml of 5% Evans blue solution via the caudal
vein. The Evans blue solution was prepared using 5 g Evans blue dye
dissolved in 100 ml 0.9% NS. Ascites fluid was collected 2 h
post-injection and the samples were centrifuged at 2,000 rpm for 5
min. The extravasated Evans blue dye in the supernatants was
assessed at 540 nm by a spectrophotometer (UV-2450, Shimadsu,
Columbia, MD, USA).
ELISA
To evaluate the influence of drugs on cytokines in
the ascites fluid, VEGF, MMP-2 and HIF1α in the ascites fluid were
analyzed using an ELISA assay. The ascites samples were collected
and centrifuged at 2,000 rpm for 5 min and the supernatants were
analyzed.
Western blot analyses
Western blotting was performed to analyze the
expression of VEGF and MMP-2 in tumor cells. Tumor cells were lysed
in 1X lysis buffer and lysates centrifuged (Centrifuge 5415R,
Eppendorf, Cambridge, UK) at 13,000 x g for 15 min at 4°C. The
protein concentration was determined by bicinchoninic acid (BCA)
assay (Pierce BCA Protein Assay kit, Thermo Fisher Scientific). The
20–50 μg samples were resolved by SDS-PAGE and transferred to a
nitrocellulose membrane. The blots were blocked with PBS containing
5% powdered milk at room temperature for 1 h, then sequentially
incubated with primary antibodies overnight at 4°C, followed by
secondary antibodies for 1 h at 37°C. Finally, the blots were
detected using electrochemiluminescence (ECL) reagents and Bio-Rad
Molecular Imager ChemiDoc XRS + imaging system (Bio-Rad, Hercules,
CA, USA). The optical densities of protein bands were analyzed with
Sigma Scan Pro 5 and normalized with a loading control.
Reverse transcription and real-time
quantitative PCR (RT-qPCR)
The RT-qPCR assay was used to analyze VEGF
mRNA in tumor cells. Total RNA was isolated from tumor cells for
reverse transcription and RT-qPCR with the appropriate primers
designed by Primer software (version 5.0). The specific primer
pairs for VEGF were: forward, 5′-AGACACACCCACCCACATACA-3′;
reverse, 5′-ACATCCTCCTCCCAACACAAG-3′. The RT-qPCR assay was
performed following the manufacturer's instructions (MultiGene
Gradient, Labnet International, Inc., Edison, NJ, USA). All samples
were subjected to 40 cycles of PCR, which included triplicate
samples and controls with no template. β-actin was used as the
reference.
Statistical analyses
Data are presented as mean ± standard deviation
(SD). SPSS software (version 16.0, SPSS, Chicago, IL, USA) was used
for data analysis. For multiple mean comparisons, the one-way ANOVA
least significant difference (LSD) method was performed to
determine the homogeneity of variance or the Games-Howell method
for heterogeneity of variance. The Kaplan-Meier method was used to
analyze survival rate and draw survival curves. The log-rank test
was applied to compare survival curves. P<0.05 was considered to
indicate a statistically significant result.
To analyze the effects of the drugs in combination,
the coefficient of drug interaction (CDI) was calculated. The CDI
was calculated as follows: CDI = AB/(A x B) (14). According to the ascites volumes of
each group, AB is the ratio of the combination group to the control
group, A or B is the ratio of the single agent group to control
group. A CDI value <1, =1 or >1 indicates the synergistic,
additive or antagonistic effect, respectively. CDI<0.7 indicates
that the drug combination is significantly synergistic.
Results
Optimal effective dose of Endostar and
β-elemene is 8 and 100 mg/kg, respectively
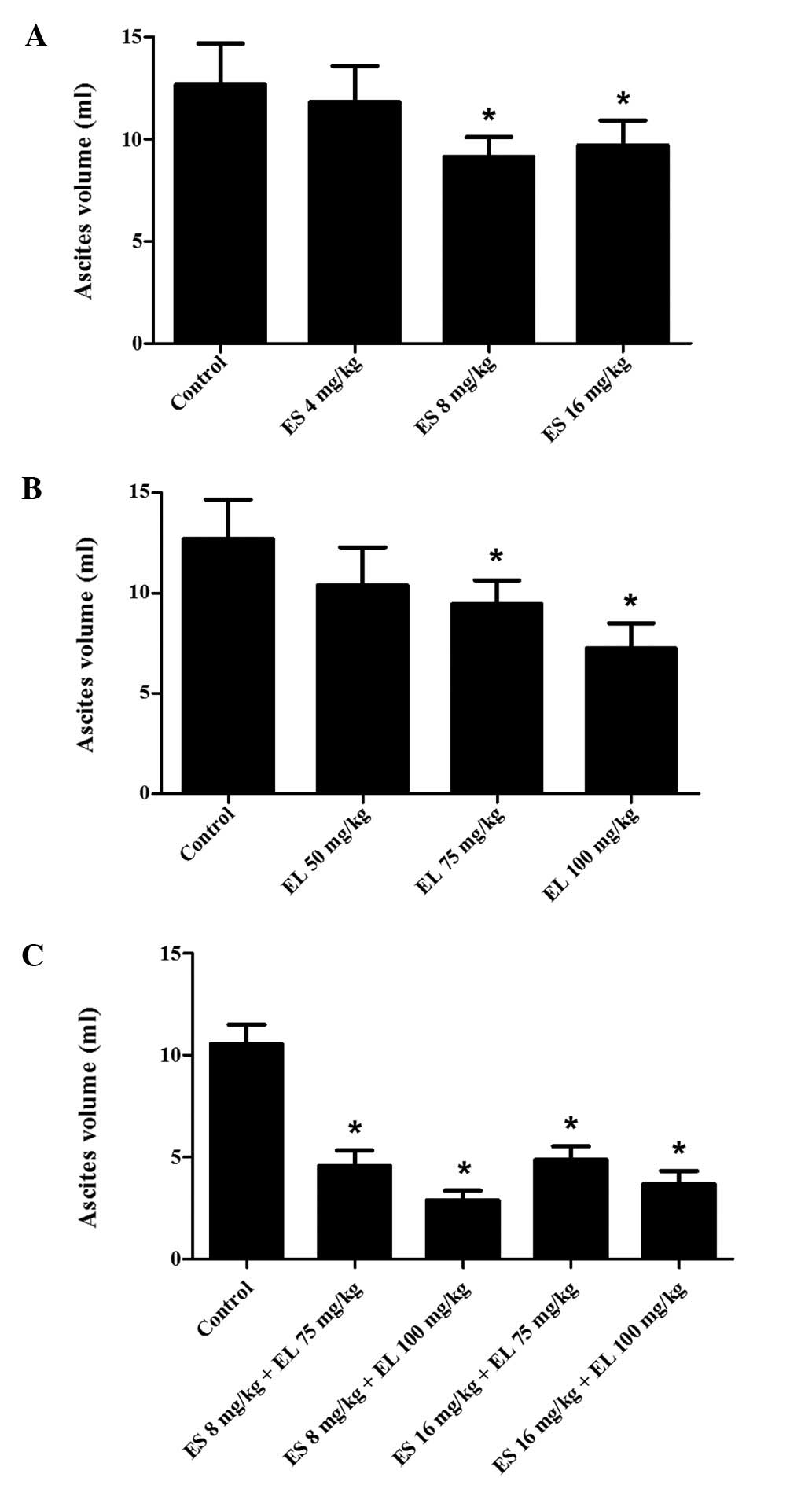
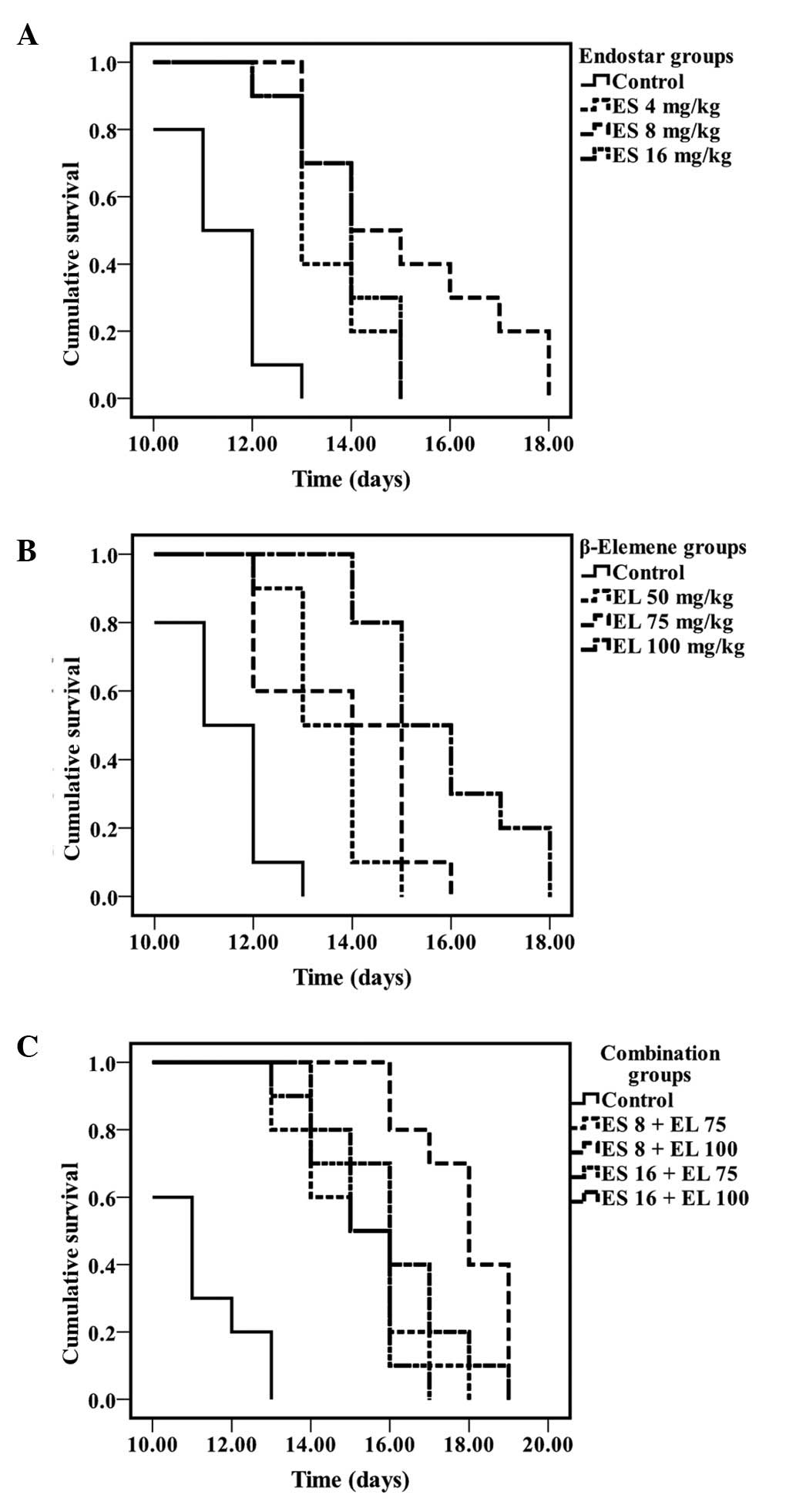
In the Endostar treatment groups, the mean ascites
volume in the 8 mg/kg group was significantly less than that of the
other two groups (P<0.05; Fig.
1A), and the survival of the 8 mg/kg group was also longest
(P<0.05; Fig. 2A). In the
β-elemene treatment groups, the mean ascites volume in 100 mg/kg
group was the lowest (P<0.05; Fig.
1B), and it improved the survival rate to a greater extent
(P<0.05; Fig. 2B). There was no
difference in the mean ascites volumes between the 4 mg/kg Endostar
and control group (P>0.05); this was also observed in the 50
mg/kg β-elemene group and the control groups (P>0.05).
Therefore, we combined 8 and 16 mg/kg Endostar with 75 and 100
mg/kg β-elemene separately, to produce four combination groups as
follows: 8 mg/ kg Endostar plus 75 mg/kg β-elemene, 8 mg/kg
Endostar plus 100 mg/kg β-elemene, 16 mg/kg Endostar plus 75 mg/kg
β-elemene and 16 mg/kg Endostar plus 100 mg/kg β-elemene.
Optimal dose combination is 8 mg/kg
Endostar plus 100 mg/ kg β-elemene
All treatment groups decreased the ascites formation
(P<0.05; Fig. 1C) and also
improved the survival of the mice (P<0.05; Fig. 2C). Among the four combination
groups, the mean ascites volume in the 8 mg/kg Endostar plus 100
mg/ kg β-elemene group was the lowest (P<0.05) and the survival
rate of mice was also the longest (P<0.05). Hence, 8 mg/kg
Endostar plus 100 mg/kg β-elemene was the optimal dose combination
in the present study.
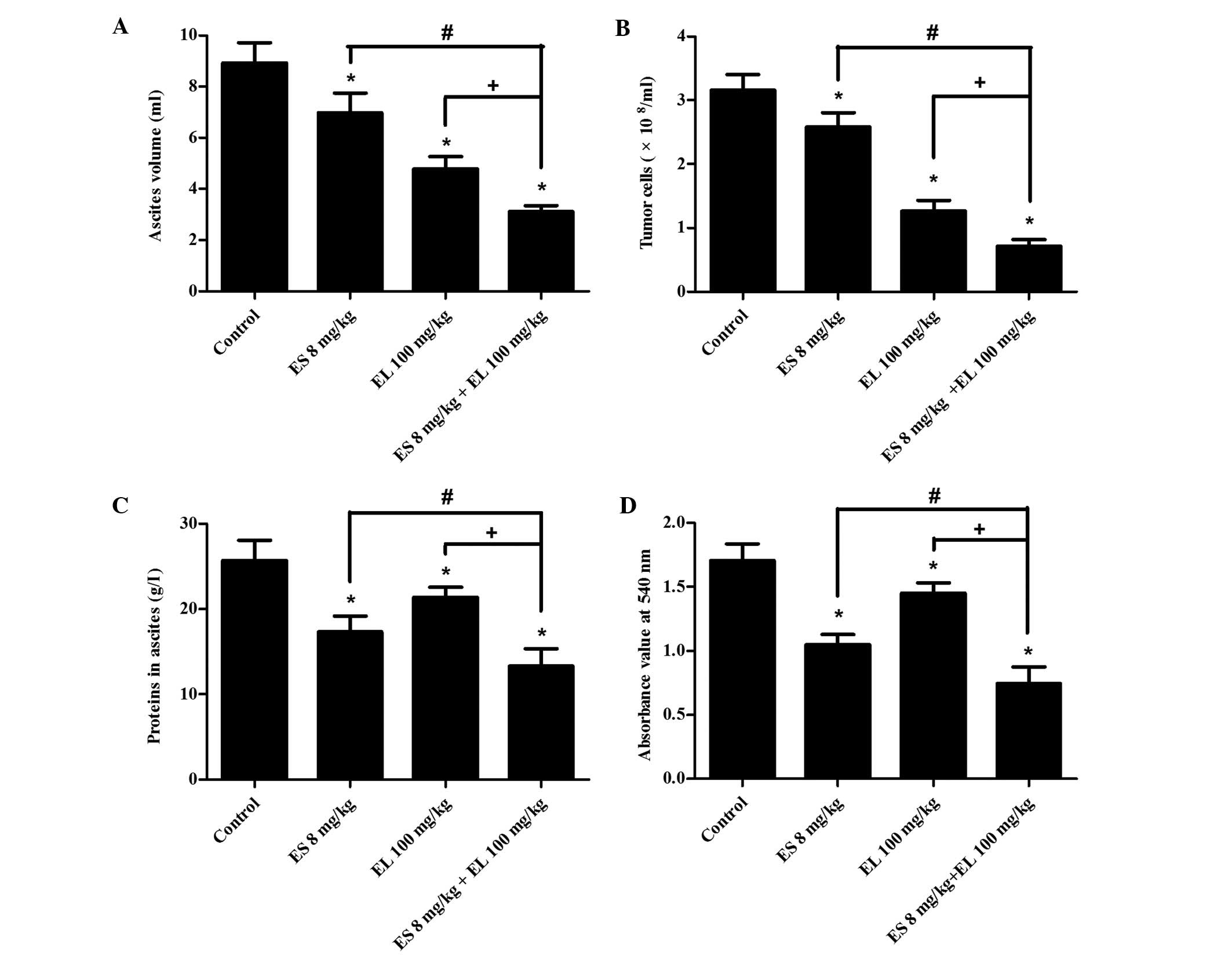
Formation of malignant ascites is
synergistically suppressed
The results of the malignant ascites fluid assays
included mean ascites volume, tumor cell number and ascitic protein
levels. The mean ascites volumes in the control, Endostar,
β-elemene and combination groups were 8.93±0.79, 7.34±0.76,
4.79±0.47 and 3.12±0.23 ml. The ascites volume in the combination
group was less than that of the other three groups (P<0.05;
Fig. 3A) and the CDI value was
0.79, which indicated that 8 mg/kg Endostar plus 100 mg/kg
β-elemene treatment synergistically suppressed the formation of
malignant ascites. Compared with Endostar and β-elemene groups, the
tumor cell number and ascitic protein in the combination group were
also significantly decreased (P<0.05; Fig. 3B and C).
Peritoneal microvascular permeability is
reduced
The extravasation of Evans blue dye into the
peritoneal cavity is an indirect indicator of peritoneal vascular
permeability. The amount of Evans blue in the peritoneal cavity was
assessed from absorbance readings (540 nm) of supernatants prepared
from ascites fluid samples. The mean absorbance value of the
control, Endostar, β-elemene and combination groups was 1.71±0.13,
1.05±0.08, 1.45±0.09 and 0.88±0.07, respectively. In the Endostar
and β-elemene groups, the mean absorbance value was significantly
lower than that of the control group (P<0.05; Fig. 3D). Among the four groups, the mean
absorbance in the combination group was the lowest (P<0.05),
suggesting that the 8 mg/kg Endostar plus 100 mg/kg β-elemene
effectively reduced peritoneal microvascular permeability.
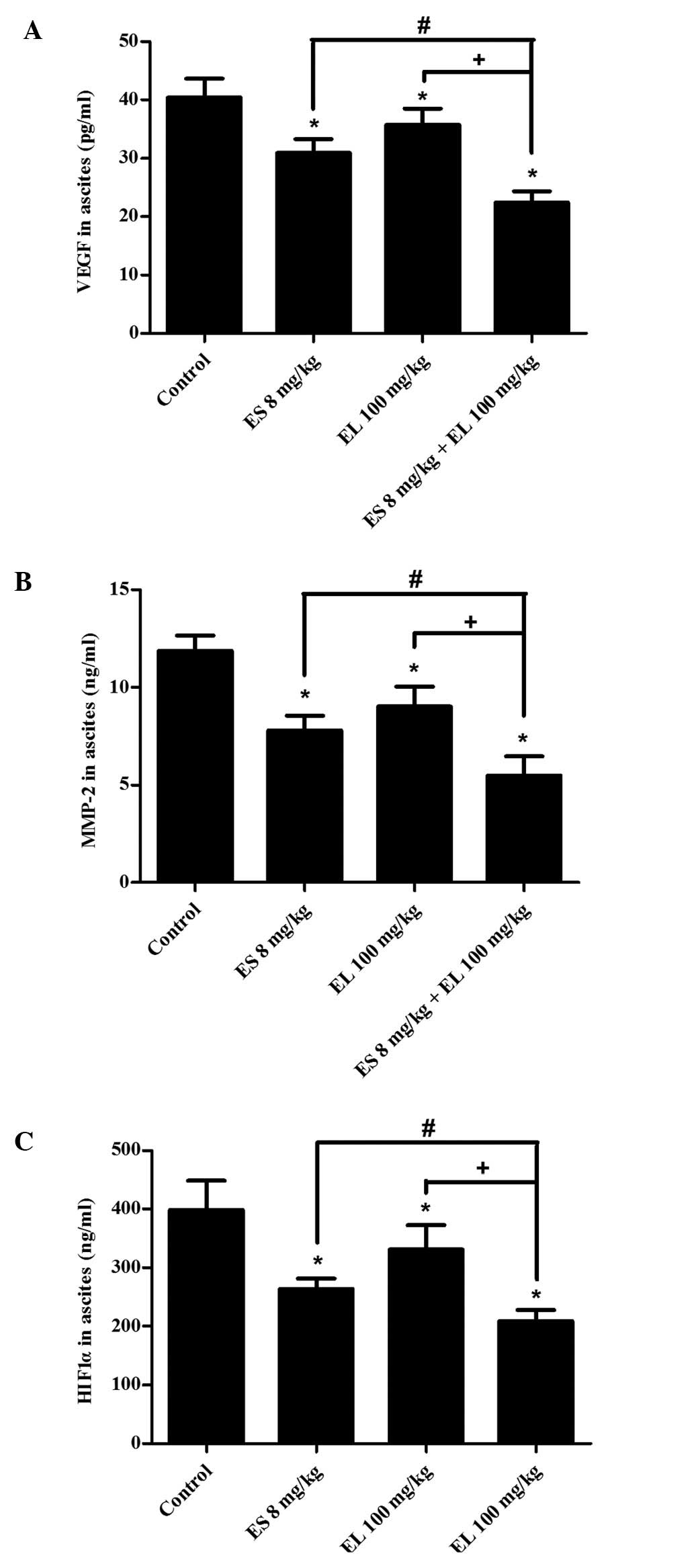
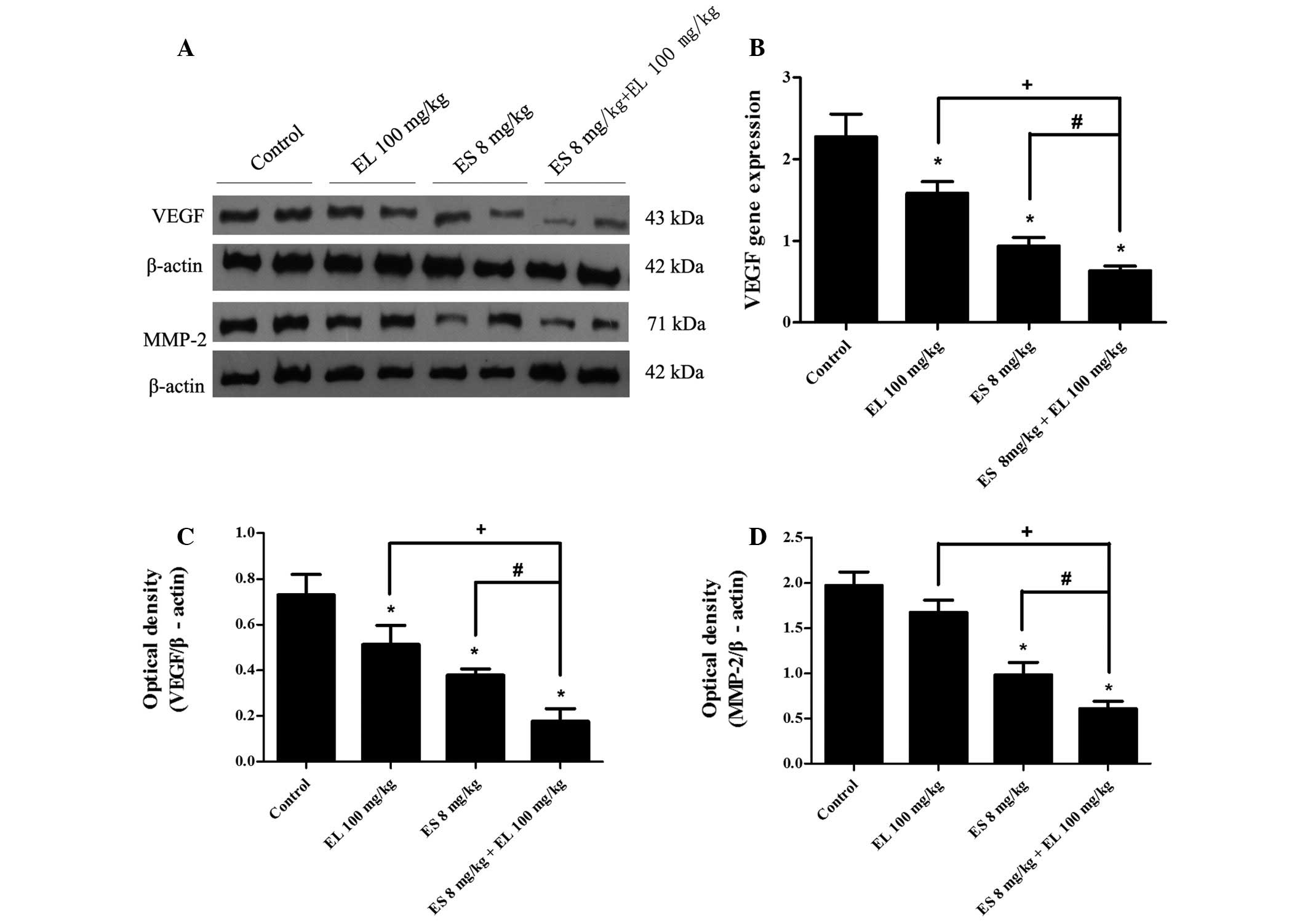
VEGF, MMP-2 and HIF1α are
downregulated
The ELISA results revealed that the levels of VEGF,
MMP-2, and HIF1α in ascites were significantly lower in the
combination group than in either the Endostar or β-elemene single
treatment group (P<0.05; Fig.
4). Western blotting showed that the levels of VEGF in ascitic
tumor cells were downregulated in both the Endostar and β-elemene
groups, and were lowest in the combination group (P<0.05;
Fig. 5A and C). There was no
difference in the levels of MMP-2 between the β-elemene group and
control group (P>0.05), but it was downregulated in the Endostar
group, and the effects were enhanced in the combination group
(P<0.05; Fig. 5A and D).
Furthermore, the relative expression of VEGF mRNA
was 2.28±0.28, 0.94±0.11, 1.58±0.15 and 0.63±0.06 in the control,
Endostar, β-elemene and combination groups, respectively. The
results showed that VEGF mRNA of tumor cells in Endostar,
β-elemene and combination groups was also suppressed, and it was
lowest in the combination group (P<0.05; Fig. 5B).
Discussion
It is generally believed that antiangiogenic therapy
mainly stabilizes tumor growth by cutting off the blood supply, but
its objective response rate (ORR) is limited. For example, the ORR
of Endostar is only 3–5%. Therefore, antiangiogenesis is usually
combined with cytotoxic agents to improve the efficiency. While
β-elemene is considered to be a powerful antineoplastic agent, it
is reasonable to apply the combination therapy of Endostar and
β-elemene in the treatment of malignant ascites and to verify the
treatment efficacy via the H22 mouse ascites model (15).
We evaluated the effects of Endostar and β-elemene
on inhibiting ascites formation and prolonging survival, and
determined their optimal dose combination. The results of this
study showed that the mice with a smaller ascites volume survived
longer, which indicates that inhibiting the ascites fluid may be an
effective method to prolong lifespan for patients with malignant
ascites in the clinic.
The formation of malignant ascites is the result of
tumor peritoneal cavity metastasis, thus suppression of tumor cells
is the most direct and effective therapy. In this study, the
combination of Endostar and β-elemene enhanced the effects of the
suppression of tumor cell growth, which may be mainly due to
β-elemene. As mentioned previously, the high peritoneal
microvascular permeability plays a significant role in the
formation of malignant ascites (3), which increases the leakage of fluid
from peritoneal microvessels to the peritoneal cavity and
accelerates the accumulation of ascites fluid. In the present
study, the peritoneal microvascular permeability was markedly
decreased by Endostar and β-elemene, and proteins in the ascites
fluid leaked from peritoneal microvessels were also reduced,
particularly with combination treatment. Thus, Endostar and
β-elemene synergistically inhibit the formation of ascites, and the
survival rate of mice was also prolonged.
The formation of malignant ascites involves
increased peritoneal microvasculature, invasion and metastasis of
tumor cells and the anoxic environment of the peritoneal cavity,
which are associated with VEGF, MMP-2 and HIF1α. Therefore, we
determined the levels of the related cytokines and factors.
Firstly, the results of the present study indicate
that combining Endostar with β-elemene causes a greater significant
reduction in VEGF mRNA and protein in ascites fluid and
tumor cells than treatment with either Endostar or β-elemene alone,
and that the levels of VEGF are correlated with the peritoneal
microvascular permeability. VEGF is a multi-functional cytokine
that contributes to stimulating angiogenesis and augmenting the
permeability of the pre-existing microvasculature. The
VEGF-mediated increase in vessel permeability for plasma proteins
is 10,000 times higher than that induced by histamine (16). Markedly elevated levels of VEGF
have been observed in malignant pleural effusions and ascites fluid
(17), and VEGF levels correlate
with its ability to induce vascular leakage, which can be blocked
by anti-VEGF therapy (18).
Therefore, blocking the high peritoneal microvascular permeability
induced by VEGF may have been the most significant reason for the
inhibition of malignant ascites in this study.
Secondly, a greater reduction of MMP-2 in ascites
fluid and tumor cells was observed in 8 mg/kg Endostar plus 100
mg/kg β-elemene treated mice than either 8 mg/kg Endostar or 100
mg/kg β-elemene treatments alone. MMPs are able to degrade
regulatory proteins associated with the tumor microenvironment and
promote the invasion of tumor cells through normal tissues and
blood vessel walls resulting in metastasis and the expression and
activities of MMPs are increased in almost all kinds of human
cancers compared with normal tissues (19). As an indication of tumor
metastasis, the formation of malignant ascites is a complex process
that includes cell adhesion, invasion and migration, while MMPs,
mainly MMP-2 and MMP-9, have been shown to be multi-functional
promoters attributing to malignant ascites formation. In a study on
type IV collagenase (MMP-2 and MMP-9) activity in benign and
malignant ascites, MMP-2 and MMP-9 were detectable only in
malignant ascites (20).
Therefore, combination treatment may suppress the invasion and
metastasis of tumor cells in the peritoneal cavity by the strong
downregulation of MMP-2, resulting in the reduction of ascites
formation.
Finally, the more marked inhibition of HIF1α in
ascites fluid was observed in mice treated with 8 mg/kg Endostar
plus 100 mg/kg β-elemene, and the levels of VEGF and MMP-2 were
simultaneously decreased by treatment. HIF1α is a transcription
factor that plays an essential role in cellular and systemic
responses to hypoxia. Under hypoxic conditions, the hypoxia
signalling pathway is activated through a series of steps involving
the upregulation of HIF1α, nuclear translocation, dimerization with
HIF1β, binding to DNA and induction of gene transcription;
VEGF, erythropoietin (EPO) and nitric oxide synthase
(NOS) are induced for angiogenesis, erythropoiesis and
glycolysis that improve cellular adaption to hypoxia and the
restoration of oxygen homeostasis (21). The upregulated MMP-2 under hypoxic
conditions, a common phenomenon in tumors, was decreased by the
inhibition of HIF1α in malignant gliomas (22). Tumor cells growing in ascites
suffer from a severe anoxic environment, and the rapid
proliferation of tumor cells aggravates hypoxia, which activates
HIF1α and induces the transcription of VEGF and
MMP-2. Elevated levels of VEGF increase high peritoneal
microvascular permeability, and over-expressed MMP-2 promotes tumor
invasion and metastasis. Consequently, VEGF and MMP-2 cooperatively
facilitate the formation of malignant ascites. The results of the
present study suggest that the inhibition of HIF1α caused by
Endostar and β-elemene may contribute to the decrease of
hypoxia-induced VEGF and MMP-2, at least in part.
In conclusion, the mechanism related to the
combination therapy may involve two mechanisms. The first is that
β-elemene inhibits the proliferation of tumor cells, and decreases
the secretion of cytokines by reducing tumor burden; while Endostar
inhibits tumor growth by its effect of antiangiogenesis and
downregulation of MMP-2 and HIF1α, which enhances the suppression
of tumor cells. The second is that Endostar decreases the
peritoneal microvascular permeability by anti-VEGF effects that are
enhanced by β-elemene. As a result, they cooperatively inhibit the
formation of malignant ascites and prolong the lifespan of
mice.
Although the decrease in VEGF, MMP-2 and HIF1α was
considered to be correlated with the inhibition of malignant
ascites in this study, the underlying mechanism remains unclear. A
variety of signaling pathways play essential roles in the
development of tumors, and further studies are needed to determine
whether signaling pathways, including PI3K/Akt, ERK1/2 or p38 MAPK,
are involved in the treatment of malignant ascites by Endostar and
β-elemene.
Our study initially demonstrated that combined
therapy with Endostar and β-elemene synergistically inhibited
ascites formation and prolonged the survival rate in a mouse model
of H22 ascitic hepatoma cells. The underlying mechanism may be
related to the enhanced effects of suppressing tumor cells and
decreasing peritoneal microvascular permeability, as well as the
inhibition of VEGF, MMP-2 and HIF1α. This study provided
substantial experimental evidence to support this combination
therapy regimen in the clinic.
Acknowledgements
The study was financially supported by
Jiangsu Simcere Pharmaceutical Research Co., Ltd. This manuscript
was edited by Medjaden Bioscience Limited. We thank members of the
laboratory and our collaborators for the numerous useful
suggestions.
References
|
1.
|
Garrison RN, Kaelin LD, Galloway RH and
Heuser LS: Malignant ascites: clinical and experimental
observations. Ann Surg. 203:644–651. 1986. View Article : Google Scholar : PubMed/NCBI
|
|
2.
|
Becker G, Galandi D and Blum HE: Malignant
ascites: systematic review and guideline for treatment. Eur J
Cancer. 42:589–597. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
3.
|
Tamsma JT, Keizer HJ and Meinders AE:
Pathogenesis of malignant ascites: Starling's law of capillary
hemodynamics revisited. Ann Oncol. 12:1353–1357. 2001.PubMed/NCBI
|
|
4.
|
O'Reilly MS, Boehm T, Shing Y, et al:
Endostatin: an endogenous inhibitor of angiogenesis and tumor
growth. Cell. 88:277–285. 1997.
|
|
5.
|
Ling Y, Yang Y, Lu N, et al: Endostar, a
novel recombinant human endostatin, exerts antiangiogenic effect
via blocking VEGF-induced tyrosine phosphorylation of KDR/Flk-1 of
endothelial cells. Biochem Biophys Res Commun. 361:79–84. 2007.
View Article : Google Scholar
|
|
6.
|
Wang J, Sun Y, Liu Y, et al: Results of
randomized, multicenter, double-blind phase III trial of
rh-endostatin (YH-16) in treatment of advanced non-small cell lung
cancer patients. Zhongguo Fei Ai Za Zhi. 8:283–290. 2005.(In
Chinese).
|
|
7.
|
Li Y, Huang XE, Yan PW, et al: Efficacy
and safety of endostar combined with chemotherapy in patients with
advanced solid tumors. Asian Pac J Cancer Prev. 11:1119–1123.
2010.PubMed/NCBI
|
|
8.
|
Jiang Z and Qin S: Study progression of
recombinant human endostatin (Endostar) for the treatment of
malignant serous effusion. Chinese-German J Clin Oncol. 10:435–441.
2011. View Article : Google Scholar
|
|
9.
|
Li QQ, Wang G, Huang F, et al:
Antineoplastic effect of beta-elemene on prostate cancer cells and
other types of solid tumor cells. J Pharm Pharmacol. 62:1018–1027.
2010. View Article : Google Scholar : PubMed/NCBI
|
|
10.
|
Chen W, Lu Y, Wu J, et al: Beta-elemene
inhibits melanoma growth and metastasis via suppressing vascular
endothelial growth factor-mediated angiogenesis. Cancer Chemother
Pharmacol. 67:799–808. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
11.
|
Zhao J, Li QQ, Zou B, et al: In vitro
combination characterization of the new anticancer plant drug
β-elemene with taxanes against human lung carcinoma. Int J Oncol.
31:241–252. 2007.
|
|
12.
|
Wang J, Zhang H and Sun Y: Phase III
clinical trial of elemenum emulsion in the management of malignant
pleural and peritoneal effusions. Zhonghua Zhong Liu Za Zhi.
18:464–467. 1996.(In Chinese).
|
|
13.
|
Kanaoka Y, Maekawa A, Penrose JF, et al:
Attenuated zymosan-induced peritoneal vascular permeability and
IgE-dependent passive cutaneous anaphylaxis in mice lacking
leukotriene C4 synthase. J Biol Chem. 276:22608–22613. 2001.
View Article : Google Scholar
|
|
14.
|
Cao SS and Zhen YS: Potentiation of
antimetabolite antitumor activity in vivo by dipyridamole and
amphotericin B. Cancer Chemother Pharmacol. 24:181–186. 1989.
View Article : Google Scholar : PubMed/NCBI
|
|
15.
|
Zhang J, Wang X and Lu H: Amifostine
increases cure rate of cisplatin on ascites hepatoma 22 via
selectively protecting renal thioredoxin reductase. Cancer Lett.
260:127–136. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
16.
|
Senger DR, Galli SJ, Dvorak AM, et al:
Tumor cells secrete a vascular permeability factor that promotes
accumulation of ascites fluid. Science. 219:983–985. 1983.
View Article : Google Scholar
|
|
17.
|
Zebrowski BK, Liu W, Ramirez K, et al:
Markedly elevated levels of vascular endothelial growth factor in
malignant ascites. Ann Surg Oncol. 6:373–378. 1999. View Article : Google Scholar : PubMed/NCBI
|
|
18.
|
Luo JC, Toyoda M and Shibuya M:
Differential inhibition of fluid accumulation and tumor growth in
two mouse ascites tumors by an antivascular endothelial growth
factor/permeability factor neutralizing antibody. Cancer Res.
58:2594–2600. 1998.
|
|
19.
|
Egeblad M and Werb Z: New functions for
the matrix metalloproteinases in cancer progression. Nat Rev
Cancer. 2:161–174. 2002. View
Article : Google Scholar : PubMed/NCBI
|
|
20.
|
Sun XM, Dong WG, Yu BP, et al: Detection
of type IV collagenase activity in malignant ascites. World J
Gastroenterol. 9:2592–2595. 2003.PubMed/NCBI
|
|
21.
|
Hewitson KS, McNeill LA and Schofield CJ:
Modulating the hypoxia-inducible factor signaling pathway:
applications from cardiovascular disease to cancer. Curr Pharm Des.
10:821–833. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
22.
|
Fujiwara S, Nakagawa K, Harada H, et al:
Silencing hypoxiainducible factor-1α inhibits cell migration and
invasion under hypoxic environment in malignant gliomas. Int J
Oncol. 30:793–802. 2007.
|