Introduction
Diffuse large B-cell lymphoma (DLBCL) is the most
common type of non-Hodgkin’s lymphoma (NHL). Recently, a large
epidemiological study was performed in the Chinese population.
Although the official data have yet to be published, the
preliminary results and other clinicopathological studies have
shown that DLBCL accounts for approximately 30–40% of new NHL cases
in China (1,2). Current insight into the pathogenesis
of DLBCL and its highly variable outcome suggest that DLBCL is a
heterogeneous group of lymphomas with various genetic
abnormalities, clinical characteristics and prognosis, as opposed
to a single clinicopathological entity (3).
During the past several decades, the
cyclophosphamide, doxorubicin, vincristine and prednisone (CHOP)
chemotherapy regimen has been the gold standard of DLBCL therapy.
However, the cure rate that is achieved using standard chemotherapy
alone is only 30–40% (4,5). Recently, the addition of rituximab to
the conventional CHOP regimen (R-CHOP) has led to a marked
improvement in survival in previously untreated elderly (older than
60 years of age) and young (60 or younger) DLBCL patients. These
results have been confirmed by the Groupe d’Etude des Lymphomes de
l’Adulte study (GELA/LNH-98-5) (6)
and the MabThera International Trial (MInT) (7).
Although considerable progress in the treatment of
DLBCL has been made in the era of rituximab, a significantly
variable outcome remains for a substantial minority of patients who
are not cured. Therefore, a well-validated and accurate prognostic
system is required to serve as the basis for risk-adjusted therapy
for DLBCL. Such a system would allow clinicians to rapidly and
easily stratify patients with various prognoses and provide a more
individualised therapy.
The International Prognostic Index (IPI) was
introduced by Shipp and the International Non-Hodgkin’s Lymphoma
Prognostic Factors Project in the 1990s (8,9) and
has become a widely accepted prognostic index for patients with
aggressive lymphomas. In this system, the patient age, tumour
stage, serum lactate dehydrogenase concentration, performance
status and number of extranodal disease sites all serve to identify
four discrete risk groups with varying 5-year overall survival
rates that range from 26 to 73%.
However, the IPI system is an individual case-based
prognostic factor for the analysis of CHOP-like regimens. In recent
studies, the question of whether (and to what extent) the
prognostic index should be changed in the context of novel
immunochemotherapy strategies has been intensely debated. More
recently, Sehn et al investigated this issue by analysing
the role of the IPI in a register-based retrospective study of 365
patients who were treated with R-CHOP (10). Their results suggested that the
revised International Prognostic Index (R-IPI) predicts patient
outcome more reliably than the standard IPI for DLBCL patients who
are treated with R-CHOP. The R-IPI is a redistribution of the
original IPI factors rather than an identification of new
prognostic markers. Using a scoring system with the same adverse
parameters, three discrete prognostic groups (0=very good; 1 or
2=good; and 3, 4, or 5=poor) can be identified as having
significantly different outcomes.
To date, most of the reports regarding the IPI or
R-IPI have been limited to Western countries. Therefore, we
conducted a multicentre retrospective analysis of Chinese DLBCL
patients who were treated with CHOP-like chemotherapy alone or
R-CHOP-like chemotherapy to reassess whether the IPI system, which
is a well-known paradigm for risk assessment, is applicable to
Chinese DLBCL populations and therefore still has value in the
immunochemotherapy era. We also assessed whether the R-IPI system
discriminates more between patients with various prognoses. To the
best of our knowledge, this is the first report of a multicentre
study in an unselected Chinese population of DLBCL patients.
Materials and methods
Patient characteristics
This study was a retrospective analysis of newly
diagnosed DLBCL patients who were treated at six participating
hospitals between 1997 and 2008, and were evaluated by the Shanghai
Lymphoma Research Group (SLRG). The histological diagnoses were
reviewed and classified according to the WHO classification system.
The clinical and demographic data were also reviewed. Patients were
selected for inclusion in this study based on the following
criteria; a histologically confirmed diagnosis of CD20-positive
DLBCL, previously untreated, aged 18 or older, no primary or
secondary central nervous system involvement, no cardiac
contraindication to anthracycline treatment, no human
immunodeficiency virus infection and no severe co-morbid illness
that precluded the treatment of lymphoma. Informed consent was
obtained from every patient. The study was approved by the
ethics-review committee of every participating centre.
Treatment and efficacy evaluation
All patients were treated with a CHOP-like regimen ±
rituximab as a first-line therapy. In the R-CHOP-like group, the
dosage and schedule of rituximab was 375 mg/m2 on day 0
of each cycle for a minimum of four cycles. The treatment cycle was
21 days in length. The patients who experienced neutropenia
received granulocyte colony-stimulating factor (G-CSF); if the
neutropenia persisted until the next cycle, the following cycle was
postponed by up to two weeks. The efficacy evaluation was performed
upon the completion of the treatment. The response of the lymphoma
was classified as a complete response (CR), a partial response
(PR), a stable disease (SD), a progressive disease (PD), or a
relapse (R) in accordance with the International Workshop Criteria
(11).
Statistical methods
The analysis was based on the follow-up information
that was available by May 1 2010. Progression-free survival (PFS)
was calculated from the date of the diagnosis until either
documented disease progression or the date that the patient was
last known to be alive for patients who succumbed to causes that
were unrelated to the lymphoma or its treatment. Overall survival
(OS) was calculated from the date of the diagnosis until mortality,
regardless of the cause. PFS and OS were assessed using the
Kaplan-Meier method and were compared between the groups using the
log-rank test. The clinical characteristics and efficacy
evaluations were compared between the subgroups using the
χ2 test. All P-values were calculated as two-sided, and
P<0.05 was considered to indicate a statistically significant
result. The data were analysed using the Statistical Software
Package for the Social Sciences (SPSS version 13.0 for Windows;
SPSS Inc., Chicago, IL, USA).
Results
Patient characteristics
A total of 438 patients who met the inclusion
criteria were identified, among which 241 were treated with a
CHOP-like regimen alone and 197 patients were treated with an
R-CHOP-like regimen. The majority of the patients (96.6%) received
an anthracycline-based regimen, and the remaining patients (3.4%)
were treated with mitoxantrone-COP. The median age at diagnosis was
50 years (range, 18–83 years) and the male:female ratio was 1.06:1.
Overall, 75.6% of the patients completed 6–8 cycles of
chemotherapy. The median follow-up was at 34 months (range, 3–145
months), and 106 mortalities were reported by the time of the last
follow-up; among these mortalities, 73 and 33 occurred in the
CHOP-like and R-CHOP-like groups, respectively. The clinical
characteristics and distributions of the individual IPI factors at
the time of diagnosis are listed in Table I. The baseline patient
characteristics were matched for age, gender, number of treatment
cycles and prognostic factors of the IPI between the two
groups.
 | Table IPatients and disease
characteristics. |
Table I
Patients and disease
characteristics.
| Characteristic | R-CHOP-like
(n=197) | CHOP-like
(n=241) |
|---|
| Age, years, median
(range) | 55 (18–80) | 54 (18–83) |
| Male | 98 (50%) | 136 (56%) |
| Median observation
time, months (range) | 31 (4–97) | 39 (3–145) |
| IPI factors | | |
| Age, years | | |
| >60 | 59 (30%) | 83 (34%) |
| ≤60 | 138 (70%) | 158 (66%) |
| Performance
status | | |
| >1 | 42 (21%) | 53 (22%) |
| ≤1 | 155 (79%) | 188 (78%) |
| Lactate
dehydrogenase | | |
| >normal | 77 (39%) | 81 (33%) |
| ≤normal | 120 (61%) | 160 (67%) |
| Stage | | |
| III–IV | 107 (54%) | 134 (56%) |
| I–II | 90 (46%) | 107 (44%) |
| Extranodal
sites | | |
| >1 | 48 (24%) | 74 (30%) |
| ≤1 | 149 (76%) | 167 (70%) |
Patient outcome according to the standard
IPI strata
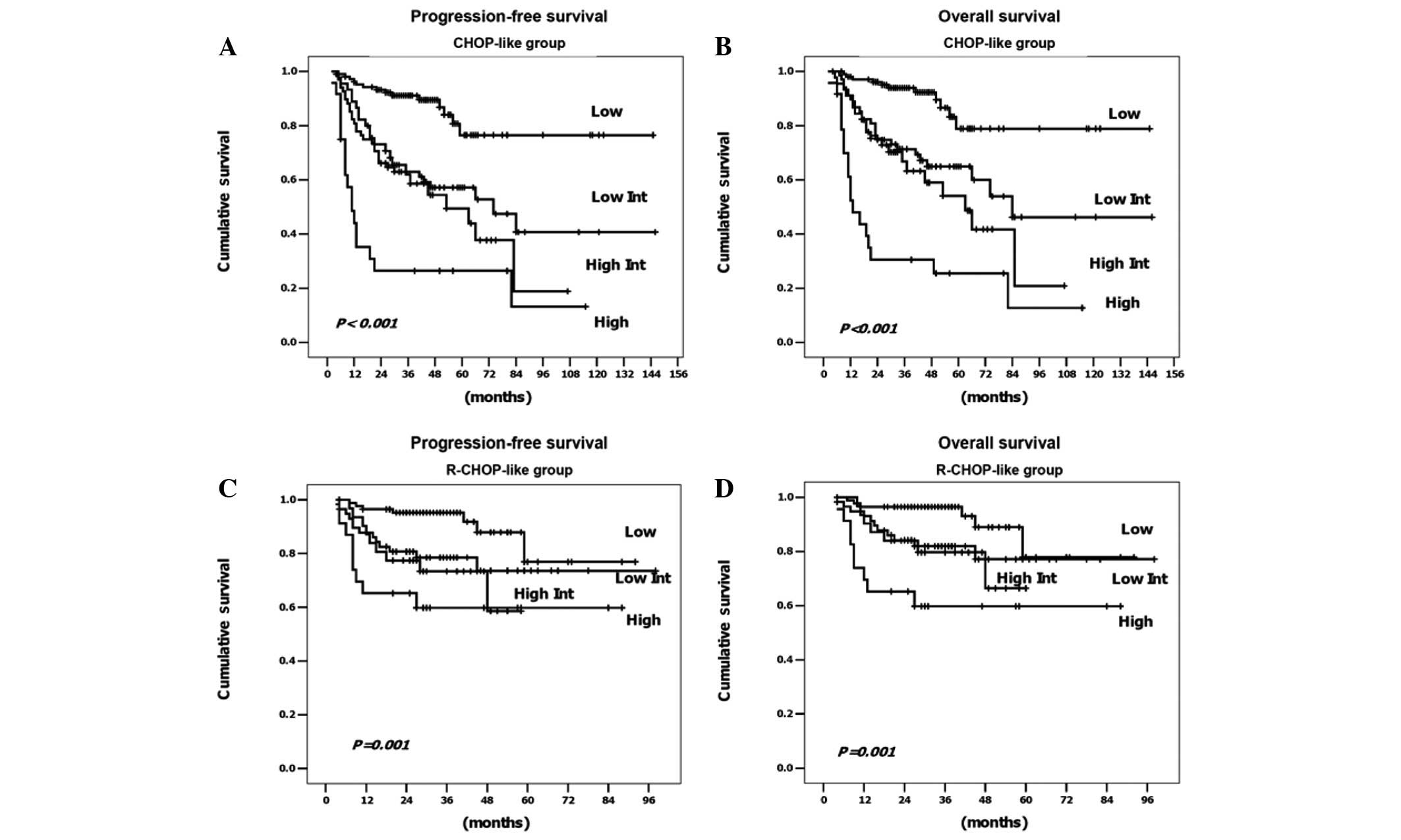
The treatment outcomes based on the standard IPI are
summarised in Table II. Within the
group of 241 patients who were treated with CHOP-like alone, the
standard IPI score was highly predictive of outcome and
discriminated well between the four groups. The 3-year PFS rates
ranged from 26.5 to 91.1% (P<0.001) and the 3-year OS rates
ranged from 30.6 to 93.9% (P<0.001). Within the group of 197
patients who were treated with R-CHOP-like, the IPI score remained
predictive. The 3-year PFS rates ranged from 59.8 to 95.2%
(P=0.001), and the 3-year OS rates ranged from 59.8 to 96.4%
(P=0.001). However, the IPI score no longer distinguished between
the four risk groups; instead, the low/low-intermediate risk group
and the high-intermediate/high risk group showed clearly
overlapping curves (Fig. 1).
| Table IIOutcome according to the standard IPI
and the revised-IPI. |
Table II
Outcome according to the standard IPI
and the revised-IPI.
| | R-CHOP-like
| CHOP-like
|
|---|
| Risk group | No. of IPI
factors | No. (%) | 3-year PFS | 3-year OS | No. (%) | 3-year PFS | 3-year OS |
|---|
| Standard IPI | | | | | | | |
| Low | 0, 1 | 84 (43) | 95.2% | 96.4% | 105 (44) | 91.1% | 93.9% |
|
Low-intermediate | 2 | 58 (29) | 78.5% | 81.9% | 67 (28) | 63.9% | 72.4% |
|
High-intermediate | 3 | 32 (16) | 73.0% | 79.7% | 45 (19) | 62.0% | 66.8% |
| High | 4, 5 | 23 (12) | 59.8% | 59.8% | 24 (10) | 26.5% | 30.6% |
| P-value | | | 0.001 | 0.001 | | <0.001 | <0.001 |
| Revised IPI | | | | | | | |
| Very good | 0 | 50 (25) | 96.0% | 96.0% | 51 (21) | 91.8% | 91.8% |
| Good | 1, 2 | 92 (47) | 84.3% | 87.6% | 121 (50) | 75.6% | 82.7% |
| Poor | 3, 4, 5 | 55 (28) | 67.5% | 71.1% | 69 (29) | 50.2% | 54.7% |
| P-value | | | 0.001 | 0.003 | | <0.001 | <0.001 |
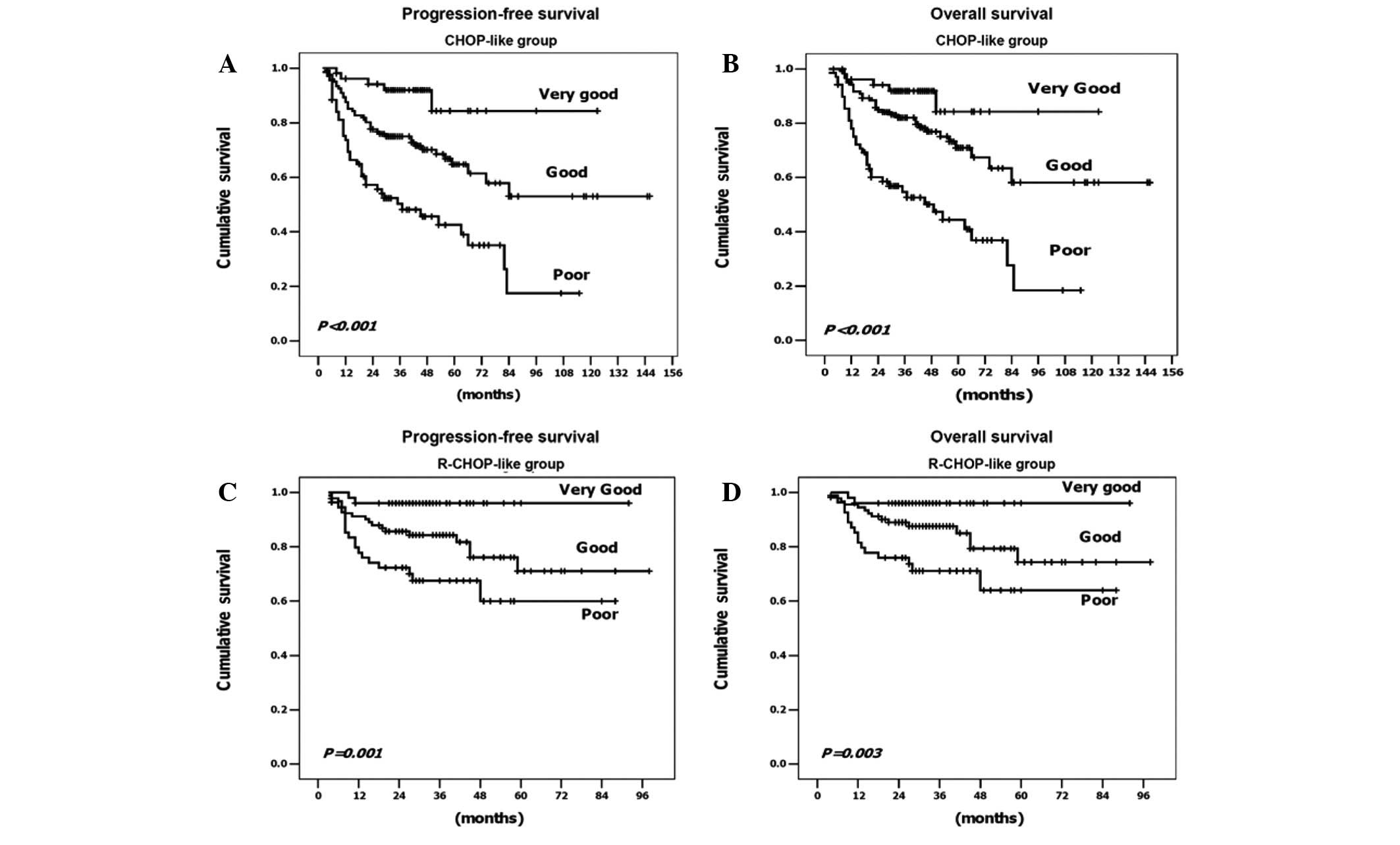
Patient outcome according to the R-IPI
strata
To determine the efficacy of the R-IPI, the patients
were redistributed into three groups containing 0, 1–2 and 3–5 risk
factors, thereby generating the following three new prognostic
groups; very good, good and poor, respectively. The PFS and OS of
the CHOP-like and R-CHOP-like patients based on their R-IPI score
are displayed in Table II and
Fig. 2. We observed three discrete
curves that represent the three prognostic groups. In the group of
patients who were treated with an R-CHOP-like regimen, the three
risk groups had distinctly different 3-year PFS rates of 96, 84.3
and 67.5% (P=0.001) and 3-year OS rates of 96, 87.6 and 71.1%
(P=0.003), respectively. In the group of patients who did not
receive rituximab, similar results were observed, except for
reduced PFS and OS in the CHOP-like group compared with the
R-CHOP-like group (this was particularly true for the patients in
the poor prognostic group). Thus, the R-IPI was prognostically
relevant for both PFS and OS in the DLBCL patients who were treated
with either an R-CHOP-like or CHOP-like regimen.
Discussion
Over the past decade, considerable effort has been
expended in the search for predictive and prognostic information to
use for risk stratification in clinical settings. Since its
introduction in 1993, the IPI system has become a well-known,
convenient and useful prognostic index for DLBCL patients. Among
the various novel prognostic models that contain numerous promising
biomarkers, including those of cellular origin (such as germinal
centre B cell and activated B cell types) and immunoexpression
patterns (including p53, Ki67, Bcl-2, Bcl-6, CD10 and CD5), none
has achieved the required level of acceptance to be routinely used
for risk stratification of DLBCL patients (12–16).
Since a number of studies have demonstrated that the
introduction of new therapies is able to change the predictive
value of established prognostic systems, the relevance of the
prognostic markers varies depending on the geographic region and
patient ethnicity, due to the various baseline clinical
characteristics of these patients. Thus, revalidation of these
systems is essential. The goal of the present study was to reassess
the current perceived value of the standard IPI system and to
determine whether the R-IPI system reliably discriminates between
patients with different survival outcomes in the Chinese
population.
Our data demonstrate that among patients who were
treated with a CHOP-like regimen alone, the standard IPI score was
able to predict the outcome and discriminate clearly among the four
groups. However, in the patients who were treated with an
R-CHOP-like regimen, although the score remained predictive, the
standard IPI could not distinguish between the patients who were at
low/low-intermediate risk and high-intermediate/high risk in the
Kaplan-Meier survival curve. The groups produced closely
overlapping curves according to the standard IPI strata and this is
consistent with the results of previous clinical studies by Sehn
et al (10) and Bari et
al (17).
In addition, in the present study, we attempted to
apply the R-IPI to the patients who were treated with a CHOP-like
or R-CHOP-like regimen. Upon redistribution of the IPI factors into
an R-IPI, a more clinically useful prediction of outcome was
observed in both groups of patients treated with or without
rituximab. In the CHOP-like group, three risk groups were
identified based on the R-IPI strata; very good, good and poor;
with 3-year PFS rates of 91.8, 75.6 and 50.2%, respectively, and
3-year OS rates of 91.8, 82.7 and 54.7%, respectively. Notably, the
results were particularly significant from the patients who
received the R-CHOP-like regimen. Three clear curves representing
prognostic groups were observed. Of these patients, 25% were
classified into the very good prognostic group, with a greater than
96% chance of 3-year PFS and OS. Therefore, according to a series
of randomised studies, R-CHOP is now preferable to CHOP as the gold
standard of therapy for this favourable prognostic group of
patients with DLBCL. However, despite the extremely favourable
outcome, care must be taken to avoid excessive toxicity that can
result from unnecessary treatments. Almost 50% of the patients were
classified in the good prognostic group and had 3-year PFS and OS
rates of 84.3 and 87.6%, respectively. To improve the outcome for
this less-favourable subgroup of patients, randomised clinical
trials may be required. Among the poor risk group, which comprised
28% of the cases, the 3-year PFS and OS rates were only 67.5 and
71.1%, respectively. To improve the prognosis for these patients,
early intervention with innovative approaches or high-dose
chemotherapy followed by autologous stem cell rescue should be
considered. In a group of 94 DLBCL patients, Vitolo et al
(on behalf of the Italy GIMURELL group) reported the following
impressive results for dose-dense and high-dose chemotherapy plus
rituximab together with autologous stem cell transplantation; in
good-risk patients, according to the R-IPI, the 4-year OS rate was
estimated at 87% and the most significant finding was that these
positive results persisted for poor-risk patients with a 4-year OS
rate that was estimated at 73% (18). These encouraging data indicate that
patients with a poor prognosis should benefit from this treatment
strategy.
We noted that the addition of the R-IPI to the
prognosis of DLBCL patients in the rituximab era has remained
controversial, as demonstrated by certain recent reports. An
analysis performed by Ziepert et al (19), which involved 1,062 patients with
DLBCL who were accrued from three prospective trials [the MinT,
RICOVER-60 (20) and MegaCHOEP
(21) trials], confirmed the
prognostic relevance of the standard IPI score for PFS, event-free
survival and OS endpoints. Thus, they concluded that the standard
IPI is still valid for patients with DLCBL in the R-CHOP era.
However, Tay et al (22)
recently noted certain weaknesses in the study. First, different
chemotherapy regimens were used in the three trials from which the
data were collected. Second, their data set was an
under-representation of young high-risk patients. Only 55 (5.2%) of
the young patients with two or more risk factors were included in
the analysis. In another study, Advani et al (23) evaluated the performance of the
standard IPI and the following modifications; age adjusted
(AA)-IPI, R-IPI and an elderly IPI with an age cut-off of 70 years
(E-IPI) in patients over 60 years of age who were treated with
R-CHOP. They found that the R-IPI did not identify a highly
favourable risk group, thus minimising its usefulness in this
population, whereas the IPI and AA-IPI were considered to be useful
tools for outcome prediction in patients over the age of 60 who
were treated with R-CHOP. However, this conclusion applies only to
elderly patients and is less appropriate for other DLBCL
populations. Notably, in our study, our data support the conclusion
that the R-IPI has a strong prognostic relevance for PFS and OS
among patients who are treated with or without rituximab. To the
best of our knowledge, this is the first multicentre study
analysing the impact of the R-IPI in an unselected Chinese
population of DLBCL patients.
In conclusion, this multicentre study provides
insights for analysing prognostic factors in DLBCL patients. Our
data indicate that the standard IPI is applicable to Chinese DLBCL
populations and remains predictive for the chemotherapy group.
However, adjustments are required for a more precise prognostic
prediction in the immunochemotherapy era. The R-IPI, which is a
redistribution of the original IPI factors, may serve as a
simplified and more clinically relevant predictor of outcome than
the standard IPI, and the use of the R-IPI may aid the
identification of poor prognostic subgroups of newly diagnosed
DLBCL patients. Since the current study was not a randomised
clinical trial, a larger population-based prospective study and
meta-analysis are highly recommended for further validation of our
conclusions. New therapeutic strategies and early interventions are
required to improve the outcome of DLCBL in the R-IPI poor
prognostic group.
Acknowledgements
This study was supported, in part, by
the Key Discipline Project of Renji hospital, Shanghai Jiaotong
University School of Medicine (RJ4101306).
References
|
1.
|
Gross SA, Zhu X, Bao L, et al: A
prospective study of 728 cases of non-Hodgkin lymphoma from a
single laboratory in Shanghai, China. Int J Hematol. 88:165–173.
2008. View Article : Google Scholar : PubMed/NCBI
|
|
2.
|
Wang J, Young L, Win W and Taylor CR:
Distribution and ZAP-70 expression of WHO lymphoma categories in
Shanxi, China: a review of 447 cases using a tissue microarray
technique. Appl Immunohistochem Mol Morphol. 13:323–332. 2005.
View Article : Google Scholar : PubMed/NCBI
|
|
3.
|
Lossos IS: Molecular pathogenesis of
diffuse large B-cell lymphoma. J Clin Oncol. 23:6351–6357. 2005.
View Article : Google Scholar : PubMed/NCBI
|
|
4.
|
Gordon LI, Harrington D, Andersen J, et
al: Comparison of a second-generation combination chemotherapeutic
regimen (m-BACOD) with a standard regimen (CHOP) for advanced
diffuse non-Hodgkin’s lymphoma. N Engl J Med. 327:1342–1349.
1992.PubMed/NCBI
|
|
5.
|
Fisher RI, Gaynor ER, Dahlberg S, et al:
Comparison of a standard regimen (CHOP) with three intensive
chemotherapy regimens for advanced non-Hodgkin’s lymphoma. N Engl J
Med. 328:1002–1006. 1993.PubMed/NCBI
|
|
6.
|
Feugier P, Van Hoof A, Sebban C, et al:
Long-term results of the R-CHOP study in the treatment of elderly
patients with diffuse large B-cell lymphoma: a study by the Groupe
d’Etude des Lymphomes de l’Adulte. J Clin Oncol. 23:4117–4126.
2005.PubMed/NCBI
|
|
7.
|
Pfreundschuh M, Trümper L, Osterborg A, et
al: CHOP-like chemotherapy plus rituximab versus CHOP-like
chemotherapy alone in young patients with good-prognosis diffuse
large-B-cell lymphoma: a randomised controlled trial by the
MabThera International Trial (MInT) Group. Lancet Oncol. 7:379–391.
2006. View Article : Google Scholar
|
|
8.
|
The International Non-Hodgkin’s Lymphoma
Prognostic Factors Project: A predictive model for aggressive
non-Hodgkin’s lymphoma. N Engl J Med. 329:987–994. 1993.
|
|
9.
|
Shipp MA: Prognostic factors in aggressive
non-Hodgkin’s lymphoma: who has ‘high-risk’ disease? Blood.
83:1165–1173. 1994.
|
|
10.
|
Sehn LH, Berry B, Chhanabhai M, et al: The
revised International Prognostic Index (R-IPI) is a better
predictor of outcome than the standard IPI for patients with
diffuse large B-cell lymphoma treated with R-CHOP. Blood.
109:1857–1861. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
11.
|
Cheson BD, Horning SJ, Coiffier B, et al:
Report of an international workshop to standardize response
criteria for non-Hodgkin’s lymphomas. NCI Sponsored International
Working Group. J Clin Oncol. 17:12441999.PubMed/NCBI
|
|
12.
|
Broyde A, Boycov O, Strenov Y, Okon E,
Shpilberg O and Bairey O: Role and prognostic significance of the
Ki-67 index in non-Hodgkin’s lymphoma. Am J Hematol. 84:338–343.
2009.
|
|
13.
|
Lossos IS and Morgensztern D: Prognostic
biomarkers in diffuse large B-cell lymphoma. J Clin Oncol.
24:995–1007. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
14.
|
Nyman H, Jerkeman M, Karjalainen-Lindsberg
ML, Banham H, Enblad G and Leppä S: Bcl-2 but not FOXP1, is an
adverse risk factor in immunochemotherapy-treated non-germinal
center diffuse large B-cell lymphomas. Eur J Haematol. 82:364–372.
2009. View Article : Google Scholar : PubMed/NCBI
|
|
15.
|
Alacacioglu I, Ozcan MA, Ozkal S, et al:
Prognostic significance of immunohistochemical classification of
diffuse large B-cell lymphoma. Hematology. 14:84–89. 2009.
View Article : Google Scholar : PubMed/NCBI
|
|
16.
|
Ennishi D, Takeuchi K, Yokoyama M, et al:
CD5 expression is potentially predictive of poor outcome among
biomarkers in patients with diffuse large B-cell lymphoma receiving
rituximab plus CHOP therapy. Ann Oncol. 19:1921–1926. 2008.
View Article : Google Scholar : PubMed/NCBI
|
|
17.
|
Bari A, Marcheselli L, Sacchi S, et al:
Prognostic models for diffuse large B-cell lymphoma in the
rituximab era: a never-ending story. Ann Oncol. 21:1486–1491. 2010.
View Article : Google Scholar : PubMed/NCBI
|
|
18.
|
Vitolo U, Chiappella A, Angelucci E, et
al: Dose-dense and high-dose chemotherapy plus rituximab with
autologous stem cell transplantation for primary treatment of
diffuse large B-cell lymphoma with a poor prognosis: a phase II
multicenter study. Haematologica. 94:1250–1258. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
19.
|
Ziepert M, Hasenclever D, Kuhnt E, et al:
Standard International prognostic index remains a valid predictor
of outcome for patients with aggressive CD20+ B-cell
lymphoma in the rituximab era. J Clin Oncol. 28:2373–2380. 2010.
View Article : Google Scholar : PubMed/NCBI
|
|
20.
|
Pfreundschuh M, Schubert J, Ziepert M, et
al: Six versus eight cycles of bi-weekly CHOP-14 with or without
rituximab in elderly patients with aggressive CD20+
B-cell lymphomas: a randomised controlled trial (RICOVER-60).
Lancet Oncol. 9:105–116. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
21.
|
Glass B, Kloess M, Bentz M, et al:
Dose-escalated CHOP plus etoposide (MegaCHOEP) followed by repeated
stem cell transplantation for primary treatment of aggressive
high-risk non-Hodgkin lymphoma. Blood. 107:3058–3064. 2006.
View Article : Google Scholar : PubMed/NCBI
|
|
22.
|
Tay K, Tai D, Tao M, Quek R, Ha TC and Lim
ST: Relevance of the International Prognostic Index in the
rituximab era. J Clin Oncol. 29:e142011. View Article : Google Scholar : PubMed/NCBI
|
|
23.
|
Advani RH, Chen H, Habermann TM, et al:
Comparison of conventional prognostic indices in patients older
than 60 years with diffuse large B-cell lymphoma treated with
R-CHOP in the US Intergroup Study (ECOG 4494, CALGB 9793):
consideration of age greater than 70 years in an elderly prognostic
index (E-IPI). Br J Haematol. 151:143–151. 2010.
|