Introduction
The American Academy of Pediatrics (1) and the World Health Organization (WHO)
(2) recommend exclusive
breast-feeding for infants until the age of 6 months. A US national
survey conducted in 2001 reported that 33% of infants were
breast-fed and 17% were exclusively breast-fed until 6 months of
age (3). Breast-feeding is the
ideal feeding mode for both infants and mothers. Breast-feeding has
beneficial effects in infants and mothers, and it plays a crucial
role in public health (1). Human
milk is species-specific and contains optimal nutrients, growth
factors and the immunological components required for infants
(4). Breast-feeding has short-term
benefits such as the prevention of infectious diseases in infants,
including diarrhea (5–8), respiratory tract infection (9–12)
and otitis media (13,14). The long-term health benefits of
breast-feeding in infants include a lower risk of developing
diseases such as obesity (15,16),
hypertension (17,18) and type 1 diabetes mellitus
(19,20) in adulthood. Gluckman and Hanson
(21) proposed the concept of
developmental origins of health and disease, which states that
unbalanced nutrition in utero and in infancy leads to subsequent
disorders.
Body weight is an important index of infant growth
and development. Neonates lose weight because of the physiologic
extracellular fluid diuresis following their transition from
intrauterine to extrauterine life (22). The normal maximal weight loss is
5.5–6.6% of birth weight in optimally exclusively breast-fed
infants and occurs between the second and third day of life
(23,24). According to the WHO Multicentre
Growth Reference Study, a male infant gains 1,200 g/month and a
female infant gains 1,000 g/month under optimal conditions. Weight
gain in the first month of life in exclusively breast-fed infants
is reported to be 18–35 g (25,26).
Although studies indicate sufficient evidence regarding
breast-feeding, there is no universal agreement among healthcare
providers regarding weight gain in breast-fed and formula-fed
infants. When weight gain occurs gradually, appropriate support
should be provided after determining whether the infant is
demonstrating delayed weight gain or a failure to thrive (27–29).
This retrospective study aimed to clarify whether
differences in feeding modes influence neonatal weight gain in the
first month of life.
Materials and methods
Study population
This retrospective study involved the review of
pregnancy charts of 422 women who delivered at a birthing center in
Aomori Prefecture, Japan. The study complied with the principles of
the Declaration of Helsinki (Seoul 2008) and the ethical guidelines
for epidemiological research issued by the Ministry of Education,
Culture, Sports, Science and Technology as well as the Ministry of
Health, Labour and Welfare in Japan (2008). All study data were
obtained from the medical records of the subjects and were coded to
avoid disclosure of the their identity. We gathered the medical
records of 579 women who had a singleton pregnancy and delivered a
live infant from August 1998 to September 2007. The inclusion
criteria were low-risk, full-term pregnancy (duration, 37–42
weeks), spontaneous vaginal delivery, <500 ml intrapartum blood
loss and a healthy infant (1 min Apgar score of ≥8) who underwent a
health check-up at 1 month postpartum. Mothers with chronic
diseases (e.g., diabetes, hypertension and hyperthyroidism),
gestational diabetes, and pregnancy-induced hypertension were
excluded from the study. Records with unknown or missing obstetric
data were not included. A total of 422 records were finally
available for analysis.
Perinatal parameters
The perinatal parameters extracted from the
pregnancy charts were maternal age, parity, smoking status,
self-reported prepregnancy weight, prepregnancy body mass index
(BMI), gestational weight gain, chronic diseases, delivery mode,
duration of pregnancy, infant gender, infant size at birth (weight,
height, head circumference and chest circumference), 1 min Apgar
score, admission to hospital, and data from the first month health
check-up (mother’s weight, feeding mode and infant size).
Feeding modes
Subjects were divided into three groups on the basis
of self-reported feeding mode used by mothers in the first
postpartum month: an exclusive breast-feeding group, a
mixed-feeding (breast-feeding and formula-feeding) group, and an
exclusive formula-feeding group.
Statistical analysis
Statistical analysis was performed using SPSS
software, version 16.0 (SPSS Japan, Inc., Tokyo, Japan) for
Windows. Descriptive statistics are indicated as arithmetic mean ±
standard deviation. A two-sample t-test, one-way analysis of
variance, and Tukey’s honestly significant difference test were
performed to determine differences across the three groups. The
χ2 statistic was used to analyze categorical variables.
Univariate analysis was performed using Pearson’s correlation
coefficient. A P-value of <0.05 was determined to be indicative
of a statistically significant result.
Results
Summary of the study population
The maternal parameters of the study population are
summarized in Table I. The mean
maternal age was 26.6±4.5 years (range, 17–38 years); 38.6%
subjects were primiparas and 17.8% were smokers. The mean duration
of pregnancy was 39.5±1.2 weeks. The infant parameters of the study
population are summarized in Table
II. The mean infant birth weight and height were 3,209±370.4 g
and 49.6±1.8 cm, respectively; 49.8% infants were male. The mean
infant weight and height at 1 month were 4,513.2±451 g and 54.9±1.6
cm, respectively; the mean total weight gain was 1,303.5±325.0 kg,
and the weight gain/day was 39.5±9.4 g. The study population was
classified into the following three groups on the basis of the
feeding mode: breast-feeding (28.9%), mixed-feeding (55.9%) and
formula-feeding (15.2%) groups. The overall maternal smoking rate
was 17.8%, the smoking rates for the exclusive breast-feeding,
mixed feeding, and exclusive formula-feeding groups were 7.4, 20.3
and 28.1%, respectively. The smoking rate was significantly lower
in the exclusive breast-feeding group than in the other groups.
Except for maternal smoking status, none of the other maternal and
infant parameters significantly differed among the three feeding
modes.
 | Table ISummary and comparison of maternal
parameters classified on the basis of feeding modes. |
Table I
Summary and comparison of maternal
parameters classified on the basis of feeding modes.
| | Feeding mode group
|
|---|
| Parameters | Total population
(n=422) | Breast-fed
(n=122) | Mixed-fed
(n=236) | Formula-fed
(n=64) |
|---|
| Age (years)a | 26.6±4.5 | 26.8±4.0 | 26.6±4.7 | 26.3±4.9 |
| Duration of pregnancy
(weeks)a | 39.5±1.2 | 39.5±1.1 | 39.6±1.2 | 39.2±1.1b |
| Primiparousc | 163 (38.6) | 44 (36.1) | 96 (40.7) | 23 (35.9) |
| Smokersc | 75 (17.8) | 9 (7.4) | 48 (20.3) | 18 (28.1)d |
| Prepregnancy weight
(kg)a | 53.3±8.4 | 52.4±6.8 | 53.7±9.3 | 54.0±7.5 |
| Prepregnancy
BMIa | 21.2±3.2 | 20.8±2.4 | 21.4±3.5 | 21.4±3.1 |
| Delivery weight | 65.2±8.7 | 64.2±7.4 | 65.7±9.2 | 65.3±8.9 |
| Gestational weight
gain (kg)a | 11.8±4.0 | 11.7±3.4 | 12.0±4.3 | 11.3±3.9 |
| Weight at 1 month
postpartum (kg)a | 57.9±8.3 | 57.0±7.2 | 58.4±8.9 | 57.6±8.1 |
| Postpartum weight
loss (kg)a | 7.3±2.3 | 7.2±2.1 | 7.3±2.3 | 7.7±2.6 |
| Table IISummary and comparison of infant
parameters classified on the basis of feeding modes. |
Table II
Summary and comparison of infant
parameters classified on the basis of feeding modes.
| | Feeding modes group
|
|---|
| Parameters | Total population
(n=422) | Breast-fed
(n=122) | Mixed-fed
(n=236) | Formula-fed
(n=64) |
|---|
| Malea | 210 (49.8) | 52 (42.6) | 126 (53.4) | 32 (50.0) |
| 1 min Apgar
scoreb | 9.8±0.4 | 9.8±0.4 | 9.8±0.4 | 9.7±0.5 |
| Birth | | | | |
| Weight (g)b | 3,209.0±370.4 | 3,203.6±319.6 | 3,222.3±402.5 | 3,170.6±337.6 |
| Height (cm)b | 49.6±1.8 | 49.6±1.6 | 49.7±2.0 | 49.5±1.7 |
| Head circumference
(cm)b | 33.4±1.3 | 33.3±1.3 | 33.5±1.3 | 33.3±1.2 |
| Chest circumference
(cm)b | 31.7±1.6 | 31.6±1.5 | 31.8±1.6 | 31.3±1.7 |
| At 1 month of
life | | | | |
| Weight (g)b | 4,513.2±451.8 | 4,504.2±447.8 | 4,525.3±470.3 | 4,485.5±390.4 |
| Height (cm)b | 54.9±1.6 | 54.8±1.5 | 55.0±1.8 | 54.8±1.3 |
| Head circumference
(cm)b | 37.1±1.1 | 37.2±1.0 | 37.2±1.1 | 37.4±1.4 |
| Chest
circumference (cm)b | 37.1±1.4 | 37.1±1.3 | 37.0±1.4 | 37.1±1.2 |
Relationship between weight gain and
maternal/neonatal parameters
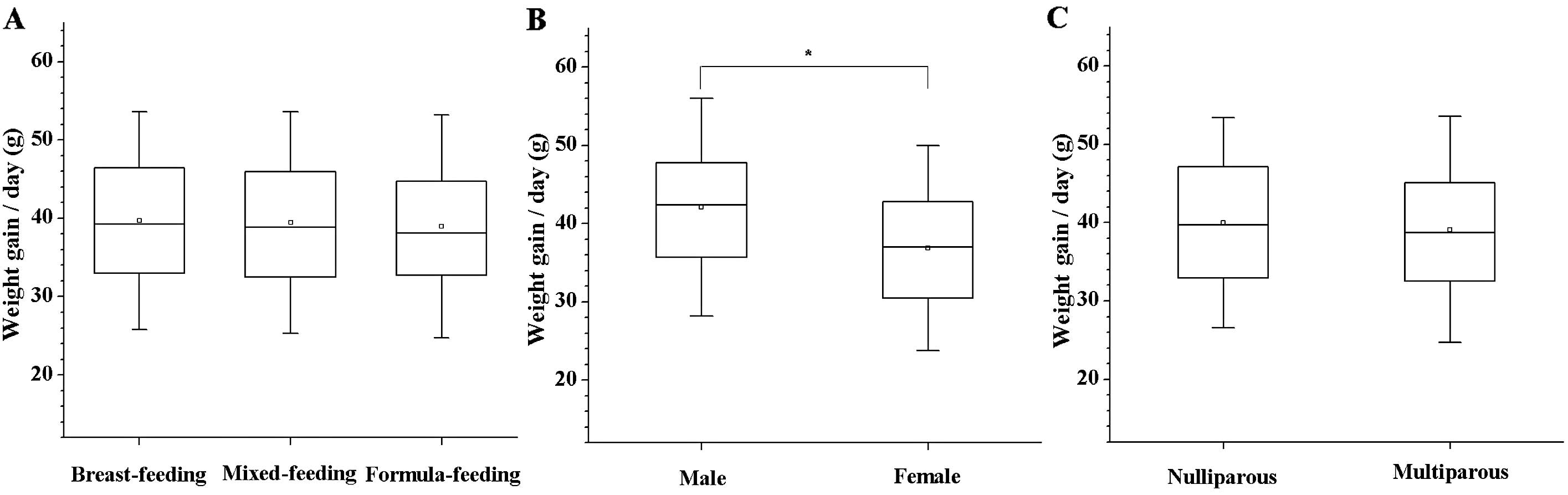
Infant weight gain/day in the first month of life
was determined for feeding modes, parity and infant gender
(Fig. 1). The daily weight gain
was 39.7±9.3 g (range, 18.5–67.4 g) in the exclusive breast-feeding
group, 39.5±9.4 g (range, 13.8–64.5 g) in the mixed-feeding group,
and 39.0±9.5 g (range, 14.4–65.3 g) in the exclusive
formula-feeding group. No significant differences in daily weight
gain were observed among the feeding modes (Fig. 1A). The daily infant weight gain was
significantly higher in the male infants (42.1±9.3 g) than in the
female infants (36.9±8.8 g) (Fig.
1B), but did not differ between primiparous and multiparous
mothers (Fig. 1C).
Multiple linear regression analysis was used to
identify independent variables associated with infant weight gain
(Table III). Although the
coefficient of determination (R2) was low, infant
gender, birth weight, birth height, and maternal age were
identified as variables that could independently predict the weight
gain/day in the first month of life (R2= 0.13,
P<0.001 by ANOVA).
| Table IIIMultiple linear regression analysis
for the association between infant weight gain/day and
maternal/infant parameters. |
Table III
Multiple linear regression analysis
for the association between infant weight gain/day and
maternal/infant parameters.
| Explanatory
variable | Standardized
partial regression coefficient (β) |
|---|
| Infant gender | −0.276a |
| Birth weight | −0.378a |
| Birth height | 0.255b |
| Maternal age | −0.119c |
Discussion
In Japan, breast-feeding has been promoted since
1989 according to a joint announcement ‘The Ten Steps to Successful
Breastfeeding’ released by WHO/UNICEF. According to a national
Japanese study in 2005, 42.4% infants aged 1 month, 38.0% aged 3
months, and 34.7% aged 6 months were exclusively breast-fed
(30). However, in our
retrospective study, 28.9% infants were exclusively breast-fed at 1
month after birth, indicating that the values in our study in Japan
were below the national average. The results obtained in the
present study were possibly affected by regional characteristics,
different attitudes, and/or lack of education on breast-feeding.
Moreover, relatively higher birth weights of both male (3,235 g)
and female (3,183 g) infants were observed in our study when
compared with the average birth weight in Japan (male infants,
3,040 g; female infants, 2,960 g) (31). This finding may be attributed to
the low-risk pregnancies, young maternal age, and high rate of
multiparity and full-term deliveries in our study. Except for the
rate of maternal smoking, which was lower in the exclusive
breast-feeding group than in other groups, none of the other
maternal and infant parameters assessed in this study significantly
differed among the three groups.
According to the WHO Multicenter Growth Reference
Study, a male infant gains 1,200 g/month and a female infant gains
1,000 g/month under optimal conditions (25). In the current study, the male
infants gained 1,391.1±328.4 g/month (42 g/day) and the female
infants gained 1,216.7±297.7 g/month (36.9 g/day). WHO (32) and Dewey (33) reported that male infants gain
significantly more weight than female infants. Breast-fed infants
weighed significantly less than formula-fed infants at ages 3
months to 2 years; however, no significant differences in weight
were observed at age 2–3 months (34–36).
The weight gained in the first month after birth did not differ
with the feeding modes; this finding was consistent with that of a
previous study (24). Exclusively
breast-fed infants may gradually gain weight in the first month of
life. However, delayed weight gain cannot be disregarded as it may
be associated with less than optimal breast-feeding or illness in
the infant (e.g., congenital heart disease, neuromuscular disease,
infection, or endocrine and metabolic abnormalities). Therefore,
infant weight gain assessments must take into account potential
illnesses in addition to maternal health, the condition of breast
milk, and infant position and latching during breast-feeding.
Furthermore, some infants gain less than 20 g/day regardless of the
feeding mode. Factors affecting the mother’s and infant’s health
after childbirth include abuse, parenting anxiety, and postpartum
depression; therefore, the mother’s physical and mental state
should be assessed along with the infant’s condition. Continuous
support provided to the mother and infant soon after discharge from
the hospital is related with improved health of both the mother and
her infant.
The present study revealed that weight gain in the
first month of life does not significantly differ between
exclusively breast-fed infants and exclusively formula-fed infants
(Fig. 1). Poor weight gain in
infants is not only caused by poor milk intake due to incorrect
suckling or insufficient lactation but may also be associated with
illness in the infant. Breast-feeding improves the health and
development of both the mother and infant. Therefore, assessment of
feeding soon after birth is crucial with regard to infant growth
and development and prevention of diseases in adulthood. Healthcare
providers working with mothers and infants should understand the
patterns of growth and development of exclusively breast-fed
infants, correctly assess the effectiveness of breast-feeding, and
provide continuous support so that both the mother and infant
benefit from breast-feeding.
Acknowledgements
We are indebted to the midwives of
Fukushi Birth Center for collecting the pregnancy charts. This
study was supported by a Grant for Hirosaki University
Institutional Research (2011).
References
|
1
|
American Academy of Pediatrics:
Breastfeeding and the use of human milk. Pediatrics. 115:196–506.
2005.
|
|
2
|
WHO: Global Strategy for Infant and Young
Child Feeding 55th World Health Assembly. World Health
Organization; Geneva: 2002
|
|
3
|
Ryan AS, Wenjun Z and Acosta A:
Breastfeeding continues to increase into the new millennium.
Pediatrics. 110:1103–1109. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Prentice A: Constituents of human milk.
Food and Nutrition Bulletin. United Nations University Press; pp.
171996, http://archive.unu.edu/unupress/food/8F174e/8F174E04.htmuri.
Accessed December 27, 2011.
|
|
5
|
Howie PW, Forsyth JS, Ogston SA, Clark A
and Florey CD: Protective effect of breast feeding against
infection. BMJ. 300:11–16. 1990. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Clemens J, Rao M, Ahmed F, et al:
Breast-feeding and the risk of life-threatening rotavirus diarrhea:
prevention or postponement? Pediatrics. 92:680–685. 1993.PubMed/NCBI
|
|
7
|
Lopez-Alarcon M, Villalpando S and Fajardo
A: Breast-feeding lowers the frequency and duration of acute
respiratory infection and diarrhea in infants under six months of
age. J Nutr. 127:436–443. 1997.PubMed/NCBI
|
|
8
|
Bhandari N, Bahl R, Mazumdar S, Martines
J, Black RE and Bhan MK; Infant Feeding Study Group: Effect of
community-based promotion of exclusive breastfeeding on diarrhoeal
illness and growth: a cluster randomized controlled trial. Lancet.
361:1418–1423. 2003. View Article : Google Scholar
|
|
9
|
Blaymore Bier J, Oliver T, Ferguson A and
Vohr BR: Human milk reduces outpatient upper respiratory symptoms
in premature infants during their first year of life. J Perinatol.
22:354–359. 2002.PubMed/NCBI
|
|
10
|
Bachrach VR, Schwarz E and Bachrach LR:
Breastfeeding and the risk of hospitalization for respiratory
disease in infancy: a meta-analysis. Arch Pediatr Adolesc Med.
157:237–243. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Chantry CJ, Howard CR and Auinger P: Full
breastfeeding duration and associated decrease in respiratory tract
infection in US children. Pediatrics. 117:425–432. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Wright AL, Holberg CJ, Martinez FD, Morgan
WJ and Taussig LM: Breast feeding and lower respiratory tract
illness in the first year of life. Group Health Medical Associates.
BMJ. 299:946–949. 1989.PubMed/NCBI
|
|
13
|
Owen MJ, Baldwin CD, Swank PR, Pannu AK,
Johnson DL and Howie VM: Relation of infant feeding practices,
cigarette smoke exposure, and group child care to the onset and
duration of otitis media with effusion in the first two years of
life. J Pediatr. 123:702–711. 1993.PubMed/NCBI
|
|
14
|
Aniansson G, Alm B, Andersson B, et al: A
prospective cohort study on breast-feeding and otitis media in
Swedish infants. Pediatr Infect Dis J. 13:183–188. 1994. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Von Kries R, Koletzko B, Sauerwald T, et
al: Breast feeding and obesity: cross sectional study. BMJ.
319:147–150. 1999.PubMed/NCBI
|
|
16
|
Owen CG, Martin RM, Whincup PH, Smith GD
and Cook DG: Effect of infant feeding on the risk of obesity across
the life course: a quantitative review of published evidence.
Pediatrics. 115:1367–1377. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Singhal A, Cole TJ and Lucas A: Early
nutrition in preterm infants and later blood pressure: two cohorts
after randomised trials. Lancet. 357:413–419. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Horta BL, Bahl R, Martinés JC and Victora
CG: Evidence on the long-term effects of breastfeeding: Systematic
reviews and meta-analysis. World Health Organization; Geneve: pp.
522007
|
|
19
|
Virtanen SM, Räsänen L, Aro A, et al:
Infant feeding in Finnish children less than 7 yr of age with newly
diagnosed IDDM. Childhood Diabetes in Finland Study Group. Diabetes
Care. 14:415–417. 1991. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Gerstein HC: Cow’s milk exposure and type
I diabetes mellitus. A critical overview of the clinical
literature. Diabetes Care. 17:13–19. 1994.
|
|
21
|
Gluckman P and Hanson M: The conceptual
basis for the developmental origins of health and disease.
Developmental Origins of Health and Disease. Cambridge University
Press; Camdridge: pp. 33–50. 2006, View Article : Google Scholar
|
|
22
|
Cunningham FG, Leveno KJ, Bloom SL, et al:
The newborn infant. Williams Obstetrics. Cunningham FG, Leveno KJ
and Bloom S: 23rd edition. McGraw-Hill; New York: pp. 590–604.
2010
|
|
23
|
Rodríguez G, Ventura P, Samper MP, Moreno
L, Sarría A and Pérez-González JM: Changes in body composition
during the initial hours of life in breast-fed healthy term
newborns. Biol Neonate. 77:12–16. 2000.PubMed/NCBI
|
|
24
|
MacDonald PD, Ross SR, Grant L and Young
D: Neonatal weight loss in breast and formula fed infants. Arch Dis
Child Fetal Neonatal Ed. 88:F472–F476. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
WHO: Evidence for the ten steps to
successful breastfeeding. World Health Organization; Geneva:
1999
|
|
26
|
UNICEF-World Health Organization:
Breastfeeding Management and Promotion in a Baby-Friendly Hospital:
an 18-hour course for maternity staff. UNICEF; New York: 1993
|
|
27
|
Mohrbancher N and Stock JMA: The
Breastfeeding Answer Book. La Leche League International; Illinois:
pp. 147–178. 2003
|
|
28
|
Lawrence RA and Lawrence RM:
Breastfeeding; A Guide for the Medical Profession. Mosby; St.
Louis: pp. 427–460. 2005
|
|
29
|
Regina E and Giugliani J: Slow weight gain
and failure to thrive. Core Curriculum for Lactation Consultant
Practice. 2nd edition. Mannel R, Martens P and Walker M: Jones and
Bartlett Publishers; Boston: pp. 727–740. 2007
|
|
30
|
Ministry of Health, Labour and Welfare
(http://www.mhlw.go.jp/) Japan: Summary of the results of a
nutrition survey in infants in FY2005, Breast-feeding division
(updated 2006 Jun 29). Available at http://www.mhlw.go.jp/shingi/2007/03/dl/s0314-17b-1.pdfuri
(In Japanese). Accessed December 27, 2011.
|
|
31
|
Health, Labour and Welfare Statistics
Association. Journal of Health and Welfare Statistics.
58:482011.(In Japanese).
|
|
32
|
World Health Organization: The WHO
Multicentre Growth Reference Study. http://www.who.int/childgrowth/mgrs/en/uri.
Accessed December 27, 2011.
|
|
33
|
Dewey KG: Nutrition, growth, and
complementary feeding of the breastfed infant. Pediatr Clin North
Am. 48:87–104. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
34
|
Dewey KG, Heinig MJ, Nommsen LA, Peerson
JM and Lönnerdal B: Growth of breast-fed and formula-fed infants
from 0 to 18 months: the DARLING Study. Pediatrics. 89:1035–1041.
1992.PubMed/NCBI
|
|
35
|
Kramer MS, Guo T, Platt RW, Vanilovich I,
et al: The promotion of breastfeeding intervention trials study
group. Feeding effects on growth during infancy. J Pediatr.
145:600–605. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
36
|
Dewey KG: Infant feeding and growth. Adv
Exp Med Biol. 639:57–66. 2009. View Article : Google Scholar
|