Introduction
High intensity focused ultrasound (HIFU) has been
investigated for its therapeutic application in selectively
destroying deep-seated tissues in the body without damage to
overlying tissues. HIFU is based on the same principles as
conventional ultrasound. HIFU propagates harmlessly through living
tissue, but if the ultrasound beam carries sufficient energy and is
brought into a tight focus, the energy in the focal volume causes a
local temperature rise that is sufficient to lead to tissue
necrosis while not damaging surrounding tissues. HIFU was initially
investigated for its potential to selectively destroy tissue
volumes in the brain, in neurobehavioral studies (1). Early clinical research in the 1960s
focused on the use of HIFU for the treatment of neurological
diseases (2). During the 1970s and
1980s, the specific properties of focused ultrasound conduction and
modes of destruction in normal tissues were investigated further
and studies using HIFU to ablate experimental tumors followed
(3). During the 1990s, animal
experiments and a number of clinical trials were performed which
fine-tuned the requirements of focusing, intensity and exposure
time in order to maximize tumor ablation effectiveness (4). The results of these experiments
indicated that HIFU selectively produced target lesions in tumor
tissues and parenchymatous organs (5,6). In
several centers worldwide, HIFU is now being used clinically to
treat solid tumors, including those of the uterus, liver, kidney,
prostate, breast, pancreas, bone and soft tissue (7). In China, there were more than 3000
patients who were treated with HIFU (8) and the clinical results indicate that
HIFU treatment is a safe, effective and feasible non-invasive
therapeutic modality for the ablation of solid tumors.
Certain studies have examined the histological and
ultrasonic changes associated with HIFU ablation in the liver,
kidney, prostate and breast (9).
Although numerous previous studies have involved ablations in
regenerative tissues such as the liver and kidney, few studies
involved non-regenerative tissues such as muscle (10). This study aimed to examine the
development of the ultrasonic image of rabbit leg muscle irradiated
by HIFU. The results provide a basis for understanding ultrasound
effects for clinical applications such as uterine fibroids and soft
tissue tumors.
Materials and methods
Animals
Twenty New Zealand white rabbits weighing 1.5–2.0
kg, were supplied by the Laboratory Animals Center of Shanghai
JiaoTong University Affiliated Sixth People’s Hospital (Shanghai,
China). The experiment was approved by an Ethics committee from and
scientifically by the hospital and complied with Practice for
Laboratory Animals in China.
HIFU treatment system
HY2900 HIFU tumor therapy system (Wuxi Haiying
Techonology, Wuxi, China) was used in this study. This device,
which was designed and manufactured for clinical tumor treatment,
comprised an ultrasonic diagnostic unit under the control of a
central processing unit. The therapeutic transducer, a self-focused
6 element transducer with a diameter of 25 cm and a focal length of
140 mm, was fixed on the top of a water capsule filled with
degassed water. A diagnostic transducer was localized in the center
of the therapeutic transducer. The frequency of the diagnostic
transducer was 3.5 MHz. Thus, the tissues in the path of
therapeutic ultrasound waves could be viewed in diagnostic
ultrasonic images. Ultrasonography was used to guide HIFU radiation
and monitor therapeutic effects in real-time. The maximum
electrical power from the amplifier was 1.02 kW. The spatially
averaged intensity level (ISAL) at −6 dB was 9366 W/cm2
based on radiation force measurements and acoustic field mapping,
while producing a maximum acoustic power of 479.2 W. The water bag
has an acoustic transparent membrane surface for HIFU to transmit
without obstruction and ultrasound coupling gel was applied to
eliminate air pockets trapped between the membrane and the rabbit
skin. The frequency of the therapeutic ultrasound wave was 1.5 MHz.
The focal region of the therapeutic transducers was an ellipsoid
with dimensions of 8 mm along the beam axis and 1.15 mm in the
transverse direction, calibrated by a PVDF needle hydrophone with
spot diameter of 0.5 mm in a tank filled with degassed water.
The follow-up equipment
The follow-up ultrasound machine was EASOTE MPX
(Esaote SPA, Genua, Italy). The frequency of the transducer was
12.6 MHz.
Muscle tissue ablation
The dorsum of the rabbits was shaved and a
depilating agent was applied to remove remaining hair one day prior
to HIFU radiation. The animals were anesthetized 10 min before HIFU
radiation. Pentobarbital sodium (3%; 25 mg/kg) was injected from
auricular veins following anesthesia, animals were positioned to
the left or right laterally to ensure the target muscles were
viewed clearly with ultrasonography. The skin of the rabbit leg was
defatted with 75% alcohol. Ultrasound coupling gel was applied to
the surface of the skin to create tight contact with the water
capsule.
According to the ultrasound images, the HIFU
radiation plane was determined. To avoid bone, vascular and
connective tissues as much as possible, the hypoechoic muscles were
selected as target tissues. The HIFU radiation depth was 15 mm. The
irradiated region was round with a diameter of 10 mm. The
electrical output power of the HIFU radiation was 0.47 kW. The HIFU
radiation time of each pulse (Ton) was 500 ms. The
interval time between two pulses (Toff) was 10 sec. The
interval distance between two points was 1 mm. The echo changes
were monitored by ultrasound.
Ultrasonic examination
The muscles of 38 legs of 19 rabbits were detected 1
day before HIFU radiation and from 10 min to 28 days after HIFU
radiation with a high-frequency transducer. The ultrasound
examinations included two-dimensional ultrasound, color Doppler and
power Doppler. There was only one coagulation necrosis lesion in
the muscle of each leg. The length (L), width (W) and depth (D) of
the coagulation necrosis lesions were measured. This procedure was
repeated 3 times. The volume of coagulation necrosis lesions was
calculated using the formula: [V = (π/6) × L × W × D]. The echo and
blood flow changes in and around the coagulation necrosis lesion
were detected. Examination was performed under the same conditions
each time.
Pathology
One and 19 rabbits were anatomized on Day 1 and Day
28, respectively, after HIFU radiation. Damage to the skin and
subcutaneous tissues was inspected and the color and hardness of
the coagulation necrosis lesions were recorded. The tissues were
processed using standard histopathological techniques and stained
with hematoxylin and eosin (H&E). The 19 rabbits were
sacrificed on Day 28 after HIFU radiation. The length (L), width
(W) and depth (D) of the coagulation necrosis lesions were measured
with a vernier caliper. This procedure was repeated 3 times. The
volume of coagulation necrosis lesions was calculated using the
formula: [V = (π/6) × L × W × D].
Statistical analysis
Data were processed using the statistical software
SPSS 12.0 (SPSS, Chicago, IL, USA). One-way ANOVA analysis was
used. P<0.05 was considered to indicate a statistically
significant result.
Results
Ultrasonic examination prior to HIFU
radiation
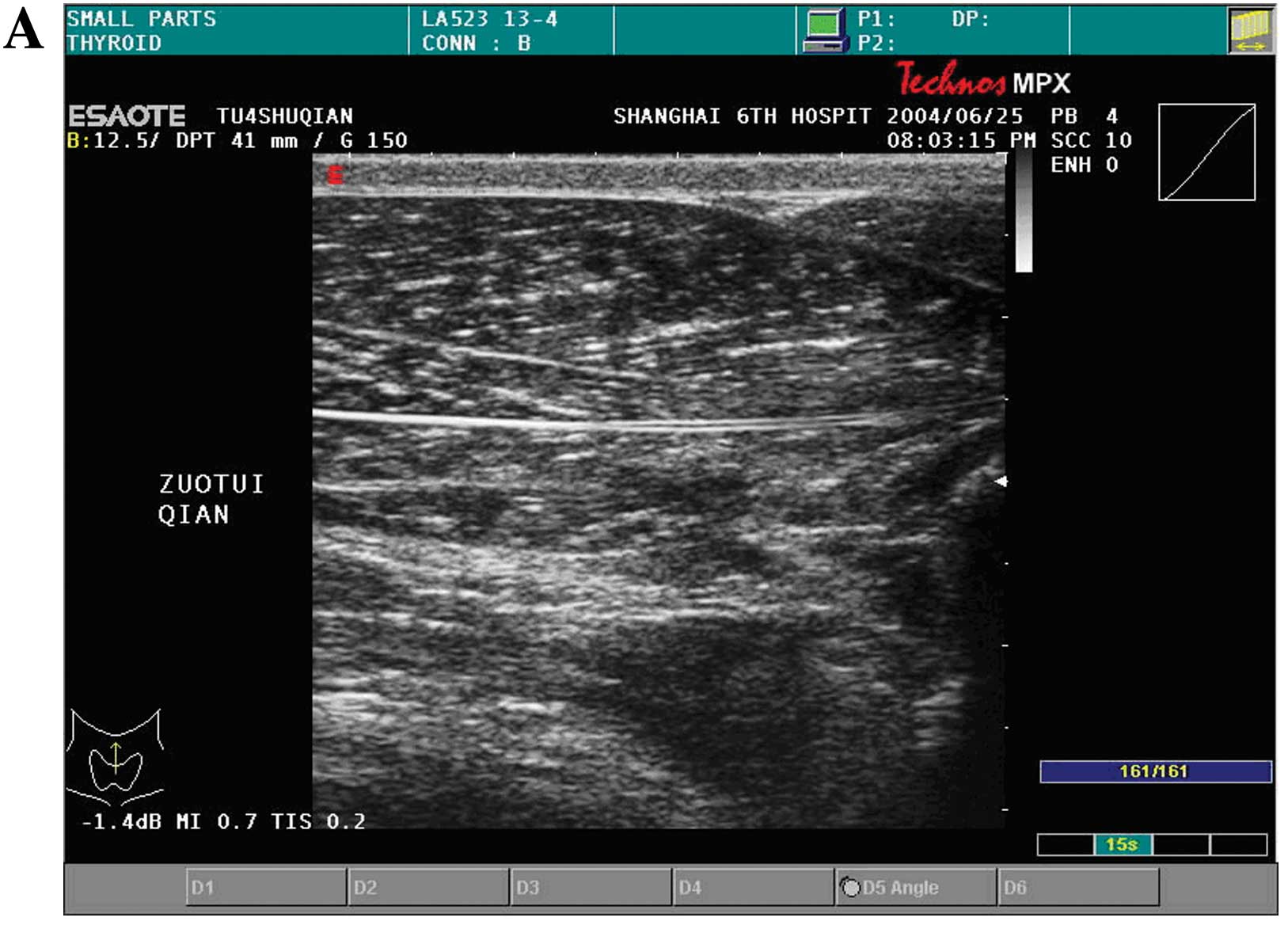
The muscles of 38 legs of 19 rabbits were detected 1
day prior to HIFU radiation and from 10 min to 28 days after HIFU
radiation with a high-frequency transducer. Two legs of l rabbit
were detected 1 day prior to HIFU radiation and from 10 min to 1
day The echo of leg muscles of 20 New Zealand white rabbits was
homogeneous and hypoechoic prior to HIFU radiation, as detected by
two-dimensional ultrasound (Fig.
1A).
Ultrasonic monitoring during HIFU
radiation
The muscle tissues prior to HIFU radiation were
hypoechoic. The echo of the irradiated region increased during HIFU
radiation. Although the echo of the irradiated region decreased
with time, the echo was also higher than that in normal muscle
tissue.
Ultrasonic image development
The echo of coagulation necrosis lesions was
hyperechoic at 10 min after HIFU radiation (Fig. 1B). The echo at the center of the
irradiated region became lower 1 h after HIFU radiation and there
was a distinct hyperechoic border zone around the coagulation
necrosis lesions (Fig. 1C). From
Day 1 to Day 3, the echo of coagulation necrosis lesions was higher
than that in normal muscle tissues. The hyperechoic zone
surrounding the coagulation necrosis lesions became shallower
(Fig. 1D and E). Although the echo
of coagul ation necrosis lesions decreased from Day 3 to Day 7
after HIFU radiation, it was higher thanthat in normal muscle
tissues. The hyperechoic zone surrounding the coagulation necrosis
lesions disappeared. By contrast, there was a hypoechoic border
zone whose width was 0.5–0.8 mm (Fig.
1F). From Day 14 to Day 28, the volume of coagulation necrosis
lesions decreased markedly. The hypoechoic zone disappeared. The
echo of coagulation necrosis lesions was homogeneous and
hypoechoic, and the border of the coagulation necrosis lesions
became unclear (Fig. 1G and
H).
Volume and diameters of coagulation
necrosis tissue
The length (L), width (W) and depth (D) of
coagulation necrosis lesions were measured by ultrasound at various
times, from 10 min to 28 days after HIFU radiation. On the Day 1
after HIFU radiation, the volume of coagulation necrosis lesions
was the greatest. From Day 3 to Day 21 after HIFU radiation, the
volume of coagulation necrosis lesions decreased gradually. On Day
28 after HIFU radiation, the volume was smallest. There was no
difference between the volumes measured by ultrasound and by
vernier caliper 28 days after HIFU radiation. Table I shows the volume and diameters of
coagulation necrosis lesions at various times.
 | Table IThe length, width, depth and volume of
coagulation necrosis lesions induced by ultrasound from 10 min to
28 days after HIFU radiation (n=38). |
Table I
The length, width, depth and volume of
coagulation necrosis lesions induced by ultrasound from 10 min to
28 days after HIFU radiation (n=38).
| Measuring time | L (mm) | W (mm) | D (mm) | V
(mm3) |
|---|
| 10 min later | 14.00±4.31 | 9.93±1.57 | 12.49±3.38 | 962.39±350.49 |
| 1 day later | 18.76±1.27 | 11.06±1.69 | 14.24±1.77 | 1476.59±308.64 |
| 3 days later | 22.33±2.79 | 9.97±1.90 | 11.76±2.29 | 1292.27±322.81 |
| 7 days later | 18.58±2.31 | 10.18±1.69 | 10.44±2.89 | 1021.93±368.86 |
| 14–21 days later | 13.08±0.81 | 8.83±0.78 | 10.47±1.06 | 612.47±127.98 |
| 21–28 days later | 9.03±0.51 | 8.77±0.47 | 8.59±0.43 | 343.29±54.79 |
| Macroscope | 8.50±0.78 | 8.11±0.78 | 8.33±0.78 | 274.12±78.69 |
Pathology results
The hair of the rabbit leg was removed and the skin
was smooth prior to HIFU irradiation. There was no skin burn
following HIFU radiation. Intervening tissue, such as the skin,
fatty tissues and muscles between the transducer and the HIFU
lesions showed no histological evidence of damage. In addition, the
HIFU lesions were observed as discrete, with sharp differentiation
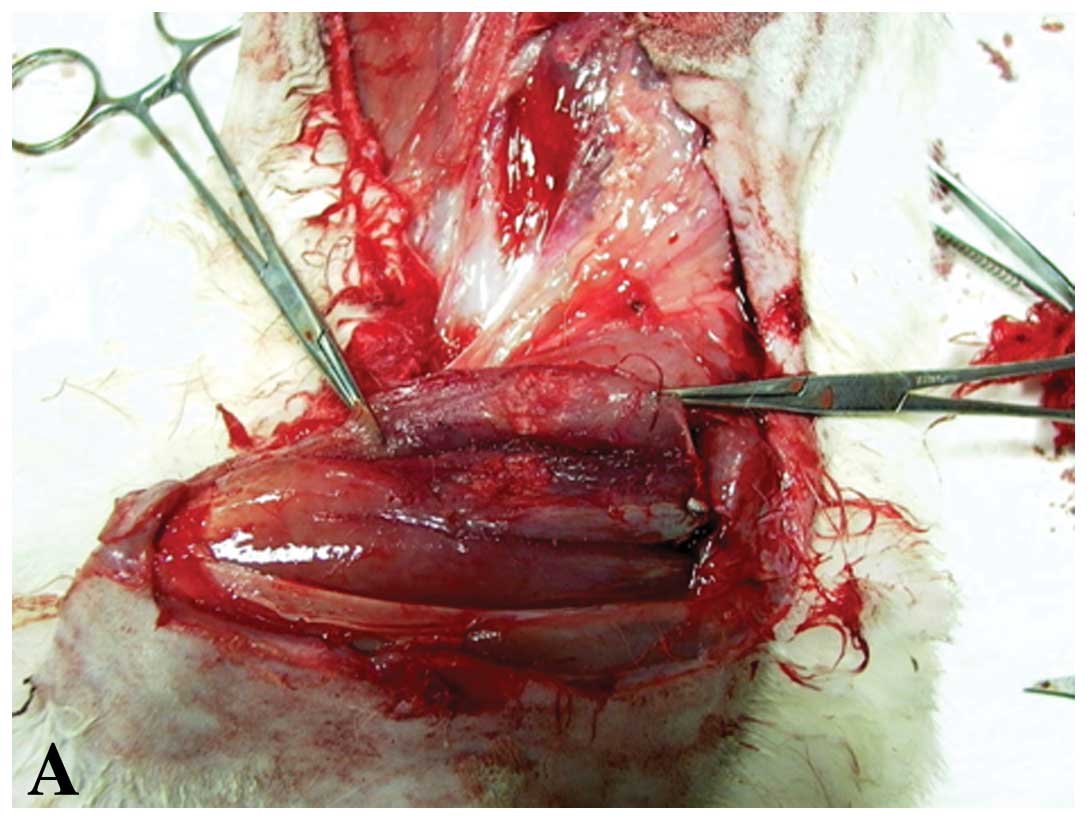
between normal and ablated tissue. From Day 1 to Day 3 after HIFU
radiation, these lesions were best observed grossly as a pale round
area and were surrounded by hyperemia (Fig. 2A). The most prominent early finding
was an inflammatory cell infiltration. The inflammation was
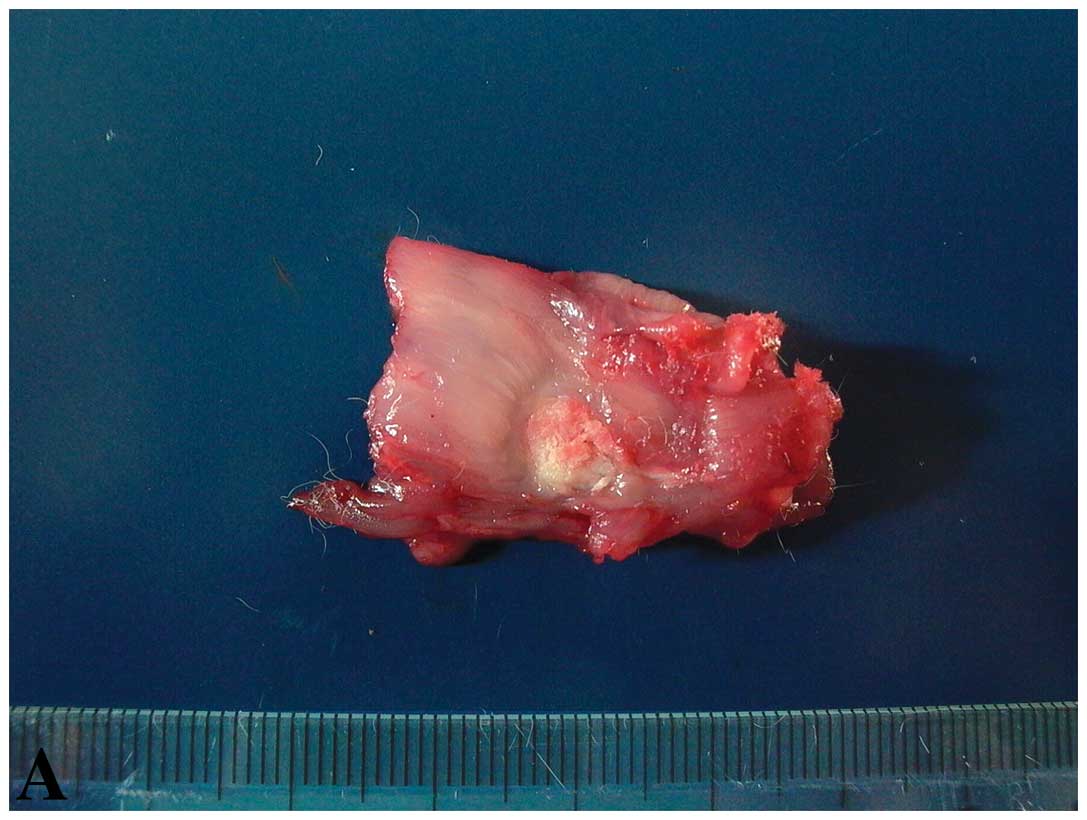
composed of leukocytes and a few lymphocytes (Fig. 2B). On Day 28 after HIFU radiation,
viewed grossly, the lesions appeared smaller. These lesions were
best observed grossly as pale-yellow round areas (Fig. 3A). No significant inflammatory
response was observed in the lesions. However, there were
fibroblasts, fatty infiltration and small scar formation in the
lesions (Fig. 3B).
Discussion
HIFU focuses sound waves to cause thermal
coagulation of tissues at the focus without harming intervening
tissues. HIFU destroys tissues mainly via heat. Due to its
non-invasive nature, HIFU is considered one of the most advanced
forms of minimally invasive therapy, the ultrasonic and
histological appearance of tissue following HIFU ablation is likely
to become critically important. Although other investigators have
studied the histological effects of HIFU in the short-term or in
externally exposed organs, this study took a systematic approach to
study the longer-term, in vivo histological effects of HIFU
lesions in a non-regenerative tissue such as muscle (11).
According to Solomon’s study (12), there were 3 stages of pathological
changes: i) early pathologic changes (Days 1–3): lesions were best
observed grossly as pale round areas surrounded by hyperemia. The
most prominent early finding was an alteration of cell properties,
with cytoplasmic filament condensation, nuclear and cytoplasmic
membrane breakdown, some edema, tissue shatter and decreased stain
uptake with a defined border. There was a distinct rim of
inflammation defining each treated area. ii) Intermediate
pathological changes (Days 14–29): where the inflammatory border
was present, there were fibroblasts admixed with the histiocytes
and the lesions appeared smaller. iii) Late pathological changes
(Days 51–100): observed grossly, the long-term lesions appeared
infiltrative and less well defined. No significant inflammatory
response was observed in any lesion (12).
In this study, we detected that the echo of
coagulation necrosis lesions was hyperechoic at 10 min after HIFU
radiation. The echo at the center of the HIFU lesion became lower 1
h after HIFU radiation, and there was a distinct hyperechoic border
zone surrounding the coagulation necrosis lesions. No apparent flow
signal was detected in the coagulation necrosis lesions. From Day 1
to Day 3 after HIFU radiation, the echo of coagulation necrosis
lesions was higher compared to normal muscle tissues. The
hyperechoic zone surrounding the coagulation necrosis lesions
became thinner. Although the echo of coagulation necrosis lesions
reduced from Day 3 to Day 7 after HIFU radiation, it was higher as
compared to normal muscle tissues. The hyperechoic zone surrounding
the coagulation necrosis lesions disappeared. By contrast, there
was a hypoechoic border zone with a width of 0.5–0.8 mm. From Day
14 to Day 28 after HIFU radiation, the volume of coagulation
necrosis lesions decreased markedly. The hypoechoic zone
disappeared gradually. The echogenicity of coagulation necrosis
lesions was homogeneous and hypoechoic. The border of the
coagulation necrosis lesions became unclear.
The diameters and volume of coagulation necrosis
lesions from 10 min to 7 days after HIFU irradiation were larger
compared to those from 14 to 28 days after HIFU irradiation. On Day
1 after HIFU radiation, the volume of coagulation necrosis lesion
was the largest, and was possibly associated with inflammation and
edema after HIFU radiation. The inflammation and edema were
relieved 14 days after HIFU radiation. The leucocyte and lymphocyte
numbers decreased while the fibroblasts regenerated markedly. The
coagulation of necrosis lesions shattered and the volume decreased
forming a scar. If the volume of coagulation necrosis was found to
have increased one week after HIFU radiation, it was considered
non-recurrent or without effect. This increase in volume may be
associated with inflammation and edema. The color Doppler, power
Doppler and other imaging technology, such as CT or MRI, were
recommended, thus the objective evaluation could be achieved. The
volume was stable 4 weeks after HIFU radiation, possibly reflecting
the effect of HIFU radiation crudely (13–16).
The ablations of rabbit muscles induced by HIFU were
performed without affecting the intervening tissues. HIFU
essentially destroys the targeted tissues via coagulation necrosis
lesions followed by inflammatory reaction, resorption, scar
formation and fatty infiltration. These observations are consistent
with those findings in other HIFU experiments and may aid in
planning clinical applications involving muscle tissues.
Ultrasound examination is crucial in the detection
after HIFU radiation, providing a basis for understanding
ultrasound effects for clinical applications, such as treatment of
uterine fibroids, cardiac tissues, sarcomas and soft tissue
tumors.
Acknowledgements
This study was financially supported
by the SJTU Medicine Engineering Interdisciplinary Research Fund
(YG2010MS39) and Shanghai Municipal Natural Science Foundation
(12ZR1422600).
References
|
1
|
Lynn JG and Putnam TJ: Histology of
cerebral lesions produced by focused ultrasound. Am J Pathol.
20:637–649. 1944.PubMed/NCBI
|
|
2
|
Ballantine HT Jr, Bell E and Manlapaz J:
Progress and problems is the neurological application of focused
ultrasound. J Neurosurg. 17:858–876. 1960. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Corry PM, Jabboury K, Kong JS, Armour EP,
McCraw FJ and Leduc T: Evaluation of equipment for hyperthermic
treatment of cancer. Int J Hyperthermia. 4:53–74. 1988. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
ter Haar G, Rivens I, Chen L and Riddler
S: High intensity focused ultrasound for the treatment of rat
tumours. Phys Med Biol. 36:1495–1501. 1991.
|
|
5
|
ter Haar GR and Robertson D: Tissue
destruction with focused ultrasound in vivo. Eur Urol. 23(Suppl 1):
8–11. 1993.PubMed/NCBI
|
|
6
|
Illing RO, Kennedy JE, Wu F, ter Haar GR,
Protheroe AS, Friend PJ, Gleeson FV, Cranston DW, Phillips RR and
Middleton MR: The safety and feasibility of extracorporeal
high-intensity focused ultrasound (HIFU) for the treatment of liver
and kidney tumours in a Western population. Br J Cancer.
93:890–895. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Kennedy JE, Wu F, ter Haar GR, Gleeson FV,
Phillips RR, Middleton MR and Cranston D: High intensity focused
ultrasound for the treatment of liver tumours. Ultrasonics.
42:931–935. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Wu F, Wang ZB, Chen WZ, Zou JZ, Bai J, Zhu
H, Li KQ, Xie FL, Jin CB, Su HB and Gao GW: Extracorporeal focused
ultrasound surgery for treatment of human solid carcinomas: early
Chinese clinical experience. Ultrasound Med Biol. 30:245–260. 2004.
View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Wu F, Wang ZB, Zhu H, Chen WZ, Zou JZ, Bai
J, Li KQ, Jin CB, Xie FL and Su HB: Extracorporeal high intensity
focused ultrasound treatment for patients with breast cancer.
Breast Cancer Res Treat. 92:51–60. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Kennedy JE: High-intensity focused
ultrasound in the treatment of solid tumours. Nat Rev Cancer.
5:321–327. 2005. View
Article : Google Scholar : PubMed/NCBI
|
|
11
|
Hazle JD, Stafford RJ and Price RE:
Magnetic resonance imaging-guided focused ultrasound thermal
therapy in experimental animal models: correlation of ablation
volumes with pathology in rabbit muscle and VX2 tumors. J Magn
Reson Imaging. 15:185–194. 2002.
|
|
12
|
Solomon SB, Nicol TL, Chan DY, Fjield T,
Fried N and Kavoussi LR: Histologic evolution of high-intensity
focused ultrasound in rabbit muscle. Invest Radiol. 38:293–301.
2003. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Hynynen K: The threshold for thermally
significant cavitation in dog’s thigh muscle in vivo. Ultrasound
Med Biol. 17:157–169. 1991.PubMed/NCBI
|
|
14
|
Moros EG and Hynynen K: A comparison of
theoretical and experimental ultrasound field distributions in
canine muscle tissue in vivo. Ultrasound Med Biol. 18:81–95. 1992.
View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Van Leenders GJ, Beerlage HP, Ruijter ET,
de la Rosette JJ and van de Kaa CA: Histopathological changes
associated with high intensity focused ultrasound (HIFU) treatment
for localised adenocarcinoma of the prostate. J Clin Pathol.
53:391–394. 2000.PubMed/NCBI
|
|
16
|
Fennessy FM, Tempany CM, McDannold NJ, So
MJ, Hesley G, Gostout B, Kim HS, Holland GA, Sarti DA, Hynynen K,
et al: Uterine leiomyomas: MR imaging-guided focused ultrasound
surgery - results of different treatment protocols. Radiology.
243:885–893. 2007. View Article : Google Scholar
|