Introduction
The number of patients with diabetes mellitus (DM)
has been increasing rapidly worldwide; the prevalence of DM has
increased from 2.5% in 1994 to 9.7% in 2008 in China (1,2), and
the incidence of diabetic foot ulcers (DFUs) has increased
concurrently (3). The prognosis
for DFUs remains poor, although our understanding and treatment of
this late-stage complication of DM have improved (4). As a common and serious complication
of diabetes, DFUs are associated with significant mortality
(5).
Patients with DM are generally considered to have
excessive food intake and medical nutrition therapy is required to
aid individuals with diabetes to achieve blood glucose targets
(6). Whereas previous studies have
shown that the nutritional status of patients in surgery, who are
critically ill, have cancer or end-stage renal disease, is markedly
correlated with the development of complications, hospital stay,
life expectancy and total outcomes (7–10);
when combined with diabetes, all the above became worse. In
clinical practice, fewer DFU patients achieved blood glucose
targets and a greater number suffer from vascular complications and
infection, or reveal a poor nutritional status compared with
non-DFU patients. These cause greater difficulties in treatment;
calorie intake should be restricted to achieve targets for blood
glucose and related metabolic markers while protein intake should
be confined to reduce proteinuria and improve the prognosis for
diabetic nephropathy (DN). However, the additional energy
expenditure due to infection requires increased energy intake, and
following surgery, patients require sufficient nutrients to recover
(11).
Weight loss during the course of diabetes reflects
changes in body composition and function, although in the context
of diabetes, this may also be a sensitive signal of nutritional
depletion. Sohn et al(12)
reported a significant J-shaped association between BMI and DFU and
Yekta et al(13) reported
that a BMI<25 kg/m2 was significantly associated with
amputation. In the present study, the mean BMI was 22.1
kg/m2 in the Wagner grade 1–5 patients and decreased as
the severity progressed; this value is lower than that of patients
at the time of diagnosis of DM in China (2). Together with decreasing BMI, vascular
complications, including neuropathy, nephropathy and peripheral
vascular disease (PVD) and certain nutritional indicators
(hemoglobin, serum albumin, total cholesterol) deteriorated
gradually. Moreover, these indicators were more serious in patients
with Wagner grade 4 and 5 ulcers. Our study hereby suggests that
the treatment of DFU should focus on foot management together with
improvements of general status, including the amelioration of
nutritional status.
Subjects and methods
Subjects
All subjects (192 DFU cases with Wagner grade 1–5
ulcers and 60 cases with Wagner grade 0 ulcers, all with type 2
diabetes) were hospitalized between January and December 2009. The
study protocol was approved by the Institutional Review Board of
Rui-Jin Hospital and the patients had provided informed consent. To
be eligible for inclusion, patients had to undergo a foot
examination and be definitively diagnosed with DFU. The severity of
the foot disease was graded according to Wagner’s classification
(14), which assesses ulcer depth
and the presence of osteomyelitis or gangrene using the following
grades: grade 0 (pre-or postulcerative lesion), grade 1
(partial/full thickness ulcer), grade 2 (probing to tendon or
capsule), grade 3 (deep with osteitis), grade 4 (partial foot
gangrene) and grade 5 (whole foot gangrene). All patients were
interviewed individually to obtain information concerning their
medical histories. Anthropometrics, evaluation of nutrition status,
assessment of diabetic complications and comorbidities and
foot-specific information at presentation were recorded, and
patients were followed up until the would was healed or for 6
months.
Measurements and evaluation of nutrition
status and clinical indicators
For anthropometrics, height and weight were measured
with light clothes and without shoes by the same physician. BMI was
calculated as the body weight in kilograms divided by the height
squared in meters. Blood pressure was measured at the right arm
with an automated electronic device (OMRON Model 1 plus; Omron
Company, Kyoto, Japan) three times consecutively at 1 min intervals
following at least 15 min rest in the seated position or in bed;
the three readings were averaged for analysis. A subjective global
assessment (SGA) was performed by a trained independent physician
within 72 h of admission, based on medical history and physical
examination, including changes in weight, dietary intake,
functional capacity, gastrointestinal symptoms, metabolic stress,
loss of subcutaneous fat, muscle wasting and ankle/sacral edema.
This information was used to classify patients into one of three
categories of nutritional status: A, well nourished; B, moderately
malnourished; or C, severely malnourished (15). Nutrition status was evaluated from
the SGA, BMI and hemoglobin, total protein, serum albumin and total
cholesterol levels.
The serum concentrations of triacylglycerol, total
cholesterol, total protein and albumin were detected using an
autoanalyser (Hitachi 7080 Automatic Analyzer; Hitachi Science
Systems, Ltd., Ibaraki, Japan). Hemoglobin was measured by
chromatometry using automatic equipment (ABX Pentra 80; Horiba,
Montpellier, France). The 24 h-urine protein was measured by
pyrogallol red molybdenum chromatometry (Dxl 800; Beckman Coulter,
Miami, FL, USA) and 24 h-urine microalbumin was tested using
immunoturbidimetry (Dade Behring BN II; Siemens, Munich, Germany).
HbA1c was analyzed by high pressure liquid chromatography with the
BioRad Variant Hemoglobin HbA1c assay (Hercules, CA, USA).
Assessment of diabetic complications and
comorbidities
Patients were screened for microalbuminuria by
measuring albumin from a 24-h urine collection. A urinary albumin
level of >30 mg per 24 h was diagnostic using a timed
accumulated sample. According to American Diabetes Association
guidelines, DN is diagnosed if two of three tests for
microalbuminuria are positive in a three- to six-month period
(16), excluding transient
albuminuria caused by exercise, urinary tract infections,
hyperglycemia, febrile illness, severe hypertension or heart
failure. Patients with overt nephropathy were detected easily by
routine urinalysis, a urinary albumin level of >300 mg per 24 h
or medical record.
Patients were identified and categorized for
diabetic peripheral neuropathy using a clinical examination and
conventional nerve conduction studies, or had been definitively
diagnosed previously. Based on the American Academy of Neurology
criteria, the classification of neuropathy is based on the presence
of at least one neuropathic symptom or sign together with
electrophysiological polyneuropathy as defined by an abnormality of
at least two parameters in at least two nerves (17). Other causes of the neuropathy
should be excluded for the diagnosis to be made.
PVD, commonly referred to as peripheral arterial
disease or peripheral artery occlusive disease, is the obstruction
of large arteries not within the coronary or aortic arch
vasculature or the brain. In the current study, PVD was examined
only in the lower extremities. Patients with calcified arteries
from DM occasionally have relatively non-compressible arteries
leading to falsely elevated ankle/brachial index (ABI) values in
the normal range. Thus, in our study, PVD was considered to be
present if the patients had acute or critical limb ischemia, or
intermittent claudication; it was documented in the medical record
or there was a history of limb revascularization (18); posterior tibialis and dorsalis
pedis pulses to palpation in the same limb were absent or
diminished (19); or stenosis or
obliteration of the lower extremity arteries was identified
following examination by doppler ultrasonography, computed
tomographic angiography, magnetic resonance angiography or contrast
arteriography.
Ulcers or gangrene were determined to be infected if
a purulent discharge and two other local signs (warmth, erythema,
lymphangitis, lymphadenopathy, edema or pain) were present
(20). The severity of infection
was evaluated according to the clinical classification of diabetic
foot infection instituted by the Infectious Diseases Society of
America (21). The classification
was described briefly as: uninfected, wound lacking purulence or
any manifestations of inflammation; mild, presence of ≥2
manifestations of inflammation (purulence, or erythema, pain,
tenderness, warmth or induration), but any cellulitis/erythema
extends ≤2 cm around the ulcer, and infection is limited to the
skin or superficial subcutaneous tissues, no other local
complications or systemic illness; moderate, infection (as above)
in a patient who is systemically well and metabolically stable but
which has at least one of the following characteristics: cellulitis
extending >2 cm, lymphangitic streaking, spread beneath the
superficial fascia, deep-tissue abscess, gangrene and involvement
of muscle, tendon, joint or bone; severe, infection in a patient
with systemic toxicity or metabolic instability (for example,
fever, chills, tachycardia, hypotension, confusion, vomiting,
leukocytosis, acidosis, severe hyperglycemia or azotemia).
Treatment of patients with foot ulcers
and outcome assessment
On the basis of the results assessed by general and
foot status, treatments were given individually. In general, for
foot ulcer care, patients were treated with insulin to control
blood glucose, hemorheologic agents and trophic nerve agents to
improve foot blood supply pro re nata, antibiotics when
infected, debridement or part amputation when abscess or gangrene
was present, or blood or albumin infusion if severe anemia or
hypoproteinemia existed, without interventional treatment.
The patients’ outcomes over the 6 months were
defined as healing (ulcer healed), deferment (ulcer did not heal),
recurrence (ulcer recurred), above-ankle amputation or
mortality.
Statistical analysis
Data are expressed as the mean and standard error
(continuous variables) or as a number and percentage (categorical
variables). Measurements with a skewed distribution were normalized
by logarithmic transformation. Comparisons of means and proportions
were performed with an ANOVA or χ2 test, as appropriate.
The homogeneity of groups was determined when the means had
significant differences. Fisher’s least significant difference
(LSD) post hoc test was applied for multiple comparisons where
appropriate. Spearman’s rank correlation analysis was used to
examine the relationship between SGA and potential affecting
factors. To assess the potential association between SGA and the
number of ulcers not healed by the end of the study period, a
χ2 analysis with odds ratio (OR) was performed. Multiple
stepwise regression analysis was conducted to examine the main
factors affecting nutrition status and outcome. SPSS 13.0 for
Windows (SPSS Inc., Chicago, IL, USA) was used for all analyses.
P<0.05 was considered to indicate a statistically significant
result.
Results
Clinical characteristics of DFU patients
with various Wagner grades
Table I shows the
baseline demographic details for the group of patients at first
presentation. For the 192 patients in the Wagner grade 1–5 groups,
the mean age and duration of DM were 68.6±11.3 and 12.3±8.1 years,
respectively. Most of these patients had poor blood glucose control
(mean HbA1c was 8.8%). Indicators of nutritional status (BMI,
albumin, total protein, hemoglobin and total cholesterol) were
lower than those in patients with Wagner grade 0 ulcers. Following
ANOVA adjustment for age, gender, duration of DM and duration of
DFU, the patients with Wagner grade 4 and 5 ulcers had
significantly lower cholesterol levels, BMI (also adjusted for SBP
and DBP), hemoglobin levels (also adjusted for HbA1c, total
protein, creatinine and 24 h-urine protein) and albumin levels
(also adjusted for total protein, creatinine, 24 h-urine protein
and 24 h-urine microalbuminuria) than the patients with Wagner
grade 0 and 1 ulcers (all P<0.05). The percentages of DFU
patients who had diabetic peripheral neuropathy, diabetic
nephropathy, peripheral vascular disease and infection at
presentation were 84.4, 45.3, 74.5 and 83.9% (161/192),
respectively. As the Wagner grade increased from 0 to 5, the
percentages of these complications and comorbidities increased.
 | Table IClinical characteristics of patients
grouped by Wagner’s classification. |
Table I
Clinical characteristics of patients
grouped by Wagner’s classification.
| Variables | W0 | W1 | W2 | W3 | W4 | W5 | (W1–5) | Total | Group comparison
|
|---|
| Statistics | P-value |
|---|
| Total (N) | 60 | 66 | 42 | 21 | 51 | 12 | 192 | 252 | | |
| Gender,
male/female | 37/23 | 39/27 | 28/14 | 15/6 | 30/21 | 6/6 | 118/74 | 155/97 | | |
| Age, years | 67.5±12.3 | 69.2±11.0 | 68.8±10.2 | 64.4±11.8 | 68.8±11.5 | 71.7±14.3 | 68.6±11.3 | 68.4±11.5 | 0.858 | 0.510 |
| BMI,
kg/m2 | 23.7±3.3 | 22.9±3.6 | 22.3±3.2 | 21.5±2.2a | 21.9±2.9a | 18.6±1.9a–e | 22.1±3.2 | 22.5±3.3 | 11.329 | 0.000 |
| Duration of DM,
years | 11.3±9.5 | 12.2±8.8 | 14.2±7.9 | 12.7±7.9 | 11.0±7.1 | 9.8±7.9 | 12.3±8.1 | 12.0±8.4 | 1.019 | 0.407 |
| Duration of DFU,
days | / | 53±105 | 129±250 | 67±86 | 72±73 | 70±50 | 77±143 | / | 1.977 | 0.100 |
| HbA1c, % | 8.5±2.1 | 8.2±2.0 | 8.7±2.0 | 8.8±1.9 | 9.0±2.4 | 11.5±2.4a–e | 8.8±2.2 | 8.7±2.2 | 4.597 | 0.001 |
| Triglyceride,
mmol/l | 1.65±1.31 | 1.65±1.44 | 1.41±1.47 | 1.07±0.50 | 1.10±0.34a | 0.97±0.41a | 1.35±1.15 | 1.43±1.19 | 4.031 | 0.003 |
| Total cholesterol,
mmol/l | 4.57±1.10 | 4.35±1.19 | 4.25±1.13 | 3.89±1.04a | 3.72±1.24ab | 3.53±1.42a,b | 4.07±1.21 | 4.19±1.20 | 3.979 | 0.002 |
| Hemoglobin,
g/l | 123.0±14.5 | 117.3±17.8 | 111.3±20.4a | 106.1±15.0a,b | 103.2±16.5a–c | 91.8±23.0a–e | 109.4±19.4 | 112.7±19.2 | 12.295 | 0.000 |
| Total protein,
g/l | 65.9±6.8 | 66.1±5.9 | 64.2±7.1 | 65.2±8.3 | 65.5±6.1 | 57.2±8.1a–e | 64.9±6.9 | 65.1±6.9 | 3.941 | 0.002 |
| Albumin, g/l | 37.9±3.7 | 36.9±3.9 | 34.3±4.7a,b | 32.0±5.5a–c | 32.8±4.2a,b | 25.2±5.4a–e | 34.0±5.3 | 34.9±5.2 | 25.935 | 0.000 |
| Creatinine,
μmol/l | 73.0±34.0 | 84.1±43.5 | 76.8±30.9 | 84.2±57.7 | 79.9±38.1 | 92.8±70.1 | 82.0±43.4 | 79.8±41.5 | 0.686 | 0.636 |
| 24 h-urine protein,
mg/24 h | 273.3±401.2 |
540.4±1025.7a |
897.5±1271.7a |
911.5±1935.8a |
772.4±1076.7a |
1043.8±850.9a | 752.9±1212.5 | 622.3±1075.6 | 5.493f | 0.000f |
| Diabetic
nephropathy, n/N (%) | 21/60 (35.0) | 20/66 (30.3) | 20/42 (47.6) | 10/21 (47.6) | 27/51 (52.9) | 10/12 (83.3) | 87/192 (45.3) | 108/252 (42.9) | 16.489 | 0.006 |
| Diabetic peripheral
neuropathy, n/N (%) | 27/60 (45.0) | 48/66 (72.7) | 38/42 (90.5) | 20/21 (95.2) | 45/51 (88.2) | 11/12 (91.7) | 162/192 (84.4) | 189/252 (75.0) | 45.477 | 0.000 |
| Peripheral vascular
disease, n/N (%) | 25/60 (41.7) | 37/66 (56.1) | 36/42 (85.7) | 17/21 (81.0) | 42/51 (82.4) | 11/12 (91.7) | 143/192 (74.5) | 168/252 (66.7) | 38.024 | 0.000 |
Nutritional status of patients with
DFU
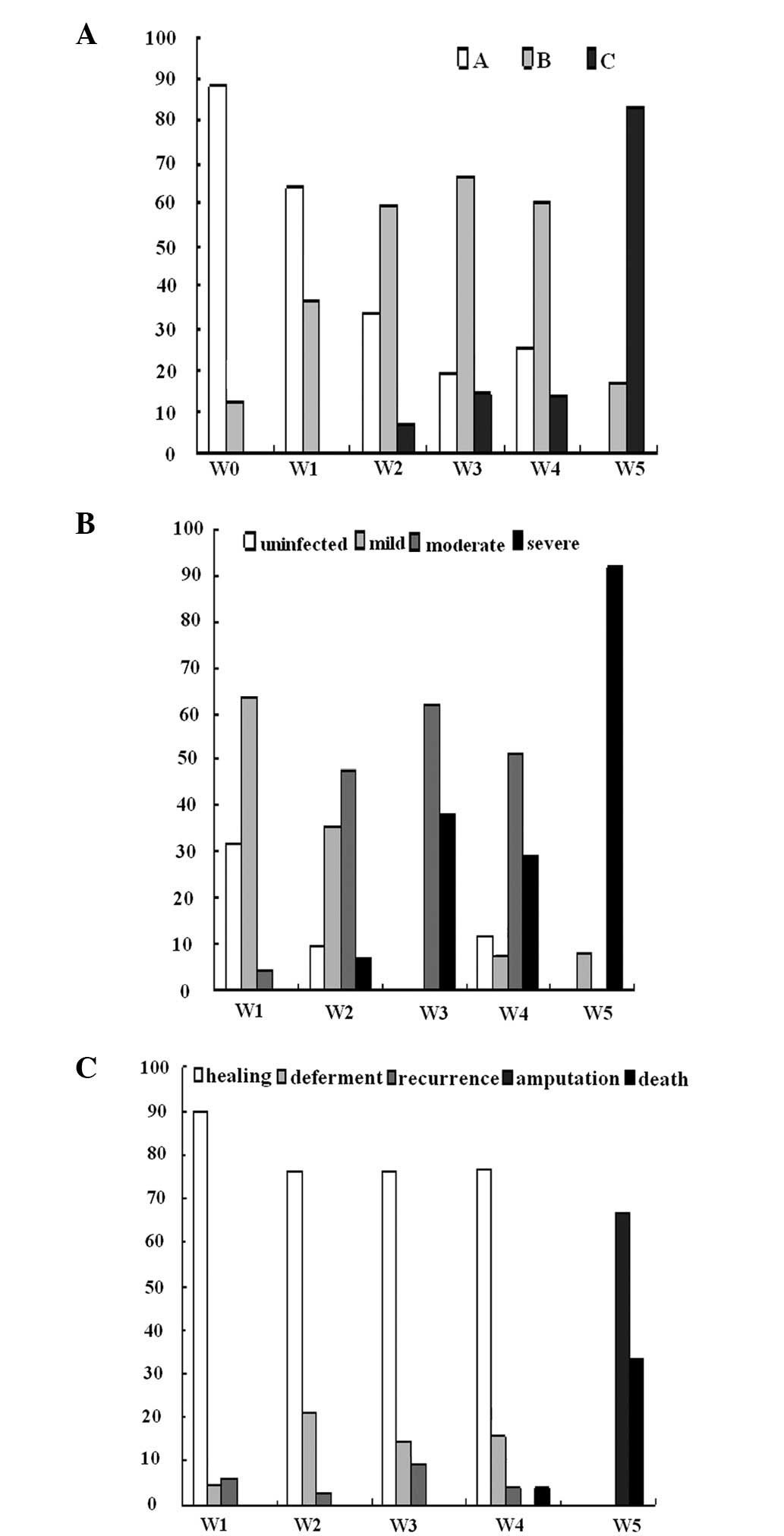
Only 11.7% of patients with Wagner grade 0 ulcers
were malnourished (SGA-B or SGA-C) compared with 62.0% of patients
with Wagner grade 1–5 ulcers at presentation. As the Wagner grade
increased, the percentage of malnutrition also increased (Fig. 1A).
Even at same levels of age, duration of DM and
HbA1c, the indicators associated with nutrition differed among the
patients in each of the SGA groups (Table II). Along with deteriorating
nutritional status, patients presented a longer duration of DFU,
higher serum creatinine levels and more protein leakage.
| Table IIClinical characteristics of studied
patients grouped by SGA. |
Table II
Clinical characteristics of studied
patients grouped by SGA.
| Variables | SGA-A | SGA-B | SGA-C | Group comparison
|
|---|
| Statistics | P-value |
|---|
| Total (N) | 126 | 103 | 23 | | |
| Gender,
male/female | 78/48 | 64/39 | 13/10 | | |
| Age, years | 67.2±11.6 | 69.5±10.5 | 69.7±14.7 | 1.246 | 0.289 |
| BMI,
kg/m2 | 23.5±3.2 | 21.8±3.1 | 19.5±2.3 | 19.725 | 0.000 |
| Duration of DM,
years | 11.6±8.3 | 13.1±8.8 | 9.9±6.5 | 1.732 | 0.179 |
| Duration of DFU,
daysa | 55±87 | 73±101 | 138±292 | 3.312 | 0.039 |
| HbA1c, % | 8.7±2.1 | 8.5±2.2 | 9.6±2.9 | 1.227 | 0.302 |
| Triglyceride,
mmol/l | 1.53±1.21 | 1.39±1.27 | 1.00±0.39 | 1.726 | 0.180 |
| Total cholesterol,
mmol/l | 4.30±1.15 | 4.20±1.24 | 3.49±1.17 | 4.006 | 0.019 |
| Hemoglobin,
g/l | 118.7±16.5 | 109.5±18.5 | 93.7±21.1 | 21.909 | 0.000 |
| Total protein,
g/l | 66.1±7.0 | 65.1±5.8 | 59.5±8.5 | 9.591 | 0.000 |
| Albumin, g/l | 36.6±4.5 | 34.6±4.1 | 27.2±6.2 | 26.725 | 0.000 |
| Creatinine,
μmol/l | 75.3±32.4 | 83.0±44.9 | 90.4±63.5 | 1.502 | 0.232 |
|
Log10UP-24hb | 2.32±0.48 | 2.46±0.57 | 2.90±0.47 | 8.692 | 0.000 |
|
Log10UMA-24hb | 1.74±0.60 | 1.87±0.76 | 2.20±0.58 | 3.038 | 0.050 |
Severity of infection in patients with
DFU
The percentage of DFU patients who had clinically
infected ulcers at presentation was 83.9% (68.2–100% from Wagner
grades 1 to 5) and the incidence of moderate and severe infection
increased for Wagner grades >3 (Fig. 1B). Due to mummification necrosis,
some patients with Wagner grade 4 and 5 ulcers were identified to
be uninfected or mildly infected.
Outcomes of DFU patients and interactions
of nutrition, infection and outcome
At the end of the study period, the majority of
ulcers of Wagner grade 1–4 were healed (146/180, 81.1%) and no
patient required amputation above the ankle. The percentages of
ulcer deferment or recurrence were also relatively low among these
grades (Fig. 1C). Two of the 51
patients with Wagner grade 4 ulcers unexpectedly succumbed
following 10 and 28 days hospitalization. For patients with Wagner
grade 5 ulcers, the outcome was either above-ankle amputation or
mortality.
Retrospective analysis identified that the DFU
patients with various outcomes had significant differences in BMI,
total protein, serum albumin, hemoglobin and HbA1c at first
presentation. The poorer the outcome, the worse these factors,
despite age, duration of DM and duration of DFU among these groups
being at similar levels (Table
III).
| Table IIIClinical characteristics of DFU
patients grouped by outcome. |
Table III
Clinical characteristics of DFU
patients grouped by outcome.
| Variables | Healing | Deferment | Recurrence | Amputation | Mortality | Group comparison
|
|---|
| Statistics | P-value |
|---|
| Total | 146 | 23 | 9 | 8 | 6 | | |
| Gender,
male/female | 92/54 | 13/10 | 7/2 | 5/3 | 1/5 | | |
| Age, years | 68.1±11.5 | 72.7±8.4 | 64.3±8.6 | 67.1±12.3 | 74.2±15.6 | 1.540 | 0.192 |
| BMI,
kg/m2 | 22.6±3.2 | 20.9±2.6 | 21.6±3.1 | 18.3±1.8 | 20.5±3.3 | 4.992 | 0.001 |
| Duration of DM,
years | 11.6±7.8 | 16.1±8.5 | 13.2±7.6 | 11.4±8.5 | 12.1±10.7 | 1.623 | 0.170 |
| Duration of DFU,
days | 77±158 | 101±96 | 29±46 | 80±48 | 57±45 | 0.437 | 0.482 |
| HbA1c, % | 8.7±2.2 | 7.6±1.2 | 8.8±1.7 | 10.5±2.7 | 11.9±2.8 | 4.941 | 0.001 |
| Triglyceride,
mmol/l | 1.44±1.27 | 1.05±0.45 | 1.24±0.55 | 0.99±0.47 | 0.98±0.14 | 0.878 | 0.479 |
| Total cholesterol,
mmol/l | 4.18±1.24 | 3.67±0.89 | 4.03±0.94 | 3.56±1.58 | 3.30±0.55 | 1.529 | 0.196 |
| Hemoglobin,
g/l | 112.2±18.3 | 101.5±17.5 | 109.0±22.7 | 84.3±24.4 | 104.0±9.9 | 5.682 | 0.000 |
| Total protein,
g/l | 65.8±6.8 | 63.0±5.2 | 63.4±3.7 | 57.4±4.4 | 60.1±12.4 | 4.468 | 0.002 |
| Albumin, g/l | 35.0±4.9 | 32.8±2.9 | 31.7±3.5 | 23.9±4.6 | 29.3±6.2 | 13.276 | 0.000 |
| Creatinine,
μmol/l | 80.0±41.2 | 82.1±34.7 | 76.8±29.4 | 88.3±72.1 | 127.8±76.6 | 0.573 | 0.686 |
|
Log10UP-24h | 2.45±0.54 | 2.72±0.55 | 2.93±0.35 | 2.79±0.66 | 2.73±0.70 | 0.728 | 0.574 |
|
Log10UMA-24h | 1.82±0.68 | 2.17±0.88 | 2.35±0.70 | 2.24±0.56 | 2.06±0.66 | 1.026 | 0.397 |
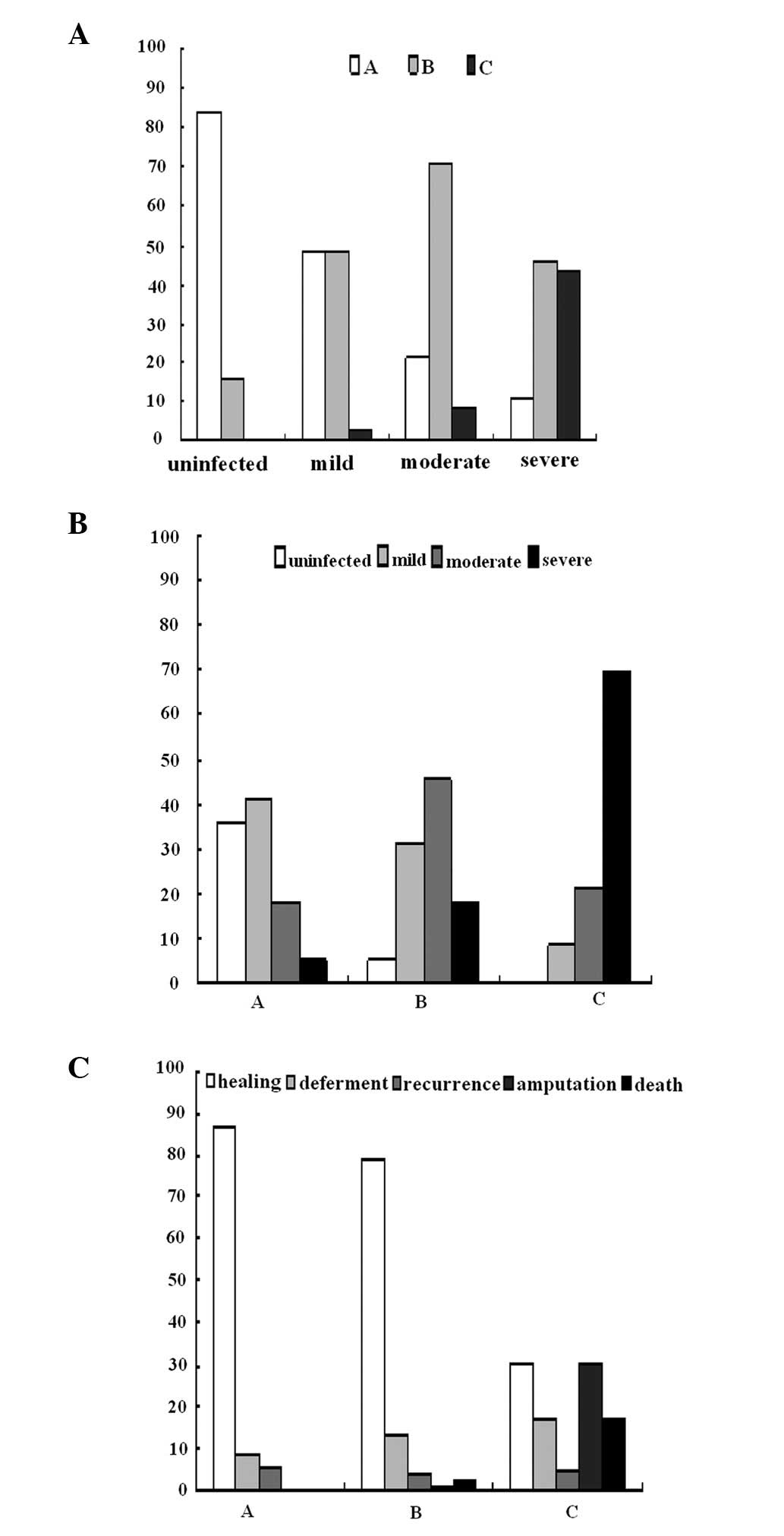
None of the DFU patients with uninfected feet were
severely malnourished, the majority of the patients with mildly or
moderately infected feet were moderately malnourished, while 43.2%
of patients with severe infection were severely malnourished
(Fig. 2A). However, few
well-nourished patients developed moderate or severe infection,
whereas 69.6% of severely malnourished patients were severely
infected (Fig. 2B). The majority
of the foot ulcers in the well nourished patients healed (86.3%),
but those in malnourished patients tended to deferment or
recurrence. Patients with SGA-C status had poor outcome (69.6%)
with high rates of mutilation (7/23, 30.4%) and mortality (4/23,
17.4%; Fig. 2C).
Malnourished patients (SGA-B and -C) were 11-fold
more likely to have a poor outcome (not healed in six months) than
SGA-A patients (69.6 vs. 17.8%; P<0.001; OR, 0.6; 95% CI,
4.1–28.0).
Correlation analysis and multiple
stepwise regression analysis of SGA, outcome and correlated
factors
The SGA result significantly correlated with
duration of DFU, infection status, Wagner grades, BMI, urine
protein leakage and outcome, all P<0.05. Multiple stepwise
regression analysis identified that the severity of infection and
outcome were independently associated with the patients’
nutritional status, and the standardized coefficient or β values
were 0.47 and 0.28 respectively, both P<0.001. Analysis also
revealed that the independent risk factors of outcome were severity
of DFU (Wagner grades, β=0.33) and nutritional status (SGA,
β=0.28), both P<0.001.
Discussion
Few studies have identified foot ulcer
classification systems as predictors of clinical outcome. The
current study not only assessed these factors, but also was the
first to identify nutritional status as a predictor for the
clinical outcome of DFU patients. As the Wagner grade of the ulcer
increased: the BMI and serum albumin, hemoglobin and total
cholesterol levels decreased; the urine protein leakage, severity
of infection and percentages of SGA grades B and C increased; and
nutritional status deteriorated. The patients’ outcome was
independently affected by the severity of the DFU and nutritional
status. Malnutrition was identified in 62.0% of the studied
patients and malnutrition at presentation was predictive of poor
outcome.
Poor nutritional status is significant in the
prognosis of most chronic, critical or infectious diseases, or
following surgery (7–10). As in uremic diabetic patients,
nutritional indicators, including age, BMI and low serum albumin
concentrations, were independent factors associated with mortality,
initiated time to dialysis and other complications (10,22).
For DFU patients, the factors affecting outcome include Wagner
grades, BMI, serum albumin and, more importantly, infection and
nutritional status; the affect of nutritional status is similar in
other diseases.
A number of factors are involved in and lead to
malnutrition in patients with DFUs. A higher resting energy
expenditure (REE) may contribute to the deterioration in
nutritional status of the diabetic patients with foot ulcers, since
type 2 DM mirrors chronic disease states associated with elevated
protein turnover and rapid loss of body protein (23). The kinetics of whole-body protein
metabolism were elevated and net balance was diminished. Elevated
flux has been identified to be associated with increased REE,
insulin resistance or lack of insulin secretion; these alterations
were worsened with the magnitude of hyperglycemia (24). DFU patients may expend more energy
and lose more protein than non-DFU patients due to elevated flux
and poorly controlled blood glucose.
Hyperglycemia and a negative nitrogen balance cause
diabetic patients to tend to malnutrition and infection. With skin
damage and poor blood supply, DFU patients have a very high rate of
infection; it was 83.9% in the current study, and a high proportion
of the ulcers were moderately or severely infected. Infection and
malnutrition have always been intricately linked (25). The interaction of the two leads to
a synergistic vicious cycle of increased susceptibility to
infection and adverse nutritional status (26).
According to our data and previous studies (4,19,27,28),
DFU patients have a long duration of DM, accompanied by a high
morbidity rate of micro- and macro-vascular complications. Diabetes
is often associated with nephropathy, which is a disturbance
involving protein leakage and a decreased glomerular filtration
rate, and peripheral neuropathy, including autonomic neuropathy
which gives rise to pain, numbness, gastroparesis, diarrhea and
movement intolerance. These, together with vascular complications,
result in sleeplessness, poor appetite, increased energy
expenditure, loss of protein, edema and deteriorating nutritional
status.
SGA is used primarily by clinicians to assess the
nutritional status of hospitalized patients. Compared with the
Nutritional Risk Index (serum albumin and recent weight loss), BMI
and serum albumin, SGA acted as a good predictor for malnutrition
and complications (10,29). In the current study, most DFU
patients with severe malnutrition had a poor prognosis: 17.4%
deferment, 30.4% above-ankle amputation, 17.4% mortality and only
30.4% healing, whereas for the moderately malnourished patients,
the ulcer healing rate sharply increased to 79.2%, and further
increased to 86.3% in patients with a well-nourished status.
Malnutrition has a marked association with increased risk of poor
outcome and predicts poor ulcer healing.
If DFU patients with severe malnutrition receive
sufficient nourishment, their prognosis may be improved. This is
clearly positive, but in chronic diseases, it may not be possible
for patients with severe malnutrition to be provided with large
amounts of calories in a short time, or quickly infused with blood
products to elevate hemoglobin or serum albumin to normal levels
(30,31), as the treatment may result in
further complications, including heart failure and impairment of
renal function. The outcome data in the current study were acquired
following proper nutritional supplementation, and our results
suggest that even with the appropriate treatments for general
condition, including nutrition amelioration, infection control and
foot care, the prognosis of severely malnourished patients remains
poor.
Certain flaws of the current study should be
addressed. The small sample size in the SGA-C, Wagner grade 5 and
certain outcome groups resulted in an unbalanced distribution of
some clinical indicators in different groups, which may limit the
power of data analysis. Increasing the number of DFU cases may
improve this defect, but data collected over a longer time or from
other centers may affect the consistency of the results due to
inequalities in the tests and treatments. The clinical
characteristics of the subjects in the current study differed from
those in a number of previous studies (32,33).
Our patients were older, with longer durations of DM and DFU, more
abnormalities of biochemical indicators and higher percentages of
complications and comorbidities. These differences may be due to
diversities of the diagnostic tests and population selection.
In conclusion, the higher the Wagner grade, the
poorer the nutritional status and outcome. Malnutrition was common
in DFU patients, and the prognosis of the severely malnourished
patients was poor, despite compensation with appropriate
treatments. Assessment of the nutritional status of DFU patients
should be emphasized since it is a key anticipator of outcome.
Acknowledgements
The present study would not have been
possible without the participation of the DFU patients. This study
was supported by the Shanghai Pujiang Project (Zhengyi Tang group)
and the National Natural Foundation of China for Preeminence Youth
(No. 30725037).
References
|
1
|
Pan XR, Yang WY, Li GW and Liu J:
Prevalence of diabetes and its risk factors in China, 1994.
National Diabetes Prevention and Control Cooperation Group.
Diabetes Care. 20:1664–1669. 1997. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Yang W, Lu J, Weng J, et al: Prevalence of
diabetes among men and women in China. N Engl J Med. 362:1090–1101.
2010. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Boulton AJ, Vileikyte L,
Ragnarson-Tennvall G and Apelqvist J: The global burden of diabetic
foot disease. Lancet. 366:1719–1724. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Ghanassia E, Villon L, Thuan Dit Dieudonné
JF, Boegner C, Avignon A and Sultan A: Long-term outcome and
disability of diabetic patients hospitalized for diabetic foot
ulcers. A 65-year follow-up study. Diabetes Care. 31:1288–1292.
2008.PubMed/NCBI
|
|
5
|
Tabatabaei Malazy O, Mohajeri-Tehrani MR,
Pajouhi M, Shojaei Fard A, Amini MR and Larijani B: Iranian
diabetic foot research network. Adv Skin Wound Care. 23:450–454.
2010.PubMed/NCBI
|
|
6
|
Swift CS and Boucher JL: Nutrition care
for hospitalized individuals with diabetes. Diabetes Spectr.
18:34–37. 2005. View Article : Google Scholar
|
|
7
|
Ozkalkanli MY, Ozkalkanli DT, Katircioglu
K and Savaci S: Comparison of tools for nutrition assessment and
screening for predicting the development of complications in
orthopedic surgery. Nutr Clin Pract. 24:274–280. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Sungurtekin H, Sungurtekin U, Oner O and
Okke D: Nutrition assessment in critically ill patients. Nutr Clin
Pract. 23:635–641. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Wu BW, Yin T, Cao WX, et al: Clinical
application of subjective global assessment in Chinese patients
with gastrointestinal cancer. World J Gastroenterol. 15:3542–3549.
2009. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Raffaitin C, Lasseur C, Chauveau P, et al:
Nutritional status in patients with diabetes and chronic kidney
disease: a prospective study. Am J Clin Nutr. 85:96–101.
2007.PubMed/NCBI
|
|
11
|
Litchford MD: Nutrition issues in the
patient with diabetes and foot ulcers. Levin and O’Neal’s The
Diabetic Foot. 7th edition. Bowker JH and Pfiefer MA: Elsevier;
Philadelphia, PA: pp. 199–217. 2008
|
|
12
|
Sohn MW, Budiman-Mak E, Lee TA, Oh E and
Stuck RM: Significant J-shaped association between body mass index
(BMI) and diabetic foot ulcers. Diabetes Metab Res Rev. 27:402–409.
2011. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Yekta Z, Pourali R, Nezhadrahim R,
Ravanyar L and Ghasemi-Rad M: Clinical and behavioral factors
associated with management outcome in hospitalized patients with
diabetic foot ulcer. Diabetes Metab Syndr Obes. 4:371–375. 2011.
View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Wagner FW: Algorithms of diabetic foot
care. The Diabetic Foot. Levin ME and O’Neil FW: 2nd edition.
Mosby; St. Louis, MO: pp. 575–585. 1996
|
|
15
|
Detsky AS, McLaughlin JR, Baker JP, et al:
What is subjective global assessment of nutritional status? JPEN J
Parenter Enteral Nutr. 11:8–13. 1987. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Thorp ML: Diabetic nephropathy: common
questions. Am Fam Physician. 72:96–99. 2005.PubMed/NCBI
|
|
17
|
England JD, Gronseth GS, Franklin G, et
al: Distal symmetric polyneuropathy: a definition for clinical
research: report of the American Academy of Neurology, the American
Association of Electrodiagnostic Medicine, and the American Academy
of Physical Medicine and Rehabilitation. Neurology. 64:199–207.
2005. View Article : Google Scholar
|
|
18
|
Hirsch AT, Criqui MH, Treat-Jacobson D, et
al: Peripheral arterial disease detection, awareness, and treatment
in primary care. JAMA. 286:1317–1324. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Amanda I, Jessie H, Edward J and Douglas
G: Lower-extremity amputation in diabetes. The independent effects
of peripheral vascular diseases, sensory neuropathy, and foot
ulcers. Diabetes Care. 22:1029–1035. 1999. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Oyibo SO, Jude EB, Tarawneh I, Nguyen HC,
Harkless LB and Boulton AJ: A comparison of two diabetic foot ulcer
classification systems: the Wagner and the University of Texas
wound classification systems. Diabetes Care. 24:84–88. 2001.
View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Lipsky BA, Berendt AR, Deery HG, et al
Infectious Diseases Society of America: Diagnosis and treatment of
diabetic foot infections. Clin Infect Dis. 39:885–910. 2004.
View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Combe C, Chauveau P, Laville M, et al
French Study Group Nutrition in Dialysis: Influence of nutritional
factors and hemodialysis adequacy on the survival of 1,610 French
patients. Am J Kidney Dis. 37(Suppl 2): S81–S88. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Biolo G, Antonione R, Barazzoni R, Zanetti
M and Guarnieri G: Mechanisms of altered protein turnover in
chronic diseases: a review of human kinetic studies. Curr Opin Clin
Nutr Metab Care. 6:55–63. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Gougeon R, Morais JA, Chevalier S, Pereira
S, Lamarche M and Marliss EB: Determinants of whole-body protein
metabolism in subjects with and without type 2 diabetes. Diabetes
Care. 31:128–133. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Katona P and Katona-Apte J: The
interaction between nutrition and infection. Clin Infect Dis.
46:1582–1588. 2008. View
Article : Google Scholar : PubMed/NCBI
|
|
26
|
Schaible UE and Kaufmann SH: Malnutrition
and infection: complex mechanisms and global impacts. PLoS Med.
4:e1152007. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Cano NJ, Roth H, Aparicio M, Azar R,
Canaud B and Chauveau P; French Study Group for Nutrition in
Dialysis (FSG-ND): Malnutrition in hemodialysis diabetic patients:
evaluation and prognostic influence. Kidney Int. 62:593–601. 2002.
View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Davis WA, Norman PE, Bruce DG and Davis
TM: Predictors, consequences and costs of diabetes-related lower
extremity amputation complicating type 2 diabetes: the Fremantle
Diabetes Study. Diabetologia. 49:2634–2641. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Thoresen L, Fjeldstad I, Krogstad K, Kaasa
S and Falkmer UG: Nutritional status of patients with advanced
cancer: the value of using the subjective global assessment of
nutritional status as a screening tool. Palliat Med. 16:33–42.
2002. View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Klein S, Kinney J, Jeejeebhoy K, et al:
Nutrition support in clinical practice: review of published data
and recommendations for future research directions. Clin Nutr.
16:193–218. 1997. View Article : Google Scholar
|
|
31
|
Beyer I, Compté N, Busuioc A, Cappelle S,
Lanoy C and Cytryn E: Anemia and transfusions in geriatric
patients: a time for evaluation. Hematology. 15:116–121. 2010.
View Article : Google Scholar : PubMed/NCBI
|
|
32
|
Shaw JE and Zimmet PZ: The epidemiology of
diabetic neuropathy. Diabetes Rev. 7:245–252. 1999.
|
|
33
|
Boulton AJ, Connor H and Cavanagh PR: The
size of the problem: epidemiological and economical aspects of the
diabetic foot. The Foot in Diabetes. Williams R and Airey M: Wiley;
Chichester: pp. 3–17. 2000
|