Introduction
Benign prostatic hyperplasia (BPH), a noncancerous
enlargement of the prostate gland, is a common prostate disorder
among older men. An estimated 50% of men have histological evidence
of BPH by age 50 years and 80% by age 70 (1). With the prolonged average life span,
increasing elderly population and increasing incidence, BPH has
become a major disease of significant interest. The enlarged
prostate gland puts pressure on the urethra and/or causes the
muscles around the urethra to contract, resulting in partial, or
sometimes virtually complete, obstruction of the urethra, which
interferes with the normal flow of urine. BPH leads to lower
urinary tract symptoms (LUTS) including urinary hesitancy, frequent
urination, urgency, thin urine flow and urinary retention (2). These symptoms greatly affect the
physical and mental health of patients, as well as their quality of
life. Delayed treatment causes numerous severe complications,
including bleeding from the prostate, recurrent infections, renal
stones and even kidney failure.
Although the pathogenesis of BPH is complex and
remains unclear, the important role of androgens, including
testosterone and its metabolite dihydrotestosterone (DHT), in the
progression of BPH is well established (3). Testosterone or DHT exerts its
function by binding to nuclear androgen receptors that are located
in the surfaces of stromal cells and epithelial cells, which in
turn promotes the transcription of growth factors, including
epidermal growth factor (EGF) (4–6). EGF
is an important mitosis- and proliferation-promoting factor that
has been shown to play a critical role in the development of the
prostate after binding to its specific receptor (EGFR, a receptor
protein tyrosine kinase) (5–8).
Upon interaction with EGF, EGFR induces the phosphorylation and
activation of signal transducer and activator of transcription 3
(STAT3), a transcription factor essential for cell survival and
proliferation. The phosphorylation of STAT3 in the cytoplasm
induces its homodimerization, nuclear translocation and DNA
binding, resulting in the expression of genes that mediate
proliferation (e.g. cyclin D1) and prevent apoptosis (e.g. Bcl-2)
(9). Abnormal activation of the
EGF/STAT3 pathway causes an increase in the total number of stromal
and epithelial cells, which is strongly associated with the
development of BPH (10–15).
At present, pharmacotherapy remains the modality of
choice for BPH treatment, and may be roughly divided into three
groups: α-blockers, 5α-reductase inhibitors and alternative
therapies. The α-blockers, including terazosin, doxazosin and
tamsulosin (16,17), inhibit α-adrenergic receptors,
thereby relaxing smooth muscle in the prostate and the bladder neck
and alleviating the restriction of urine flow. The 5α-reductase
inhibitors, including finasteride and dutasteride, suppress
5α-reductase, thereby inhibiting DHT production and the enlargement
of prostate. However, these prescription medications may have
adverse side effects, including orthostatic hypotension, decreased
libido and ejaculatory or erectile dysfunction (18–22).
Due to these risks, natural products that appear to have limited
adverse events are becoming increasingly important in the treatment
of BPH. Although the mechanisms of action are unknown, herbal
remedies, including saw palmetto, Pygeum africanum and
Hypoxis rooperi(23–25),
have long been used to treat BPH successfully.
Qianliening capsule (QC) is a traditional Chinese
medicine formulation that consists of a combination of five natural
products (Table I), including
rhubarb, leech, Astragalus, Achyranthes and Dodder. These products
together confer properties of heat-clearing, detoxification,
promotion of blood circulation, removal of blood stasis, tonifying
the kidney and nourishing vitality (replenishing the kidney qi in
Chinese medicine) (26,27). In the past two decades, QC has been
shown to have significant therapeutic effects on BPH (27–29).
In clinical trials, QC markedly improved BPH symptoms, by
increasing the free maximum urinary flow rate and average urinary
flow rate, alleviating frequent urination and urinary urgency, and
improving the dynamic index of urine flow (30). In addition, in tests with
experimental animals, QC significantly decreased the prostatic
volume and weight, inhibited prostatic hyperplasia, attenuated the
abnormal serum levels of estrogen and androgen, regulated the
expression of estrogen receptor (ER), androgen receptor (AR) and
related mRNA, and inhibited the expression of pro-proliferative
PCNA, cyclin D1 and CDK4 in the prostatic tissues of BPH rats
(26–30). However, the mechanism of its
anti-BPH activity remains largely unknown. Therefore we evaluated
the effect of QC in a rat model of BPH, established by the
injection of testosterone following castration, and investigated
the underlying molecular mechanism.
 | Table IComposition of Qianliening capsule
(QC). |
Table I
Composition of Qianliening capsule
(QC).
| Common name | Latin name | Part used | Daily adult dose
(g) |
|---|
| Rhubarb | Radix et Rhizoma
Rhei | Dried root | 15 |
| Leech | Hirudo | Dried body | 3 |
| Astragalus | Radix
Astragali | Dried root | 12 |
| Achyranthes | Radix
Achyranthis Bidentatae | Dried root | 9 |
| Dodder | Semen
Cuscutae | Dried seed | 6 |
Materials and methods
Animals
Sixty SPF grade male Sprague-Dawley (SD) rats (with
an initial body weight of 200–220 g) were purchased from Shanghai
Si-Lai-Ke Experimental Animal Ltd. (Shanghai, China). The rats were
housed in clean pathogen-free rooms in an environment with
controlled temperature (22°C), humidity and a 12 h light/dark cycle
with free access to water and standard laboratory food. All animal
treatment was strictly in accordance with international ethical
guidelines and the guide for the Care and Use of Laboratory Animals
(31), and the experiments were
approved by the Institutional Animal Care and Use Committee of
Fujian University of Traditional Chinese Medicine (Fuzhou,
China).
Drugs and reagents
QC (Fujian, China, FDA approval No.: Z09104065) is a
capsule of five Chinese products, as listed in Table I, that was provided by the Academy
of Pharmacology of Fujian University of Traditional Chinese
Medicine. The drug powder inside the capsule was dissolved in
distilled water and stored at 4°C. Testosterone propionate
injection solution (25 mg/ml) was obtained from Shanghai GM
Pharmaceutical Co., Ltd. (Shanghai, China; batch number:
H31020524). Finasteride was obtained from Merck (Hangzhou, China;
batch number: J20050041). TRIzol reagent was purchased from
Invitrogen (Carlsbad, CA, USA). SuperScript II reverse
transcriptase was obtained from Promega (Madison, WI, USA). Rat EGF
ELISA kit was obtained from Shanghai Xitang Biological Technology
Ltd. (Shanghai, China). EGF, EGFR, p-STAT3, Bcl-2 and cyclin D1
primary antibodies, secondary antibody, streptavidin-peroxidase
(SP) and 3,3’-diaminobenzidine (DAB) were purchased from Bohai
Biotechnology Development Co., Ltd. (Shijiazhuang, China). All
other chemicals, unless otherwise stated, were obtained from
Sigma-Aldrich (St. Louis, MO, USA).
Construction of the rat BPH model and
drug administration
The rat model of BPH was induced by the subcutaneous
injection of testosterone propionate following castration. The
scrota of 50 rats from a total 60 male SD rats were removed. One
week after surgery, the rats were randomly divided into six groups
(n=10), termed the normal group (saline 10 ml/kg), model group
(saline 10 ml/kg), finasteride group (0.5 mg/kg) and three QC
groups in which rats were orally treated with 2.25, 4.5 or 9 g/kg
of QC. The rats in the treated groups received the corresponding
drug dose via gastrogavage, together with a subcutaneous injection
of testosterone propionate (5 mg/kg), daily for 28 days. The body
weight (BW) was measured once per week.
Sample collection
At the end of the experiments, the animals were
weighed, anesthetized with ketamine-diazepam by intraperitoneal
injection and the blood was obtained aseptically from the abdominal
aorta. The blood-containing tubes were allowed to stand at room
temperature for 2 h and sera were obtained by centrifuging at 3000
× g for 20 min in 4°C and stored in −80°C. The intact prostate
tissue was dissociated and removed with caution. The prostate
weight (PW) and prostatic volume (PV) were measured and the
prostatic index (PI) was calculated as: PW/BW×100. One piece of
prostate tissue was collected from the same position and fixed with
10% formalin or stored in liquid nitrogen for further analyses.
Histopathological examination
Small sections of the prostatic specimens were fixed
with 10% buffered formalin for 24 h. The samples were then
paraffin-embedded, sectioned and stained with hematoxylin and eosin
(H&E). Histopathological changes were observed under a light
microscope.
Detection of EGF level in serum by
ELISA
The serum level of EGF was measured using an ELISA
kit according to the manufacturer’s instructions. The wells were
coated with 100 μl capture antibody diluted in coating
buffer. The plate was sealed and incubated overnight at 4°C. After
three washes, the wells were blocked with 200 μl assay
diluents at room temperature for 1 h, followed by another three
washes. Diluted EGF standard (100 μl) and test samples were
added and incubated for 2 h at room temperature. After repeated
washing, the substrate (O-Phenylenediamine, OPD) was added and
incubated for 20 min at room temperature and the absorbance was
measured at 450 nm using an ELISA reader (Model ELX800; BioTek,
Winooski, VT, USA).
RNA extraction and RT-PCR analysis
Total RNA was isolated from fresh prostate tissues
with TRIzol reagent. Oligo (dT)-primed RNA (1 μg) was
reverse-transcribed with SuperScript II reverse transcriptase
(Promega) according to the manufacturer’s instructions. The
obtained cDNA was used to determine the mRNA levels of EGF, EGFR,
Bcl-2 and cyclin D1 by PCR with Taq DNA polymerase (Fermentas,
Burlington, Canada). β-actin was used as an internal control. The
sequences of the primers used for amplification of EGF, EGFR,
Bcl-2, cyclin D1 and β-actin transcripts were as follows: EGF,
forward: 5′-GCC AAT GCT CAG AAG GCT AC-3′ and reverse: 5′-CGT AAG
TCT CGG TGC TGA CA-3′ (temperature=55°C, 361 bp); EGFR, forward:
5′-TCG GTG CTG TGC GAT TTA-3′ and reverse: 5′-TTT CTG GCA GTT CTC
CTC-3′ (temperature=50°C, 194 bp); Bcl-2, forward: 5′-GGT GGT GGA
GGA ACT CTT CA-3′ and reverse: 5′-GAG CAG CGT CTT CAG AGA CA-3′
(temperature=56°C, 268 bp); cyclin D1, forward: 5′-GGA GCA GAA GTG
CGA AGA-3′ and reverse: 5′-GGG TGG GTT GGA AAT GAA-3′
(temperature=57°C, 394 bp); β-actin, forward: 5′-ACT GGC ATT GTG
ATG GAC TC-3′ and reverse: 5′-CAG CAC TGT GTT GGC ATA GA-3′
(temperature=55°C, 453 bp). The samples were analyzed by gel
electrophoresis (1.5% agarose). The DNA bands were examined using a
Gel Documentation system (Bio-Rad, Hercules, CA, USA; Model Gel Doc
2000).
Immunohistochemical (IHC) analysis
A 0.5×0.5×0.1 cm block of tissue was collected from
the lateral lobe of the prostate gland of each rat. Tissue blocks
were rinsed with phosphate-buffered saline (PBS), fixed with 10%
formaldehyde for 12–24 h, embedded in paraffin, archived and
sliced. The paraffin sections were used for EGF, EGFR, p-STAT3,
Bcl-2 and cyclin D1 IHC staining. The primary antibodies employed
were polyclonal rabbit anti-rat EGF, EGFR, p-STAT3, Bcl-2 and
cyclin D1. PBS was used to replace the primary antibody as a
negative control. Color was developed using DAB chromogen, as per
the manufacturer’s instructions. After staining, five high-power
fields (magnification, ×400) were randomly selected in each slide,
and the average proportions of positive cells in each field were
counted using the true color multi-functional cell image analysis
management system (Image-Pro Plus, Media Cybernetics, Rockville,
MD, USA).
Statistical analysis
Data are expressed as mean ± standard deviation
(SD). The comparisons between the six groups were performed using
the Kruskal-Wallis test and the comparisons between two groups were
conducted using the Mann-Whitney U test. For categorical variables,
data are presented by number and percentage. The associations
between categorical variables were tested using Fisher’s exact
test. P<0.05 was considered to indicate a statistically
significant result. Statistical analyses were performed using SPSS
15.0 statistics software (SPSS Inc, Chicago, IL, USA).
Results
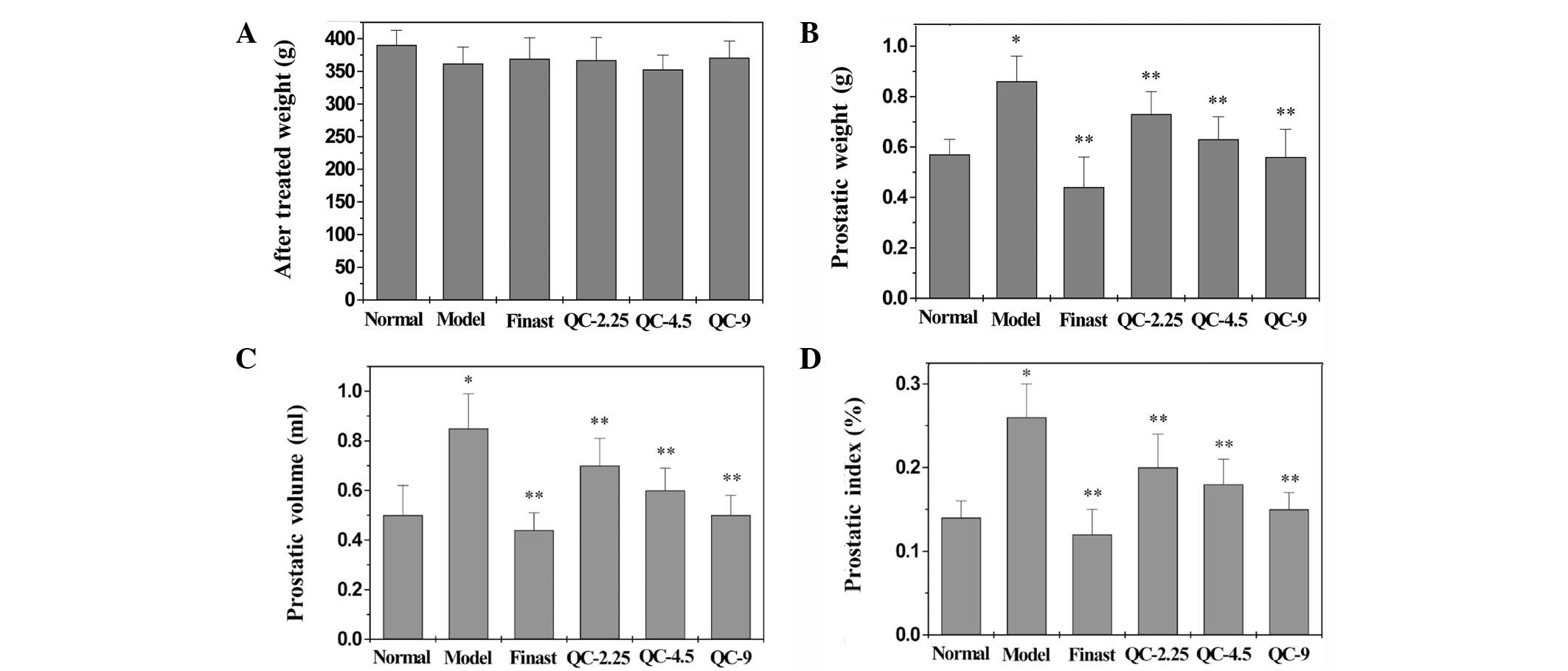
Effects of QC on BW, PW, PV and PI
We monitored whether QC or finasteride treatment
caused any adverse health effects during the study by measuring BW
gain, which is a relevant and widely used primary indicator for
assessing the gross toxicity of drugs in intervention studies. As
shown in Fig. 1A, oral
administration of QC and finasteride did not affect BW gain
(P>0.05, versus control group), which was consistent with our
previous study of toxicity (32).
In the model group, the PW, PV and PI increased significantly
compared with those in the normal group (P<0.05; Fig. 1B–D), and remained elevated for a
continuous period of 28 days, indicating successful model
construction. However, treatment with finasteride or different
doses of QC significantly reduced the PW, PV or PI in BPH rats
compared with those in the model group (P<0.05; Fig. 1B–D). These findings suggest that QC
has comparable efficacy to finasteride in the treatment of BPH in
rats, without any apparent signs of toxicity.
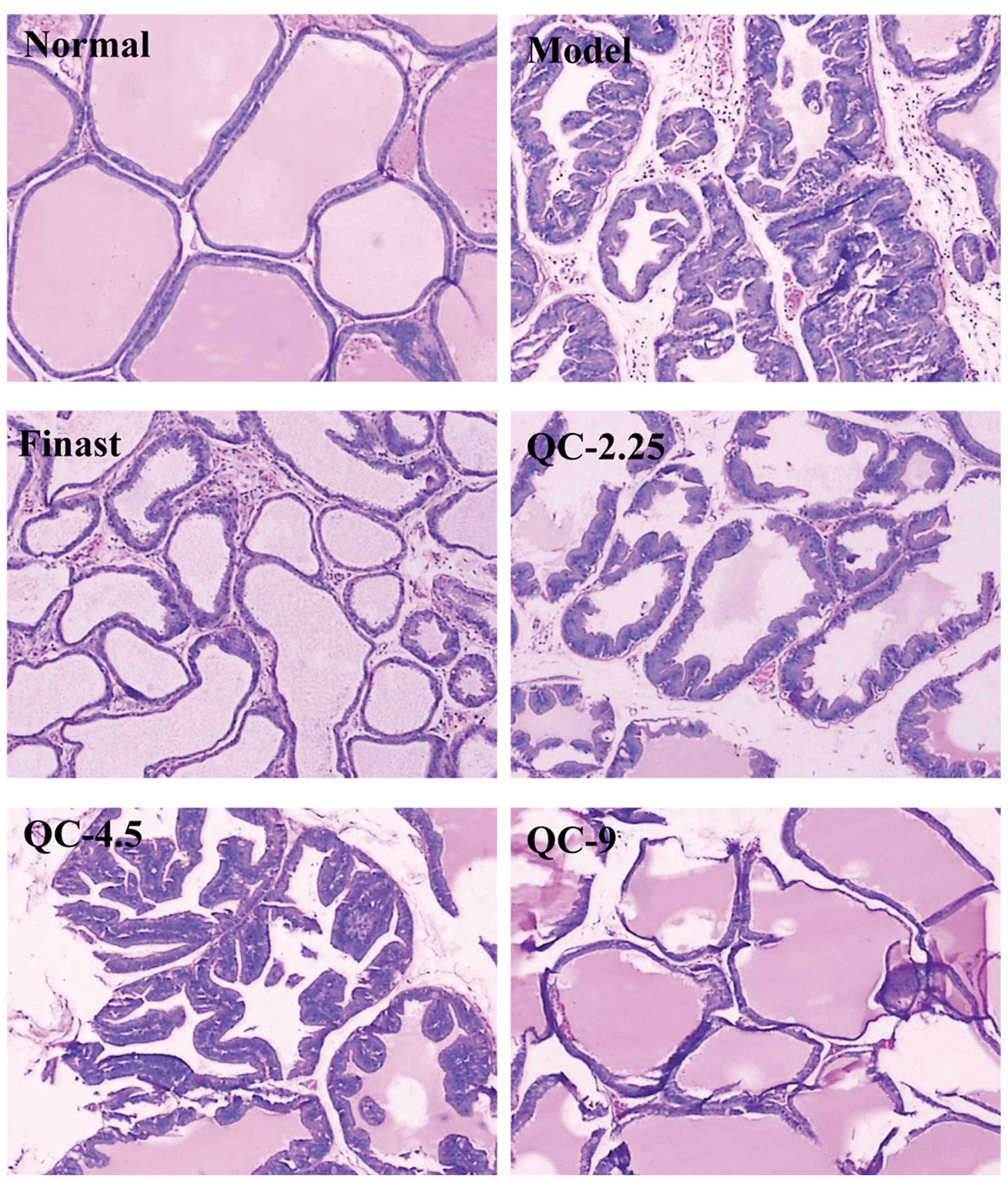
QC treatment ameliorates the damage to
prostate tissue
In the normal group, low columnar epithelial cells
were arranged as a single layer forming a secretary lumen which was
filled with thin acidophilic materials. In the model group, the
epithelial cells proliferated markedly to develop excessive glands
and cells were arranged as multiple unorganized layers. In all
treated groups, the cell proliferation and gland development were
significantly inhibited. In addition, QC treatment ameliorated the
histopathological changes in a dose-dependent manner (Fig. 2).
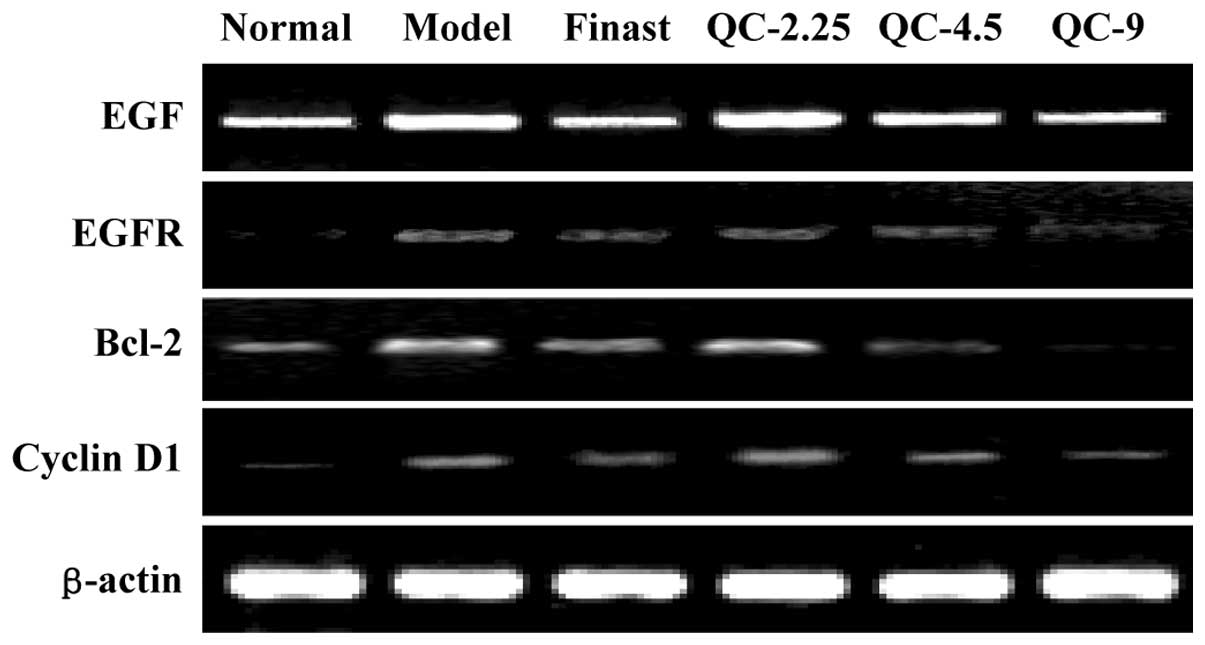
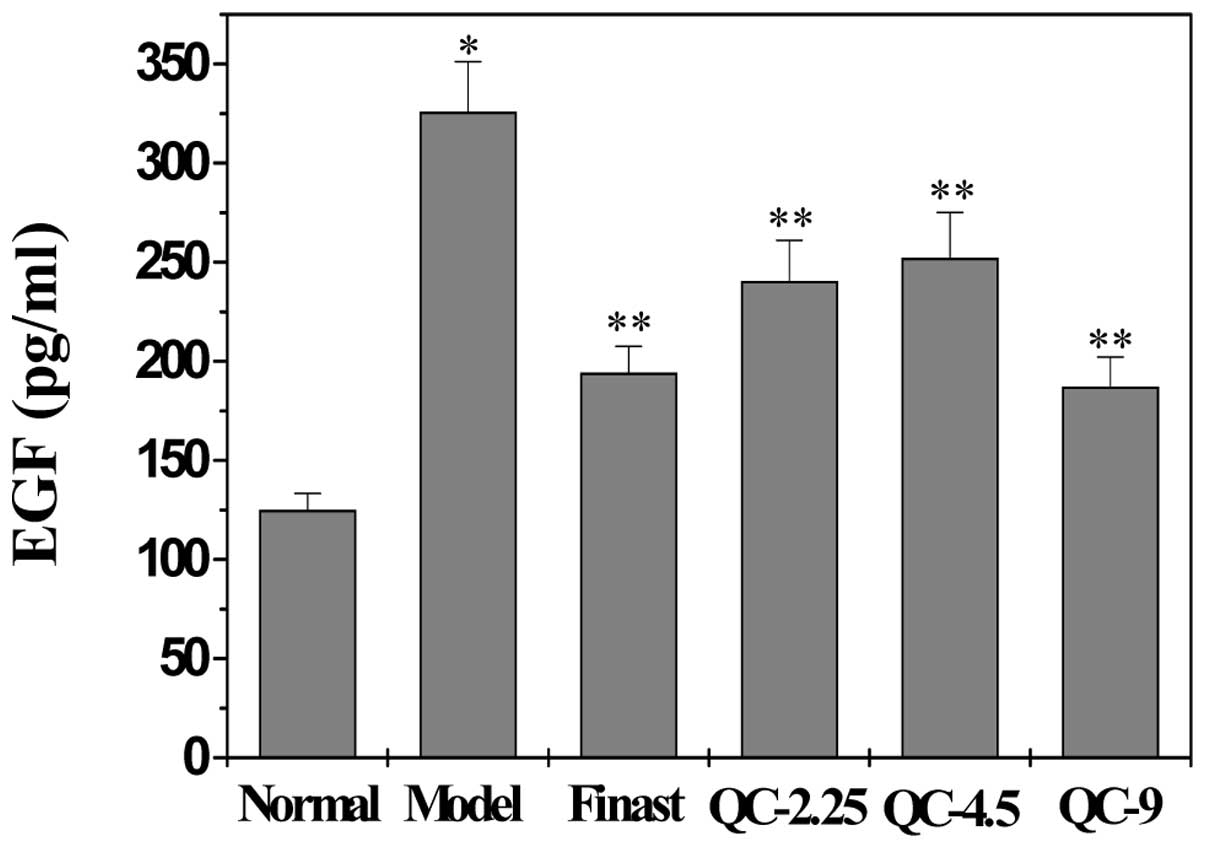
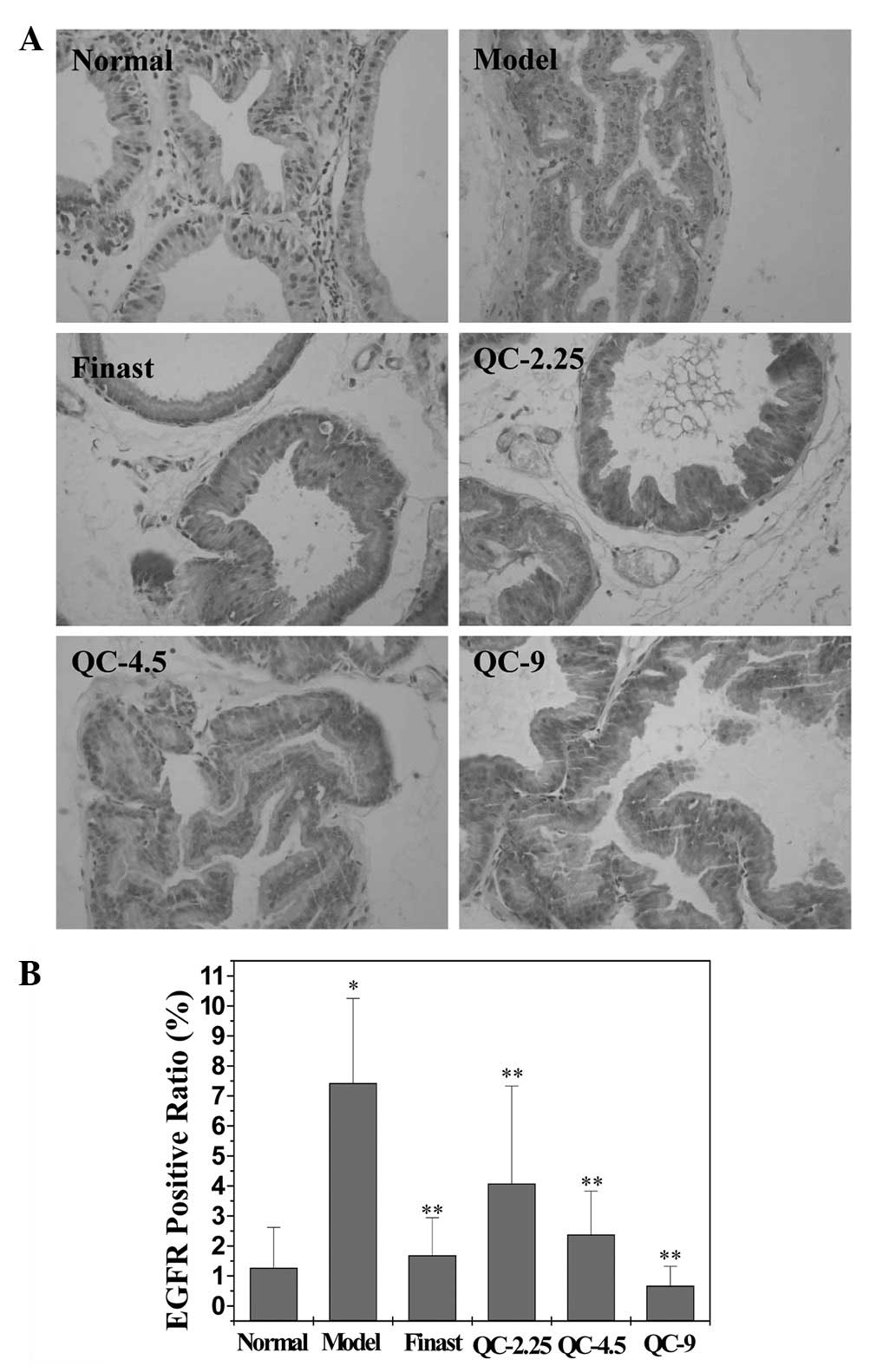
QC downregulates the expression of EGF
and EGFR in BPH rats
The mRNA or protein expression of EGF and EGFR in
the prostatic tissue of BPH rats was detected using RT-PCR or IHC
analysis, respectively, and the secretion level of EGF in serum was
examined by ELISA. The results of the RT-PCR assay showed that the
mRNA expression levels of EGF and EGFR in the model group were
significantly increased, compared with those in the normal group
(P<0.05), and these elevations were attenuated by treatment with
finasteride or different doses of QC (Fig. 3). Data from IHC analysis and ELISA
showed that the pattern of protein expression of EGF and EGFR was
similar to that of their respective mRNA levels (Figs. 4–6).
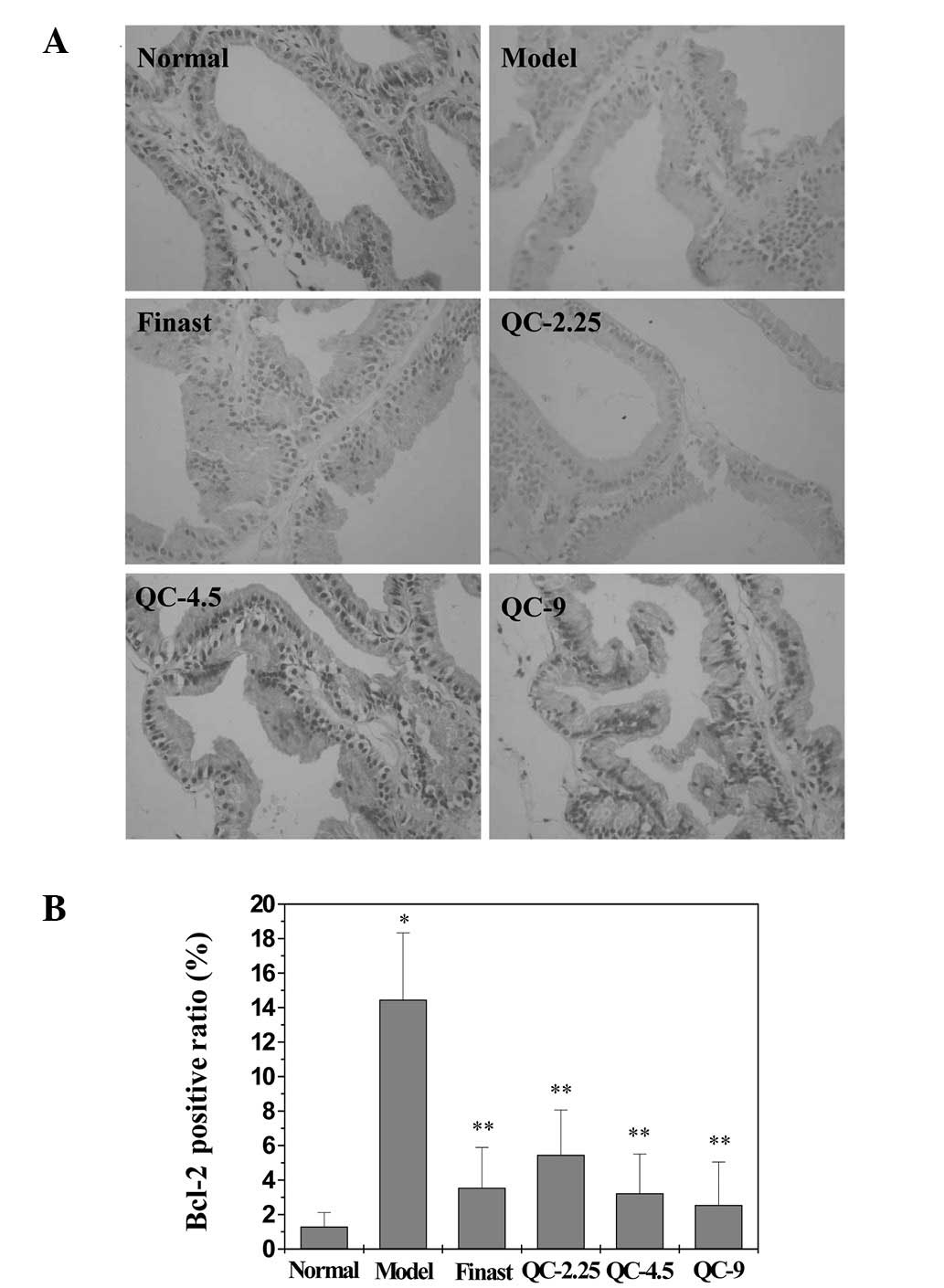
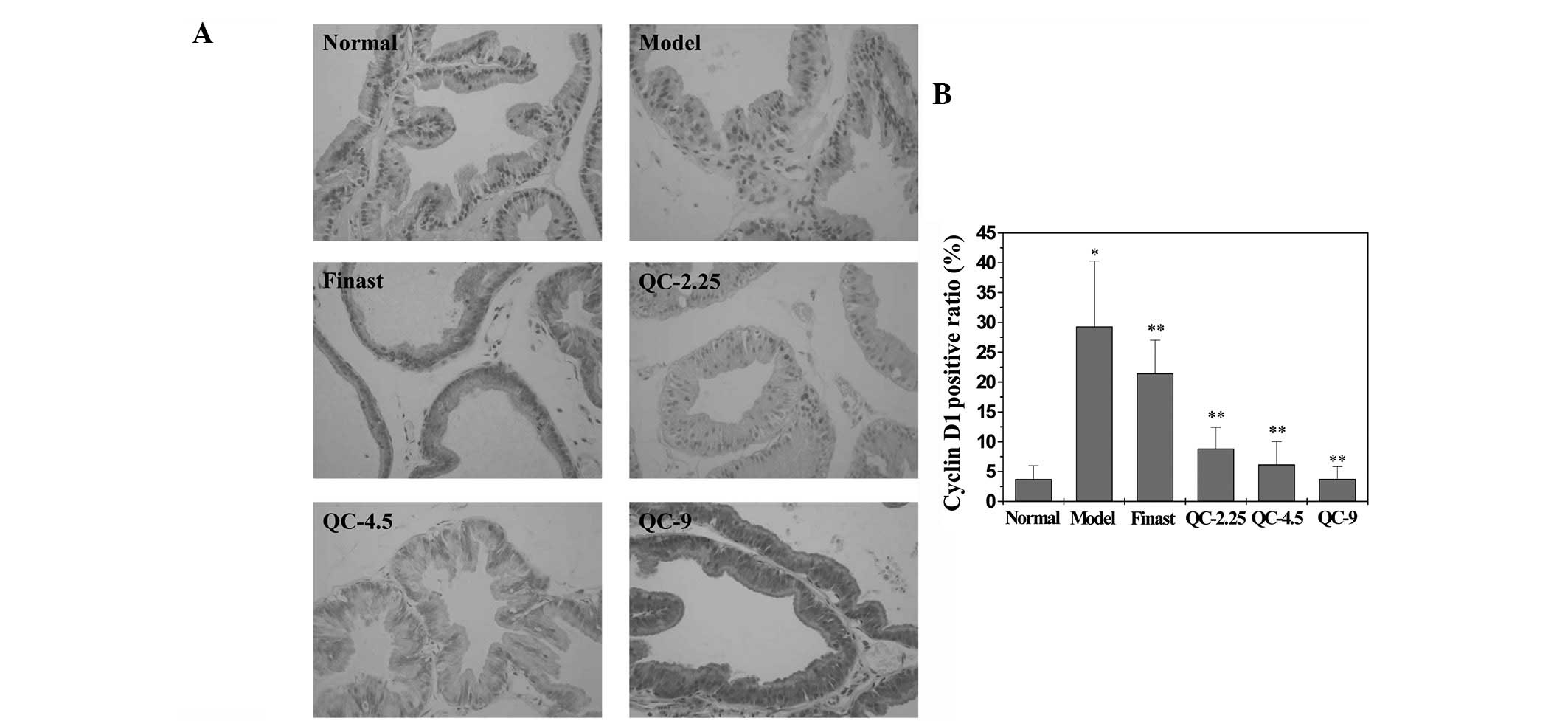
QC suppresses the STAT3 signaling pathway
in BPH rats
STAT3 phosphorylation in the prostatic tissue of BPH
rats was determined using an IHC assay. As shown in Fig. 7, the positive expression level of
phosphorylated STAT3 (p-STAT3) in the model group was markedly
increased compared with that in the normal group (P<0.05), but
treatment with finasteride or QC significantly inhibited the effect
of BPH model construction on the STAT3 phosphorylation. The
expression of cyclin D1 and Bcl-2, two important target genes of
STAT3 pathway, was also detected by RT-PCR and IHC analysis. As
shown in Figs. 3, 8 and 9,
finasteride or QC treatment profoundly inhibited the expression of
cyclin D1 and Bcl-2 induced by the construction of the BPH model,
at the transcriptional and translational levels.
Discussion
Although surgical therapy is of superior efficacy
for aged patients and those with severe heart, lung and kidney
dysfunction, pharmacotherapy remains the modality of choice for BPH
treatment. Pharmacotherapy may be divided into three groups,
including α-blockers, 5α-reductase inhibitors and alternative
therapies. The α-blockers inhibit α-adrenergic receptors, thereby
relaxing smooth muscle in the prostate and the bladder neck and
alleviating the blockage of urine flow. The 5α-reductase inhibitors
suppress 5α-reductase, thereby inhibiting DHT production and the
enlargement of the prostate. However, both α-blockers and
5α-reductase inhibitors induce unfavorable side effects, including
orthostatic hypotension, decreased libido and ejaculatory or
erectile dysfunction (18–22). Therefore, the investigation of
natural products for BPH treatment is important, since natural
medicines usually display fewer adverse effects and have long been
used clinically to treat various diseases, including BPH (23,24).
QC is a traditional Chinese medicine formulation
composed of rhubarb, leech, astragalus, achyranthes and Dodder. QC
has been used clinically in China for several years, displaying a
significant efficacy in BPH treatment (26–30).
However, the mechanism of its anti-BPH activity remains largely
unknown.
In the present study, we demonstrated that QC
significantly reduced the PI and alleviated the prostatic
hyperplasy in BPH rats, indicating its anti-BPH efficacy. In
addition, the administration of QC did not affect the BW of the
rats, suggesting that QC has no apparent toxicity. Although the
cause of BPH is not well understood, it is generally considered
that excessive cell proliferation and/or reduction of cell
apoptosis, usually resulting from the abnormal activation of the
EGF/STAT3 pathway, plays a critical role in the development of BPH.
EGF exerts its biological function through binding to its specific
receptor, EGFR, that is mainly present in epithelial cells on the
basal layer of the prostate gland. It has been shown that the
expression of EGF and EGFR is increased in the prostatic tissue of
patients with BPH (4,8), suggesting that the overexpression of
EGF and EGFR participates in the epithelial cell proliferation
process in patients with BPH. In addition to directly promoting
proliferation through binding to EGFR, EGF inhibits the
TGF-β-mediated apoptosis of prostate cells (33). Our data indicated that QC treatment
may significantly decrease the serum level of EGF in BPH rats, as
well as downregulate the mRNA and protein levels of EGF and EGFR in
prostatic tissue.
STAT3 is a member of the STAT family of
transcription factors. STAT3 is activated by numerous growth
factors and cytokines, including EGF (27). Activation of STAT3 activates a
variety of genes, including Bcl-2 and cyclin D1 (9,34–36).
Bcl-2 is an apoptosis inhibitory factor which inhibits programmed
cell death (7). Bcl-2 is present
in normal basal epithelial cells of the prostate gland and is
expressed at significantly higher levels in BPH compared with
normal prostatic tissue. Cyclin D1 is a key regulatory protein
promoting cell cycle progression from the G1 to the S phase. The
IHC data in this study showed that QC lowers the expression levels
of p-STAT3, Bcl2 and cyclin D1 in the prostatic tissues of BPH
rats.
In summary, we report that inhibition of the
EGF/STAT3 pathway may be one of the mechanisms by which QC treats
BPH.
Abbreviations:
|
QC
|
Qianliening capsule
|
|
BPH
|
benign prostatic hyperplasia
|
|
EGF
|
epidermal growth factor
|
|
STAT3
|
signal transducer and activator of
transcription 3
|
|
PW
|
prostatic weight
|
|
PV
|
prostatic volume
|
|
PI
|
prostatic index
|
|
SP
|
streptavidin-peroxidase
|
Acknowledgements
This study was supported by the Nature
Science Foundation of China (81173433, 81072927), the Natural
Science Foundation of Fujian Province of China (2010J01199,
2009J01169) and the Research Foundation of Education Bureau of
Fujian Province of China (JA09128).
References
|
1.
|
Paolone DR: Benign prostatic hyperplasia.
Clin Geriatr Med. 26:223–239. 2010. View Article : Google Scholar
|
|
2.
|
Roehrborn CG: Male lower urinary tract
symptoms (LUTS) and benign prostatic hyperplasia (BPH). Med Clin
North Am. 95:87–100. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
3.
|
Gat Y, Gornish M, Heiblum M and Joshua S:
Reversal of benign prostate hyperplasia by selective occlusion of
impaired venous drainage in the male reproductive system: novel
mechanism, new treatment. Androl. 40:273–281. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
4.
|
Xie Q, Wang H, Lin F and Liao Y:
Abnormality of growth regulatory factors in benign prostatic
hyperplasia. Chin J Urol. 22:520–522. 2001.(In Chinese).
|
|
5.
|
Steiner MS: Review of peptide growth
factors in benign prostatic hyperplasia and urological malignancy.
J Urol. 153:1085–1096. 1995. View Article : Google Scholar : PubMed/NCBI
|
|
6.
|
Li Y, Fang Y, Xu Youqi, Li Q, Deng X and
Jiang J: Role of the epidermal growth factor receptor in human
benign hyperplastic prostate tissue. J Clin Urol. 11:199–201.
1996.(In Chinese).
|
|
7.
|
Jia B, Tang Z, Li WM and Cai WQ: The
effects of epidermal growth factor on the expression of Bcl-2, Bax
and c-myc in mice prostate cells. Chin J Gerontol. 27:251–252.
2007.(In Chinese).
|
|
8.
|
Lin JM, Hong ZF, Zhou JH, Zhuang QC, Zhao
JY and Zhou HT: Expression of growth factor related to angiogenesis
on prostatic hyperplasia in rats. J Fujian Univ Tradit Chin Med.
18:63–66. 2008.(In Chinese).
|
|
9.
|
Darnell JE Jr: STATs and gene regulation.
Science. 277:1630–1635. 1997. View Article : Google Scholar : PubMed/NCBI
|
|
10.
|
Hong ZF: Candidate targets for research on
benign prostatic hyperplasia. Zhonghua Nan Ke Xue. 14:771–774.
2008.(In Chinese).
|
|
11.
|
Haura EB, Turkson J and Jove R: Mechanisms
of disease: Insights into the emerging role of signal transducers
and activators of transcription in cancer. Nat Clin Pract Oncol.
2:315–324. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
12.
|
Catlett-Falcone R, Landowski TH, Oshiro
MM, Turkson J, Levitzki A, Savino R, Ciliberto G, Moscinski L,
Fernández-Luna JL, Nuñez G, Dalton WS and Jove R: Constitutive
activation of Stat3 signaling confers resistance to apoptosis in
human U266 myeloma cells. Immunity. 10:105–115. 1999. View Article : Google Scholar : PubMed/NCBI
|
|
13.
|
Karni R, Jove R and Levitzki A: Inhibition
of pp60c-Src reduces Bcl-XL expression and reverses the transformed
phenotype of cells overexpressing EGF and HER-2 receptors.
Oncogene. 18:4654–4662. 1999. View Article : Google Scholar
|
|
14.
|
Coqueret O and Gascan H: Functional
interaction of STAT3 transcription factor with the cell cycle
inhibitor p21WAF1/CIP1/SDI1. J Biol Chem. 275:18794–18800. 2000.
View Article : Google Scholar : PubMed/NCBI
|
|
15.
|
Bienvenu F, Gascan H and Coqueret O:
Cyclin D1 represses STAT3 activation through a Cdk4-independent
mechanism. J Biol Chem. 276:16840–16847. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
16.
|
Roehrborn CG, Nuckolls JG, Wei JT and
Steers W; BPH Registry and Patient Survey Steering Committee: The
benign prostatic hyperplasia registry and patient survey: study
design, methods and patient baseline characteristics. BJU Inter.
100:813–819. 2007. View Article : Google Scholar
|
|
17.
|
Black L, Naslund MJ, Gilbert TD Jr, Davis
EA and Ollendorf DA: An examination of treatment patterns and costs
of care among patients with benign prostatic hyperplasia. Amer J
Manag Care. 12(4 Suppl): S99–S110. 2006.PubMed/NCBI
|
|
18.
|
MacDonald R and Wilt TJ: Alfuzosin for
treatment of lower urinary tract symptoms compatible with benign
prostatic hyperplasia: A systematic review of efficacy and adverse
effects. Urology. 66:780–788. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
19.
|
Roehrborn CG: Efficacy and safety of
once-daily alfuzosin in the treatment of lower urinary tract
symptoms and clinical benign prostatic hyperplasia: a randomized,
placebo-controlled trial. Urology. 58:953–959. 2001. View Article : Google Scholar
|
|
20.
|
Djavan B and Marberger M: A meta-analysis
on the efficacy and tolerability of α1-adrenoceptor antagonists in
patients with lower urinary tract symptoms suggestive of benign
prostatic obstruction. Eur Urol. 36:1–13. 1999.
|
|
21.
|
Gormley GJ, Stoner E, Bruskewitz RC,
Imperato-McGinley J, Walsh PC, McConnell JD, Andriole GL, Geller J,
Bracken BR and Tenover JS: The effect of finasteride in men with
benign prostatic hyperplasia. The Finasteride Study Group. N Engl J
Med. 327:1185–1191. 1992. View Article : Google Scholar : PubMed/NCBI
|
|
22.
|
Roehrborn C, Boyle P, Nickel JC, Hoefner K
and Andriole G; ARIA3001 ARIA3002 and ARIA3003 Study Investigators:
Efficacy and safety of a dual inhibitor of 5-alpha-reductase types
1 and 2 (dutasteride) in men with benign prostatic hyperplasia.
Urology. 60:434–441. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
23.
|
Boyle P, Robertson C, Lowe F and Roehrborn
C: Meta-analysis of clinical trials of permixon in the treatment of
symptomatic benign prostatic hyperplasia. Urology. 55:533–539.
2000. View Article : Google Scholar : PubMed/NCBI
|
|
24.
|
Wilt T, Ishani A, MacDonald R, Stark G,
Mulrow C and Lau J: Beta-sitosterols for benign prostatic
hyperplasia. Cochrane Database of Syst Rev. (2):
CD0010432000.PubMed/NCBI
|
|
25.
|
Wilt T, Ishani A, Mac Donald R, Rutks I
and Stark G: Pygeum africanum for benign prostatic
hyperplasia. Cochrane Database of Syst Rev. (1):
CD0010442002.PubMed/NCBI
|
|
26.
|
Zhou J, Lin J, Xu W, Zhong X, Xie J and
Hong Z: Effects of Qianliening capsule on the expression of IL-10
and TNF-α in benign prostatic hyperplasia. Chin Arch Tradit Chin
Med. 28:2657–2569. 2010.(In Chinese).
|
|
27.
|
Zhou JH, Hong ZF, Lin JM, Zhao JY and Zhou
HT: Effect of Qianliening granule on experimental hyperplasia of
prostate. J Fujian Univ Tradit Chin Med. 18:45–47. 2008.(In
Chinese).
|
|
28.
|
Zhou HT, Lin JM, Zhao JY, Zhou JH and Hong
ZF: Inhibition effects of qianliening granule on IL-1β and its mRNA
expression in model rats. J Fujian Univ Tradit Chin Med. 20:21–24.
2010.
|
|
29.
|
Zhou J, Lin J, Xu W, Zhong X, Zheng Y,
Hong Z and Peng J: Qianliening capsule treats benign prostatic
hyperplasia through regulating the expression of sex hormones,
estrogen receptor and androgen receptor. Afr J Pharm Pharmacol.
6:173–180. 2012. View Article : Google Scholar
|
|
30.
|
Zhong X, Lin J, Zhou J, Xu W, Hong Z and
Peng J: Qianliening capsule treats benign prostatic hyperplasia
(BPH) by down-regulating the expression of PCNA, CyclinD1 and CDK4.
Afr J Biotechnol. 11:7731–7737. 2012.
|
|
31.
|
National Advisory Committee for Laboratory
Animal Research. Guidelines on the Care and Use of Animals for
Scientific Purposes. 2004
|
|
32.
|
Zheng HY, Xu W, Lin JM, Li H, Zhou JH and
Hong ZF: Toxicological studies on qianliening capsule. J Zhejiang
Univ Tradit Chin Med. 35:63–65. 2011.(In Chinese).
|
|
33.
|
Ilio KY, Sensibar JA and Lee C: Effect of
TGF-beta 1, TGF-alpha, and EGF on cell proliferation and cell death
in rat ventral prostatic epithelial cells in culture. J Androl.
16:482–490. 1995.PubMed/NCBI
|
|
34.
|
Peng J, Chen Y, Lin J, Zhuang Q, Xu W,
Hong Z and Sferra TJ: Patrinia scabiosaefolia extract
suppresses proliferation and promotes apoptosis by inhibiting the
STAT3 pathway in human multiple myeloma cells. Mol Med Report.
4:313–318. 2011.
|
|
35.
|
Ball S, Li C, Li PK and Lin J: The small
molecule, LLL12, inhibits STAT3 phosphorylation and induces
apoptosis in medulloblastoma and glioblastoma cells. PLoS One.
6:e188202011. View Article : Google Scholar : PubMed/NCBI
|
|
36.
|
Masuda M, Suzui M, Yasumatu R, Nakashima
T, Kuratomi Y, Azuma K, Tomita K, Komiyama S and Weinstein IB:
Constitutive activation of signal transducers and activators of
transcription 3 correlates with cyclin D1 overexpression and may
provide a novel prognostic marker in head and neck squamous cell
carcinoma. Cancer Res. 62:3351–3355. 2002.PubMed/NCBI
|