Introduction
Acute ischemic cerebrovascular disease is the most
common of the nervous vascular diseases. According to the
Framingham epidemiological studies, 65% of stroke cases result from
an occlusion of the middle cerebral artery (1). Thus, the ischemia model created
through middle cerebral artery occlusion (MCAO) is often employed
in studies concerning cerebral ischemia diseases. The suture method
is more widely used than other methods (2,3); it
avoids opening the skull, leads to less injury, indicates the
precise location of the occlusion and controls the duration of
ischemia and reperfusion (4).
Researchers in this field are refining a suitable method by
modifying the end of the line, implantation depth and occlusion
time to improve the MCAO model. However, the extent of cerebral
infarction remains uncertain due to the inter-individual anatomical
variety of cerebrovascular structures. The success rate and
reliability of the model are affected by numerous factors,
including strain, gender, weight, age, incision, ligation, quality
and hardness of the materials, shape of the end of the line and the
anesthetics used. Currently, there are no systematic studies on the
size of the nylon line and particularly on the location of the neck
incision and the vessel ligation. The tip diameter of the suture
varies largely from 0.18 to 0.30 mm (5–7). The
present study was performed to systematically demonstrate the
effects of suture diameter (type 1.0, 2.0 and 3.0, suture diameters
ranging from 0.16 to 0.28 mm), the arterial location of the
ligation and the surgical approaches. The focal MCAO model was used
in an effort to identify a simple and reliable focal cerebral
ischemia model for use in clinical and experimental studies.
Subjects and methods
Animals
The animals were purchased from the Vital River
Laboratories (VRL; Beijing, China). The rats were kept in isolators
at a temperature of 23±20°C and a relative humidity of 55±10%, on a
12 h dark/light cycle (06:00–18:00) with air exchanged ≥12 times
per hour.
The animals were treated humanely, according to the
Animal Ethics Procedures and Guidelines of the People’s Republic of
China and the study was approved by Anhui Medical University.
Experimental design
A total of 84 adult male Sprague-Dawley rats
weighing 250–300 g were randomly divided into three groups with 28
rats each according to the type of nylon line: Group A (type 1.0;
suture diameter, 0.16–0.17 mm; and tip, 0.21–0.22 mm); group B
(type 2.0; suture diameter, 0.22–0.23 mm; and tip, 0.27–0.28 mm);
and group C (type 3.0, suture diameter, 0.28–0.29 mm; and tip,
0.33–0.34 mm). The animals in each group were then subdivided into
two subgroups: In the 1st groups (A1, B1 and C1) the nylon line was
inserted through the common carotid artery (CCA); and in the 2nd
group (A2, B2 and C2) the nylon line was inserted through the
external carotid artery (ECA). In each of the subgroups, half of
the animals were subjected to incisions in the middle of the neck
and the other half were subjected to lateral incisions (subgroups 1
and 2).
Apparatus and reagents
The nylon line was purchased from Seaguar (Tokyo,
Japan), the 2,3,5-triphenyltetrazolium chloride (TTC) was purchased
from Sigma (St. Louis, MO, USA) and the electronic vernier caliper
was purchased from Hangzhou Meka Tools Co., Ltd (Hangzhou,
China).
Occluding suture preparation
Three types of nylon lines were prepared according
to the method reported by Ma et al(8) with minor modifications. A 6–10 cm
line was then curved by knotting it at a site between one-third and
one-half of the length. A 170° angles was formed automatically
between the two sides of this knot, 20 and 10 mm lateral to the
knot. The site 5 mm from the end of the 20-mm segment was embedded
in silica gel. The diameter of the tip was precisely controlled by
an electronic vernier caliper to fit one of the three size ranges:
0.21–0.22 mm, 0.27–0.28 mm or 0.33–0.34 mm. The prepared occluding
sutures were sterilized by UV for storage and treated sequentially
with iodophor, alcohol and saline prior to use.
Operation
Incision and insertion
The two approaches used in this study were those of
anterior middle and lateral incisions with the line inserted
through one of two arteries, the right ECA or the right CCA,
respectively. All male SD rats were anesthetized with 10% chloral
hydrate. With the use of aseptic surgical techniques, catheters
were inserted into the right femoral artery and vein to measure the
arterial blood pressure (MABP) and arterial blood gases (pH,
PaCO2 and PaO2). The rectal temperature was
maintained at 36.5–37.5°C using an electric blanket during the
surgery. These physiological parameters were monitored prior to,
during and subsequent to the MCAO.
ECA insertion
This method was based on the study by Longa et
al(9) with slight
modifications. The animals were anesthetized by an intraperitoneal
injection of 10% chloral hydrate (0.4 ml/100 g) following a 24-h
fast. A 20-mm middle or lateral incision was made in the neck
following skin preparation, sterilization and exposing neck fully.
The subcutaneous tissue was dissected bluntly to expose the right
CCA and to isolate the internal carotid artery (ICA), ECA and vagus
nerve along the CCA. The ECA was ligated at its first bifurcation
and a small opening was made on the proximal ECA at the site that
was 4–5 mm distal to the CCA bifurcation, subsequent to temporarily
blocking the blood flow in the CCA and ICA with an artery clip. A
silicone-coated nylon suture was introduced into the ECA through
the small opening. A 6-0 silk suture was placed loosely around the
ECA near the small opening to avoid blood backflow through the ECA
and maintain the mobility of the intraluminal nylon suture. Caution
was taken so as not to traumatize the arterial wall. The ECA was
cut off between the small opening and the first nylon tie, then the
artery clip was withdrawn. The ECA was pulled in the direction of
the heart and the ECA and ICA were arranged in a line and the
suture was continuously pushed into the ICA until it met
resistance. The 6-0 silk suture was tightened around the ECA to fix
the occluding suture. Typically, an 18±2 mm length of line is
pushed into the vessels (10). If
the length is <15 mm, the occluding suture must be pulled out
and inserted again. The extravascular nylon suture was cut off with
micro scissors. The incision was sutured with a 3-0 silk suture and
then the rat was placed in a 35°C nursing box to recover from the
anesthesia prior to being returned to the cage.
CCA insertion
This method was based on the study by Engel et
al(11) with minimal
modifications. The surgical preparation was the same as previously
described. Following the exposure of the CCA, ICA, ECA and vagus
nerve, the ECA was ligated at its first bifurcation. The CCA was
then ligated 5 mm from its bifurcation to the ECA and ICA,
following the separation of the ICA and vagus nerve and the
temporary blockade of the blood flow in the ICA with an artery
clip. A small hole was opened in the CCA 2–4 mm from the
bifurcation and the occluding suture was inserted into the ICA. A
6-0 silk suture was loosely tied around the CCA to avoid any blood
backflow from the small opening. The artery clip was removed and
the blood flow was released, then the nylon suture was pushed
forward until it met resistance. The loose silk suture was
lightened to fix the intraluminal nylon suture. In this procedure,
the 18±2 mm nylon suture was pushed into the vessels to avoid
having to pull out the nylon suture embolism and insert it
again.
Evaluation index and method
Neurological deficit function
The severity of the neurological deficit was
assessed at 4, 8, 24, 48 and 72 h post-surgery according to the
Zea-Longa neurological deficit score. A score of 0 was given to
normal animals with no signs of neurological deficit. A score of 1
was given to those with mild neurological disorders, including
dysfunction in stretching the left anterior limb. A score of 2 was
given to animals that intorted the left anterior limb and adducted
the shoulder when they were lifted by the tails and also turned
left when they walked. A score of 3 was given to animals with
neurologic abnormalities so severe that they fell to the left side
when they walked. Rats with a score of 4 did not walk spontaneously
and had a depressed level of consciousness.
Detecting cerebral ischemia volume and
edema
All surviving rats were sacrificed 72 h post-surgery
in accordance with a previous study (12). The brains were dissociated on ice
and boxed into a special brain mold following the depletion of the
cerebellum and brain stem. The brains were cut into a series of
2-mm thick coronal slices and incubated in 1% TTC for 20 min at
37°C and then in 4% paraformaldehyde for 30 min. The
cross-sectional area of the infarction and the non-infarcted tissue
in each brain slice was measured using Image J analysis software
(version 1.6 NIH). The infarct volume was indirectly calculated
according to the following formula: Infarct volume = (Σ infarct
area × thickness) / (Σ whole area × thickness) × 100. Extent of
edema = (volume of right hemisphere - volume of left hemisphere /
volume of left hemisphere) × 100. To calculate the relative
standard deviation (RSD), first the whole brain was weighed (Tm),
then the infarcted region was dissociated and weighed (Pm). The RSD
of the infarction = (Pm / Tm) × 100. Success rate = number of
successful models / total number of models × 100.
Statistical analysis
Continuous variables are shown as the mean ± SD.
Statistical analysis was carried out using SPSS 13.0 software. A
comparison of the differences between the experimental groups was
performed using the one-way ANOVA test. Rate comparisons were
analyzed using the Chi-square (χ2) test. P<0.05 was
considered to indicate a statistically significant difference.
Results
General features and physiological
parameters of the animals
Several systemic factors may affect the preparation
of a MCAO rat model. These factors include rectal temperature,
blood pressure and blood pH. A total of 84 adult male SD rats
weighing 250–300 g were used in the present study. The
physiological variables were monitored 10 min prior to the onset of
MCAO (prior to ischemia), 10 min subsequent to the onset of MCAO
(during ischemia) and 30 min subsequent to the end of MCAO
(subsequent to ischemia) in groups A, B and C. All data were kept
within normal physiological limits prior to, during and subsequent
to ischemia. There were no significant differences in weight,
rectal temperature, PaO2, PaCO2, pH, blood
pressure or blood glucose among the three groups (P>0.05).
Cerebral edema rate, cerebral
infarction rate and RSD
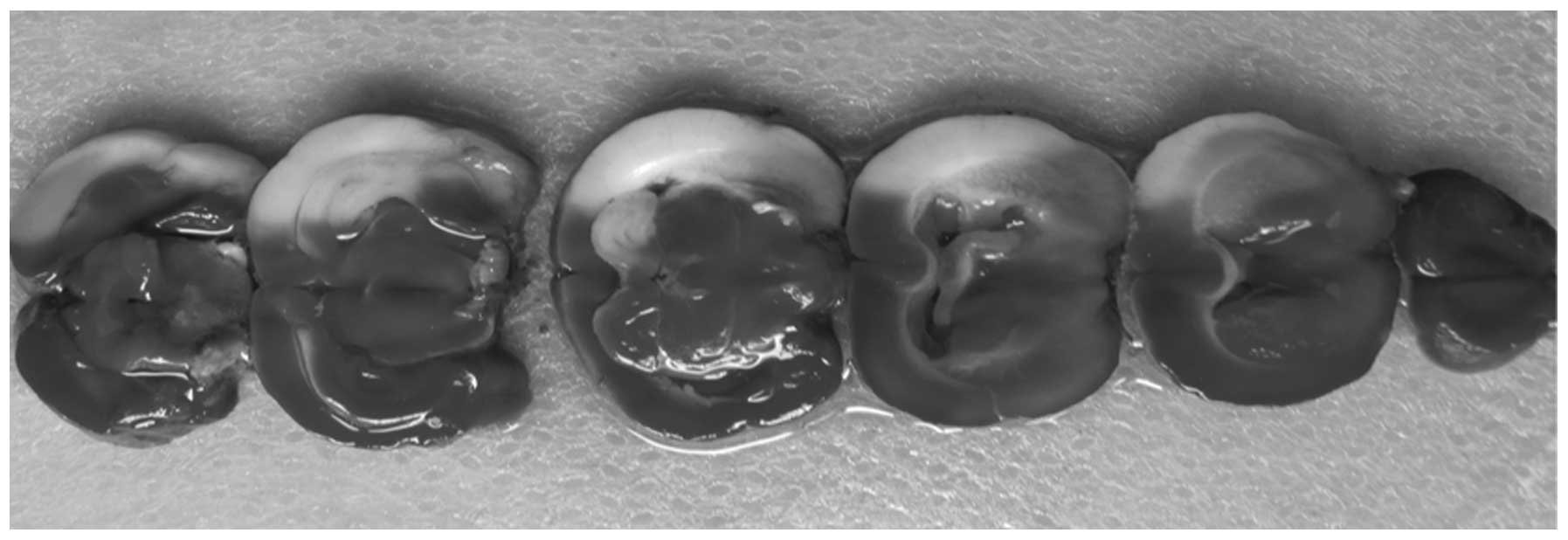
Fig. 1 shows
typical images of the TTC-stained sections of the infarct and
normal tissue. There was a clear border between the red and white
matter; the ischemic region was white and the normal tissue was
rose-colored. The cerebral edema rate, cerebral infarction rate and
RSD in all groups were evaluated subsequent to MCAO. There was no
significant difference in the cerebral edema rate among groups A, B
and C (F=1.426; P=0.243). The cerebral infarction rates in groups
A, B and C were 20.723±1.419, 21.063±1.163 and 21.614±1.067%,
respectively; these values were significantly different (F=7.024;
P=0.001). A Student-Newman-Keuls(S-N-K) comparison showed that the
cerebral infarction rate was significantly different between groups
A and C or B and C (P<0.05), but not between groups A and B
(P>0.05). There also were no significant differences in the
cerebral infarction rate between the subgroups or small subgroups
in the 3 groups (P>0.05). The RSDs of the cerebral infarction
rates in groups A, B and C were 6.85, 5.52 and 4.94%,
respectively.
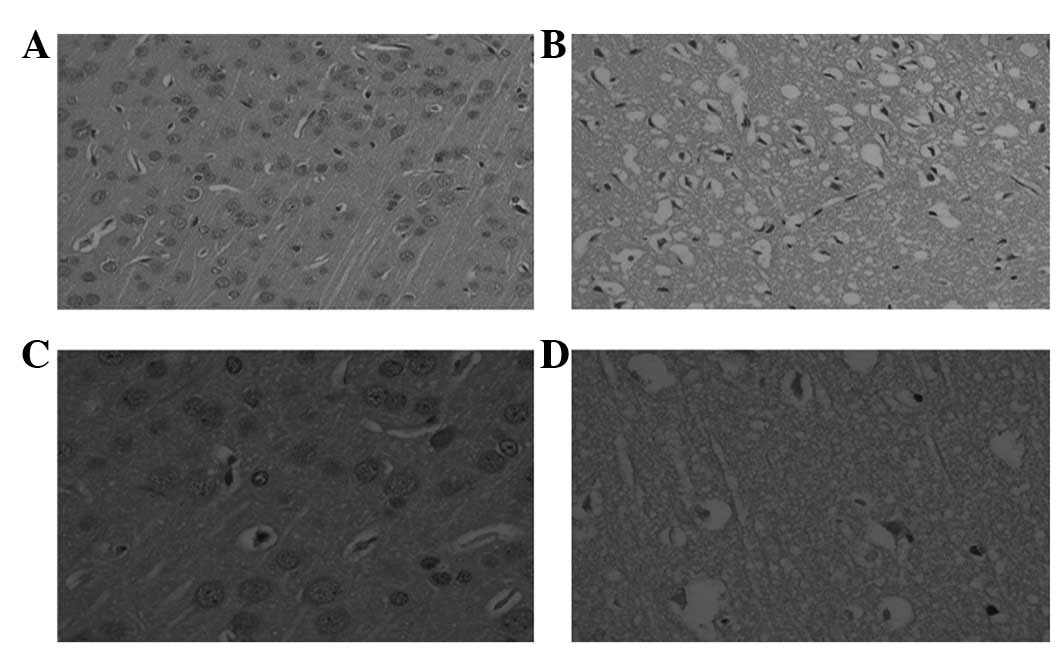
Pathomorphology of the rat brain
At 72 h post-surgery, the brains were subjected to
TTC staining, 4% paraformaldehyde treatment, dehydration and
paraffin embedding. Coronal sections were observed under the
microscope following the creation of the pathological slide and HE
staining. The normal zone is shown in Fig. 2A and B; the neural cells had normal
laminar structures and there was no edema, abnormal vasculature or
inflammatory cell infiltration. However, on the artery-blocked side
shown in Fig. 2C and D, the
infarcted region displayed liquefaction, necrosis and inflammatory
cell infiltration. The neural cells swelled then broke down into
fragments, underwent karyopyknosis and disappeared. The tissue
around the necrotic region loosened, the cells swelled and the
perivascular space enlarged.
Nervous behavior scoring
When evaluated using neurological deficit scoring, 8
rats received a score of zero: 7 (87.5%), 1 (12.5%) and 0 (0%) in
groups A, B and C, respectively. Seven animals received a score of
4: 0 (0%), 1 (14.3%) and 6 (85.7%) in groups A, B and C,
respectively. A score of 1 was given to 15 animals, including 9
(60.0%) in group A, 4 (26.7%) in group B and 2 (13.3%) in group C.
A total of 33 rats achieved a score of 2, including 7 (21.2%) in
group A, 15 (45.5%) in group B and 11 (33.3%) in group C. Only 3
rats scored 3 marks: 0 (0%) in group A, 1 (33.3%) in group B and 2
(66.7%) in group C. In total, 18 animals died during the surgery; 2
(11.1%) from excessive anesthesia, 5 (27.8%) from subarachnoid
hemorrhage (SAH), 2 (11.1%) from dyspnea, 6 (33.3%) from epilepsy
and 3 (16.7%) for no clear reason. These 18 animals were not
included in the neurological deficit scoring.
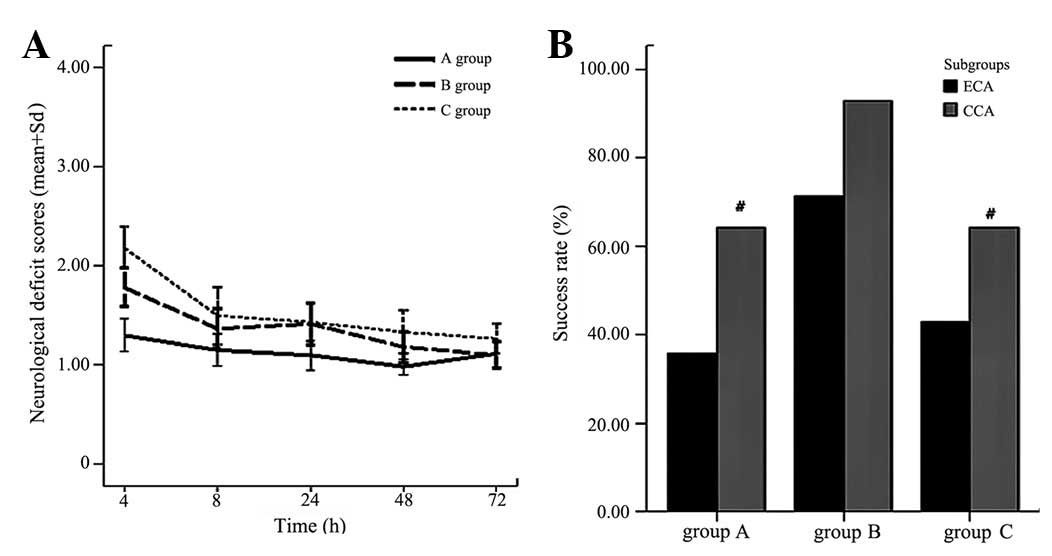
The variation curves of the Zea-Longa scores at 4,
8, 24, 48 and 72 h subsequent to MCAO in all three groups are shown
in Fig. 3A. There were no
significant differences among the 5 time-points in group A
(F=0.393; P=0.814). However, the scores in group B differed
significantly at 4, 8, 24, 48 and 72 h (F=16.315; P=0.000). A
marked difference was observed between hour 4 and the other
time-points subsequent to MCAO (P<0.05), but not among the 8,
24, 48 and 72 h time-points (P>0.05). Similar to group B, group
C displayed scores with a significant difference abetween hour 4
and the subsequent time-points (F=13.911; P=0.000). A paired
comparison showed that the scores at 4 and 8 h were significantly
different from those observed at 24, 48 and 72 h (P<0.05). There
were no significant differences among the 8, 24, 48 and 72 h
time-points subsequent to MCAO (P>0.05).
Success rate
The criteria for a successful MCAO model was that
the animals scored 1, 2 or 3 marks in the neurological deficit
scoring at 4 h post-surgery and survived for 72 h. Also, TTC
staining indicated an evident infarcted region. Fig. 3B shows that the success rate in
group B was the highest while that of group C was the lowest; there
was a significant difference in the success rate among groups A, B
and C (χ2=7.370; P=0.025). The S-N-K paired comparison
showed that the success rate was significantly different between
groups A and B (χ2=6.452; P=0.011) and between groups B
and C (χ2=5.240; P=0.022), but not between groups A and
C (χ2=0.072; P=0.789). The CCA insertion was associated
with a higher success rate than the ECA insertion in each group,
however, there was no significant difference between the two
insertion methods. The success rate of the models subjected to
incisions in the middle of the neck corresponded to that of those
subjected to lateral neck incisions [A1-(1) vs. A1-(2),
χ2=0.311, P=0.577; A2-(1) vs. A2-(2),
χ2=0.311, P=0.577; B1-(1) vs. B1-(2),
χ2=0.000, P=1.000; B2-(1) vs. B2-(2),
χ2=1.077, P=0.299; C1-(1) vs. C1-(2),
χ2=0.000, P=1.000; C2-(1) vs. C2-(2),
χ2=1.167, P=0.288].
Discussion
The MCAO model is a typical model widely used in
studies on cerebral infarction (13,14).
MCAO-induced ischemia-reperfusion injury in the mammalian cerebrum
resembles that in humans (15,16),
therefore, this animal model has been widely used to study ischemic
brain diseases (4,17,18).
The disadvantages of the model are its low success rate and the
high mortality that results from a number of factors that may
affect it, including gender, age, strain (17,19),
body temperature (20,21), weight, anesthetics (22,23),
blood pressure, blood gas (24),
occluding suture size and shape, ligation, insertion (25) and post-operative care. Occluding
sutures with varying tip diameters ranging from 0.18–0.30 mm have
been used in previous studies (5–7) as
even the size of the line tip is taken into consideration during
MCAO surgery. The effect of these factors, as well as artery
ligation and incision, on the success rate of the MCAO model has
not been studied systematically thus far. Previous reports showed
that the diameter and length of the MCA were positively correlated
with the body weight of the rat, indicating that body weight is
critical when creating the MCAO model (26). Animals >350 g in weight have a
wider MCA, which makes it difficult to block the blood flow. By
contrast, the occluding suture is not easily be inserted into the
MCA of rats weighing <240 g. Therefore, rats weighing 250–300 g
are suitable for use in an MCAO model, as in the present study.
The infarcted area is a critical factor in assessing
therapeutic effects in cerebral infarction cases. An ideal animal
model should be stable for repetition; MCAO surgery should generate
a stable model of cerebral infarction with consistent ischemia.
However, in clinical cases, the size and location of the infarcted
region are not consistent, which results in varying effects in
animal and clinical experiments (27). Although laser-doppler scanning of
the cerebral blood flow was suggested to effectively predict the
infarct volume (28), the extent
of the infarct was directly evaluated by TTC in the present study.
The study demonstrated that the cerebral infarction rates in groups
A, B and C were 20.723±1.419, 21.063±1.163 and 21.614±1.067%,
respectively; these values were significantly different among the
three groups (F=7.024; P=0.001). A paired comparison showed that
the cerebral infarction rate in groups A and C or B and C, were
significantly different (P<0.05), while the rate in groups A and
B was not significantly different (P>0.05). There were no
significant differences in the cerebral infarction rate between the
ECA and CCA insertion subgroups of the 3 groups nor between the
smaller middle and lateral neck incision subgroups of the ECA or
CCA (P>0.05). Group C, with the largest diameter (0.28–0.29 mm),
had the highest cerebral infarction rate of the three groups. These
results indicate that the cerebral infarction volume in models
weighing 250–300 g varies with the diameter of the occluding suture
or its tip. The RSD of the cerebral infarction rate decreased when
the diameter of the line became larger. The RSD of type 1.0, 2.0
and 3.0 lines were 6.85, 5.52 and 4.94%, respectively, depending on
whether the diameter of the line coincided with the ICA or the size
of the tip coincided with the anterior cerebral artery as the
artery may be relatively plastic when the occluding suture is
inserted. The occluding suture blocks blood flow only if it is
suitable for the artery. In such situations, the infarcted volume
steadily increases in size. If the occluding suture is unsuitable,
the blood flow is not blocked completely and the infarcted volume
also becomes unstable. Other factors, including the material,
insertion depth, damage to the artery or brain, inflammation,
thrombosis, hemorrhage and individual differences, may affect the
cerebral infarction volume. The results of the present study
indicated that an occluding suture with a larger diameter was able
to give rise to a more stable infarction volume in this MCAO model.
However, a stable infarcted volume is not the only criteria for an
ideal MCAO-induced cerebral infarction model, which should also
simulate the pathology of clinical cases. The model must have a
high success rate and the surgery must be convenient. The nervous
behavior scores in clinical cases improve with the course of the
disease. The present study showed that Zea-Longa scores of nervous
behavior in group A (type 1.0 line) did not differ among the 5
time-points (F=0.393; P=0.814), but differed markedly in groups B
(type 2.0 line; F=16.315; P=0.000) and C (type 3.0 line; F=16.315;
P=0.000). HE staining indicated a typical pathology among the
brains of animals in group B (type 1.0 line). These results
suggested that the suture diameter was able to directly and/or
indirectly affect the clinical pathophysiological features. The
lack of a difference in group A (type 2.0) may be the result of an
incomplete blockage and a small infarction volume.
Compared with group B (type 1.0), groups A (type
2.0) and C (type 3.0) had lower success rates. The reasons for this
may be that: in group A, the diameter of the occluding suture was
not large enough to block the blood flow, and the line was too soft
and easy to curve into the pterygopalatine artery (PPA); and in
group B, the line was too hard and thick and it was difficult to
control the size of the tip. The insertion surgery readily leads to
vasospasms, which make it difficult to control the insertion force
and may lead to SAH. The line tends to pierce into brain tissue,
which may result in severe infarction, epilepsy and cerebral
hernia. As the nervous behavior scores and infarction rate were
higher in group C than those in the other two groups, this
demonstrated that the MCAO-induced injury in group C was more
severe. The curves of the nervous behavior scores showed that group
A was stable while group C changed greatly.
ECA insertion is a conventional and widely used
method, which swerves the normal artery, therefore, passive
distraction leads to excitation of the vagus nerve, which is
harmful to the cerebral infarction. The segment of the line
remaining outside of the ECA continuously changes the normal artery
and results in a lasting distraction. However, CCA insertion
appears to be much more simple than ECA as it does not alter the
normal direction of the artery. Furthermore, the sinuosity between
the CCA and ICA is limited and the CCA is larger than the line
diameter. The rapid nature of the surgery and the brief duration of
exposure also contribute to the high success rate. Variations in
artery insertion have rarely been studied, particularly in the CCA
(Fig. 4). An occluding suture is
made by knotting the line. The intravascular nylon suture is 18±2
mm long so that the segment behind the knot may be either short for
permanent cerebral infarction models or long for
ischemia-reperfusion cerebral infarction models. Subsequent to
ligation, the segment outside the artery forms an arch, which
prevents insertion into the PPA. Consistent with a previous study
(29), the PPA was exposed but not
intercepted in the present study.
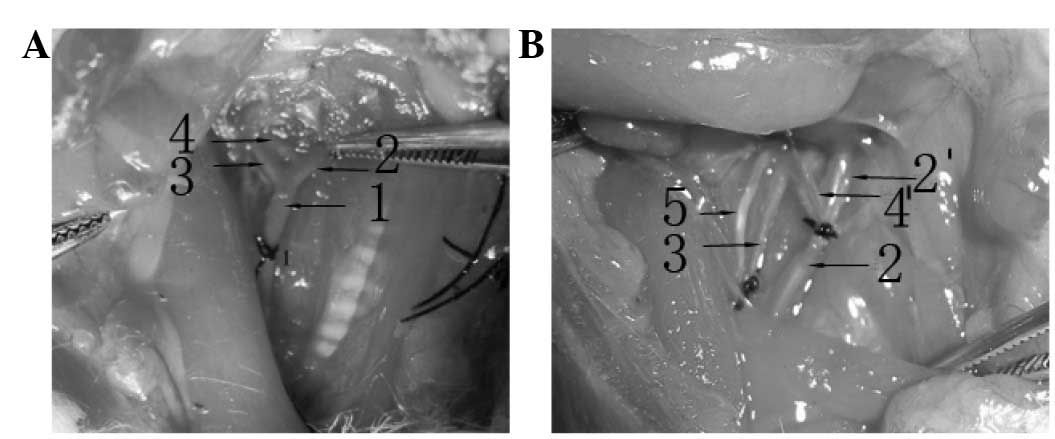 | Figure 4(A) The CCA usually divides into the
ICA and ECA at the level of the sternocleidomastoid and sternohyoid
muscles with one branch originating from the ECA and linked to the
ICA. (B) Variations in the branch point of the ICA and ECA were
observed. The branch point was inferior to the normal branch point.
Four branches originated from the ECA and two were linked to the
ICA. CCA, common carotid artery; ICA, internal carotid artery; ECA,
external carotid artery; 1, CCA; 2, ECA; 2′, ECA variation; 3, ICA;
4, branch from the ECA; 4′, variation branch from the ECA; 5, vagus
nerve. |
In summary, the results of the present study suggest
that the suture diameter and insertion route are able to affect the
infarct volume and success rate in the preparation of suture MCAO
rat models. However, a limitation of this study was that the
cerebral infarction and edema rate were only detected at 72 h
post-surgery as the model animals in group B were used for further
pharmacological experiments. If the detailed time-dependent changes
were determined accurately at 4, 8, 24, 48 and 72 h subsequent to
the MCAO operation, the results should reveal the subtle
differences between the groups and provide an improved model for
the clinic. The data suggest that the suture diameter and insertion
route may be associated with the change in cerebral infarction and
the success rate, however, the exact mechanism is not clear. The
disturbance of blood from the ICA to the PCA (posterior cerebral
artery) may affect the size of the infarction (30). Thus, the results would be more
rigorous if cerebral blood flow was monitored. Considering that a
large sample size is likely to diminish the interference of factors
to a certain degree, the results of the present study may be
reliable as a total of 84 rats were used.
Acknowledgements
This study was supported by the
Province Science Foundation of China (No. 090413120), the Natural
Science Foundation of the Higher Education Institutions of Anhui
Province, China (KJ2007B147) and the Medical Scientific Research
Foundation of Anhui Province (2010B003).
References
|
1.
|
Rubiera M, Ribo M, Delgado-Mederos R, et
al: Tandem internal carotid artery/middle cerebral artery
occlusion: an independent predictor of poor outcome after systemic
thrombolysis. Stroke. 37:2301–2305. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
2.
|
Hossmann KA: Cerebral ischemia: models,
methods and outcomes. Neuropharmacology. 55:257–270. 2008.
View Article : Google Scholar : PubMed/NCBI
|
|
3.
|
Li Y, Chen J, Chen XG, et al: Human marrow
stromal cell therapy for stroke in rat: neurotrophins and
functional recovery. Neurology. 59:514–523. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
4.
|
Lubjuhn J, Gastens A, von Wilpert G, et
al: Functional testing in a mouse stroke model induced by occlusion
of the distal middle cerebral artery. J Neurosci Methods.
184:95–103. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
5.
|
Koizumi J, Yoshida Y, Nakazawa T and
Ooneda G: Experimental studies of ischemic brain edema, I: a new
experimental model of cerebral embolism in rats in which
recirculation can be introduced in the ischemic area. Jpn J Stroke.
8:1–8. 1986.
|
|
6.
|
Wang Y, Tong ET and Xiao XH: Evaluation of
the modified model of reversible focal cerebral ischemia in rats by
MRI. Stroke Nervous Dis. 3:171–173. 1999.
|
|
7.
|
Chiang T, Messing RO and Chou WH: Mouse
model of middle cerebral artery occlusion. J Vis Exp. 27612011.
|
|
8.
|
Ma J, Zhao L and Nowak TS Jr: Selective,
reversible occlusion of the middle cerebral artery in rats by an
intraluminal approach. Optimized filament design and methodology. J
Neurosci Methods. 156:76–83. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
9.
|
Longa EZ, Weinstein PR, Carlson S and
Cummins R: Reversible middle cerebral artery occlusion without
craniectomy in rats. Stroke. 20:84–91. 1989. View Article : Google Scholar : PubMed/NCBI
|
|
10.
|
Holland JP, Sydserff SG, Taylor WA and
Bell BA: Rat models of middle cerebral artery ischemia. Stroke.
24:1423–1424. 1993.PubMed/NCBI
|
|
11.
|
Engel O, Kolodziej S, Dirnagl U and Prinz
V: Modeling stroke in mice - middle cerebral artery occlusion with
the filament model. J Vis Exp. 24232011.PubMed/NCBI
|
|
12.
|
Taniguchi H and Andreasson K: The
hypoxic-ischemic encephalopathy model of perinatal ischemia. J Vis
Exp. 9552008.PubMed/NCBI
|
|
13.
|
Uluç K, Miranpuri A, Kujoth GC, Aktüre E
and Başkaya MK: Focal cerebral ischemia model by endovascular
suture occlusion of the middle cerebral artery in the rat. J Vis
Exp. 19782011.
|
|
14.
|
Ansari S, Azari H, McConnell DJ, Afzal A
and Mocco J: Intraluminal middle cerebral artery occlusion (MCAO)
model for ischemic stroke with laser doppler flowmetry guidance in
mice. J Vis Exp. 28792011.PubMed/NCBI
|
|
15.
|
Li Y, Chopp M, Chen J, Wang L, Gautam SC,
Xu YX and Zhang Z: Intrastriatal transplantation of bone marrow
nonhematopoietic cells improves functional recovery after stroke in
adult mice. J Cereb Blood Flow Metab. 20:1311–1319. 2000.
View Article : Google Scholar : PubMed/NCBI
|
|
16.
|
Chen J, Li Y, Wang L, Lu M and Chopp M:
Caspase inhibition by Z-VAD increases the survival of grafted bone
marrow cells and improves functional outcome after MCAo in rats. J
Neurol Sci. 199:17–24. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
17.
|
Harper AJ: Production of transgenic and
mutant mouse models. Methods Mol Med. 104:185–202. 2005.PubMed/NCBI
|
|
18.
|
Koh PO: Melatonin attenuates decrease of
protein phosphatase 2A subunit B in ischemic brain injury. J Pineal
Res. 52:57–61. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
19.
|
Carmichael ST: Rodent models of focal
stroke: size, mechanism, and purpose. NeuroRx. 2:396–409. 2005.
View Article : Google Scholar : PubMed/NCBI
|
|
20.
|
Florian B, Vintilescu R, Balseanu AT, et
al: Long-term hypothermia reduces infarct volume in aged rats after
focal ischemia. Neurosci Lett. 438:180–185. 2008.PubMed/NCBI
|
|
21.
|
Barber PA, Hoyte L, Colbourne F and Buchan
AM: Temperature-regulated model of focal ischemia in the mouse: a
study with histopathological and behavioral outcomes. Stroke.
35:1720–1725. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
22.
|
Kapinya KJ, Prass K and Dirnagl U:
Isoflurane induced prolonged protection against cerebral ischemia
in mice: a redox sensitive mechanism? Neuroreport. 13:1431–1435.
2002. View Article : Google Scholar : PubMed/NCBI
|
|
23.
|
Sakai H, Sheng H, Yates RB, Ishida K,
Pearlstein RD and Warner DS: Isoflurane provides long-term
protection against focal cerebral ischemia in the rat.
Anesthesiology. 106:92–99. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
24.
|
Browning JL, Heizer ML, Widmayer MA and
Baskin DS: Effects of halothane, alpha-chloralose, and
pCO2 on injury volume and CSF beta-endorphin levels in
focal cerebral ischemia. Mol Chem Neuropathol. 31:29–42.
1997.PubMed/NCBI
|
|
25.
|
Bouley J, Fisher M and Henninger N:
Comparison between coated vs. uncoated suture middle cerebral
artery occlusion in the rat as assessed by perfusion/diffusion
weighted imaging. Neurosci Lett. 412:185–190. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
26.
|
Roos MW, Sperber GO, Johansson A and Bill
A: An experimental model of cerebral microischemia in rabbits. Exp
Neurol. 137:73–80. 1996. View Article : Google Scholar : PubMed/NCBI
|
|
27.
|
Alonso de Leciñana M, Diez-Tejedor E,
Gutierrez M, Guerrero S, Carceller F and Roda JM: New goals in
ischemic stroke therapy: the experimental approach - harmonizing
science with practice. Cerebrovasc Dis. 2(Suppl 2): 159–168.
2005.PubMed/NCBI
|
|
28.
|
Kim DE, Kim JY, Nahrendorf M, et al:
Direct thrombus imaging as a means to control the variability of
mouse embolic infarct models: the role of optical molecular
imaging. Stroke. 42:3566–3573. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
29.
|
Dittmar M, Spruss T, Schuierer G and Horn
M: External carotid artery territory ischemia impairs outcome in
the endovascular filament model of middle cerebral artery occlusion
in rats. Stroke. 34:2252–2257. 2003. View Article : Google Scholar
|
|
30.
|
Akamatsu Y, Shimizu H, Saito A, Fujimura M
and Tominaga T: Consistent focal cerebral ischemia without
posterior cerebral artery occlusion and its real-time monitoring in
an intraluminal suture model in mice. J Neurosurg. 116:657–664.
2012. View Article : Google Scholar : PubMed/NCBI
|