Introduction
Takotsubo cardiomyopathy is a transient ventricular
akinesia without the appearance of coronary artery disease of
sufficient magnitude to explain the extent of cardiac dysfunction
(1). Typically, it occurs on the
left ventricular (LV) apex and normally presents as apical
ballooning with hypercontraction of basement segments. It is often
accompanied by chest pain, dynamic reversible electrocardiographic
abnormalities and mild elevation of cardiac enzyme levels (2). However, variants of Takotsubo
cardiomyopathy have been described (3,4). We
present the case of an 83-year-old woman who demonstrated isolated
right ventricular (RV) involvement of Takotsubo cardiomyopathy at
the first presentation and LV involvement during recurrence.
Case report
An 83-year-old female patient with a history of
hypertension and diabetes mellitus presented to the emergency
department at Kyung Hee University Hospital (Seoul, Korea) with a
left hip fracture resulting from a fall. The patient complained of
chest discomfort and mild dyspnea. On admission, the patient’s
blood pressure was 128/83 mmHg and heart rate was 108 beats/min.
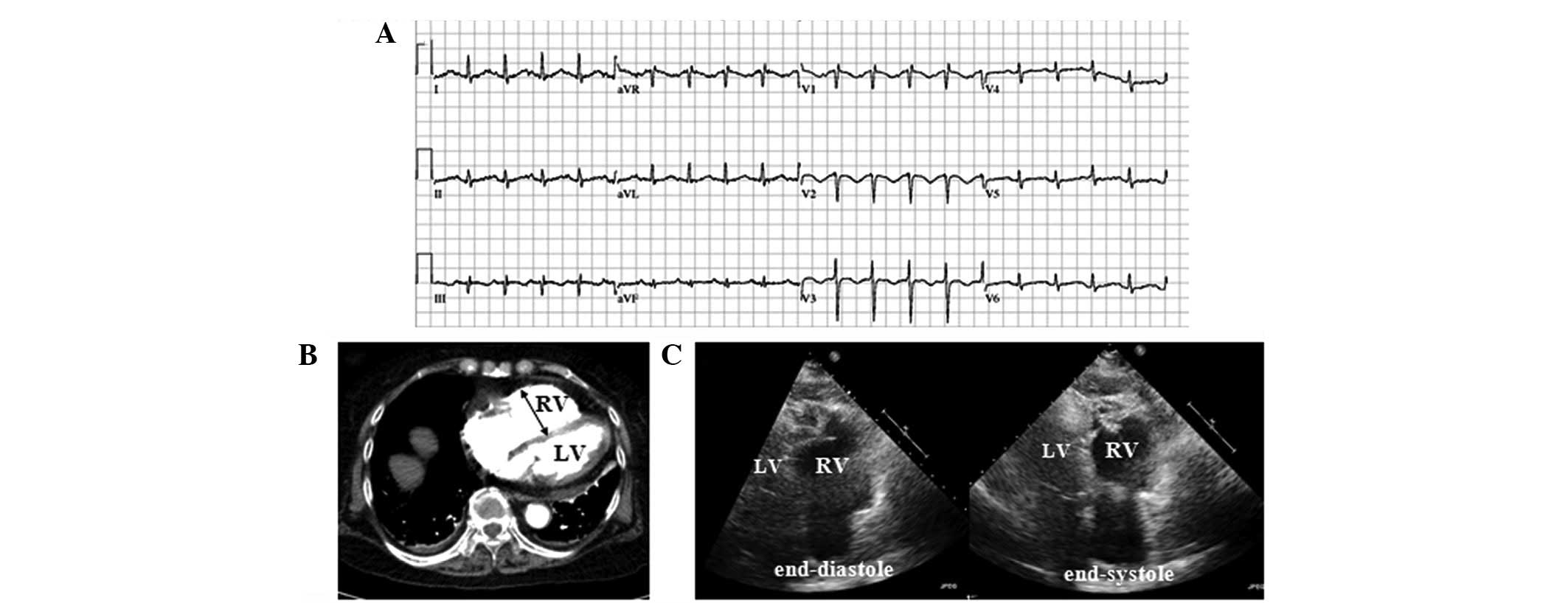
Electrocardiography (ECG) revealed sinus tachycardia with an RSR
pattern in lead V1, T wave inversion and poor R progression in
leads V1-3 and S1/Q3 (Fig. 1A).
Serum troponin I was elevated to 0.380 ng/ml. Multi-slice computed
tomography pulmonary angiography demonstrated mild dilatation of
the right atrium (RA) and right ventricle, as well as mild
pulmonary edema with small bilateral pleural effusions (Fig. 1B); however, there was no filling
defect in the pulmonary arteries. Transthoracic echocardiography
(TTE) revealed akinesia of the apico-mid RV free wall with RV
dilatation (Fig. 1C) and a mild
reduction of RV systolic function. LV ejection fraction was
preserved (65%) without regional wall motion abnormality. The
patient’s coronary angiography was normal. Potential malignancy was
excluded by chest and abdominal computed tomography. The symptoms
of chest discomfort and mild dyspnea resolved following
conservative treatment. Follow-up TTE on the sixth day of
hospitalization revealed normalized RV size and function, as well
as resolution of the RV wall motion abnormality. The patient
underwent surgery for the left hip fracture. On the day after
surgery, the patient complained of chest pain and dyspnea. The
patient’s blood pressure, heart rate and respiratory rate were
91/59 mmHg, 104 beats/min and 25 breaths/min, respectively. On ECG,
deep T wave inversion was observed to be newly developed in leads
I, aVL and V2-6 (Fig. 2A).
Troponin I levels were elevated to 0.226 ng/ml. Portable
echocardiography revealed akinetic and dilated LV apex and
hyperkinetic basal segments with an LV ejection fraction of 56%
(Fig. 2B). The RV function and
wall motion was normal. Following conservative treatment, follow-up
TTE revealed a good LV systolic function with normal wall motion.
The patient was discharged uneventfully. The study was approved by
the IRB ethics committee (KHNMC IRB 2013-027)
Discussion
By considering the clinical course and the actual
findings, the patient was diagnosed with recurrent Takotsubo
cardiomyopathy, which involved the right ventricle at initial
presentation and the left ventricle during recurrence. The
provoking factor was considered to be an acute medical illness or
intense physical stress.
The pathophysiology of Takotsubo cardiomyopathy has
not been clearly established. A number of studies have suggested
that an induced severe transient mid-ventricular cavity dynamic
gradient and catecholamine-induced reduction in subendocardial
blood flow lead to significant LV outflow tract obstruction and
secondary ischemia of the LV apex and anterior wall in Takotsubo
cardiomyopathy (5,6). However, this finding may be a
phenomenon observed in only certain patients with LV involvement of
Takotsubo cardiomyopathy (7,8). It
does not explain the development of other variants of Takotsubo
cardiomyopathy. Other studies have suggested that an anatomically
different distribution of cardiac adrenergic receptors, the degree
of stimulation by sympathetic activity and different
susceptibilities to sympathetic stimulation are responsible for the
development of variants (9,10).
However, the present observation of a patient with Takotsubo
cardiomyopathy involving different cardiac locations during
recurrence may provide evidence against this suggestion.
Elesber et al (11) reported that patients with a
clinical manifestation of biventricular involvement of Takotsubo
cardiomyopathy differ from patients with LV involvement, which is
associated with lower LV ejection fraction, longer hospitalization
and more complications, including severe congestive heart failure,
intra-aortic balloon pump and cardio-pulmonary resuscitation.
Additionally, isolated RV Takotsubo cardiomyopathy may represent a
distinct manifestation compared with LV Takotsubo cardiomyopathy,
including acute right heart failure (3). Unfortunately, cases with isolated RV
involvement are rarely reported (3,12).
Therefore, further verification is required by additional
observations in the future.
The prognosis of Takotsubo cardiomyopathy is
considered favorable. However, it may be fatal and recurrent
Takotsubo cardiomyopathy may cause several problems, including the
misdiagnosis of acute coronary syndrome or sepsis, leading to
incorrect management, repetitive symptoms, interruption of
treatment for original medical problem and longer periods of
hospitalization.
In conclusion, we report a unique case demonstrating
recurrence with LV apical involvement following the occurrence of
isolated RV Takotsubo cardiomyopathy. To our knowledge, this is the
first report to describe such a case. The pathophysiology may be
different from previous suggested mechanisms of Takotsubo
cardiomyopathy.
References
|
1.
|
Bybee KA, Kara T, Prasad A, Lerman A,
Barsness GW, Wright RS and Rihal CS: Systematic review: transient
left ventricular apical ballooning: a syndrome that mimics
ST-segment elevation myocardial infarction. Ann Intern Med.
141:858–865. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
2.
|
Kurowski V, Kaiser A, von Hof K, et al:
Apical and midventricular transient left ventricular dysfunction
syndrome (tako-tsubo cardiomyopathy): frequency, mechanisms, and
prognosis. Chest. 132:809–816. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
3.
|
Stähli BE, Ruschitzka F and Enseleit F:
Isolated right ventricular ballooning syndrome: a new variant of
transient cardiomyopathy. Eur Heart J. 32:18212011.PubMed/NCBI
|
|
4.
|
Surapaneni P, Vittala SS, Vinales KL,
Najib MQ and Chaliki HP: Atypical presentation of takotsubo
cardiomyopathy. Eur J Echocardiogr. 12:E312011. View Article : Google Scholar : PubMed/NCBI
|
|
5.
|
Villareal RP, Achari A, Wilansky S and
Wilson JM: Anteroapical stunning and left ventricular outflow tract
obstruction. Mayo Clin Proc. 76:79–83. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
6.
|
Merli E, Sutcliffe S, Gori M and
Sutherland GG: Tako-Tsubo cardiomyopathy: new insights into the
possible underlying pathophysiology. Eur J Echocardiogr. 7:53–61.
2006. View Article : Google Scholar : PubMed/NCBI
|
|
7.
|
Haghi D, Athanasiadis A, Papavassiliu T,
et al: Right ventricular involvement in Takotsubo cardiomyopathy.
Eur Heart J. 27:2433–2439. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
8.
|
Sharkey SW, Lesser JR, Zenovich AG, et al:
Acute and reversible cardiomyopathy provoked by stress in women
from the United States. Circulation. 111:472–479. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
9.
|
Yasu T, Tone K, Kubo N and Saito M:
Transient mid-ventricular ballooning cardiomyopathy: a new entity
of Takotsubo cardiomyopathy. Int J Cardiol. 110:100–101. 2006.
View Article : Google Scholar : PubMed/NCBI
|
|
10.
|
Eitel I, Schuler G, Gutberlet M and Thiele
H: Biventricular stress-induced (takotsubo) cardiomyopathy with
left midventricular and right apical ballooning. Int J Cardiol.
151:e63–e64. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
11.
|
Elesber AA, Prasad A, Bybee KA, et al:
Transient cardiac apical ballooning syndrome: prevalence and
clinical implications of right ventricular involvement. J Am Coll
Cardiol. 47:1082–1083. 2006. View Article : Google Scholar
|
|
12.
|
Mrdovic I, Kostic J, Perunicic J, Asanin
M, Vasiljevic Z and Ostojic M: Right ventricular Takotsubo
cardiomyopathy. J Am Coll Cardiol. 55:17512010. View Article : Google Scholar : PubMed/NCBI
|