Introduction
The diaphragm is a dome-shaped sheet of muscle with
a central tendinous component that separates the thorax from the
abdomen and maintains the pressure gradient between those two
cavities (1). It arises from the
crura, the arcuate ligaments, the costal margin and the posterior
aspects of the xiphoid (2). It has
essential anatomic and functional roles necessary for the breathing
process, which undertakes 60–75% of the total tidal volume of
respiration (3).
The morphology and movement of the diaphragm may be
detected by fluoroscopy, chest radiography, computed tomography
(CT) and magnetic resonance imaging (MRI) (4–7).
Using these techniques to diagnose weakness or paralysis of the
diaphragm results in exposure to radiation, requires patient
transportation and is time-consuming. Ultrasound (US) allows direct
visualization of the displacement of the diaphragm in humans
breathing freely, as well as inspection of critical patients at the
bedside without the use of ionizing radiation. Several authors have
reported the use of M-mode US for the evaluation of the
diaphragmatic displacement (8–10);
however, their results were inconsistent. Different positions of
the patients, the transducer placement, the direction of the US
beam and the compressive maneuvers during US examination may affect
the results of the measurements (11). Furthermore, M-mode US measurements
only reflect the diaphragmatic motion where the exploration line
is. Thus, different locations of the exploration line generate
different results, due to the asynchronicity of the diaphragmatic
motions.
In recent years, 2-dimensional (2D) deformation
imaging (strain and strain-rate imaging) has emerged as a new
noninvasive method for assessing myocardial function and
differentiating between active and passive movement of myocardial
segments (12). It analyzes the
myocardial motion by tracking speckles (natural acoustic markers)
in the 2D US image. The geometric shift of each speckle represents
local tissue movement (13). In
this study, we describe a novel method utilizing 2D strain imaging
to quantify segmental longitudinal deformation (strain) of the
right diaphragm using specially designed software for tracking
cardiac motion.
Materials and methods
Subjects, setting and study design
Twenty-one healthy volunteers (12 male and 9 female)
without specific sporting training were selected from April 1, 2012
to June 30, 2012 in the Ultrasound Department, Shanghai East
Hospital affiliated to Tongji University. None of the subjects had
a history of diaphragm dysfunction, chronic obstructive pulmonary
diseases, asthma, thoracic surgery, pleural thickening or smoking.
No fasting or preparation was required. After providing informed
consent, all subjects underwent a medical history interview,
physical examination and pulmonary function tests by standard
spirometry (Ilmeter 1304; Masterlab Jaeger, Würzberg, Germany)
according to the standards of the American Thoracic Society. The
criteria for classification as normal consisted of a forced vital
capacity (FVC) >80% of predicted, a forced expiratory volume in
1 sec (FEV1) >80% of predicted and a FEV1/FVC ratio >80% of
predicted. The measurements of right hemidiaphragm kinetics were
made on the B- and M-mode frozen images using the US machine
calibration and algorithm in supine position during quiet and
forced breathing. The study was performed following the approval of
the ethics committee of Shanghai East Hospital affiliated to Tongji
University.
US technique
US examinations were performed by an experienced
investigator using a commercially available Doppler echocardiograph
(Vivid E9 Diagnostic Ultrasound System; GE Healthcare, Horten,
Norway), with an appropriate total gain and depth, 50–70 frames/sec
and equipped with a M5S convex transducer. Assessment of right
diaphragm excursion on the cranial-caudal axis was performed in B-
and M-mode, with a frequency between 3.5 and 5.0 MHz depending on
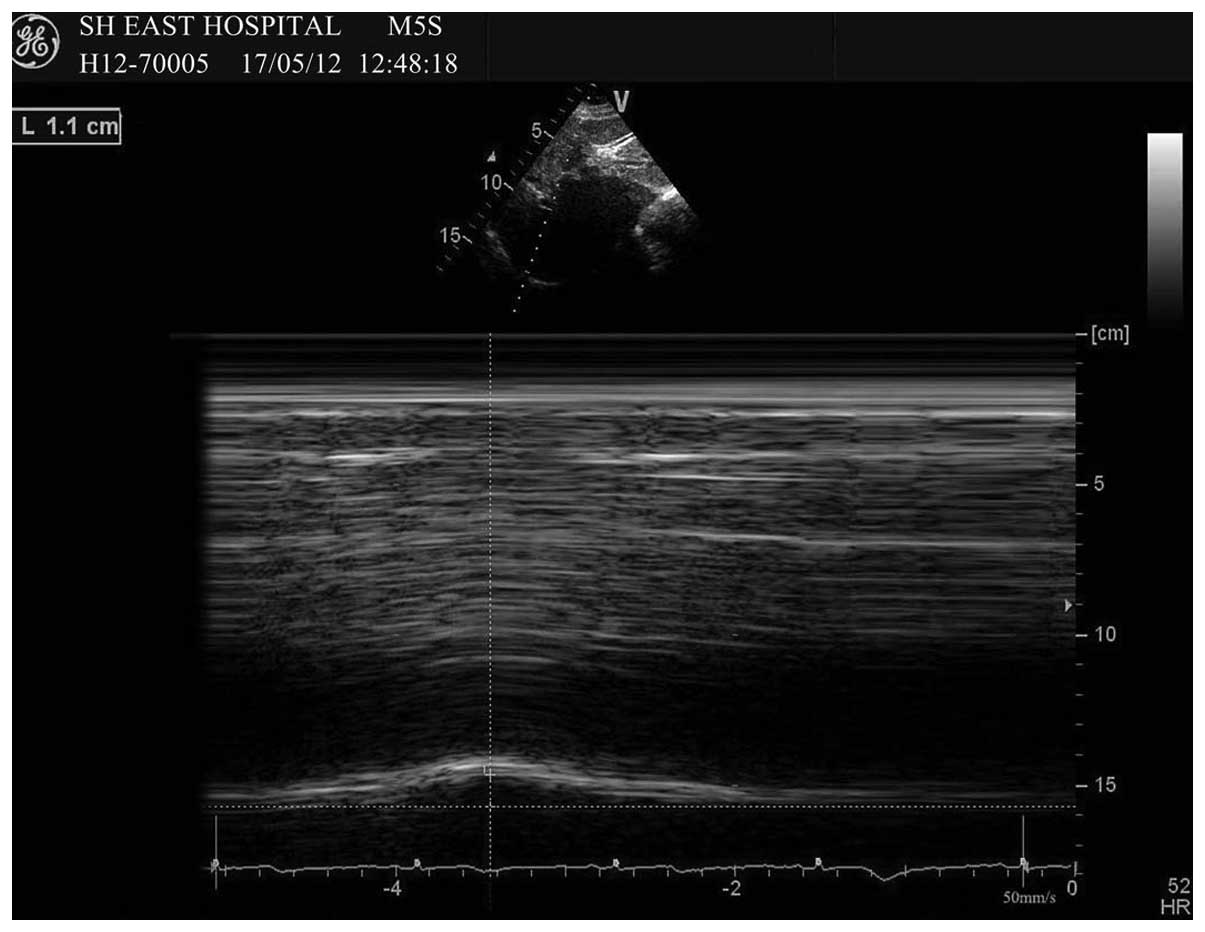
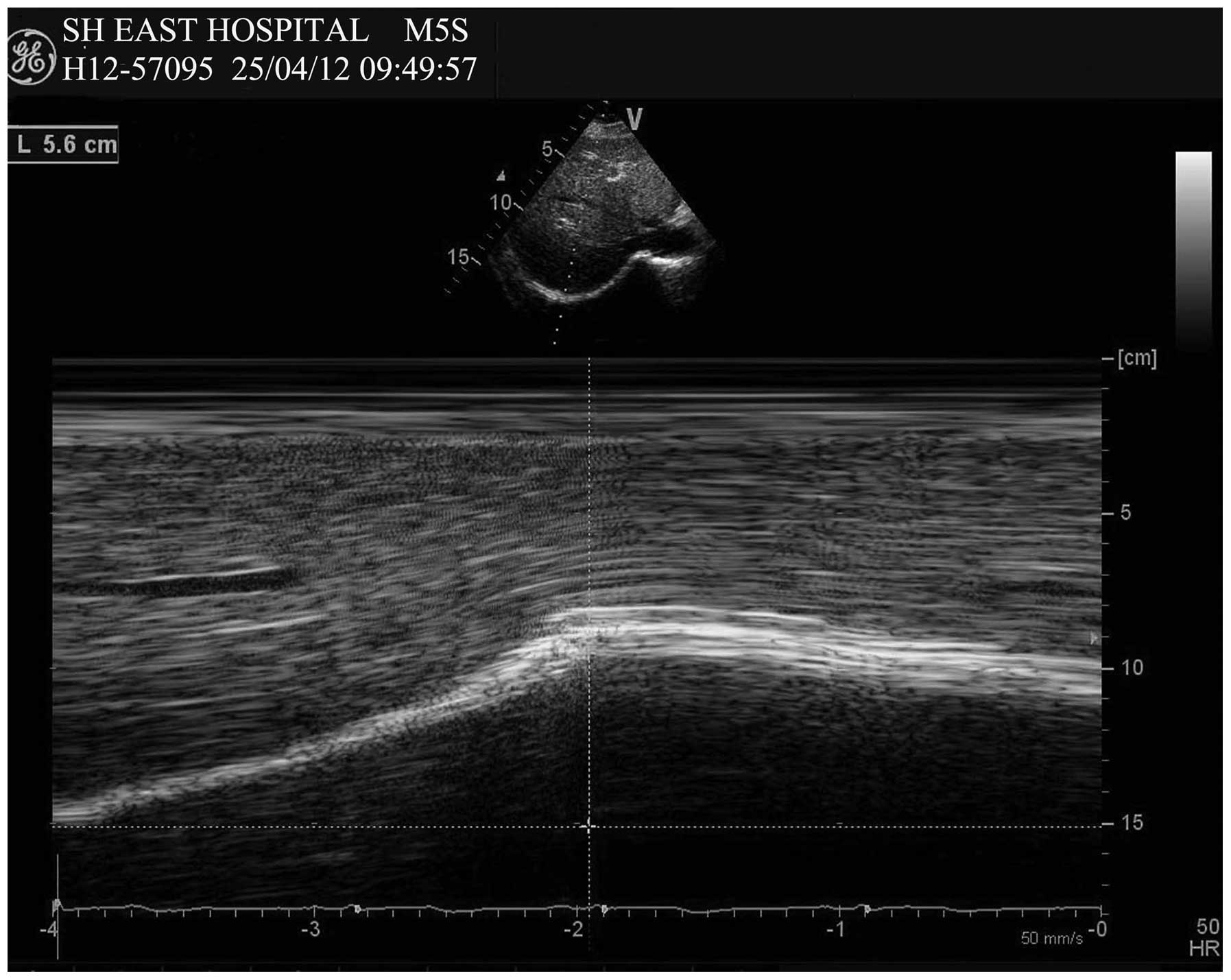
the depth of the structure for optimal visualization. The excursion
of the right hemidiaphragm was measured from the condition of
functional residual capacity to reaching tidal volume (quiet
breathing; Fig. 1) and total lung
capacity (forced breathing; Fig.
2). To obtain the images, the transducer was positioned on the
abdominal wall just below the right costal margin around the
midclavicular line with the right intrahepatic vein branch as an
anatomical landmark. In this view, the right hemidiaphragm appeared
as a thick hyper-echogenic curved line. The transducer was firmly
held in this position during all phases of the respiratory cycle.
M-mode US of right diaphragm motions and electrocardiogram were
performed synchronously with a 50 mm/sec paper speed.
Diaphragm strain measurements
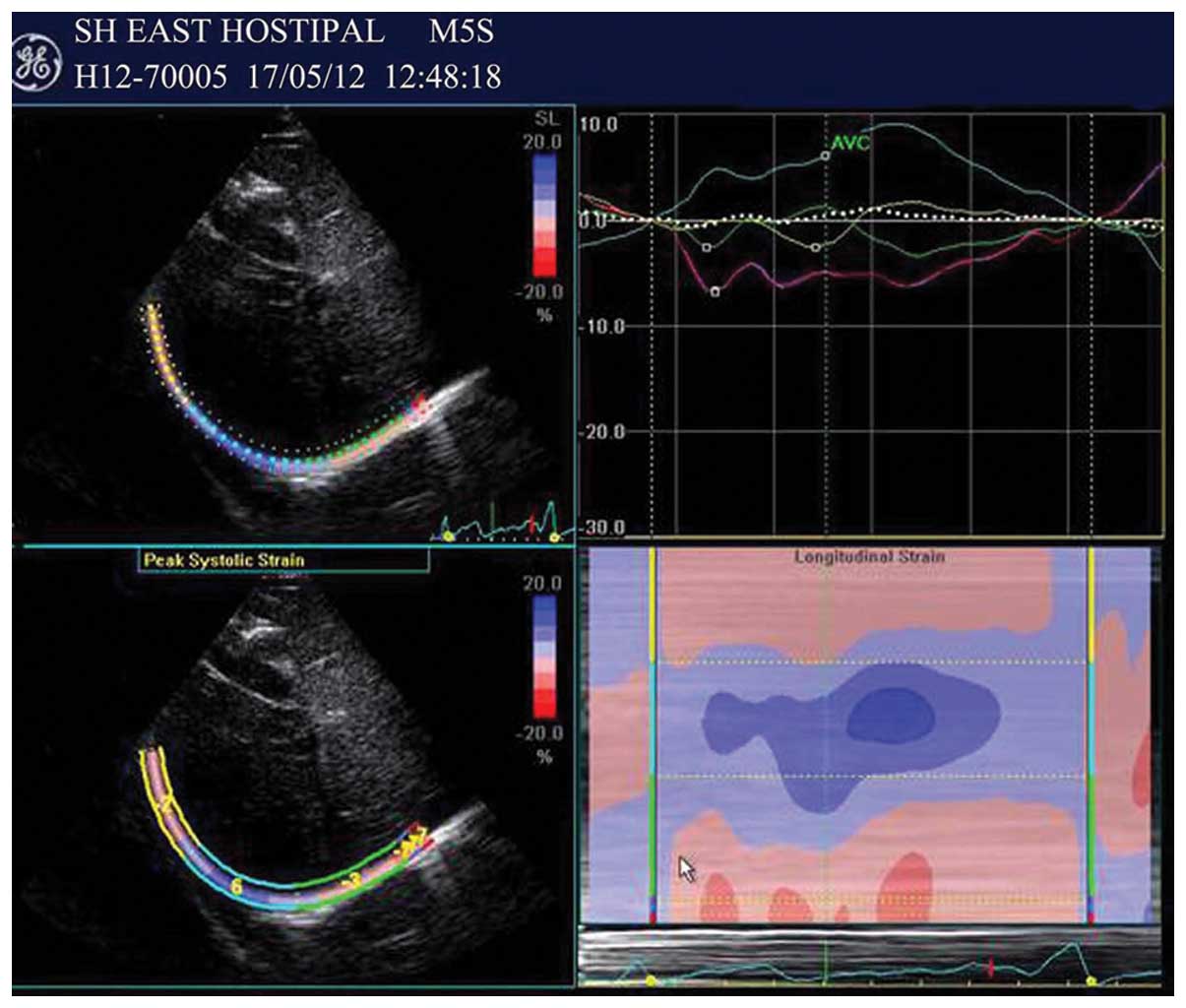
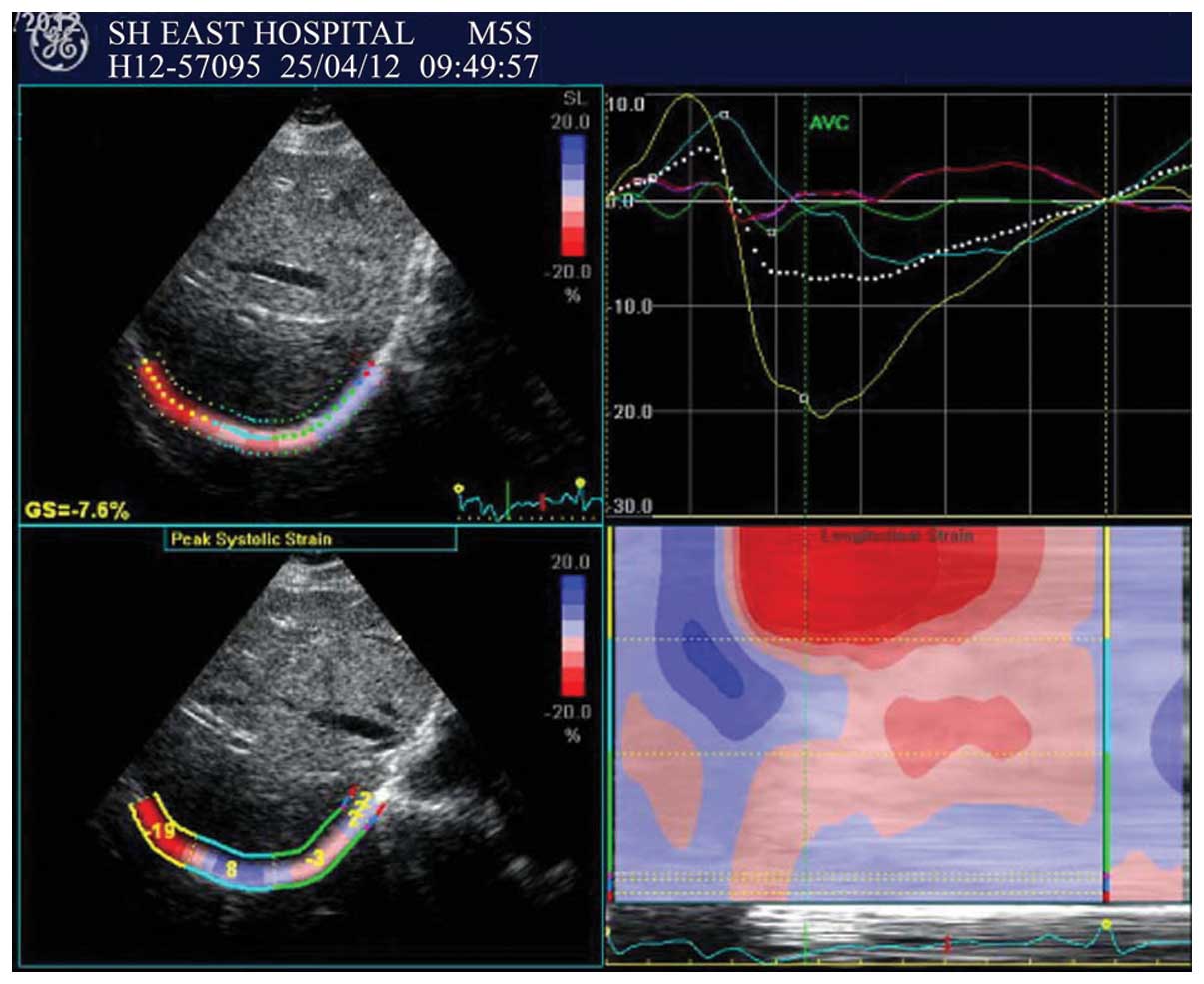
The videos of the right diaphragm motions for four
continuous cardiac cycles were saved and diaphragm strains were
detected using automatic function imaging and cardiac cycle
analysis in M-mode US in turns. The peritoneum, mid-diaphragm and
pleural border were equivalent to the epicardial, midmyocardial and
endocardial lines according to the manual of the analytical
software devised for cardiac motion as a region of interest (ROI).
After stopping the motion of the cursor for several seconds, the
software detected longitudinal deformation of the diaphragm and
exhibited the results automatically. The value obtained from the
cardiac cycle under the maximal inspiratory slope represented the
longitudinal deformation of the diaphragm in the inspiratory phase
(Figs. 3 and 4). The tracking time was from the R wave
to aortic valve closure (AVC) in the same cardiac cycle. The right
diaphragm hyper-echogenic curved line was divided into three
segments in the majority of the results: the dome position (the
highest point of the diaphragm) in the middle; the zone of
apposition (the cylindrical region of the diaphragm that apposes
the lower rib cage) in the right; and the crural of the diaphragm
in the left. A negative value indicated active systole of the
diaphragm-corresponding segment and a positive value indicated
passive stretching.
Statistical analysis
Statistical analysis of data was performed using
SPSS 16.0 software (SPSS, Inc., Chicago, IL, USA). Continuous
variables are expressed as mean ± standard deviation. The
distribution of data was analyzed with a Kolmogorov-Smirnov test.
For a normal distribution, differences were compared using an
unpaired Student’s t-test and data that were not normally
distributed were compared using the Mann-Whitney U test. P<0.05
was considered to indicate a statistically significant
difference.
Results
Twenty-one healthy volunteers were enrolled in the
present study. Demographic, anthropometric and spirometric data of
the volunteers are reported in Table
I. Pulmonary function assessments by spirometry were normal in
all subjects. The mean quiet and forced diaphragm excursion values
were 15.52±0.60 and 59.29±1.88 mm, respectively, measured by M-mode
US. Negative strain values first appeared in the zone of apposition
and then in the crura of the right diaphragm, through analysis the
cardiac cycle under M-mode US. The absolute value of the negative
strain values increased from the beginning of inspiration to the
maximal inspiratory slope. The right diaphragm real-time 2D
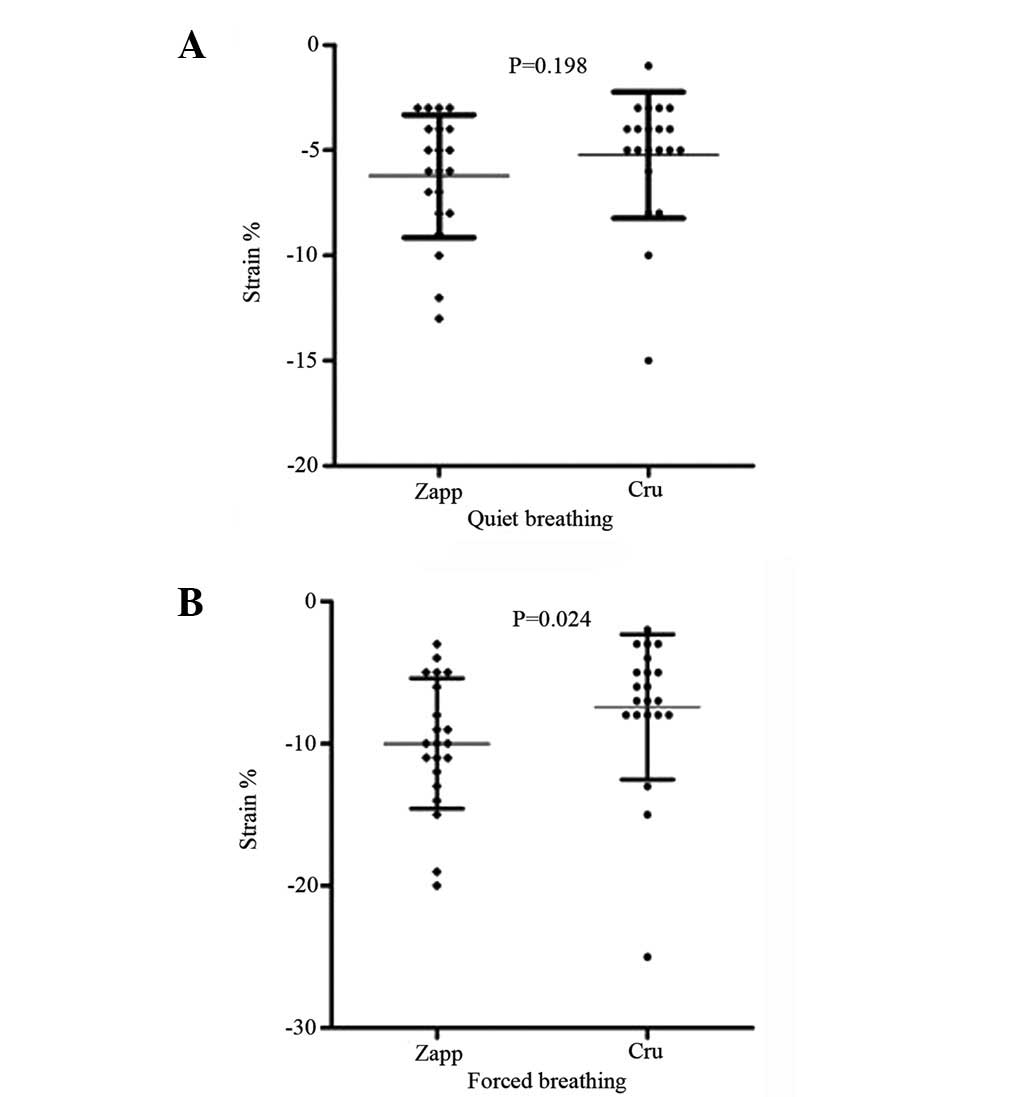
segmental strains are reported in Table II. Positive strain values describe
passive extension and negative values describe active shortening of
a given diaphragm segment related to the length at a previous time
point. In quiet breathing, there was no significant difference in
the strains of the crura of the right diaphragm and the zone of
apposition (P=0.198); however, there was a significant difference
in forced breathing (P=0.024; Fig.
5).
 | Table I.Demographic data, anthropometric
characteristics and pulmonary function spirometry test results of
the healthy volunteers. |
Table I.
Demographic data, anthropometric
characteristics and pulmonary function spirometry test results of
the healthy volunteers.
| Characteristics | Value |
|---|
| Number of
subjects | 21 |
| Gender (M/F) | 12/9 |
| Age (years) | 43±11 |
| BMI
(kg/m2) | 22±3.0 |
| Heart rate | 65±12 |
| FVC (predicted
%) | 3.9±1.1 |
| 98.2±11.0 |
| FEV1 (predicted
%) | 3.7±1.6 |
| 96±13.2 |
| FEV1/FVC (predicted
%) | 89±7.5 |
| 98.2±10.3 |
| Table II.Right diaphragm real-time 2D segmental
strains of the healthy volunteers. |
Table II.
Right diaphragm real-time 2D segmental
strains of the healthy volunteers.
| Segment | Quiet breathing | Forced breathing | P-value |
|---|
| Crura of
diaphragm | −5.24±3.00 | −7.42±5.10 | 0.0709 |
| Dome of
diaphragm | 3.24±1.64 | 4.10±2.34 | 0.2780 |
| Zone of
apposition | −6.24±2.91 | −10.00±4.58 | 0.0051 |
| Whole diaphragm | −2.14±1.80 | −4.62±2.56 | 0.0002 |
Discussion
The diaphragm is active throughout the life of an
individual. Dysfunction of the diaphragm, including paralysis,
weakness and eventration, is a frequent contributor to dyspnea.
Despite its importance, the diaphragm is often underappreciated and
incompletely evaluated by clinicians and radiologists (14). M-mode US allows visualization of
the displacement of the diaphragm. The role of M-mode US in the
qualitative assessment of diaphragm amplitude has been investigated
in normal and pathological conditions (15–17).
Our results of M-mode US measurements are similar to these previous
findings. Motion measurements do not differentiate between active
and passive movement of a moving object, whereas deformation
analyses (strain imaging) allow discrimination between active and
passive tissue movement (12).
Strain imaging (deformation analysis) is more useful than wall
motion analysis (velocity and displacement) for the detection of
regional myocardial dysfunction (18). Longitudinal strain of the diaphragm
may be as important to its function as myocardial strain is for
cardiac function.
In this study, 2D strain US speckle tracking was
used as a novel approach for analyzing right hemidiaphragm
deformation in healthy subjects. After analyzing the cardiac cycle
in each individual using M-mode US, we found that negative strain
values first appeared in the zone of apposition and then in the
crura. The negative strain values describe active shortening of a
given segment of the diaphragm related to the length at a previous
time point. The positive strain values describe passive extension;
the dome of the diaphragm stretches passively. The right diaphragm
longitudinal strains of the crura and the zone of apposition
presented no significant difference in quiet breathing; however,
there was a significant difference in forced breathing (P=0.198 and
P=0.024, respectively). The strains of the whole diaphragm and the
zone of apposition changed significantly in quiet and forced
breathing (P=0.000 and P=0.005, respectively); however, there were
no differences in the crura and the dome (P=0.071 and P=0.278,
respectively). The possible interpretation is that the costal and
crural segments of the diaphragm have different embryological
origins, different segmental innervations and different functional
attributes (2). There are regional
differences in diaphragm thickness, in vivo fiber length and
the degree of shortening within the costal diaphragm of
anesthetized dogs during passive lung inflation (19). This suggests that the potential of
generating force and causing displacement is not uniform throughout
the diaphragm (19). However,
Suzuki et al examined the shortening of the parasternal
intercostal muscles, crural diaphragm and costal diaphragm in dogs
through implanted sonomicrometers. The authors identified no
difference in the shortening pattern between crural and costal
diaphragms (20). The advantage of
right diaphragm strain imaging using non-Doppler 2D speckle
tracking is that it tracks in two dimensions, along the direction
of the longitudinal shortening and extension of the diaphragm, not
along the US beam, and since it is not based on tissue Doppler
measurements, it is angle-independent (18). The non-Doppler 2D speckle tracking
provides a bedside, non-invasive and low-cost examination method
for detecting changes of diaphragm length, compared with dynamic CT
and MRI.
There is a limitation that the analysis time is from
the R wave to AVC in one cardiac cycle, which corresponds to the
maximum inspiratory slope under M-mode US, and the results only
reflect diaphragm deformation of this short time period. These
results do not represent the maximum deformation of the diaphragm
in an entire inspiratory phase. One potential solution for this
limitation is to develop new specialized software that is triggered
by the breathing cycle to allow for a simple, fast, accurate and
reproducible measurement of diaphragm deformation. Another
limitation of this study is that it was performed on only 21
healthy volunteers without grouping according to age and gender.
Although it is difficult to draw major conclusions on such small
numbers, we consider that based on these preliminary results, 2D
strain US speckle tracking has the potential to detect deformation
of the diaphragm. All analyses were performed by one skilled US
expert; therefore, the intra- and inter-observer variability is
unknown. Further studies on diaphragm speckle tracking compared
with sonomicrometer or MRI tagging as a reference are required to
validate the precision of this technique for measurement of
diaphragm mechanics.
In conclusion, we have demonstrated the potential
application of 2D strain US speckle tracking in the evaluation of
right diaphragm deformation, and shown that it is a promising new
tool for the quantification of diaphragm function. The method is
safe and may enhance our understanding and diagnosis of abnormal
diaphragm mechanics in pulmonary disease. Further studies for
tracking diaphragm strain in a larger number of patients with
obstructive or restrictive lung disease, receiving mechanical
ventilation or before and after thorax or abdominal surgery are
required.
References
|
1.
|
Downey R: Anatomy of the normal diaphragm.
Thorac Surg Clin. 21:273–279. 2011. View Article : Google Scholar
|
|
2.
|
Poole DC, Sexton WL, Farkas GA, Powers SK
and Reid MB: Diaphragm structure and function in health and
disease. Med Sci Sports Exerc. 29:738–754. 1997. View Article : Google Scholar : PubMed/NCBI
|
|
3.
|
Maish MS: The diaphragm. Surg Clin North
Am. 90:955–968. 2010. View Article : Google Scholar
|
|
4.
|
Kamata S, Usui N, Sawai T, Nose K,
Kamiyama M and Fukuzawa M: Radiographic changes in the diaphragm
after repair of congenital diaphragmatic hernia. J Pediatr Surg.
43:2156–2160. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
5.
|
Plathow C, Fink C, Ley S, et al:
Measurement of diaphragmatic length during the breathing cycle by
dynamic MRI: comparison between healthy adults and patients with an
intrathoracic tumor. Eur Radiol. 14:1392–1399. 2004. View Article : Google Scholar
|
|
6.
|
Chen M and Siochi RA: Diaphragm motion
quantification in megavoltage cone-beam CT projection images. Med
Phys. 37:2312–2320. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
7.
|
Gethin-Jones TL, Noble VE and Morse CR:
Quantification of diaphragm function using ultrasound: evaluation
of a novel technique. Ultrasound Med Biol. 36:1965–1969. 2010.
View Article : Google Scholar : PubMed/NCBI
|
|
8.
|
Gerscovich EO, Cronan M, McGahan JP, Jain
K, Jones CD and McDonald C: Ultrasonographic evaluation of
diaphragmatic motion. J Ultrasound Med. 20:597–604. 2001.PubMed/NCBI
|
|
9.
|
Testa A, Soldati G, Giannuzzi R, Berardi
S, Portale G and Gentiloni Silveri N: Ultrasound M-mode assessment
of diaphragmatic kinetics by anterior transverse scanning in
healthy subjects. Ultrasound Med Biol. 37:44–52. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
10.
|
Ayoub J, Cohendy R, Dauzat M, et al:
Non-invasive quantification of diaphragm kinetics using m-mode
sonography. Can J Anaesth. 44:739–744. 1997. View Article : Google Scholar : PubMed/NCBI
|
|
11.
|
Houston JG, Angus RM, Cowan MD, McMillan
NC and Thomson NC: Ultrasound assessment of normal
hemidiaphragmatic movement: relation to inspiratory volume. Thorax.
49:500–503. 1994.PubMed/NCBI
|
|
12.
|
Gilman G, Khandheria BK, Hagen ME, Abraham
TP, Seward JB and Belohlavek M: Strain rate and strain: a
step-by-step approach to image and data acquisition. J Am Soc
Echocardiogr. 17:1011–1020. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
13.
|
Dandel M, Lehmkuhl H, Knosalla C,
Suramelashvili N and Hetzer R: Strain and strain rate imaging by
echocardiography - basic concepts and clinical applicability. Curr
Cardiol Rev. 5:133–148. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
14.
|
Nason LK, Walker CM, McNeeley MF, Burivong
W, Fligner CL and Godwin JD: Imaging of the diaphragm: anatomy and
function. Radiographics. 32:E51–E70. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
15.
|
Cohen E, Mier A, Heywood P, Murphy K,
Boultbee J and Guz A: Diaphragmatic movement in hemiplegic patients
measured by ultrasonography. Thorax. 49:890–895. 1994. View Article : Google Scholar : PubMed/NCBI
|
|
16.
|
Kleinman BS, Frey K, VanDrunen M, et al:
Motion of the diaphragm in patients with chronic obstructive
pulmonary disease while spontaneously breathing versus during
positive pressure breathing after anesthesia and neuromuscular
blockade. Anesthesiology. 97:298–305. 2002. View Article : Google Scholar
|
|
17.
|
Boussuges A, Gole Y and Blanc P:
Diaphragmatic motion studied by m-mode ultrasonography: methods,
reproducibility, and normal values. Chest. 135:391–400. 2009.
View Article : Google Scholar : PubMed/NCBI
|
|
18.
|
Perk G, Tunick PA and Kronzon I:
Non-Doppler two-dimensional strain imaging by echocardiography -
from technical considerations to clinical applications. J Am Soc
Echocardiogr. 20:234–243. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
19.
|
Boriek AM, Wilson TA and Rodarte JR:
Displacements and strains in the costal diaphragm of the dog. J
Appl Physiol. 76:223–229. 1994.PubMed/NCBI
|
|
20.
|
Suzuki M, Suzuki S, Akahori T, et al:
Patterns of inspiratory muscle shortening during hypoxia and
hypercapnia in dogs. Eur Respir J. 10:430–436. 1997. View Article : Google Scholar : PubMed/NCBI
|