Introduction
Hepatic encephalopathy (HE) is a clinical
neuro-psychiatric syndrome based on metabolic disturbances and
caused by severe liver diseases and/or portal-systemic shunts. The
World Congress of Gastroenterology (WCOG) in Vienna classified HE
into types A, B and C depending on the nature of hepatic
disturbances or dysfunctions (1).
Type A describes HE associated with acute liver failure and type B
includes HE associated with portal-systemic bypass. Type C, the
most common, is HE associated with cirrhosis and portal
hypertension and/or portal-systemic shunts, and may also be
subdivided into minimal hepatic encephalopathy (MHE) and
symptomatic hepatic encephalopathy (SME) according to the clinical
manifestations.
Alcoholic liver disease is common in certain
countries, but viral hepatitis-associated cirrhosis is more
prevalent in China. Notably, the incidence of drug-induced liver
disease is increasing (2). Many
patients may develop fibrosis, or even cirrhosis, and may
subsequently develop certain complications of cirrhosis, including
HE.
There are a number of potential precipitating
factors contributing to HE in patients with end-stage cirrhosis.
The most common precipitating factor is gastrointestinal bleeding,
which leads to the increased production of proteins and,
consequently, the increased production of nitrogenous products,
particularly ammonia, in the gut. Other precipitating factors
include constipation, excessive dietary protein, shock,
hyponatremia, hypokalemia, alkalosis and certain sedatives
(3). In the majority of cases, HE
is caused by a single precipitating factor. Treatment or removal of
the precipitating factor may allow the patient to recover from HE
within 12–24 h. Shawcross et al observed that infection is a
frequent precipitating factor of HE in cirrhosis and also revealed
an association between infection and systemic inflammation, but not
ammonia, in cirrhotic patients that develop severe HE (4).
Patients with serious liver disease often acquire
serious infections and endotoxic blood diseases, including
spontaneous bacterial peritonitis (SBP), sepsis, pneumonia and
urinary tract infections, due to a weakened mononuclear macrophage
system. These infections and endotoxic diseases aggravate liver
damage and increase ammonia production. Bacterial infection is a
main cause of mortality in cirrhotic patients with HE (5). At present, the removal of the
precipitating agent is regarded as the primary approach for
preventing HE. In the current study, 137 patients had clear
precipitating factors of HE and the encephalopathy subsided
following the resolution of the precipitating problem. A number of
studies have focused on the infection precipitating HE, however,
the sites of infection remain controversial (4,6,7). Our
previous study demonstrated that infection was a common
precipitating factor for the development of HE in patients with
hepatitis B virus-related cirrhosis (HBC) (8). In the present study, we aimed to
clarify the differences in the main infection sites between HE
patients with cirrhosis induced by hepatitis B virus and those with
cirrhosis induced by alcohol.
In this study, we analyzed infection as a
precipitating factor of HE, in order to identify the most common
infection site and the etiology. The findings may aid in the early
diagnosis and prevention of HE and the identification of effective
treatments.
Materials and methods
Patients
A total of 92 inpatients with HE caused by HBC, who
were treated at the Department of Gastroenterology (First
Affiliated Hospital of Dalian Medical University, Dalian, China)
were enrolled in the HBC-HE group according to the exclusion
criteria. From March 2003 to October 2012, 45 inpatients with HE
caused by alcoholic liver disease (ALD) were selected as a control
group (ALD-HE). The patients in the two groups received the same
treatment, regained recognizable signs of awareness following the
administration of therapies including oxygen inhalation,
hepatoprotectants, diuretics and antiencephalopathic agents, and
complications were prevented.
The diagnosis of HBC and alcoholic cirrhosis were
based on patient history, physical examination, liver imaging and
laboratory findings. The diagnosis of alcoholic cirrhosis was also
carried out according to the Alcoholic Liver Disease Diagnosis and
Treatment Guidelines (9). The
diagnosis of HE was made according to the recommendations of the
working party of the 11th World Congress of Gastroenterology and
the diagnosis of HE grades was based on the West Haven criteria
(1). The investigation conformed
to the principles outlined in the Declaration of Helsinki and was
approved by the ethics committee of The First Affiliated Hospital
of Dalian Medical University. All participants in the study
provided informed written consent.
Exclusion criteria
The patients were excluded if they had the
following: i) severe cerebrovascular, heart, lung or renal disease,
intracranial tumor or infection; ii) craniocerebral disease,
epilepsy, psychosis, coma or mental disorder due to other causes;
iii) metabolic or toxic encephalopathy (e.g., uremia, hypoglycemia
or diabetes); iv) mortality following treatment; v) abdominal
surgery history (e.g., upper digestive tract sclerosis surgery,
splenectomy, portal-systemic shunt or portal-systemic
disconnection) or had undergone treatments using an artificial
liver support system or for hepatic cancer.
Data collection
We collected and classified the clinical data
including gender, age and precipitating factor of HE. The
laboratory test report further confirmed the sites of infection.
White blood cell (WBC) counts, neutrophil (NEUT) numbers, plasma
ammonia levels and bacterial culture results were also recorded in
this study.
Statistics
SPSS 11.5 software (SPSS, Inc., Chicago, IL, USA)
was used for statistical analysis. Measurement data and qualitative
data were expressed as mean ± standard deviation (SD) and
frequency, respectively. Differences between the two groups were
evaluated by an independent sample Student’s t-test. Percentages
were used to analyze constituent ratio and a χ2 test was
used for qualitative data. P<0.05 was considered to indicate a
statistically significant result.
Results
Incidence of HE precipitating factors in
patients with cirrhosis
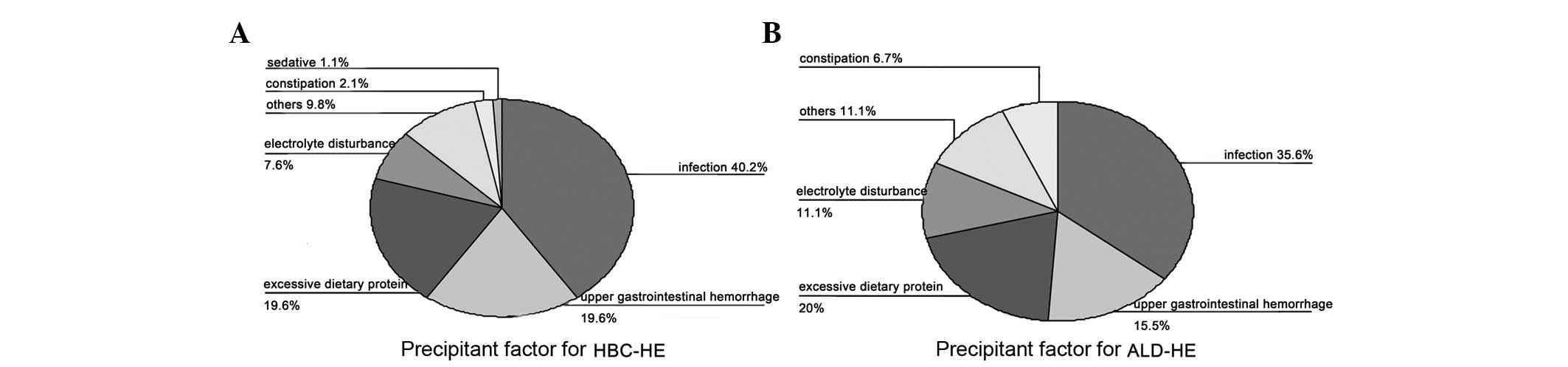
Analysis of the proportions of various precipitating
factors in the HBC-HE group showed that infection was the most
common precipitating factor (40.2%), followed by upper
gastrointestinal hemorrhage (19.6%), excessive dietary protein
(19.6%), electrolyte disturbance (7.6%), constipation (2.1%),
certain sedatives (1.1%) and others (9.8%; Fig. 1A).
In the ALD-HE group, infection was observed to be
the primary precipitating factor (35.6%), followed by upper
gastrointestinal hemorrhage (15.5%), excessive dietary protein
(20%), electrolyte disturbance (11.1%), constipation (6.7%) and
others (11.1%; Fig. 1B).
In the infection group Child-Pugh class A, B and C
accounted for 12, 30 and 11 patients, respectively. Ascites and
splenomegaly were observed in 44 (83.02%) and 48 patients (90.57%),
respectively. These were significantly different to the incidences
in the non-infection group (P<0.05; Table I). Infection was the precipitating
factor for 37 cases (40.2%), in the HBC-HE group and 16 cases in
the ALD-HE group (35.6%; P>0.05). Gender, age and the incidence
of gastroesophageal varices were not significantly different
between the infection and non-infection groups (Table I).
 | Table I.Comparison of clinical features
between the infection and non-infection groups. |
Table I.
Comparison of clinical features
between the infection and non-infection groups.
| Clinical feature | Infection (n=53) | Non-infection
(n=84) | P-value |
|---|
| HBC-HE/ALD-HE | 37/16 | 55/29 | 0.599 |
| Gender
(male/female) | 36/17 | 53/31 | 0.564 |
| Age (years) | 60.01±11.99 | 67.23±10.32 | 0.187 |
| Child-Pugh class
(A/B/C) | 12/30/11 | 39/33/12 | 0.007 |
| Ascites, n (%) | 44 (83.02) | 53 (63.10) | 0.012 |
| Gastroesophageal
varices, n (%) | 39 (73.58) | 60 (71.43) | 0.784 |
| Splenomegaly, n
(%) | 48 (90.57) | 56 (66.67) | 0.001 |
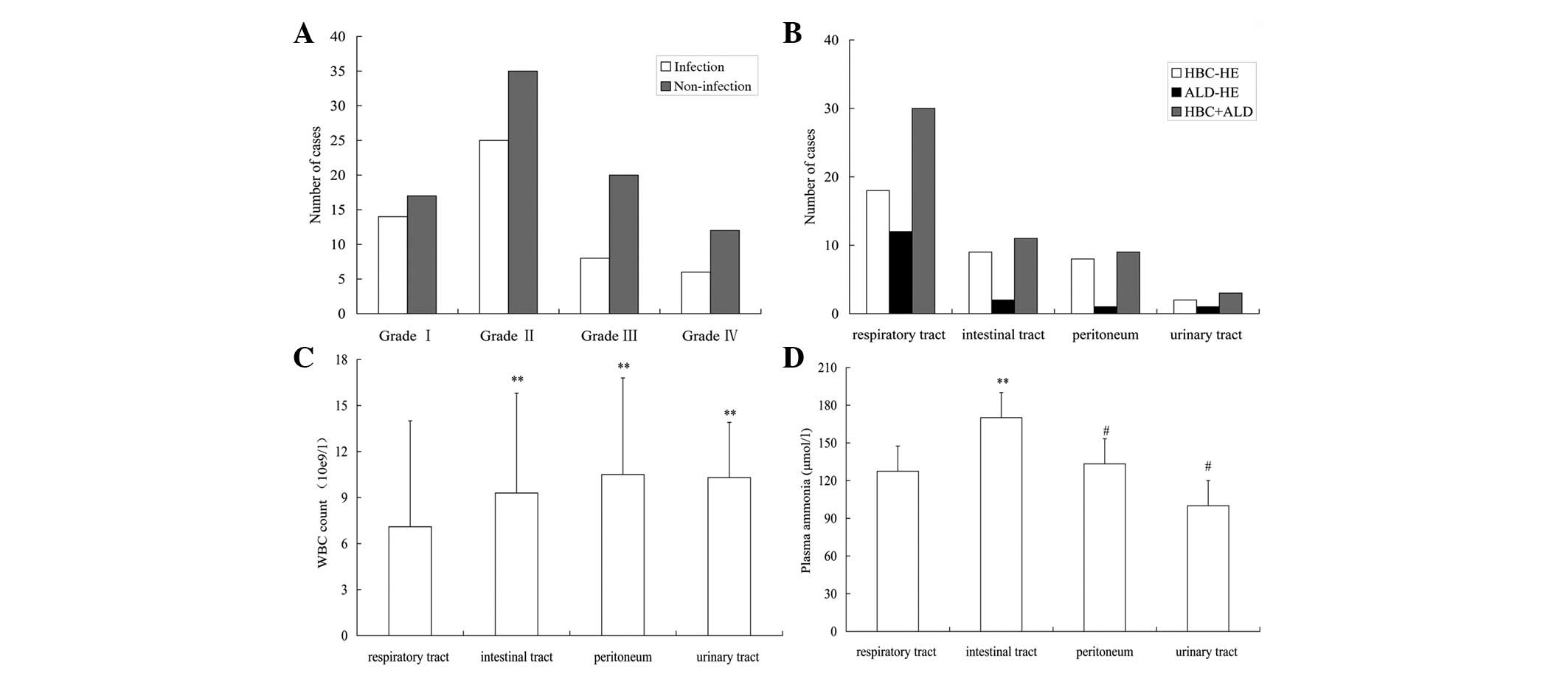
The grades of HE according to the West Haven
criteria were grade I in 14 (26.4%), grade II in 25 (47.2%), grade
III in 8 (15.1%) and grade IV in 6 (11.3%) patients in the
infection group. In the non-infection group, grade I HE was
observed in 17 patients (20.2%), grade II in 35 (41.7%), grade III
in 20 (23.8%) and grade IV in 12 (14.3%; Fig. 2A). There were no significant
differences in HE grades among patients with different infection
sites (P=0.233; Table II).
| Table II.Comparison of hepatic encephalopathy
(HE) grades in patients with different sites of infection. |
Table II.
Comparison of hepatic encephalopathy
(HE) grades in patients with different sites of infection.
| Infection site | n | Grade I (n=14) n
(%) | Grade II (n=25) n
(%) | Grade III (n=8) n
(%) | Grade IV (n=6) n
(%) | P-value |
|---|
| | | | | | 0.233 |
| Respiratory
tract | 30 | 8 (26.7) | 17 (56.7) | 4 (13.3) | 1 (3.3) | |
| Intestinal
tract | 11 | 3 (27.3) | 5 (45.5) | 2 (18.2) | 1 (9.1) | |
| Peritoneum | 9 | 1 (11.1) | 2 (22.2) | 2 (22.2) | 4 (44.4) | |
| Urinary tract | 3 | 2 (66.7) | 1 (33.3) | 0 (0.0) | 0 (0.0) | |
Distribution of infection sites in
cirrhosis with HE
There were 53 patients with HE who had infection as
a precipitating factor. The infections were observed in the
respiratory tract in 30 cases (56.6%), intestinal tract in 11 cases
(20.7%), peritoneum in 9 cases (17.0%) and urinary tract in 3 cases
(5.7%; Fig. 2B). The number of
intestinal tract infections was increased compared with peritoneum
infections (P<0.01; Fig. 2B).
The number of patients who presented with infection at one of the
four sites was greater in the HBC-HE group than in the ALD-HE
group, however the difference was not statistically significant
(P>0.05).
For the HBC-HE and ALD-HE groups, the incidences of
respiratory tract infection (n=18, 48.6% and n=12, 75%,
respectively), intestinal tract infection (n=9, 24.3% and n=2,
12.5%, respectively), peritoneal infection (n=8, 21.6% and n=1,
6.2% respectively) and urinary tract infection (n=2, 5.4% and n=1,
6.2%, respectively) were not statistically significant between the
groups (P>0.05; Fig. 2B).
WBC count and plasma ammonia in cirrhosis
with HE with different infection sites
The comparison of WBC counts in HE patients with
different infection sites determined by blood cell analysis showed
that the WBC count was significantly lower in patients with
respiratory tract infection compared with those in patients with
infections in the intestinal tract (P=0.037), peritoneum (P=0.029)
and urinary tract (P=0.032). There were no significant differences
of WBC count among patients with intestinal tract, peritoneum and
urinary tract infections (P>0.05; Fig. 2C).
There were 53 (38.7%) cases with infection as a
precipitating factor out of a total of 137 cases as determined by
blood cell analysis, including cases with increased WBC counts
(n=17, 32.1%), normal WBC counts (n=24, 45.3%) and decreased WBC
counts (n=12, 22.6%). The majority of the 53 patients with
infection had an increased neutrophil count (NEUT; n=39, 73.6%).
Compared with the non-infection group, the infection group had a
significantly greater incidence of increased NEUT count cases
(χ2=59.173, P<0.0001; Table III).
| Table III.Comparison of biochemical
characteristics between the infection and non-infection groups. |
Table III.
Comparison of biochemical
characteristics between the infection and non-infection groups.
| Biochemical
characteristics | Infection (n=53) n
(%) | Non-infection
(n=84) n (%) | P-value |
|---|
| Hyperammonemia | 49 (92.45) | 64 (76.19) | 0.015 |
| Increased NEUT | 39 (73.58) | 8 (9.52) | <0.0001 |
|
Hyperbilirubinemia | 24 (45.28) | 35 (41.67) | 0.677 |
| Hyponatremia | 40 (75.47) | 39 (46.43) | 0.001 |
| Low albumin | 42 (79.25) | 53 (63.1) | 0.046 |
| Long PT (%) | 34 (64.15) | 50 (59.52) | 0.588 |
Notably, the incidence of hyperammonemia in the
infection group was higher than that in the non-infection group (P=
0.015; Table III). The levels of
plasma ammonia were greatly increased when the infection was in the
intestinal tract compared with when it was in the peritoneum,
respiratory tract or urinary tract (Fig. 2D).
Hyponatremia and low albumin were more common in the
infection group (75.47 and 79.25%, respectively) than in the
non-infection group (46.43 and 63.1%, respectively; Table III). However, there were no
significant differences between the proportions of cases with
hyperbilirubinemia and long prothrombin time (PT) between the two
groups (P>0.05; Table III).
Etiology of infection at different
sites
Pneumococci and Pseudomonas aeruginosa were
the most commonly identified pathogenic bacteria (40 and 53.33%,
respectively) in respiratory tract infection in liver cirrhotic
patients with HE. E. coli was the most prevalent pathogenic
bacteria identified in the intestinal tract, peritoneum and urinary
tract infections in these patients (Table IV).
| Table IV.Comparison of etiology at different
infection sites. |
Table IV.
Comparison of etiology at different
infection sites.
| Infection site | n | Etiology (n,
%) |
|---|
| Respiratory
tract | 30 | Pneumococci (12,
40.00) |
| Pseudomonas
aeruginosa (16, 53.33) |
| Other (2,
6.67) |
| Intestinal
tract | 11 | E. coli (7,
63.64) |
| Clostridium
perfringens (3, 27.27) |
| Other (1,
9.09) |
| Peritoneum | 9 | E. coli (7,
77.78) |
| Other (2,
22.22) |
| Urinary tract | 3 | E. coli (3,
100.00) |
Discussion
HE is a common complication of posthepatitic
cirrhosis and severe hepatitis, and it is the most common cause of
mortality in cirrhotic patients (10). HE may be induced by a variety of
factors and the recognition of precipitating factors and their
correction or early removal is regarded as the primary approach for
improving prognosis and reducing mortality.
In the current study, infection was a common
precipitating factor, in addition to upper gastrointestinal
hemorrhage, excessive dietary protein, electrolyte disturbance,
constipation and sedatives. A previous study also showed that
infection and upper gastrointestinal hemorrhage were primary
precipitating factors in patients with HE (11). We observed that infection was a
main precipitating factor for HE, with an incidence of 40.2% in the
HBC-HE group and 35.6% in the ALD-HE group. It has been reported
that upper gastrointestinal hemorrhage is the most common
precipitating factor in cirrhotic patients (12). However, infection was the most
common precipitating factor identified in the present study. This
difference may be due to dietary habits, living environment and
etiology in different regions. In our routine treatment, a
prevention strategy for HE was often performed, so the incidence of
HE in patients with upper gastrointestinal hemorrhage was less than
that which would otherwise occur. In addition, only HBC-HE and
ALD-HE patients were selected for this study, so the results may
have limited etiology. In addition, we also observed the proportion
of upper gastrointestinal hemorrhage was 19.6% in the HBC-HE group
and 15.5% in the ALD-HE group. Portal hypertension may occur
earlier in HBC-HE group than in the ALD-HE group and lead to
increased upper gastrointestinal hemorrhage. The lower number of
ALD-HE cases may be another reason for the difference in
results.
Oxidative/nitrosative stress and a low-grade
cerebral edema are key events in the pathogenesis of ammonia
toxicity and hepatic encephalopathy (13). Patients with advanced liver disease
are susceptible to infection due to a dysfunction of host defense
mechanisms (14).
Infection/systemic inflammatory response has been reported to
contribute to the exacerbation of HE in patients with
acetaminophen-induced acute liver failure (15). The peripheral immune system
normally produces various pro-inflammatory cytokines, including
interleukin-1β (IL-1β), IL-6 and tumor necrosis factor-α (TNF-α)
during infection. These peripheral cytokines may either directly
cross the blood-brain barrier or indirectly signal the brain to
interact with circumventricular organs, and activate afferent
neurons of the vagus nerve via other informational substances
(16). Another study clarified
that IL-1 or TNF-α receptor gene deletions delayed the onset of
encephalopathy and attenuated brain edema in experimental acute
liver failure (17). In addition,
mild hypothermia resulted in reduced expression of circulating
proinflammatory cytokines, improved neurological function,
normalized glutathione levels and attenuated hepatic damage
(17). This suggests that
infection/systemic inflammatory response is a key factor
contributing to HE (Fig. 3).
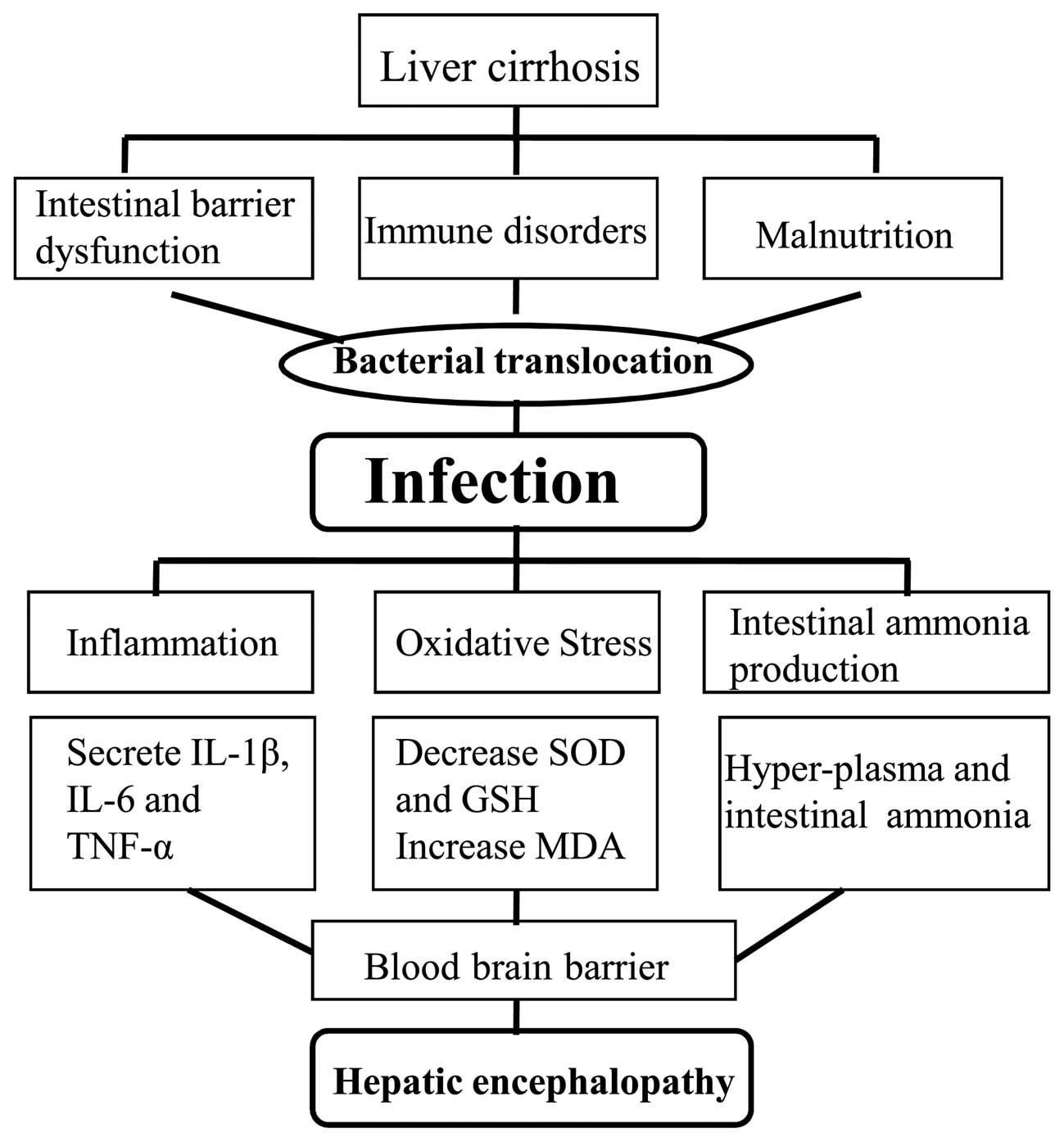 | Figure 3.Infection-induced hepatic
encephalopathy in liver cirrhosis. Patients with liver cirrhosis
develop intestinal barrier dysfunction, immune disorders and
malnutrition due to portal hypertension. Bacteria then invade the
body via the respiratory, intestinal and urinary tracts and result
in various infections. Infection may activate inflammatory reaction
and oxidative stress, and cause the secretion of several cytokines,
including IL-1β, IL-6 and TNF-α. Reduced cerebral SOD levels and
increased production of intestinal ammonia is observed in patients
with HE. These inflammatory mediators selectively cross the
blood-brain barrier and lead to hepatic encephalopathy (brain
injury, edema). IL-1β, interleukin-1β; TNF-α, tumor necrosis
factor-α; SOD, superoxide dismutase; GSH, glutathione; MDA,
malondialdehyde; HE, hepatic encephalopathy. |
Non-steroidal anti-inflammatory drugs (NSAIDs), such
as ibuprofen, may reduce hypokinesia and microglial activation,
thereby restoring normal motor activity and cognitive function in
rats with HE (18,19). These results may further support
the role of inflammation in the induction of HE.
In addition, patients with liver cirrhosis are
abnormally susceptible to infection as a result of immunological
deficits. The mechanisms of action include reduced hepatic
production of complement (reduced C3 and C5 levels), impaired
phagocytosis of Kupffer cells and clearance of inflammatory
cytokines, and altered neutrophil chemotaxis (20). In the liver, the function of
reticuloendothelial cells is to remove bacteria from the blood. The
activation of macrophages in cirrhosis is dysfunctional and the
sterilization ability reduced, leading to a dysfunction of the
reticuloendothelial system. Shawcross et al demonstrated
that downregulation of HLA-DR expression on monocytes resulted in
immunogical deficits in decompensated liver cirrhosis (21).
Astrocytes and endothelial cells are able to release
a variety of inflammatory cytokines, which lead to intracranial
hypertension and brain edema when the body is in infection status.
NSAIDs have been reported to ameliorate intracranial hypertension
and brain edema in patients and rats with HE due to a portacaval
shunt (22).
Shawcross et al (23) proposed that systemic inflammation
exacerbates the neuropsychological alterations induced by
hyperammonemia. Previous studies have shown that inflammation and
ammonia act synergistically to exacerbate HE symptoms (24–26).
Ammonia contributes to neutrophil swelling and phagocytosis
dysfunction (27). In the current
study, we observed that the majority of cirrhotic patients with HE
due to infection had hyperammonemia. In addition, the levels of
plasma ammonia were greatly increased in patients with intestinal
tract infection compared with those in patients with infections at
other sites. We suggest that intestinal tract infection may lead to
hyperammonemia in these patients by increasing the production of
intestinal ammonia. Neutrophils are an important component of the
body’s immune system. High levels of ammonia have been demonstrated
to induce neutrophil swelling and impaired neutrophil phagocytosis,
resulting in neutrophil dysfunction in rats fed an ammoniagenic
diet and in patients with cirrhosis (28). Patients with acute-on-chronic liver
failure had a similar degree of depression of cellular immunity and
monocyte levels, which contributed to the increased infection
morbidity of these patients (29,30).
In a previous study, Child-Pugh class C cirrhotic patients that
presented with downregulation of HLA-DR expression on monocytes
exhibited immune dysfunctions (31). Consequently, infection-enhancing
catabolism led to an increasing production of ammonia; therefore,
the prevention and control of infection may reduce the incidence of
HE in cirrhotic patients.
The incidence of infection in patients with HBC-HE
and ALD-HE remains uncertain. With a group of 382 cirrhotic
inpatients, Rosa et al (32) demonstrated that alcoholic patients
with Child-Pugh class A/B disease were more susceptible to
infection compared with nonalcoholic patients, but in those
patients with Child-Pugh class C disease, no statistical difference
was observed in the infection or mortalities between alcoholics and
nonalcoholics. Borzio et al (33) demonstrated that the infection rate
was not statistically different between alcoholic patients and
HBC-HE patients with advanced cirrhosis, and was associated more
closely with the severity than with the etiology of the hepatic
disease. There was no statistical difference in the incidence of
infection between the HBC-HE and the ALD-HE groups in this study.
This may be due to the relatively smaller number of alcoholic
patients (45 cases) enrolled, and therefore a larger number of
cases should be collected for further study. The mechanism by which
alcoholic patients become more susceptible to infection and
endoxemia may be through alcohol-induced damage to the immune
system.
A previous study reported that spontaneous bacterial
peritonitis (SBP) is currently the most frequent infection in
cirrhosis (6). A domestic clinical
study revealed that pulmonary infection was the most common,
followed by peritoneal infection and urinary tract infection
(7). In a total of 53 cases of HE
with infection in the current study, we observed that respiratory
tract infection (n=30, 56.6%) was the primary precipitating factor,
followed by intestinal infection (n=11, 20.7%), peritoneal
infection (n=9, 17.0%) and urinary tract infection (n=3, 5.7%). The
result was not in accordance with the findings of previous studies
which reported that SBP was the primary precipitating factor in
cirrhotic patients with HE due to infection. This may be due to
differences in etiologies, Child-Pugh classes, treatments, regions
and ethnic origins. Bacterial overgrowth, intestinal motility and
barrier dysfunction were conducive to bacterial translocation
leading to bacteremia. The mononuclear phagocyte system is
suppressed and the ability of the liver to remove bacteria
declines, leading to reductions in immunoglobulin, complement and
albumin and ultimately results in ascites infection (34). The risk for SBP in cirrhotic
patients with ascites was associated with Child-Pugh class and
patients with Child-Pugh class C disease were susceptible to
peritoneal infection (35). A
greater number of Child-Pugh class A/B patients and fewer
Child-Pugh class C patients were enrolled in our study. In
addition, a high proportion of grade II (47.2%) patients with HE
had infection as a precipitating factor.
A significantly lower WBC count was observed in the
patients with respiratory tract infection than in patients with
infection at other sites. Respiratory infection included upper and
lower respiratory tract infection, and viral infection was more
common in the upper respiratory tract, which is likely to cause the
WBC count to decrease. However, in the current study, the
intestinal tract, peritoneum and urinary tract presented with more
bacterial infections, which led to an increased WBC count. The WBC
count increased in 32.1% of the patients with HE due to infection
in our study. In addition, NEUT counts were significantly different
between the infection and non-infection cases and, as expected, the
NEUT count increased in infection cases. Fewer patients with
bacterial infection had a high WBC count, due to immune dysfunction
and hypersplenism. Therefore, doctors may not make a diagnosis on
the basis of WBC count changes and left shift should be observed in
cirrhotic patients with complicated infectious diseases.
Shawcross et al also observed that grade
III/IV encephalopathy correlates with the presence of systemic
inflammatory response syndrome (SIRS) and not with ammonia
(4). We observed in the present
study that the grade of encephalopathy had no significant
association with different infection sites.
Ascites, hyponatremia and low albumin were common in
the infection group. Cirrhotic patients with ascites are
susceptible to bacterial infection which develops into SBP and is
predominantly caused by enteric organisms (36). Hyponatremia is common in patients
with cirrhosis and correlates with the complications of cirrhosis,
including hepatorenal syndrome, encephalopathy and SBP (37). In cirrhotic patients with ascites,
∼50% have a certain degree of hyponatremia (38). Hyponatremia complicates the
management of cerebral edema and increases the risk of developing
or exacerbating HE (39). Serum
sodium and ammonia levels are major factors determining
electroencephalographic abnormalities in cirrhosis (40). In a previous study, serum sodium
was an independent predictive factor of HE in patients with
cirrhosis (41). In addition,
there was a close association between hyponatremia and HE, which
was in accordance with other studies (39).
Enteric gram-negative cocci have been reported to be
the microorganisms most frequently isolated in SBP patients with
hospital-acquired infections (42). We observed that E. coli was
a prevalent bacteria in intestinal tract, peritoneum and urinary
tract infections.
In conclusion, respiratory infection was a common
precipitating factor for HE in patients with cirrhosis. The WBC
count was not always increased in cirrhotic patients with HE
induced by infection. An increased WBC count combined with left
shift may indicate the occurrence of infection. As a retrospective
analysis, the number of cases was inadequate and the study lacked
patients with other types of cirrhosis. The control of respiratory
tract infection is pivotal in the prevention and treatment of HE in
the future. Mortality from HE is likely to decrease due to early
diagnosis, the use of appropriate antibiotic therapy and albumin
administration.
Acknowledgements
The study was supported by the
National Natural Science Foundation of China, No. 30970886; and the
Science, Technology Project of Dalian, No. 2010E15SF179 and
Doctoral initial funding of Liaoning province, No. 20121110.
References
|
1.
|
Ferenci P, Lockwood A, Mullen K, Tarter R,
Weissenborn K and Blei AT: Hepatic encephalopathy - definition,
nomenclature, diagnosis, and quantification: final report of the
working party at the 11th World Congresses of Gastroenterology,
Vienna, 1998. Hepatology. 35:716–721. 2002. View Article : Google Scholar
|
|
2.
|
Zhang FK, Zhang JY and Jia JD: Treatment
of patients with alcoholic liver disease. Hepatobiliary Pancreat
Dis Int. 4:12–17. 2005.PubMed/NCBI
|
|
3.
|
Häussinger D: Hepatic encephalopathy. Acta
Gastroenterol Belg. 73:457–464. 2010.
|
|
4.
|
Shawcross DL, Sharifi Y, Canavan JB, et
al: Infection and systemic inflammation, not ammonia, are
associated with Grade 3/4 hepatic encephalopathy, but not mortality
in cirrhosis. J Hepatol. 54:640–649. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
5.
|
Bustamante J, Rimola A, Ventura PJ, et al:
Prognostic significance of hepatic encephalopathy in patients with
cirrhosis. J Hepatol. 30:890–895. 1999. View Article : Google Scholar : PubMed/NCBI
|
|
6.
|
Bellot P, Jara Pérez López N, Martínez
Moreno B and Such J: Current problems in the prevention and
treatment of infections in patients with cirrhosis. Gastroenterol
Hepatol. 33:729–740. 2010.(In Spanish).
|
|
7.
|
Zhuang J: 52 cases analysis of
precipitating factors in cirrhosis with hepatic encephalopathy. J
Clin Hepatol. 10:57–58. 2007.(In Chinese).
|
|
8.
|
Zhang M and Duan ZJ: Retrospective
analysis of factors influencing the development and progression of
hepatic encephalopathy in patients with hepatitis B virus related
cirrhosis. Shi Jie Hua Ren Xiao Hua Za Zhi. 20:1148–1155. 2012.(In
Chinese).
|
|
9.
|
O’Shea RS, Dasarathy S, McCullough AJ, et
al Practice Guideline Committee of the American Association for the
Study of Liver Diseases; Practice Parameters Committee of the
American College of Gastroenterology: Alcoholic liver disease.
Hepatology. 51:307–328. 2010.
|
|
10.
|
Papadopoulos N, Soultati A, Goritsas C, et
al: Nitric oxide, ammonia, and CRP levels in cirrhotic patients
with hepatic encephalopathy: is there a connection? J Clin
Gastroenterol. 44:713–719. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
11.
|
Devrajani BR, Shah SZ, Devrajani T and
Kumar D: Precipitating factors of hepatic encephalopathy at a
tertiary care hospital Jamshoro, Hyderabad. J Pak Med Assoc.
59:683–686. 2009.PubMed/NCBI
|
|
12.
|
McAvoy HC and Hayes PC: Hepatic
encephalopathy. Medicine. 35:108–111. 2006. View Article : Google Scholar
|
|
13.
|
Häussinger D and Görg B: Interaction of
oxidative stress, astrocyte swelling and cerebral ammonia toxicity.
Curr Opin Clin Nutr Metab Care. 13:87–92. 2010.PubMed/NCBI
|
|
14.
|
Atluri DK, Prakash R and Mullen KD:
Pathogenesis, diagnosis, and treatment of hepatic encephalopathy. J
Clin Exp Hepatol. 1:77–86. 2011. View Article : Google Scholar
|
|
15.
|
Vaquero J, Polson J, Chung C, et al:
Infection and the progression of hepatic encephalopathy in acute
liver failure. Gastroenterology. 125:755–764. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
16.
|
Licinio J and Wong ML: Pathways and
mechanisms for cytokine signaling of the central nervous system. J
Clin Invest. 100:2941–2947. 1997. View Article : Google Scholar : PubMed/NCBI
|
|
17.
|
Bémeur C, Desjardins P and Butterworth RF:
Antioxidant and anti-inflammatory effects of mild hypothermia in
the attenuation of liver injury due to azoxymethane toxicity in the
mouse. Metab Brain Dis. 25:23–29. 2010.PubMed/NCBI
|
|
18.
|
Cauli O, Rodrigo R, Piedrafita B, Llansola
M, Mansouri MT and Felipo V: Neuroinflammation contributes to
hypokinesia in rats with hepatic encephalopathy: ibuprofen restores
its motor activity. J Neurosci Res. 87:1369–1374. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
19.
|
Rodrigo R, Cauli O, Gomez-Pinedo U, et al:
Hyperammonemia induces neuroinflammation that contributes to
cognitive impairment in rats with hepatic encephalopathy.
Gastroenterology. 139:675–684. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
20.
|
Karvellas CJ, Pink F, McPhail M, et al:
Bacteremia, acute physiology and chronic health evaluation II and
modified end stage liver disease are independent predictors of
mortality in critically ill nontransplanted patients with
acute-on-chronic liver failure. Crit Care Med. 38:121–126.
2010.
|
|
21.
|
Shawcross DL, Olde Damink SW, Butterworth
RF and Jalan R: Ammonia and hepatic encephalopathy: the more things
change, the more they remain the same. Metab Brain Dis. 20:169–179.
2005. View Article : Google Scholar : PubMed/NCBI
|
|
22.
|
Cauli O, Rodrigo R, Piedrafita B, Boix J
and Felipo V: Inflammation and hepatic encephalopathy: ibuprofen
restores learning ability in rats with portacaval shunts.
Hepatology. 46:514–519. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
23.
|
Shawcross DL, Davies NA, Williams R and
Jalan R: Systemic inflammatory response exacerbates the
neuropsychological effects of induced hyperammonemia in cirrhosis.
J Hepatol. 40:247–254. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
24.
|
Blei AT: Infection, inflammation and
hepatic encephalopathy, synergism redefined. J Hepatol. 40:327–330.
2004. View Article : Google Scholar : PubMed/NCBI
|
|
25.
|
Shawcross DL, Wright G, Olde Damink SW and
Jalan R: Role of ammonia and inflammation in minimal hepatic
encephalopathy. Metab Brain Dis. 22:125–138. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
26.
|
Sharifi Y, Canavan JB, Yeoman AD, et al:
Defining the outcome, precipitants and cost of severe hepatic
encephalopathy (HE) in cirrhosis. Hepatology. 48(Suppl):
1061A2008.
|
|
27.
|
Shawcross DL, Shabbir SS, Taylor NJ and
Hughes RD: Ammonia and the neutrophil in the pathogenesis of
hepatic encephalopathy in cirrhosis. Hepatology. 51:1062–1069.
2010. View Article : Google Scholar : PubMed/NCBI
|
|
28.
|
Shawcross DL, Wright GA, Stadlbauer V, et
al: Ammonia impairs neutrophil phagocytic function in liver
disease. Hepatology. 48:1202–1212. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
29.
|
Wasmuth HE, Kunz D, Yagmur E, et al:
Patients with acute-on-chronic liver failure display ‘sepsis-like’
immune paralysis. J Hepatol. 42:195–201. 2005.
|
|
30.
|
Antoniades CG, Wendon J and Vergani D:
Paralysed monocytes in acute-on-chronic liver disease. J Hepatol.
42:163–165. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
31.
|
Lin CY, Tsai IF, Ho YP, et al: Endotoxemia
contributes to the immune paralysis in patients with cirrhosis. J
Hepatol. 46:816–826. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
32.
|
Rosa H, Silvério AO, Perini RF and Arruda
CB: Bacterial infection in cirrhotic patients and its relationship
with alcohol. Am J Gastroenterol. 95:1290–1293. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
33.
|
Borzio M, Salerno F, Piantoni L, et al:
Bacterial infection in patients with advanced cirrhosis: a
multicentre prospective study. Dig Liver Dis. 33:41–48. 2001.
View Article : Google Scholar : PubMed/NCBI
|
|
34.
|
Wiest R and Rath HC: Gastrointestinal
disorders of the critically ill. Bacterial translocation in the
gut. Best Pract Res Clin Gastroenterol. 17:397–425. 2003.
View Article : Google Scholar : PubMed/NCBI
|
|
35.
|
Andreu M, Sola R, Sitges-Serra A, et al:
Risk factors for spontaneous bacterial peritonitis in cirrhotic
patients with ascites. Gastroenterology. 104:1133–1138.
1993.PubMed/NCBI
|
|
36.
|
Bernardi M: Spontaneous bacterial
peritonitis: from pathophysiology to prevention. Intern Emerg Med.
5(Suppl 1): S37–S44. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
37.
|
Sigal SH: Hyponatremia in cirrhosis. J
Hosp Med. 7(Suppl 4): S14–S17. 2012. View
Article : Google Scholar
|
|
38.
|
Angeli P, Wong F, Watson H and Ginès P;
CAPPS Investigators: Hyponatremia in cirrhosis: Results of a
patient population survey. Hepatology. 44:1535–1542. 2006.
View Article : Google Scholar : PubMed/NCBI
|
|
39.
|
Häussinger D and Schliess F: Pathogenetic
mechanisms of hepatic encephalopathy. Gut. 57:1156–1165. 2008.
|
|
40.
|
Amodio P, Del Piccolo F, Pettenò E, et al:
Prevalence and prognostic value of quantified electroencephalogram
(EEG) alterations in cirrhotic patients. J Hepatol. 35:37–45. 2001.
View Article : Google Scholar : PubMed/NCBI
|
|
41.
|
Baccaro ME, Guevara M, Torre A, Arcos E,
Martin-Llahí M, Terra C, Gómez-Anson B, Rami L, Arroyo V and Ginès
P: Hyponatremia predisposes to hepatic encephalopathy in patients
with cirrhosis. Results of a prospective study with time-dependent
analysis. Hepatology. 44(Suppl 1): 233A2006.
|
|
42.
|
Fernández J, Navasa M, Gómez J, et al:
Bacterial infections in cirrhosis: epidemiological changes with
invasive procedures and norfloxacin prophylaxis. Hepatology.
35:140–148. 2002.PubMed/NCBI
|