Introduction
Primary percutaneous coronary intervention (PCI)
significantly improves the survival of patients with ST-segment
elevation myocardial infarction (STEMI) (1). However, post-procedural microvascular
obstruction, despite the presence of normal epicardial flow,
remains an important limitation of the procedure, which
substantially reduces the beneficial effects of PCI (2,3).
This complication occurs in 0.6–5% of elective PCIs but it may be
observed in up to 50% of primary PCI cases, involving the treatment
of thrombus-containing lesions (4).
An optimal standard treatment for no-reflow (NR) has
not yet been established. Based on the multifactorial pathogenesis
of NR during STEMI, a combination of mechanical and pharmacological
approaches appears to offer an enhanced solution for achieving the
desired microvascular reperfusion.
Thrombus-aspiration-assisted primary intervention
achieves complete ST-segment resolution (STR) in only 60% of
patients (5). Importantly, the
administration of current anti-platelet therapies during
reperfusion therapy for STEMI has not eliminated the NR phenomenon
(6). Nitroprusside (NTP) is an
alternative drug that is, at present, being used for the reversal
of the NR phenomenon. A study investigating the use of this agent
in the treatment of the NR phenomenon revealed some promising
preliminary results (7).
To date, to the best of our knowledge, there have
been no investigations into the combined strategy of thrombus
aspiration and tirofiban plus NTP. Thus, the aim of the present
prospective randomized control study was to assess the effect of
NTP in combination with the therapy currently considered the most
efficacious for STEMI, that is, thrombus aspiration and tirofiban,
in the prevention of NR.
Patients and methods
Study population
From January 2010 to December 2012, all consecutive
patients with STEMI occurring within 12 h of the onset of symptoms
who underwent emergency PCI in the Department of Cardiology of the
Second Hospital of Hebei Medical University (Shijiazhuang, China)
were enrolled in the study.
Inclusion criteria: i) Acute STEMI was diagnosed on
the basis of typical chest pain lasting >30 min; ii)
ST-elevation of ≥1 mm in at least two contiguous electrocardiogram
(ECG) leads and/or ≥2 mm in the precordial leads; iii) thrombolysis
in myocardial infarction (TIMI) flow ≤2 at baseline
angiography.
The exclusion criteria were: i) An age of >75
years; ii) cardiogenic shock (defined as a systolic blood pressure
of <90 mmHg for >30 min or the requirement for intravenous
pressors or intra-aortic balloon counter pulsation); iii) a history
of bleeding diathesis; iv) major surgery during the previous 6
weeks; v) gastrointestinal or genitourinary bleeding in the
preceding 6 months; vi) a cerebrovascular event in the previous
year; vii) a platelet count of <100,000/mm3; viii)
renal insufficiency, defined as a serum creatinine level of >2.5
mg/dl; ix) chronic hemodialysis or pregnancy; x) rescue
intervention following failed thrombolysis; xi) contraindications
to aspirin or clopidogrel; xii) inability to provide informed
consent.
Procedure
Following diagnostic coronary angiography, patients
who met the eligibility criteria were assigned in a 1:1 ratio into
two groups. Subsequent to wire crossing, thrombus aspiration was
performed. A ZEEK aspiration thrombectomy catheter (Zeon Medical
Inc., Tokyo, Japan) was removed from the body, flushed with
heparinized saline and subsequently reintroduced into the culprit
vessel beyond the occlusion site, prior to the selective
administration of intracoronary (IC) drugs. The drugs were infused
into the infarct-related artery (IRA) only if the distal vessels
were visualized following aspiration. Conversely, balloon
predilatation was permitted if thrombus aspiration was ineffective.
At this stage, prior to the coronary stent implantation, the
patient was randomly assigned either to group A (100 μg NTP
as a fast bolus, followed by 10 μg/kg tirofiban,
administered in 20 ml heparinized saline in 2 min as a slow bolus)
or group B (5 ml heparinized saline as a fast bolus followed by 10
μg/kg tirofiban, administered in 20 ml heparinized saline in
2 min as a slow bolus). In addition, the patients in the two groups
received a 12-h intravenous infusion of 0.15 μg/kg/min
tirofiban following angioplasty. If it was not possible to advance
the thrombus aspiration device in the culprit vessel for mechanical
reasons, drug administration was performed through a guiding
catheter following predilatation. Patients subject to this method
of administration were included in the overall and the subgroup
analyses. The data were analyzed according to the
intention-to-treat principle.
Following the injection, the surgeon proceeded with
the angioplasty in the usual fashion. Multiple types of balloons
and drug-eluting stents were used. For NR occurring during the
subsequent stages of the angioplasty, the surgeons used any drug
other than NTP. The ECG and blood pressure were monitored during
the procedure. Following the procedure, patients in either group
were treated with standard therapies for coronary heart disease,
including aspirin, clopidogrel, fluvastatin calcium, nitrate
esters, β-receptor antagonists and angiotensin converting enzyme
inhibitor/angiotensin II receptor blockers. All patients were
orally pretreated with 300 mg aspirin and 300 mg clopidogrel prior
to the procedure. The study was approved by the ethics committee of
the Second Hospital of Hebei Medical University, and each patient
provided written, informed consent.
For each patient, routine demographic and clinical
data, procedural results and in-hospital complications were
prospectively entered into a computerized databank. All data were
verified by a retrospective review of the patient records.
Study end-points
The following were the primary end-points of the
study: i) Coronary blood flow in the IRA subsequent to angioplasty,
as determined by the corrected TIMI frame count (CTFC) (8); ii) the proportion of patients with
TIMI myocardial perfusion grade (TMPG) 2–3 following the procedure
(9); iii) the proportion of
patients with complete STR at 90 min subsequent to the
intervention. CTFCs and MBG were assessed by two experienced
surgeons who were blinded to the study medications according to
standardized methods. The qualifying cine run was the first one
obtained following satisfactory relief of the epicardial culprit
stenosis. STR was measured immediately subsequent to the
angioplasty using a 12-lead ECG tracing by a separate investigator
who was blinded to the angiographic data. Complete STR was defined
as >70% reduction in the ST-segment elevation of the lead with
the highest elevation on admission.
Secondary end-points included the proportion of
patients with TIMI grade-3 (10)
flow following the procedure, left ventricular ejection fraction
(LVEF) and the combined rate of cardiac death, reinfarction and
target-vessel revascularization at 180 days.
Statistical analysis
Sample size was calculated for the first primary
end-point. To detect a difference in CTFC of 10 frames (11), assuming a standard deviation of 15
frames in each group with a=5% and power of 80%, 50 patients were
required to be randomized to each arm. Differences in the
end-points between the groups were compared using the Student’s
t-test for continuous variables and the χ2 test for
categorical data. Clinical follow-up data were obtained from the
composite clinical end-point and were analyzed using Kaplan-Meier
survival curve analysis, while differences between the groups were
compared using the log rank test. Statistical analysis was
performed using SPSS statistical software for Windows version 13.0
(SPSS, Inc., Chicago, IL, USA). P<0.05 was considered to
indicate a statistically significant difference.
Results
Baseline clinical and angiographic
characteristics
A total of 165 patients were randomized, among whom
three did not undergo primary PCI (two patients underwent an
emergency bypass procedure and one was excluded due to a lack of
consent). A total of 162 patients were included in the per-protocol
analysis.
The clinical and angiographic characteristics of the
patients are presented in Table I.
The age, gender distribution, incidence of coronary risk factors
and recanalization time from symptom onset, as well as the IRA and
pre-TIMI flow grade were similar between the two groups.
 | Table I.Baseline demographic and clinical
characteristics. |
Table I.
Baseline demographic and clinical
characteristics.
| Variables | Group A (n=80) | Group B (n=82) | t/χ2 | P-value |
|---|
| Age (years) | 63±9 | 64±10 | 0.668 | 0.500 |
| Male (%) | 63 (78.7) | 65 (79.2) | 0.010 | 0.910 |
| DM (%) | 16 (20.0) | 13 (15.9) | 0.226 | 0.630 |
| HTN (%) | 59 (73.7) | 67 (81.7) | 0.959 | 0.330 |
| Smokers (%) | 51 (63.7) | 51 (62.2) | 0.010 | 0.972 |
| Dyslipidemia (%) | 56 (70) | 52 (63.4) | 0.524 | 0.468 |
| Previous angina
(%) | 67 (83.7) | 69 (84.1) | 0.027 | 0.880 |
| Killip class (%) | | | 0.950 | 0.622 |
| I | 57 (71.3) | 60 (73.2) | | |
| II | 21 (26.2) | 18 (22.0) | | |
| III | 2 (2.5) | 4 (4.8) | | |
| SBP (mmHg) | 135±23 | 129±35 | 1.286 | 0.200 |
| DBP (mmHg) | 72±8 | 71±9 | 0.747 | 0.450 |
| HR (bpm) | 79±20 | 75±17 | 1.373 | 0.170 |
| LVEF (%) | 63±9 | 53±11 | 4.679 | 0.001 |
| Peak CK-MB (U/l) | 170±56 | 210±48 | 4.885 | 0.010 |
Procedural characteristics
The PCI procedures were observed to be successful in
all patients in the two groups. The post-procedural CTFC in group A
was significantly lower than that in group B (23±7 versus 29±11,
respectively; P=0.000), while the post-procedural TMPG 2–3 ratio in
group A was significantly higher than that in group B (71.3 versus
53.7%, respectively; P=0.030). There was significant difference in
the ratio of complete STR between groups A and B at 90 min
subsequent to PCI. (72.5 versus 55.9%, respectively; P=0.04).
However, considerable improvements in epicardial coronary flow were
observed in the two groups immediately following the procedure.
There were no statistically significant differences in the final
TIMI-3 flow between the two groups (92.5 versus 91.5% for groups A
and B, respectively; P=0.956; Table
II).
| Table II.Angiographic and procedural
features. |
Table II.
Angiographic and procedural
features.
| Variables | Group A (n=80) | Group B (n=82) | t/χ2 | P-value |
|---|
| Pain onset to PCI
(h) | 5.5±2.2 | 6.0±2.5 | 1.350 | 0.180 |
| Door to PCI
(min) | 70±9 | 68±11 | 1.265 | 0.210 |
| IRA | | | 1.114 | 0.573 |
| LAD | 44 (55.0) | 45 (54.9) | | |
| LCX | 16 (20.0) | 12 (14.6) | | |
| RCA | 20 (25.0) | 25 (30.5) | | |
| Stent diameter
(mm) | 3.1±0.3 | 3.2±0.4 | 1.797 | 0.070 |
| Stent length
(mm) | 21.2±6.5 | 20.1±7.2 | 1.020 | 0.310 |
| Initial TIMI
(%) | | | 0.080 | 0.929 |
| 0 | 60 (75.0) | 61 (74.4) | | |
| 1–2 | 20 (25.0) | 21 (25.6) | | |
| Final TIMI 3
(%) | 74 (92.5) | 75 (91.5) | 0.003 | 0.956 |
| Final CTFC
(frames) | 23±7 | 29±11 | 4.130 | 0.000 |
| Final TMPG 2–3
(%) | 57 (71.3) | 44 (53.7) | 4.351 | 0.030 |
| Complete STR
(%) | 58 (72.5) | 46 (55.9) | 4.540 | 0.040 |
No statistically significant differences were
observed in stent diameter and stent length between the two groups
following PCI. At discharge, there were no differences in the rate
of use of aspirin, clopidogrel, β-blockers, angiotensin converting
enzyme inhibitors or statins.
Feasibility and safety
A transient systolic pressure drop below 90 mmHg
occurred in three patients in group A (3.75%) and none in group B.
There were no severe hemorrhage symptoms in either group. The
occurrence of minor bleeding events in group A (3.75%) was not
significantly higher than that in group B (6.1%; P>0.05).
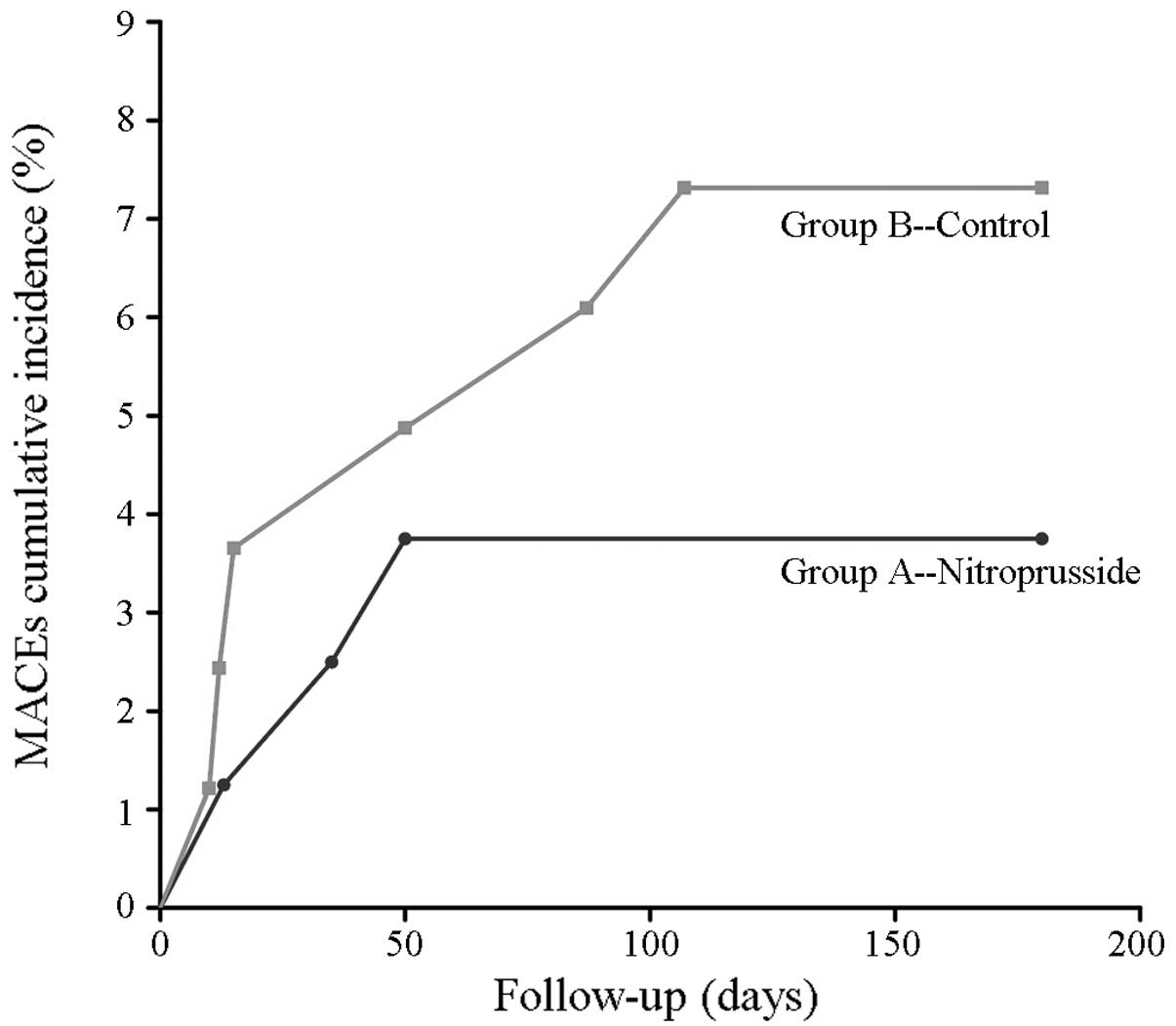
Follow-up results at 6 months
By 6 months, the LVEF was higher in group A (63±9
versus 53±11 for groups A and B, respectively; P<0.01). The
Kaplan-Meier analysis showed that the separation trend of the two
curves appeared to continue subsequent to the 6 months. The rates
of cardiac death, reinfarction and target-vessel revascularization
in group A were 1.25% (1/80), 1.25% (1/80) and 1.25% (1/80),
respectively, while in group B the rates were 3.66% (3/82), 1.22%
(1/82) and 2.44% (2/82), respectively. The incidence of major
adverse cardiac events (MACEs) was not statistically different
between the two groups (P>0.05), although there was a trend
indicating improvement in group A (log rank χ2=0.953,
P=0.489; Fig. 1).
Discussion
The results of the present study suggested that the
combination of a fixed dose of sodium NTP (100 μg) and
tirofiban, delivered via a thrombus aspiration catheter, was an
effective strategy to prevent NR in patients with STEMI undergoing
primary PCI. This study revealed several notable clinical
implications, such as the fact that NTP plus tirofiban was more
effective than tirofiban alone in improving the final CTFC, STR and
TMBG of the IRA. Furthermore, the direct administration of NTP to
the IRA via the thrombus aspiration catheter was generally safe and
reasonably well tolerated. In addition, the peak creatine kinase
(CK)-MB value was lower and the LVEF value was higher in group A
than in group B. However, the incidence of MACEs was not
statistically different between the two groups, although there was
a trend indicating improvement in group A.
The causes of NR are complex and multifactorial. The
most likely causes include platelet aggregation, distal
embolization, spasm of the microcirculation, neutrophilic plugging,
tissue edema or a combination of these factors (12). Prevention comprises strategies
adopted prior to complete vessel re-opening, in order to prepare
the microcirculation for reperfusion. Prevention strategies may be
targeted to the different mechanisms of NR. Manual aspiration
thrombectomy is reasonable for patients undergoing primary PCI.
However, infarct size was not reduced by manual aspiration
thrombectomy in the INFUSE-AMI trial of patients with large
anterior STEMI (13). This may be
due to the complex nature of NR, in which remote thromboembolism
plays only a partial role. However, of the several mechanisms that
have been proposed to explain the NR phenomenon, vasoconstriction
is considered one of the most important and potentially reversible,
as suggested by the numerous positive reports of therapeutic
vasodilatation in this context.
NTP is a direct donor of nitric oxide (NO) and
requires no intracellular metabolism to generate NO (14). It has been shown that IC NTP may
lead to coronary hyperemia. Furthermore, IC NTP produces an
equivalent, but more prolonged, coronary hyperemia to adenosine.
Therefore, we postulated that NTP was likely to have a beneficial
effect on the prevention of the NR phenomenon. However, the present
study differs from previous studies in a number of respects. In
previous studies, NTP was administered following the appearance of
slow or no reflow, whereas in the present study the combination of
NTP plus tirofiban was administered before balloon dilatation and
prior to the appearance of slow or no reflow. Furthermore, in
previous studies, NTP was predominantly injected into the coronary
artery through the guiding catheter, whereas in the present study,
NTP was injected through the thrombus aspiration catheter into the
distal coronary artery to reach the occluded target lesion. The
dose used in the present study is probably equivalent to a higher
dose given nonselectively, as described in some of the previous
studies. Therefore, the positive clinical findings of the present
study were most likely due to the fact that in the clinical
situation sodium NTP may alter the pathophysiology underlying the
NR. NO may positively affect latent collaterals or collateral blood
flow by eliciting vasodilatation or inhibiting platelet aggregation
in the vascular bed distal to the target lesion (15,16).
The results from the present study indicated that the delivery
method used in the study was more effective than the methods used
in previous studies.
The doses of NTP that have been shown to effectively
treat NR have been variable, ranging from 50 to 1,000 μg
(7,17,18).
In these previous studies, the final cumulative dose was not
predefined, but was rather dictated by the ability to achieve
satisfactory coronary flow and myocardial blush. We chose to use
100 μg based on previous studies suggesting that doses from
0.3 to 0.9 μg/kg achieved maximal coronary vasodilatation in
normal coronary arteries (19). An
earlier study showed that in patients with STEMI, selective IC
administration of a fixed dose (60 μg) of NTP failed to
improve coronary flow and myocardial tissue reperfusion; however,
clinical outcomes were improved at 6 months (20). The combination therapy of the
PercuSurge device and 100 μg NTP has been demonstrated to
provide an additional benefit to NTP alone for improving
microvascular circulation (9).
However, that study was nonrandomized and uncontrolled. The choice
of using a fixed, rather than a weight-based, dose was based upon
simplicity and ease. The use of a distal injection, however, has
the potential to accurately deliver medications irrespective of the
proximal arterial flow.
The present study revealed positive results with
regard to the epicardial flow grade and also with regard to the
myocardial perfusion grade, which is thought to reflect the
functionality of the coronary microvascular circulation (21). Both the TMPG and the CTFC have been
shown to be associated with the extent of STR, enzymatic infarct
size, nonreperfusion as defined by myocardial contrast
echocardiography, left ventricular function and long-term mortality
(9,22–26).
It was observed in the present study that the final TMPG and CTFC
in group A were significantly better than those in group B.
In the present study, selective IC NTP and tirofiban
administration via a thrombus aspiration catheter was safe and
well-tolerated. NTP is a potent vasodilator, and the intravenous
systemic administration of NTP may sometimes markedly reduce blood
pressure. However, the fixed dosage (100 μg) used in this
study did not result in the severe or prolonged hypotension that
may have triggered a shock state.
The results of this study revealed a lower peak
CK-MB value and improved TMPG, CTFC and STR trends in group A,
which reflected an enhanced myocardial reperfusion and greater
myocardial salvage. This may have resulted in a reduction in the
incidence of composite clinical end-points. The LVEF at 6 months
was higher in group A than in group B, although the incidence of
MACEs was not identified to be statistically different between the
two groups. However, there was a trend indicating improvement in
group A. The sample size in the study may have been too small to
adequately display the significance. A further study with a larger
sample size and a longer follow-up period is required to further
elucidate the effect of thrombus aspiration in combination with
tirofiban plus NTP on the composite clinical end-points.
References
|
1.
|
Grines CL, Browne KF, Marco J, et al The
Primary Angioplasty in Myocardial Infarction Study Group: A
comparison of primary angioplasty with thrombolytic therapy for
acute myocardial infarction. N Engl J Med. 328:673–679. 1993.
View Article : Google Scholar : PubMed/NCBI
|
|
2.
|
Lee CH and Tse HF: Microvascular
obstruction after percutaneous coronary intervention. Catheter
Cardiovasc Interv. 75:369–377. 2010.PubMed/NCBI
|
|
3.
|
Eeckhout E and Kern MJ: The coronary
no-reflow phenomenon: a review of mechanisms and therapies. Eur
Heart J. 22:729–739. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
4.
|
Tesic MB, Stankovic G, Vukcevic V and
Ostojic MC: The use of intracoronary sodium nitroprusside to treat
no-reflow after primary percutaneous coronary intervention in acute
myocardial infarction. Herz. 35:114–118. 2010.
|
|
5.
|
Burzotta F, Trani C, Romagnoli E, et al:
Manual thrombus-aspiration improves myocardial reperfusion: the
randomized evaluation of the effect of mechanical reduction of
distal embolization by thrombus-aspiration in primary and rescue
angioplasty (REMEDIA) trial. J Am Coll Cardiol. 46:371–376. 2005.
View Article : Google Scholar
|
|
6.
|
Chaitman BR and Lim MJ: No reflow and the
quest to achieve optimal perfusion during the acute phase of
myocardial infarction. J Am Coll Cardiol. 44:313–315. 2004.
View Article : Google Scholar : PubMed/NCBI
|
|
7.
|
Pasceri V, Pristipino C, Pelliccia F, et
al: Effects of the nitric oxide donor nitroprusside on no-reflow
phenomenon during coronary intervention for acute myocardial
infarction. Am J Cardiol. 95:1358–1361. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
8.
|
Gibson CM, Cannon CP, Daley WL, et al:
TIMI frame count: a quantitative method of assessing coronary
artery flow. Circulation. 93:879–888. 1996. View Article : Google Scholar : PubMed/NCBI
|
|
9.
|
Gibson CM, Cannon CP, Murphy SA, et al:
Relationship of TIMI myocardial perfusion grade to mortality after
administration of thrombolytic drugs. Circulation. 101:125–130.
2000. View Article : Google Scholar : PubMed/NCBI
|
|
10.
|
TIMI Study Group: The Thrombolysis in
Myocardial Infarction (TIMI) trial. Phase I findings. N Engl J Med.
312:932–936. 1985. View Article : Google Scholar : PubMed/NCBI
|
|
11.
|
Hamada S, Nishiue T, Nakamura S, et al:
TIMI frame count immediately after primary coronary angioplasty as
a predictor of functional recovery in patients with TIMI 3
reperfused acute myocardial infarction. J Am Coll Cardiol.
38:666–671. 2001. View Article : Google Scholar
|
|
12.
|
Rezkalla SH and Kloner RA: Coronary
no-reflow phenomenon: from the experimental laboratory to the
cardiac catheterization laboratory. Catheter Cardiovasc Interv.
72:950–957. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
13.
|
Stone GW, Maehara A, Witzenbichler B, et
al: Intracoronary abciximab and aspiration thrombectomy in patients
with large anterior myocardial infarction: the INFUSE-AMI
randomized trial. JAMA. 307:1817–1826. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
14.
|
Bates JN, Baker MT, Guerra R Jr and
Harrison DG: Nitric oxide generation from nitroprusside by vascular
tissue-evidence that reduction of the nitroprusside anion and
cyanide loss are required. Biochem Pharmacol. 42(Suppl): S157–S165.
1991. View Article : Google Scholar : PubMed/NCBI
|
|
15.
|
Hillegass WB, Dean NA, Liao L, Rhinehart
RG and Myers PR: Treatment of no-reflow and impaired flow with the
nitric oxide donor nitroprusside following percutaneous coronary
interventions: Initial human clinical experience. J Am Coll
Cardiol. 37:1335–1343. 2001. View Article : Google Scholar
|
|
16.
|
Traverse JH, Kinn JW, Klassen C, Duncker
DJ and Bache RJ: Nitric oxide inhibition impairs blood flow during
exercise in heart with a collateral dependent myocardial region. J
Am Coll Cardiol. 31:67–74. 1997. View Article : Google Scholar
|
|
17.
|
Hillegass WB, Dean NA, Liao L, Rhinehart
RG and Myers PR: Treatment of no-reflow and impaired flow with the
nitric oxide donor nitroprusside following percutaneous coronary
interventions: initial human clinical experience. J Am Coll
Cardiol. 37:1335–1343. 2001. View Article : Google Scholar
|
|
18.
|
Barcin C, Denktas AE, Lennon RJ, et al:
Comparison of combination therapy of adenosine and nitroprusside
with adenosine alone in the treatment of angiographic no-reflow
phenomenon. Catheter Cardiovasc Interv. 61:484–491. 2004.
View Article : Google Scholar
|
|
19.
|
Parham WA, Bouhasin A, Ciaramita JP,
Khoukaz S, Herrmann SC and Kern MJ: Coronary hyperemic dose
responses of intracoronary sodium nitroprusside. Circulation.
109:1236–1243. 2004.PubMed/NCBI
|
|
20.
|
Amit G, Cafri C, Yaroslavtsev S, et al:
Intracoronary nitroprusside for the prevention of the no-reflow
phenomenon after primary percutaneous coronary intervention in
acute myocardial infarction. Am Heart J. 152:e9–e14. 2006.
View Article : Google Scholar
|
|
21.
|
Youssef AA, Wu CJ, Hang CL, et al: Impact
of PercuSurge device conjugative with intracoronary administration
of nitroprusside on no-reflow phenomenon following primary
percutaneous coronary intervention. Circ J. 70:1538–1542. 2006.
View Article : Google Scholar
|
|
22.
|
van 't Hof AW, Liem A, Suryapranata H,
Hoorntje JC, de Boer MJ and Zijlstra F; Zwolle Myocardial
Infarction Study Group: Angiographic assessment of myocardial
reperfusion in patients treated with primary angioplasty for acute
myocardial infarction: myocardial blush grade. Circulation.
97:2302–2306. 1998.
|
|
23.
|
Lepper W, Sieswerda GT, Vanoverschelde JL,
et al: Predictive value of markers of myocardial reperfusion in
acute myocardial infarction for follow-up left ventricular
function. Am J Cardiol. 88:1358–1363. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
24.
|
Angeja BG, Gunda M, Murphy SA, et al: TIMI
myocardial perfusion grade and ST segment resolution: association
with infarct size as assessed by single photon emission computed
tomography imaging. Circulation. 105:282–285. 2002.
|
|
25.
|
Gibson CM, Cannon CP, Murphy SA, et al:
Relationship of the TIMI myocardial grades, flow grades, frame
count, and percutaneous coronary intervention to long-term outcomes
after thrombolytic administration in acute myocardial infarction.
Circulation. 105:1909–1913. 2002. View Article : Google Scholar
|
|
26.
|
Stone GW, Peterson MA, Lansky AJ, Dangas
G, Mehran R and Leon MB: Impact of normalized myocardial perfusion
after successful angioplasty in acute myocardial infarction. J Am
Coll Cardiol. 39:591–597. 2002. View Article : Google Scholar
|