Introduction
Fat embolism syndrome (FES) is a severe complication
of orthopedic surgery or trauma. It occurs in ∼1.29% of patients
with multiple fractures, particularly those with a femoral fracture
(1). Typically, it triggers the
development of pulmonary fat embolism (PFE), which has been
reported to be present in 82% of trauma patients (2). The acute consequences of fat embolism
are hemodynamic disorders and, in severe cases, right-sided heart
failure or hypoxemia (3,4). Intraoperative cardiovascular
deterioration, as a result of the pulmonary embolization of bone
marrow fat, is a potential complication (5). Although numerous animal models that
reveal many aspects of PFE have been developed (5–9), the
underlying mechanisms of the syndrome, including the early
hemodynamic effects, the potential inflammatory responses and the
risk factors of PFE, are not fully understood. The aim of the
present study was to develop a clinically relevant animal model,
and to investigate the initial changes in the hemodynamics,
cytokines, arterial blood gases and the risk factors involved in
PFE that are caused by femoral intramedullary procedures.
Subjects and methods
Subjects
The study was approved by the Animal Research
Committee of the Chinese People’s Liberation Army (PLA) General
Hospital (Beijing, China). Sixteen healthy male outbred dogs
(weight, 14.7–22.3 kg), were randomly divided into two groups:
Group A (intramedullary reaming and bone cement injection, n=8) and
Group B (surgical approach without opening the medullar cavity,
n=8).
Surgical procedure and measurement of
biochemical parameters
Anesthesia was induced with an intravenous injection
of sodium pentobarbital (30 mg/kg), and maintained with a
continuous infusion (5 mg/kg/min). Each dog was orally intubated
with an endotracheal tube, and mechanically ventilated with a
Servo-i Ventilator [Maquet, Inc., Rastatt, Germany; basic setting:
volume control ventilation, initial rate 18/min and tidal volume 12
ml/kg; I:E=1:2; positive end expiratory pressure (PEEP), 4 cm
H2O; and FiO2, 40%] during the experiment. A
pulmonary artery catheter (Arrow International, Inc., Reading, PA,
USA) was inserted through the external jugular vein. A pulse
contour cardiac output (PiCCO) hot dilated catheter was inserted
via femoral cut-down and connected to the PiCCO monitor (PiCCO
Plus, Pulsion Medical System AG, Munich, Germany) for the
determination of pulmonary and systemic hemodynamics. The
biochemical parameters, including hemodynamic parameters, arterial
blood gases and cytokine levels, were measured. Hemodynamic data
were recorded at specific time points, and blood samples were
collected for the measurement of arterial blood gases and cytokine
levels at such time points (Fig.
1). The biochemical parameters comprised heart rate (HR), mean
arterial pressure (MAP), central venous pressure (CVP), mean
pulmonary arterial pressure (MPAP), pulmonary capillary wedge
pressure (PCWP) and extravascular lung water (EVLW). In the
arterial blood gas tests, the pH, arterial oxygen tension
(PaO2) and arterial carbon dioxide tension
(PaCO2) were evaluated. In addition, the cytokine levels
that were measured were those of tumor necrosis factor-α (TNF-α),
interleukin-1β (IL-1β) and IL-6. The time points at which
measurements were taken were as follows: T0, prior to surgery; T1,
prior to unilateral medullary reaming; T2, following the first
unilateral medullary reaming; T3, following the second unilateral
medullary reaming; T4, following the third unilateral medullary
reaming; T5, prior to unilateral bone cement injection; T6, 5 min
following unilateral bone cement injection; T7, following
unilateral femur surgery; T8, following bilateral femur surgery;
T9, 60 min following bilateral femur surgery; T10, 240 min
following bilateral femur surgery.
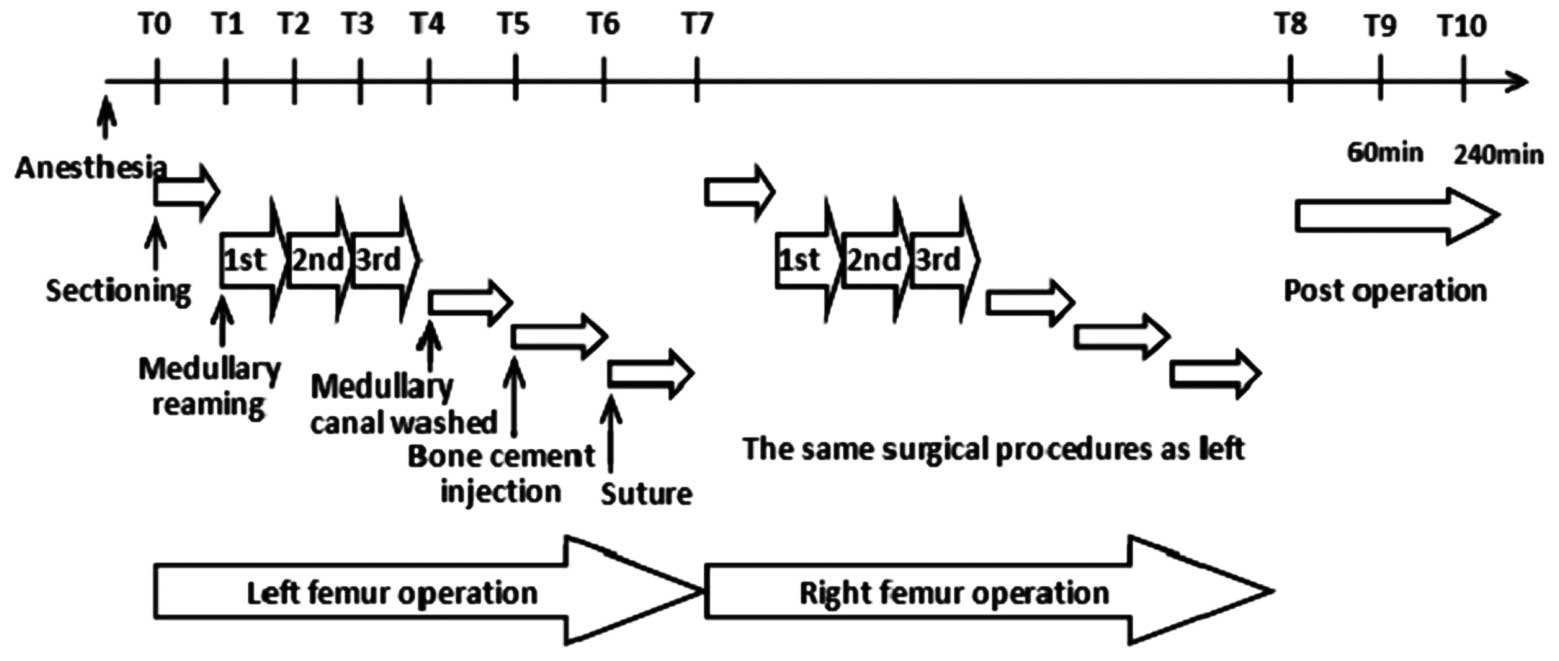 | Figure 1.Surgical approaches and associated
time points. T0, prior to surgery; T1, prior to unilateral
medullary reaming; T2, following the first unilateral medullary
reaming; T3, following the second unilateral medullary reaming; T4,
following the third unilateral medullary reaming; T5, prior to
unilateral bone cement injection; T6, 5 min following unilateral
bone cement injection; T7, following unilateral femur surgery; T8,
following bilateral femur surgery; T9, 60 min following bilateral
femur surgery; T10, 240 min following bilateral femur surgery. |
In Group A, the greater lateral trochanter of the
left femur was resected through a muscle gap by the posterior
lateral femur approach. The intertrochanteric fossa and entry of
the medullary canal were exposed and followed by intramedullary
reaming to one-half the length of the femur. The medullary canal
was washed with saline to remove destroyed myeloid tissues, and
dried with gauze. Bone cement (Tianjin Synthetic Material Research
Institute, Hexi, China) was prepared by manually stirring the
powder into the solution at a ratio of 2:1, until a dough was
formed, which was then used to fill the medullary canal. When
completely solidified, the incision was sutured. The same surgical
approaches were repeated in the right femurs of the dogs in Group
A. The femurs of the dogs in Group B were subjected to the same
surgical methods as those in Group A, with the exception of the
resection of the greater trochanter and the opening of the
medullary cavity. The anesthetized dogs were sacrificed by the
intravenous injection of 5 ml potassium chloride (15 meq) 240 min
following bilateral femur surgery. Necropsies were performed
immediately following sacrifice, to obtain the right and left
lungs. Oil Red O staining was used to identify the presence of
fatty deposits in these tissues.
Statistical analysis
Data are presented as the mean ± standard deviation.
The mean differences between the study groups and within groups
among different time points were analyzed by analysis of variance
(ANOVA) for repeated measures. Correlations between variables were
analyzed and expressed as correlation coefficients. P<0.05 was
considered to indicate a statistically significant difference. The
statistical analysis was performed using SPSS 13.0 for Windows
(SPSS, Inc., Chicago, IL, USA).
Results
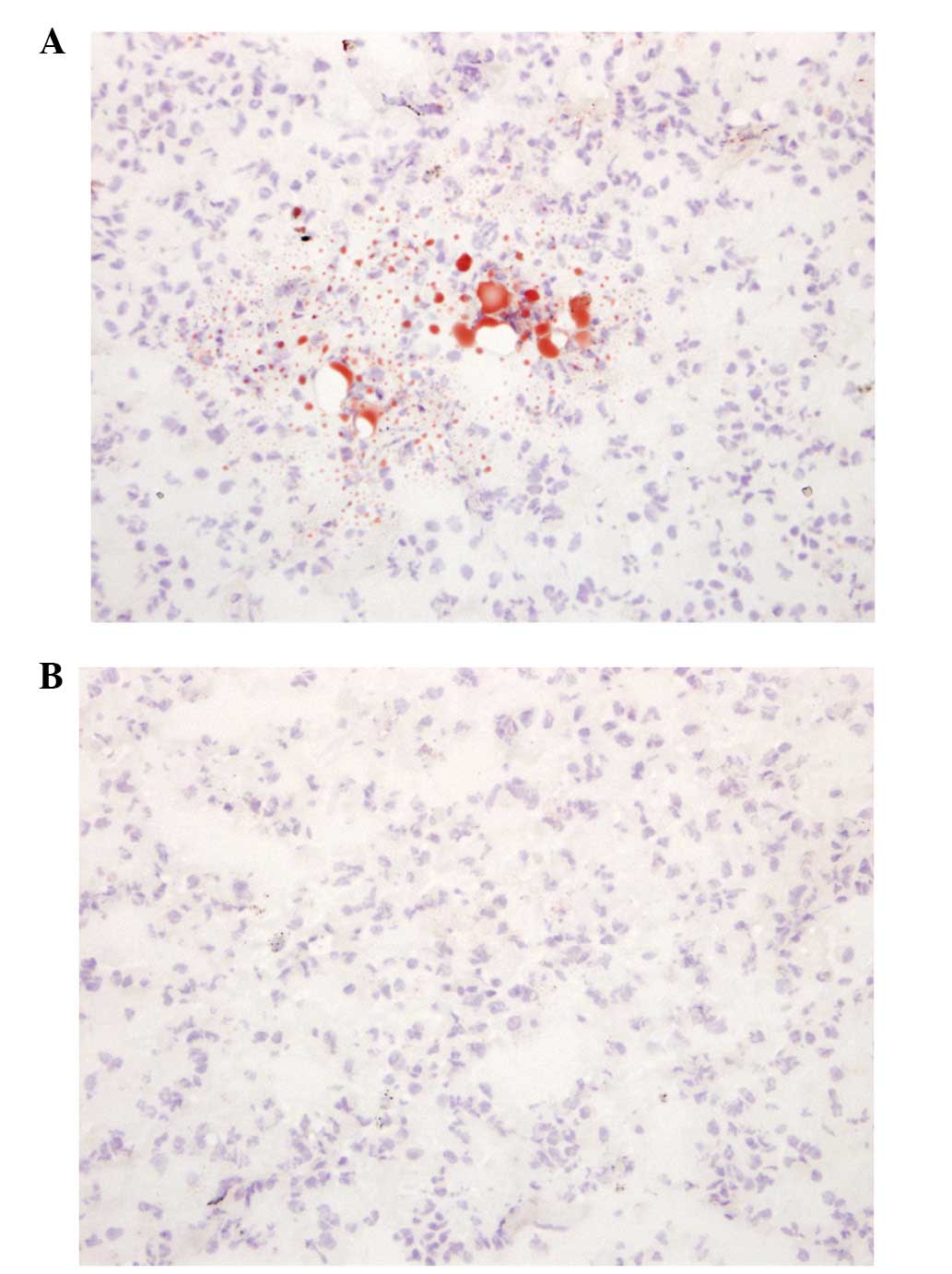
All animals survived the experimental procedure. In
all lung sections from Group A, fat emboli stained by Oil Red O
were observed, which demonstrated that the animals had developed
PFE (Fig. 2A). However, no fat
emboli were identified in any of the lung sections from Group B
(Fig. 2B).
Figs. 3A and B
demonstrate the changes in the hemodynamics in Group A. The HR,
CVP, MPAP, PCWP and EVLW increased, while the MAP decreased,
immediately following the reaming and bone cement infusion,
compared with those values at T0. In addition, the values at T4 and
T6 were significantly different from those at T0 (P<0.05).
Changes in the HR, MAP and PCWP were observed at T10; the values of
the parameters were no longer significantly different from those at
T0 (P>0.05). By contrast, the CVP, MPAP and EVLW remained high
at this time point, compared with those at T0 (P<0.05). However,
there were no significant differences in the hemodynamics in Group
B (P>0.05). Significant differences were identified in the HR,
MAP, and PCWP at T8, as well as in the CVP, MPAP and EVLW at T8, T9
and T10 in Group A (Table I),
compared with those in Group B.
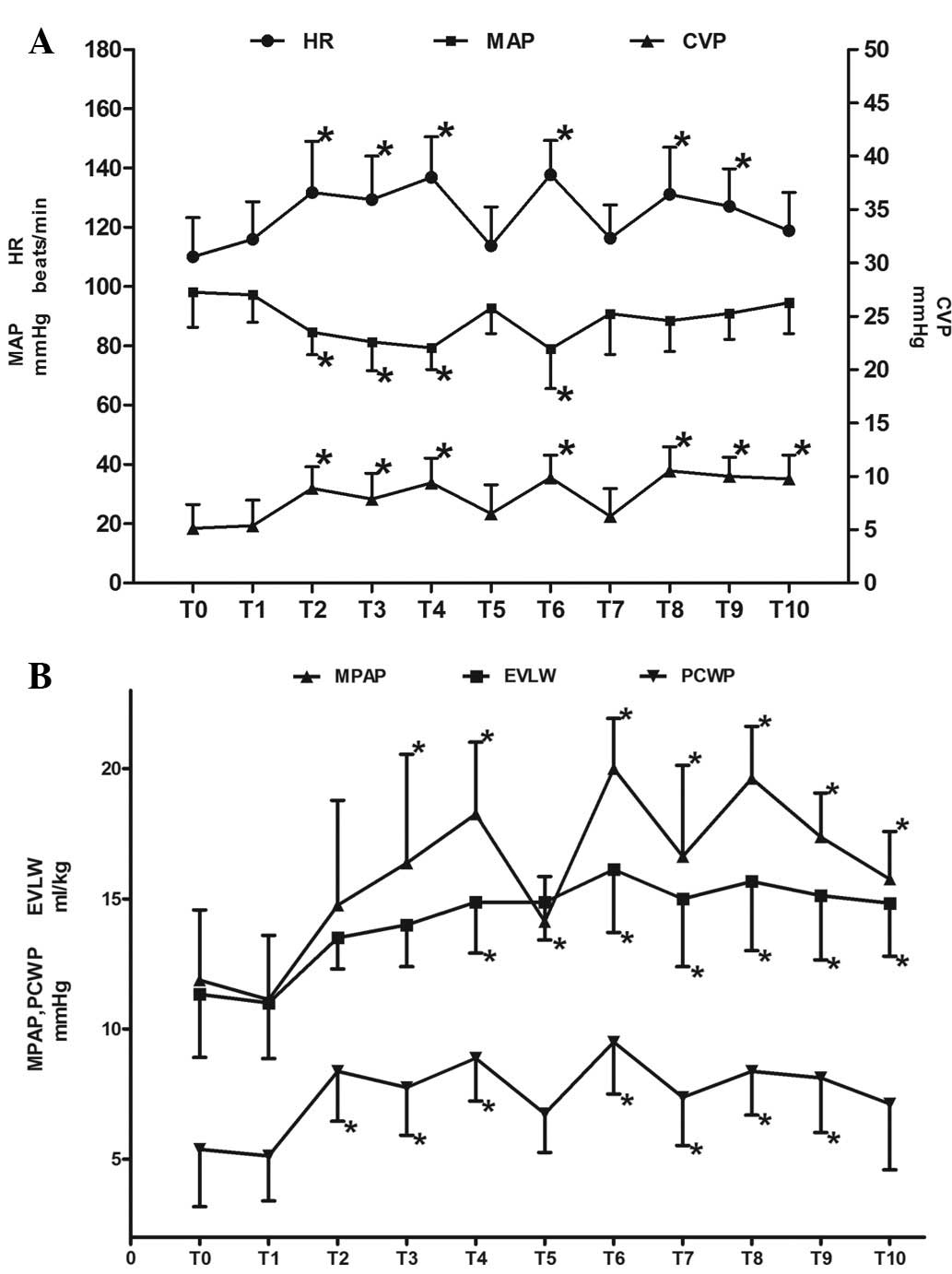 | Figure 3.Alterations in the hemodynamic
paramters at various time points during and following
intramedullary surgery in Group A. (A) Changes in heart rate (HR),
mean arterial pressure (MAP) and central venous pressure (CVP). (B)
Changes in mean pulmonary arterial pressure (MPAP), extravascular
lung water (EVLW) and pulmonary capillary wedge pressure (PCWP).
*P<0.05 vs. T0. T0, prior to surgery; T1, prior to
unilateral medullary reaming; T2, following the first unilateral
medullary reaming; T3, following the second unilateral medullary
reaming; T4, following the third unilateral medullary reaming; T5,
prior to unilateral bone cement injection; T6, 5 min following
unilateral bone cement injection; T7, following unilateral femur
surgery; T8, following bilateral femur surgery; T9, 60 min
following bilateral femur surgery; T10, 240 min following bilateral
femur surgery. |
 | Table I.Hemodynamic data summary for Groups A
and B. |
Table I.
Hemodynamic data summary for Groups A
and B.
| Parameter | Group | T0 | T1 | T7 | T8 | T9 | T10 |
|---|
| HR (beats/min) | A | 110.13±13.18 | 116.00±12.71 | 116.38±11.17 | 131.13±15.91 | 127.13±12.68 | 118.88±12.84 |
| B | 115.63±12.93 | 117.13±10.30 | 118.38±9.10 | 116.13±7.86a | 120.62±10.41 | 117.50±10.18 |
| MAP (mmHg) | A | 98.13±11.79 | 97.25±9.32 | 90.88±13.71 | 88.50±10.41 | 91.00±8.72 | 94.63±10.42 |
| B | 100.13±9.33 | 97.75±9.22 | 98.00±6.01 | 101.25±6.34a | 99.38±6.25 | 101.38±5.73 |
| CVP (mmHg) | A | 5.13±2.23 | 5.38±2.39 | 6.25±2.60 | 10.50±2.27 | 10.00±1.77 | 9.75±2.25 |
| B | 5.12±1.36 | 5.00±1.76 | 4.88±1.13 | 5.25±1.28a | 5.50±1.51a | 5.38±1.19a |
| MPAP (mmHg) | A | 11.88±2.70 | 11.13±2.47 | 16.63±3.50 | 19.63±1.99 | 17.38±1.69 | 15.75±1.83 |
| B | 10.88±2.90 | 10.63±1.85 | 11.13±2.99 | 12.12±2.18a | 11.37±2.50a | 11.87±3.04a |
| PCWP (mmHg) | A | 5.38±2.20 | 5.13±1.73 | 7.38±1.85 | 8.37±1.69 | 8.13±2.10 | 7.12±2.53 |
| B | 5.50±2.45 | 5.63±2.20 | 5.38±1.19 | 5.75±1.04a | 6.13±1.36 | 6.63±1.41 |
| EVLW (ml/kg) | A | 11.33±2.42 | 11.00±2.14 | 15.00±2.61 | 15.67±2.66 | 15.13±2.47 | 14.83±2.04 |
| B | 11.13±3.48 | 10.50±1.77 | 11.25±2.66a | 10.75±2.49a | 10.63±1.99a | 11.37±1.77a |
Group A demonstrated reductions in the pH and the
PaO2, but an increase in the PaCO2, at T8,
which were significantly different compared with those at T0
(P<0.05; Table II). Although
there was an increase in the pH and the PaO2, and a
reduction in the PaCO2, at T10, the PaCO2
(46.6±7.5 mmHg) remained high and was significantly different
compared with that at T0 (P<0.05). The PaO2 was
correlated with the EVLW [linear correlation coefficient, −0.5664;
95% confidence interval (CI), −12.181 to −3.614; P<0.001].
Similar results were identified between PaCO2 and EVLW
(linear correlation coefficient, 0.3560; 95% CI, 0.02409–2.216;
P=0.046). However, no significant changes were observed in the
arterial blood gases in Group B. Significant differences were
identified in the PaCO2 at T8, as well as in the
PaO2 at T7 and T8, between Group B and Group A (Table II).
| Table II.Parameters of arterial blood gases
analyzed at different time points in Groups A and B. |
Table II.
Parameters of arterial blood gases
analyzed at different time points in Groups A and B.
| Parameter | Group | T0 | T7 | T8 | T10 |
|---|
| pH | A | 7.420±0.075 | 7.370±0.062 | 7.336±0.072a | 7.360±0.065 |
| B | 7.399±0.068 | 7.414±0.066 | 7.386±0.088 | 7.396±0.047 |
| PaO2
(mmHg) | A | 191.1±34.1 | 180.1±38.7a | 156.4±30.9a | 186.5±34.2 |
| B | 206.8±45.2 | 212.1±50.8b | 208.3±49.1b | 202.4±28.6 |
| PaCO2
(mmHg) | A | 36.6±6.0 | 43.6±7.7 | 48.4±7.6a | 46.6±7.5a |
| B | 38.5±6.3 | 40.1±7.0 | 39.8±4.4b | 39.3±2.4 |
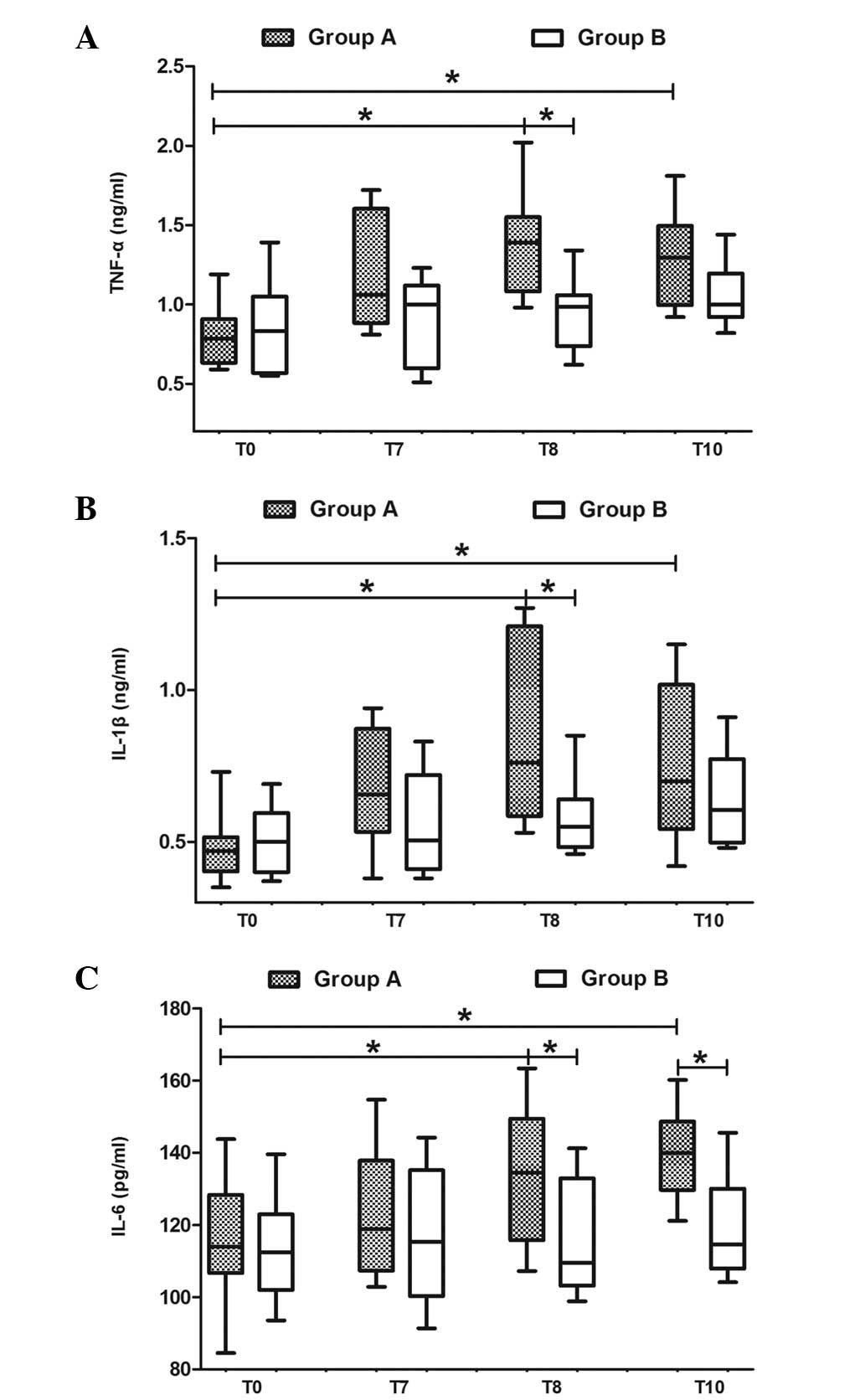
Following the surgery, there were increases in the
TNF-α, IL-1β and IL-6 levels in Group A. Significant differences
were observed in the TNF-α levels at T8 and T10, as well as in the
IL-1β and IL-6 levels at T8 and T10, compared with those at T0
(P<0.05; Fig. 4). However,
there were no significant differences in the levels of these
cytokines in Group B. There were significant differences in the
TNF-α and IL-1β levels at T8, as well as in the IL-6 levels at T8
and T10, in Group A, when compared with those in Group B
(P<0.05; Fig. 4).
Discussion
The present study demonstrated that femoral
intramedullary surgery may induce PFE and subsequently affect
hemodynamics and arterial blood gases. The EVLW was correlated with
the PaO2 and the PaCO2, and may serve as a
predictor of the development of FES. Cytokines were significant
during these procedures, and may be further predictors for the
development of FES. To the best of our knowledge, this study is the
first to demonstrate a correlation between the EVLW, cytokines and
FES, providing potential methods for the diagnosis and treatment of
FES.
The clinical manifestation of PFE ranges from no
impairment, in mild cases, to death, in severe cases (4). As for the pathogenesis of fat
embolism, there are currently two hypotheses; the mechanical
occlusion theory and the biochemical theory (10). In the most severe case, extensive
embolization has been shown to be associated with lung injury and
acute respiratory distress syndrome (ARDS) (11). With an enhanced understanding of
the disease, an increasing number of studies are currently
investigating the inflammatory response in PFE (12–15).
In a study on fat embolism in rats, Liu et al demonstrated
that serum TNF-α, IL-1β and neutrophil elastase levels were
increased in pulmonary alveolus irrigating solution, in accordance
with an altered lung weight and pulmonary hypertension, and an
increased capillary filtration coefficient (14). Blankstein et al identified
that the combination of hemorrhagic shock, resuscitation and fat
embolism elicited neutrophil activation, infiltration of the
alveoli by polymorphonuclear leukocytes and inflammatory cytokine
expression, in bronchoalveolar lavage fluid (12). Furthermore, serum IL-6 is
considered to be a potential early marker of fat embolism (13). The present study identified that
serum TNF-α, IL-1β and IL-6 levels were higher than those at the
baseline, following the surgical process. These results were
consistent with other animal studies (13,14),
as well as with certain clinical investigations (16,17).
This suggests that these inflammatory cytokines are important
during PFE, and subsequently lead to lung injury. Therefore, the
early removal of these inflammatory mediators is a potential target
of therapy.
Intraoperative cardiovascular deterioration, as a
result of pulmonary embolization of bone marrow fat, is a
potentially fatal complication during total hip and knee
arthroplasty, intramedullary nailing and spine surgery (18). It is important to correct the
hemodynamic changes caused by fat embolism. Therefore,
comprehensive studies of hemodynamics and early interventions are
required. Aebli et al conducted a study in which bone cement
was injected into the L1 vertebral bodies of six sheep, and
demonstrated that following the injection of the bone cement, there
were reflective reductions in the HR and arterial pressure, and
that the second reduction in the arterial pressure was caused by
secondary PFE (19). Similar
results were observed in the present study. Significant increases
in the HR, CVP, MPAP, PCWP and EVLW and a significant reduction in
the MAP occurred immediately following the reaming and bone cement
infusion processes. It was thought that the changes were associated
with the intramedullary procedures, leading to the release of bone
marrow particles and the formation of microthrombi in the pulmonary
artery. This was confirmed by Oil Red O staining of pulmonary
sections from the current study animals. Wheelwright et al
also concluded that pulmonary fat and marrow embolism were key
factors of cardiorespiratory and hemodynamic instability, following
canal pressurization (20). It is
likely that the methylmethacry-late monomer, acting as a systemic
vasodilator, is also a factor during this procedure (21).
Pathological examinations are able to reveal the
presence of alveolar edema and hemorrhage with multiple fat droplet
depositions and fibrin thrombi; however, chest radiography is
unable to locate these during the early stages of fat embolism
(16). EVLW is a useful measure of
the accumulation of parenchymal lung edema, and there has
previously been shown to be a significant correlation between EVLW
measurements indexed to all body weights and the severity of lung
injury in patients with ARDS (22). In the present study, the EVLW
levels remained continuously high from the completion of the
intramedullary procedure to 240 min following the bilateral femur
surgery. Furthermore, following the bilateral femoral
intramedullary procedure, there was a reduction in the pH and the
PaO2, and an increase in the PaCO2. The
cytokine levels, specifically those of TNF-α, IL-1β and IL-6, were
also higher compared with those prior to surgery. Thus, the
intramedullary surgery resulted in the formation of PFE and the
release of inflammatory cytokines. This increased the permeability
of the pulmonary microcirculation and the EVLW, which subsequently
resulted in a reduction in the PaO2 and an increase in
the PaCO2. The PaO2 and the PaCO2
were correlated with the EVLW (P<0.05), indicating that EVLW, as
an independent index, may be valuable in the evaluation of
pulmonary edema during the early stages of PFE.
The present study employed tracheal intubation,
general anesthesia and controlled mechanical ventilation
procedures. The basic settings of the ventilator remained
unchanged, and therefore minimized the influence of other factors
on respiration. The pathological results indicated that
intramedullary procedures were able to evoke PFE, which mainly
resulted in a reduced PaO2 and an increased
PaCO2 during surgery. Similar results have been
identified in other studies (6,23). A
potential reason for the induction of PFE may be that a fat embolus
entered the lung, which decreased the blood perfusion and exchange
area, and subsequently increased the dead space area.
Alternatively, in this study, as the basic settings of the
ventilator remained unchanged, the pulmonary edema caused by fat
embolism and the release of inflammatory cytokines may have
resulted in an increased airway pressure and a decreased tidal
volume. Bilateral procedures carry higher risks compared with
unilateral ones.
Although the results of the present study indicated
that the pulmonary tissue sections of all animals in Group A
exhibited fat particles, the present embolism model did not lead to
severe changes in clinical symptoms. Arterial blood gases and
certain hemodynamic parameters, such as HR and MAP, improved 240
min following the bilateral procedures (T10). These results were in
accordance with the fact that the majority of intramedullary
reaming processes do not induce FES (24). Discordance between the clinical and
experimental diagnosis of fat embolism, or ARDS, was mainly due to
pulmonary infiltration (25,26)
or compensation of the patient and the size of the fat embolus
(27). In a clinical study, Kim
revealed that 65% of patients who underwent bilateral knee joint
replacement and 46% of patients who underwent unilateral knee joint
replacement demonstrated positive Oil Red O staining of fat
particles in their blood (28).
Pitto et al studied patients with a femoral neck fracture
who received cemented total hip joint replacement and identified,
using transesophageal echocardiography (TEE), that 95% of the
patients had fat embolism presentations (29). The aforementioned studies suggest a
high prevalence of PFE induced by intramedullary procedures, with
PFE as a potential complication of such procedures. The treatment
options, such as clofibrate, dextran-40, ethyl alcohol, heparin and
aspirin, have been evaluated previously and shown to cause no
significant changes in the clinical outcomes of PFE and FES
(27,30). Strict monitoring of the
hemodynamics during surgery is essential if a patient has high risk
factors, such as multiple injuries and infection, in the clinical
setting. In the case of continuously abnormal hemodynamics, an
early intervention is required to prevent fat embolism from
developing into FES.
There were several limitations to this study. In
Group B, the surgery was conducted without opening the medullary
cavity. Therefore, it was not possible to compare the hemodynamic
parameters of the two groups during the surgical procedure in the
medullary cavity, such as medullary reaming and bone cement
injection. However, comparisons between Groups A and B demonstrated
that the animals in Group A were effective models in which to
evaluate PFE through postmortem pulmonary tissues. Furthermore, the
model allowed for the creation of fat embolism and the tracking of
the changes in cytokine levels and arterial blood gas parameters
during the surgical procedure. Another limitation of this study was
that the dogs were kept alive for only four hours following
surgery, and the risk factors were determined during the early
stages of PFE. Therefore, it was not possible to draw conclusions
regarding the development of fat embolism and inflammation over a
period of several days following the procedure. The focus was on
the initial impact of PFE, during or following the surgery.
Therefore, further experimental studies in animals are required to
investigate these possible events.
In conclusion, femoral intramedullary surgery may
induce PFE and affect the hemodynamics and arterial blood gases,
for example, by reducing the PaO2 and increasing the
PaCO2. The EVLW was demonstrated to correlate with the
PaO2 and the PaCO2, and may serve as a
predictor for the development of FES. Positive Oil Red O staining
in pulmonary tissue sections was observed in animals that received
intramedullary surgery, indicating the high prevalence of PFE
induced by such a surgical procedure. The serum concentrations of
TNF-α, IL-1β and IL-6 increased following the intramedullary
surgery, and these cytokines may therefore be a risk factor for the
development of FES.
References
|
1.
|
Stein PD, Yaekoub AY, Matta F and
Kleerekoper M: Fat embolism syndrome. Am J Med Sci. 336:472–477.
2008. View Article : Google Scholar : PubMed/NCBI
|
|
2.
|
Eriksson EA, Pellegrini DC, Vanderkolk WE,
Minshall CT, Fakhry SM and Cohle SD: Incidence of pulmonary fat
embolism at autopsy: an undiagnosed epidemic. J Trauma. 71:312–315.
2011. View Article : Google Scholar : PubMed/NCBI
|
|
3.
|
Ereth MH, Weber JG, Abel MD, et al:
Cemented versus noncemented total hip arthroplasty - embolism,
hemodynamics, and intrapulmonary shunting. Mayo Clin Proc.
67:1066–1074. 1992. View Article : Google Scholar : PubMed/NCBI
|
|
4.
|
Bolliger SA, Muehlematter K, Thali MJ and
Ampanozi G: Correlation of fat embolism severity and subcutaneous
fatty tissue crushing and bone fractures. Int J Legal Med.
125:453–458. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
5.
|
Krebs J, Ferguson SJ, Hoerstrup SP, Goss
BG, Haeberli A and Aebli N: Influence of bone marrow fat embolism
on coagulation activation in an ovine model of vertebroplasty. J
Bone Joint Surg Am. 90:349–356. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
6.
|
Blankstein M, Byrick RJ, Richards RR,
Mullen JB, Zdero R and Schemitsch EH: Pathophysiology of fat
embolism: a rabbit model. J Orthop Trauma. 25:674–680. 2011.
View Article : Google Scholar : PubMed/NCBI
|
|
7.
|
McIff TE, Poisner AM, Herndon B,
Lankachandra K, Molteni A and Adler F: Mitigating effects of
captopril and losartan on lung histopathology in a rat model of fat
embolism. J Trauma. 70:1186–1191. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
8.
|
Liu DD, Hsieh NK and Chen HI:
Histopathological and biochemical changes following fat embolism
with administration of corn oil micelles: a new animal model for
fat embolism syndrome. J Bone Joint Surg Br. 90:1517–1521.
2008.PubMed/NCBI
|
|
9.
|
McIff TE, Poisner AM, Herndon B, et al:
Fat embolism: evolution of histopathological changes in the rat
lung. J Orthop Res. 28:191–197. 2010.PubMed/NCBI
|
|
10.
|
Shaikh N: Emergency management of fat
embolism syndrome. J Emerg Trauma Shock. 2:29–33. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
11.
|
Fong DL, Murnane RD, Hotchkiss CE, Green
DJ and Hukkanen RR: Pulmonary embolization of fat and bone marrow
in cynomolgus Macaques (Macaca fascicularis). Comp Med.
61:86–91. 2011.PubMed/NCBI
|
|
12.
|
Blankstein M, Byrick RJ, Nakane M, et al:
Amplified inflammatory response to sequential hemorrhage,
resuscitation, and pulmonary fat embolism: an animal study. J Bone
Joint Surg Am. 92:149–161. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
13.
|
Yoga R, Theis JC, Walton M and Sutherland
W: Interleukin-6 as an early marker for fat embolism. J Orthop Surg
Res. 4:182009. View Article : Google Scholar : PubMed/NCBI
|
|
14.
|
Liu DD, Kao SJ and Chen HI:
N-acetylcysteine attenuates acute lung injury induced by fat
embolism. Crit Care Med. 36:565–571. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
15.
|
Kao SJ and Chen HI: Nitric oxide mediates
acute lung injury caused by fat embolism in isolated rat’s lungs. J
Trauma. 64:462–469. 2008.PubMed/NCBI
|
|
16.
|
Kao SJ, Yeh DY and Chen HI: Clinical and
pathological features of fat embolism with acute respiratory
distress syndrome. Clin Sci (Lond). 113:279–285. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
17.
|
Hsu YH, Kao SJ, Lee RP and Chen HI: Acute
pulmonary oedema: Rare causes and possible mechanisms. Clin Sci
(Lond). 104:259–264. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
18.
|
Krebs J, Ferguson SJ, Nuss K, et al:
Sildenafil prevents cardiovascular changes after bone marrow fat
embolization in sheep. Anesthesiology. 107:75–81. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
19.
|
Aebli N, Krebs J, Davis G, Walton M,
Williams MJ and Theis JC: Fat embolism and acute hypotension during
vertebroplasty: an experimental study in sheep. Spine. (Phila Pa
1976). 27:460–466. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
20.
|
Wheelwright EF, Byrick RJ, Wigglesworth
DF, et al: Hypotension during cemented arthroplasty. Relationship
to cardiac output and fat embolism. J Bone Joint Surg Br.
75:715–723. 1993.PubMed/NCBI
|
|
21.
|
Peebles DJ, Ellis RH, Stride SD and
Simpson BR: Cardiovascular effects of methylmethacrylate cement. Br
Med J. 1:349–351. 1972. View Article : Google Scholar : PubMed/NCBI
|
|
22.
|
Berkowitz DM, Danai PA, Eaton S, Moss M
and Martin GS: Accurate characterization of extravascular lung
water in acute respiratory distress syndrome. Crit Care Med.
36:1803–1809. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
23.
|
Whelan DB, Byrick RJ, Mazer CD, et al:
Posttraumatic lung injury after pulmonary contusion and fat
embolism: factors determining abnormal gas exchange. J Trauma.
69:512–518. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
24.
|
Kaufmann TJ, Jensen ME, Ford G, Gill LL,
Marx WF and Kallmes DF: Cardiovascular effects of
polymethylmethacrylate use in percutaneous vertebroplasty. AJNR Am
J Neuroradiol. 23:601–604. 2002.PubMed/NCBI
|
|
25.
|
Murphy P, Edelist G, Byrick RJ, Kay JC and
Mullen JB: Relationship of fat embolism to haemodynamic and
echocardio-graphic changes during cemented arthroplasty. Can J
Anaesth. 44:1293–1300. 1997. View Article : Google Scholar : PubMed/NCBI
|
|
26.
|
Lehnert BE: Pulmonary and thoracic
macrophage subpopulations and clearance of particles from the lung.
Environ Health Perspect. 97:17–46. 1992. View Article : Google Scholar : PubMed/NCBI
|
|
27.
|
Mellor A and Soni N: Fat embolism.
Anaesthesia. 56:145–154. 2001. View Article : Google Scholar
|
|
28.
|
Kim YH: Incidence of fat embolism syndrome
after cemented or cementless bilateral simultaneous and unilateral
total knee arthroplasty. J Arthroplasty. 16:730–739. 2001.
View Article : Google Scholar : PubMed/NCBI
|
|
29.
|
Pitto RP, Blunk J and Kössler M:
Transesophageal echocardiography and clinical features of fat
embolism during cemented total hip arthroplasty. A randomized study
in patients with a femoral neck fracture. Arch Orthop Trauma Surg.
120:53–58. 2000.
|
|
30.
|
Taviloglu K and Yanar H: Fat embolism
syndrome. Surg Today. 37:5–8. 2007. View Article : Google Scholar
|